Embed Size (px)
Citation preview

RESEARCH ARTICLE Open Access
The effect of motivational interviewing onoral healthcare knowledge, attitudes andbehaviour of parents and caregivers ofpreschool children: an exploratory clusterrandomised controlled studyRahul Naidu1*, June Nunn2 and Jennifer D. Irwin3
Abstract
Background: Motivational Interviewing (MI) has been used across primary healthcare and been shown to beeffective in reducing the prevalence of early childhood caries (ECC) in preschool children. This study aimed tocompare the effect of MI, in contrast to traditional dental health education (DHE), on oral health knowledge,attitudes, beliefs and behaviours among parents and caregivers of preschool children in Trinidad.
Method: The design of this exploratory study included a cluster randomised controlled trial and semi-structuredfocus groups. Six preschools (79 parents and caregivers) in Eastern Trinidad were randomly assigned to a test orcontrol group (3 preschools in each group). Parents and caregivers in the test-group (n = 25) received a talk on dentalhealth using an MI approach and the control-group (n= 54) received a talk using traditional DHE. Both groups receivedadditional, written dental health information. The MI group also received two telephone call follow-ups as part of the MIprotocol. Both groups were given questionnaires before the talks and four months later. Question items included oralhealth knowledge, beliefs, attitudes, brushing behaviour, oral health self-efficacy, oral health fatalism and a specificinstrument to asses ‘readiness for change’, the Readiness Assessment of Parents Concerning Infant Dental Decay(RAPIDD). Participants in the test-group were also invited to take part in a focus group to share their views on the dentalhealth talk.
Results: At four month follow-up, knowledge items on fluoride use, tooth brushing, dietary practice and dentalattendance increased in both the test (DHE +MI) and control (DHE) groups ((p < 0.05, Chi Square test). In the test-groupthere were increases in mean child tooth brushing frequency and reduction in oral health fatalism (p < 0.05 t-test).Findings from a thematic analysis of the focus group suggested that the MI talk and telephone follow-upwere well accepted and helpful in supporting parent and caregiver efforts to improve oral health practices fortheir preschool children.
Conclusion: In this exploratory controlled study there was some evidence that using an MI approach when deliveringoral health information had a positive effect on parent/ caregiver oral health knowledge, attitudes and behaviourscompared to traditional DHE. There is need for further research involving the use of brief-counselling techniques in thisCaribbean population.
Keywords: Preschool children, Oral health motivational interviewing, West Indies
* Correspondence: [email protected] of Dentistry, The University of the West Indies, St Augustine, Trinidadand TobagoFull list of author information is available at the end of the article
© 2015 Naidu et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium,provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Naidu et al. BMC Oral Health (2015) 15:101 DOI 10.1186/s12903-015-0068-9

BackgroundParents and caregivers can be considered gatekeepers forthe oral healthcare of preschool children, therefore theiroral health knowledge, beliefs, attitudes and behaviour maydirectly, or indirectly, influence early childhood oral health.Traditional dental health education approaches with a
main focus on improving parental oral health knowledgehave not been effective in improving preschool children’soral health [1–3]. For instance, traditional generic recom-mendations such as ‘brush your child’s teeth twice a dayand reduce consumption of sweet snacks and drinks’ havehad limited success in changing oral health practices [4].Behaviour change techniques (BCT), including face-
to-face counselling, have been effective across primaryhealthcare [5]. BCTs have been described as an ‘observ-able, replicable and irreducible component of an inter-vention designed to alter or redirect causal processedthat regulate behaviour’ [6]. One such BCT is Motiv-ational Interviewing (MI), defined as “a person-centredcounselling style for addressing the common problem ofambivalence about change” [7]. MI differs radically fromtraditional health education approaches in which it is as-sumed from the outset that a person is prepared to act
upon information imparted to them by an expert(health professional/ educator). Rather than the healthprofessional assuming the role of ‘expert’, MI places theclient/ patient in that role, letting them decide how tointerpret and integrate information in the context oftheir lives own and social circumstances and whether itis relevant for them [3].During MI the health professional/educator attempts to
resolve ambivalence toward change in the client/patientand ‘evoke’ motivation that is already there by the eliciting‘change-talk’ and using ‘reflective listening’. This meansasking questions like: What do you want to change? Howmight you go about it? What are the best reasons for doingit and how important is it you? [7]. MI therefore sees be-haviour change as a partnership between the client / patientand counsellor / health educator that respects autonomy,enabling the client / patient to feel engaged, understoodand empowered.Though not strictly a theory of behaviour change, MI
does share some elements of the Transtheoretical Model(TTM) as proposed by Prochaska et al. [8]. Throughwork with people with addictive behaviour, the TTMwas developed to understand self-initiated and profes-sionally assisted changes in health behaviour. The TTMpresents a series of key stages though which an individ-ual must pass before adopting a new behaviour. Thesestages are (a) Precontemplative, (individual has noawareness of the problem or intention to change behav-iour) (b) Contemplative (Individual aware of problemand thinking about change) (c) Preparation (Individualhas intention to change but not yet ready), (d) Action(Individual attempts behaviour change), and (e) Main-tenance (individual consolidates change to prevent re-lapse) [9]. As in MI, the concept of increasing self-efficacy and personal empowerment are believed to bekey elements in the process of change, these also beingfundamental aims of health promotion.Despite a sizable body of evidence from medical re-
search, the potential of MI in dental health care isless well understood [10]. A recent systematic review onthe effectiveness of MI compared to conventional healtheducation (CE) suggested that MI outperformed CE in im-proving oral health behaviours in infants and preschoolchildren, mainly in relation to oral hygiene, but not indietary habits [10]. This evidence is largely based on studiesby Weinstein et al. and Harrison et al. [11–13]. These stud-ies reported findings of a two-year randomized controlledtrial of MI involving 240 infants aged 6–18 months fromPunjabi Sikh immigrant families living in British Columbia,Canada. In this blinded, randomized control trial, the ex-perimental group received a dental health pamphlet andvideo, along with MI delivered by trained Indo-Canadianwomen lay counsellors (who were not health professionals),using a specifically developed protocol. Mothers in the
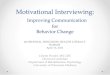
Fig. 1 Response to the study
Naidu et al. BMC Oral Health (2015) 15:101 Page 2 of 15

control group received only the initial pamphlet and videoand no telephone follow-up. After two years, a 46 % lowerprevalence of decayed tooth surfaces was reported in chil-dren whose mother had received MI compared to thosewhose mothers received only pamphlets and videos. Itshould be stated that in these studies the oral health behav-iour that most likely related to the reduction in ECC, wasthat families in the MI group attended more routinely forfluoride varnish application than the control families. Thiscould also suggest that mothers in the MI group felt morepositive about oral health care for their children and moti-vated to access preventive dental services.Less promising results were reported in a randomized
study of over 1000 low-income African-American familieswith children (0–5 years) [14]. The test-group involvedMI for caregivers, a 40-min discussion about whatchanges they could make to achieve oral health goals fortheir child delivered by trained interviewers and a 15-minhealth education DVD. The control-group received thehealth educational DVD only. At two-year follow-up,apart from ‘checking the child’s mouth for pre-cavities’,there were no statistically significant differences in oralhealth behaviour of caregivers between test and controlgroups and no statistically significant difference in the de-velopment of untreated caries in the children.The potential of MI in improving oral health care
may therefore still be considered controversial [10].Nevertheless, a recent evidence-based national clinicalguidelines for caries prevention from the UK states“oral health promotion interventions should be basedon recognised health theory behaviour and modelssuch as MI [15].Previous research as shown the prevalence and severity
of ECC in Trinidad (an island nation in the West Indies)to be related to parental oral health behaviours and accessto dental care [16] as well as families with preschool chil-dren being in need of practical support to overcome bar-riers to achieving effective preventive care [17]. However,no research has been conducted in the English-speakingCaribbean, assessing the effectiveness and appropriatenessof community-based oral health promotion that includesthe use of brief-counselling approaches such as MI forfamilies with preschool children.The aim of this study was to assess the effect of an MI
approach delivered in a group-setting, on parent /care-giver oral health knowledge, beliefs, attitudes and behav-iour toward the oral healthcare of their preschoolchildren, by contrast with traditional dental health edu-cation (DHE), in an exploratory community-based study.
Objectives
� To assess the effect of MI on participants’ oralhealth knowledge, beliefs and attitudes, tooth
brushing behaviour, oral health self-efficacy and oralhealth fatalism compared to DHE.
� To assess the effect of MI on participants’ ‘readinessfor change’, compared to DHE.
� To assess the effectiveness of MI delivered in agroup-setting.
� To explore participants’ views and opinions of theMI intervention.
MethodTo achieve the objectives of this exploratory study twostudy designs were employed, a cluster randomised con-trolled trial and semi-structured focus groups. Quantita-tive methods were used to test the effectiveness of MIcompared to DHE and a qualitative approach employed toexplore participant experience with the MI intervention.
Sample selectionThe accessible population group for the MI interven-tion were families of children attending preschoolswithin the catchment area of the Arima District HealthFacility (Eastern Trinidad). This Health Centre alsohoused the local dental clinic, staffed by Dental Nurses(the equivalent of dental therapists in the UK), whowould be assisting in the research.The sampling frame consisted of 12 preschools on a con-
tact list for community dental outreach activity by DentalNurses working at the Arima District Health Facility. Toenable involvement of the two Dental Nurses in this re-search concurrent to their clinical commitments in the Dis-trict Health Facility, it was decided that a maximum of sixpreschool would be manageable within the time-frame ofthis pilot study. The 6 preschools (clusters) were drawnrandomly from the contact list and subsequently assignedto the test group (DHE+MI) or the control group (DHE),with 3 preschool clusters in each group. The placement ofpreschools in a particular study group was based on simplerandomization (preschools numbered 1–6 and these num-bers randomly assigned to test or control group).
Approval and consentEthical approval was obtained from the Faculty of MedicalSciences Research Ethics Committee (The University of theWest Indies). For the selected preschools, letters of requestto be included in the study were sent to the head teacher /preschool administrator, for each preschool. When approvalwas obtained, packages were then hand–delivered by a den-tal nurse to each preschool. These packages contained in-formation about the study and a consent form requestingparent/caregiver participation and the study questionnaire.These documents were distributed to parents/caregivers viathe head teachers, who were also asked to collate thereturned consent forms and completed questionnaires, forcollection by the study team.
Naidu et al. BMC Oral Health (2015) 15:101 Page 3 of 15

Experimental design and MI protocol
� Control group – (Dental Health Education)All participants (parents and caregivers) in thecontrol group were given a 30 -min talk (as a group)on dental care of preschool children’s teeth by aDental Nurse. This talk included advice on diet, oralhygiene, fluoride use and dental attendance. At theend of the talk, participants were given a DHEleaflet reinforcing the information to take home. Allparticipants in the control-group were given dentalhealth products (toothpaste samples and floss) as atoken of appreciation for taking part in the study.The three control group-talks included 6, 13 and 35participants, respectively.
� Test group – (Motivational Interviewing & DentalHealth Education)Participants in the intervention group received a 30-min talk (as a group) based on a Motivational Inter-viewing approach, delivered by an MI counsellor/educator (RN) (a dentist trained in MI), assisted bya Dental Nurse. Training of the MI counsellor /edu-cator involved a one-day course (8 h) on Motiv-ational Interviewing and coaching skills for healthprofessionals that included both applied (hands-on)and theoretical elements, with the theoretical mate-rials also made available for self-study.The group-talk was based on an MI protocol designedto aid delivery of oral health information to familieswith young children: Motivate your Dental Patient: Aworkbook -Public Health / Paediatric Edition [18].All participants in the test group received the sameDHE information leaflet as the control group alongwith toothpaste samples as tokens of appreciation.All the talks took place at the preschools after a
normal school day. The three test group-talks in-cluded 4, 9 and 12 participants respectively.The outline of the study protocol and MIintervention with intended goals of each contact andthe time-line is shown in Table 1.
Details of the MI group-talkThe MI provider established rapport by showing concernand getting the parent/caregiver to talk about their child’soral health and their goals for their own and their child’soral health and oral healthcare (using open-ended questionsand affirming positive efforts). Questions were themedaround the following topics: Eliciting commitment tochange, identifying potential problems, enhancing commit-ment to change, and recognizing resistance to change.Examples of these questions were:
Tell me about your child? What do you want for yourchild’s oral health teeth? “What are your worst fearsabout your child’s teeth? What are you dental carechallenges? How would you like things to have turnedout? How could it be better? “What do you want foryour child’s teeth in the future?” If you could have onewith wish for your child’s teeth, what would it be?”
� Paraphrasing the parent/caregiver’s wants anddesires for their child’s oral health. (Using reflectivelistening and summarizing parent/caregiver goals).For example:
“Thank you for telling me about your child, what Iunderstand is that you would like your child to……isthat accurate?”
Table 1 Summary of the MI intervention / study protocol
Mode of contact, venue & time-line Objective
First contact Test-group - MI group-talk Given at preschools by MIcounsellor / educator (RN) and Dental Nurse
For Test-group - Establish rapport and discuss oral health goals. Introducedental health menu items. Use of MI to support change to participant’s oralheath behaviour (OARS approach). Given written dental health information.
Control-group - DHE group-talk Given at preschools by Dental Nurse. For Control-group–delivery of verbal and written dental health information.
Oral health questionnaire given to all participants in Test andControl-group.
Collection of baseline data on oral health knowledge, attitudes and behaviour& Readiness Assessment of Parents Concerning Infant Dental Decay (RAPIDD)
1st MI follow-up with Test-group 2 weeks after MI group-talk.(telephone contact by Dental Nurse)
As part of MI, provide support and encouragement for participants. Re-establish oral health goals and commitment to items selected from oral healthmenu options. Help to solve problems encountered.
2nd MI follow-up to Test-group 1 month after MI group-talk(telephone contact by Dental Nurse)End of MI intervention
As part of MI, promote maintenance of any positive changes made to oralhealth behaviour. If needed offer further advice and help with problemsencountered.
Oral health questionnaires to all participants in Test and Control-group(4 months after MI group-talk)
Collection of questionnaire data:Oral health knowledge, attitudes andbehaviour.& RAPIDD.
Focus group with a sub-sample of participants in Test-group atpreschool.(7 months after MI group-talk)
Collection of qualitative data on participant experience of the MI intervention.
Naidu et al. BMC Oral Health (2015) 15:101 Page 4 of 15

� Presenting dental health menu options.Participants in the MI group were shown andencouraged to share their thoughts about a writtenlist of preventive options, termed the Dental HealthMenu (Table 2). These options were based on thoselisted in the Weinstein protocol [18] but modified totake account of participants with older children,along with items based on views expressed byparents and caregivers of preschool children fromprevious research in Trinidad [17]. From this list,participants were asked to choose and to commit toitems they felt able to, as part of the interventionand follow-up.
Telephone follow-upAs well as the MI group-talk at baseline, for those includedin the test group, there was a follow-up of participants viatelephone contact at two weeks and at one month. Thiswas to maintain contact between participants and the MIteam, problem solve, reinforce commitment and providesupport. Without follow-up, new behaviours may not betried out or the new behaviour may be tried out but notmaintained because of (a) unanticipated problems (b) newbehaviour was not integrated into daily routine causing re-lapse [12]. The telephone follow-up was undertaken by adental nurse who had been taking field notes.Two dental nurses were trained for this phase of the
intervention by the MI counsellor /educator (RN) in aone-hour, face-to-face training session that includedreviewing the written follow-up protocol. This documentcontained a telephone ‘script’ used in the Weinsteinprotocol. It was agreed that the script was not to befollowed word-for-word but used as a basis / referencepoint for the telephone conversations.Questions included in the telephone follow-up in-
cluded the following: “I am calling to go over your plan
(dental health menu choices).” “Let’s go over parts of theplan that are a problem, sometimes a small adjustmentcan make a big difference” “Another mother I spoke to,had a similar problem …she tried (insert example)…itseemed to work for her family…you are the expert onyour family, what do you think?” [18]
InstrumentsAt baseline and 4 months later, parents and caregiverswere asked to complete a self-administered oral healthquestionnaire This instrument contained two main ele-ments (a) Oral health knowledge, attitude and behaviourand (b) An assessment of ‘readiness for change’.
(a)Oral health knowledge, attitude and behaviourThe oral health section of the instrument includeddemographic information, along with aquestionnaire on oral health knowledge, beliefs andattitudes, previously used in research among familieswith young children attending a dental hospital inTrinidad [19]. All questions in this instrument wereincluded in the present study. Additional questionson brushing frequency (how many times in the lastweek did your child brush his/her teeth in the lastweek?), oral health self-efficacy (OHSE) and oralhealth fatalism (OHF) were item subscales used in astudy of children aged 1–5 from low-income AfricanAmerican children in the USA (Detroit DentalHealth Project), which were found to have good in-ternal reliability and validity [20, 21].The adapted instrument in the present study (i.e.combination of the Trinidad questionnaire and thequestion items from the Detroit questionnaire) wasreviewed for face validity by the local researchcoordinators (RN, JN) and found to be appropriatefor language and question structure.OHSE was scored as follows: How confident are youthat you can get your child’s teeth brushed atbedtime in the following situations?: When under alot of stress, when feeling low, when feeling anxious,feeling too busy, when feeling tired, worrying aboutthings, when your child doesn’t stay still when youyou want to brush them, when told by your child he/she does not feeling brushing.For each of these items the responses were recordedon a 4-point scale: (4 = Very confident to 1 = Not allconfident). OHF was measured on a 5-point scale, 5= Strongly agree to 1 = Strongly disagree, for the fol-lowing statements: ‘Most children eventually developcavities’, ‘Cavities in Baby teeth don’t matter sincethey fall out anyway’.
(b)The Readiness Assessment of Parents ConcerningInfant Dental Decay (RAPIDD)
Table 2 The Dental Health Menu (participants could selectsome or all of the advice options)
• If breastfeeding discontinue.
• Stop bottle feeding (switch to cup).
• Don’t give sugary drinks at night.
• Limit sweet drinks to mealtimes and try to give natural fruit juiceinstead of colas or other sweet drinks.
• Help to brush your child’s teeth twice a day (one of which should beat bedtime)
• Help to brush from behind your child.
• Use fluoride toothpaste (pea size amount)
• Limit sweet snack to no more than three times a day at mealtime.
• Use fruits and savoury snacks instead of chocolates and candies.
• Register child with a dental clinic.
• Take your child for a dental check-up and fluoride varnish treatmentevery six months.
Naidu et al. BMC Oral Health (2015) 15:101 Page 5 of 15

The parent/ caregiver oral health questionnaire alsoincluded a specific instrument, the ReadinessAssessment of Parents Concerning Infant DentalDecay (RAPIDD) developed by Weinstein and Reidy[22]. Based on the Transtheoretical /stages of changemodel (TTM), this instrument was designed tomeasure parent/caregiver ‘readiness for change’.Using four constructs: Openness to HealthInformation, Valuing Dental Health, Convenienceand Change Difficulty and Child Permissiveness,RAPIDD attempts to assess whether the parent/caregiver is at one of the following stages: pre-contemplative, contemplative, preparing for action,with respect to their child’s oral healthcare. TheRAPIDD instrument was validated in a study amongfamilies with young children (age 6 to 36 months) inthe US Commonwealth of the Northern MarianaIslands, in the Pacific. Again, for use in the presentstudy, the instrument was assessed for face validityand modified for use with a slightly older age-group(3 to 5 years) by the authors (RN, JN). This includedrewording of questions relating to bottle-use. Table 3shows the four RAPIDD constructs and correspond-ing construct items. It should be noted that, withinthe questionnaire, these items are not themed byconstruct but listed as statements for which the par-ticipant is asked to agree with on a 5-point Likertscale (5 = Strongly Agree, 4 = Agree, 3 = Neitheragree or disagree, 2 = Disagree, 1 = Strongly Dis-agree). Mean scores are derived for each of the fourRAPIDD constructs.
In the present study, RAPIDD data were used toassess participant’s ‘readiness for change’ as anoutcome measure of the MI intervention based onmean scores for the above-listed constructs andidentified as pros and cons. As parents and care-givers weigh both the pros and cons of changingtheir behaviour, tipping the balance in favour of prosand reducing the cons may facilitate behaviourchange. Two constructs assess pros: ‘Openness toHealth Information’ and ‘Valuing Dental Health’ andtwo constructs assess cons: ‘Convenience andChange Difficulty’ and ‘Child Permissiveness’.
Statistical analysisThe Chi square test was employed for categorical vari-ables related to oral health knowledge (baseline versusfollow-up), for test and control-group. These were: causesof caries, toothbrush size, brushing position, diet / frequencyof sweet snacks, toothpaste and fluoride use (significancelevel: p < 0.05).Independent sample t-test was employed to assess the
effect of the intervention on continuous variables relatedto oral health behaviours and attitudes. These wereTooth brushing frequency, Oral health Self-efficacy, Oralhealth fatalism, and RAPIDD constructs. Mean scoresfor these items were compared at follow-up between testand control-group (significance level: p < 0.05).
Qualitative study (Focus groups)The present study used a focus group approach to col-lect qualitative data on participants’ experiences with the
Table 3 Modified RAPIDD constructs
Construct Construct items
Openness to health information • I would take my child off the bottle if a healthcare professional told me to do so.
• I get advice on taking care of my baby from TV, radio, magazines and internet.
• I feel comfortable asking a healthcare professional about ways to care for my child.
• It is easier for me to get answers about ways to take care of my child from the healthcare professional
Valuing Dental Health • Keeping my child’s teeth healthy is important to me.
• My child benefits a lot when I clean his/her teeth.
• I like the idea of a dentist or dental nurse putting fluoride on my child’s teeth to protect them from cavities
• I believe using fluoride toothpaste every day would help my child’s teeth
Convenience and Change Difficulty • It would be hard to give my child less sweets.
• My child gives me a hard time when I try to brush his/her teeth.
• It is not easy to use fluoride toothpaste every day.
• I am unable to put my child to sleep without feeding him/her.
Child Permissiveness • Food and drinks that are not sweet don’t taste good to my child.
• I feel like a bad parent if I don’t give my child sweets.
• My child is happier when I give him/her something sweet in the bottle.
• I makes me feel good to give my child something sweet to eat.
Naidu et al. BMC Oral Health (2015) 15:101 Page 6 of 15

MI intervention. Focus groups are one of severalmethods for acquiring qualitative data. They can be con-sidered as an semi-structured interview with a group ofpeople who are encouraged to interact with each otherand the facilitator, using group dynamics to stimulatediscussion, gain insights and generate ideas to explore achosen topic in depth.
Focus group sample selectionIn liaison with the preschool head teachers / administra-tors, a focus group discussion was arranged for parents/caregivers from one of the three preschool (clusters) thathad received the MI intervention. This took place6 months after the end of MI intervention (i.e. last tele-phone follow-up). Due to the busy schedule of events inthe other two preschools their head-teachers /adminis-trators indicated that they were unavailable for inclusionin this phase of the study. All parents /caregivers fromthe preschool who had attended the group-talk and en-gaged in the follow-up were invited to participate,through the head-teacher/ administrator. The venue forthe focus group discussion was the preschool mainclassroom, after working hours, during the middle of aschool week.The focus group was run by a facilitator / moderator
(RN), previously trained in qualitative methodology(26 h, didactic and practical,) and a dental nurse, whoserved as the assistant moderator.
Conduct of the focus groupThe facilitator/ moderator, welcomed the parent’s andcaregivers to the event. To obtain informed consent forparticipation in the focus group, the purpose and conductof the event (focus group) was explained i.e. an open dis-cussion (not an interview) around the theme of preschoolchildren’s dental healthcare based on the dental healthgroup-talk and telephone calls given some months previ-ously. It was explained that an audio recording of the dis-cussion would be made but that all comments andopinions offered would remain anonymous and individ-uals would not be identified by name during transcriptionand reporting of the findings. It was also emphasized thatall comments (positive or negative) would be consideredof value. All the parents and caregivers present gave verbalconsent to participate in the focus group discussion. Par-ticipants were also invited to complete a short form torecord socio-demographic information.To initiate and facilitate the discussion the moderator
used a focus group topic guide (Table 4). This topic guidewas designed to help explore how participants felt aboutreceiving the MI intervention (group talk, dental healthmenu and telephone follow-up), along with specific issuesrelated to making changes to oral healthcare practices androutines following the intervention. Questions in the topic
guide were open-ended and not asked in a specific orderbut rather in response to the flow of the discussion.The discussion was recorded on a digital audio recorder
and field notes taken by the assistant moderator. At theend of the session, participants were thanked and givendental products as tokens of appreciation (toothpaste /floss samples). Light refreshments were provided beforeand during the discussion.
Qualitative data analysisA thematic content analysis was used to analyse thequalitative data collected in the focus group session. Asa first step, the focus group audio recording was tran-scribed into a Word document. The verbatim transcriptwas then numbered line-by-line for identification. Afterseveral readings of the transcript, field notes and listen-ing to the audio recording, the data underwent a processof initial labelling of sections of the transcript by placingcodes in the text margin. Similarly coded pieces of thetranscript were re-assembled near to each other by cut-ting and pasting text sections into a new Word docu-ment. These initial codes (which could overlap) were thenfurther developed to identify emerging early ‘themes’(proto-themes) which were themselves further refined intothe final themes These themes were reported in the resultswith supporting verbatim quotes from the transcript.
Data trustworthiness and reflexivityTo determine data credibility (member checking), at theend of the session participants were invited to give theiropinion (off-record) as to whether the discussion had ac-curately documented their own experiences [23]. Allfocus group participants agreed that the points discussedand views presented had been a good representation oftheir collective and individual experiences with the MI
Table 4 Focus group topic guide
• After the group talk how confident were you in making any changes?
• Did any of the things we talked about help you to make a change? (Ifyes, what were they/)
• What did you find most difficult to change?
• What were the easiest things to change?
• What experiences did you have with tooth brushing or changing thetype of feeding?
• Did any of you have to change from a feeding bottle to a cup? Howwas that for you?
• Did the talk feel different to any dental talks / advice you had before?(If so how?)
• Was the dental health menu helpful? (If so how?)
• What did you feel about the telephone follow-up calls (Were theyhelpful)?
• Overall how have you been managing with your child’s oralhealthcare and are there any problems you are still having?
Naidu et al. BMC Oral Health (2015) 15:101 Page 7 of 15

intervention. Reflexivity in qualitative research recog-nises that the researcher is part of the process of produ-cing the data and interpreting their meaning [23, 24].Furthermore, consideration was given to the facilitator/moderator having also been an active part of the MIintervention. This was not however, believed to have in-fluenced the views expressed in the focus group discus-sion or subsequent interpretation of the data.
ResultsThe following section describes the results of the MIintervention study, from the data gathered in the oralhealth questionnaire as well as the results for thequalitative study, based on a thematic analyses of thefocus group data.
Intervention study enrolment and retentionFrom 150 parents/caregivers that were invited, 79 agreedto participate in the study (response rate 53 %). From thisinitial study enrolment, at follow-up 20 and 21 partici-pants remained in the test and control-groups, respect-ively (Fig. 1). A significantly higher proportion ofparticipants dropped out of the control-group com-pared to the test-group by the end of the study (ChiSquare p < 0.001). Based on post-hoc analysis thepower of this study was 61 %.
Sample characteristicsTable 5 shows the sample characteristics at baseline. Themajority of the participants were in the 25–34 year agerange indicating a sample of young adults as would beexpected among parents of preschool age children. Themajority were females of mixed ethnicity and most par-ticipants were in manual employment or housewives.Most participants were educated to secondary level andcared for 1–2 children. At baseline in the test-groupthere were significantly less participants of African eth-nicity, a greater proportion employed in professional /managerial jobs and having tertiary level education,compared to the control-group (Chi square p < 0.05).Compared to the control group, a significantly greaterproportion of participants in the test-group did nothave a regular dental clinic for their child and reportedfinding it easier to find a medical doctor than a dentist(Chi square p < 0.05)
Oral health knowledgeTable 6 describes the effect of the MI and traditionalDHE, on oral health knowledge in the test and control-groups respectively, at 4-month follow-up. Compared tobaseline, in the control-group there was a significant in-crease in the proportion of participants who correctlyknew that their child’s teeth should be brushed from
behind and that fluoride varnish should be administeredevery six months.In the test-group, compared to baseline, significantly
greater proportions of participants, as compared withthe test group, knew the correct quantity of toothpasteto use (pea size amount), the correct brushing position,importance of six monthly fluoride varnish applicationand that main mealtimes were the safest time to givesugary snacks was at mealtimes (Chi square test).
Oral health behaviour and attitudes and RAPIDDTable 7 describes the effect of the MI and traditionalDHE, on oral behaviours and attitudes at 4-monthfollow-up. In the test-group there was a significant in-crease in the child weekly brushing frequency and a sig-nificant reduction in oral health fatalism, compared tothe control-group (independent sample t-test). Therewere no statistically significant changes in mean scoresfor the oral health self-efficacy or the RAPIDD con-structs / RAPIDD pros and cons.
Qualitative findingsThe following section describes the results of thequalitative study, based on the thematic analysis ofthe focus group discussion. Six participants from the20 parents and caregivers who had remained in theMI intervention study at the four-month follow-up,accepted an invitation to take part in the focus groupdiscussion. All participants were female, ranging inage from 25–34, with two thirds (4) of Indian ethni-city. Four participants stated secondary school wastheir highest level of education the remainder edu-cated to tertiary level. Three participants were in pro-fessional / managerial occupation, the others being inmanual occupation and housewives. Two participantscared for more than one child.
Views on the MI group-talkDuring the discussion it became apparent that participantshad not had any kind of dental health education (DHE)delivered to them prior to the MI group talk, thereforethey could not compare it to other types of DHE delivery.However, they all appeared to feel comfortable with theMI approach in particular, the open discussion of oralhealth goals and barriers along with sharing of experienceswith other parents / caregivers. Opinions offered on thetelephone follow-up element of the MI protocol suggestedthat it did not feel intrusive and was helpful; no partici-pants indicated discomfort with that aspect of the MI.
I think it (MI group talk) was better because sometimeyou might even forget about something to mention andanother parent might bring it up and you know youwould benefit from it.
Naidu et al. BMC Oral Health (2015) 15:101 Page 8 of 15

Yes, it was really good (MI group talk), because Inever knew about the fluoride varnish before and I didenquire from my dentistThat helped me amm… a lot (telephone follow-up)..and making sure that she brushes her teeth twice-a-day… because sometimes you know, they small soyou’ll say well if they fall asleep, so we now try to kindof wake her up and brush it…
Mode of delivery of oral health informationMixed opinions were expressed about the value of givingwritten material but most found written information help-ful as a reinforcement / reminder of issues presented in theMI group talk. It was unclear at times if participants werereferring to the value of the dental health information leaf-let or the dental health menu used as part of the MI, as tosome participants they may have seemed similar in content.
I don’t think it would matter to me to much because Imean at the end of the day we could verify theinformation (information leaflet) on the internet ‘causeeverything is there on the internet.I find the talk does be better because sometimes youget the hand-out (Information leaflet) and youmisplace itYou should give both (MI group talk and writteninformation)
Changing oral health practicesAs a result of the MI intervention most participants hadtried to implement some changes to oral health practicesfor their child such as twice daily tooth brushing, changeof brushing position, use of fluoride toothpaste etc. In par-ticular, after the MI intervention some participants ap-peared to have made concerted effort to overcomepractical difficulties such as their child falling asleep be-fore night-time brushing. Following the intervention therealso appeared to be greater understanding of the import-ance of using fluoride toothpaste and supervision of toothbrushing. Despite it being a little challenging, after theintervention, participants seemed to feel more confidentin adopting the brushing from behind method. For someparticipants the follow-up phase of the intervention wasparticularly helpful to support changes that had beenmade.
I did learn from the talk because the amount oftoothpaste.. so I changed that…she kind of like wants to brush her teeth on her ownnow but I still make sure and do with her it at leastonce-a-day especially by bedtime to make sure and doit properly.How I position the child, ‘cause I used to do it from infront and now I know how to do it from behind so I
Table 5 Sample characteristics at baseline
Control Test All
Age group n % n % n %
18-24 9 16.7 1 4.0 10 12.7
25-34 22 40.7 16 64.0 38 48.1
35-44 17 31.5 5 20.0 22 27.8
45-54 2 3.7 2 8.0 4 5.1
55-64 2 3.7 0 0.0 2 2.5
0ver 65 1 1.9 0 0.0 1 1.3
Missing 1 1.9 1 4.0 2 2.5
Total 54 100 25 100 79 100
Not significant (Chi square)
Gender
Female 45 83.3 21.0 84.0 66 83.5
Male 7 13.0 13.0 16.0 11 13.9
Missing 2 3.7 3.7 0.0 2 2.5
Total 54 100 100 100 79 100
Not significant (Chi square)
Ethnic group
African 24 44.4 7 28.0 31 39.2
Indian 3 5.6 7 28.0 10 12.7
Mixed 26 48.1 9 36.0 35 44.3
Missing 1 1.9 2 8.0 3 3.8
Total 54 100 25 100 79 100
p < 0.05 (Chi square)
Occupational group
Professional 1 1.9 2 8.0 3 3.8
Managerial / lower professional 6 11.1 9 36.0 15 19.0
Non manual (skilled) 13 24.1 3 12.0 16 20.3
Skilled manual 6 11.1 2 8.0 8 10.1
Semi-skilled manual 3 5.6 1 4.0 4 5.1
Non-skilled manual 7 13.0 0 0.0 7 8.9
Housewife/ unemployed 13 24.1 7 28.0 20 25.3
Missing 5 9.3 1 4.0 6 7.6
Total 54 100 25 100 79 100
p < 0.05 (Chi square)
Highest level of education
University 8 14.8 9 36.0 17 21.5
Technical college 6 11.1 4 16.0 10 12.7
Secondary 32 59.3 9 36.0 41 51.9
Primary 7 13.0 2 8.0 9 11.4
Missing 1 1.9 1 4.0 2 2.5
Total 54 100 25 100 79 100
p < 0.05 (Chi square)
Naidu et al. BMC Oral Health (2015) 15:101 Page 9 of 15

learnt about that. I guess he is more comfortable withme doing it that way.For me it wasn’t a must before (night-time brushing)…then I tried to make sure …
Changing dietary practicesSome of the participants had children who were stillusing the feeding bottle (mainly at night). Though theyexpressed difficulty changing this behaviour in the past,following the MI intervention new efforts were made todiscontinue this practice.
She still begs for the bottle. Well I threw away thenipple (feeding bottle) recently because it was likereally bad but only like in the night.., like if she get uparound three o’clock in the morning but we cut itdown like real plenty.… but you know when she sleeping and start crying forthis bottle, it real hard to go back to sleep. But now Ithrow away the bottle.She would drink the Milo (cocoa drink) in the bottlebut when you give it to her in the pack she would havetwo or three sips and that is it, she want that bottle..
Table 6 Oral health knowledge for control group and test-group – baseline versus follow-up (Chi square test)
Question ControlBaseline
Control Follow-up p value TestBaseline
Test Follow-up p value
n % n % n % n %
Bacteria on the teeth of young children cancause cavities
Yes 50 92.6 18 90.0 22 88.0 18 85.7
No 1 1.5 1 5.0 0.758 0 0 0 0 0.819
Don’t know 3 5.6 1 5.0 3 12.0 3 14.3
What size of toothbrush is best for a young child Small 42 79.2 18 90.0 19 79.0 17 81.0
Medium 8 15.1 2 10.0 0.447 4 16.7 4 19.0 0.633
Don’t know 3 5.7 0 0 1 5.3 0 0
How much toothpaste should be placed on thebrush
Enough to coverbrush
10 18.5 3 15 6 24 0 0
Pea size 33 61.1 17 85 0 .144 14 56.0 19 90.5
Smear 8 14.8 0 0 2 8.0 2 9.5 <0.05
Don’t know 3 5.6 0 0 3 12.0 0 0
From what position should you help to brush In front of the child 35 64.8 9 45.0 11 44.0 0 0
Behind the child 9 16.7 9 45.0 6 24.0 19 90.5 <0.001
From the side 4 7.4 2 10.0 <0.05 4 16.0 2 9.5
Don’t know 6 11.4 0 0 4 16.0 0 0
How much fluoride should be in the toothpaste Not less than1000 ppm
1 1.9 1 5.0 1 4.0 1 4.8
450-600 ppm 3 5.6 2 10.0 0.590 0 0 4 19.0 0.071
Don’t know 50 92.6 17 85.0 20 83.3 16 76.2
Fluoride varnish should be placed on teethevery 6 months
Yes 2 3.7 10 50.0 4 16.7 16 76.2
No 8 14.8 1 5.0 <0.05 0 0 1 4.8 <.0001
Don’t know 14 81.5 9 45.0 20 83.3 4 19.0
When is it safe to give sugary drinks and snacks Between meals 25 46.3 9 45.0 7 28.0 9 42.9
At mealtimes 5 9.3 1 5.0 4 16.0 11 52.4
At night 0 0 2 10.0 0.200 0 0 0 0 <0.05
in the morning 7 13.0 3 15.0 3 12 0 0
Don’t know 17 31.5 5 25.0 11 44.0 1 4.8
When should you take your child for their firstdental visit
Only if problems 1 1.9 1 5.0 2 8.0 1 4.8
By 1 year-old 21 38.9 4 20.0 5 20.0 7 33.2
When some adulttooth
1 1.9 1 5.0 0.412 1 4.0 0 0 0.178
When all baby teeth 20 37.0 11 55.0 8 32.0 11 52.4
Don’t know 11 20.4 3 15.0 9 36.0 2 9.4
Naidu et al. BMC Oral Health (2015) 15:101 Page 10 of 15

Changing dental attendance behaviourAfter the MI intervention some participants had madeattempts at taking their child for a dental visit but hadbeen hampered by difficulty in getting appointments.Overall, participants’ awareness of dental service avail-ability for young children appeared to have improvedwith more considering the dental hospital along withprivate practice. There was a persisting view that dentalattendance was only for problems and, in one instance,an inquiry about fluoride varnish at a private dentalpractice was met with the general dental practitioner(GDP) not being aware of this as a preventive option forprimary teeth.
Well we brought her to a private dentist andsometimes you have a waiting period, like if it’s aemergency probably have to wait for an appointment.
…sometimes you might have to get like four Saturdaysafter, or something like that….even if the child in pain.
Barriers to changeFor some participants, the main barrier to changing oralhealthcare practices was the child’s non-acceptance ofnew brushing regimes, toothpaste use and change fromfeeding bottle to cup. Participants recounted concertedattempts to implement new oral health practices. Some-times these efforts were further hampered by other fam-ily member involvement, in particular grandparents.
…she not even giving up the comforter right now, shewant that to sleep whole night, if that out the mouth,she not sleeping, she will be searching for it on the bed.She just cried and cried…I hide the bottle and give herthe cup.., she says “No Mummy I don’t want it”.
Table 7 Oral health behavior and attitudes at 4-month follow-up, control v test group (Independent sample t-test)
Variable Group n Mean sd 95 %CI p value
Child weekly tooth brushing
Control 20 10.55 4.07 8.77-12.33 <0.01
Test 21 13.09 1.44 12.47-13.71
Self-efficacy
Control 20 24.60 6.91 21.57-27.62 0.379
Test 21 26.79 5.14 24.59-28.99
Oral health fatalism
Control 20 5.95 2.04 5.06-6.84 <0.05
Test 21 4.09 1.73 3.35-4.83
Openness to health information
Control 20 15.35 2.64 14.19-16.51 0.593
Test 21 15.86 3.32 14.73-16.99
Valuing dental health
Control 20 19.80 8.71 16.07-23.52 0.847
Test 21 19.42 0.81 19.07-19.77
Convenience and change difficulty
Control 19 9.58 2.34 9.23-9.94 0.410
Test 21 7.67 3.21 6.30-9.04
Child permissiveness
Control 20 8.30 3.86 6.61-9.99 0.352
Test 21 7.33 3.63 5.78-8.88
RAPIDD pros
Control 20 35.15 9.58 30.95-39.35 0.952
Test 21 35.29 3.38 33.84-36.74
RAPIDD cons
Control 19 17.37 4.98 15.13-19.61 0.154
Test 21 15.00 5.28 12.74-17.26
Naidu et al. BMC Oral Health (2015) 15:101 Page 11 of 15

…she likes to lie down and drink her tea…not sitdown. The only way she drinking from a cup is withMilo (sweetened cocoa drink)….It does be harder for you too, cause they think theyright (grandparents).. I tell them she is three, shesupposed to cut off the bottle….
DiscussionAlthough not directly linked to behaviour change, im-proving the knowledge and awareness of parents andcaregivers is a key element of dental prevention in pre-school children [25–27].In this study, participants who received MI showed im-
proved knowledge across a wider range of knowledgeitems (correct amount of toothpaste, supervised brushingposition, fluoride varnish, and safest time to give sugaryfoods and drinks) compared to those who received trad-itional DHE. Importantly knowledge of the importance offluoride varnish application also has practical implicationsfor preventive strategies as this clinical intervention is ef-fective in reducing ECC separately and in combinationwith fluoride toothpaste [28, 29]. The reduction in preva-lence of early childhood caries (ECC) following an MIintervention reported in Asian families in Canada, waslargely attributed to a greater uptake of fluoride varnish bythose families [13] possibly due to the parents attachinggreater value to professional preventive care.On the issue of tooth brushing practices, understand-
ing these parents and caregivers’ perspective was vitaland this aspect formed part of the MI conversation thatuses ‘reflective listening’, where, over the course of thesession, the educator / counsellor seeks to increase theclients strength for expressed motivation in order to tar-get a behaviour change. Establishing good tooth brush-ing habits and routines in preschool children can be achallenge for families particularly where it involvedchanges to established daily routines [30].Regular (at least twice daily) brushing with fluoride
toothpaste is a core aspect of caries prevention in pre-school children [31, 32, 27]. Importantly, in this presentstudy, the MI intervention had a significant effect on thispreventive oral health behaviour, with the test-groupclaiming an increased frequency of weekly brushing.Brushing with fluoride toothpaste before the child’sevening bedtime gives further protection, as during thistime the teeth are more vulnerable to the effects ofplaque bacteria [26]. Also, from the views expressed inthe focus group it could be inferred that after the inter-vention, participants felt more confident in their abilityto use the oral health information that was provided. Ex-ploring practical ways to overcome barriers to oralhealthcare for their child/children may also have helpedparticipants to persist with introducing new oral health-care regimes about which they had learned. However,
getting the child to brush at night-time was one of themore difficult behaviours for parents and caregiver tochange, often because the child refused or fell asleep.This is consistent with findings from the UK, where par-ents of preschool children found more difficulty in es-tablishing a routine of tooth brushing at that time of day[30]. Again, based on findings from the focus group, itappeared that some participants in the test-group hadexperienced success with efforts to stop use of the night-time feeding bottle. This was encouraging as this routinemay also have been a particularly difficult one to changeas bottle-use has been associated with issues of closenessand comforting by the mother, as well as ‘buying time’time away from their crying child [33].Miller and Rollnick state that “for a person to change
they must feel both confident in their ability to changeand believe the change is important to them” [34].Brushing behaviour has been reported to be positivelyrelated to maternal self-efficacy [21], therefore, increas-ing parental involvement in tooth brushing for preschoolchildren would requires them knowing it is important[35]. In the present study, differences in self-efficacy didnot reach statistical significance at the four-monthfollow-up. However, an MI approach significantly re-duced parent/caregiver OHF which in turn, may lead toa more positive attitudes toward oral health and in-creased motivation to adopt preventive practices [15].Therefore, how BCTs are delivered may have as muchimpact on outcomes as the technique itself, suggestingthe need for development of a BCT Taxonomy (i.e. amethod of specifying, evaluating and implementing be-haviour change interventions) [6].The concept of ‘readiness for change’, in this study was
explored using the RAPIDD instrument. ‘Readiness forchange’ has been defined as ‘a person’s current thoughts,feelings and attitudes regarding their intention to insti-tute a change in their habits’ [34]. The analyses did notdemonstrate a statistically significant effect of MI on theRAPIDD construct scores. The present findings are alsosimilar to those of Freudenthal who reported an effect ofimprovement in brushing frequency in mothers who re-ceived MI but, apart from ‘valuing dental health’, re-ported no significant changes in the RAPIDD scoresbetween test and control-groups [36].A systematic review, of parental influences on ECC,
highlighted the importance of socio-cultural factors thatare likely to affect mediating variables such as attitudesand oral health beliefs [37] and it has also been suggestedthat the MI approach enables oral health professionals tofocus more on underlying social determinants of disease,by tailoring interventions to suit social circumstances [38]while attempting to develop their ‘readiness for change’.From another perspective, it has been suggested that
MI provides an opportunity to address ‘felt needs’ [39],
Naidu et al. BMC Oral Health (2015) 15:101 Page 12 of 15

which supports a view that primary healthcare profes-sionals should address the needs of families in the contextof their environment and experience [40]. It has also beensuggested that health practitioners are likely to gain agreater sense of achievement from recognising progress inan individual’s ‘readiness for change’ as an important out-come rather than using behaviour change as the only goalsince this may not be measurable in the short term [41].The MI intervention led to a much higher retention
rate of participants in the study, compared to thecontrol-group. This may be a benefit of the MI ap-proach. Importantly, comments from the focus group in-dicated participants in the test-group were comfortablewith the telephone contacts made by the Dental Nursessuggesting that this element of the protocol may havehelped to maintain motivation and commitment fromparticipants. This is consistent with the findings ofWeinstein, who believed that longer telephone or in-person follow-up could add even more value to theprocess [11]. Also the challenges the participants in thepresent study encountered, in trying to alter dietary anddental attendance behaviour, indicates the value of on-going support to achieve these goals.
Limitations of the studySome limitations of the present study must be consid-ered when interpreting the findings.
1. Sample sizes and subsequent group allocations wererelatively small due to difficulty in subjectrecruitment and retention, which has implicationsfor potential coverage of this type of communityintervention. The low response rate may have alsohave resulted in a more motivated group ofparticipants at baseline compared to the targetpopulation, masking effects of the intervention.Furthermore, the sample size in this study resultedin a low study power increasing the probability oftype II errors.
2. In the present study lack of a clear effect of MI onparticipants on oral health attitudes and behavioursmay also have been due to the extent the actual MIdelivered matched the principles of MI i.e. fidelity .Fidelity refers to assessment and monitoring of anintervention as it is actually delivered to clients andits assessment is key to the validity of behaviouralchange interventions [42]. Interestingly, one of thereasons suggested for lack of effectiveness inimproving oral health in one study of preschoolchildren was lack of fidelity to the MI process [14].With regards to this, Moyers et al. have developedan instrument to help clinicians improve in their useof MI by providing feedback by use of theMotivational Interviewing Treatment Integrity
(MITI) code [43]. For the MITI, recordings of theMI session are reviewed by trained coders whoassign a global score based on a 5-point scale for anoverall impression and for each of five specific di-mensions: Evocation, Collaboration, Autonomy/Support, Direction and Empathy [43].
3. Differences in characteristics between the test andcontrol-group at baseline (education level, occupa-tion, experiences of accessing dental care) may haveinfluenced the effect of the intervention. Althoughthe groups were randomly allocated, these socio-demographics imbalances may have been due tosome preschools having significantly more parentsfrom a particular ethnic or socioeconomic group.This also prevents more sophisticated analyses.
4. The duration of the study was short (4 months).This was to avoid further drop-out and loss of con-tact with participants as their children moved on toprimary school / families leave the area.
5. Self-reported questionnaires can be affected byparticipant recall [44]. Furthermore, some responsebias may have resulted from ‘social desirability’ i.e.bias due to clients who misrepresent self-reportedbehaviours by over-reporting behaviours consideredsocially desirable, and under-reporting undesirableones [45].
6. As only one individual was trained to provide theMI talk, the MI method may not be representativeof other MI providers, which limits the ability togeneralize conclusions about its utility.
7. More extensive training in MI for the dental nurseswho undertook the telephone follow-up may havehelped increase fidelity to the MI protocol.
8. Delivery of MI in group settings has not been asextensively evaluated as one-to-one counselling,therefore MI delivered in a group setting has lesspredictable outcomes [7]. Specific limitations being:(a) each group member has less time to engage inthe process of evoking and change-talk (b) Groupdynamics can alter the probability of change-talkand (c) people within the group may reinforce am-bivalence in others.
9. It was not possible to include all parents andcaregivers who received the MI in the focus groupdiscussion as most were unavailable. This limited thesample size and group size of the focus group.However, minimum sample size for focus group hasbeen stated as six [45] and, where there is a highdegree of homogeneity for qualitative studies,samples of less than ten can still achieve datasaturation [46]. Also, as a focus group was notconducted with the control-group it cannot be con-cluded whether participants' experiences of MI weremore positive in comparison to traditional DHE.
Naidu et al. BMC Oral Health (2015) 15:101 Page 13 of 15

10.The impact of the MI intervention compared to thecontrol group may have been exaggerated as DHE isknown to be ineffective for changing oral healthbehaviour.
ConclusionAlthough the findings should be considered as explora-tory, in this controlled study there was some evidencethat using an MI approach when delivering oral healthinformation had a positive effect on parent/ caregiveroral health knowledge, tooth brushing behaviour andoral health fatalism compared to traditional DHE. Theacceptability of the MI protocol, which included follow-uptelephone contact was also good, as indicated by discus-sions with the recipients both during and after the deliveryof the programme. These findings suggest that further de-velopment of this person-centred counselling approachcould be of benefit for improving oral health of preschoolchildren in Trinidad and could form part of oral healthpromotion strategies for this population group.
AbbreviationsBCT: Behaviour change technique; DHE: Dental health education; ECC: Earlychildhood caries; GDP: General dental practitioner; MI: Motivationalinterviewing; OHF: Oral health fatalism; OHSE: Oral health self-efficacy;RAPIDD: Readiness assessment of parents concerning infant dental decay;TTM: Transtheoretical model..
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsRN conducted the fieldwork and data collection. RN and JN contributed tothe design of the study, RN, JN and JI contributed to data interpretation andpreparation of the manuscript. All authors read and approved the finalmanuscript.
Authors’ informationRahul Naidu: Senior Lecturer Community Dentistry, The University of theWest Indies, Trinidad and Tobago. June Nunn: Professor of Special CareDentistry & Dean, School of Dental Sciences, Trinity College Dublin, Ireland.Jennifer Irwin: Associate Professor. School of Health Studies. WesternUniversity. London Ontario.
AcknowledgementsThe authors would like to thank the following for their assistance with thisresearch: Elizabeth Prayman, June Bascombe, Azeeda Ramkissoon, ProfessorAlan Kelly, Dr. Don Morrow, Dr. Tracy Finlayson.
Author details1School of Dentistry, The University of the West Indies, St Augustine, Trinidadand Tobago. 2School of Dental Science, Trinity College Dublin, Dublin 2,Ireland. 3School of Health Studies, Western University, Ontario, Canada.
Received: 26 February 2015 Accepted: 14 July 2015
References1. Tinanoff N, Daley NS, O-Sullivan DM, Douglass JM. Failure of intense
preventive efforts to arrest early childhood and rampant caries: three casereports. Paed Dent. 1999;21:160–3.
2. Weinstein P. Motivational interviewing concepts and the relationship to riskmanagement and patient counselling. J Cal Dent Association. 2011;39:742–5.
3. Yevlahova D, Satur J. Models for individual oral health promotion and theireffectiveness: a systematic review. Austr Dent J. 2009;54:190–7.
4. Ramos-Gomez F, Crystal YO, Domejean S, Featherstone JDB. Minimalintervention dentistry: part 3. Paediatric dental care - prevention andintervention protocols using caries risk assessment for infants and youngchildren. Br Dent J. 2012;213:501–8.
5. Noordman J, van der Weijden T, van Dulman S. Communication-relatedbehaviour change techniques used in face-to-face lifestyle interventions inprimary care: A systematic review of the literature. Patient Ed Counselling.2012;89:227–44.
6. Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W,et al. The Behaviour Change technique (v1) of 93 hierarchically clusteredtechniques: Building an international consensus for the reporting ofbehavior change interventions. Ann Behav Med. 2013;46:46–81.
7. Miller W, Rollnick S. Motivational Interviewing: Helping People Change. NewYork: Guilford Press; 2013.
8. Prochaska JO, DiClimente CC. The transtheoretical approach: crossingtraditional boundries of therapy. Illinois: Don Jones / Irwin; 1984.
9. Prochaska JO, DiClemente CC, Norcross JC. In search of how peoplechange: Applications to the addictive behaviours. Am Psychol.1992;47:1102–14.
10. Gao X, Lo ECM, Ching Ching Kot S, Chi Wai Chan K. Motivationalinterviewing in improving oral health: A systematic review of randomizedcontrolled trials. J Periodontol. 2013;85:426–37.
11. Weinstein P, Harrison R, Benton T. Motivating parents to prevent caries intheir young children. J Am Dent Assoc. 2004;135:731–8.
12. Weinstein P, Harrison R, Benton T. Motivating mothers to prevent caries:confirming the beneficial effect of counselling. J Am Dent Assoc.2006;137:789–93.
13. Harrison R, Benton T, Everson Stewart S, Weinstein P. Effect of motivationalinterviewing on rates of early childhood caries: a randomized controlledtrial. Paed Dent. 2007;29:16–22.
14. Ismail AI, Odersma S, Willem Jedele JM, Little RJ, Lepkowski JM.Evaluation of a brief tailored motivational intervention to preventearly childhood caries. Community Dent Oral Epidemiol.2011;39:433–48.
15. Scottish Intercollegiate Guideline Network (SIGN). Dental interventions toprevent caries in children. Healthcare Improvement Scotland. Edinburgh:2014.
16. Naidu R, Nunn J, Kelly A. Socio-behavioural factors and early childhoodcaries: a cross-sectional study of preschool children in central Trinidad. BMCOral Health. 2013;13:30. http://www.biomedcentral.com/1472-6831/13/30.
17. Naidu R, Nunn J, Forde M. Oral healthcare of preschool children in Trinidad:a qualitative study of parents and caregivers. BMC Oral Health. 2012;12:27.http://www.biomedcentral.com/1472-6831/12/27.
18. Weinstein PW. Motivate Your Dental Patients A Workbook: The PublicHealth / Paediatric Edition. Seattle: University of Washington; 2002.
19. Naidu R, Davis L. Parent's views on factors influencing the dental health ofTrinidadian preschool children. Community Dent Health. 2008;25:44–9.
20. Finlayson T, Siefert K, Ismail AI, Delva J, Sohn W. Reliability andvalidity of brief measures of oral health-related knowledge, fatalismand self-efficacy in mothers of African-American Children. Paed Dent.2005;27:422–48.
21. Finlayson T, Siefert K, Ismail AI, Sohn W. Maternal self-efficacy and 1–5 year-old children's brushing habits. Community Dent Oral Epidemiol.2007;35:272–81.
22. Weinstein P, Reidy CA. The reliability and validity of the RAPIDD Scale:readiness assessment of parents concerning infant dental decay. ASDC JDent Child. 2001;68:129–35.
23. Green J, Thorogood N. Qualitative methods for health research. London:Sage Publications Ltd; 2009.
24. Masood M, Masood Y, Newton JT. Methods of qualitative research indentistry. Dent Update. 2010;37:326–36.
25. Blinkhorn A. Promoting dietary changes in order to control dental caries.Dent Health. 1991;29:3–6.
26. Levine R, Stillman-Lowe CR. The Scientific Basis of Oral Health Education.London: BDJ Books; 2009.
27. Santos A, Nandanovsky P, Oliveira BH. A systematic review and meta-analysisof the effects of fluoride toothpaste on the prevention of dental caries in theprimary teeth of preschool children. Community Dent Oral Epidemiol.2013;41:1–12.
28. Weintraub J, Ramos-Gomez F, Jue B, et al. Fluoride varnish should be part ofcaries prevention programmes. Evidence-Based Dent. 2006;7:65–6.
Naidu et al. BMC Oral Health (2015) 15:101 Page 14 of 15

29. Marinho V. Cochrane reviews of randomized trials of fluoride therapies forpreventing dental caries. Eur Archives Paed Dent. 2009;10:183–91.
30. Trubey R, Moore SC, Chestnutt IG. Parent's reasons for brushing or notbrushing their child's teeth: a qualitative study. Int J Paed Dent.2014;24:104–12.
31. Uribe S. Prevention and management of dental decay in the pre-schoolchild. Evidence-Based Dent. 2006;7:4–7.
32. Macpherson L, Anopa Y, Conway DI, McMahon AD. National supervisedtooth brushing programme and dental decay in Scotland. J Dent Res.2013;92:109–1113.
33. Freeman R, Stevens A. Nursing caries and buying time: an emerging theory ofprolonged bottle feeding. Community Dent Oral Epidemiol. 2008;63:425–33.
34. Miller W, Rollnick S. Motivational Interviewing: Preparing people for change.New York: The Guilford Press; 2002.
35. Blinkhorn A, Wainwright-Stringer YM, Holloway PJ. Dental health knowledgeand attitudes of regularly attending mothers of high-risk preschool children.Int Dent J. 2001;31:435–8.
36. Freudenthal J, Bowen DM. Motivational interviewing to decrease parentalrisk factors for early childhood caries. J Dent Hygiene. 2010;84:29–35.
37. Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N. Parental influenceand the development of dental caries in children aged 0–6 years: Asystematic review of the literature. J Dent. 2012;40:873–85.
38. Watt R. Motivational interviewing may be effective in dental settings.Evidence-Based Dent. 2010;11:13.
39. Wanyonyi K, Themessi-Huber M, Humphris G, Freeman R. A systematicreview and meta-analyses of face-to-face communication of tailored healthmessages: Implications for practice. Patient Ed and Counselling.2011;85:348–55.
40. Williams DM, Sheiham A, Watt RG. Oral health professionals and socialdeterminants. Br Dent J. 2013;214:427.
41. Britt E, Hudson SM, Blampied NM. Motivational interviewing in healthsettings: a review. Patient Ed and Counselling. 2004;53:147–55.
42. Weinstein P, Milgrom P, Reidy CA, Mancl LA, Garson G, Huebner CE, et al.Treatment fidelity of brief motivational interviewing and health education in arandomized clinical trial to promote attendance of low income mothers andchildren: Community –based integration oral health study “Baby Smiles”. BMCOral Health. 2014;14:15. http://www.biomedcentral.com/1472-6831/14/15.
43. Moyers TB, Matrtin T, Manuel JK, Miller WR, Ernst D. Revised Global Scales:Motivational Interviewing Treatment Integrity 3.1.1. University of NewMexico, Centre on Alcoholism, Substance Abuse and Addictions; HealthcareImprovemnet Scotland. Edinburgh: 2010.
44. Bowling A. Research methods in health. Buckingham: Open University Press;1999.
45. Sanzone L, Lee JY, Divaris K, Dewalt DA, Baker AD, Vann WF. A cross-sectional study examining social desirability bias in caregiver reporting ofchildren's oral health. BMC Oral Health. 2013;13:24. http://www.biomedcentral.com/content/pdf/1472-6831-13-24.pdf.
46. Guest G, Bunce A, Johnson L. How many interviews are enough? Anexperiment in data saturation and variability. Field Methods. 2006;18:59–82.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
Naidu et al. BMC Oral Health (2015) 15:101 Page 15 of 15