Embed Size (px)
Citation preview
THE EFFECT OF ISOBUTYL-CYANOACRYLATE MONOMER ADHESIVE ON CLOSURE OF NEPHROTOMY AND PARTIAL NEPHRECTOMY INCISIONS
By MILES Fox, M.D., Ch.M., F.R.C.S., L. HENRY, M.D., M.R.C.P., M.C.PATH., A . H . LOMAX, M.B. and R. W. M. REES, F.R.C.S.
Royal Hospital, Shefield
SUTURES inserted into the renal substance for approximation of incised surfaces and for hamo- stasis produce localised destruction and subsequent fibrosis of surrounding renal tissue by pressure necrosis (Jordan and Tomskey, 1957; Maddern, 1967). A tissue adhesive, if efficient, rapidly acting and non-irritant, could have considerable advantages over methods of suture. Methyl 2-cyanoacrylate (Eastman), a rapidly polymerising monomer is one of the agents tried and the results have approached to some extent those desired (Coover et a/., 1959). Adhesiveness is rapid and firm in the kidney and hamostasis is achieved, but there are disadvantages. Inflammatory changes with subsequent fibrosis and stone formation have been reported (Mather and Terry, 1963; Truss et a/., 1966). The material is not entirely inert in the tissues and produces chronic irritation particularly in the initial stages after application.
A derivative, isobutyl cyanoacrylate, developed more recently, has been found to be less histotoxic (Woodward et a/., 1965; Gottlob and Blumel, 1967). The present experiments were designed to investigate the immediate and delayed effects of isobutyl cyanoacrylate on the kidney with particular reference to hamostasis and healing over a prolonged period following nephrotomy and closure of partial nephrectomy incisions.
Material and Methods.-Twenty-eight adult albino rats and 10 mongrel dogs weighing between 9 and 15 kg. were used. The rats were anasthetised with ether, the dogs with intravenous butobarbitone. Kidneys were exposed transperitoneally through a midline upper abdominal incision and a vascular clamp was placed across the pedicle with the ureter included. A guillotine- type partial nephrectomy, removing the upper or lower quarter of one kidney, was then performed in both species on one side. I n the dog the capsule was initially incised and peeled back to the line of the incision. A calyx, if opened, was approximated with 4/0 plain catgut sutures. The renal substance was dried with gauze and a thin layer of isobutyl cyanoacrylate monomer was applied with a small gauze pledget. In the dog the loose capsule was placed over the divided surface; it did not cover it entirely in most cases. The surface was left bare in the rat. The pedicle clamp was removed 20 to 30 seconds after application of the monomer.
Nephrotomy was performed in the contralateral kidney also with the vascular clamp in place, by incising the kidney along the convex surface from pole to pole through the cortex and medulla. The pelvis was opened in most cases. After drying the surfaces, a thin layer of the mono- mer was applied to the cut renal substance, care being taken not to introduce it, or as little as possible, into the opened pelvis and calyces. The surfaces were then immediately approximated and mild digital pressure was maintained for 20 to 30 seconds, after which the vascular clamp was removed.
In four dog kidneys the nephrotomy incision was closed with sutures on one side while on the other the monomer was employed. Plain catgut (4/0) was used to underrun visible larger blood vessels and the renal substance was approximated with through-and-through 2/0 plain catgut sutures with as little tension as possible.
A small amount of monomer was also placed on the normal surface of each rat kidney and posterior abdominal wall to determine whether the substance had any irritant effect at those sites. The vault of the bladder was opened in 12 rats and closed after application of a thin layer of the monomer.
539
540 B R I T I S H J O U R N A L O F U R O L O G Y
Dogs were sacrificed at periods between 2 hours and 15 weeks after operation and rats at intervals over one year. Excretion urograms were performed in some dogs and retrograde pyelograms in rats (by injecting dye into the bladder). Kidneys were weighed after death and X-rays taken outside the body.
Specimens were fixed in 4 per cent. formaldehyde. Biocks were taken from the kidneys subjected to nephrotomy and partial nephrectomy and from areas where the material had been placed in the bladder and abdominal wall. The tissues were processed routinely and embedded in paraffin wax. Sections were cut at 5 p and stained with haematoxylin and eosin. Where appropriate, Masson’s stain for coIlagen, PAS and Gram stains were also used.
FIG. 1 Dog kidney after partial nephrectorny, and application of isobutyl cyanoacrylate monomer, immediately after removal of vascular
clamp.
Results.-Bleeding, either immediate or delayed, did not occur in any of the cases of nephro- tomy or partial nephrectomy apart from a little initial localised oozing of blood for which a second application of monomer was required in some of the dogs. Urinary leakage was not seen apart from the bladder opening in one rat. Renal ischEmia lasted for two to four minutes; the longest time was taken up with drying of the cut surfaces. The blood supply was restored immediately after the clamps were removed and normal colour returned to the kidney.
Partial Nephreetomy.-Figure 1 shows the appearance of a dog kidney following partial nephrectomy, after application of the monomer. The capsule has not yet been turned back over the bare surface. The cut surface of the kidney is covered by a shiny film of the monomer which appears within a few seconds and there is no bleeding. After two weeks, dense adhesions were usually found in both species of animal between the affected renal surface and surrounding structures, particularly the liver on the right side. No calcification in the renal substance was noted on X-ray examination over the period of observation.
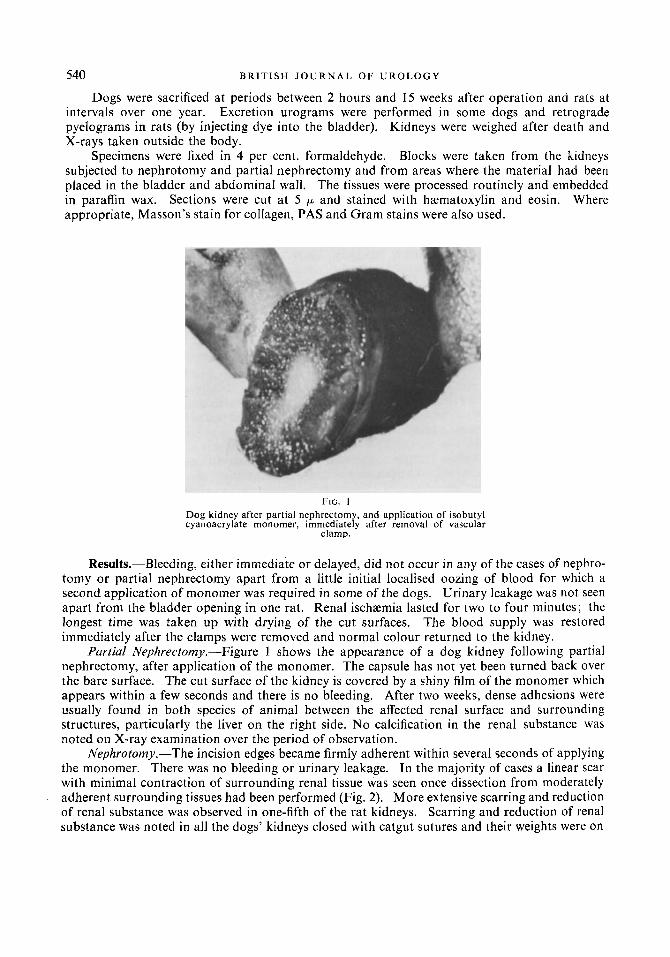
Nephrotomy.-The incision edges became firmly adherent within several seconds of applying the monomer. There was no bleeding or urinary leakage. In the majority of cases a linear scar with minimal contraction of surrounding renal tissue was seen once dissection from moderately adherent surrounding tissues had been performed (Fig. 2). More extensive scarring and reduction of renal substance was observed in one-fifth of the rat kidneys. Scarring and reduction of renal substance was noted in all the dogs’ kidneys closed with catgut sutures and their weights were on
E F F E C T O F I S O B U T Y L - C Y A N O A C R Y L A T E M O N O M E R A D H E S I V E 54 t
the average 10 per cent. less than the contralateral ones closed with the monomer. Calcification was seen on X-ray examination in 2 out of 28 rat kidneys, in no cases in the dogs. Pyelograms showed minimal distortion of the calyces.
Bladder and Abdominal Walllncisions (Rat).-Closure was firm in all cases within 20 seconds. Urine leakage occurred from the bladder in one out of 12 closures. No calcification was seen in the abdominal wounds but bladder stones, adherent to the area of application were seen on X-ray in one-third of the cases.
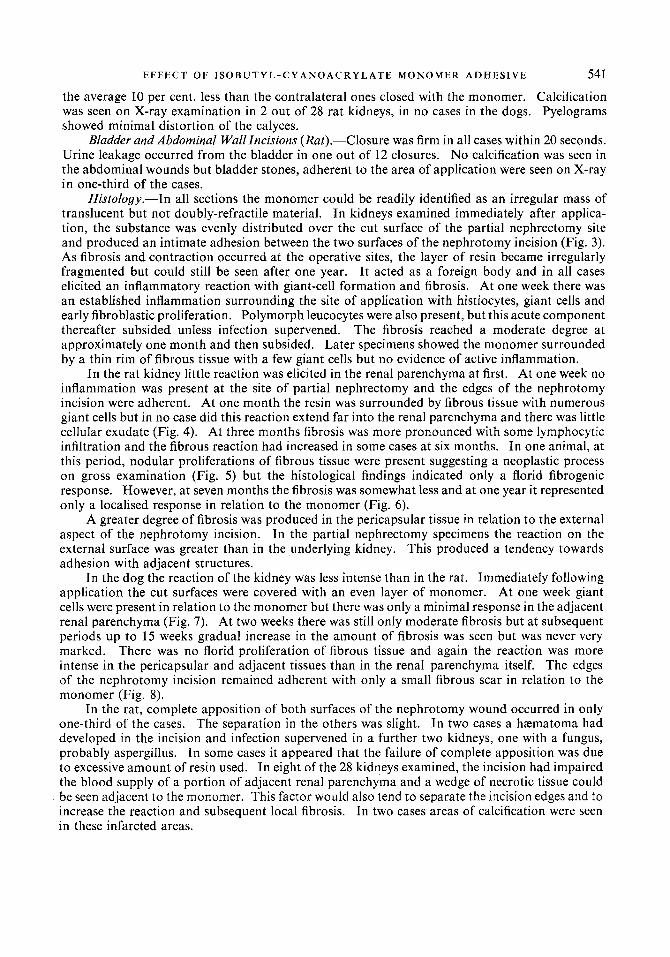
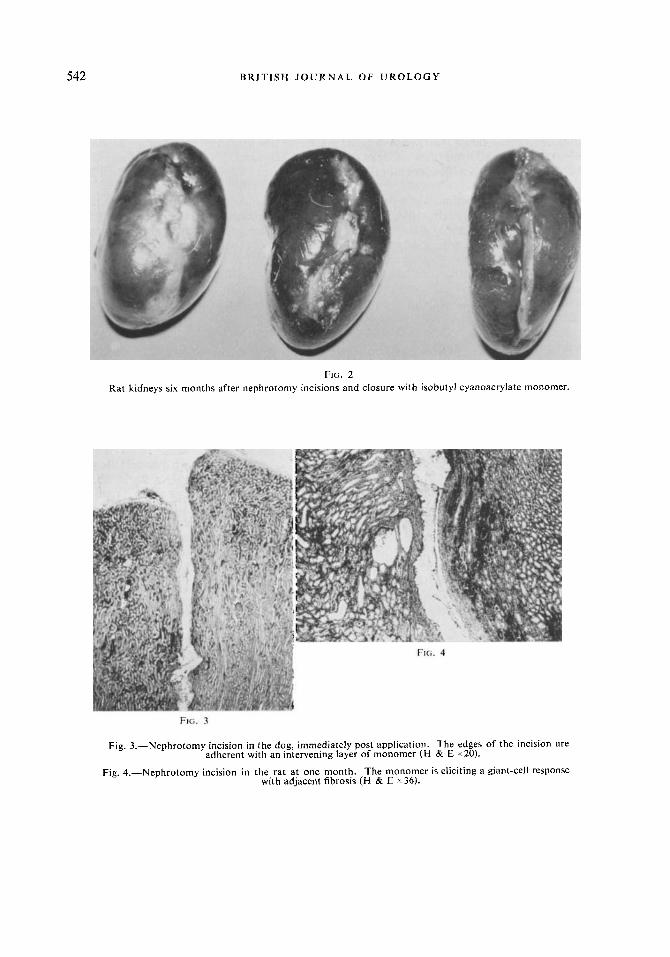
Histology.-In all sections the monomer could be readily identified as an irregular mass of translucent but not doubly-refractile material. In kidneys examined immediately after applica- tion, the substance was evenly distributed over the cut surface of the partial nephrectomy site and produced an intimate adhesion between the two surfaces of the nephrotomy incision (Fig. 3). As fibrosis and contraction occurred at the operative sites, the layer of resin became irregularly fragmented but could still be seen after one year. I t acted as a foreign body and in all cases elicited an inflammatory reaction with giant-cell formation and fibrosis. At one week there was an established inflammation surrounding the site of application with histiocytes, giant cells and early fibroblastic proliferation. Polymorph leucocytes were also present, but this acute component thereafter subsided unless infection supervened. The fibrosis reached a moderate degree at approximately one month and then subsided. Later specimens showed the monomer surrounded by a thin rim of fibrous tissue with a few giant cells but no evidence of active inflammation.
In the rat kidney little reaction was elicited in the renal parenchyma at first. At one week no inflammation was present at the site of partial nephrectomy and the edges of the nephrotomy incision were adherent. At one month the resin was surrounded by fibrous tissue with numerous giant cells but in no case did this reaction extend far into the renal parenchyma and there was little cellular exudate (Fig. 4). At three months fibrosis was more pronounced with some lymphocytic infiltration and the fibrous reaction had increased in some cases at six months. In one animal, at this period, nodular proliferations of fibrous tissue were present suggesting a neoplastic process on gross examination (Fig. 5) but the histological findings indicated only a florid fibrogenic response. However, at seven months the fibrosis was somewhat less and at one year it represented only a localised response in relation to the monomer (Fig. 6) .
A greater degree of fibrosis was produced in the pericapsular tissue in relation to the external aspect of the nephrotomy incision. In the partial nephrectomy specimens the reaction on the external surface was greater than in the underlying kidney. This produced a tendency towards adhesion with adjacent structures.
In the dog the reaction of the kidney was less intense than in the rat. Immediately following application the cut surfaces were covered with an even layer of monomer. At one week giant cells were present in relation to the monomer but there was only a minimal response in the adjacent renal parenchyma (Fig. 7). At two weeks there was still only moderate fibrosis but at subsequent periods up to 15 weeks gradual increase in the amount of fibrosis was seen but was never very marked. There was no florid proliferation of fibrous tissue and again the reaction was more intense in the pericapsular and adjacent tissues than in the renal parenchyma itself. The edges of the nephrotomy incision remained adherent with only a small fibrous scar in relation to the monomer (Fig. 8).
In the rat, complete apposition of both surfaces of the nephrotomy wound occurred in only one-third of the cases. The separation in the others was slight. In two cases a hrematoma had developed in the incision and infection supervened in a further two kidneys, one with a fungus, probably aspergillus. In some cases it appeared that the failure of complete apposition was due to excessive amount of resin used. In eight of the 28 kidneys examined, the incision had impaired the blood supply of a portion of adjacent renal parenchyma and a wedge of necrotic tissue could be seen adjacent to the monomer. This factor would also tend to separate the incision edges and to increase the reaction and subsequent local fibrosis. In two cases areas of calcification were seen in these infarcted areas.
542 B R I T I S H J O U R N A L O F U R O L O G Y
FIG. 2 Rat kidneys six months after nephrotomy incisions and closure with isobutyl cyanoacrylate monomer.
FIG. 3
Fig. 3.-Nephrotomy incision in the dog, immediately post application. The edges of the incision are
Fig. 4.-Nephrotomy incision in the rat at one month. The monomer is eliciting a giant-cell response
adherent with an intervening layer of monomer (H & E x 20).
with adjacent fibrosis (H & E x 36).
E F F E C T O F I S O B U T Y L - C Y A N O A C R Y L A T E MONOMER A D H E S I V E 543
FIG. 5 FIG. 6
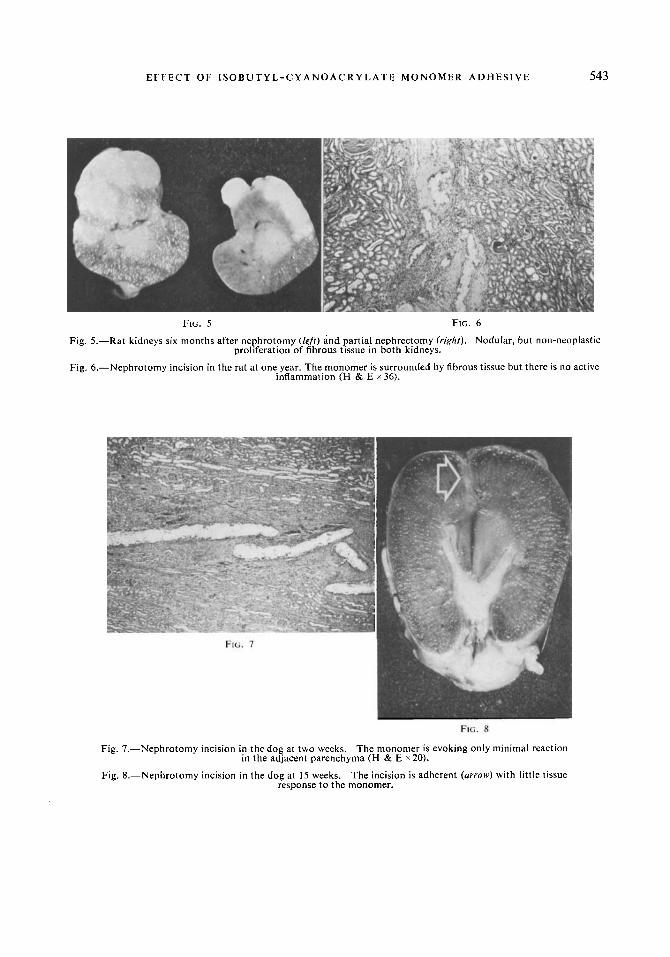
Fig. 5.-Rat kidneys six months after nephrotomy (lefr) and partial nephrectomy (right). Nodular, but non-neoplastic proliferation of fibrous tissue in both kidneys.
Fig. 6.-Nephrotomy incision in the rat at one year. The monomer is surrounded by fibrous tissue but there is no active inflammation (H & E x 36).
FIG. 8
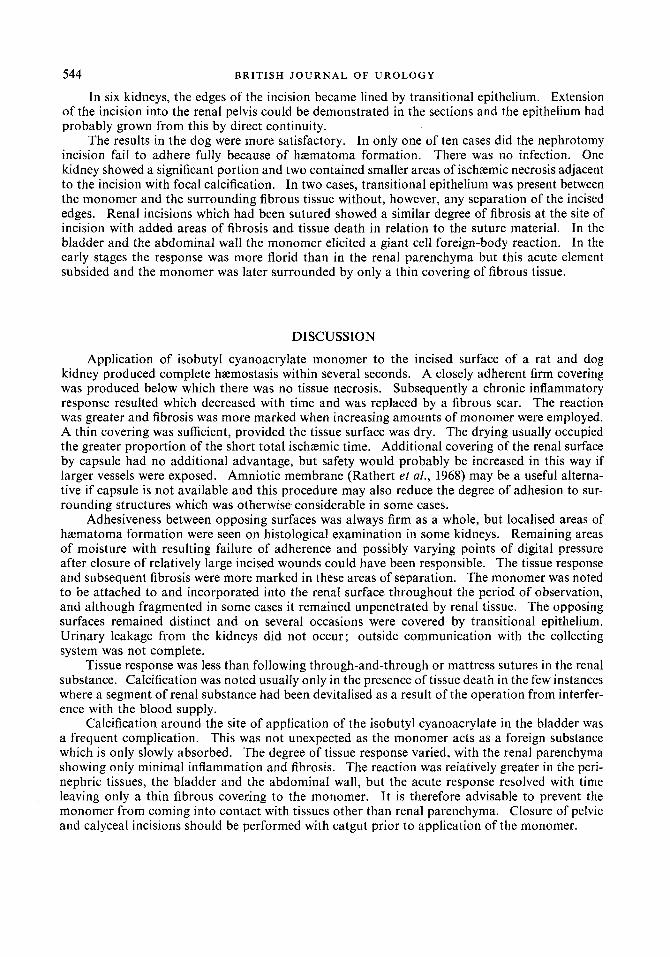
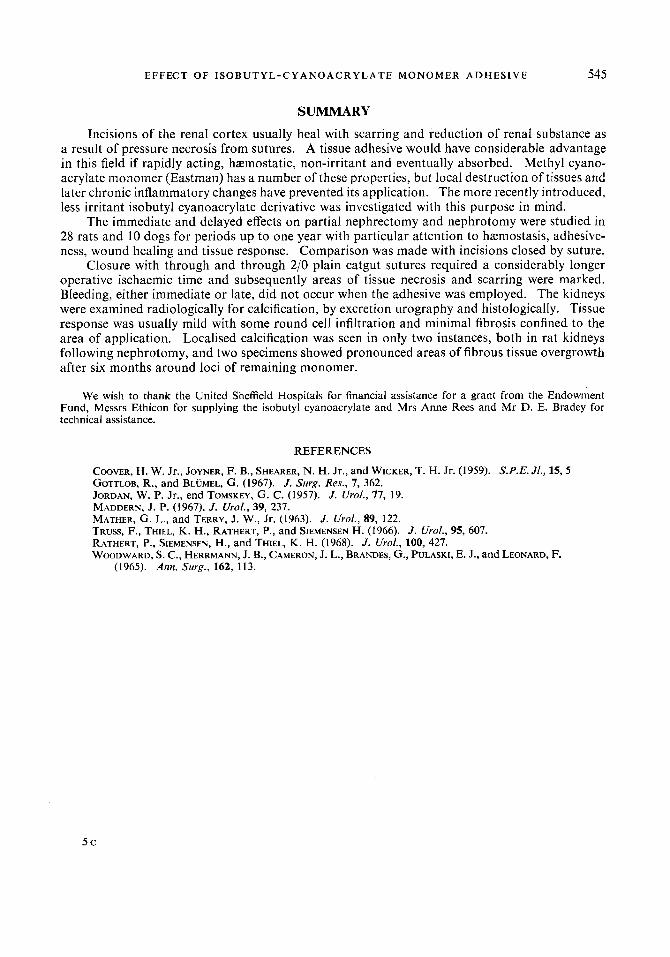
Fig. 7.-Nephrotomy incision in the dog at two weeks.
Fig. 8.-Nephrotomy incision in the dog at 15 weeks.
The monomer is evoking only minimal reaction
The incision is adherent (arrow) with little tissue
in the adjacent parenchyma (H & E x20).
response to the monomer.
544 B R I T I S H J O U R N A L O F U R O L O G Y
In six kidneys, the edges of the incision became lined by transitional epithelium. Extension of the incision into the renal pelvis could be demonstrated in the sections and the epithelium had probably grown from this by direct continuity.
The results in the dog were more satisfactory. In only one of ten cases did the nephrotomy incision fail to adhere fully because of hamatoma formation. There was no infection. One kidney showed a significant portion and two contained smaller areas of ischamic necrosis adjacent to the incision with focal calcification. In two cases, transitional epithelium was present between the monomer and the surrounding fibrous tissue without, however, any separation of the incised edges. Renal incisions which had been sutured showed a similar degree of fibrosis at the site of incision with added areas of fibrosis and tissue death in relation to the suture material. In the bladder and the abdominal wall the monomer elicited a giant cell foreign-body reaction. In the early stages the response was more florid than in the renal parenchyma but this acute element subsided and the monomer was later surrounded by only a thin covering of fibrous tissue.
DISCUSSION
Application of isobutyl cyanoacrylate monomer to the incised surface of a rat and dog kidney produced complete hamostasis within several seconds. A closely adherent firm covering was produced below which there was no tissue necrosis. Subsequently a chronic inflammatory response resulted which decreased with time and was replaced by a fibrous scar. The reaction was greater and fibrosis was more marked when increasing amounts of monomer were employed. A thin covering was sufficient, provided the tissue surface was dry. The drying usually occupied the greater proportion of the short total ischzmic time. Additional covering of the renal surface by capsule had no additional advantage, but safety would probably be increased in this way if larger vessels were exposed. Amniotic membrane (Rathert et al., 1968) may be a useful alterna- tive if capsule is not available and this procedure may also reduce the degree of adhesion to sur- rounding structures which was otherwise considerable in some cases.
Adhesiveness between opposing surfaces was always firm as a whole, but localised areas of hamatoma formation were seen on histological examination in some kidneys. Remaining areas of moisture with resulting failure of adherence and possibly varying points of digital pressure after closure of relatively large incised wounds could have been responsible. The tissue response and subsequent fibrosis were more marked in these areas of separation. The monomer was noted to be attached to and incorporated into the renal surface throughout the period of observation, and although fragmented in some cases it remained unpenetrated by renal tissue. The opposing surfaces remained distinct and on several occasions were covered by transitional epithelium. Urinary leakage from the kidneys did not occur; outside communication with the collecting system was not complete.
Tissue response was less than following through-and-through or mattress sutures in the renal substance. Calcification was noted usually only in the presence of tissue death in the few instances where a segment of renal substance had been devitalised as a result of the operation from interfer- ence with the blood supply.
Calcification around the site of application of the isobutyl cyanoacrylate in the bladder was a frequent complication. This was not unexpected as the monomer acts as a foreign substance which is only slowly absorbed. The degree of tissue response varied, with the renal parenchyma showing only minimal inflammation and fibrosis. The reaction was reIativeIy greater in the peri- nephric tissues, the bladder and the abdominal wall, but the acute response resolved with time leaving only a thin fibrous covering to the monomer. It is therefore advisable to prevent the monomer from coming into contact with tissues other than renal parenchyma. Closure of pelvic and calyceal incisions should be performed with catgut prior to application of the monomer.
E F F EC T 0 F I S 0 B U T Y L - C Y A N O A C R Y L A T E M 0 N 0 M E R ADHESIVE 545
SUMMARY
Incisions of the renal cortex usually heal with scarring and reduction of renal substance as a result of pressure necrosis from sutures. A tissue adhesive would have considerable advantage in this field if rapidly acting, haemostatic, non-irritant and eventually absorbed. Methyl cyano- acrylate monomer (Eastman) has a number of these properties, but local destruction of tissues and later chronic inflammatory changes have prevented its application. The more recently introduced, less irritant isobutyl cyanoacrylate derivative was investigated with this purpose in mind.
The immediate and delayed effects on partial nephrectomy and nephrotomy were studied in 28 rats and 10 dogs for periods up to one year with particular attention to hremostasis, adhesive- ness, wound healing and tissue response. Comparison was made with incisions closed by suture.
Closure with through and through 2/0 plain catgut sutures required a considerably longer operative ischaemic time and subsequently areas of tissue necrosis and scarring were marked. Bleeding, either immediate or late, did not occur when the adhesive was employed. The kidneys were examined radiologically for calcification, by excretion urography and histologically. Tissue response was usually mild with some round cell infiltration and minimal fibrosis confined to the area of application. Localised calcification was seen in only two instances, both in rat kidneys following nephrotomy, and two specimens showed pronounced areas of fibrous tissue overgrowth after six months around loci of remaining monomer.
We wish to thank the United Sheffield Hospitals for financial assistance for a grant from the Endowment Fund, Messrs Ethicon for supplying the isobutyl cyanoacrylate and Mrs Anne Rees and Mr D. E. Bradey for technical assistance.
REFERENCES
COOVER, H. W. Jr., JOYNER, F. B., SHEARER, N. H. Jr., and WICKER, T. H. Jr. (1959). S.P.E. Jl., 15,5 GOTTLOB, R., and BLUMEL, G. (1967). J. Suvg. Res., 7, 362. JORDAN, W. P. Jr., end TOMSKEY, G. C. (1957). J. Urol., 77, 19. MADDERN, J. P. (1967). J. Urof., 39, 237. MATHER, G. L., and TERRY, J. W., Jr. (1963). J. Urol., 89, 122. TRUSS, F., THIEL, K. H., RATHERT, P., and SIEMENSEN H. (1966). J. Urol., 95, 607. RATHERT, P., SIEMENSEN, H., and THIEL, K. H. (1968). J. Uvol., 100, 427. WOODWARD, S. C., HERRMANN, J. B., CAMERON, J. L., BRANDES, G., PULASKI, E. J., and LEONARD, F.
(1965). Ann. Suvg., 162, 113.
5 c





























