Embed Size (px)
Citation preview

INTRODUCTION
The recent technical explosion of cellular phoneshas changed the typical usage pattern of telephonedevices worldwide. The Cellular Telecommun-ications and Internet Association reported thatthere were 158.7 million subscribers by Decem-ber 2003. The numbers of users is increasing, asis the amount of time spent using cellular phones.Minutes of usage went up more than 30% from2002 to 2003, with year-end totals yielding 800billion minutes of call time used in 2003 alone(Cellular Telecommunications and Internet Asso-ciation, 2004).
With the convenience of cellular phones in-creasing their frequency and duration of use, thedesign characteristics of these phones give rise to
concerns regarding their impact upon body me-chanics and the musculoskeletal system. Thenature of cell phone use may facilitate the poten-tial for the development of musculoskeletal symp-toms. Continually ignored symptoms may lead toa musculoskeletal disorder over time. Upper ex-tremity musculoskeletal disorders are associatedwith the following risk factors: repeated loading,awkward postures, mechanical pressure, forceexertion, and duration of loading. Of these riskfactors, awkward postures and the extended dura-tion of loading are associated with cell phone use.The most reported upper extremity musculoskele-tal symptom is muscle pain (Buckle & Devereux2002).
Phone use is not traditionally thought of asphysically taxing on the musculoskeletal system.
The Effect of Phone Design on Upper Extremity Discomfortand Muscle Fatigue
Anne-Marie Chany, William S. Marras, and Deborah L. Burr, Ohio State University,Columbus, Ohio
Objective: To compare a small cellular clamshell phone with a traditional office phonein the development of discomfort and muscle fatigue over time during phone use. Back-ground: Phone use involves low-level static exertions that may be influenced by phonedesign. Phone design and its interactions with anthropometry may change shoulderand hand postures assumed during use, which in turn may modify the length-strengthrelationship and moment arms of the muscles. Method: Ten adults participated in astudy that simulated phone use using a small clamshell and a traditional office phone.Discomfort information and electromyographic (EMG) muscle activity were moni-tored on four upper extremity muscles. Discomfort and fatigue data (EMG median fre-quency shifts) were analyzed to assess differences between phones as well as differingeffects attributable to anthropometry. Results: Median frequency shifts supporteddiscomfort claims and indicated muscle fatigue in the deltoid and thenar muscles.Biomechanical measures demonstrated that participants with short limb lengths devel-oped more severe signs of thenar fatigue. Participants with longer arms developedgreater discomfort in the neck, shoulder, and back. The deltoid confirmed this occur-rence, showing signs of muscle fatigue. Conclusion: Phone design and anthropom-etry influenced the development of discomfort and fatigue during phone use. Phonedesign dictated grip style, resulting in differing discomfort and fatigue levels. Anthro-pometry influenced the severity of the discomfort and fatigue present in the shoulderand hand. Application: Use of small clamshell phones may contribute to a lack of restand recovery from typical workday exposures. It should be explored from an ergonom-ic perspective.
Address correspondence to William S. Marras, Biodynamics Laboratory, Ohio State University, 210 Baker Systems, 1971 NeilAve., Columbus, OH 43210; [email protected]. HUMAN FACTORS, Vol. 49, No. 4, August 2007, pp. 602–618. DOI 10.1518/001872007X215683. Copyright © 2007, Human Factors and Ergonomics Society. All rights reserved.

However, the repeated light exertions performedover long periods of time may link phone use torisk of upper extremity musculoskeletal disordersvia awkward postures and low-level static exer-tions. In phone use, the upper extremity is requiredto perform light work with little to no rest, oftenwhile stabilizing the head and neck for visualpurposes (Punnett & Wegman, 2004; Nordin,Andersson, & Pope, 1997). Although low-levelstatic exertions do not initially appear hazardous,if performed for extended durations they are asso-ciated with musculoskeletal complaints and signsof fatigue (Sjogaard & Jensen, 1999).
There are known preferred grip sizes andlength-strength muscle relationships that maxi-mize strength and minimize muscle activity. Mo-ment arms, controlled by postural demands, altermuscle length. The length-strength relationshipof muscles demonstrates that muscles have thegreatest ability to generate active force when theyare close to their resting length. Therefore, stretch-ing or shortening the muscle length inhibits itsability to produce tension within the muscle (Mar-ras, 1999).
Phone designs can be compared in order to ex-pose inefficiencies in the muscle length-strengthrelationship (Chaffin, Andersson, & Martin, 1999;Marras, 1999). The current trend in cellular phonedesign continues to decrease the size of the de-vices, which may force the user into postures thatsuboptimize length-strength principles. Standardtraditional office and cellular phones require theuser to grip the device with a combination of thepower and precision grips depending upon the sizeof the phone and the anthropometry of the user(Karwowski, 2001; Salvendy, 1997). If length-strength muscle properties are ignored in devicedesign, musculoskeletal symptoms and fatiguewill arise through product use.
The majority of research publications thus farhave focused on either the implications of cellu-lar phone use on driving or the exposure to radiofrequency radiation during cellular phone use(McKnight & McKnight, 1993; Oftedal, Wilen,Sandstrom, & Mild, 2000; Redelmeier & Tibshir-ani, 1997; Salvucci & Macuga, 2002; Strayer & Johnston, 2001; Sundeen, 2003; Wilen, Sand-strom, & Mild, 2003). There is a void in the liter-ature regarding upper extremity musculoskeletalsymptoms, biomechanics, and cellular phonedevices. Therefore, the objective of this researchis to assess how two differing phone designs and
participant anthropometry affect the developmentof discomfort and muscle fatigue over time dur-ing use.
This study involved the collection of bodydiscomfort information and electromyographic(EMG) muscle activity of the trapezius, deltoid,flexor digitorum superficialis (FDS), and thenarmuscles during a 1-hr simulated phone use ses-sion. In two separate sessions, two phone designmodels were tested: one small cellular clamshellphone and one traditional office phone. In thisstudy, subjective discomfort surveys and musclefatigue (median frequency analysis) were used asindicators of musculoskeletal stress. From thesefindings, design suggestions were made.
METHODS
Participants
The user population for telephones is general-ly representative of the general U.S. population,given their widespread use across the country. Tenhealthy participants (5 men, 5 women) from thegeneral population with no prior history of upperextremity musculoskeletal disorders volunteeredto participate in the study. Calculations for anacceptable sample size were performed using datacollected during a pilot study. The age range of theparticipants was 23 to 30 years, with an average ageof 25 years (SD ± 2). Anthropometric data werecollected for each of the participants for age, gen-der, height, weight, handedness, arm length, handlength, wrist circumference, palm width, elbow-to-fingertip length, thumb breadth, and thumblength (Kroemer & Grandjean, 2001). This infor-mation is shown in Table 1.
Experimental Design
Asimple randomized paired comparison exper-imental design was used for this study. Upper ex-tremity muscle activity and subjective discomfortmeasures during the static task were monitoredunder controlled laboratory conditions. The inde-pendent measure used in the experiment wasphone design. Anthropometry measures of the up-per extremity taken from each participant werealso used as independent variables in statisticalanalyses. The dependent measures of this studywere EMG median frequency slope for four upperextremity muscles and mean discomfort scoresfor each of five body regions for the duration ofthe task.
DISCOMFORT AND FATIGUE FROM PHONE DESIGN 603

TAB
LE 1
: Par
ticip
ants
’ Ant
hro
po
met
ric D
ata
Smal
lLa
rge
Wo
men
(n=
5)
Men
(n=
5)
U.S
. Mea
n (S
D)a
Mea
sure
(cm
)M
ean
Ran
ge
Mea
nR
ang
eM
ean
(SD
)R
ang
eM
ean
(SD
)R
ang
eW
om
enM
en
Arm
leng
th74
.79
73.0
–77.
4780
.84
78.5
–83.
075
.4 (3
.1)
73.0
–80.
380
.2 (2
.3)
77.4
–83.
072
.3 (3
.8)
78.8
(3.9
)H
and
leng
th16
.54
15.4
–17.
618
.66
17.7
–19.
716
.6 (1
.1)
15.4
–17.
918
.6 (0
.9)
17.4
–19.
718
.0 (1
.0)
19.3
(1.0
)W
rist
circ
umfe
renc
e14
.96
14.5
–15.
218
.15
17.4
–19.
314
.9 (0
.2)
14.5
–15.
117
.6 (1
.5)
15.2
–19.
317
.4 (0
.8)
15.1
(0.7
)P
alm
wid
th8.
848.
3–9.
410
.09.
5–10
.48.
9 (0
.5)
8.3–
9.5
9.9
(0.6
)8.
9–10
.49.
0 (0
.4)
7.9
(0.4
)E
lbo
w–fi
nger
tip
leng
th41
.98
40.9
–43.
346
.92
45.0
–48.
842
.7 (1
.9)
40.9
–45.
546
.9 (1
.6)
45.0
–48.
848
.3 (2
.3)
44.2
(2.3
)Th
umb
bre
adth
1.37
1.3–
1.4
1.65
1.5–
1.8
1.4
(0.1
)1.
3–1.
51.
6 (0
.2)
1.5–
1.8
2.3
(0.2
)1.
9 (0
.2)
Thum
b le
ngth
5.28
4.8–
5.6
6.23
6.0–
6.6
5.8
(0.6
)5.
1–6.
65.
5 (0
.5)
4.8–
6.1
5.1
(0.4
)4.
7 (0
.4)
No
te.H
and
edne
ss: 9
rig
ht, 1
left
. Sid
e m
oni
tore
d f
or
stud
y: 7
rig
ht, 3
left
.a D
ata
fro
m P
heas
ant
(199
9), p
p. 8
4–85
.
604

DISCOMFORT AND FATIGUE FROM PHONE DESIGN 605
Apparatus
Phone models were selected after surveying thedesign parameters of both cellular and traditionaloffice phone models currently in use. The designsvaried in length, depth, breadth, and grip style be-cause of the extensions at the heads of traditionaloffice phones, which do not exist in cellular mod-els. From information obtained in the market sur-vey, cellular phones typically had a grip area of 600to 1,300 mm2 (Nokia, 2007a, 2007b). Traditionaloffice phones’ grip areas ranged from 550 to1,860 mm2. To minimize variability between thesetwo categories, we selected two phones (one tra-ditional office phone and one small cellular clam-shell phone) that have similar small grip areaopenings (clamshell phone = 792 mm2 ; tradition-al office phone = 558 mm2), depth (clamshell andtraditional office phones = 18 mm), and breadthparameters (clamshell phone = 44 mm; tradition-al office phone = 31 mm).
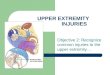
Panasonic Model KX-T3165, a traditionaloffice-style desk phone, served as the control. Thecell phone model used for the study, LG VX440,was a small clamshell or flip-style model (Fig-ure 1). These models were chosen to minimize thechange in the length-strength relationship of the muscles involved during their use.
The subjective measures consisted of a Borgsurvey for work-related discomfort that was ad-ministered every 10 min over the 1-hr period and
at the beginning and end of the study period. TheBorg scale ranged from 1 to 7, using the verballandmarks of 1 = no discomfort, 4 = some discom-fort, and 7 = high discomfort (Borg, 1982). Statis-tical analyses were performed using the mean ofthe seven readings taken over the 1-hr duration of the task.
Muscle activity was collected using surfaceelectromyography. EMG activity was collectedby bipolar silver-silver chloride surface electrodesspaced approximately 2 cm apart over four upperextremity muscles (the trapezius, the deltoid, theFDS, and the thenar muscle group).
A four-channel EMG amplification systemwas used to record the muscle activity informa-tion. Data signals were collected at 1024 Hz, thenrecorded and saved on a computer via an analog-to-digital conversion board (National InstrumentsPCI-6033E) and stored for later analysis.
Procedure
Upon their arrival, informed consent was ob-tained from the study participants. Participantswere asked to select a preferred side (dominant ornondominant) with which they would typicallyhold a telephone. EMG was monitored on the pre-ferred side only. Anthropometric measurementswere taken, and electrodes were placed on theparticipants’ trapezius, deltoid, FDS, and thenarmuscles. Electrode locations were determinedusing palpation according to Cram & Kasman
Figure 1. Phone designs used in experiment.
Small Clamshell Traditional Office

606 August 2007 – Human Factors
(1998) and Delagi, Perotto, Iazzetti, and Morrison(1980).
Specifically, the trapezius electrodes wereplaced 2 cm lateral to the midpoint of the line join-ing C7 to the acromion (Hermans & Spaepen,1997). The deltoid electrodes were placed threefingerbreadths below the anterior margins of theacromion found by palpation during a test con-traction of forward flexion of the arm. The flexorelectrode locations were found by grasping theparticipant’s volar surface of the wrist with the in-dex finger pointed to the biceps tendon. The elec-trodes were placed just ulnarly to the tip of theindex finger. The applicable test contraction wasto flex only the fingers while supporting the armwith the wrist in the neutral position. The thenarelectrodes were placed on either side of the mid-point line between the volar aspect of the firstmetacarpophalangeal joint and the carpometacar-pal joint. The test contraction used was the palmarabduction of the thumb.
The resistance between the electrodes was keptbelow 300 kΩ. Aground electrode was placed onthe lateral epicondyle.
Participants were asked to perform maximumvoluntary contractions (MVCs). They were in-structed to build up to their maximum exertionlevel over a period of 2 s and then to maintain theexertion for 4 s (Marras & Davis, 2001). The EMGof the monitored muscles was captured while theparticipant maintained a constant maximum ex-ertion.
For the trapezius and deltoid MVC exertion, theparticipant was seated. With the shoulder in a neu-
tral position (0º flexion, 0º abduction) and the el-bow at a 90º angle, a cuff was wrapped around thebicep. This cuff was linked to a chain that provid-ed constant resistance. To perform the MVC ex-ertion, the participant exerted force in shoulderabduction, keeping the elbow at 90º (Schuldt &Harms-Ringdahl, 1988), and pulled against the re-straint system. The maximum exertion of the flex-or and thenar muscles was obtained by squeezinga grip dynamometer (TM Stoelting Co.). The gripopening was fixed for all participants at 7.49 cm.The shoulder and wrist were in neutral (shoulder:0º flexion, 0º abduction; wrist: slight extension)and the elbow at 90º.
A standard protocol for capturing EMG max-imum exertions using static muscle strength test-ing procedures were used (Caldwell et al., 1974;Redfern, 1992; Soderberg, 1992). The posturesused for maximum exertions were close to thepostures assumed during the low-level static exer-tion task to control for variability in muscle lengthand volume and to capture a maximum exertionin this posture.
Task
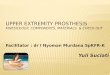
The static task performed by the participantsrequired simulated use of the phone designs. Liveairtime was not used because of the expense andpotential interference with the electromyographyequipment. Participants were placed in a supported-back sitting position and instructed to grip thephone with a grip using the index finger as a coun-terbalance (Figure 2). This posture was found tobe prevalent through separate observation studies
Figure 2. Grips used during small clamshell phone (left) and traditional office phone (right) conditions.

DISCOMFORT AND FATIGUE FROM PHONE DESIGN 607
done by the experimenters. No arm supports wereused. During the task, the participants were askedto hold the phone up to their ear as they would dur-ing actual use. The participant then engaged inconversation with the experimenter. Once the par-ticipant selected a posture and data recordingbegan, he or she was not allowed to change posture.
Although participants were instructed to use asimilar posture for both phone conditions, thedesign of the phones led them use a power gripwith the traditional office model and a combina-tion precision-power grip with the small clamshellphone. The index finger was used as a counterbal-ance; thus it was placed on the portion of the phonecontaining the ear receiver. The index finger wasin slight flexion in this posture. The thumb andremaining three fingers were used in flexion tostabilize the phone in the user’s hand. Thumb ori-entation was not controlled in the grip. The tradi-tional office phone allowed for some support fromthe palm, and the thumb and fingers were able towrap fully in flexion around the device. For thesmall clamshell phone, the thumb and fingers wereutilized at their tips to create phone stability foruse. Figure 2 displays common postures adoptedby the participants during the experiment.
Participants were required to maintain theirposture as still as possible for the duration of theexperiment. Participants were monitored to ensurecompliance with the experimental protocol. Therecorded video allowed the experimenter to deter-mine after the fact if participant movement madethe data unacceptable. EMG data were taken con-tinuously throughout the 1-hr experiment. Sub-jective discomfort scores were taken every 10 minthroughout the experiment using a body discom-fort map.
Data Analysis
EMG data were converted to the frequencydomain using a fast Fourier transform for spec-tral analysis. From the spectral information, themedian frequency was determined.
Data from the 1-hr experiment were saved intoseveral individual data files 5 min in length. Onesummary median frequency was generated foreach 5-min file. These summary median frequen-cy data for each 5-min interval were plotted in timesequence to show the changing median frequen-cy values of each muscle over the 1-hr duration ofthe experiment. Regression lines were generated
from the series of median frequency data pointsover the 1 hr.
The slope of the regression line for muscle fa-tigue was then extracted for use in statistical com-parisons in SAS (1999). If a monitored musclegenerated a negative slope, as seen when lookingat the regression line through the median frequen-cy points of that muscle over the duration of thetask, this was an indicator of fatigue. The literaturehas not quantified the amount of frequency drop(i.e., negative slope) needed to demonstrate fa-tigue (DeLuca, 1985). In contrast, if the regressionline yields a positive slope, there is no fatigue and the muscle has been allowed rest and recovery(McLean, Tingley, Scott, & Rikards, 2000, 2001).
Statistical Analysis
A paired comparison test of the two test condi-tions (small clamshell vs. traditional office phones)was performed on all four monitored muscles.The difference between the test conditions wasfound and then compared with zero using theProc Means procedure in SAS (1999). To betterdescribe the factors associated with significanteffects, we used a paired comparison using a two-sample Proc T-Test (SAS, 1999, Release 8.02) toisolate data into groups for comparison.
The means for the U.S. population norms forthe studied anthropometry measures were com-pared with the means of the study population. Thestudy population means adequately fit the normsfor the U.S. male and U.S. female populations. Ini-tial analyses found no significant effects of gender.However, separating the study population basedupon anthropometric dimensions yielded a betterfit than the traditional gender split. The mean ofeach anthropometry independent measure wasfound and determined to be the breakpoint forsplitting the anthropometry measures into two cat-egories. Participants with an anthropometry mea-sure (i.e., hand length) below the collective studypopulation mean were classified as small. Partici-pants with anthropometry measures greater thanthe mean were classified as large.
This classification of anthropometry groupspredominantly followed gender, with women pre-dominantly constituting the small-anthropometrygroup. However, no participant belonged entirelyto the small- or large-anthropometry group. Eachanthropometry measure was classified indepen-dently. It is well documented in the literature thatthere is much variability in the anthropometry of

608 August 2007 – Human Factors
an individual, and each body segment will belongto a different percentile of the population. Data forthe study population are shown in Table 1 by bothgender and anthropometry.
This allowed for four separate t test compar-isons of the phone conditions and the anthropom-etry groupings. The first t test made comparisonsbetween the two anthropometry groups within thesmall clamshell phone test condition; the secondt test made comparisons between the anthropom-etry groups within the traditional office phone testcondition; the third t test made comparisons be-tween the two phone models within the small-anthropometry group; and the fourth t test madecomparisons between the phone models within thelarge-anthropometry group. This controlled forany confounding that may have been present if thedata had been tested collectively. This type ofanalysis was performed on the regression lineslopes from the task duration and mean discom-fort data.
The mean subjective discomfort for the sevenreadings of each body part was analyzed to findout where participants were experiencing discom-fort throughout the experiment. Then, objectivefrequency analysis was performed to determineif there were physical manifestations of fatiguethat supported the discomfort information. The lit-erature on frequency analysis did not identify afatigue effect threshold for median frequency dropnecessary to indicate fatigue. Given the lack ofliterature on this issue, we examined the data forstatistical significance between conditions via theslope of the median frequency.
RESULTS
Discomfort scores in five body regions werecollected from participants at 10-min intervals.The mean discomfort score for each time intervalfor all participants in each of the phone conditionsis shown in Table 2. Although the small clamshellphone test condition showed increased discomfortfor the individual 10-min readings and the meandiscomfort score for the entire test duration, theoverall main effect of phone results are not statis-tically significant (see Table 3a).
Table 4 summarizes the mean body region dis-comfort findings for the effect of phone model byanthropometry group. Table 5 summarizes themean body region discomfort for the effect of an-thropometry by phone condition. Collecting this
information was critical in exposing the test con-ditions in which greater discomfort developed.Participants with more abduction strength, largerpalm widths, and larger thumb breadths had in-creased mean discomfort in the neck and shoulderin the small clamshell phone condition. When par-ticipants with large anthropometry were isolatedto allow us to examine effects of the phone condi-tions, the hand/wrist and fingers demonstrated aclear significant effect. The majority of the sur-veyed anthropometry dimensions showed thesmall clamshell phone condition led to increasedhand/wrist and finger discomfort for this group(shown in Table 4).
Analyzing the median frequency slope was anobjective measure used to explain the develop-ment of discomfort. Table 3 shows that the maineffect of phone design was significant for the the-nar muscle (p = .0028), for which the mean slopeof the small clamshell condition was –1.49 (SD =2.38), whereas for the traditional office conditionthe mean slope was 1.15 (SD = 1.98).
To further demonstrate the main effect ofphone, Table 6 summarizes the median frequencyslope findings for the effect of phone model with-in an anthropometry group. Table 7 summarizesthe median frequency slope for the effect of an-thropometry within each phone condition. Parti-cipants with small anthropometry dimensionsgenerally tended to show significant fatigue in thesmall clamshell phone condition, with median fre-quency slopes ranging from –2.05 to –3.30. Thelarge-anthropometry group had lesser negativeslopes (ranging from –1.00 to 0.24) in the smallclamshell phone condition (significant for armlength and elbow-to-fingertip length). Both anthro-pometry groups showed positive slopes in the tra-ditional office phone test condition.
A secondary finding of the frequency analysisshowed that large-anthropometry participantsdeveloped significant deltoid fatigue for bothphone conditions, with a slope near –2. Small-anthropometry participants developed fatigueslower, with slopes near –1 (significant for gripstrength and elbow-to-fingertip length).
DISCUSSION
The primary finding of this study involved thepresence of thenar muscle fatigue in the smallclamshell phone condition and the lack thereof inthe traditional office phone condition. Frequency

609
TAB
LE 2
: Dis
com
fort
Sum
mar
y b
y R
ead
ing
fo
r th
e 1-
hr E
xper
imen
t D
urat
ion
by
Pho
ne C
ond
itio
n
Mea
n R
ead
ing
in M
inut
es (S
D)
Ave
rag
eP
art
of
Bo
dy
010
2030
4050
60o
f 60
min
Smal
l Cla
msh
ell P
hone
Co
ndit
ion
Nec
k1
(0)
1.4
(0.5
1)1.
4 (0
.69)
1.8
(0.7
8)2.
1 (0
.99)
2.2
(0.9
1)2.
5 (1
.08)
1.8
(0.5
3)Sh
oul
der
1.1
(0.3
1)2.
1 (0
.99)
2.4
(0.9
6)2.
7 (1
.15)
3.4
(1.2
6)3.
6 (1
.26)
4.1
(1.4
4)2.
8 (1
.02)
Elb
ow
/fo
rear
m1
(0)
1.1
(0.3
1)1.
3 (0
.48)
1.6
(0.5
1)1.
6 (0
.51)
1.8
(0.7
8)1.
9 (0
.73)
1.5
(0.3
5)H
and
/wri
st1
(0)
1.6
(0.6
9)1.
7 (0
.48)
2.3
(0.9
4)2.
4 (0
.69)
2.5
(0.9
7)2.
8 (1
.31)
2.0
(0.6
2)Fi
nger
s1
(0)
1.8
(0.6
3)2.
0 (0
.66)
2.4
(0.5
1)2.
9 (0
.56)
3.5
(0.8
4)3.
8 (0
.63)
2.5
(0.9
9)
Trad
itio
nal O
ffice
Pho
ne C
ond
itio
nN
eck
1 (0
)1.
1 (0
.31)
1.5
(0.5
2)1.
6 (0
.69)
1.8
(0.7
8)2.
0 (0
.94)
2.1
(0.5
6)1.
6 (0
.42)
Sho
uld
er1
(0)
1.9
(0.7
3)2.
3 (0
.67)
2.5
(0.7
0)3.
0 (1
.05)
3.2
(1.2
2)3.
7 (1
.25)
2.5
(0.8
9)E
lbo
w/f
ore
arm
1 (0
)1.
1 (0
.31)
1.1
(0.3
1)1.
4 (0
.69)
1.4
(0.6
9)1.
6 (0
.84)
1.7
(0.8
2)1.
3 (0
.27)
Han
d/w
rist
1 (0
)1.
2 (0
.42)
1.6
(0.5
1)1.
8 (0
.78)
2.0
(0.6
6)2.
3 (0
.67)
2.3
(0.6
7)1.
7 (0
.51)
Fing
ers
1 (0
)1.
4 (0
.51)
2.1
(0.7
3)2.
3 (0
.82)
2.8
(1.1
3)2.
9 (1
.10)
3.1
(0.9
9)2.
2 (0
.79)

analysis showed a negative slope in the smallclamshell phone condition, indicating fatigue de-velopment over time. The traditional office phonecondition’s positive slope indicated recovery. In-dividual thenar data showed that the positive slopewas generated because of on/off activity of thethenar muscle during the traditional office phonecondition. It is suggested that this on/off activityallowed the muscle to rest and recover from anydetrimental effects.
Afundamental difference in grip style betweenthe two phone conditions (shown in Figure 2) mayhave resulted in the different thenar muscle acti-vations required for the two phone models. Al-though participants were instructed to use a similarposture for both phone conditions, the design ofthe phone led the user into a power grip when usingthe traditional office phone model and a combi-nation precision-power grip when using the smallclamshell phone. The power grip was facilitated bythe traditional office phone design because the bodyof the phone, where the hand gripped the device,was recessed from the circular ends for the ear andmouth. The traditional office phone power gripcreated an ideal length-strength position that re-quired only an extremely low level of activation ofthe thenar muscle, if activation was required at all.
The combination precision-power grip was re-quired for use in the small clamshell phone condi-tion because the body of the phone rested againstthe face of the user. This prevented the use of thepower grip in the small clamshell phone conditionand altered the length-strength position of themuscles. Precision grips are known to reduce gripstrength (Eastman-Kodak Co., 1986; Karwowski,2001; Swanson, Matev, & de Groot, 1970) andthus may have influenced the development of fa-tigue with the small clamshell phone. This mayexplain the primary differences seen between thetwo phone conditions for the thenar muscle.
Additionally, there appeared to be basic differ-ences in thenar fatigue between the small- andlarge-anthropometry groups when using the smallclamshell phone. Although signs of thenar musclefatigue were present in both groups, it was worsefor those participants with smaller anthropometrydimensions.
There were interesting postural differences be-tween the anthropometry groups. Participants withmostly small anthropometry dimensions tendedto hold the small clamshell phone with the thumbpad flat against the phone, in parallel with the longedge of the phone (see Figure 3a). The bottomcorner of the small clamshell phone along the
TABLE 3b: Main Effect of Phone for Median Frequency Slope
Mean Slope (SE) Mean Slope (SE) DifferenceSmall Clamshell Traditional Between the
Muscle Phone Office Phone Mean Slopes (SE) p Value
Trapezius –0.68 (1.01) –0.05 (1.15) –0.63 (0.62) .3351Deltoid –1.46 (0.85) –1.65 (1.03) 0.19 (0.21) .3756Flexor –1.60 (1.18) –2.24 (2.35) 0.64 (0.69) .3834Thenar –1.49 (2.38) 1.15 (1.98) –2.65 (0.65) .0028*
*Statistical significance at p < .05.
TABLE 3a: Main Effect of Phone for Discomfort
Mean MeanDiscomfort (SE) Discomfort (SE) DifferenceSmall Clamshell Traditional Between the Mean
Body Part Phone Office Phone Discomfort (SE) p Value
Neck 1.78 (0.91) 1.61 (0.77) 0.17 (0.19) .3608Shoulder 2.80 (1.42) 2.49 (1.19) 0.31 (0.24) .3133Elbow/forearm 1.48 (0.61) 1.31 (0.63) 0.17 (0.09) .1483Hand/wrist 2.06 (0.98) 1.77 (0.75) 0.29 (0.20) .1748Fingers 2.51 (1.07) 2.22 (1.09) 0.29 (0.18) .1879
*Statistical significance at p < .05.
Continued on page 615
610 August 2007 – Human Factors

611
TAB
LE 4
:Dis
com
fort
Ana
lysi
s Si
gni
fican
t E
ffec
ts o
f P
hone
(Cla
msh
ell v
s. T
rad
itio
nal O
ffice
) With
in t
he A
nthr
op
om
etry
Gro
up
Ant
hro
po
met
ry D
imen
sio
n
Elb
ow
-to
-P
art
of
Han
dA
rmG
rip
Ab
duc
tio
nFi
nger
tip
Pal
mTh
umb
Thum
bB
od
yP
hone
Leng
thLe
ngth
Stre
ngth
Stre
ngth
Leng
thW
idth
Bre
adth
Leng
th
Smal
l Ant
hro
po
met
ryN
eck
Cla
msh
ell
1.85
1.97
1.95
1.73
1.85
1.47
1.69
1.97
*Tr
adit
iona
l1.
531.
811.
781.
691.
711.
681.
691.
50*
Sho
uld
erC
lam
shel
l2.
642.
742.
632.
432.
532.
612.
542.
37Tr
adit
iona
l2.
252.
412.
392.
452.
282.
712.
572.
28E
lbo
w/f
ore
arm
Cla
msh
ell
1.53
1.57
1.51
*1.
531.
571.
551.
381.
53Tr
adit
iona
l1.
321.
361.
19*
1.35
1.02
1.40
1.16
1.40
Han
d/w
rist
Cla
msh
ell
2.04
2.06
1.75
1.92
1.96
1.73
1.90
2.24
*Tr
adit
iona
l1.
891.
891.
651.
881.
851.
881.
801.
76*
Fing
ers
Cla
msh
ell
2.46
2.37
2.51
2.41
2.39
2.38
2.35
2.63
Trad
itio
nal
2.46
2.36
2.31
2.38
2.46
2.31
2.38
2.47
Larg
e A
nthr
op
om
etry
Nec
kC
lam
shel
l1.
731.
591.
531.
851.
732.
08*
1.92
*1.
50Tr
adit
iona
l1.
661.
411.
371.
501.
501.
48*
1.42
*1.
71Sh
oul
der
Cla
msh
ell
2.90
2.85
3.03
3.32
*2.
952.
94*
3.14
*2.
85Tr
adit
iona
l2.
642.
552.
622.
52*
2.66
2.31
*2.
42*
2.85
Elb
ow
/fo
rear
mC
lam
shel
l1.
431.
381.
511.
392.
581.
401.
621.
39Tr
adit
iona
l1.
301.
261.
421.
252.
071.
251.
571.
21H
and
/wri
stC
lam
shel
l2.
07*
2.06
*2.
50*
2.25
*2.
09*
2.34
*2.
25*
1.75
Trad
itio
nal
1.69
*1.
64*
1.93
*1.
60*
1.66
*1.
60*
1.64
*1.
71Fi
nger
sC
lam
shel
l2.
54*
2.65
*2.
502.
64*
2.58
*2.
62*
2.74
*2.
32Tr
adit
iona
l2.
07*
2.09
*2.
102.
00*
2.07
*2.
14*
2.00
*1.
85
No
te.D
isco
mfo
rt a
naly
sis
rep
rese
nts
the
mea
n o
f th
e re
po
rted
dis
com
fort
leve
ls f
or
the
1-hr
dur
atio
n o
f th
e ex
per
imen
t.
*Sta
tist
ical
sig
nific
ance
at
p<
.05.

612
TAB
LE 5
: Dis
com
fort
Ana
lysi
s Si
gni
fican
t E
ffec
ts o
f A
nthr
op
om
etry
Gro
up W
ithin
the
Pho
ne C
ond
itio
n
Ant
hro
po
met
ry D
imen
sio
n
Ant
hro
-E
lbo
w-t
o-
Par
t o
fp
om
etry
Han
dA
rmG
rip
Ab
duc
tio
nFi
nger
tip
Pal
mTh
umb
Thum
bB
od
yG
roup
Leng
thLe
ngth
Stre
ngth
Stre
ngth
Leng
thW
idth
Bre
adth
Leng
th
Smal
l Cla
msh
ell P
hone
Nec
kSm
all
1.85
1.97
*1.
95*
1.73
1.85
1.47
*1.
691.
97*
Larg
e1.
731.
58*
1.53
*1.
851.
732.
08*
1.92
1.50
*Sh
oul
der
Smal
l2.
642.
742.
632.
43*
2.53
2.61
2.54
2.37
Larg
e2.
902.
853.
033.
32*
2.95
2.94
3.14
2.85
Elb
ow
/fo
rear
mSm
all
1.53
1.57
1.51
1.53
1.57
*1.
551.
381.
53La
rge
1.43
1.38
1.42
1.39
2.58
*1.
401.
621.
39H
and
/wri
stSm
all
2.04
2.06
1.75
*1.
921.
961.
83*
1.90
2.24
*La
rge
2.07
2.06
2.50
*2.
252.
092.
62*
2.25
1.75
*Fi
nger
sSm
all
2.46
2.37
2.51
2.41
2.39
2.38
2.35
2.63
Larg
e2.
542.
652.
502.
642.
582.
622.
742.
32
Trad
itio
nal O
ffice
Pho
neN
eck
Smal
l1.
531.
80*
1.78
*1.
691.
711.
681.
691.
50La
rge
1.66
1.41
*1.
37*
1.50
1.50
1.48
1.42
1.71
Sho
uld
erSm
all
2.25
2.41
2.39
2.45
2.28
2.71
2.57
2.28
Larg
e2.
642.
552.
622.
532.
662.
312.
422.
85E
lbo
w/f
ore
arm
Smal
l1.
321.
361.
19*
1.35
1.02
*1.
401.
16*
1.40
Larg
e1.
301.
261.
48*
1.25
2.07
*1.
251.
57*
1.21
Han
d/w
rist
Smal
l1.
891.
891.
651.
881.
851.
88*
1.80
1.76
Larg
e1.
691.
641.
931.
601.
662.
14*
1.64
1.71
Fing
ers
Smal
l2.
462.
362.
312.
382.
462.
312.
382.
47*
Larg
e2.
072.
092.
102.
002.
071.
602.
001.
85*
No
te.D
isco
mfo
rt a
naly
sis
rep
rese
nts
the
mea
n o
f th
e re
po
rted
dis
com
fort
leve
ls f
or
the
1-hr
dur
atio
n o
f th
e ex
per
imen
t.
*Sta
tist
ical
sig
nific
ance
at
p<
.05.

613
TAB
LE 6
: Med
ian
Freq
uenc
y Sl
op
e A
naly
sis
Sig
nific
ant
Eff
ects
of
Pho
ne W
ithin
the
Ant
hro
po
met
ry G
roup
Ant
hro
po
met
ry D
imen
sio
n
Elb
ow
-to
-P
art
of
Han
dA
rmG
rip
Ab
duc
tio
nFi
nger
tip
Pal
mTh
umb
Thum
bB
od
yP
hone
Leng
thLe
ngth
Stre
ngth
Stre
ngth
Leng
thW
idth
Bre
adth
Leng
th
Smal
l Ant
hro
po
met
ryTr
apez
ius
Cla
msh
ell
–0.3
5–0
.68
–0.4
4–0
.32
–0.4
8–0
.06
–0.7
5–1
.14
Trad
itio
nal
–0.6
3–0
.56
–0.3
3–0
.40
–0.6
3–0
.37
0.19
0.02
Del
toid
Cla
msh
ell
–1.2
1–0
.99
–0.8
4–1
.18
–0.7
6–1
.26
–1.2
0–1
.55
Trad
itio
nal
–0.9
5–1
.27
–1.1
0–1
.27
–0.9
6–1
.47
–1.5
5–1
.52
Flex
or
Cla
msh
ell
–1.7
8–1
.50
–0.9
8–1
.54
–1.3
5–1
.32
–1.3
1–1
.88
Trad
itio
nal
–1.0
6–1
.14
0.98
–1.1
6–0
.81
–1.1
8–2
.16
–2.6
4Th
enar
Cla
msh
ell
–2.5
0*–3
.24*
–2.4
5*–2
.27*
–3.3
0*–1
.98
–2.0
5–2
.05*
Trad
itio
nal
2.00
*0.
48*
0.20
*1.
04*
0.45
*1.
090.
42–1
.15*
Larg
e A
nthr
op
om
etry
Trap
eziu
sC
lam
shel
l–0
.89
–0.6
7–1
.02
–1.2
1–0
.80
–1.2
9–0
.55
0.01
Trad
itio
nal
0.34
0.47
0.38
0.49
0.33
0.27
–0.4
0–0
.15
Del
toid
Cla
msh
ell
1.61
–1.9
1–2
.38
–1.8
5–1
.91
–1.6
5–1
.83
–1.3
0Tr
adit
iona
l–2
.11
–2.0
2–2
.47
–2.2
1–2
.11
–1.8
3–1
.79
–1.8
4Fl
exo
rC
lam
shel
l–1
.48
–1.7
0–2
.53
–1.6
8–1
.76
–1.8
8–2
.03
–1.1
7Tr
adit
iona
l–3
.02
–3.3
3–4
.12
–3.8
4–3
.18
–3.2
9–2
.35
–1.6
3Th
enar
Cla
msh
ell
–0.8
30.
24–0
.07
–0.3
3–0
.02
–1.0
00.
650.
66Tr
adit
iona
l0.
581.
812.
581.
301.
621.
212.
241.
15
*Sta
tist
ical
sig
nific
ance
at
p<
.05.

614
TAB
LE 7
: Med
ian
Freq
uenc
y Sl
op
e A
naly
sis
Sig
nific
ant
Eff
ects
of
Ant
hro
po
met
ry G
roup
With
in t
he P
hone
Co
nditi
on
Ant
hro
po
met
ry D
imen
sio
n
Ant
hro
-E
lbo
w-t
o-
Par
t o
fp
om
etry
Han
dA
rmG
rip
Ab
duc
tio
nFi
nger
tip
Pal
mTh
umb
Thum
bB
od
yG
roup
Leng
thLe
ngth
Stre
ngth
Stre
ngth
Leng
thW
idth
Bre
adth
Leng
th
Smal
l Cla
msh
ell P
hone
Trap
eziu
sSm
all
–0.3
5–0
.68
–0.4
4–0
.32
–0.4
8–0
.06
–0.7
5–1
.14
Larg
e–0
.89
–0.6
7–1
.02
–1.2
1–0
.80
–1.2
9–0
.55
0.01
Del
toid
Smal
l–1
.21
–0.9
9–0
.84*
–1.1
8–0
.76*
–1.2
6–1
.20
–1.5
5La
rge
–1.6
1–1
.91
–2.3
8*–1
.85
–1.9
1*–1
.65
–1.8
3–1
.30
Flex
or
Smal
l–1
.78
–1.5
0–0
.98*
–1.5
4–1
.35
–1.3
2–1
.31
–1.8
8La
rge
–1.4
8–1
.70
–2.5
3*–1
.68
–1.7
6–1
.88
–2.0
3–1
.17
Then
arSm
all
–2.5
0–3
.24*
–2.4
5–2
.27
–3.3
0*–1
.98
–2.0
5–2
.05
Larg
e–0
.38
0.24
*–0
.07
–0.3
3–0
.02*
–1.0
0–0
.65
–0.6
6
Trad
itio
nal O
ffice
Pho
neTr
apez
ius
Smal
l–0
.63
–0.5
6–0
.33
–0.4
0–0
.63
–0.3
70.
190.
02La
rge
0.34
0.47
0.38
0.49
0.33
0.27
–0.4
0–0
.15
Del
toid
Smal
l–0
.95
–1.2
7–1
.10*
–1.2
7–0
.96
–1.4
7–1
.55
–1.5
2La
rge
–2.1
1–2
.02
–2.4
7*–2
.21
–2.1
1–1
.83
–1.7
9–1
.84
Flex
or
Smal
l–1
.06
–1.1
40.
98–1
.16
–0.8
1–1
.18
–2.1
6–2
.64
Larg
e–3
.02
–3.3
3–4
.12
–3.8
4–3
.18
–3.2
9–2
.35
–1.6
3Th
enar
Smal
l2.
000.
480.
201.
040.
451.
090.
421.
15La
rge
0.58
1.81
2.58
1.30
1.62
1.21
2.24
1.15
*Sta
tist
ical
sig
nific
ance
at
p<
.05.

DISCOMFORT AND FATIGUE FROM PHONE DESIGN 615
thenar side of the palm was cradled into the palm,supported by the thenar eminence. As a result ofthe posture used for balance of the phone, it wasnecessary for the wrist to be in extension. Thelarge-anthropometry group held the small clam-shell phone differently, with the thumb perpen-dicular to the long edge of the phone (see Figure3b). The phone was thus more free standing thanresting in the palm. This posture of the thumb andfingers allowed for a more neutral wrist posture.All participants were required to use the index fin-ger as a counterbalance.
The signs of fatigue in the small-anthropome-try group may be attributable to the extension ofthe wrist. This wrist posture changed the musclelengths in the arm and hand. Any deviation of thewrist from neutral is known to produce losses ingrip strength (Karwowski, 2001; Sporrong, Palm-erud, & Herberts, 1996). Wrist posture may haveaffected the strength and endurance of the hand;also, the fundamental muscle length of the thumbwas altered between the two anthropometry groups.The direction of applied force for the thumb re-mained the same in both cases, but the thumbchanged orientation. The presence of more fatiguein the small-anthropometry group suggests thatthe thumb muscle length was not optimized in theparallel position. Fatigue developed quicker inparticipants performing static exertions using non-neutral postures and muscle lengths that were notoptimal (Chaffin et al., 1999; Karwowski, 2001;Langton, 1998; Watkins, 1999).
Fatigue in the thenar muscle may prove to besignificant when office occupational tasks are ex-amined. The thenar muscle is being used more fre-quently with the advent of highly intensive handand finger tasks associated with technology in theworkplace. A lack of rest and recovery from typ-ical workday office exposures may occur whensimilar tasks such as typing, using a mouse, andusing a Blackberry are combined with using asmall clamshell phone.
The secondary finding of this study was thatlarge-anthropometry participants had increasedfatigue in the deltoid in both phone conditions,which may be explained by the influence of an-thropometry on biomechanics. In this task, the armposture relative to the neck and shoulder for bothphone conditions was not altered by phone design.Similar steep fatigue patterns in the deltoid devel-oped for participants with long arm segments.
It is suggested that the presence of fatigue wasattributable to the internal moment arm associatedwith holding the phone (Marras, 1999). The addi-tional length of the arm segments changed thecenter of mass of the arm and created a longer mo-ment arm. The resultant internal force increasedto maintain shoulder stability during phone usefor these participants. These accommodations forlink length altered the length-strength relationshipof the muscles when the anthropometry groupswere compared (Chaffin et al., 1999). The longerarm segments may also have increased body massassociated with the additional length. Overcoming
Figure 3. Postures observed during the study for small clamshell phone between anthropometry groups: (a) wrist inextension for the small-anthropometry group; (b) wrist in neutral position for the large-anthropometry group.
(a) (b)

616 August 2007 – Human Factors
these additional forces to maintain stability mayhave caused muscle fatigue to develop at a fast-er rate.
In summary, the posture facilitated by the phonedesign was a significant contributor to the develop-ment of fatigue through an altering of the length-strength relationship. Anthropometry additionallymodified the body’s reaction to the phone designs.Specifically, the small clamshell phone presentedan increase in discomfort for the hand, wrist, andfingers for all participants. Biomechanical mea-sures demonstrated that participants with smallerlimb lengths developed significant signs of fatiguein the thumb. This is proposed to be a result ofusing suboptimal length-strength positions of thehand. Also, participants with longer arms tended todevelop greater discomfort in the neck and shoul-der. Biomechanical data supported this theory,with signs of muscle fatigue attributed to increasedmoment and mass in participants with long limbs.
Statistical power for this study was based on apilot investigation. Although this study had a lim-ited sample size, statistically significant differ-ences were observed in some of the muscles. Alarger population of participants may have allowedus to identify even more statistically significantdifferences. These findings suggest that a studywith more phone design styles may result in agreater understanding of proper design principles.Also, given the large number of tests that weredone (128 t tests for frequency analysis, of which12 were significant, and 160 t tests for discomfortanalysis, of which 33 were significant), Type I er-ror probability of any false significances is greaterthan the individual significance level of .05. Thus,the recommendations about phone design can bemade only under the assumption that the multipletests are simultaneously correct; they have notbeen proved by this single study alone.
Muscular fatigue as measured by the EMG me-dian frequency shift may be confounded by mus-cle force and muscle length. Changes in muscleforce and length also change the correspondingEMG signal and frequency spectrum. It is verydifficult to isolate the true effects of fatigue. Thisexperiment attempted to control for this effect bymaking the task a static activity and making theposture used by the hand and shoulder during the two test conditions constant. There was nofeedback mechanism for isokinetic force duringthe task, but participants were asked to utilize thedevices as they normally would use them.
In real-life phone use with live airtime, userswill shift and adjust postures to better hear the con-versation and optimize their body’s use of thedevice. Users may adjust the forces with whichthey hold the phone, rather than remaining still asin our simulated task. For example, users mayneed to strain to hear the conversation through thedevice, possibly increasing the forces used to gripthe phone when using live airtime. For the pur-poses of monitoring fatigue via EMG shifts forlow-level exertions, we instructed participants tokeep the task static during this study. The 1-hrduration was chosen based upon pilot data in aneffort to capture enough data for fatigue to appearin a low-level static exertion. Despite the attemptto make the task purely static, during the experi-ment many participants subconsciously allowedtheir head and neck to nod as it would during con-versation and actual phone use. The introductionof some movement allows for muscle recovery,and yet signs of fatigue were still present in themonitored muscles.
Although the long-duration, static use of thesmall clamshell phone in this study does not reflecttypical phone use patterns, it is likely that inter-mittent small clamshell phone use contributes to alack of rest and recovery from typical workdayexposures when combined with other occupation-al upper extremity tasks, such as typing, using amouse, and using a Blackberry.
Design Suggestions
The primary differences between phone con-ditions and anthropometry groups may highlightareas that need attention in order to optimizephone design for minimal fatigue and discomforteffects. The traditional office phone facilitated apower grip that required little use of the thenarmuscle. Some participants also had a variation ofthe power grip when using a small clamshellphone, yielding less fatigue than those participantsusing a precision-pinch style. Thumb and fingergrooves added to the side of the phone may facil-itate a power-style grip, optimizing the length-strength relationship and correcting the nonneutralwrist posture.
Studies may be done to optimize the width ofthe phone. Anthropometry is known to influencegrip capacity, which directly interacts with the pa-rameters of phone design. Although this study can-not identify the ideal phone width, the importanceof moment arms and length-strength properties

DISCOMFORT AND FATIGUE FROM PHONE DESIGN 617
of muscles was suggested by this study. Thewidth of the phone may have a direct impact onthese concepts. Additionally, studies comparinggrip styles during identical tasks may highlightdifferences between anthropometry groups.
Although the static simulated phone use testeddoes not depict typical phone use patterns and thisstudy was limited to testing one small clamshellphone design and one traditional office phone de-sign, it is suggested that small clamshell phone usemay contribute to a lack of rest and recovery fromworkday exposures. This study may serve as aninitial investigation; further in-depth studies, in-cluding multiple phone models, are necessary tofully understand how phone use impacts fatigue incombination with the many upper extremity occu-pational tasks performed daily.
CONCLUSIONS
The small clamshell phone increased handdiscomfort and thenar muscle fatigue during use,in comparison with the traditional office phone.Phone design and anthropometry interact to influ-ence discomfort and the development of musclefatigue. Grip style, as facilitated by phone design,contributed to the development of discomfort andmuscle fatigue by changing muscle lengths. An-thropometry was found to additionally modifymuscle length within the small clamshell phonetest condition.
In general, the results of this study providedsome insight into the effect of phone design ondiscomfort and muscle fatigue. The long-durationphone use tested in this study does not depict typ-ical phone use patterns; however, it is possible thatsmall clamshell phone use contributes to a lack ofrest and recovery from typical workday expo-sures. This activity may contribute to the cumula-tive effect of exposures to risk factors in the upperextremity.
Although this study was limited to testing onlytwo phone designs, one small clamshell phone andone traditional office phone, we hope it raisesawareness of the biomechanical and ergonomicissues in this particular area of consumer productdesign. This study alone cannot yield definitive de-sign recommendations, but it does provide a preliminary glance at the biomechanical conse-quences of the continuous miniaturization of cel-lular phones. Considering the increasing usage ofthese devices for both occupational and personal
use, it is hoped that this study inspires further in-vestigation into this topic.
REFERENCES
Borg, G. (1982). Psychophysical bases of perceived exertion. Medicineand Science in Sports and Exercise, 14, 377–381.
Buckle, P. W., & Devereux, J. J. (2002). The nature of work-related neckand upper limb musculoskeletal disorders. Applied Ergonomics,33, 207–217.
Caldwell, L. S., Chaffin, D. B., Dukes-Dobos, F. N., Kroemer, K. H.,Laubach, L. L., Snook, S. H., et al. (1974). A proposed standardprocedure for static muscle strength testing. American IndustrialHygiene Association Journal, 35, 201–206.
Cellular Telecommunications and Internet Association. (2004). CTIA’ssemi-annual wireless industry survey. Washington, DC: Author.
Chaffin, D. B., Andersson, G., & Martin, B. (1999). Occupational bio-mechanics. New York: Wiley.
Cram, J., & Kasman, G. (1998). Introduction to surface electromyog-raphy. Gaithersburg, MD: Aspen.
Delagi, E., Perotto, A., Iazzetti, J., & Morrison, D. (1980). Anatomicguide for the electromyographer. Springfield, IL: Charles C.Thomas.
DeLuca, C. J. (1985). Myoelectrical manifestations of localized muscu-lar fatigue in humans. Critical Reviews in Biomedical Engineering,11, 251–279.
Eastman-Kodak Company. (1986). Ergonomic design for people atwork. New York: Van Nostrand Reinhold.
Hermans, V., & Spaepen, A. J. (1997). Influence of electrode position onchanges in electromyography parameters of the upper trapezius mus-cle during submaximal sustained contractions. European Journal ofApplied Physiology and Occupational Physiology, 75, 319–325.
Karwowski, W. (2001). International encyclopedia of ergonomics andhuman factors. New York: Taylor & Francis.
Kroemer, K., & Grandjean, E. (2001). Fitting the task to the human: Atextbook of occupational ergonomics. Philadelphia: Taylor &Francis.
Langton, P. (1998). The [muscle] length-tension relation. RetrievedAugust 15, 2004, from http://www.bris.ac.uk/Depts/Physiology/ugteach/ugindex/m1_index/nm_tension/page1.htm
Marras, W. S. (1999). Occupational biomechanics. In W. Karwowski& W. S. Marras (Eds.), The occupational ergonomics handbook(pp. 167–204). Boca Raton, FL: CRC Press.
Marras, W. S., & Davis, K. G. (2001). A non-MVC EMG normaliza-tion technique for the trunk musculature: Part I. Method develop-ment. Journal of Electromyography and Kinesiology, 11, 1–9.
McKnight, A. J., & McKnight, A. S. (1993). The effect of cellularphone use upon driver attention. Accident Analysis and Prevention,25, 259–265.
McLean, L., Tingley, M., Scott, R. N., & Rickards, J. (2000). Myoelectricsignal measurement during prolonged computer terminal work.Journal of Electromyography and Kinesiology, 10, 33–45.
McLean, L., Tingley, M., Scott, R. N., & Rickards, J. (2001). Computerterminal work and the benefit of microbreaks. Applied Ergonomics,32, 225–237.
Nokia. (2007a). Nokia 7380 phone features. Retrieved April 3, 2007,from www.nokiausa.com/phones/7380/0,7747,feat;1;00.html
Nokia. (2007b). Nokia N80ie device features. Retrieved April 3, 2003,from www.nokiausa.com/phones/N80ie/0,7747,feat:1,00.html
Nordin, M., Andersson, G., & Pope, M. (Eds). (1997). Musculoskeletaldisorders in the workplace: Principles and practice. Philadelphia:Mosby.
Oftedal, G., Wilen, J., Sandstrom, M., & Mild, K. H. (2000). Symptomsexperienced in connection with mobile phone use. OccupationalMedicine, 50, 237–245.
Pheasant, S. (1999). Bodyspace: Anthropometry, ergonomics and thedesign of work. London: Taylor & Francis.
Punnett, L., & Wegman, D. H. (2004). Work-related musculoskeletaldisorders: The epidemiologic evidence and the debate. Journal ofElectromyography and Kinesiology, 14, 13–23.
Redelmeier, D. A., & Tibshirani, R. J. (1997). Association between cellular-telephone calls and motor vehicle collisions. New EnglandJournal of Medicine, 336, 453–458.
Redfern, Mark. (1992). Functional muscle: Effects on electromyo-graphic output. In G. L. Soderberg (Ed.), Selected topics in surface

618 August 2007 – Human Factors
electromyography for use in the occupational setting: Expert per-spectives (DHHS [NIOSH] Publication No. 91-100, pp. 104–120).Atlanta, GA: U.S. Department of Health and Human Services,Public Health Service, Center for Disease Control.
Salvendy, G. (1997). Handbook of human factors and ergonomics.New York: Wiley.
Salvucci, D., & Macuga, K. (2002). Predicting the effects of cellularphone dialing on driver performance. Cognitive Systems Research,3, 95–102.
SAS. (1999). The SAS system for Windows (Release 8.02) [Computersoftware]. Cary, NC: Author.
Schuldt, K., & Harms-Ringdahl, K. (1988). Activity levels during iso-metric test contractions of neck and shoulder muscles. ScandinavianJournal of Rehabilitation Medicine, 20, 117–127.
Sjogaard, G., & Jensen, B. R. (1999). Low level static exertions. In W.Karwowski & W. S. Marras (Eds.), The occupational ergonomicshandbook (pp. 167–204). Boca Raton, FL: CRC Press.
Soderberg, G. L. (1992). Recording techniques. In In G. L. Soderberg(Ed.), Selected topics in surface electromyography for use in theoccupational setting: Expert perspectives (DHHS [NIOSH]Publication No. 91-100, pp. 24–41). Atlanta, GA: U.S. Departmentof Health and Human Services, Public Health Service, Center forDisease Control.
Sporrong, H., Palmerud, G., & Herberts, P. (1996). Hand grip increasesshoulder muscle activity: An EMG analysis with static hand con-tractions in 9 subjects. Acta Orthopaedica Scandinavica, 67,485–490.
Strayer, D. L., & Johnston, W. A. (2001). Driven to distraction: Dual-taskstudies of simulated driving and conversing on a cellular telephone.Psychological Science, 12, 462–466.
Sundeen, M. (2003). Cell phones and highway safety: 2003 State leg-islative update. Washington, DC: National Conference of StateLegislatures.
Swanson, A. B., Matev I. B., & de Groot. G. (1970). The strength of thehand. Bulletin of Prosthetics Research, 10(14), 145–153.
Watkins, J. (1999). Structure and function of the musculoskeletal system.Champaign, IL: Human Kinetics.
Wilen, J., Sandstrom, M., & Mild, K. H. (2003). Subjective symptomsamong mobile phone users – A consequence of absorption ofradiofrequency fields? Bioelectromagnetics, 24, 152–159.
Anne-Marie L. Chany is a researcher at the Center forInjury Research and Policy at Columbus Children’sHospital, Columbus, Ohio. She received her M.S. inindustrial engineering/ergonomics at the Ohio StateUniversity in 2004.
William S. Marras is the director of the BiodynamicsLaboratory at the Ohio State University, Columbus,Ohio. He received his Ph.D. in bioengineering andergonomics at Wayne State University in 1982.
Deborah L. Burr is an associate professor of biostatisticsat the University of Florida, Gainesville, Florida. Shereceived her Ph.D. in biostatistics at Stanford Universityin 1985.
Date received: September 30, 2005Date accepted: August 31, 2006