Embed Size (px)
Citation preview

COMMUNICATION AND BRIEF REPORT
The Effect of Photodynamic Therapy on Contiguous UntreatedTumor
HUMBERTO CABRERA, PHD,*† JORGE CASTRO, MD,‡ HILDA C. GRASSI, MSC,§
EFREN D. J. ANDRADES, MSC,§ AND SANTOS A. LOPEZ-RIVERA, PHD¶
The authors have indicated no significant interest with commercial supporters.
Photodynamic therapy (PDT) is an antitumor
method that uses a nontoxic photosensitizer
and visible light to produce cytotoxic reactive oxy-
gen species (ROS) that destroy malignant cells. It
has been increasingly used in the treatment of non-
melanoma skin cancers, particularly basal cell car-
cinoma (BCC), providing a high degree of tumor
regression and excellent aesthetic results. We report
the case of a patient with histopathologically pro-
ven superficial BCC in which regression of
untreated contiguous tumor was noted after PDT.
Case Report
PDT was administered to a 60-year-old woman
with histopathologically proven superficial BCC
near the nasal tip. Informed consent was obtained
from the patient according to the approved proto-
col of the institutional ethics committee, which
was in agreement with the guidelines of the 1975
Declaration of Helsinki. The patient reported no
prior personal history of skin cancer and subse-
quently consented to PDT at the Plastic Surgery
Unit of the Hospital Oncology Service, Instituto
Venezolano de los Seguros Sociales. The physician
observed the vital signs of the patient as well as
the response of the tumor to the treatment during
the first minutes; at 6, 24, and 48 hours; at the first
week; weekly for 8 weeks; and every 3 months for
1 year.
The photosensitizer used in this treatment was the
commercial chlorin derivative Photolon (Chlorine
e6-PVP, Scientific Pharmaceutical Center, RUE
Belmedpreparaty, Minsk, Belarus). The drug dose
was 1.7 mg/kg of body weight diluted in 200 mL
of saline solution injected intravenously slowly
over a 20-minute period; the drug–light application
interval was 3 hours. The light source used was
the diode laser (ML-662-SP, Milon Laser Ltd.,
Sain-Peterburg, Russia) with 662-nm wavelength
and 2.5-W optical power, and the light dose was
100 J/cm2, delivered at a fluency rate of 170 mW/
cm2 with a 12-mm spot size, which covered only
the detected lesion.1 The patient was kept in the
dark from the application of the photosensitizer
until she left the hospital unit, during the night.
No serious side effects or complications during or
after treatment were observed other than transient
mild local pain and moderate edema followed by a
crusted ulcer formation after 1 week.
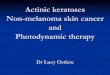
Figure 1 shows the 10-mm tumor zone before
PDT, including the area on the left of the photo-
*CEIF, Instituto Venezolano de Investigaciones Cientıficas, Merida, Venezuela; †International Centre for TheoreticalPhysics Abdus Salam, Trieste, Italy; ‡Unidad de Cirugıa Plastica, Servicio Oncologico Hospitalario, InstitutoVenezolano de los Seguros Sociales, Caracas, Venezuela; §Facultad de Farmacia y Bioanalisis, Universidad de LosAndes, Merida, Venezuela; ¶Laboratorio de Fısica Aplicada, Universidad de Los Andes, Merida, Venezuela
© 2012 by the American Society for Dermatologic Surgery, Inc. � Published by Wiley Periodicals, Inc. �ISSN: 1076-0512 � Dermatol Surg 2012;1–3 � DOI: 10.1111/j.1524-4725.2012.02400.x
1

graph that has no visual evidence of a tumor. Fig-
ure 2 shows that, after light treatment, the crust
formed on the area of the tumor and toward a
contiguous area that was not treated with light
(Figure 3). Although we have no direct evidence,
and because this was an unexpected result, we
assumed that the left untreated side of the irradi-
ated zone was part of the BCC. Healing occurred
within 3–4 weeks, with complete regression of the
tumor confirmed by biopsy, with the observation
period of 1 year without recurrence. The aesthetic
results were acceptable (Figure 4).
Discussion
Selective accumulation of chlorine e6-PVP in tumor
cells has already been demonstrated, and this is the
basis for selective PDT and diagnosis.2 Moreover,
according to this report, the e6-PVP induced cell
death via apoptosis and also via necrosis.2 Photo-
sensitizers are known to induce cell killing through
type I reactions in which electron transfer occurs
between the light-excited photosensitizer and cellu-
lar constituents or type II reactions that involve
energy transfer between the excited photosensitizer
and molecular oxygen to produce singlet oxygen.3
For Photolon, it has been demonstrated that the
mechanism of induced cell death involves the
induction of ROS through a type I mechanism.4
The fact that, even under normal physiologic con-
ditions, ROS can oxidize blood and structural pro-
teins and inhibit the proteolytic system can explain
Figure 1. Photograph showing the 10-mm basal cell carci-noma near the nasal tip before photodynamic therapy.
Figure 2. Seven days after photodynamic therapy, photo-graph showing crusted ulcer formation in a 10-mm treatedtumor and in a contiguous untreated zone.
Figure 3. Spot laser illumination over the treated tumorarea during photodynamic therapy.
Figure 4. Eighty days after photodynamic therapy. Healingof the tumor with epithelialization and acceptable aestheticresults.
CASE REPORT OF THE EFFECT OF PHOTODYNAMIC THERAPY
DERMATOLOGIC SURGERY2

this. During oxidation, proteins can lose amino
acids or can be fragmented. Those reactions lead
to alteration of structural proteins or alteration of
enzyme functions. Overall increases in the relative
level of organic hydroxyl, carbonyl, and carboxyl-
free radical groups (alkoxyl radical RO• half-life
1 ls, peroxyl radical ROO• half-life 7 seconds, and
hydroperoxyl radical ROOH•), generating a diffus-
ible effect that can extend to nearby tissue, accom-
pany protein and amino acid oxidation. Free
radicals produced by type II reactions have a half-
life that lasts from 1 ns to 10 ls (superoxide ion
O2•� 10 ls, singlet oxygen 1O2 1 ls. and hydroxyl
radical OH• 1 ns).5 This is in agreement with the
report of deeper and more-extensive necrosis in
patients treated with Photolon than in those trea-
ted with Radachlorin and Photoditazine1 which
may be acting through a type II reaction.
The findings of this study suggest that the necrosis
and regression of the untreated tumor area shown
in Figure 2 may be related to the ROS generated at
the irradiated tumor site. It may be that the diffu-
sion of these cytotoxic agents from the irradiated
zone to the neighborhood tumor zone causes the
simultaneous development of the necrosis also on
this untreated zone. This is in agreement with the
fact that BCC has greater microvessel density than
surrounding normal tissue.6
In summary, PDT with Photolon is an effective
method for the treatment of BCC that provides
acceptable functional and aesthetic results without
major adverse effects. We hypothesize that, in
addition to its direct effect on BCC tumor cells,
Photolon-PDT generates diffusible and relatively
stable ROS so as to produce regression of contigu-
ous untreated tumors.
References
1. Stranadko EF, Purtskhvanidze VA, Radaev AA. Photodynamic
therapy for skin cancer with chlorine derivatives under the
outpatient conditions. Proceedings of 13th EMLA Congress
2008; 59.
2. Chin WWL, Heng PWS, Thong PSP, Bhuvaneswari R, et al.
Improved formulation of photosensitizer chlorin e6
polyvinylpyrrolidone for fluorescence diagnostic imaging and
photodynamic therapy of human cancer. Eur J Pharm Biopharm
2008;69:1083–93.
3. Calzavara-Pinton PG, Venturini M, Sala R. Photodynamic
therapy: update 2006. Part 1. Photochemistry and photobiology.
J Eur Acad Dermatol Venereol 2007;21:293–302.
4. Copley L, van der Watt P, Wirtz KW, Parker MI, et al.
Photolon, a chlorin e6 derivative, triggers ROS production and
light-dependent cell death via necrosis. Int J Biochem Cell Biol
2008;40:227–35.
5. Finaud J, Lac G, Filaire E. Oxidative stress. Sports Med
2006;36:327–58.
6. Chu C-Y, Cha S-T, Lin W-C, Lu P-H, et al. Stromal-cell-derived
factor-1a (SDF-a/CXCL12)-enhanced angiogenesis of human
basal cell carcinoma cells involves ERK1/2-NF-j/interleukin-6pathway. Carcinogenesis 2009;30:205–13.
Address correspondence and reprint requests to:Humberto Cabrera, PhD, Instituto Venezolano deInvestigaciones Cientıficas, Carretera a Jajı,Km 29, Merida 5101, Venezuela, or e-mail:[email protected]; [email protected]
CABRERA ET AL.
2012 3