Embed Size (px)
Citation preview
The economic Burden of PaTienT SafeTy in acuTe care 1
The Economics of Patient Safety in Acute Care
Technical RepoRT
Safe care... accepting no less
invesTigaToRs: Dr. Edward Etchells (Team Lead), Dr. Nicole Mittmann (Co-Lead), Ms. Marika Koo, Dr. Michael Baker, Dr. Murray Krahn, Dr. Kaveh Shojania, Dr. Andrew McDonald, Ms. Rupinder Taggar, Dr. Anne Matlow, Dr. Nick Daneman

ISBN: 978-1-926541-48-8
Acknowledgements:
The authors acknowledge Ms. Peggy Kee, Ms. Evelyn Worthington, Dr. William Geerts, Dr. Damon Scales and Dr. Andrew Simor for their assistance with this project.
The economic Burden of PaTienT SafeTy in acuTe care i
TAblE of ConTEnTSExEcutivE SummAry ............................................................................................................................ 1
METhoDS ..................................................................................................................................................1
RESuLTS .....................................................................................................................................................2
CoNCLuSIoNS ..........................................................................................................................................3
introduction ........................................................................................................................................ 4
ECoNoMIC BuRDEN STuDIES .............................................................................................................4
CoMPARATIvE ECoNoMIC ANALySIS (CoST EffECTIvENESS ANALySIS) ................................5
objEctivES ............................................................................................................................................... 7
mEthodS ................................................................................................................................................... 8
IDENTIfICATIoN of PS TARGETS ........................................................................................................8
SySTEMATIC REvIEW of PuBLIShED LITERATuRE ........................................................................9
ASSESSMENT of STuDy QuALITy......................................................................................................11
rESultS .................................................................................................................................................... 12
SCoPE of PuBLIShED RESEARCh ......................................................................................................12
ECoNoMIC BuRDEN STuDIES ..........................................................................................................13
Adverse events, including adverse drug events (eight studies) ............................................................13
Nosocomial Infections .......................................................................................................................14
Nosocomial venous Thromboembolism ............................................................................................17
Nosocomial falls ...............................................................................................................................18
CoST EffECTIvENESS ANALySES ......................................................................................................18
Adverse Drug Events .........................................................................................................................18
Transfusion-related Adverse Events in Critically Ill Patients ...............................................................18
vascular Catheter Associated Bloodstream Infection ..........................................................................19
Retained Surgical foreign Body .........................................................................................................19
ECoNoMIC BuRDEN of PATIENT SAfETy IN ACuTE CARE IN CANADA ...............................21
overall Cost ......................................................................................................................................21
Clostridium Difficile-Associated Disease (CDAD) ............................................................................22
Methicillin-Resistant Staphylococcus Aureus (MRSA) Infection ........................................................22
vancomycin-Resistant Enterococci (vRE) Infection ..........................................................................22
Surgical Site Infections (SSI) .............................................................................................................22
CANADIAN PAtIeNt SAfety INStItUteii
GuidElinES And FrAmEwork For Economic EvAluAtionS in PAtiEnt SAFEty ........ 24
diScuSSion ............................................................................................................................................. 25
limitAtionS ........................................................................................................................................... 28
SummAry ................................................................................................................................................. 29
concluSionS ......................................................................................................................................... 30
rEFErEncES ............................................................................................................................................ 31
APPEndicES ............................................................................................................................................. 43
The economic Burden of PaTienT SafeTy in acuTe care 1
ExECuTivE SummAryPatient safety has received considerable public, professional, political, and scientific attention over the past 12 years. Adverse events are injuries caused by healthcare, rather than the patient’s underlying condition, leading to disability (prolonged length of stay, morbidity at the time of discharge, or death) (1). Although the human burden associated with adverse events is well established, the economic burden has received less attention. A fuller understanding of the economic burden of unsafe care may inform Canadian health policy, health services research priorities, patient safety research programs, and patient safety improvement priorities for healthcare organizations.
our objectives were to:
1. Summarize the scope and quality of published studies on the economic burden of adverse events in the acute care setting.
2. Summarize the scope and quality of published comparative economic evaluations (cost effectiveness analyses) of patient safety improvement strategies in the acute care setting.
3. Estimate the economic burden of adverse events on the Canadian acute care system.
4. Provide a framework and guidelines for performing economic burden studies and comparative economic evaluations (cost effectiveness analyses) in patient safety.
MeThodsWe searched the published literature from the year 2000 to 2011, linking eight patient safety targets and six patient safety improvement strategies with the following search terms for costs: “costs and cost analysis,” “cost-effectiveness,” “cost,” and “financial management, hospital.”
We searched eight patient safety targets:
1. Adverse events (including adverse drug events)
2. Nosocomial colonization and infections
3. Nosocomial pressure ulcers
4. Wrong-site surgery
5. Retained surgical foreign body
6. Contrast nephropathy
7. Nosocomial venous thromboembolism
8. fall-related injuries.
We also searched six patient safety improvement strategies
1. hand hygiene
2. Rapid response teams
3. Bundles
4. Checklists
5. Automatic stop orders
6. Bar-coded medication administration.

CANADIAN PAtIeNt SAfety INStItUte2
Potentially relevant abstracts were obtained and reviewed in duplicate using standard economic evaluation methods. for cost effectiveness evaluations, we expected evidence of effectiveness based on the rules of evidence described by the Cochrane Effective Practice and organisation of Care Group.
We estimated the economic burden of adverse events for the Canadian acute care hospital system based on the results of our systematic review, the results of the Canadian Adverse Events Study (1)
and data from the Canadian Institute for health Information (2).
ResulTs We identified 158 potentially eligible studies of economic burden, of which only 61 (39 per cent) reported any costing methodology. We found wide estimates of economic burden from these 61 studies, due to variations in case definitions, patient populations, costing methodology, and study setting. The majority of studies reported the economic burden of adverse events and nosocomial infections. We found that the reported attributable costs of adverse events ranged from uS$2,162 (CAN$4,028) to AuS$11,846 (CAN$12,648). In general hospital populations, the cost per case of hospital-acquired infection ranged from uS$2,027 (CAN$2,265) to uS$12,197 (CAN$22,400). Nosocomial bloodstream infection was associated with costs ranging from €1,814 (CAN$3,268) to €16,706 (CAN$29,950).
We found five cost effectiveness analyses that reported a total of seven comparisons based on at least one study with adequate evidence of effectiveness. Based on these limited studies, pharmacist-led medication reconciliation, the Keystone Michigan ICu Intervention for central line associated blood stream infections, chlorhexidine for vascular catheter site care, and standard surgical sponge counts were economically attractive patient safety improvement strategies.
We calculated a preliminary estimate of the economic burden of adverse events in Canada in 2009–2010 was $1,071,983,610 ($1.1 billion), including $396,633,936 ($397 million) for preventable adverse events. This estimate does not include the direct costs of care after hospital discharge, or societal costs of illness, such as loss of functional status or occupational productivity.
We developed a guideline for future economic evaluations in patient safety (see page 24 and Appendix 2).
The economic Burden of PaTienT SafeTy in acuTe care 3
conclusions1. The majority of published studies on the economic burden of patient safety in acute care
describes no costing methodology.
2. for studies that report a costing methodology, there is variability in methods for measuring and attributing costs.
3. Most studies report on the economic burden of adverse events and nosocomial infections.
4. The reported attributable costs of adverse events ranged from uS$2,162 (CAN$4,028) to AuS$11,846 (CAN$12,648).
5. The cost per case of hospital-acquired infection ranged from uS$2,027 (CAN$2,265) to uS$12,197 (CAN$22,400). Nosocomial bloodstream infection was associated with costs ranging from €1,814 (CAN$3,268) to €16,706 (CAN$29,950).
6. We found only five comparative economic analyses of patient safety improvement strategies in the acute care setting based on adequate evidence of effectiveness based on guidelines from the Cochrane Effective Practice and organisation of Care Group.
7. Based on these limited analyses, the following patient safety improvement strategies are economically attractive:
• Pharmacist-led medication reconciliation to prevent potential adverse drug events was the dominant strategy (improved safety and lower cost) when compared to no reconciliation.
• The Keystone ICu Patient Safety Program to prevent central line associated bloodstream infections was the dominant strategy compared to usual care. The Keystone ICu Patient Safety Program included two key components: (a) a Comprehensive unit-Based Safety Program, which included interventions to improve safety culture, teamwork, and communication; a daily goals sheet; and other communication tools; and (b) specific interventions to improve compliance with evidence-based care to reduce CLABSI.
• Chlorhexidine for catheter site care to prevent catheter-related bloodstream infections was the dominant strategy when compared to povidone-iodine.
• Standard counting was associated with a cost of uS$1,500 (CAN$1,676) for each surgical foreign body detected, when compared to a strategy of no counting.
8. We estimate that the economic burden of preventable adverse events in the Canadian acute care system was approximately $397 million in 2009-2010.
9. Safety improvement programs should consider the EPoC standards when planning their program evaluations.
10. Cost effectiveness analyses should explicitly consider the impact of patient safety on economically important parameters such as staff retention, staff absenteeism, and patient (market) retention.
11. Cost effectiveness analyses should explicitly consider the societal value of improving safety over improving care of primary clinical conditions.
12. Studies of the health-related quality of life associated with patient safety targets are needed.
13. Guidelines for performing or assessing economic research in patient safety could be based on the Drummond Checklist (3) (Appendix 2).
CANADIAN PAtIeNt SAfety INStItUte4
inTroduCTionPatient safety (PS) has received considerable public, professional, political, and scientific attention over the past 12 years. Adverse events are injuries caused by healthcare, rather than the patient’s underlying condition, leading to disability such as prolonged length of acute care stay, morbidity at the time of discharge or death (1).
Although the human burden associated with adverse events is well established, the economic costs have received less attention. Despite the substantial effort that has been expended to develop and implement safety improvements, there is uncertainty about both the economic impact of unsafe care and the improvement strategies that offer the best value.
A fuller understanding of the economic burden of unsafe care may inform Canadian health policy, health services research priorities, PS research programs and PS improvement priorities for healthcare organizations.
Economic evaluations should be based on rigorous analytical methods, be impartial and credible in the use of data, and be transparent for and accessible by the reader (4).
The purpose of an economic evaluation is to “identify, measure, value and compare the costs and consequences of alternatives being considered” to inform “value for money” judgments about an intervention or program (5). In Canada, national guidance on the conduct of resource costing and economic evaluations has been available through the Canadian Agency for Drugs and Technologies in health (CADTh) since 1994 (4;6;7).
There are two common types of economic evaluations in healthcare: the economic burden study and the comparative economic analysis.
econoMic BuRden sTudiesThe objective of an economic burden study is to describe the economic impact of a PS target. We highlight three important methodologic considerations in economic burden studies: economic perspective, time horizon and attribution of healthcare resources to the care of the PS target, rather than the care of the patient’s underlying condition.
The choice of economic perspective will determine the type of resources and costs measured and attributed to the PS target. for example, a study with an acute care hospital perspective will focus on the direct medical costs of providing hospital care. In this perspective, costs of care after hospital discharge or societal costs of illness, such as loss of functional status or occupational productivity, are not measured.
The choice of time horizon will influence the amount and types of resources measured. The optimal time horizon for many PS target conditions is not known, but a significant proportion of the cost of severe PS events is accrued after acute care hospital discharge (8).
The attribution of healthcare resources to the management of a PS target, rather than the patient’s underlying condition, is particularly important. Patients with more comorbidity, and longer hospital
The economic Burden of PaTienT SafeTy in acuTe care 5
stays, are more likely to consume healthcare resources for the management of their underlying condition, and these resources are therefore not attributable to PS. however, these individuals are also more likely to experience an adverse event.
There are several methodologic approaches to the attribution of healthcare resources. In the case review method, a clinical expert explicitly attributes resources to the care of the PS target or the underlying condition. for example, a specialist could review the chart of a patient admitted with congestive heart failure who develops a nosocomial infection on day four. The expert would determine which resources, and which hospital days, were directed primarily for the treatment of the infection, rather than the congestive heart failure. This method was used in the Canadian Adverse Events Study (1). Major limitations of this study design are its resource-intensive effort, and the potential unreliability of retrospective judgments.
A second burden of illness approach compares groups of patients with (cases) and without (controls) the PS target. In this approach, the resource use for patients who develop post-operative infections is compared to the resource use for similar patients who do not develop infections. A limitation of this study design is that there may be resource and cost differences between cases and controls that are unrelated to the PS target (confounders). Several analytic techniques are used to reduce the effect of these confounders. Matched case-control studies can reduce the confounding effect of a small number of known variables, but matching is usually performed on a limited number of variables. Propensity score methods can accommodate many more potential confounding variables than case-control methods. Traditional multivariable statistics can also be used to estimate the impact of known confounders on differences between cases and controls (9). Differential timing of the occurrence of adverse events can lead to wide estimates of attributable costs (10-12).
coMpaRaTive econoMic analysis (cosT effecTiveness
analysis)The second type of economic evaluation is the comparative economic analysis. Comparative economic analyses in PS should compare the costs and outcomes of one or more safety improvement strategies aimed at a PS target. The goal is to identify interventions that provide the best value for money. Many people are familiar with the term cost effectiveness analysis, which is a common type of comparative economic analysis. for ease of reading of this report, we will use the term cost effectiveness analysis throughout. Cost effectiveness analyses are conducted using widely accepted frameworks, which can be modified for specific target conditions (3;13-15).
An ideal improvement strategy will be associated with lower costs and greater safety; such an intervention is considered economically dominant. In some cases, a strategy can be associated with greater costs and less safety; such strategies are considered economically dominated and should not be adopted. other improvement strategies can be associated with increased cost and greater safety. In these situations, the additional dollars spent for the gain in PS can be calculated. The relative value must be weighed against other available interventions, which could be implemented within our resource-constrained healthcare systems.

CANADIAN PAtIeNt SAfety INStItUte6
There are several key considerations in cost effectiveness analyses. first, evidence of effectiveness is a prerequisite for any meaningful cost effectiveness analysis. The rules of evidence for evaluation of PS improvements has been debated for many years (16;17). We used the rules of evidence described by the Cochrane Effective Practice and organisation of Care (EPoC) Group: randomized control studies, controlled clinical trials, controlled before-and-after studies and interrupted time series (18).
Second, the choice of comparator will have a major influence on the results of a cost effectiveness analysis. Any intervention will look good if compared with an unattractive alternative. The standard of care is often an appropriate comparator.
Third, several potential analytic approaches can be used. In a cost effectiveness analysis, an incremental cost effectiveness ratio is the additional cost divided by the number of life years gained. Life year gained is an appropriate choice when death is the outcome of interest, but may not be appropriate for other outcomes, such as adverse events. In a cost utility analysis, an incremental cost-utility ratio uses estimates the incremental cost to improve health-related quality of life, or quality adjusted life year (QALy). These cost-utility ratios can be compared across many disease states. unfortunately, health related quality of life estimates used to create cost utility ratios are unknown for many PS targets. In a cost consequence analysis, a cost consequence ratio estimates the incremental cost per event avoided. Cost consequence ratios are easier to calculate, but can make comparisons between different studies or conditions difficult.
finally, as in the economic burden of illness studies, the choice of perspective, the choice of time horizon and the attribution of healthcare resources to the management of a PS target, rather than the patient’s underlying condition, are also important.
We did not include budget impact analyses in our review. Budget impact analyses predict how an intervention will impact spending on a target condition (19). Budget impact analyses do not explicitly incorporate evidence of effectiveness, and often do not specify economic perspectives or time horizons.
The economic Burden of PaTienT SafeTy in acuTe care 7
objECTivESour objectives were to:
1. Summarize the scope and quality of published studies on the economic burden of adverse events in the acute care setting.
2. Summarize the scope and quality of published comparative economic evaluations (cost effectiveness analyses) of PS improvement strategies in the acute care setting.
3. Estimate the economic burden of adverse events on the Canadian acute care system.
4. Provide a framework and guidelines for performing economic burden studies and comparative economic evaluations (cost effectiveness analyses) in PS.
CANADIAN PAtIeNt SAfety INStItUte8
mEThodS
idenTificaTion of ps TaRgeTsour first step was to develop a list of PS targets in the acute care hospital setting. We used an iterative process with co-investigators (n=9), informed by prior systematic reviews (20), Canadian provincial government PS priorities, Canadian Patient Safety Institute (CPSI) improvement priorities and the American healthcare research and Quality (AhRQ) Patient Safety Net website
We selected our targets based on three characteristics:
• A clinical outcome (e.g., hospital-acquired methicillin-resistant Staphylococcus aureus [MRSA] infection) or a surrogate with an established link to a clinical outcome (e.g. MRSA colonization).
• high specificity as a measure of PS, as opposed to being a naturally occurring condition.• A sufficiently long history of measuring this outcome in the literature, such that some studies on
the economic burden or cost effectiveness can be expected.
We presented our initial list of PS targets to over 200 delegates at the 2010 halifax pre-conference plenary session on the economics of PS, and five members of our pre-conference advisory group: Dr. Sven Grisvold (past editor of Acta Anaesthesiologica Scandinavica); Dr. Kathleen Sutcliffe (Gilbert and Ruth Whitaker Professor of Business Administration and Professor of Management and organizations, university of Michigan); and Mr. Steven Lewis, Mr. Blair Sadler, and Mr. Joseph Gebran (CPSI).
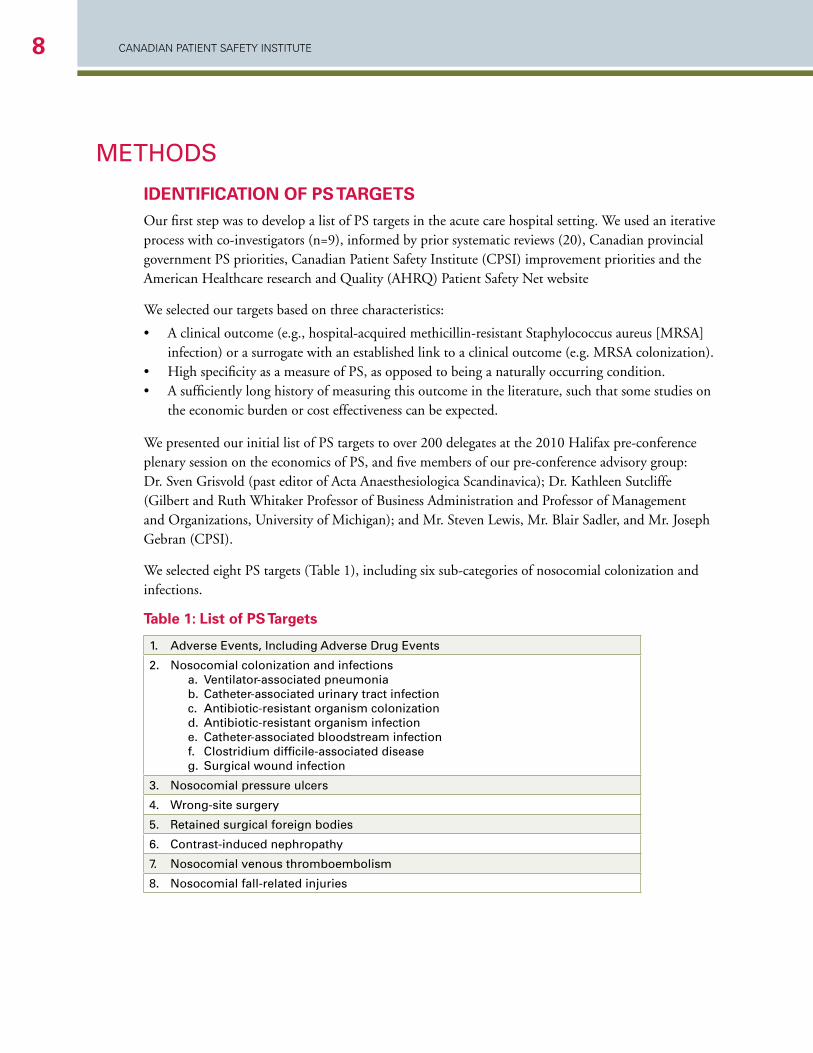
We selected eight PS targets (Table 1), including six sub-categories of nosocomial colonization and infections.
Table 1: list of ps Targets
1. Adverse Events, including Adverse drug Events
2. nosocomial colonization and infections a. ventilator-associated pneumonia b. Catheter-associated urinary tract infection c. Antibiotic-resistant organism colonization d. Antibiotic-resistant organism infection e. Catheter-associated bloodstream infection f. Clostridium difficile-associated disease g. Surgical wound infection
3. nosocomial pressure ulcers
4. Wrong-site surgery
5. retained surgical foreign bodies
6. Contrast-induced nephropathy
7. nosocomial venous thromboembolism
8. nosocomial fall-related injuries
The economic Burden of PaTienT SafeTy in acuTe care 9
sysTeMaTic Review of puBlished liTeRaTuReWe then conducted a systematic review of published literature. our goal was to identify, review, and summarize the scope and quality of evidence of published economic evaluations in the area of PS.
We searched the MEDLINE database for articles published between 2000 and 2010 (using the following search terms for costs: “costs and cost analysis,” “cost-effectiveness,” “cost,” and “financial management, hospital.”
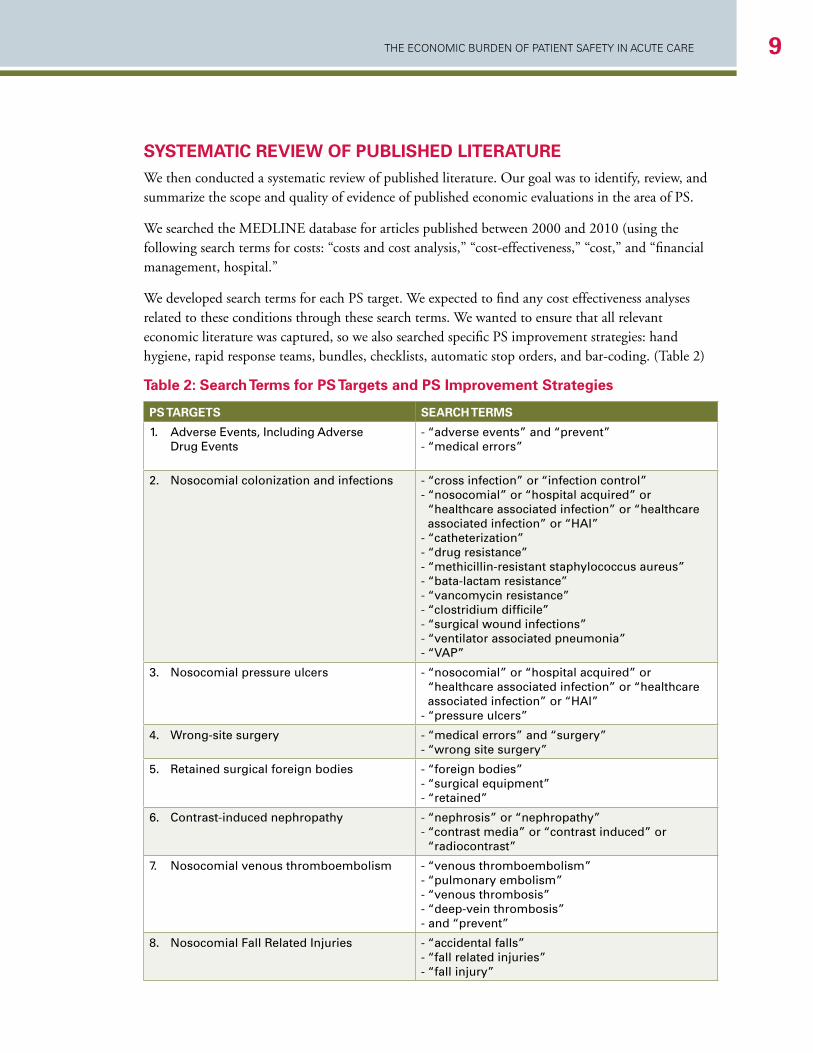
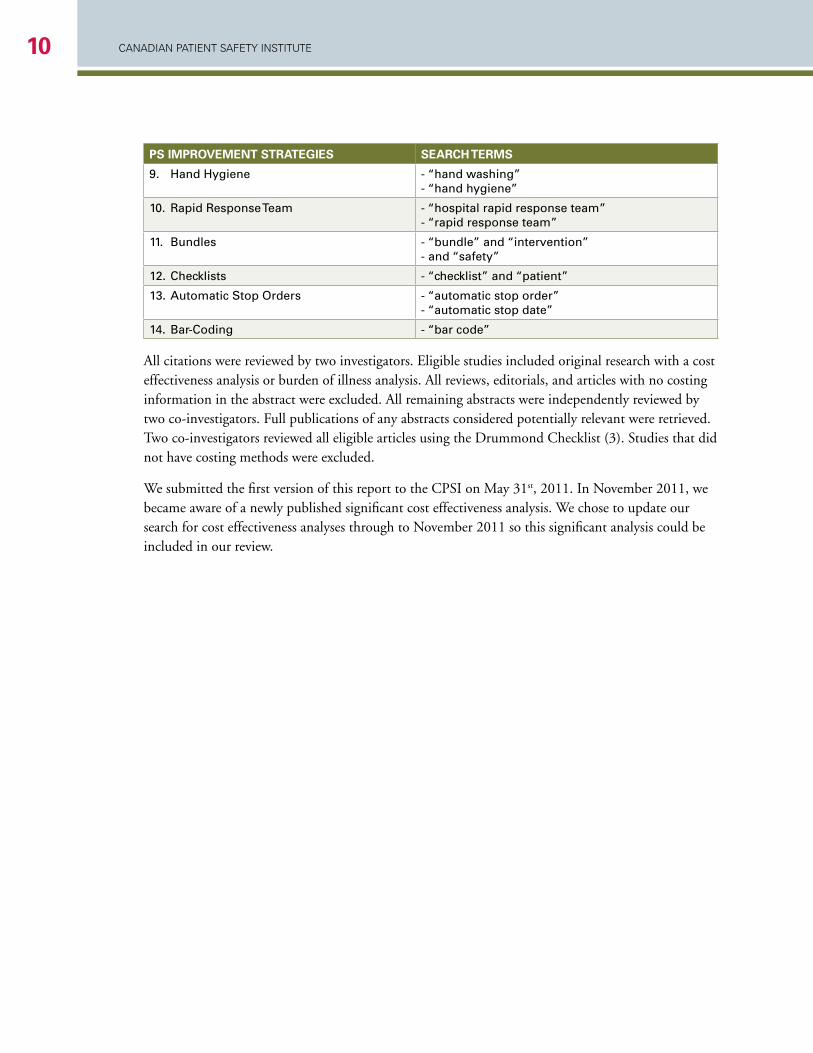
We developed search terms for each PS target. We expected to find any cost effectiveness analyses related to these conditions through these search terms. We wanted to ensure that all relevant economic literature was captured, so we also searched specific PS improvement strategies: hand hygiene, rapid response teams, bundles, checklists, automatic stop orders, and bar-coding. (Table 2)
Table 2: search Terms for ps Targets and ps improvement strategies
ps TaRgeTs seaRch TeRMs
1. Adverse Events, including Adverse drug Events
- “adverse events” and “prevent”- “medical errors”
2. nosocomial colonization and infections - “cross infection” or “infection control”- “nosocomial” or “hospital acquired” or
“healthcare associated infection” or “healthcare associated infection” or “hAi”
- “catheterization”- “drug resistance”- “methicillin-resistant staphylococcus aureus”- “bata-lactam resistance”- “vancomycin resistance”- “clostridium difficile”- “surgical wound infections”- “ventilator associated pneumonia”- “vAP”
3. nosocomial pressure ulcers - “nosocomial” or “hospital acquired” or “healthcare associated infection” or “healthcare associated infection” or “hAi”
- “pressure ulcers”
4. Wrong-site surgery - “medical errors” and “surgery”- “wrong site surgery”
5. retained surgical foreign bodies - “foreign bodies”- “surgical equipment”- “retained”
6. Contrast-induced nephropathy - “nephrosis” or “nephropathy”- “contrast media” or “contrast induced” or
“radiocontrast”
7. nosocomial venous thromboembolism - “venous thromboembolism”- “pulmonary embolism”- “venous thrombosis”- “deep-vein thrombosis”- and “prevent”
8. nosocomial fall related injuries - “accidental falls”- “fall related injuries”- “fall injury”
CANADIAN PAtIeNt SAfety INStItUte10
ps iMpRoveMenT sTRaTegies seaRch TeRMs
9. hand hygiene - “hand washing”- “hand hygiene”
10. rapid response Team - “hospital rapid response team”- “rapid response team”
11. bundles - “bundle” and “intervention”- and “safety”
12. Checklists - “checklist” and “patient”
13. Automatic Stop orders - “automatic stop order”- “automatic stop date”
14. bar-Coding - “bar code”
All citations were reviewed by two investigators. Eligible studies included original research with a cost effectiveness analysis or burden of illness analysis. All reviews, editorials, and articles with no costing information in the abstract were excluded. All remaining abstracts were independently reviewed by two co-investigators. full publications of any abstracts considered potentially relevant were retrieved. Two co-investigators reviewed all eligible articles using the Drummond Checklist (3). Studies that did not have costing methods were excluded.
We submitted the first version of this report to the CPSI on May 31st, 2011. In November 2011, we became aware of a newly published significant cost effectiveness analysis. We chose to update our search for cost effectiveness analyses through to November 2011 so this significant analysis could be included in our review.
The economic Burden of PaTienT SafeTy in acuTe care 11
assessMenT of sTudy QualiTy(Appendix 1)
Economic studies are conducted using recognized frameworks that can be modified for specific target conditions (13;14). Drummond and Jefferson constructed a checklist to evaluate the quality of economic studies in healthcare that is used worldwide (3;15) (see Appendix 1). We used the entire Drummond Checklist (3) to evaluate the quality of cost effectiveness analyses. The Drummond Checklist rates 35 parameters as present (yes), absent (no), not clear, and not applicable. for the burden of illness studies, the Drummond Checklist was modified to 22 items, excluding those items required only for cost effectiveness analyses. We arbitrarily assigned one point for each item present, then calculated a total score. Scores are presented as means and medians for the number of yes parameters.
Cost effectiveness analyses require evidence of effectiveness of the PS improvement strategy that is being evaluated. We used the rules of evidence described by the Cochrane Effective Practice and organisation of Care (EPoC) Group: randomized control studies, controlled clinical trials, controlled before-and-after studies, and interrupted time series analyses (18). uncontrolled before-after studies do not provide sufficient evidence of effectiveness of a PS improvement strategy.
Two independent reviewers evaluated each manuscript. If the scores were within five points, then the higher of the two scores was taken. We discussed and resolved discrepancies between reviews of five or more points. We had no difficulty resolving these discrepancies and achieving consensus. We made some standard assumptions to facilitate our reviews. for example, most studies took a short-term acute care hospital perspective, so discounting was not relevant.
our third objective was to estimate the economic burden of adverse events on the Canadian acute care system. We used data obtained from our systematic review wherever possible. We also sought additional data from the Canadian Adverse Events Study (1) and data from the Canadian Institute for health Information (2) on Canadian estimates on the incidence of PS targets, including estimates of preventability, Canadian estimates of the population at risk for each PS target, and Canadian estimates of the attributable length of stay, or attributable costs for each PS target.
CANADIAN PAtIeNt SAfety INStItUte12
rESulTS
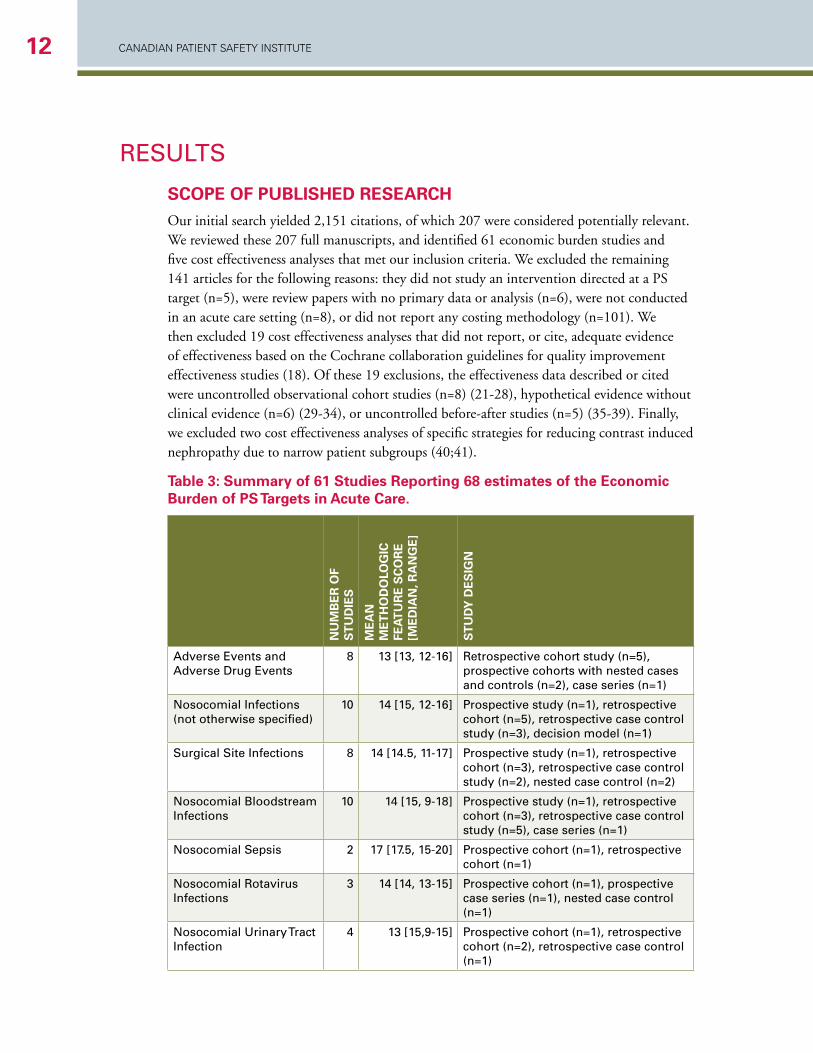
scope of puBlished ReseaRchour initial search yielded 2,151 citations, of which 207 were considered potentially relevant. We reviewed these 207 full manuscripts, and identified 61 economic burden studies and five cost effectiveness analyses that met our inclusion criteria. We excluded the remaining 141 articles for the following reasons: they did not study an intervention directed at a PS target (n=5), were review papers with no primary data or analysis (n=6), were not conducted in an acute care setting (n=8), or did not report any costing methodology (n=101). We then excluded 19 cost effectiveness analyses that did not report, or cite, adequate evidence of effectiveness based on the Cochrane collaboration guidelines for quality improvement effectiveness studies (18). of these 19 exclusions, the effectiveness data described or cited were uncontrolled observational cohort studies (n=8) (21-28), hypothetical evidence without clinical evidence (n=6) (29-34), or uncontrolled before-after studies (n=5) (35-39). finally, we excluded two cost effectiveness analyses of specific strategies for reducing contrast induced nephropathy due to narrow patient subgroups (40;41).
Table 3: summary of 61 studies Reporting 68 estimates of the economic Burden of ps Targets in acute care.
nu
MB
eR
of
sT
ud
ies
Me
an
M
eT
ho
do
log
ic
fea
Tu
Re
sc
oR
e
[Me
dia
n, R
an
ge
]
sT
ud
y d
es
ign
Adverse Events and Adverse drug Events
8 13 [13, 12-16] retrospective cohort study (n=5), prospective cohorts with nested cases and controls (n=2), case series (n=1)
nosocomial infections (not otherwise specified)
10 14 [15, 12-16] Prospective study (n=1), retrospective cohort (n=5), retrospective case control study (n=3), decision model (n=1)
Surgical Site infections 8 14 [14.5, 11-17] Prospective study (n=1), retrospective cohort (n=3), retrospective case control study (n=2), nested case control (n=2)
nosocomial bloodstream infections
10 14 [15, 9-18] Prospective study (n=1), retrospective cohort (n=3), retrospective case control study (n=5), case series (n=1)
nosocomial Sepsis 2 17 [17.5, 15-20] Prospective cohort (n=1), retrospective cohort (n=1)
nosocomial rotavirus infections
3 14 [14, 13-15] Prospective cohort (n=1), prospective case series (n=1), nested case control (n=1)
nosocomial urinary Tract infection
4 13 [15,9-15] Prospective cohort (n=1), retrospective cohort (n=2), retrospective case control (n=1)
The economic Burden of PaTienT SafeTy in acuTe care 13
nu
MB
eR
of
sT
ud
ies
Me
an
M
eT
ho
do
log
ic
fea
Tu
Re
sc
oR
e
[Me
dia
n, R
an
ge
]
sT
ud
y d
es
ign
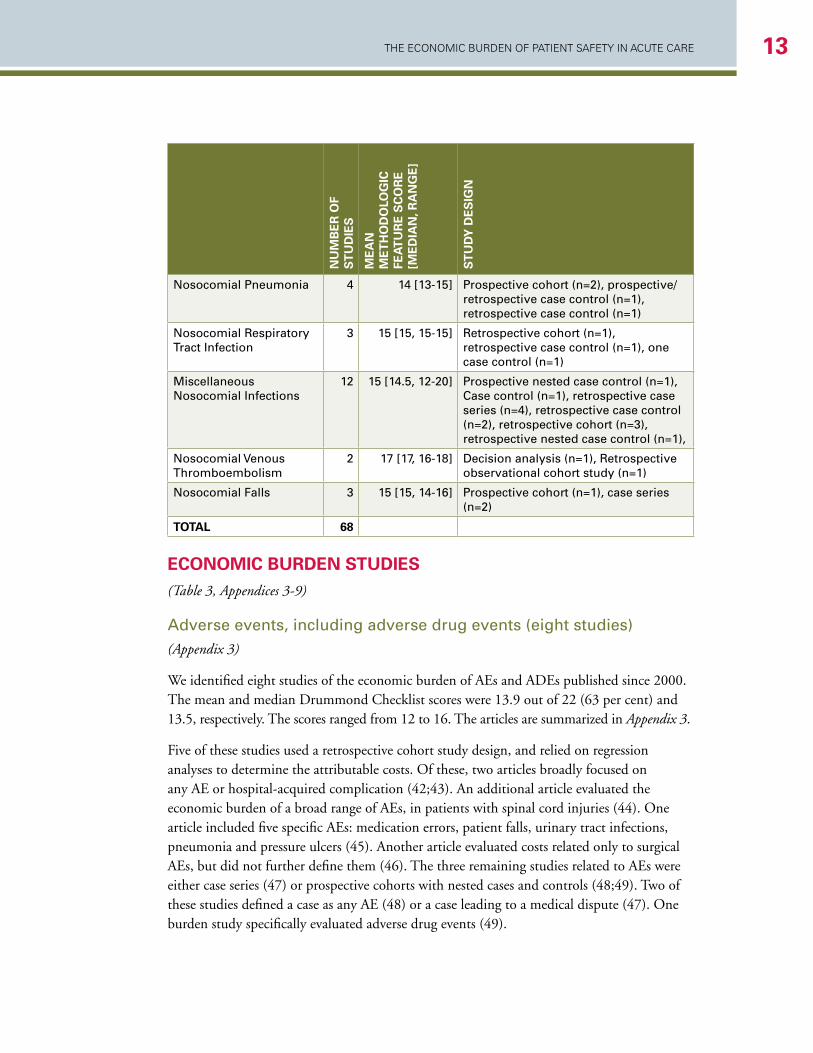
nosocomial Pneumonia 4 14 [13-15] Prospective cohort (n=2), prospective/retrospective case control (n=1), retrospective case control (n=1)
nosocomial respiratory Tract infection
3 15 [15, 15-15] retrospective cohort (n=1), retrospective case control (n=1), one case control (n=1)
miscellaneous nosocomial infections
12 15 [14.5, 12-20] Prospective nested case control (n=1), Case control (n=1), retrospective case series (n=4), retrospective case control (n=2), retrospective cohort (n=3), retrospective nested case control (n=1),
nosocomial venous Thromboembolism
2 17 [17, 16-18] decision analysis (n=1), retrospective observational cohort study (n=1)
nosocomial falls 3 15 [15, 14-16] Prospective cohort (n=1), case series (n=2)
ToTal 68
econoMic BuRden sTudies (Table 3, Appendices 3-9)
Adverse events, including adverse drug events (eight studies) (Appendix 3)
We identified eight studies of the economic burden of AEs and ADEs published since 2000. The mean and median Drummond Checklist scores were 13.9 out of 22 (63 per cent) and 13.5, respectively. The scores ranged from 12 to 16. The articles are summarized in Appendix 3.
five of these studies used a retrospective cohort study design, and relied on regression analyses to determine the attributable costs. of these, two articles broadly focused on any AE or hospital-acquired complication (42;43). An additional article evaluated the economic burden of a broad range of AEs, in patients with spinal cord injuries (44). one article included five specific AEs: medication errors, patient falls, urinary tract infections, pneumonia and pressure ulcers (45). Another article evaluated costs related only to surgical AEs, but did not further define them (46). The three remaining studies related to AEs were either case series (47) or prospective cohorts with nested cases and controls (48;49). Two of these studies defined a case as any AE (48) or a case leading to a medical dispute (47). one burden study specifically evaluated adverse drug events (49).

CANADIAN PAtIeNt SAfety INStItUte14
Costs1 attributable to AEs were reported to be uS$3,857 (CAN$6,124) (48) and AuS$11,846 (CAN$12,648) (43) per case in two studies. In patients with spinal cord injury, the cost attributable to general AEs was AuS$7,359 (CAN$7,857), but was significantly higher for specific complications; for example, procedural complications in these patients were associated with additional costs of AuS$21,821(CAN$23,299) (44). The cost attributable to adverse drug events specifically was reported to be uS$2,162 (CAN$4,028) per ADE (49). In another study, medication errors in medical and surgical cases were associated with costs of uS$334 (CAN$402) and uS$525 (CAN$632), respectively (45). Additional length of stay related to AEs of any type ranged from 0.77 days to 32 days. Three of the eight articles did not collect length-of-stay data.
In summary, studies of adverse events used variable methods, different definitions of adverse events, and different methods for attributing costs. Attributable costs of adverse events ranged from uS$2,162 (CAN$4,028) to AuS$11,846 (CAN$12,648); medication errors had an attributable cost of uS$334 (CAN$402) to AuS$525 (CAN$632).
nosocomial infections(Appendix 5)
• General Nosocomial Infections (10 studies)
We identified 10 studies of the economic burden of general nosocomial infections, not otherwise specified by type of infection. These included one prospective design, five retrospective cohort designs, three retrospective case-control designs, and one study used a decision model. Analytic methods included regression analysis, including linear regression, multivariate regression, and ordinary least-squares regression analysis. The mean Drummond Checklist score for these articles was 13.5 out of 22 (61 per cent). The median score was 14. The scores ranged from 11 to 16 out of a total of 22.
In general hospital populations, the cost per case of hospital-acquired infection ranged from uS$2,027 (CAN$2,265) to uS$12,197 (CAN$22,400) (52-58). hospital-acquired infections cost uS$2,767 (CAN$3,091) in gastrectomy patients (58) and €11,750 (CAN$27,796) (59) in neonates. The estimated costs of hospital-acquired infections over one fiscal year in New Zealand in medical and surgical patients were uS$4,569,826 (CAN$8,392,705) and uS$3,900,922 (CAN$7,164,231), respectively (60).
• Surgical Site Infections (eight studies)
We found eight studies of the economic burden of surgical site infections. Study designs included prospective cohort (N=1), retrospective cohort (N=3), retrospective case-control (N=2), and two nested case-control designs. The mean Drummond Checklist scores for these articles were 14 out of 22 (64 per cent). The median score was 14. The scores ranged from 12 to 17 out of a total of 22.
1 All costs are reported in their original currency. for comparison purposes, they have also been converted to 2010 Canadian dollars based on the Bank of Canada currency converter and inflation calculator (50;51). Each cost was first converted to Canadian dollars of the same year indicated in the study; the converted cost was then inflated to 2010. Due to conversion and inflation rates fluctuating yearly, the proportion of the original cost compared to the 2010 Canadian cost is not the same. The 2010 Canadian costs were used for comparison purposes only and do not reflect how much Canada spent in each safety target.
The economic Burden of PaTienT SafeTy in acuTe care 15
Three studies reported the average cost per case of surgical site infection in a general patient population to be uS$1,051 (CAN$1,174) (52), €1,814 (CAN$3,268) (61), and 19,638 Swiss francs (CAN$21,392) (62). In orthopaedic patients, the median attributable cost of surgical site infection was uS$17,708 (CAN$31,527) (63). Surgical site infection in patients after colorectal procedures, head-and-neck cancer-related surgery, coronary artery bypass graft procedures, and low transverse Caesarean delivery were associated with costs of uS$13,746 (CAN$16,560) (64), €16,000 (CAN$26,273) (65), AuS$12,419 (CAN$14,934) (66), and uS$2,852 (CAN$3,107) to uS$3,529 (CAN$3,845) (67) per case, respectively.
• Nosocomial Bloodstream Infections (11 studies)
We found 10 studies of the economic burden of nosocomial bloodstream infections. These included one prospective, three retrospective cohort, five retrospective case-control, and one case series. The mean Drummond Checklist score for these articles was 13.5 out of 22 (61 per cent). The median score was 14.5. The scores ranged from 10 to 16 out of a total of 22.
In general European patient populations, nosocomial bloodstream infection was associated with costs ranging from €1,814 (CAN$3,268) to €16,706 (CAN$29,950) (52;61;68-71). one American study reported average incremental costs of uS$19,427 (CAN$23,404) (72). In a pediatric ICu, nosocomial bloodstream infection was estimated to cost uS$39,219 (CAN$71,500) (73). very low-birth-weight infants with nosocomial bloodstream infection incurred average total costs uS$54,539 (CAN$101,621) higher than those without the infection (74). S. aureus bacteraemia in patients with prosthetic implants was associated with uS$67,439 (CAN$123,469) in costs per nosocomial case, in one prospective case series (75).
• Nosocomial Sepsis (two studies)
In one retrospective cohort study, nosocomial sepsis was associated with mean additional costs of uS$27,510 (CAN$50,523) (76) per case. In one prospective cohort, ICu-acquired sepsis was associated with a mean increase of €39,908 (CAN$65,644) in total costs per case (77). The mean and median Drummond Checklist scores for these articles were 16.5 out of 22 (75 per cent). The scores ranged from 13 to 20 out of a total of 22.
• Nosocomial Rotavirus Infection (three studies)
one prospective cohort study estimated the costs associated with nosocomial rotavirus infection in children under 30 months of age, but did not provide a per-case result; this study estimated that the national cost of all cases in one year in Italy is €8,019,155 (CAN$12,787,889) (78). Rotavirus in children under 48 months of age was associated with €2,442 (CAN$5,144) in costs per case in one prospective case series (79). one prospective study with a nested case control reported €1,930 (CAN$3,337) in mean excess costs per case (80). The mean Drummond Checklist score for these articles was 13.3 out of 22 (60 per cent). The median score was 14. The scores ranged from 12 to 14 out of a total of 22.
CANADIAN PAtIeNt SAfety INStItUte16
• Nosocomial Urinary Tract Infection (four studies)
We found four studies of the economic burden of nosocomial urinary tract infections. These included one prospective, two retrospective cohort, and one retrospective case-control study. The average costs attributable to urinary tract infection ranged from uS$589 (CAN$1,114) to uS$14,300 (CAN$26,645) (52;61;81;82). The mean Drummond Checklist score for these articles was 12.5 out of 22 (57 per cent). The median score was 13. The scores ranged from 9 to 15 out of a total of 22.
• Nosocomial Pneumonia (four studies)
Nosocomial pneumonia was associated with average additional costs of 2,255 Argentinian pesos ($1,309 CAN) (83) and €17,000 ($27,915 CAN) (65) in two studies. one German article detailed both a prospective case control and a retrospective case control, reporting average excess costs of DM 14,606 ($14,840 CAN) and DM 29,610 ($30,085 CAN), respectively (84). In one study, the average cost attributable to ventilator-associated pneumonia in a pediatric ICu was uS$51,157 ($61,630 CAN) (85). The mean Drummond Checklist score for these articles was 14 out of 22 (64 per cent). The median score was 13.5. The scores ranged from 13 to 16 out of a total of 22.
• Nosocomial Respiratory Tract Infection (three studies)
Three studies reported on the economic burden of nosocomial respiratory tract infections. These included one retrospective cohort, one retrospective case-control, and one case-control study. The mean Drummond Checklist score for these articles was 15 out of 22 (68 per cent). The median score was 15. All three scores were 15 out of a total of 22.
Single-site respiratory tract infections were associated with additional mean costs of €2,421 (CAN$4,362) (61) and uS$4,287 (CAN$4,789) (52) in two studies, respectively. In one additional study, a case was defined as an infection of nosocomial respiratory syncytial virus; this infection was associated with a mean uS$9,414 (CAN$16,788) per case (86).
• Nosocomial Antibiotic-Resistant Organisms (four studies)
In one Irish hospital, postoperative methicillin-resistant Staphylococcus aureus (MRSA) infection incurred additional costs of ₤6,485 (CAN$14,484) (87). one case-control study reported the attributable costs of vancomycin-resistant Enterococcus infection in the medical ICu and in hospital to be uS$7,873 (CAN$14,414) and uS$11,989 (CAN$21,950), respectively (88). In one drug-resistant S. typhimurium outbreak in a Turkish neonatal ICu, cases incurred charges uS$1,082 (CAN$1,427) higher than controls (89). A pertussis outbreak incurred total hospital costs of uS$30,282 (CAN$43,917) and uS$43,893 (CAN$63,657) in two hospitals (90). one retrospective case-control study defined a case as a multidrug-resistant infection of Acenitobacter bowmanii in burn patients, and reported a mean additional cost per case of uS$98,575 (CAN$181,038) (91).
• Nosocomial Clostridium Difficile-Associated Disease (one study)
one prospective study with a nested case control reported a median incremental cost of €7,147 (CAN$10,809) per case of Clostridium difficile–associated disease (CDAD) (92).

The economic Burden of PaTienT SafeTy in acuTe care 17
• Other Nosocomial Infections (10 studies)
The mean Drummond Checklist score for these articles was 12.7 out of 22 (58 per cent). The median score was 13. The scores ranged from 10 to 18 out of a total of 22. During a P. aeruginosa outbreak, it was retrospectively estimated that infected patients who had been on mechanical ventilation incurred excess costs of €18,408 (CAN$28,109) (93). Another retrospective case series investigated the economic impact of a norovirus outbreak that affected patients and staff, and did not provide a per-case cost estimate; dividing the total outbreak costs by the given number of case infections yields a crude estimate of €890 (CAN$1,359) per case (94). Another similar study yielded an estimate of uS$2,452 (CAN$4,489) per case of outbreak-related norovirus (95). The attributable costs during a Salmonella outbreak in one Australian tertiary care complex were reported in total costs rather than per case, and dividing by the number of cases yields an estimate of AuS$2,308 (CAN$3,222) per case (96).
• Summary
In summary, studies of the economic burden of nosocomial infection are heterogeneous in methodological characteristics, country setting, case definitions, and patient populations. A summary estimate was not possible. Nevertheless, most studies describe significant costs attributable to hospital-acquired infections. for example, in general hospital populations, the cost per case of hospital-acquired infection ranged from uS$2,027 (CAN$2,265) to uS$12,197 (CAN$22,400) (52-54;54-57).
nosocomial venous Thromboembolism(Appendix 8)
We identified two burden studies published since 2000. The mean and median Drummond Checklist scores were 17 and 17, respectively (77 per cent). The scores ranged from 16 to 18.
one study focused on nosocomial deep-vein thrombosis (DvT) after hip replacement surgery (97). The cost of DvT was modelled in patients undergoing total hip replacement surgery, with Markov decision analysis. The article reported the annual per-patient cost of DvT to be uS$3,798 (CAN$6,975), with discounted lifetime costs uS$3,069 (CAN$5,696). Costs of DvT-related complications were uS$3,817 (CAN$7,010) for post-thrombotic syndrome with ulcer, and uS$6,604 (CAN$12,219) for pulmonary embolism. A retrospective u.S. study of DvT (n=15,679), PE (n=7,653), and post-thrombotic syndrome (n=624) found annual attributable direct medical costs of $16,832 (CAN$24,411) for DvT, $18,221 (CAN$26,426) for PE, $24,874 (CAN$36,074) for combined DvT and PE, and $4,726 (CAN$6,854) for post thrombotic syndrome. This study did not explicitly distinguish cases of nosocomial DvT, but 78 per cent of the study cohort had abdominal or orthopaedic surgery prior to the index vTE event (98).
CANADIAN PAtIeNt SAfety INStItUte18
nosocomial falls(Table 3 and Appendix 9)
We reviewed three burden of illness studies related to nosocomial falls. The mean Drummond Checklist score was 12.7 out of 22 (58 per cent). The median score was 13. The scores ranged from 12 to 13 out of a total of 22. These articles are summarized in detail in Appendix 9.
Two of three burden studies were case series (99;100). The third study had a prospective cohort design (101). one study (101) identified cases only in patients over 60 years of age. one study focused on legal compensation rather than hospital-related costs (100), and neither of the other two articles (99;101) clearly stated what methods were used for determining attributable costs. There was one additional case-control study that reported attributable length of stay, but not costs (102).
oliver found that 60.5 per cent of legal claims related to in-hospital falls resulted in payment of costs or damages, with mean payment of ₤12,945 (CAN$28,721) (100). Nurmi provided the cost per treatment of an in-hospital fall, estimated at €944 (CAN$1,876) (101). The third study did not describe costs per case or per fall, but did provide the total estimated attributable cost of all cases included in the study; dividing by the provided number of cases yields a crude estimate of ₤1,667 (CAN$4,321) per case (99).
cosT effecTiveness analyses (Table 4, Appendix 4)
We identified five cost effectiveness analyses that were based on at least one study of effectiveness with adequate methods. These five analyses reported a total of seven cost effectiveness comparisons.
Adverse drug Eventsone comparative analysis studied the impact of various strategies for reducing potential adverse drug events (103). The methodological feature score was 27/35. Pharmacist-led medication reconciliation was the only strategy with adequate effectiveness data, based on one randomized trial and several non-randomized controlled trials (104-108). Pharmacist-led medication reconciliation dominated over a strategy of no reconciliation (103). The main limitation of this analysis was the assumption that a reduction in potential adverse drug events leads to a reduction in preventable adverse drug events.
Transfusion-related Adverse Events in Critically ill Patientsone analysis compared the strategy of erythropoietin to reduce transfusion related adverse events to standard care in critically ill patients (109). The methodologic feature score was 28/35. Effectiveness data was derived from a randomized clinical trial, where outcomes were measured as units of recombinant human erythropoietin needed to reduce allogeneic blood transfusions (110). The strategy of giving erythropoietin had an incremental cost of uS$4,700,000 (CAN$6,816,309) to avoid one transfusion-related adverse event (109).

The economic Burden of PaTienT SafeTy in acuTe care 19
vascular Catheter Associated bloodstream infectionone analysis compared chlorhexidine gluconate and povidone-iodine for catheter site care, with an outcome of catheter-related bloodstream infections in a Thailand hospital (111). The methodologic feature score was 25/35. The effectiveness data came from a meta-analysis based on several randomized controlled trials (112). Chlorhexidine gluconate was a dominant strategy over povidone-iodine in both central-line catheter and peripheral-line catheter sites, showing a cost savings of 304.49 baht (CAN$9.98) per central line catheters and 13.56 baht (CAN$0.45) per peripheral catheter, with fewer infections (111). A similar analysis published three years earlier yielded a similar result; chlorhexidine was a dominant strategy, showing a cost savings of uS$113 (CAN$209) per catheter used, and fewer infections (113).
one analysis compared the Keystone ICu Patient Safety Program in six hospitals to usual care. The Keystone ICu Patient Safety Program included 2 key components: (a) a Comprehensive unit-Based Safety Program, which included interventions to improve safety culture, teamwork, and communication; a daily goals sheet; and other communication tools; and (b) specific interventions to improve compliance with evidence-based care to reduce central line associated blood stream infections. The methodologic feature score was 20/35. The effectiveness data came from an interrupted time series study (114). The main finding was that the Keystone ICu patient safety program had low development and implementation costs. The intervention cost about $5,404 per case of central line associated blood stream infection averted, and the cost of a central line associated blood stream infection is $12,208 to $56,167. Therefore the intervention can be considered economically dominant (115).
retained Surgical foreign bodyone cost effectiveness analysis was related to retained surgical foreign bodies (116). This analysis compared eight strategies: no sponge tracking, standard counting, universal radiography without counting, universal radiography with standard counting, selective mandatory radiography for high-risk operations, bar-coded sponges, and radiofrequency-tagged sponges. The methodologic feature score was 24/35. The effectiveness data came from a randomized control study and diagnostic test studies (117-119). Detection of surgical foreign bodies can be considered a diagnostic test; some of the evidence for effectiveness came from studies that evaluated the sensitivity and specificity of standard surgical counting compared to other detection methods, such as routine postoperative radiography. Standard counting was predicted to prevent 82 per cent of retained surgical sponges with an incremental cost of uS$1,500 (CAN$1,676) for each surgical foreign body detected, compared to a strategy of no counting. Bar-coded sponges would prevent 95 per cent of retained surgical sponges, with an incremental cost of uS$95,000 (CAN$106,132) for each surgical foreign body detected, compared to a strategy of standard counting. Selective mandatory radiography for high-risk operations, universal radiography without counting, and universal radiography with standard counting were less effective and more expensive than bar-coded sponges. The downstream costs of retained surgical foreign bodies were not included in this study, as these costs have not been described. If these downstream costs were included, then standard counting would probably be the dominant strategy compared to no counting, and bar-coded sponges would be more economically attractive (116).
CANADIAN PAtIeNt SAfety INStItUte20
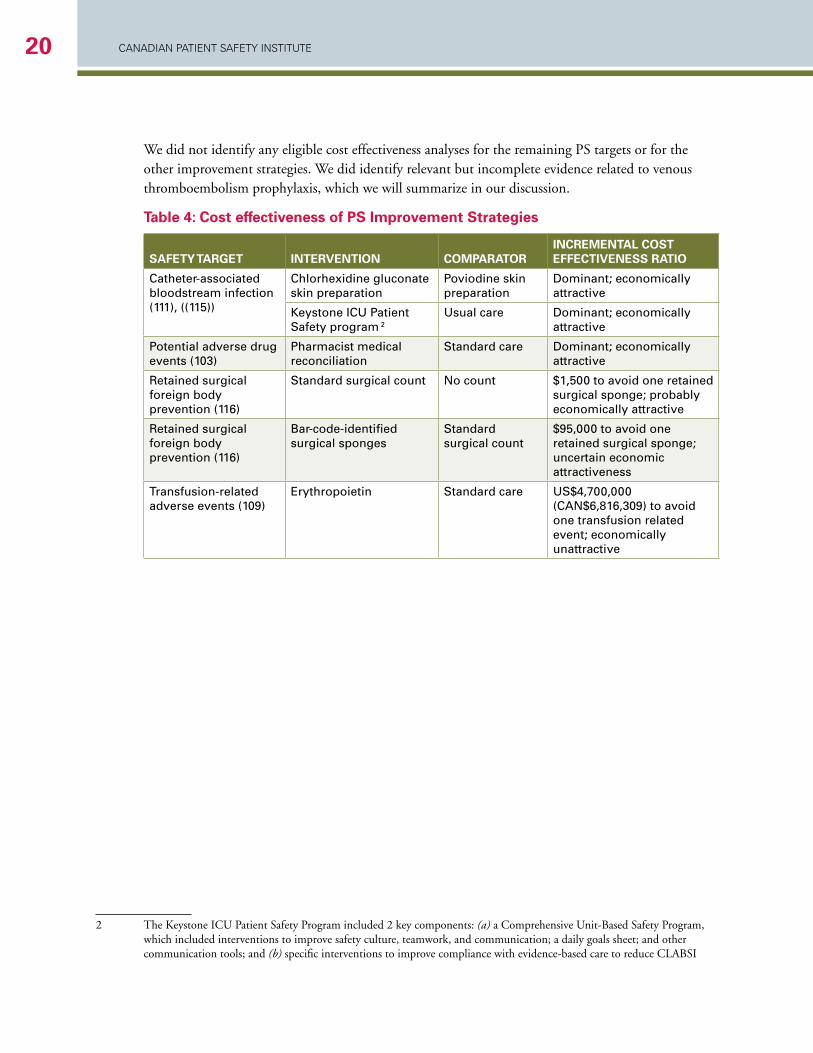
We did not identify any eligible cost effectiveness analyses for the remaining PS targets or for the other improvement strategies. We did identify relevant but incomplete evidence related to venous thromboembolism prophylaxis, which we will summarize in our discussion.
Table 4: cost effectiveness of ps improvement strategies
safeTy TaRgeT inTeRvenTion coMpaRaToRincReMenTal cosT effecTiveness RaTio
Catheter-associated bloodstream infection (111), ((115))
Chlorhexidine gluconate skin preparation
Poviodine skin preparation
dominant; economically attractive
Keystone iCu Patient Safety program 2
usual care dominant; economically attractive
Potential adverse drug events (103)
Pharmacist medical reconciliation
Standard care dominant; economically attractive
retained surgical foreign body prevention (116)
Standard surgical count no count $1,500 to avoid one retained surgical sponge; probably economically attractive
retained surgical foreign body prevention (116)
bar-code-identified surgical sponges
Standard surgical count
$95,000 to avoid one retained surgical sponge; uncertain economic attractiveness
Transfusion-related adverse events (109)
Erythropoietin Standard care uS$4,700,000(CAn$6,816,309) to avoid one transfusion related event; economically unattractive
2
2 The Keystone ICu Patient Safety Program included 2 key components: (a) a Comprehensive unit-Based Safety Program, which included interventions to improve safety culture, teamwork, and communication; a daily goals sheet; and other communication tools; and (b) specific interventions to improve compliance with evidence-based care to reduce CLABSI
The economic Burden of PaTienT SafeTy in acuTe care 21
econoMic BuRden of paTienT safeTy in acuTe caRe in canada
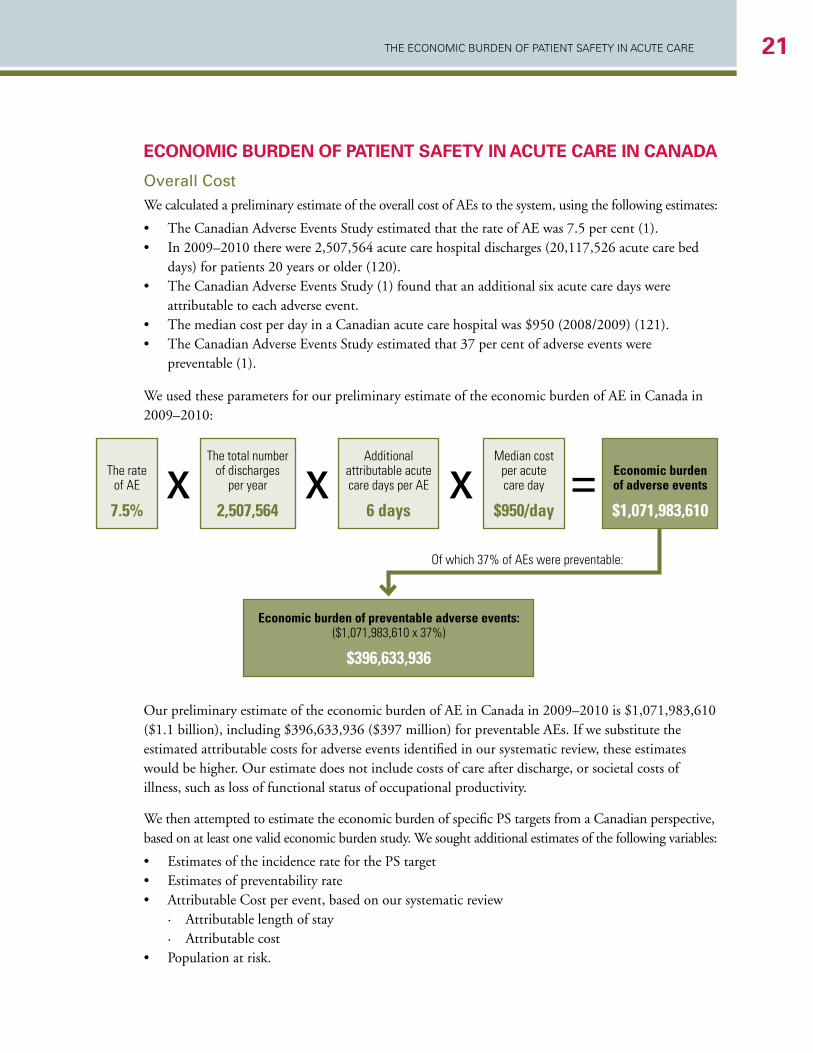
overall CostWe calculated a preliminary estimate of the overall cost of AEs to the system, using the following estimates:
• The Canadian Adverse Events Study estimated that the rate of AE was 7.5 per cent (1). • In 2009–2010 there were 2,507,564 acute care hospital discharges (20,117,526 acute care bed
days) for patients 20 years or older (120). • The Canadian Adverse Events Study (1) found that an additional six acute care days were
attributable to each adverse event.• The median cost per day in a Canadian acute care hospital was $950 (2008/2009) (121). • The Canadian Adverse Events Study estimated that 37 per cent of adverse events were
preventable (1).
We used these parameters for our preliminary estimate of the economic burden of AE in Canada in 2009–2010:
our preliminary estimate of the economic burden of AE in Canada in 2009–2010 is $1,071,983,610 ($1.1 billion), including $396,633,936 ($397 million) for preventable AEs. If we substitute the estimated attributable costs for adverse events identified in our systematic review, these estimates would be higher. our estimate does not include costs of care after discharge, or societal costs of illness, such as loss of functional status of occupational productivity.
We then attempted to estimate the economic burden of specific PS targets from a Canadian perspective, based on at least one valid economic burden study. We sought additional estimates of the following variables:
• Estimates of the incidence rate for the PS target• Estimates of preventability rate• Attributable Cost per event, based on our systematic review
· Attributable length of stay · Attributable cost
• Population at risk.
The rate of AE
7.5%
The total number of discharges
per year
2,507,564
Additional attributable acute care days per AE
6 days
Median cost per acute care day
$950/day
Economic burden of adverse events
$1,071,983,610
Economic burden of preventable adverse events: ($1,071,983,610 x 37%)
$396,633,936
x x x =Of which 37% of AEs were preventable:

CANADIAN PAtIeNt SAfety INStItUte22
We were able to calculate preliminary estimates for Clostridium difficile-associated disease, MRSA infection, vRE infection, and surgical site infection. We consider these to be very rough estimates due to the lack of preventability data for most events, and the limited number of economic burden studies, none of which report primary Canadian data.
Clostridium difficile-Associated disease (CdAd)The Canadian incidence rate of hospital-acquired CDAD infection in adult patients is 4.6 cases per 1,000 patient admissions and 65 per 100,000 patient-days (122). Specific measures of preventability of CDAD are not known, but nosocomial infections are considered to be 20–70 per cent preventable. We used a conservative estimate of 37 per cent preventability, based on the Canadian Adverse Events Study (1). Based on our systematic review, the attributable cost of CDAD is €7,147 (CAN$10,809) (92). In 2009–2010 there were 2,507,564 adult acute care hospital discharges (127). using these estimates, the economic burden of CDAD is $46.1 million (Table 3).
methicillin-resistant Staphylococcus Aureus (mrSA) infectionThere were approximately 2.70 MRSA infections per 1,000 admissions in Canada in the year 2006 (123). We used the baseline estimate of 37 per cent preventability from the Canadian Adverse Events Study (1). Based on our systematic review, the attributable cost of these infections is ₤6,485 (CAN$14,484) (87). In 2009–2010 there were 2,507,564 adult acute care hospital discharges. using these estimates, the economic burden of MRSA is $36.3 million (Table 3).
vancomycin-resistant Enterococci (vrE) infectionThere were approximately 0.052 nosocomial acute care vRE infections per 1,000 admissions in Canada in 2006 (124). We used the baseline estimate of 37 per cent preventability from the Canadian Adverse Events Study (1). Based on our systematic review, the attributable costs of these infections are uS$7,873 (CAN$14,414) and uS$11,989 (CAN$21,950), respectively (88). In 2009–2010 there were 2,507,564 acute care hospital discharges (127). using these estimates, the economic burden of vRE is $695,411 (Table 3).
Surgical Site infections (SSi)Approximately 4 per cent of patients undergoing surgical procedures in ontario between 1992 and 2006 developed SSIs during their index acute care stay. Most of these infections related to abdominal, urologic, gynaecologic, and musculoskeletal procedures (125). Approximately 65 per cent of SSIs can be considered preventable (126). Based on our systematic review, we found wide ranges for the cost of an SSI, depending on the type of surgical site infection. We will use the conservative low estimate of uS$1,051 (CAN$1,174). According to the CIhI Discharge Abstract Database for 2009–2010, there were 799,513 surgical discharges in Canada (127). using these estimates, a conservative low end estimate of the economic burden of SSIs is $24.4 million (Table 3).
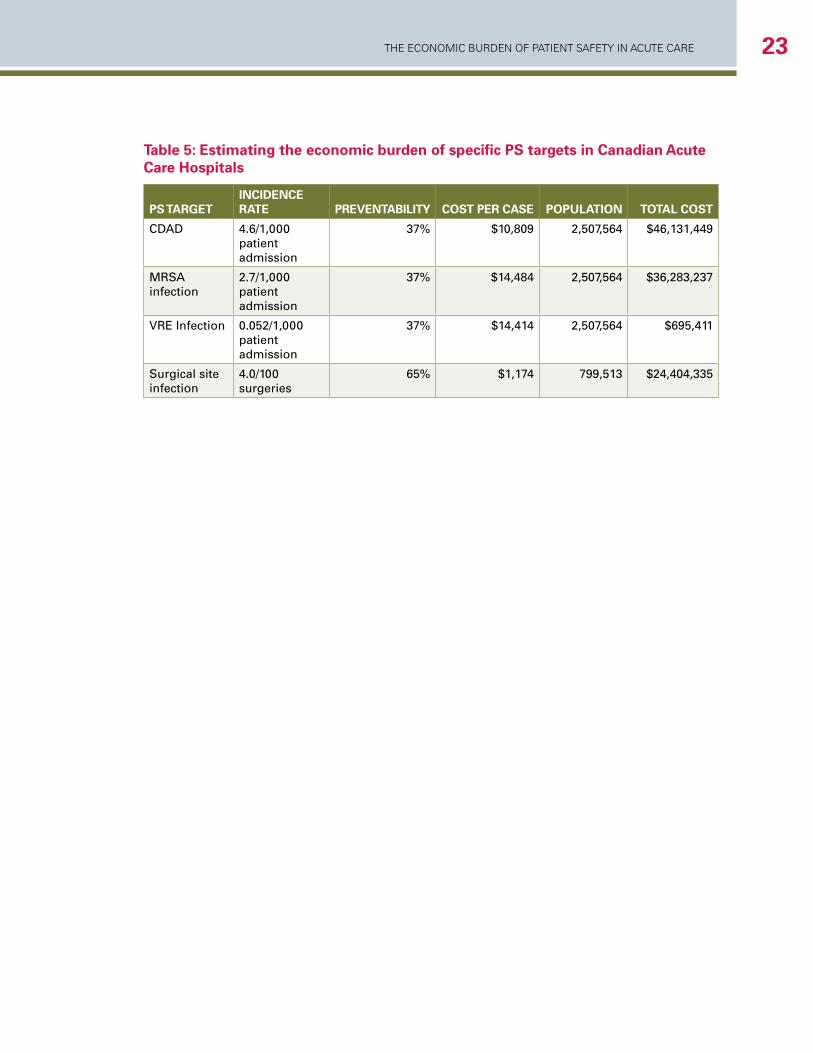
The economic Burden of PaTienT SafeTy in acuTe care 23
Table 5: Estimating the economic burden of specific PS targets in Canadian Acute care hospitals
ps TaRgeTincidence RaTe pRevenTaBiliTy cosT peR case populaTion ToTal cosT
CdAd 4.6/1,000 patient admission
37% $10,809 2,507,564 $46,131,449
mrSA infection
2.7/1,000 patient admission
37% $14,484 2,507,564 $36,283,237
vrE infection 0.052/1,000 patient admission
37% $14,414 2,507,564 $695,411
Surgical site infection
4.0/100 surgeries
65% $1,174 799,513 $24,404,335
CANADIAN PAtIeNt SAfety INStItUte24
GuidElinES And frAmEWorK for EConomiC EvAluATionS in PATiEnT SAfETy
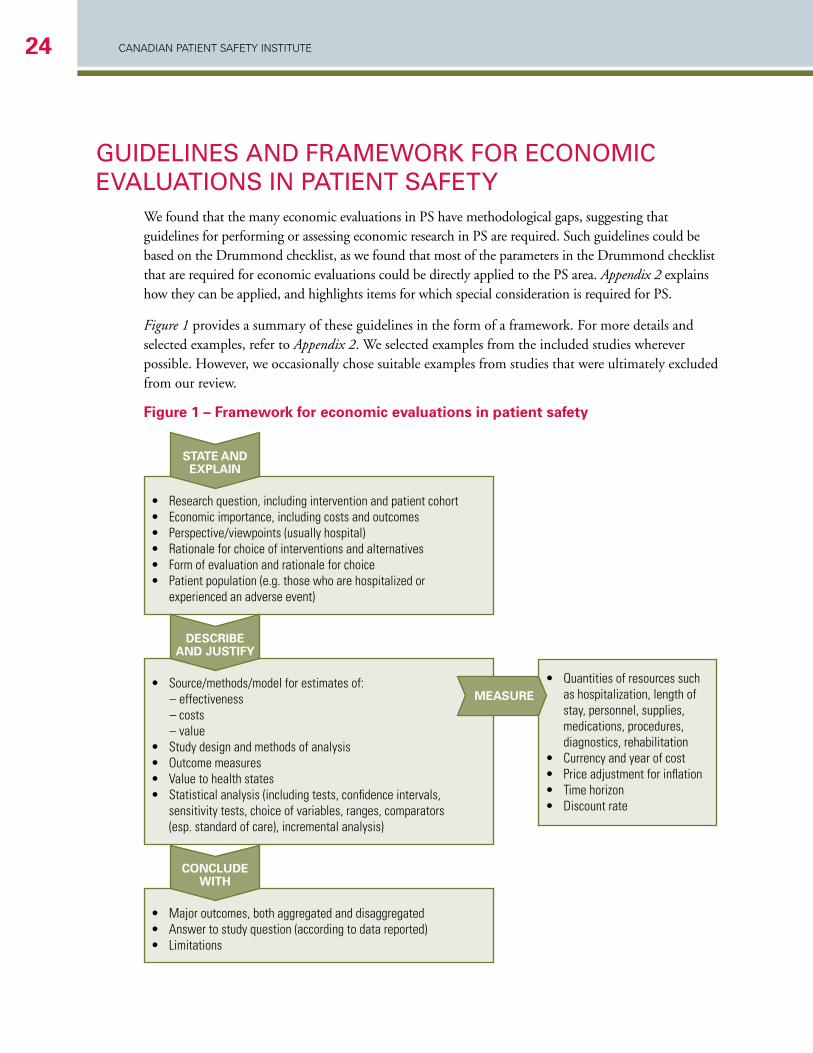
We found that the many economic evaluations in PS have methodological gaps, suggesting that guidelines for performing or assessing economic research in PS are required. Such guidelines could be based on the Drummond checklist, as we found that most of the parameters in the Drummond checklist that are required for economic evaluations could be directly applied to the PS area. Appendix 2 explains how they can be applied, and highlights items for which special consideration is required for PS.
Figure 1 provides a summary of these guidelines in the form of a framework. for more details and selected examples, refer to Appendix 2. We selected examples from the included studies wherever possible. however, we occasionally chose suitable examples from studies that were ultimately excluded from our review.
Figure 1 – Framework for economic evaluations in patient safety
• Research question, including intervention and patient cohort• Economic importance, including costs and outcomes• Perspective/viewpoints (usually hospital)• Rationale for choice of interventions and alternatives• Form of evaluation and rationale for choice• Patient population (e.g. those who are hospitalized or
experienced an adverse event)
• Quantities of resources such as hospitalization, length of stay, personnel, supplies, medications, procedures, diagnostics, rehabilitation
• Currency and year of cost• Price adjustment for inflation• Time horizon• Discount rate
sTaTe and explain
• Source/methods/model for estimates of: – effectiveness – costs – value• Study design and methods of analysis• Outcome measures• Value to health states• Statistical analysis (including tests, confidence intervals,
sensitivity tests, choice of variables, ranges, comparators (esp. standard of care), incremental analysis)
descRiBe and jusTify
• Major outcomes, both aggregated and disaggregated• Answer to study question (according to data reported)• Limitations
conclude wiTh
MeasuRe

The economic Burden of PaTienT SafeTy in acuTe care 25
diSCuSSionThe majority of economic burden studies that we identified had no costing methodology. The remaining economic burden studies reported wide estimates of the economic burden, due to variations in case definitions, patient populations, costing methodology, and study setting. The majority of studies reported the economic burden of adverse events and nosocomial infections. We found that the reported attributable costs of adverse events ranged from uS$2,162 (CAN$4,028) to AuS$11,846 (CAN$12,648). In general hospital populations, the cost per case of hospital-acquired infection ranged from uS$2,027 (CAN$2,265) to uS$12,197 (CAN$22,400). Nosocomial bloodstream infection was associated with costs ranging from €1,814 (CAN$3,268) to €16,706 (CAN$29,950).
We found five comparative economic analyses that reported a total of seven comparisons based on at least one effectiveness study of adequate methodologic quality. Based on these limited studies, pharmacist-led medication reconciliation, the Keystone Michigan ICu Intervention for central line associated blood stream infections, chlorhexidine for vascular catheter site care and standard surgical sponge counts were economically attractive PS improvement strategies.
our preliminary estimate of the economic burden of AE in Canada in 2009–2010 was $1,071,983,610 ($1.1 billion), including $396,633,936 ($397 million) for preventable adverse events. This estimate does not include the direct costs of care after hospital discharge, or societal costs of illness, such as loss of functional status or occupational productivity.
We found significant gaps in the economic methods, which is consistent with the few prior reviews of the economics of patient safety in the acute care setting. A 2005 review identified 165 PS articles that included an economic analysis as an objective, but 35 per cent of these articles provided no economic analysis, and 25 per cent provided no primary economic data. The remaining studies had significant gaps in their costing methodology, and only 16 per cent conducted sensitivity analyses that could address these limitations (128). Another review of economic evaluations of patient safety programs identified 40 studies published between 2001–2004, none of which provided sufficient information about both the cost of the prevention program and the cost of the AE being targeted (129). A 2005 review of cost effectiveness analyses related to bloodstream infections found that the existing analyses were characterized by low data quality, lack of transparency, short time-horizons, and narrow economic perspectives (130).
We did not find cost effectiveness analyses for many improvement strategies that are well known to the safety improvement community. Some improvement strategies, such as rapid response teams to reduce adverse events, or smart infusion pumps to reduce adverse drug events, have not been consistently effective in evaluative studies (131;132). other improvement strategies, such as improving venous thromboembolism prevention or bar coded medication administration, have sufficient evidence of effectiveness, but we were unable to identify an appropriate cost effectiveness analysis.
Although we did not find any recent cost effectiveness analyses on improvement programs in venous thromboembolism based on adequate evidence of effectiveness, we speculate that such an analysis would likely find such programs to be economically attractive. Prevention of venous thromboembolism is a leading safety best practice, based on a large body of high-quality effectiveness evidence for many
CANADIAN PAtIeNt SAfety INStItUte26
prophylaxis regimens (20;133). first, there are numerous economic analyses published before 2000 showing that many forms of prophylaxis are economically attractive compared to no prophylaxis (134-136). The most economically attractive choice among various forms of thromboprophylaxis in specific patient subgroups remains an active area of research, which was beyond the scope of our review (26;27;29-31). Second, gaps in thromboprophylaxis are well described (137;138). Third, computer reminders, standardized order sets, and audit and feedback can improve adherence to appropriate venous thromboembolism prophylaxis (139;140). Despite this significant body of knowledge, we found no published cost effectiveness analyses that explicitly cited adequate evidence of effectiveness for safety improvement programs. one cost-effectiveness analysis evaluated implementation of clinical guidelines on thromboprophylaxis, but this analysis used effectiveness estimates from a single-site uncontrolled before-and-after study. The study assumed that guideline implementation would be 100 per cent effective with no incremental costs beyond the cost of administering prophylaxis (36). Implementing vTE risk assessment and ensuring adequate prophylaxis for medical and surgical patients would likely reduce total costs by £0.9 million (2007 currency) from the perspective of a national healthcare system, according to a large budget-impact analysis published by the National Institute for Clinical Effectiveness (NICE) in the united Kingdom in 2010. This was not a cost effectiveness analysis, because it did not model the effectiveness of guideline implementation, and did not consider any incremental costs of developing, organizing, implementing, and maintaining national and local vTE prevention improvement programs. Despite these limitations, the NICE analysis suggests that ensuring adequate vTE prophylaxis in the acute care setting could be economically attractive (141). finally, an analysis that was published after we completed our review found that a hypothetical program that increased compliance with thromboprophylaxis in critical care from 85 to 95 per cent had an incremental cost effectiveness ratio of approximately $25,000 per quality adjusted life year gained, which would generally be considered economically attractive (142).
our review also found limited cost effectiveness data related to prevention of adverse drug events, even though there are many well-known medication safety improvement strategies. We identified one analysis showing that medication reconciliation by clinical pharmacist was a dominant strategy, based on reductions in potential adverse drug events. We acknowledge that the relationship between preventing potential adverse drug events and preventable adverse drug events remains an area of uncertainty in PS improvement.
Bar-coded medication administration, with electronic medication administration records, reduces potential adverse drug events, based on one study with adequate evidence of effectiveness (143). however, we could not find an economic analysis of bar-coded medication administration that cited evidence other than from simple before-after comparisons (144). We also excluded one cost effectiveness analysis (144) because it did not cite effectiveness data of sufficient quality on rounding clinical ward pharmacists. one Canadian economic analysis of a computerized order entry system to prevent adverse drug events was excluded due to lack of effectiveness data on ADE rates for their computerized physician order entry (CPoE) system (145). When effectiveness data from other systems were included in their analysis, the incremental cost of their CPoE system was estimated at uS$12,700 (CAN$18,704) per ADE prevented, which would make their CPoE system a moderately attractive healthcare intervention (145). As expected, this result was sensitive to the effectiveness and cost of the CPoE system, as well as the baseline rate of ADEs at the hospital.

The economic Burden of PaTienT SafeTy in acuTe care 27
We identified several cost effectiveness analyses related to hand hygiene that cited only evidence from before-and-after studies. one analysis found that alcohol-based hand hygiene product was cheaper and faster, and yielded better hand hygiene compliance, than a detergent-based antiseptic (146), but there was no data on adherence and no data on the impact of safety targets. Another study found that failure to perform hand hygiene by a healthcare worker moving between two unknown MRSA status patients incurred a mean cost per noncompliant event of uS$1.98 (CAN$2.16) (if leaving a room with unknown MRSA status) to $52.53 (if leaving a room of a patient known to be MRSA-positive) (147).
We can make several additional recommendations from our review of cost effectiveness analyses in PS. first, we identified many cost effectiveness analyses that were not based on adequate effectiveness data. Safety improvement programs should consider the EPoC standards when planning their program evaluations. Simple before after studies are insufficient bases for drawing conclusions about effectiveness and cost effectiveness. Second, we did not identify economic analyses that explicitly considered the impact of PS on economically important parameters such as staff retention, staff absenteeism, and patient (market) retention. These parameters should be considered in future cost effectiveness analyses in PS. Third, the relative value of investing in PS improvement as opposed to investing in other healthcare interventions, such as new treatments or diagnostic tests, has not been explicitly considered in cost effectiveness analyses. The relative societal value of improving safety over improving care of primary clinical conditions should be considered in future cost effectiveness analyses in PS. finally, we found no data on the health-related quality of life for many PS targets. Studies of the health-related quality of life associated with PS targets are needed to inform comparative cost-utility analyses with other interventions.
We calculated a preliminary estimate that the economic burden of adverse events in Canada in 2009–2010 was $1.1 billion, including $397 million for preventable adverse events. We consider this a preliminary estimate, and we emphasize that it is based on information that was not obtained as part of our systematic review. We are unaware of prior estimates of the economic burden of adverse events on the Canadian acute care system. for comparison, the most expensive medical condition within the Canadian acute care system in 2005 was acute myocardial infarction (CAN$511 million [2005], or CAN$556 million [2010]) (2). The estimated 1,128,404 acute hospital bed days used each year to care for patients who suffer any adverse event is similar to the total number of acute hospital bed days in Manitoba each year. The estimated 417,509 acute hospital bed days used each year to care for patients who suffer a preventable AE is equivalent to the total number of acute hospital bed days in Newfoundland and Labrador each year.
We attempted to use our review to estimate the economic burden of specific PS targets, but most necessary data for such estimates was lacking. We consider our estimates to be crude and preliminary. We did find a recent estimate of the cost of ventilator associated pneumonia (vAP) to the Canadian healthcare system is CAN$46 million (possible range: $10 million to $82 million) per year (148). This estimate was primarily based on an estimated 1,150 ventilator days per 100,000 Canadians, which yielded 388,009 ventilator days. The attributable ICu length of stay due to vAP is 4.3 days, and the cost for a critical care bed is CAN$2,396 per day (149), giving a total of CAN$10,303. Approximately 55 per cent of vAP was considered preventable (126). using these estimates, the economic burden of vAP in Canada is $23.3 million.
CANADIAN PAtIeNt SAfety INStItUte28
limiTATionSour review has several important limitations.
first, we focused on studies published between 2000-2011 and indexed in MEDLINE. Studies outside of our search strategy may contain potentially useful data. for example, we did not include a 2010 study by the Society of American Actuaries, that was not indexed in MEDLINE (150). We may have missed other studies not published in the traditional literature. however, our major finding that 61 per cent of studies provide no or limited costing methodology would be unchanged by inclusion of a few additional studies.
Second, we focused on the acute care hospital setting because it consumes a significant proportion of Canadian healthcare expenditures, and because a large number of evaluative PS studies have been conducted in the acute care setting. The economic perspective should extend beyond the acute care hospital, as only 22-66 per cent of the economic burden of AEs in acute care are borne by the hospital (151;152). future work could focus on the economic burden and cost effectiveness of safety improvement strategies in other settings, such as long-term care and the community.
Third, we did not evaluate the interrater reliability of our methodologic reviews. our review method was designed to yield higher methodologic ratings, as we always took the higher rating of the two reviewers, yet we still identified a significant lack of methodologic features.
fourth, we arbitrarily assigned one point for each methodologic feature, so that we could report a simple summary measure of methodologic features. however, we recognize that methodologic features are not all equally important.
fifth, the heterogeneity in study methods and methodologic features made it impossible to generate summary estimates of economic burden.
Sixth, we chose to apply the rules of evidence of effectiveness from the Cochrane Effective Practice and organisation of Care (EPoC) Group. We acknowledge that some may not share the opinion that uncontrolled before-after studies are insufficient evidence of effectiveness.
The economic Burden of PaTienT SafeTy in acuTe care 29
SummAryIn summary, we found that most studies of the economic burden of PS in acute care do not report any costing methodology. We found wide estimates of the economic burden from these 61 studies, due to variations in case definitions, patient populations, costing methodology, and study setting. The majority of studies reported the economic burden of adverse events and nosocomial infections.
We found five comparative economic analyses that reported a total of seven comparisons based on at least one effectiveness study of adequate methodologic quality. Based on these limited studies, pharmacist-led medication reconciliation, the Keystone Michigan ICu Intervention for central line associated blood stream infections, chlorhexidine for vascular catheter site care, and standard surgical sponge counts were economically attractive PS improvement strategies.
We calculated a preliminary estimate of the economic burden of AE in Canada in 2009–2010 was $1,071,983,610 ($1.1 billion), including $396,633,936 ($397 million) for preventable adverse events.
CANADIAN PAtIeNt SAfety INStItUte30
ConCluSionS1. The majority of published studies on the economic burden of PS in acute care describes no
costing methodology.
2. for studies that report a costing methodology, there is variability in methods for measuring and attributing costs.
3. Most studies report on the economic burden of adverse events and nosocomial infections.
4. The reported attributable costs of adverse events ranged from uS$2,162 (CAN$4,028) to AuS$11,846 (CAN$12,648). In general hospital populations
5. The cost per case of hospital-acquired infection ranged from uS$2,027 (CAN$2,265) to uS$12,197 (CAN$22,400). Nosocomial bloodstream infection was associated with costs ranging from €1,814 (CAN$3,268) to €16,706 (CAN$29,950).
6. We found only five comparative economic analyses of PS improvement strategies in the acute care setting based on adequate evidence of effectiveness based on guidelines from the Cochrane Effective Practice and organisation of Care (EPoC) Group.
7. Based on these limited analyses, the following PS improvement strategies are economically attractive:
• Pharmacist-led medication reconciliation to prevent potential adverse drug events was the dominant strategy (improved safety and lower cost) when compared to no reconciliation.
• The Keystone ICu Patient Safety Program to prevent central line associated bloodstream infections was the dominant strategy compared to usual care. The Keystone ICu Patient Safety Program included two key components: (a) a Comprehensive unit-Based Safety Program, which included interventions to improve safety culture, teamwork, and communication; a daily goals sheet; and other communication tools; and (b) specific interventions to improve compliance with evidence-based care to reduce central line associated blood stream infections.
• Chlorhexidine for catheter site care to prevent catheter-related bloodstream infections was the dominant strategy when compared to povidone-iodine.
• Standard counting was associated with a cost of uS$1,500 (CAN$1,676) for each surgical foreign body detected, when compared to a strategy of no counting.
8. We estimate that the economic burden of preventable adverse events in the Canadian acute care system was approximately $397 million in 2009-2010.
9. Safety improvement programs should consider the EPoC standards when planning their program evaluations.
10. Cost effectiveness analyses should explicitly consider the impact of patient safety on economically important parameters such as staff retention, staff absenteeism and patient (market) retention.
11. Cost effectiveness analyses should explicitly consider the societal value of improving safety over improving care of primary clinical conditions.
12. Studies of the health-related quality of life associated with PS targets are needed.
13. Guidelines for performing or assessing economic research in PS could be based on the Drummond Checklist (3) (Appendix 2).
The economic Burden of PaTienT SafeTy in acuTe care 31
rEfErEnCES1. Baker GR, Norton PG, flintoft v, Blais R, Brown A, Cox J, et al. The Canadian Adverse Events Study:
the incidence of adverse events among hospital patients in Canada. CMAJ 2004;170(11):1678-86.
2. Canadian Institute for health Information. The cost of acute care hospital stays by medical condition in Canada, 2004-2005. Available at: http://secure.cihi.ca/cihiweb/products/nhex_acutecare07_e.pdf. Accessed on: May 17,2011. 2008.
3. Drummond Mf, Jefferson To. Guidelines for authors and peer reviewers of economic submissions to the BMJ. British Medical Journal 1996;313:275-83.
4. Canadian Agency for Drugs and Technologies in health. Guidelines for the economic evaluation of health technologies: Canada [Internet]. 3rd ed. ottawa: Canadian Agency for Drugs and Technologies in health; vii, 46, A17 p. [cited oct 20]. Available from: http://www.cadth.ca/media/pdf/186_EconomicGuidelines_e.pdf. 2006.
5. Contandriopoulos AP, Champagne f, Denis JL, Avargues MC. L’évalution dans le domaine de la santé: concepts et méthodes [Evaluation in the health sector: concepts and methods]. Rev Epidemiol Sante Publique 2000;48(6):517-39.
6. Canadian Coordinating office for health Technology Assessment. Guidelines for economic evaluation of pharmaceruticals: Canada. ottawa: The Canadian Coordinating office for health Technology Assessment. 1994.
7. Canadian Coordinating office for health Technology Assessment. Guidelines for economic evaluation of pharmaceuticals: Canada [Internet]. 2nd ed. ottawa: The Canadian Coordinating office for health Technology Assessment; vi, 885p. [cited 2008 Jan 31]. Available from: http://www.cadth.ca/media/pdf/peg_e/pdf. 1997.
8. Thomas EJ, Studdert DM, Burstin JR, orav EJ, Zeena T, Williams EJ, et al. Incidence and types of adverse events and negligent care in utah and Colorado. Med Care 2000;38(3):261-71.
9. Graves N, harbarth S, Beyersmann J, Barnett A, halton K, Copper B. Estimating the cost of healthcare-associated infecitons: mind your p’s and q’s. Clin Infect Dis 2010;50(7):1017-21.
10. Barnett AG, Batra R, Graves N, Edgeworth J, Robotham J, Cooper B. using a longitudinal model to estimate the effect of methicillin-resistant Staphylococcus aureus infection on length of stay in an intensive care unit. Am J Epidemiol 2009;170(9):1186-94.
11. Graves N, Weinhold D, Roberts JA. Correcting for bias when estimating the cost of hospital-acquired infection: an analysis of lower repiratory tract infections in non-surgical patients. health Econ 2005;14(7):755-61.
12. Beyersmann J, Kneib T, Schumacher M, Gastmeier P. Nosocomial infection, length of stay, and time-dependent bias. Infect Control hosp Epidemiol 2009;30(3):273-6.
13. Mittmann N, Evans WK, Rocchi A, Longo CJ, Au hJ, husereau D, et al. Addendum to CADTh’s guidelines for the economic evaluation of health technologies: specific guidance for oncology products. ottawa: Canadian Agency for Drugs and Technologies in health. 2009.
CANADIAN PAtIeNt SAfety INStItUte32
14. Gabriel S, Drummond M, Maetzel A, Boers M, Coyle D, Welch v, et al. oMERACT 6 Economics working group report: a proposal for a reference case for economic evaluation in rheumatoid arthritis. J Rheumatol 2003;30:886-90.
15. Drummond Mf, o’Brien B, Stoddart GL, et al. Methods for the economic evaluation of healthcare programmes. Second Edition. oxford. uK: oxford Medical Publications; 1997.
16. Berwick B. The science of improvement. JAMA 2008;299:1182-4.
17. Auerbach AD, Landefeld CS, Shojania KG. The tension between needing to improve care and knowing how to do it. N Engl J Med 2007;357:608-13.
18. A Review Group of the Cochrane Collaboration. Cochrane Effective practice and orangization of care group: EPoC resources for review authors. Available at: http://epoc.cochrane.org/epoc-resources-review-authors. 2011.
19. Mauskopf JA, Sullivan SD, Annemans L, Caro JJ, Mullins CD, Nuijten M, et al. Principles of good practice for budget impact analysis: Report of the ISPoR Task force on Good Research Practices - Budget Impact Analysis. Available at http://www.ispor.org/workpaper/research_practices/Principles_of_Good_Research_Practices-Budges_Impact_Analysis.pdf. [Accessed on october 11, 2011]. value in health 2007;10(5):336-47.
20. Shojania KG, Duncan BW, McDonald KM, Wachter RM. Making health practices safer: a critical analysis of patient safety practices. 2001. Report No.: Evidence Report/Technology Assessment No. 43.
21. haines T, Kuys SS, Morrison G, Clarke J, Bew P. Cost-effectivness analysis of screening for risk of in-hospital falls using physiotherapist clinical judgement. Med Care 2009;47(4):448-56.
22. Spetz J, Jacobs J, hatler C. Cost effectiveness of a medical vigilance system to reduce patient falls. Nursing Economics 2007;25(6):333-52.
23. De Giorgi I, fonzo-Christe C, Cingria L, Caredda B, Meyer v, Pfister RE, et al. Risk and pharmacoeconomic analyses of the injectable medication process in the paediatric and neonatal intensive care units. Int J Qual healthcare 2010;22(3):170-8.
24. Plowman R, Graves N, Esquivel J, Roberts JA. An economic model to assess the cost and benefits of the routine use of silver alloy coated urinary catheters to reduce the risk of urinary tract infections in catheterized patients. J hosp Infect 2001;48:33-42.
25. Marchetti A, Jacobs J, young M, Martin J, Rossiter R. Costs and benefits of an early-alert surveillance system for hospital inpatients. Current Medical Research and opinions 2007;23(1):9-16.
26. Amin AN, Lin J, Johnson Bh, Schulman KL. Clinical and economic outcomes with appropriate or partial prophylaxis. Thrombosis Research 2010;125:513-7.
27. Chiasson TC, Manns BJ, Stelfox hT. An economic evaluation of venous thromboembolism prophylaxis strategies in critically III trauma patients at risk of bleeding. PLoS Med 2009;6(6):e1000098.
28. unruh L, Agrawal M, hassmiller S. The business case for transforming care at the bedside among the “TCAB 10” and lessons learned. Nurs Admin Q 2011;35(2):97-109.
The economic Burden of PaTienT SafeTy in acuTe care 33
29. Bradley CT, Brasel KJ, Miller JJ, Pappas SG. Cost-effectivness of prolonged thromboprophylaxis after cancer surgery. Ann Surg oncol 2010;17:31-9.
30. Cox CE, Carson SS, Biddle AK. Cost-effectiveness of ultrasound in preventing femoral venous catheter-associated pulmonary embolism. Am J Respir Crit Care Med 2003;168:1481-7.
31. Nicolaides A, Goldhaber SZ, Maxwell GL, Labropoulos N, Clark-Pearson DL, Tyllis Th, et al. Cost benefit of intermittent pneumatic compression for venous thromboembolism prophylaxis in general surgery. Int Angiol 2008;27:500-6.
32. hubben G, Bootsma M, Luteijin M, Glynn D, Bishai D, Bonten M, et al. Modelling the costs and effects of selective and universal hospital admission screening for methicillin-resistant Staphylococcus aureus. PLoS oNE 2011;6(3):e14783.
33. Lee By, Wettstein ZS, McGlone SM, Bailey RR, umscheid CA, Smith KJ, et. Economic value of norovirus outbreak control measures in healthcare settings. Clin Microbiol Infect 2011;17:640-6.
34. Padula Wv, Mishra MK, Makic MBf, Sullivan PW. Improving the quality of pressure ulcer care with prevention a cost-effectiveness analysis. Med Care 2011;49:385-92.
35. Echols J, friedman BC, Mullins Rf, hassan Z, Shaver JR, Brandigi C, et al. Clinical utility and economic impact of introducing a bowel management system. J Wound ostomy Continence Nurs 2007;34(6):664-70.
36. ferrando A, Pagano E, Scaglione L, Petrinco M, Gregori D, Ciccone G. A decision-tree model to estimate the impact on cost-effectivness of a venous thromboembolism prophylaxis guideline. Qual Saf healthcare 2009;18:309-13.
37. Dossett LA, Dittus RS, Speroff T, May AK, Cotton BA. Cost-effectiveness of routine radiographs after emergent open cavity operations. Surgery 2008;144(2):317-21.
38. Speroni KG, Lucas J, Dugan L, o’meara-Lett M, Putman M, Daniel M, et al. Comparative effectiveness of standard endotracheal tubes vs. endotracheal tubes with continuous subglottic suctioning on ventilator-associated pneumonia rates. Nursing Economics 2011;29:15-20.
39. Lecumberri R, Panizo E, Gomez-Guiu A, varea S, Garcia-Quetglas E, Serrano M, et al. Economic impact of an electronic alert system to prevent venous thromboembolism in hospitalised patients. J Thromb haemost 2011;9:1108-15.
40. Aspelin P, Aubry P, fransoon SG, Strasser R, Willenbrock R, Lundkvist J. Cost-effectiveness of iodixanol in patients at highrisk of contrast-induced nephropathy. Am heart J 2005;149(2):298-303.
41. Klarenbach SW, Pannu N, Tonelli MA, Manns BJ. Cost-effectiveness of hemofiltration to prevent contrast nephropathy in patients with chronic kidney disease. Crit Care Med 2006;34(4):1044-51.
42. hoonhout Lh, de Bruijne MC, Wagner C, Zegers M, Waaijman R, Spreeuwenberg P, et al. Direct medical costs of adverse events in Dutch hospitals. BMC health Services Research 2009;9:27-37.
43. Ehsani JP, Jackson T, Duckett SJ. The incidence and cost of adverse events in victorian hospitals 2003-04. MJA 2006;184(11):551-5.
CANADIAN PAtIeNt SAfety INStItUte34
44. New PW, Jackson T. The costs and adverse events associated with hospitalization of patients with spinal cord injury in victoria, Australia. SPINE 2010;35(7):796-802.
45. Pappas Sh. The cost of nurse-sensitive adverse events. JoNA 2008;38(5):230-6.
46. Morris JA, Carrillo y, Jenkins JM, Smith PW, Bledsoe S, Pichert J, et al. Surgical adverse events, risk management, and malpractice outcome: Morbidity and mortality review in not enough. Ann Surg 2003;237(6):844-52.
47. Aoki N, uda K, ohta S, Kiuchi T, fukui T. Impact of miscommunication in medical dispute cases in Japan. Int J Qual healthcare 2008;20(5):358-62.
48. Kaushal R, Bates DW, franz C, Soukup JR, Rothschild JM. Costs of adverse events in intensive care units. Crit Care Med 2007;35(11):2479-83.
49. Senst BL, Achusim LE, Genest RP, Cosentino LA, ford CC, Little JA, et al. Practical approach to determining costs and frequency of adverse drug events in a healthcare network. Am J health-Syst Pharm 2001;58:1126-32.
50. Daily currency converter. Available at: http://www.bankofcanada.ca/rates/exchange/daily-converter/ Bank of Canada. 2011.
51. Inflation Calculator. Available at: http://www.bankofcanada.ca/rates/related/inflation-calculator/ Bank of Canada. 2011.
52. Chen yy, Wang fD, Liu Cy, Chou P. Incidence rate and variable cost of nosocomial infections in different types of intensive care units. Infect Control hosp Epidemiol 2009;30:39-46.
53. Chen yy, Chou yC, Chou P. Impact of nosocomial infection on cost of illness and length of stay in intensive care units. Infect Control hosp Epidemiol 2005;26(3):281-7.
54. Plowman R, Graves N, Griffin MAS, Roberts JA, Swan Av, Cookson B, et al. The rate and cost of hospital-acquired infections occurring in patients admitted to selected specialties of a distract general hosptial in England and the national burden imposed. J hosp Infect 2001;47(198):209.
55. Kilgore ML, Ghosh K, Beavers M, Wong Dy, hymel PA, Brossette SE. The costs of nosocomial infections. Med Care 2008;46(1):101-4.
56. Esatoglu AE, Agirbas I, onder oR, Celik y. Additional cost of hospital-acquired infection to the patient: a case study in Turkey. health Services Management Research 2006 Aug;19(3):137-43.
57. Sheng Wh, Wang JT, Lu DCT, Chie WC, Chen yC, Chang SC. Comparative impact of hospital-acquired infections on medical costs, length of hospital stay and outcome between community hospitals and medical centres. J hosp Infect 2005;59:205-14.
58. Lee J, Imanaka y, Sekimoto M, Ishizaki T, hayashida K, Ikai h, et al. Risk-adjusted increases in medical resource utilization assocated with healthcare-associated infections in gastrectomy patients. J Eval Clin Pract 2010;16:100-6.
The economic Burden of PaTienT SafeTy in acuTe care 35
59. Mahieu LM, Buitenweg N, Beutels P, De Dooy JJ. Additional hospital stay and charges due to hospital-acquired infections in a neonatal intensive care unit. Journal of hospital Infection 2001 Mar;47(3):223-9.
60. Graves N, Nicholls TM, Morris AJ. Modeling the costs of hospital-acquired infections in New Zealand. Infect Control hosp Epidemiol 2003;24(3):214-23.
61. Defez C, fabbro-Peray P, Cazaban M, Boudemaghe T, Sotto A, Daures JP. Additional direct medical costs of nosocomial infections: an estimation from a cohort of patients in a french university hospital. J hosp Infect 2008;68:130-6.
62. Weber WP, Zwahlen M, Reck S, feder-Mengus C, Widmer Af, Marti WR. Economic burden of surgical site infections at a European university hospital. Infect Control hosp Epidemiol 2008;29(7):623-9.
63. Whitehouse JD, friedman D, Kirkland KB, Richardson WJ, Sexton DJ. The impact of surgical-site infections following orthopedic surgery at a community hospital and a university hospital: adverse quality of life, excess length of stay, and extra cost. Infect Control hosp Epidemiol 2002;23(4):183-9.
64. Mahmoud NN, Turpin RS, yang G, Saunders WB. Impact of surgical site infections on length of stay and costs in selected colorectal procedures. Surg Infect 2009;10(6):539-44.
65. Penel N, Lefebvre JL, Cazin JL, Clisant S, Neu JC, Dervaux B, et al. Additional direct medical costs associated with mosocomial infections after head and neck cancer surgery: a hosptial-perspective analysis. Int J oral Maxillofac Surg 2008;37:135-9.
66. Jenney AW, harrington GA, Russo PL, Spelman DW. Cost of surgical site infections following coronary artery bypass surgery. ANZ Journal of Surgery 2001 Nov;71(11):662-4.
67. olsen MA, Butler AM, Willers DM, Gross GA, hamilton Bh, fraser vJ. Attributable costs of surgical site infection and endometritis after low transverse cesarean delivery. Infect Control hosp Epidemiol 2010;31(3):276-82.
68. Blot SI, Depuydt P, Annemans L, Benoit D, hoste E, De Waele JJ, et al. Clinical and economic outcomes in critically ill patients with nosocomial catheter-related bloodstream infections. Clin Infect Dis 2005;41:1591-8.
69. orsi BG, Di Stefano L, Noah N. hospital-acquired, laboratory-confirmed bloodstream infection: Increased hospital stay and direct costs. Infect Control hosp Epidemiol 2002;23(4):190-7.
70. Pirson M, Dramaix M, Struelens M, Riley Tv, Leclercq P. Costs associated with hospital-acquired bacteraemia in a Belgian hospital. Journal of hospital Infection 2005 Jan;59(1):33-40.
71. Pirson M, Leclercq P, Jackson T, Leclercq M, Garrino M, Sion C. financial consequences of hospital-acquired bacteraemia in three Belgian hospitals in 2003 and 2004. J hosp Infect 2008;68:9-16.
72. Kilgore M, Brossette SE. Cost of bloodstream infections. Am J Infect Control 2008;36:S172.e1-S172.e3.
73. Elward AM, hollenbeak CS, Warren DK, fraser vJ. Attributable cost of nosocomial primary bloodstream infection in pediatric intensive care unit patients. Pediatrics 2005 Apr;115(4):868-72.
CANADIAN PAtIeNt SAfety INStItUte36
74. Payne NR, Carpenter Jh, Badger GJ, horbar JD, Rogowski J. Marginal increase in cost and excess length of stay associated with nosocomial bloodstream infections in surviving very low birth weight infants. Pediatrics 2004 Aug;114(2):348-55.
75. Chu vh, Crosslin DR, friedman Jy, Reed SD, Cabell Ch, Griffiths RI, et al. Staphylococcus aureus bateremia in patients with prosthetic devices: costs and outcomes. Am J Med 2005;118:1416.e19-1416.e24.
76. Adrie C, Alberti C, Chaix-Couturier C, Azoulay E, de Lassence A, Cohen y, et al. Epidemiology and economic evaluation of severe sepsis in france: age, severity, infection site, and palce of acquisition (community, hospital, or intensive care unit) as determinants of workload and cost. Journal of Critical Care 2005;20:46-58.
77. Brun-Buisson C, Roudot-Thoraval f, Girou E, Grenier-Sennelier C, Durand-Zaleski I. The costs of septic syndromes in the intensive care unit and influence of hospital-acquired sepsis. Intensive Care Medicine 2003 Sep;29(9):1464-71.
78. festini f, Cocchi P, Mambretti D, Tagliabue B, Carotti M, Coifi D, et al. Nosocomial rotavirus gastroenteritis in pediatric patients: a multi-centre prospective cohort study. BMC Infectious Diseases 2010;10:235-42.
79. fruhwirth M, Berger K, Ehlken B, Moll-Schuler I, Brosl S, Mutz I. Economic impact of community- and nosocomially acquired rotavirus gastroenteritis in Austria. Pediatr Infect Dis J 2001;20:184-8.
80. Piednoir E, Bessaci K, Bureau-Chalot f, Sabouraud P, Brodard v, Andreoletti L, Bajolet o. Economic impact of healthcare-associated rotavirus infection in a paediatric hospital. Journal of hospital Infection 2003 Nov;55(3):190-5.
81. Tambyah PA, Knasinski v, Maki DG. The direct costs of nosocomial catheter-associated urinary tract infection in the era of managed care. Infect Control hosp Epidemiol 2002;23(1):27-31.
82. Morse BC, Boland BN, Blackhurst DW, Roettger Rh. Analysis of centers for medicaid and medicare services ‘Never events’ in elderly patients undergoing bowel operations. The American Surgeon 2010;76(8):841-5.
83. Rosenthal vD, Buzman S, Migone o, Safdar N. The attributable cost and length of hospital stay because of nosocomial pneumonia in intensive care units in 3 hospitals in Argentina: A prospective matched analysis. Am J Infect Control 2005;33:157-61.
84. Dietrich ES, Demmler M, Schulgen G, fekec K, Mast o, Pelz K, Daschner fD. Nosocomial pneumonia: a cost-of-illness analysis. Infection 2002 Apr;30(2):61-7.
85. Brilli RJ, Sparling KW, Lake MR, Butcher J, Myers SS, Clark MD, et al. The business case for preventing ventilator-associated pneumonia in pediatric intensive care unit patients. Jt Comm J Qual Saf 2008;34(11):629-38.
86. Macartney KK, Gorelick Mh, Manning ML, hodinka RL, Bell LM. Nosocomial respiratory syncytial virus infections: the cost-effectiveness and cost-benefit of infection control. Pediatrics 2000 Sep;106(3):520-6.
The economic Burden of PaTienT SafeTy in acuTe care 37
87. Watters K, o’Dwyer TP, Rowley h. Cost and morbidity of the MRSA in head and neck cancer patients: what are the consequences? J Laryngol otol 2004;118:694-9.
88. Puzniak LA, Gillespie KN, Leet T, Kollef M, Mundy LM. A cost-benefit analysis of gown use in controlling vancomycin-resistant enterococcus transmission: Is it worth the price? Infect Control hosp Epidemiol 2004;25(5):418-24.
89. Anil M, helvaci M, ozkalay N, Toprak E, Anil AB, Dilek M, et al. Salmonella typhimurium outbreak in a neonatal unit in Turkey. Indian J Pediatr 2009;76:629-33.
90. Baggett hC, Duchin JS, Shelton W, Zerr DM, heath J, ortega-Sanchez IR, et al. Two nosocomial pertussis outbreaks and their associated costs - King County, Washington, 2004. Infect Control hosp Epidemiol 2007;28(5):537-43.
91. Wilson SJ, Knipe CJ, Zieger MJ, Gabehart KM, Goodman JE, volk hM, et al. Direct costs of multidrug-resistance acinetobater baumannii in the burn unit of a public teaching hospital. Am J Infect Control 2004;32:342-4.
92. vonberg RP, Reichardt C, Behnke M, Schwab f, Zindler S, Gastmeier P. Cost of nosocomial Clostridium difficile-associated diarrhoea. J hosp Infect 2008;70:15-20.
93. Bou R, Lorente L, Aguilar A, Perninan J, Ramos P, Peris M, et al. hospital economic impact of an outbreak of Pseudomonas aeruginosa infections. J hosp Infect 2009;71:138-42.
94. fretz R, Schmid D, Jelovcan S, Tschertou R, Krassnitzer E, Schirmer M, et al. An outbreak of norovirus gastroenteritis in an Austrian hospital, winter 2006-2007. Wien Klin Wochenschr 2009;121:137-43.
95. Zingg W, Colombo C, Jucker T, Bossart W, Ruef C. Impact of an outbreak of norovirus infection on hospital resources. Infect Control hosp Epidemiol 2005;26(3):263-7.
96. Spearing NM, Jensen A, McCall BJ, Neill AS, McCormack JG. Direct costs associated with a nosocomial outbreak of Salmonella infection: An ounce of prevention is worth a pound of cure. Am J Infect Control 2000;28:54-7.
97. Caprini JA, Botteman Mf, Stephens JM, Nadipelli v, Ewing MM, Brandt S, et al. Economic burden of long-term complications of deep vein thrombosis after total hip replacement surgery in the united States. value in health 2003;6(1):59-74.
98. MacDougall DA, feliu AL, Boccuzzi SJ, Lin J. Economic burden of deep-vein thrombosis, pulmonary embolism, and post-thombotic syndrome. Am J health-Syst Pharm 2006;63(Suppl 6):S5-S15.
99. Nadkarni JB, Iyengar KP, Dussa C, Watve S, vishwanath K. orthopaedic injuries foloowing falls by hospital in-patients. Gerontology 2005;51:329-33.
100. oliver D, Killick S, Even T, Willmott M. Do falls and falls-injuries in hospital indicate negligent care - and how big is the risk? A retrospective analysis of hte NhS litigation authority database of clinical negligence claims, resulting from falls in hospitals in England 1995 to 2006. Qual Saf healthcare 2008;17:431-6.
CANADIAN PAtIeNt SAfety INStItUte38
101. Nurmi I, Luthje P. Incidence and costs of falls and fall injuries among elderly in institutional care. Scand J Prim healthcare 2002;20:118-22.
102. hill KD, vu M, Walsh W. falls in the acute hospital setting - impact on resource utilisation. Australian health Review 2007;31(3):471-7.
103. Karnon J, Campbell f, Czoski-Murray C. Model-based cost-effectivness analysis of interventions aimed at preventing medication error at hospital admission (medicines reconciliation). J Eval Clin Pract 2009;15:299-306.
104. Kwan y, fernandes o, Nagge J, Wong G, huh J, hurn D, et al. Implementation and a randomized controlled evlauation of pharmacists medication assessments in a surgical preadmission clinic. Pharmacotherapy 2005;25:1462.
105. Mcfazdean E, Isles C, Moffar J, Norrie J, Steward DI. Is there a role for a prescribing pharmacist in preventing prescribing errors in the medical admissions ward? Pharmaceutical Journal 2003;270:896-9.
106. Scarsi KK, fotis MA, Noskin GA. Pharmacist participation in medical rounds reduces medication errors. Am J health-Syst Pharm 2002;59:2089-92.
107. Bates DW, Leape LL, Petrycki S. Incidence and preventability of adverse drug events in hospitalized adults. J Gen Intern Med 1993;8:289-94.
108. Collins DJ, Nickless GD, Green Cf. Medication histories: does anyone know what medicines a patients should be taking? International Journal of Pharmacy Practice 2004;12:173-8.
109. Shermock KM, horn E, Lipsett PA, Pronovost PJ, Dorman T. Number needed to treat and cost of recombinant human erythropoeitin to avoid one transfusion-related adverse event in critically ill patients. Crit Care Med 2005;33(3):497-503.
110. Corwin hL, Gettinger A, Pearl RG, et al. Efficacy of reconbinant human erythropoietin in critically ill patients. JAMA 2002;288:2827-35.
111. Maenthaisong R, Chaiyakunapruk N, Thamlikitkul v. Cost-effectiveness analysis of chlorhexidine gluconate compared with povidone-iodine solution for catheter-site care in Siriraj hospital, Thailand. J Med Assoc Thai 2006;89(Suppl. 5):S94-S101.
112. Chaiyakunapruk N, veenstra DL, Lipsky BA, Saint S. Chlorhexidine compared with povidone-iodine solution for vascular catheter-site care: A meta-analysis. Ann Intern Med 2002;136:792-801.
113. Chaiyakunapruk N, veenstra DL, Lipsky BA, Sullivan SD, Saint S. vascular catheter site care: the clinical and economic benefits of chlorhexidine gluconate compared with povidone iodine. Clin Infect Dis 2003;37:764-71.
114. Pronovost P, Needleman J, Berenholtz SM, et al. An intervention to reduce catheter-related bloodstream infections in the ICu. N Engl J Med 2006;355(26):2725-32.
115. Waters hR, Korn R Jr., Colantuoni E, Berenholtz SM, Goeschel CA, Needham DM, et al. The business case for quality: Economic analysis of the Michican Keyston patient safety program in ICus. Am J Med Qual 2011;26(5):333-9.
The economic Burden of PaTienT SafeTy in acuTe care 39
116. Regenbogen SE, Greenberg CC, Resch SC, Kollengode A, Cima RR, Zinner MJ, et al. Prevention of retained surgical sponges: A decision-analytic model predicting relative cost-effectiveness. Surgery 2009;145(5):527-35.
117. Greenberg CC, Diaz-flores R, Lipsitz SR, et al. Bar-coding surgical sponges to improve safety: A randomized control trial. Ann Surg 2008;247:612-6.
118. Cima RR, Kollengode A, Garnatz J, Storsween A, Weisbrod C, Deschamps C. Incidence and characteristics of potential and actual retained foreign object events in surgical patients. J Am Coll Surg 2008;207:80-7.
119. Revesz G, Siddiqi TS, Buchheit WA, Bonitatibus M. Detection of retained surgical sponges. Radiology 1983;149:411-3.
120. Inpatient hospitalizations: volume, length of stay and standarized rates. Available at: http://apps.cihi.ca/MicroStrategy/asp/Main.aspx?server=torapprd30.cihi.ca&project=Quick+Stats&uid=pce_pub_en&pwd=&evt=2048001&visualizationMode=0&documentID=C6f8B4144B03958E3AE3CAB5DD440EA7. Accessed on: May 17,2011 Canadian Institute for health Information. 2010.
121. Canadian Institute for health Information. Canadian MIS Database: Cost per day for a general hospital ward bed in fiscal year 2008-2009 by province. 2011.
122. Gravel D, Miller M. Canadian Nosocomial Infection Surveillance Program final Report Clostridium difficile Associated Diarrhea in Acute-Care hospitals Participating in CNISP: November 1, 2004 to April 30, 2005. Available at: http://www.phac-aspc.gc.ca/nois-sinp/pdf/c-difficile_cnisp-pcsin-eng.pdf. [Access Date:April 11, 2011]. 2007.
123. Public health Agency of Canada. Canadian Nosocomial Infection Surveillance Program (CNISP) Surveillance for Methicillin-resistant Staphylococcus aureus (MRSA) in Patients hospitalized in Canadian Acute-Care hospitals Participating in CNISP 2006-2007 Preliminary Results. Available at: http://www.phac-aspc.gc.ca/nois-sinp/pdf/mrsa-sarm-eng.pdf. [Access Date: April 11, 2011]. 2008.
124. Public health Agency of Canada. Surveillance for vancomycin Resistant Enterococci (vRE) in Patients hospitalized in Canadian Acute-Care hospitals Participating in CNISP 2006 Results. Available at: http://www.phac-aspc.gc.ca/nois-sinp/pdf/vre-erv06-result-eng.pdf. [Access Date: April 11, 2011]. 2008.
125. Daneman N, Thiruchelvam D, Redilmeier DA. Statin use and the risk of surgical site infections in elderly patients undergoing elective surgery. Arch Surg 2009;144(10):938-45.
126. umscheid CA, Mitchell MD, Doshi JA, Agarwal R, Kendal W, Brennan PJ. Estimating the proportion of healthcare associated infections that are reasonably preventable and the related mortality and costs. Infect Control hosp Epidemiol 2011;32(2):101-14.
127. Number of Surgical Discharges. Available at: http://www.cihi.ca/cihi-ext-portal/internet/en/applicationfull/types+of+care/hospital+care/cihi021685. Accessed on: May 17, 2011 Canadian Institute for health Information. 2010.
128. Schmidek JM, Weeks WB. What do we know about financial returns on investments in patient safety? A literature review. Jt Comm J Qual Patient Saf 2005;31(12):690-9.
CANADIAN PAtIeNt SAfety INStItUte40
129. fukuda h, Imanaka y. Assessment of transparency of cost estimates in economic evaluations of patient safety programmes. J Eval Clin Pract 2009;15:451-9.
130. halton K, Graves N. Economic evaluation and catheter-related bloodstream infections. Emerg Infect Dis 2007;13(6):815-23.
131. Chan PS, Renuka J, Nallmothu BK, Berg RA, Sasson C. Rapid response teams a systematic review and meta-analysis. Arch Intern Med 2010;170(1):18-26.
132. Rothschild JM, Keohane CA, Cook Ef, orav EJ, Burdick E, Thompson S, et al. A controlled trial of smart infusion pumps to improve medication safety in critically ill patients. Crit Care Med 2005;33:533-40.
133. Geerts W, Bergqvist D, Pineo Gf, heit JA, Samama CM, Lassen MR, et al. Prevention of venous thromboembolism: American college of chest physicians evidence-based clinical practice guidelines (8th edition). Chest 2008;133(Suppl 6):381S-453S.
134. Mamdani MM, Weingarten CM, Stevenson JG. Thromboembolic prophylaxis in moderate-risk patients undergoing elective abdominal surgery: decision and cost-effectiveness analyses. Pharmacotherapy 1996;16(6):1111-27.
135. Bergqvist D, Lindgren B, Matzsch T. Comparison of the cost of preventiong postoperative deep vein thrombosis with either unfractionated or low molecular weight heparin. Brit J Surg 1996;83:1548-52.
136. Borris LC, Lassen MR. Thrombroprophylaxis with low molecular weight heparin after major orthopaedic surgery is cost effective. Drugs 1996;52(Suppl 7):42-6.
137. Kahn SR, Panju A, Geerts W, Pineo Gf, Desjardins L, Turpie AG, et al. Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada. Thromb Res 2007;119(2):145-55.
138. Cohen AT, Tapson vf, Bergmann Jf, Goldhaber SZ, Kakkar AK, Deslandes B, et al. venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDoRSE study): a multinational cross-sectional study. Lancet 2008;371(9610):387-94.
139. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med 2005;352:969-77.
140. McMullin J, Cookd D, Griffith L, et al. Minimixing errors of omission: Behavioural reinforcement of heparin to avert venous emboli: The BEhAvE study. Crit Care Med 2006;34:694-9.
141. National Institute for Clinical Excellence. venous thromboembolism: reducing the risk. Costing report. Implementing NICE Guidance. NICE Clinical Guideline 92. Revised May 2010. Available at: http://guidance.nice.org.uk/CG92/CostingReport/pdf/English. 2010.
142. Sud S, Mittmann N, Cook DJ, Geerts W, Chan B, Dodek P, et , et al. Screening and prevention of venous thromboembolism in critically ill patients: a decision analysis and economic evaluation. Am J Respir Crit Care Med 2011;184(11):1289-98.
The economic Burden of PaTienT SafeTy in acuTe care 41
143. Poon EG, Keohane CA, yoon CS, Ditmore M, Bane A, Levtzion-Korach o, et al. Effect of bar-code technology on the safety of medication administration. N Engl J Med 2010;362:1698-707.
144. Karnon J, McIntosh A, Dean J, Bath P, hutchinson A, oakley J, et al. Modelling the expected net benefits of interventions to reduce the burden of medication errors. J health Serv Res Policy 2008;13(2):85-91.
145. Wu RC, Laporte A, ungar WJ. Cost-effectiveness of an electronic medication ordering and administration system in reduing adverse drug events. J Eval Clin Pract 2007;13:440-8.
146. Cimiotti JP, Stone PW, Larson EL. A cost comparison of hand hygiene regimens. Nursing Economics 2004;22(4):196-204.
147. Cummings KL, Anderson DJ, Kaye KS. hand hygiene noncompliance and the cost of hospital-acquired methicillin-resistant Staphylococcus aureus infection. Infect Control hosp Epidemiol 2010;31(4):357-64.
148. Muscedere JG, Marin CM, heyland DK. The impact of ventilator-associated pneumonia on the Canadian healthcare system. J Crit Care 2008;23:5-10.
149. ontario case costing initiative. Available at: www.occp.com. 2011.
150. Shreve J, van Den Bos J, Gray T, halford M, Rustagi K, Ziemkiewicz E. The economic measurement of medical errors. Available at: http://www.soa.org/files/pdf/research-econ-measurement.pdf. 2010.
151. Zhan C, friedman B, Mosso A, Pronovost P. Medicare payment for selected adverse events: building the business case for investing in patient safety. health Affairs 2006;25(5):1386-93.
152. Mello MM, Studdert DM, Thomas EJ, yoon CS, Brennan TA. Who pays for medical errors? An analysis of adverse events costs, the medical liabililty system, and incentives for patient safety improvement. Journal of Empirical Legal Studies 2011;4(4):835-60.
153. Perras C, Tsakonas E, Ndegwa S, Conly J, aliquette L, t al. vancomycin or metronidazole for treatment of Clostridium difficile infection: Clinical and economic analyses [Internet]. ottawa: Canadian Agency for Drugs and Technologies in health. (Technology report; no.136). [cited 2011-01-26]. Available from http://www.cadth.ca/preview.php/en/hta/reports-publications/search/publication/2775. 2011.
154. Dainty L, Maxwell GL, Clarke-Pearson DL, Myers ER. Cost-effectiveness of combination thromboembolism prophylaxis in gynecologic oncology surgery. Gynecologic oncology 2004;93:366-73.
155. Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. Adverse Drug Events Prevention Study Group 1997;307-11.
156. Pinilla J, Murillo C, Carrasco f, humet C. Case-Control analysis of the financial cost of medication errors in hospitalized patients. European Journal of health Economics 2006;7:66-71.
157. Classen DC. Adverse drug events in hospitalized patients: excess length of stay, extra costs, and attributable mortality. JAMA 1997;277:301-6.

CANADIAN PAtIeNt SAfety INStItUte42
158. Thongpiyapoom S, Narong MN, uwalak N, amulitrat S, ntaraksa P, oonrat J, t al. Device-associated infections and patterns of antimicrobial resistance in a medical-surgical intensive care unit in a univeristy hospital in Thailand. J Med Assoc Thai 2004;87:819-24.
159. National health Secutiry office. J Diagnosis Related Group Relative Weight 2002-2003. 2003. 182-8 p.
160. Gawande AA, Studdert DM, orav EJ, BrennanTA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med 2003;348:229-35.
161. Egorova NN, Moskowits A, Gelijins A, Weinberg A, Curty J, Rabin-fastman B, et al. Managing the prevention of retained surgical instruments. What is the value of counting? Ann Surg 2008;247(1):13-8.
162. forgue E, Aimes A. Les “Pieges” de la Chirurgie. Paris: Masson et Cie; 1939.
163. Roberts RR, Scott D, Cordell R, Solomon SL, Steele L, Kampe LM, et al. The use of economic modeling to determine the hospital costs associated with nosocomial infections. Clin Infect Dis 2003;36:1424-32.
164. fuller RL, McCullough EC, Bao MZ, Averill Rf. Estimating the costs of potentially preventable hospital acquired complications. healthcare financing Review 2009;30(4):17-32.
165. Mauldin PD, Salgado CD, Durkalski vL, et al. Nosocomial infections due to mechicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus: relationships with antibiotic use and cost drivers. Ann Pharmacother 2008;42(3):317-26.
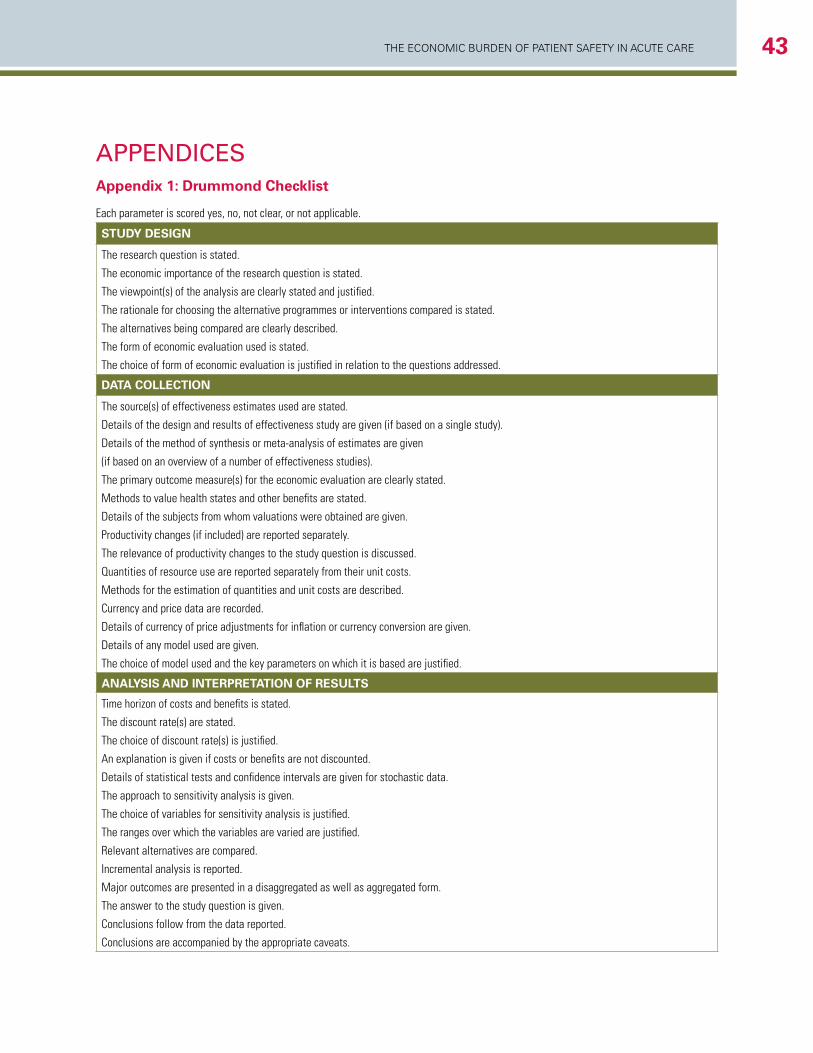
The economic Burden of PaTienT SafeTy in acuTe care 43
APPEndiCESAppendix 1: Drummond Checklist
Each parameter is scored yes, no, not clear, or not applicable.
sTudy design
The research question is stated.
The economic importance of the research question is stated.
The viewpoint(s) of the analysis are clearly stated and justified.
The rationale for choosing the alternative programmes or interventions compared is stated.
The alternatives being compared are clearly described.
The form of economic evaluation used is stated.
The choice of form of economic evaluation is justified in relation to the questions addressed.
daTa collecTion
The source(s) of effectiveness estimates used are stated.
Details of the design and results of effectiveness study are given (if based on a single study).
Details of the method of synthesis or meta-analysis of estimates are given
(if based on an overview of a number of effectiveness studies).
The primary outcome measure(s) for the economic evaluation are clearly stated.
Methods to value health states and other benefits are stated.
Details of the subjects from whom valuations were obtained are given.
Productivity changes (if included) are reported separately.
The relevance of productivity changes to the study question is discussed.
Quantities of resource use are reported separately from their unit costs.
Methods for the estimation of quantities and unit costs are described.
Currency and price data are recorded.
Details of currency of price adjustments for inflation or currency conversion are given.
Details of any model used are given.
The choice of model used and the key parameters on which it is based are justified.
analysis and inTeRpReTaTion of ResulTs
Time horizon of costs and benefits is stated.
The discount rate(s) are stated.
The choice of discount rate(s) is justified.
An explanation is given if costs or benefits are not discounted.
Details of statistical tests and confidence intervals are given for stochastic data.
The approach to sensitivity analysis is given.
The choice of variables for sensitivity analysis is justified.
The ranges over which the variables are varied are justified.
Relevant alternatives are compared.
Incremental analysis is reported.
Major outcomes are presented in a disaggregated as well as aggregated form.
The answer to the study question is given.
Conclusions follow from the data reported.
Conclusions are accompanied by the appropriate caveats.
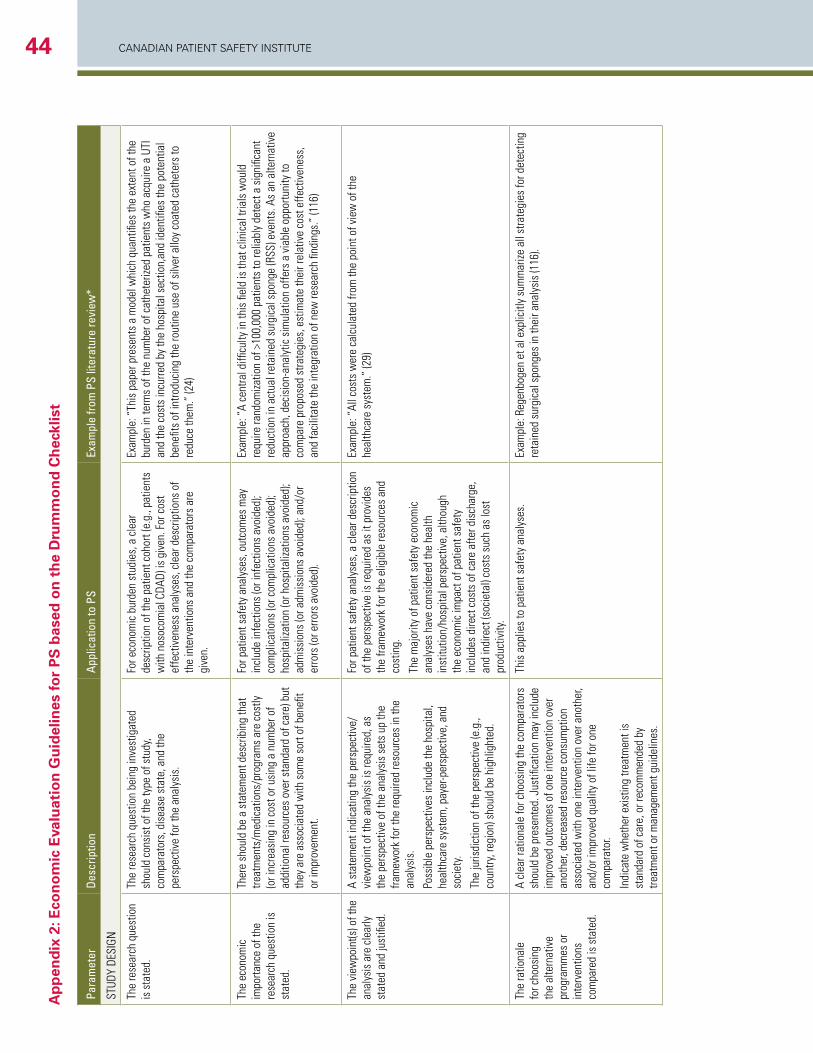
CANADIAN PAtIeNt SAfety INStItUte44A
pp
end
ix 2
: Eco
no
mic
Eva
luat
ion
Gu
idel
ines
for
PS
bas
ed o
n t
he
Dru
mm
on
d C
hec
klis
t
Para
met
erDe
scrip
tion
Appl
icat
ion
to P
SEx
ampl
e fro
m P
S lit
erat
ure
revi
ew*
STUD
Y DE
SIGN
The
rese
arch
que
stio
n is
sta
ted.
The
rese
arch
que
stio
n be
ing
inve
stig
ated
sh
ould
con
sist
of t
he ty
pe o
f stu
dy,
com
para
tors
, dis
ease
sta
te, a
nd th
e pe
rspe
ctiv
e fo
r the
ana
lysi
s.
For e
cono
mic
bur
den
stud
ies,
a c
lear
de
scrip
tion
of th
e pa
tient
coh
ort (
e.g.
, pat
ient
s w
ith n
osoc
omia
l CDA
D) is
giv
en. F
or c
ost
effe
ctiv
enes
s an
alys
es, c
lear
des
crip
tions
of
the
inte
rven
tions
and
the
com
para
tors
are
gi
ven.
Exam
ple:
“Th
is p
aper
pre
sent
s a
mod
el w
hich
qua
ntifi
es th
e ex
tent
of t
he
burd
en in
term
s of
the
num
ber o
f cat
hete
rized
pat
ient
s w
ho a
cqui
re a
UTI
an
d th
e co
sts
incu
rred
by th
e ho
spita
l sec
tion,
and
iden
tifies
the
pote
ntia
l be
nefit
s of
intro
duci
ng th
e ro
utin
e us
e of
silv
er a
lloy
coat
ed c
athe
ters
to
redu
ce th
em.”
(24)
The
econ
omic
im
porta
nce
of th
e re
sear
ch q
uest
ion
is
stat
ed.
Ther
e sh
ould
be
a st
atem
ent d
escr
ibin
g th
at
treat
men
ts/m
edic
atio
ns/p
rogr
ams
are
cost
ly
(or i
ncre
asin
g in
cos
t or u
sing
a n
umbe
r of
addi
tiona
l res
ourc
es o
ver s
tand
ard
of c
are)
but
th
ey a
re a
ssoc
iate
d w
ith s
ome
sort
of b
enefi
t or
impr
ovem
ent.
For p
atie
nt s
afet
y an
alys
es, o
utco
mes
may
in
clud
e in
fect
ions
(or i
nfec
tions
avo
ided
); co
mpl
icat
ions
(or c
ompl
icat
ions
avo
ided
); ho
spita
lizat
ion
(or h
ospi
taliz
atio
ns a
void
ed);
adm
issi
ons
(or a
dmis
sion
s av
oide
d); a
nd/o
r er
rors
(or e
rrors
avo
ided
).
Exam
ple:
“A
cent
ral d
ifficu
lty in
this
fiel
d is
that
clin
ical
tria
ls w
ould
re
quire
rand
omiza
tion
of >
100,
000
patie
nts
to re
liabl
y de
tect
a s
igni
fican
t re
duct
ion
in a
ctua
l ret
aine
d su
rgic
al s
pong
e (R
SS) e
vent
s. A
s an
alte
rnat
ive
appr
oach
, dec
isio
n-an
alyt
ic s
imul
atio
n of
fers
a v
iabl
e op
portu
nity
to
com
pare
pro
pose
d st
rate
gies
, est
imat
e th
eir r
elat
ive
cost
effe
ctiv
enes
s,
and
faci
litat
e th
e in
tegr
atio
n of
new
rese
arch
find
ings
.” (1
16)
The
view
poin
t(s) o
f the
an
alys
is a
re c
lear
ly
stat
ed a
nd ju
stifi
ed.
A st
atem
ent i
ndic
atin
g th
e pe
rspe
ctiv
e/vi
ewpo
int o
f the
ana
lysi
s is
requ
ired,
as
the
pers
pect
ive
of th
e an
alys
is s
ets
up th
e fra
mew
ork
for t
he re
quire
d re
sour
ces
in th
e an
alys
is.
Poss
ible
per
spec
tives
incl
ude
the
hosp
ital,
heal
thca
re s
yste
m, p
ayer
-per
spec
tive,
and
so
ciet
y.
The
juris
dict
ion
of th
e pe
rspe
ctiv
e (e
.g.,
coun
try, r
egio
n) s
houl
d be
hig
hlig
hted
.
For p
atie
nt s
afet
y an
alys
es, a
cle
ar d
escr
iptio
n of
the
pers
pect
ive
is re
quire
d as
it p
rovi
des
the
fram
ewor
k fo
r the
elig
ible
reso
urce
s an
d co
stin
g.
The
maj
ority
of p
atie
nt s
afet
y ec
onom
ic
anal
yses
hav
e co
nsid
ered
the
heal
th
inst
itutio
n/ho
spita
l per
spec
tive,
alth
ough
th
e ec
onom
ic im
pact
of p
atie
nt s
afet
y in
clud
es d
irect
cos
ts o
f car
e af
ter d
isch
arge
, an
d in
dire
ct (s
ocie
tal)
cost
s su
ch a
s lo
st
prod
uctiv
ity.
Exam
ple:
“Al
l cos
ts w
ere
calc
ulat
ed fr
om th
e po
int o
f vie
w o
f the
he
alth
care
sys
tem
.” (2
9)
The
ratio
nale
fo
r cho
osin
g th
e al
tern
ativ
e pr
ogra
mm
es o
r in
terv
entio
ns
com
pare
d is
sta
ted.
A cl
ear r
atio
nale
for c
hoos
ing
the
com
para
tors
sh
ould
be
pres
ente
d. J
ustifi
catio
n m
ay in
clud
e im
prov
ed o
utco
mes
of o
ne in
terv
entio
n ov
er
anot
her,
decr
ease
d re
sour
ce c
onsu
mpt
ion
asso
ciat
ed w
ith o
ne in
terv
entio
n ov
er a
noth
er,
and/
or im
prov
ed q
ualit
y of
life
for o
ne
com
para
tor.
Indi
cate
whe
ther
exi
stin
g tre
atm
ent i
s st
anda
rd o
f car
e, o
r rec
omm
ende
d by
tre
atm
ent o
r man
agem
ent g
uide
lines
.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
Reg
enbo
gen
et a
l exp
licitl
y su
mm
arize
all
stra
tegi
es fo
r det
ectin
g re
tain
ed s
urgi
cal s
pong
es in
thei
r ana
lysi
s (1
16).
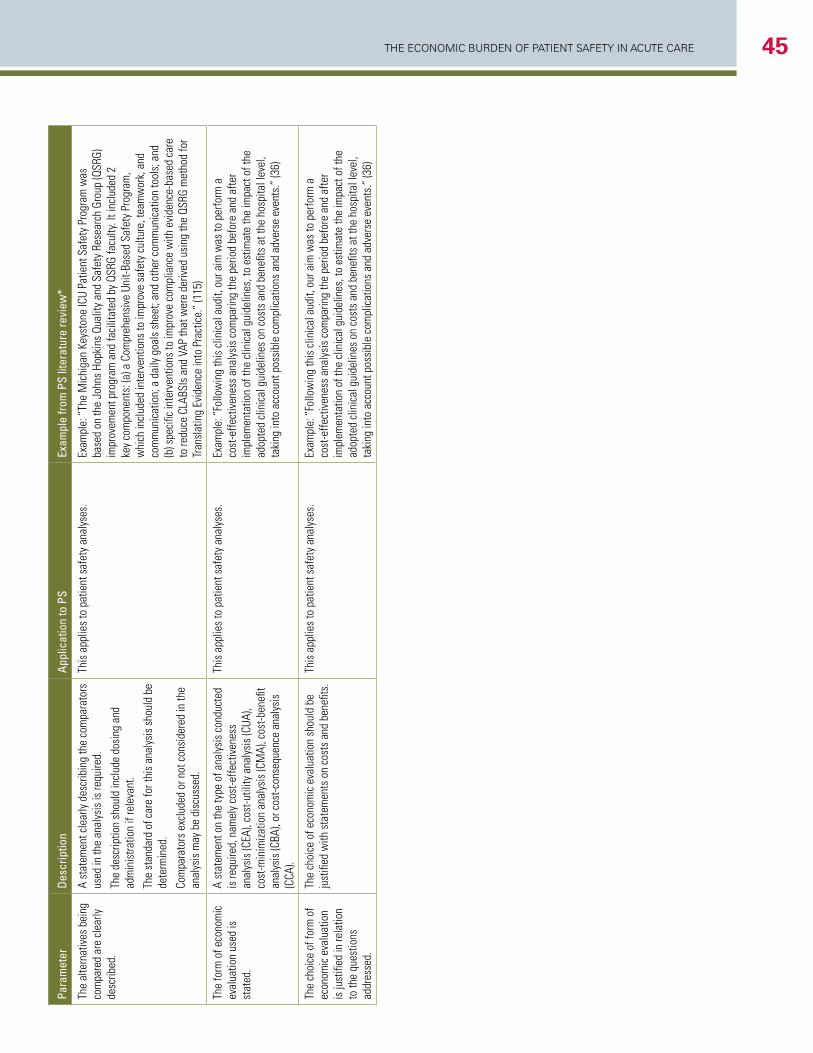
The economic Burden of PaTienT SafeTy in acuTe care 45Pa
ram
eter
Desc
riptio
nAp
plic
atio
n to
PS
Exam
ple
from
PS
liter
atur
e re
view
*
The
alte
rnat
ives
bei
ng
com
pare
d ar
e cl
early
de
scrib
ed.
A st
atem
ent c
lear
ly d
escr
ibin
g th
e co
mpa
rato
rs
used
in th
e an
alys
is is
requ
ired.
The
desc
riptio
n sh
ould
incl
ude
dosi
ng a
nd
adm
inis
tratio
n if
rele
vant
.
The
stan
dard
of c
are
for t
his
anal
ysis
sho
uld
be
dete
rmin
ed.
Com
para
tors
exc
lude
d or
not
con
side
red
in th
e an
alys
is m
ay b
e di
scus
sed.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Th
e M
ichi
gan
Keys
tone
ICU
Patie
nt S
afet
y Pr
ogra
m w
as
base
d on
the
John
s Ho
pkin
s Qu
ality
and
Saf
ety
Rese
arch
Gro
up (Q
SRG)
im
prov
emen
t pro
gram
and
faci
litat
ed b
y QS
RG fa
culty
. It i
nclu
ded
2 ke
y co
mpo
nent
s: (a
) a C
ompr
ehen
sive
Uni
t-Bas
ed S
afet
y Pr
ogra
m,
whi
ch in
clud
ed in
terv
entio
ns to
impr
ove
safe
ty c
ultu
re, t
eam
wor
k, a
nd
com
mun
icat
ion;
a d
aily
goa
ls s
heet
; and
oth
er c
omm
unic
atio
n to
ols;
and
(b
) spe
cific
inte
rven
tions
to im
prov
e co
mpl
ianc
e w
ith e
vide
nce-
base
d ca
re
to re
duce
CLA
BSIs
and
VAP
that
wer
e de
rived
usi
ng th
e QS
RG m
etho
d fo
r Tr
ansl
atin
g Ev
iden
ce in
to P
ract
ice.
” (1
15)
The
form
of e
cono
mic
ev
alua
tion
used
is
stat
ed.
A st
atem
ent o
n th
e ty
pe o
f ana
lysi
s co
nduc
ted
is re
quire
d, n
amel
y co
st-e
ffect
iven
ess
anal
ysis
(CEA
), co
st-u
tility
ana
lysi
s (C
UA),
cost
-min
imiza
tion
anal
ysis
(CM
A), c
ost-b
enefi
t an
alys
is (C
BA),
or c
ost-c
onse
quen
ce a
naly
sis
(CCA
).
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Fo
llow
ing
this
clin
ical
aud
it, o
ur a
im w
as to
per
form
a
cost
-effe
ctiv
enes
s an
alys
is c
ompa
ring
the
perio
d be
fore
and
afte
r im
plem
enta
tion
of th
e cl
inic
al g
uide
lines
, to
estim
ate
the
impa
ct o
f the
ad
opte
d cl
inic
al g
uide
lines
on
cost
s an
d be
nefit
s at
the
hosp
ital l
evel
, ta
king
into
acc
ount
pos
sibl
e co
mpl
icat
ions
and
adv
erse
eve
nts.
” (3
6)
The
choi
ce o
f for
m o
f ec
onom
ic e
valu
atio
n is
just
ified
in re
latio
n to
the
ques
tions
ad
dres
sed.
The
choi
ce o
f eco
nom
ic e
valu
atio
n sh
ould
be
just
ified
with
sta
tem
ents
on
cost
s an
d be
nefit
s.Th
is a
pplie
s to
pat
ient
saf
ety
anal
yses
.Ex
ampl
e: “
Follo
win
g th
is c
linic
al a
udit,
our
aim
was
to p
erfo
rm a
co
st-e
ffect
iven
ess
anal
ysis
com
parin
g th
e pe
riod
befo
re a
nd a
fter
impl
emen
tatio
n of
the
clin
ical
gui
delin
es, t
o es
timat
e th
e im
pact
of t
he
adop
ted
clin
ical
gui
delin
es o
n co
sts
and
bene
fits
at th
e ho
spita
l lev
el,
taki
ng in
to a
ccou
nt p
ossi
ble
com
plic
atio
ns a
nd a
dver
se e
vent
s.”
(36)
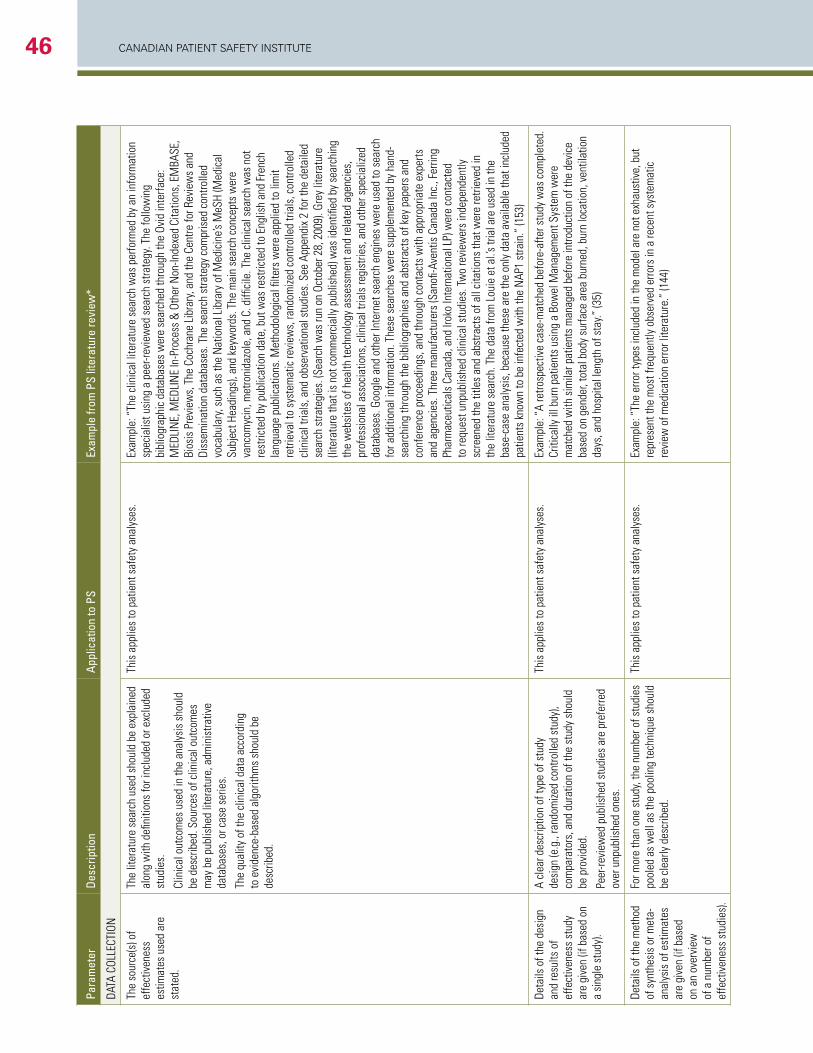
CANADIAN PAtIeNt SAfety INStItUte46
Para
met
erDe
scrip
tion
Appl
icat
ion
to P
SEx
ampl
e fro
m P
S lit
erat
ure
revi
ew*
DATA
COL
LECT
ION
The
sour
ce(s
) of
effe
ctiv
enes
s es
timat
es u
sed
are
stat
ed.
The
liter
atur
e se
arch
use
d sh
ould
be
expl
aine
d al
ong
with
defi
nitio
ns fo
r inc
lude
d or
exc
lude
d st
udie
s.
Clin
ical
out
com
es u
sed
in th
e an
alys
is s
houl
d be
des
crib
ed. S
ourc
es o
f clin
ical
out
com
es
may
be
publ
ishe
d lit
erat
ure,
adm
inis
trativ
e da
taba
ses,
or c
ase
serie
s.
The
qual
ity o
f the
clin
ical
dat
a ac
cord
ing
to e
vide
nce-
base
d al
gorit
hms
shou
ld b
e de
scrib
ed.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Th
e cl
inic
al li
tera
ture
sea
rch
was
per
form
ed b
y an
info
rmat
ion
spec
ialis
t usi
ng a
pee
r-rev
iew
ed s
earc
h st
rate
gy. T
he fo
llow
ing
bibl
iogr
aphi
c da
taba
ses
wer
e se
arch
ed th
roug
h th
e Ov
id in
terfa
ce:
MED
LIN
E, M
EDLI
NE
In-P
roce
ss &
Oth
er N
on-In
dexe
d Ci
tatio
ns, E
MBA
SE,
Bios
is P
revi
ews,
The
Coc
hran
e Li
brar
y, an
d th
e Ce
ntre
for R
evie
ws
and
Diss
emin
atio
n da
taba
ses.
The
sea
rch
stra
tegy
com
pris
ed c
ontro
lled
voca
bula
ry, s
uch
as th
e N
atio
nal L
ibra
ry o
f Med
icin
e’s M
eSH
(Med
ical
Su
bjec
t Hea
ding
s), a
nd k
eyw
ords
. The
mai
n se
arch
con
cept
s w
ere
vanc
omyc
in, m
etro
nida
zole
, and
C. d
iffici
le. T
he c
linic
al s
earc
h w
as n
ot
rest
ricte
d by
pub
licat
ion
date
, but
was
rest
ricte
d to
Eng
lish
and
Fren
ch
lang
uage
pub
licat
ions
. Met
hodo
logi
cal fi
lters
wer
e ap
plie
d to
lim
it re
triev
al to
sys
tem
atic
revi
ews,
rand
omize
d co
ntro
lled
trial
s, c
ontro
lled
clin
ical
tria
ls, a
nd o
bser
vatio
nal s
tudi
es. S
ee A
ppen
dix
2 fo
r the
det
aile
d se
arch
stra
tegi
es. (
Sear
ch w
as ru
n on
Oct
ober
28,
200
9). G
rey
liter
atur
e (li
tera
ture
that
is n
ot c
omm
erci
ally
pub
lishe
d) w
as id
entifi
ed b
y se
arch
ing
the
web
site
s of
hea
lth te
chno
logy
ass
essm
ent a
nd re
late
d ag
enci
es,
prof
essi
onal
ass
ocia
tions
, clin
ical
tria
ls re
gist
ries,
and
oth
er s
peci
alize
d da
taba
ses.
Goo
gle
and
othe
r Int
erne
t sea
rch
engi
nes
wer
e us
ed to
sea
rch
for a
dditi
onal
info
rmat
ion.
The
se s
earc
hes
wer
e su
pple
men
ted
by h
and-
sear
chin
g th
roug
h th
e bi
blio
grap
hies
and
abs
tract
s of
key
pap
ers
and
conf
eren
ce p
roce
edin
gs, a
nd th
roug
h co
ntac
ts w
ith a
ppro
pria
te e
xper
ts
and
agen
cies
. Thr
ee m
anuf
actu
rers
(San
ofi-A
vent
is C
anad
a In
c., F
errin
g Ph
arm
aceu
tical
s Ca
nada
, and
Irok
o In
tern
atio
nal L
P) w
ere
cont
acte
d to
requ
est u
npub
lishe
d cl
inic
al s
tudi
es. T
wo
revi
ewer
s in
depe
nden
tly
scre
ened
the
title
s an
d ab
stra
cts
of a
ll ci
tatio
ns th
at w
ere
retri
eved
in
the
liter
atur
e se
arch
. The
dat
a fro
m L
ouie
et a
l.’s tr
ial a
re u
sed
in th
e ba
se-c
ase
anal
ysis
, bec
ause
thes
e ar
e th
e on
ly d
ata
avai
labl
e th
at in
clud
ed
patie
nts
know
n to
be
infe
cted
with
the
NAP
1 st
rain
.” (1
53)
Deta
ils o
f the
des
ign
and
resu
lts o
f ef
fect
iven
ess
stud
y ar
e gi
ven
(if b
ased
on
a si
ngle
stu
dy).
A cl
ear d
escr
iptio
n of
type
of s
tudy
de
sign
(e.g
., ra
ndom
ized
cont
rolle
d st
udy)
, co
mpa
rato
rs, a
nd d
urat
ion
of th
e st
udy
shou
ld
be p
rovi
ded.
Peer
-revi
ewed
pub
lishe
d st
udie
s ar
e pr
efer
red
over
unp
ublis
hed
ones
.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“A
retro
spec
tive
case
-mat
ched
bef
ore-
afte
r stu
dy w
as c
ompl
eted
. Cr
itica
lly il
l bur
n pa
tient
s us
ing
a Bo
wel
Man
agem
ent S
yste
m w
ere
mat
ched
with
sim
ilar p
atie
nts
man
aged
bef
ore
intro
duct
ion
of th
e de
vice
ba
sed
on g
ende
r, to
tal b
ody
surfa
ce a
rea
burn
ed, b
urn
loca
tion,
ven
tilat
ion
days
, and
hos
pita
l len
gth
of s
tay.”
(35)
Deta
ils o
f the
met
hod
of s
ynth
esis
or m
eta-
anal
ysis
of e
stim
ates
ar
e gi
ven
(if b
ased
on
an
over
view
of
a n
umbe
r of
effe
ctiv
enes
s st
udie
s).
For m
ore
than
one
stu
dy, t
he n
umbe
r of s
tudi
es
pool
ed a
s w
ell a
s th
e po
olin
g te
chni
que
shou
ld
be c
lear
ly d
escr
ibed
.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Th
e er
ror t
ypes
incl
uded
in th
e m
odel
are
not
exh
aust
ive,
but
re
pres
ent t
he m
ost f
requ
ently
obs
erve
d er
rors
in a
rece
nt s
yste
mat
ic
revi
ew o
f med
icat
ion
erro
r lite
ratu
re.”
(144
)
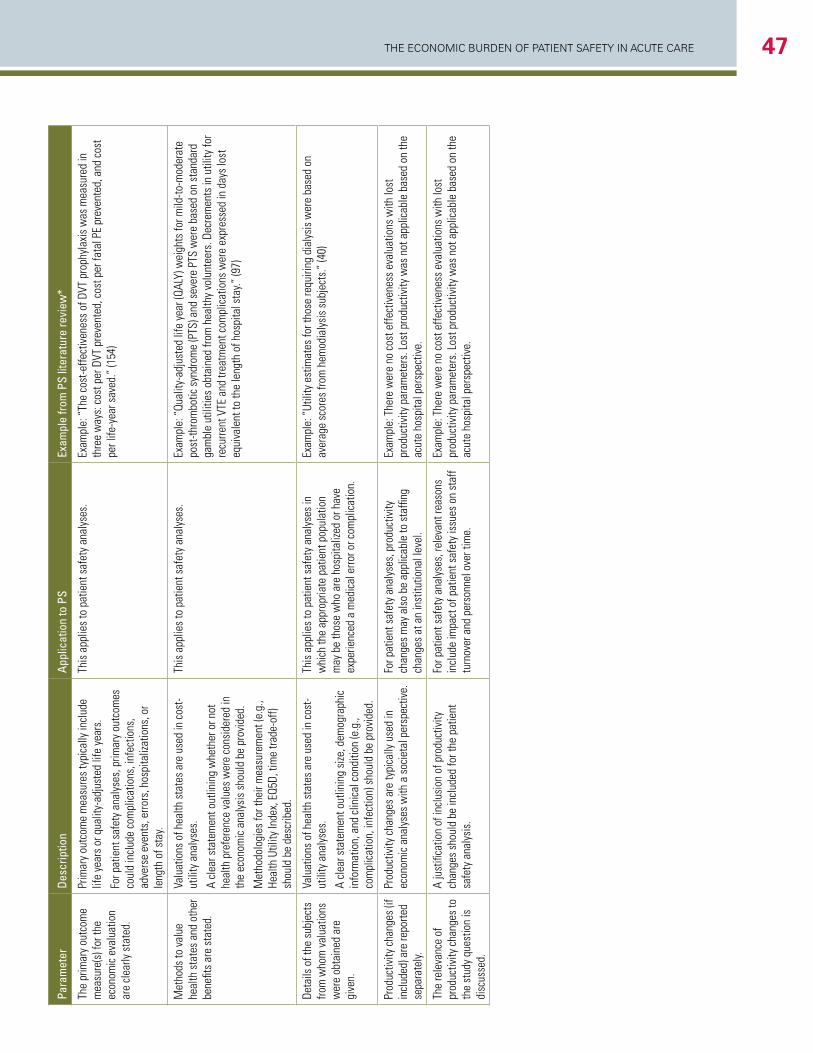
The economic Burden of PaTienT SafeTy in acuTe care 47Pa
ram
eter
Desc
riptio
nAp
plic
atio
n to
PS
Exam
ple
from
PS
liter
atur
e re
view
*
The
prim
ary
outc
ome
mea
sure
(s) f
or th
e ec
onom
ic e
valu
atio
n ar
e cl
early
sta
ted.
Prim
ary
outc
ome
mea
sure
s ty
pica
lly in
clud
e lif
e ye
ars
or q
ualit
y-ad
just
ed li
fe y
ears
.
For p
atie
nt s
afet
y an
alys
es, p
rimar
y ou
tcom
es
coul
d in
clud
e co
mpl
icat
ions
, inf
ectio
ns,
adve
rse
even
ts, e
rrors
, hos
pita
lizat
ions
, or
leng
th o
f sta
y.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Th
e co
st-e
ffect
iven
ess
of D
VT p
roph
ylax
is w
as m
easu
red
in
thre
e w
ays:
cos
t per
DVT
pre
vent
ed, c
ost p
er fa
tal P
E pr
even
ted,
and
cos
t pe
r life
-yea
r sav
ed.”
(154
)
Met
hods
to v
alue
he
alth
sta
tes
and
othe
r be
nefit
s ar
e st
ated
.
Valu
atio
ns o
f hea
lth s
tate
s ar
e us
ed in
cos
t-ut
ility
ana
lyse
s.
A cl
ear s
tate
men
t out
linin
g w
heth
er o
r not
he
alth
pre
fere
nce
valu
es w
ere
cons
ider
ed in
th
e ec
onom
ic a
naly
sis
shou
ld b
e pr
ovid
ed.
Met
hodo
logi
es fo
r the
ir m
easu
rem
ent (
e.g.
, He
alth
Util
ity In
dex,
EQ5
D, ti
me
trade
-off)
sh
ould
be
desc
ribed
.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Qu
ality
-adj
uste
d lif
e ye
ar (Q
ALY)
wei
ghts
for m
ild-to
-mod
erat
e po
st-th
rom
botic
syn
drom
e (P
TS) a
nd s
ever
e PT
S w
ere
base
d on
sta
ndar
d ga
mbl
e ut
ilitie
s ob
tain
ed fr
om h
ealth
y vo
lunt
eers
. Dec
rem
ents
in u
tility
for
recu
rrent
VTE
and
trea
tmen
t com
plic
atio
ns w
ere
expr
esse
d in
day
s lo
st
equi
vale
nt to
the
leng
th o
f hos
pita
l sta
y.” (9
7)
Deta
ils o
f the
sub
ject
s fro
m w
hom
val
uatio
ns
wer
e ob
tain
ed a
re
give
n.
Valu
atio
ns o
f hea
lth s
tate
s ar
e us
ed in
cos
t-ut
ility
ana
lyse
s.
A cl
ear s
tate
men
t out
linin
g si
ze, d
emog
raph
ic
info
rmat
ion,
and
clin
ical
con
ditio
n (e
.g.,
com
plic
atio
n, in
fect
ion)
sho
uld
be p
rovi
ded.
This
app
lies
to p
atie
nt s
afet
y an
alys
es in
w
hich
the
appr
opria
te p
atie
nt p
opul
atio
n m
ay b
e th
ose
who
are
hos
pita
lized
or h
ave
expe
rienc
ed a
med
ical
erro
r or c
ompl
icat
ion.
Exam
ple:
“Ut
ility
est
imat
es fo
r tho
se re
quiri
ng d
ialy
sis
wer
e ba
sed
on
aver
age
scor
es fr
om h
emod
ialy
sis
subj
ects
.” (4
0)
Prod
uctiv
ity c
hang
es (i
f in
clud
ed) a
re re
porte
d se
para
tely.
Prod
uctiv
ity c
hang
es a
re ty
pica
lly u
sed
in
econ
omic
ana
lyse
s w
ith a
soc
ieta
l per
spec
tive.
Fo
r pat
ient
saf
ety
anal
yses
, pro
duct
ivity
ch
ange
s m
ay a
lso
be a
pplic
able
to s
taffi
ng
chan
ges
at a
n in
stitu
tiona
l lev
el.
Exam
ple:
The
re w
ere
no c
ost e
ffect
iven
ess
eval
uatio
ns w
ith lo
st
prod
uctiv
ity p
aram
eter
s. L
ost p
rodu
ctiv
ity w
as n
ot a
pplic
able
bas
ed o
n th
e ac
ute
hosp
ital p
ersp
ectiv
e.
The
rele
vanc
e of
pr
oduc
tivity
cha
nges
to
the
stud
y qu
estio
n is
di
scus
sed.
A ju
stifi
catio
n of
incl
usio
n of
pro
duct
ivity
ch
ange
s sh
ould
be
incl
uded
for t
he p
atie
nt
safe
ty a
naly
sis.
For p
atie
nt s
afet
y an
alys
es, r
elev
ant r
easo
ns
incl
ude
impa
ct o
f pat
ient
saf
ety
issu
es o
n st
aff
turn
over
and
per
sonn
el o
ver t
ime.
Exam
ple:
The
re w
ere
no c
ost e
ffect
iven
ess
eval
uatio
ns w
ith lo
st
prod
uctiv
ity p
aram
eter
s. L
ost p
rodu
ctiv
ity w
as n
ot a
pplic
able
bas
ed o
n th
e ac
ute
hosp
ital p
ersp
ectiv
e.
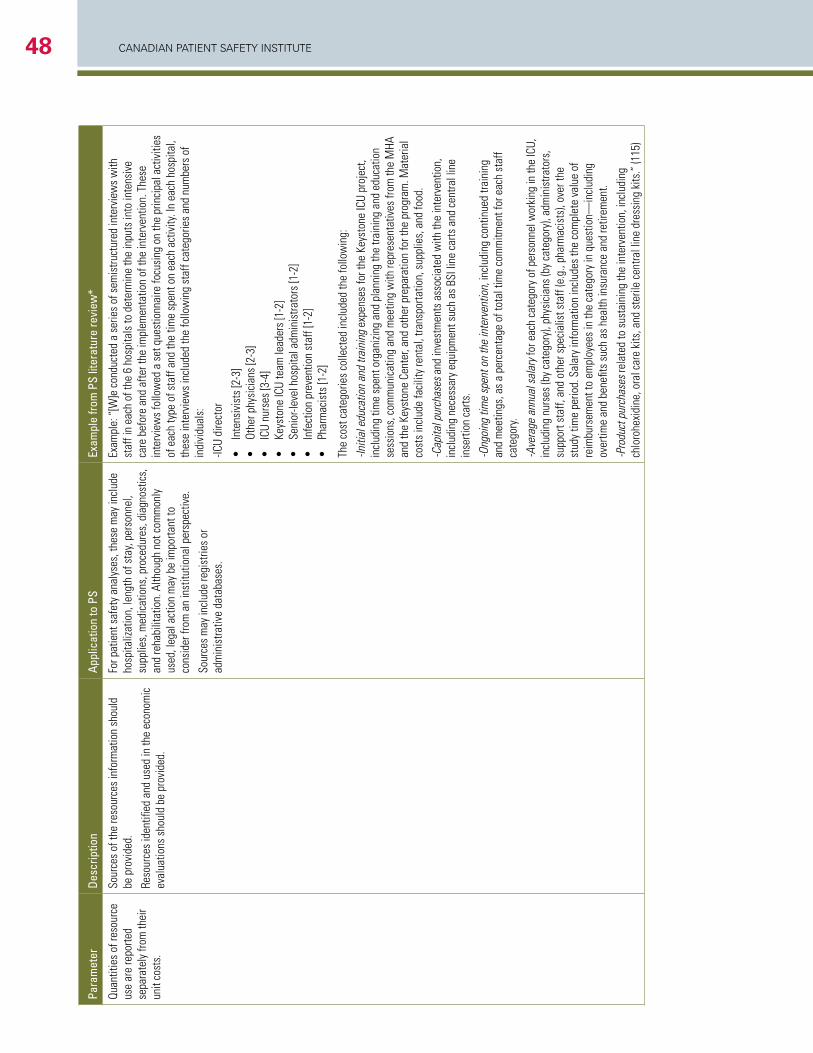
CANADIAN PAtIeNt SAfety INStItUte48
Para
met
erDe
scrip
tion
Appl
icat
ion
to P
SEx
ampl
e fro
m P
S lit
erat
ure
revi
ew*
Quan
titie
s of
reso
urce
us
e ar
e re
porte
d se
para
tely
from
thei
r un
it co
sts.
Sour
ces
of th
e re
sour
ces
info
rmat
ion
shou
ld
be p
rovi
ded.
Reso
urce
s id
entifi
ed a
nd u
sed
in th
e ec
onom
ic
eval
uatio
ns s
houl
d be
pro
vide
d.
For p
atie
nt s
afet
y an
alys
es, t
hese
may
incl
ude
hosp
italiz
atio
n, le
ngth
of s
tay,
pers
onne
l, su
pplie
s, m
edic
atio
ns, p
roce
dure
s, d
iagn
ostic
s,
and
reha
bilit
atio
n. A
lthou
gh n
ot c
omm
only
us
ed, l
egal
act
ion
may
be
impo
rtant
to
cons
ider
from
an
inst
itutio
nal p
ersp
ectiv
e.
Sour
ces
may
incl
ude
regi
strie
s or
ad
min
istra
tive
data
base
s.
Exam
ple:
“[W
]e c
ondu
cted
a s
erie
s of
sem
istru
ctur
ed in
terv
iew
s w
ith
staf
f in
each
of t
he 6
hos
pita
ls to
det
erm
ine
the
inpu
ts in
to in
tens
ive
care
bef
ore
and
afte
r the
impl
emen
tatio
n of
the
inte
rven
tion.
The
se
inte
rvie
ws
follo
wed
a s
et q
uest
ionn
aire
focu
sing
on
the
prin
cipa
l act
iviti
es
of e
ach
type
of s
taff
and
the
time
spen
t on
each
act
ivity
. In
each
hos
pita
l, th
ese
inte
rvie
ws
incl
uded
the
follo
win
g st
aff c
ateg
orie
s an
d nu
mbe
rs o
f in
divi
dual
s:
-ICU
dire
ctor
•
Inte
nsiv
ists
[2-3
]•
Ot
her p
hysi
cian
s [2
-3]
•
ICU
nurs
es [3
-4]
•
Keys
tone
ICU
team
lead
ers
[1-2
]•
Se
nior
-leve
l hos
pita
l adm
inis
trato
rs [1
-2]
•
Infe
ctio
n pr
even
tion
staf
f [1-
2]•
Ph
arm
acis
ts [1
-2]
The
cost
cat
egor
ies
colle
cted
incl
uded
the
follo
win
g:
-Initi
al e
duca
tion
and
train
ing
expe
nses
for t
he K
eyst
one
ICU
proj
ect,
incl
udin
g tim
e sp
ent o
rgan
izing
and
pla
nnin
g th
e tra
inin
g an
d ed
ucat
ion
sess
ions
, com
mun
icat
ing
and
mee
ting
with
repr
esen
tativ
es fr
om th
e M
HA
and
the
Keys
tone
Cen
ter,
and
othe
r pre
para
tion
for t
he p
rogr
am. M
ater
ial
cost
s in
clud
e fa
cilit
y re
ntal
, tra
nspo
rtatio
n, s
uppl
ies,
and
food
.
-Cap
ital p
urch
ases
and
inve
stm
ents
ass
ocia
ted
with
the
inte
rven
tion,
in
clud
ing
nece
ssar
y eq
uipm
ent s
uch
as B
SI li
ne c
arts
and
cen
tral l
ine
inse
rtion
car
ts.
-Ong
oing
tim
e sp
ent o
n th
e in
terv
entio
n, in
clud
ing
cont
inue
d tra
inin
g an
d m
eetin
gs, a
s a
perc
enta
ge o
f tot
al ti
me
com
mitm
ent f
or e
ach
staf
f ca
tego
ry.
-Ave
rage
ann
ual s
alar
y fo
r eac
h ca
tego
ry o
f per
sonn
el w
orki
ng in
the
ICU,
in
clud
ing
nurs
es (b
y ca
tego
ry),
phys
icia
ns (b
y ca
tego
ry),
adm
inis
trato
rs,
supp
ort s
taff,
and
oth
er s
peci
alis
t sta
ff (e
.g.,
phar
mac
ists
), ov
er th
e st
udy
time
perio
d. S
alar
y in
form
atio
n in
clud
es th
e co
mpl
ete
valu
e of
re
imbu
rsem
ent t
o em
ploy
ees
in th
e ca
tego
ry in
que
stio
n—in
clud
ing
over
time
and
bene
fits
such
as
heal
th in
sura
nce
and
retir
emen
t.
-Pro
duct
pur
chas
es re
late
d to
sus
tain
ing
the
inte
rven
tion,
incl
udin
g ch
loro
hexi
dine
, ora
l car
e ki
ts, a
nd s
teril
e ce
ntra
l lin
e dr
essi
ng k
its.”
(115
)
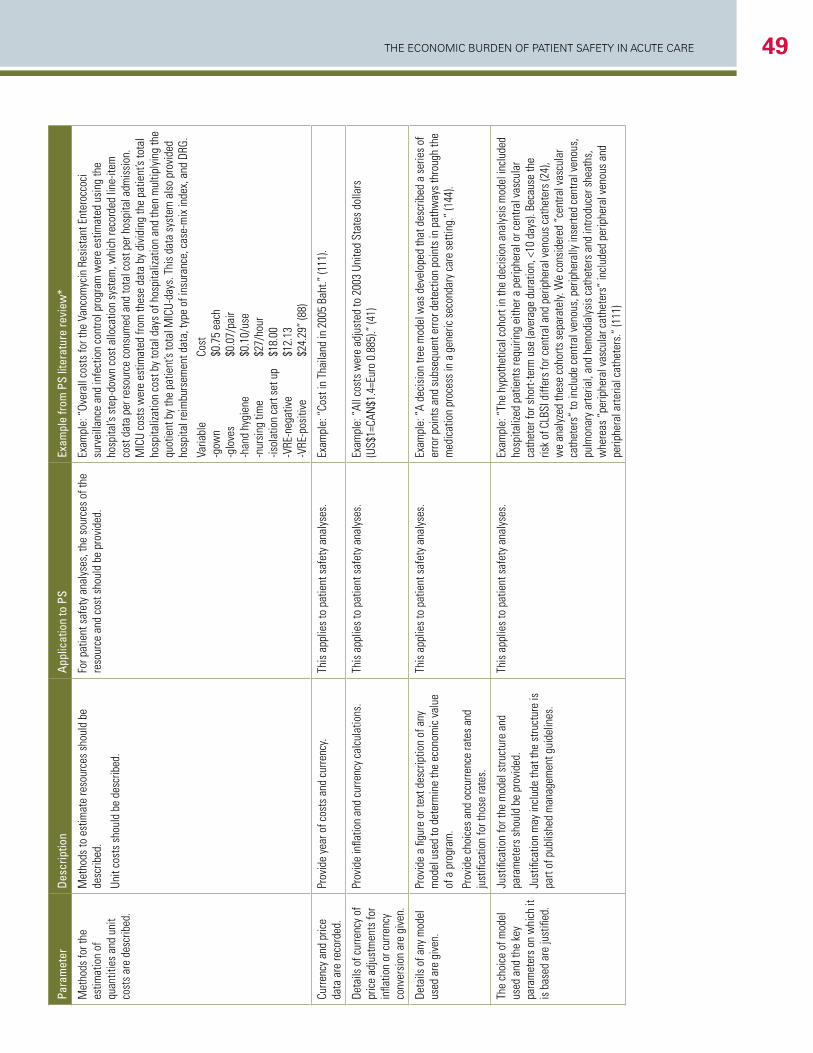
The economic Burden of PaTienT SafeTy in acuTe care 49Pa
ram
eter
Desc
riptio
nAp
plic
atio
n to
PS
Exam
ple
from
PS
liter
atur
e re
view
*
Met
hods
for t
he
estim
atio
n of
qu
antit
ies
and
unit
cost
s ar
e de
scrib
ed.
Met
hods
to e
stim
ate
reso
urce
s sh
ould
be
desc
ribed
.
Unit
cost
s sh
ould
be
desc
ribed
.
For p
atie
nt s
afet
y an
alys
es, t
he s
ourc
es o
f the
re
sour
ce a
nd c
ost s
houl
d be
pro
vide
d.Ex
ampl
e: “
Over
all c
osts
for t
he V
anco
myc
in R
esis
tant
Ent
eroc
coci
su
rvei
llanc
e an
d in
fect
ion
cont
rol p
rogr
am w
ere
estim
ated
usi
ng th
e ho
spita
l’s s
tep-
dow
n co
st a
lloca
tion
syst
em, w
hich
reco
rded
line
-item
co
st d
ata
per r
esou
rce
cons
umed
and
tota
l cos
t per
hos
pita
l adm
issi
on.
MIC
U co
sts
wer
e es
timat
ed fr
om th
ese
data
by
divi
ding
the
patie
nt’s
tota
l ho
spita
lizat
ion
cost
by
tota
l day
s of
hos
pita
lizat
ion
and
then
mul
tiply
ing
the
quot
ient
by
the
patie
nt’s
tota
l MIC
U-da
ys. T
his
data
sys
tem
als
o pr
ovid
ed
hosp
ital r
eim
burs
emen
t dat
a, ty
pe o
f ins
uran
ce, c
ase-
mix
inde
x, a
nd D
RG.
Varia
ble
Co
st-g
own
$0
.75
each
-glo
ves
$0
.07/
pair
-han
d hy
gien
e
$0.1
0/us
e-n
ursi
ng ti
me
$2
7/ho
ur-is
olat
ion
cart
set u
p
$18.
00-V
RE-n
egat
ive
$1
2.13
-VRE
-pos
itive
$2
4.29
” (8
8)
Curre
ncy
and
pric
e da
ta a
re re
cord
ed.
Prov
ide
year
of c
osts
and
cur
renc
y.Th
is a
pplie
s to
pat
ient
saf
ety
anal
yses
.Ex
ampl
e: “
Cost
in T
haila
nd in
200
5 Ba
ht.”
(111
).
Deta
ils o
f cur
renc
y of
pr
ice
adju
stm
ents
for
infla
tion
or c
urre
ncy
conv
ersi
on a
re g
iven
.
Prov
ide
infla
tion
and
curre
ncy
calc
ulat
ions
.Th
is a
pplie
s to
pat
ient
saf
ety
anal
yses
.Ex
ampl
e: “
All c
osts
wer
e ad
just
ed to
200
3 Un
ited
Stat
es d
olla
rs
(US$
1=CA
N$1
.4=E
uro
0.88
5).”
(41)
Deta
ils o
f any
mod
el
used
are
giv
en.
Prov
ide
a fig
ure
or te
xt d
escr
iptio
n of
any
m
odel
use
d to
det
erm
ine
the
econ
omic
val
ue
of a
pro
gram
.
Prov
ide
choi
ces
and
occu
rrenc
e ra
tes
and
just
ifica
tion
for t
hose
rate
s.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“A
deci
sion
tree
mod
el w
as d
evel
oped
that
des
crib
ed a
ser
ies
of
erro
r poi
nts
and
subs
eque
nt e
rror d
etec
tion
poin
ts in
pat
hway
s th
roug
h th
e m
edic
atio
n pr
oces
s in
a g
ener
ic s
econ
dary
car
e se
tting
.” (1
44).
The
choi
ce o
f mod
el
used
and
the
key
para
met
ers
on w
hich
it
is b
ased
are
just
ified
.
Just
ifica
tion
for t
he m
odel
stru
ctur
e an
d pa
ram
eter
s sh
ould
be
prov
ided
.
Just
ifica
tion
may
incl
ude
that
the
stru
ctur
e is
pa
rt of
pub
lishe
d m
anag
emen
t gui
delin
es.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Th
e hy
poth
etic
al c
ohor
t in
the
deci
sion
ana
lysi
s m
odel
incl
uded
ho
spita
lized
pat
ient
s re
quiri
ng e
ither
a p
erip
hera
l or c
entra
l vas
cula
r ca
thet
er fo
r sho
rt-te
rm u
se (a
vera
ge d
urat
ion,
<10
day
s). B
ecau
se th
e ris
k of
CLB
SI d
iffer
s fo
r cen
tral a
nd p
erip
hera
l ven
ous
cath
eter
s (2
4),
we
anal
yzed
thes
e co
horts
sep
arat
ely.
We
cons
ider
ed “
cent
ral v
ascu
lar
cath
eter
s” to
incl
ude
cent
ral v
enou
s, p
erip
hera
lly in
serte
d ce
ntra
l ven
ous,
pu
lmon
ary
arte
rial,
and
hem
odia
lysi
s ca
thet
ers
and
intro
duce
r she
aths
, w
here
as “
perip
hera
l vas
cula
r cat
hete
rs”
incl
uded
per
iphe
ral v
enou
s an
d pe
riphe
ral a
rteria
l cat
hete
rs.”
(111
)
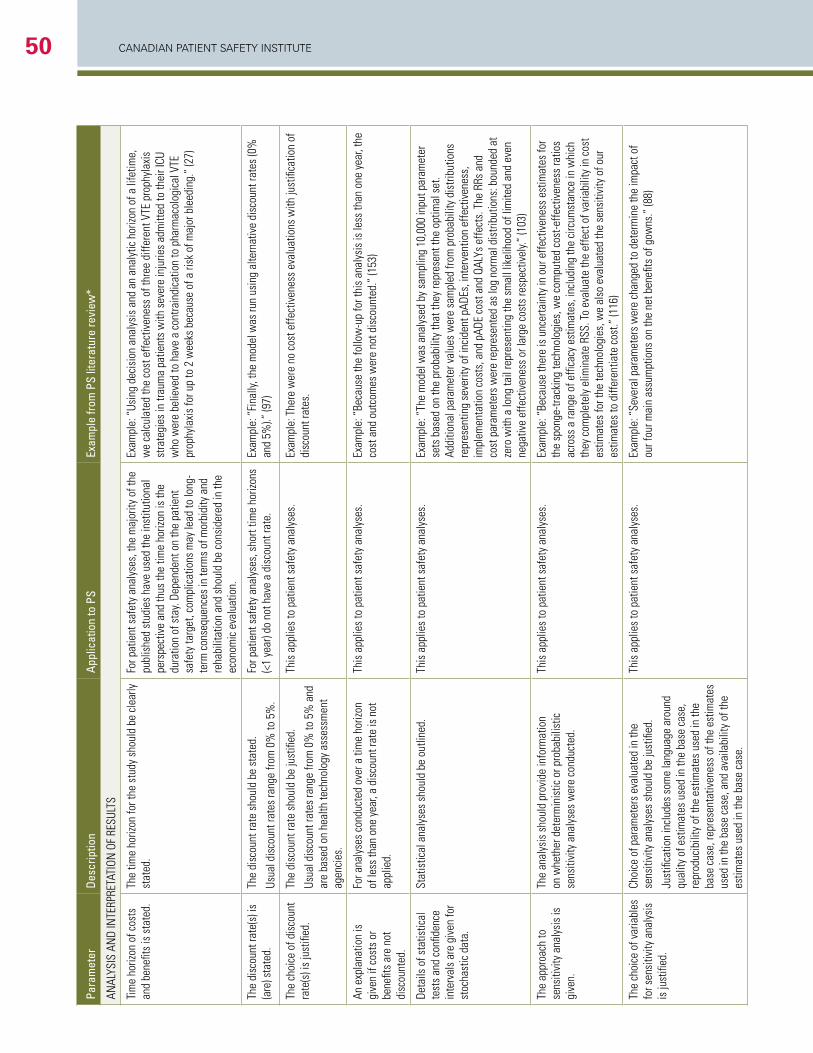
CANADIAN PAtIeNt SAfety INStItUte50
Para
met
erDe
scrip
tion
Appl
icat
ion
to P
SEx
ampl
e fro
m P
S lit
erat
ure
revi
ew*
ANAL
YSIS
AN
D IN
TERP
RETA
TION
OF
RESU
LTS
Tim
e ho
rizon
of c
osts
an
d be
nefit
s is
sta
ted.
The
time
horiz
on fo
r the
stu
dy s
houl
d be
cle
arly
st
ated
. Fo
r pat
ient
saf
ety
anal
yses
, the
maj
ority
of t
he
publ
ishe
d st
udie
s ha
ve u
sed
the
inst
itutio
nal
pers
pect
ive
and
thus
the
time
horiz
on is
the
dura
tion
of s
tay.
Depe
nden
t on
the
patie
nt
safe
ty ta
rget
, com
plic
atio
ns m
ay le
ad to
long
-te
rm c
onse
quen
ces
in te
rms
of m
orbi
dity
and
re
habi
litat
ion
and
shou
ld b
e co
nsid
ered
in th
e ec
onom
ic e
valu
atio
n.
Exam
ple:
“Us
ing
deci
sion
ana
lysi
s an
d an
ana
lytic
hor
izon
of a
life
time,
w
e ca
lcul
ated
the
cost
effe
ctiv
enes
s of
thre
e di
ffere
nt V
TE p
roph
ylax
is
stra
tegi
es in
trau
ma
patie
nts
with
sev
ere
inju
ries
adm
itted
to th
eir I
CU
who
wer
e be
lieve
d to
hav
e a
cont
rain
dica
tion
to p
harm
acol
ogic
al V
TE
prop
hyla
xis
for u
p to
2 w
eeks
bec
ause
of a
risk
of m
ajor
ble
edin
g.”
(27)
The
disc
ount
rate
(s) i
s (a
re) s
tate
d.Th
e di
scou
nt ra
te s
houl
d be
sta
ted.
Usua
l dis
coun
t rat
es ra
nge
from
0%
to 5
%.
For p
atie
nt s
afet
y an
alys
es, s
hort
time
horiz
ons
(<1
year
) do
not h
ave
a di
scou
nt ra
te.
Exam
ple:
“Fi
nally
, the
mod
el w
as ru
n us
ing
alte
rnat
ive
disc
ount
rate
s (0
%
and
5%).”
(97)
The
choi
ce o
f dis
coun
t ra
te(s
) is
just
ified
.Th
e di
scou
nt ra
te s
houl
d be
just
ified
.
Usua
l dis
coun
t rat
es ra
nge
from
0%
to 5
% a
nd
are
base
d on
hea
lth te
chno
logy
ass
essm
ent
agen
cies
.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
The
re w
ere
no c
ost e
ffect
iven
ess
eval
uatio
ns w
ith ju
stifi
catio
n of
di
scou
nt ra
tes.
An e
xpla
natio
n is
gi
ven
if co
sts
or
bene
fits
are
not
disc
ount
ed.
For a
naly
ses
cond
ucte
d ov
er a
tim
e ho
rizon
of
less
than
one
yea
r, a
disc
ount
rate
is n
ot
appl
ied.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Be
caus
e th
e fo
llow
-up
for t
his
anal
ysis
is le
ss th
an o
ne y
ear,
the
cost
and
out
com
es w
ere
not d
isco
unte
d.”
(153
)
Deta
ils o
f sta
tistic
al
test
s an
d co
nfide
nce
inte
rval
s ar
e gi
ven
for
stoc
hast
ic d
ata.
Stat
istic
al a
naly
ses
shou
ld b
e ou
tline
d.Th
is a
pplie
s to
pat
ient
saf
ety
anal
yses
.Ex
ampl
e: “
The
mod
el w
as a
naly
sed
by s
ampl
ing
10,0
00 in
put p
aram
eter
se
ts b
ased
on
the
prob
abili
ty th
at th
ey re
pres
ent t
he o
ptim
al s
et.
Addi
tiona
l par
amet
er v
alue
s w
ere
sam
pled
from
pro
babi
lity
dist
ribut
ions
re
pres
entin
g se
verit
y of
inci
dent
pAD
Es, i
nter
vent
ion
effe
ctiv
enes
s,
impl
emen
tatio
n co
sts,
and
pAD
E co
st a
nd Q
ALYs
effe
cts.
The
RRs
and
co
st p
aram
eter
s w
ere
repr
esen
ted
as lo
g no
rmal
dis
tribu
tions
: bou
nded
at
zero
with
a lo
ng ta
il re
pres
entin
g th
e sm
all l
ikel
ihoo
d of
lim
ited
and
even
ne
gativ
e ef
fect
iven
ess
or la
rge
cost
s re
spec
tivel
y.” (1
03)
The
appr
oach
to
sens
itivi
ty a
naly
sis
is
give
n.
The
anal
ysis
sho
uld
prov
ide
info
rmat
ion
on w
heth
er d
eter
min
istic
or p
roba
bilis
tic
sens
itivi
ty a
naly
ses
wer
e co
nduc
ted.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Be
caus
e th
ere
is u
ncer
tain
ty in
our
effe
ctiv
enes
s es
timat
es fo
r th
e sp
onge
-trac
king
tech
nolo
gies
, we
com
pute
d co
st-e
ffect
iven
ess
ratio
s ac
ross
a ra
nge
of e
ffica
cy e
stim
ates
, inc
ludi
ng th
e ci
rcum
stan
ce in
whi
ch
they
com
plet
ely
elim
inat
e RS
S. To
eva
luat
e th
e ef
fect
of v
aria
bilit
y in
cos
t es
timat
es fo
r the
tech
nolo
gies
, we
also
eva
luat
ed th
e se
nsiti
vity
of o
ur
estim
ates
to d
iffer
entia
te c
ost.”
(116
)
The
choi
ce o
f var
iabl
es
for s
ensi
tivity
ana
lysi
s is
just
ified
.
Choi
ce o
f par
amet
ers
eval
uate
d in
the
sens
itivi
ty a
naly
ses
shou
ld b
e ju
stifi
ed.
Just
ifica
tion
incl
udes
som
e la
ngua
ge a
roun
d qu
ality
of e
stim
ates
use
d in
the
base
cas
e,
repr
oduc
ibili
ty o
f the
est
imat
es u
sed
in th
e ba
se c
ase,
repr
esen
tativ
enes
s of
the
estim
ates
us
ed in
the
base
cas
e, a
nd a
vaila
bilit
y of
the
estim
ates
use
d in
the
base
cas
e.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Se
vera
l par
amet
ers
wer
e ch
ange
d to
det
erm
ine
the
impa
ct o
f ou
r fou
r mai
n as
sum
ptio
ns o
n th
e ne
t ben
efits
of g
owns
.” (8
8)
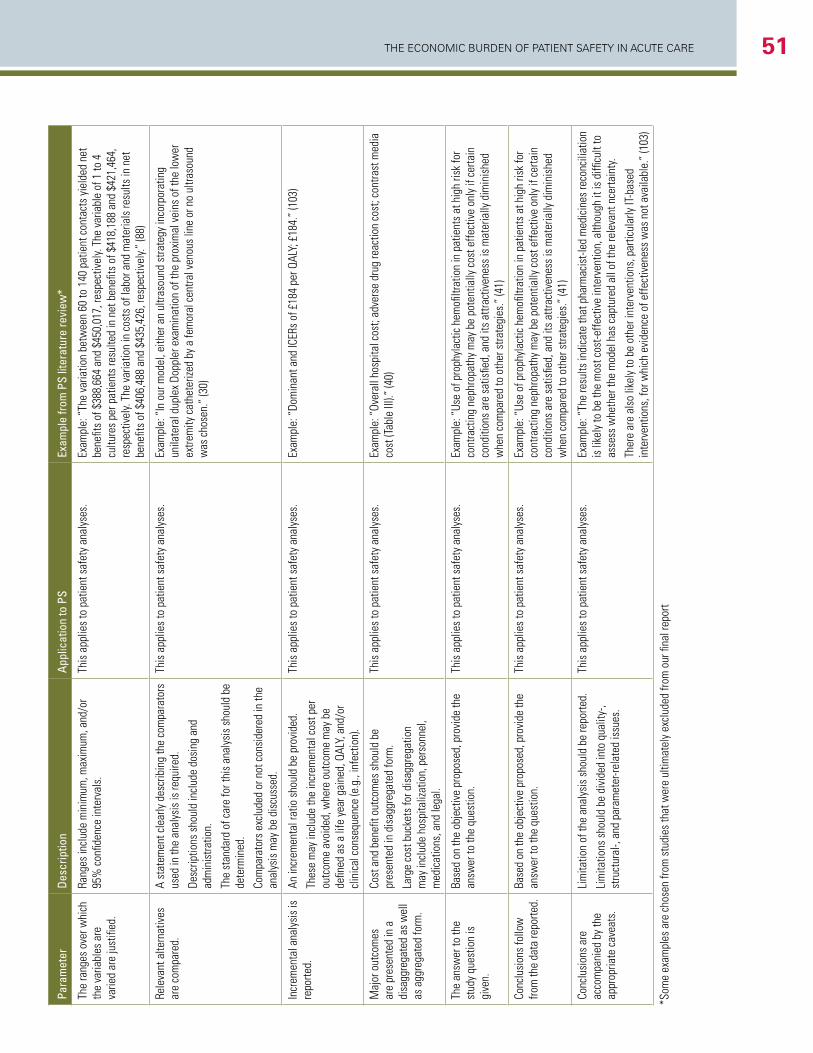
The economic Burden of PaTienT SafeTy in acuTe care 51
Para
met
erDe
scrip
tion
Appl
icat
ion
to P
SEx
ampl
e fro
m P
S lit
erat
ure
revi
ew*
ANAL
YSIS
AN
D IN
TERP
RETA
TION
OF
RESU
LTS
Tim
e ho
rizon
of c
osts
an
d be
nefit
s is
sta
ted.
The
time
horiz
on fo
r the
stu
dy s
houl
d be
cle
arly
st
ated
. Fo
r pat
ient
saf
ety
anal
yses
, the
maj
ority
of t
he
publ
ishe
d st
udie
s ha
ve u
sed
the
inst
itutio
nal
pers
pect
ive
and
thus
the
time
horiz
on is
the
dura
tion
of s
tay.
Depe
nden
t on
the
patie
nt
safe
ty ta
rget
, com
plic
atio
ns m
ay le
ad to
long
-te
rm c
onse
quen
ces
in te
rms
of m
orbi
dity
and
re
habi
litat
ion
and
shou
ld b
e co
nsid
ered
in th
e ec
onom
ic e
valu
atio
n.
Exam
ple:
“Us
ing
deci
sion
ana
lysi
s an
d an
ana
lytic
hor
izon
of a
life
time,
w
e ca
lcul
ated
the
cost
effe
ctiv
enes
s of
thre
e di
ffere
nt V
TE p
roph
ylax
is
stra
tegi
es in
trau
ma
patie
nts
with
sev
ere
inju
ries
adm
itted
to th
eir I
CU
who
wer
e be
lieve
d to
hav
e a
cont
rain
dica
tion
to p
harm
acol
ogic
al V
TE
prop
hyla
xis
for u
p to
2 w
eeks
bec
ause
of a
risk
of m
ajor
ble
edin
g.”
(27)
The
disc
ount
rate
(s) i
s (a
re) s
tate
d.Th
e di
scou
nt ra
te s
houl
d be
sta
ted.
Usua
l dis
coun
t rat
es ra
nge
from
0%
to 5
%.
For p
atie
nt s
afet
y an
alys
es, s
hort
time
horiz
ons
(<1
year
) do
not h
ave
a di
scou
nt ra
te.
Exam
ple:
“Fi
nally
, the
mod
el w
as ru
n us
ing
alte
rnat
ive
disc
ount
rate
s (0
%
and
5%).”
(97)
The
choi
ce o
f dis
coun
t ra
te(s
) is
just
ified
.Th
e di
scou
nt ra
te s
houl
d be
just
ified
.
Usua
l dis
coun
t rat
es ra
nge
from
0%
to 5
% a
nd
are
base
d on
hea
lth te
chno
logy
ass
essm
ent
agen
cies
.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
The
re w
ere
no c
ost e
ffect
iven
ess
eval
uatio
ns w
ith ju
stifi
catio
n of
di
scou
nt ra
tes.
An e
xpla
natio
n is
gi
ven
if co
sts
or
bene
fits
are
not
disc
ount
ed.
For a
naly
ses
cond
ucte
d ov
er a
tim
e ho
rizon
of
less
than
one
yea
r, a
disc
ount
rate
is n
ot
appl
ied.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Be
caus
e th
e fo
llow
-up
for t
his
anal
ysis
is le
ss th
an o
ne y
ear,
the
cost
and
out
com
es w
ere
not d
isco
unte
d.”
(153
)
Deta
ils o
f sta
tistic
al
test
s an
d co
nfide
nce
inte
rval
s ar
e gi
ven
for
stoc
hast
ic d
ata.
Stat
istic
al a
naly
ses
shou
ld b
e ou
tline
d.Th
is a
pplie
s to
pat
ient
saf
ety
anal
yses
.Ex
ampl
e: “
The
mod
el w
as a
naly
sed
by s
ampl
ing
10,0
00 in
put p
aram
eter
se
ts b
ased
on
the
prob
abili
ty th
at th
ey re
pres
ent t
he o
ptim
al s
et.
Addi
tiona
l par
amet
er v
alue
s w
ere
sam
pled
from
pro
babi
lity
dist
ribut
ions
re
pres
entin
g se
verit
y of
inci
dent
pAD
Es, i
nter
vent
ion
effe
ctiv
enes
s,
impl
emen
tatio
n co
sts,
and
pAD
E co
st a
nd Q
ALYs
effe
cts.
The
RRs
and
co
st p
aram
eter
s w
ere
repr
esen
ted
as lo
g no
rmal
dis
tribu
tions
: bou
nded
at
zero
with
a lo
ng ta
il re
pres
entin
g th
e sm
all l
ikel
ihoo
d of
lim
ited
and
even
ne
gativ
e ef
fect
iven
ess
or la
rge
cost
s re
spec
tivel
y.” (1
03)
The
appr
oach
to
sens
itivi
ty a
naly
sis
is
give
n.
The
anal
ysis
sho
uld
prov
ide
info
rmat
ion
on w
heth
er d
eter
min
istic
or p
roba
bilis
tic
sens
itivi
ty a
naly
ses
wer
e co
nduc
ted.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Be
caus
e th
ere
is u
ncer
tain
ty in
our
effe
ctiv
enes
s es
timat
es fo
r th
e sp
onge
-trac
king
tech
nolo
gies
, we
com
pute
d co
st-e
ffect
iven
ess
ratio
s ac
ross
a ra
nge
of e
ffica
cy e
stim
ates
, inc
ludi
ng th
e ci
rcum
stan
ce in
whi
ch
they
com
plet
ely
elim
inat
e RS
S. To
eva
luat
e th
e ef
fect
of v
aria
bilit
y in
cos
t es
timat
es fo
r the
tech
nolo
gies
, we
also
eva
luat
ed th
e se
nsiti
vity
of o
ur
estim
ates
to d
iffer
entia
te c
ost.”
(116
)
The
choi
ce o
f var
iabl
es
for s
ensi
tivity
ana
lysi
s is
just
ified
.
Choi
ce o
f par
amet
ers
eval
uate
d in
the
sens
itivi
ty a
naly
ses
shou
ld b
e ju
stifi
ed.
Just
ifica
tion
incl
udes
som
e la
ngua
ge a
roun
d qu
ality
of e
stim
ates
use
d in
the
base
cas
e,
repr
oduc
ibili
ty o
f the
est
imat
es u
sed
in th
e ba
se c
ase,
repr
esen
tativ
enes
s of
the
estim
ates
us
ed in
the
base
cas
e, a
nd a
vaila
bilit
y of
the
estim
ates
use
d in
the
base
cas
e.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Se
vera
l par
amet
ers
wer
e ch
ange
d to
det
erm
ine
the
impa
ct o
f ou
r fou
r mai
n as
sum
ptio
ns o
n th
e ne
t ben
efits
of g
owns
.” (8
8)
Para
met
erDe
scrip
tion
Appl
icat
ion
to P
SEx
ampl
e fro
m P
S lit
erat
ure
revi
ew*
The
rang
es o
ver w
hich
th
e va
riabl
es a
re
varie
d ar
e ju
stifi
ed.
Rang
es in
clud
e m
inim
um, m
axim
um, a
nd/o
r 95
% c
onfid
ence
inte
rval
s.Th
is a
pplie
s to
pat
ient
saf
ety
anal
yses
.Ex
ampl
e: “
The
varia
tion
betw
een
60 to
140
pat
ient
con
tact
s yi
elde
d ne
t be
nefit
s of
$38
8,66
4 an
d $4
50,0
17, r
espe
ctiv
ely.
The
varia
ble
of 1
to 4
cu
lture
s pe
r pat
ient
s re
sulte
d in
net
ben
efits
of $
418,
188
and
$421
,464
, re
spec
tivel
y. Th
e va
riatio
n in
cos
ts o
f lab
or a
nd m
ater
ials
resu
lts in
net
be
nefit
s of
$40
6,48
8 an
d $4
35,4
26, r
espe
ctiv
ely.”
(88)
Rele
vant
alte
rnat
ives
ar
e co
mpa
red.
A st
atem
ent c
lear
ly d
escr
ibin
g th
e co
mpa
rato
rs
used
in th
e an
alys
is is
requ
ired.
Desc
riptio
ns s
houl
d in
clud
e do
sing
and
ad
min
istra
tion.
The
stan
dard
of c
are
for t
his
anal
ysis
sho
uld
be
dete
rmin
ed.
Com
para
tors
exc
lude
d or
not
con
side
red
in th
e an
alys
is m
ay b
e di
scus
sed.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“In
our
mod
el, e
ither
an
ultra
soun
d st
rate
gy in
corp
orat
ing
unila
tera
l dup
lex
Dopp
ler e
xam
inat
ion
of th
e pr
oxim
al v
eins
of t
he lo
wer
ex
trem
ity c
athe
teriz
ed b
y a
fem
oral
cen
tral v
enou
s lin
e or
no
ultra
soun
d w
as c
hose
n.”
(30)
Incr
emen
tal a
naly
sis
is
repo
rted.
An in
crem
enta
l rat
io s
houl
d be
pro
vide
d.
Thes
e m
ay in
clud
e th
e in
crem
enta
l cos
t per
ou
tcom
e av
oide
d, w
here
out
com
e m
ay b
e de
fined
as
a lif
e ye
ar g
aine
d, Q
ALY,
and
/or
clin
ical
con
sequ
ence
(e.g
., in
fect
ion)
.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Do
min
ant a
nd IC
ERs
of £
184
per Q
ALY;
£18
4.”
(103
)
Maj
or o
utco
mes
ar
e pr
esen
ted
in a
di
sagg
rega
ted
as w
ell
as a
ggre
gate
d fo
rm.
Cost
and
ben
efit o
utco
mes
sho
uld
be
pres
ente
d in
dis
aggr
egat
ed fo
rm.
Larg
e co
st b
ucke
ts fo
r dis
aggr
egat
ion
may
incl
ude
hosp
italiz
atio
n, p
erso
nnel
, m
edic
atio
ns, a
nd le
gal.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Ov
eral
l hos
pita
l cos
t; ad
vers
e dr
ug re
actio
n co
st; c
ontra
st m
edia
co
st (T
able
III).
” (4
0)
The
answ
er to
the
stud
y qu
estio
n is
gi
ven.
Base
d on
the
obje
ctiv
e pr
opos
ed, p
rovi
de th
e an
swer
to th
e qu
estio
n.Th
is a
pplie
s to
pat
ient
saf
ety
anal
yses
.Ex
ampl
e: “
Use
of p
roph
ylac
tic h
emofi
ltrat
ion
in p
atie
nts
at h
igh
risk
for
cont
ract
ing
neph
ropa
thy
may
be
pote
ntia
lly c
ost e
ffect
ive
only
if c
erta
in
cond
ition
s ar
e sa
tisfie
d, a
nd it
s at
tract
iven
ess
is m
ater
ially
dim
inis
hed
whe
n co
mpa
red
to o
ther
stra
tegi
es.”
(41)
Conc
lusi
ons
follo
w
from
the
data
repo
rted.
Base
d on
the
obje
ctiv
e pr
opos
ed, p
rovi
de th
e an
swer
to th
e qu
estio
n.Th
is a
pplie
s to
pat
ient
saf
ety
anal
yses
.Ex
ampl
e: “
Use
of p
roph
ylac
tic h
emofi
ltrat
ion
in p
atie
nts
at h
igh
risk
for
cont
ract
ing
neph
ropa
thy
may
be
pote
ntia
lly c
ost e
ffect
ive
only
if c
erta
in
cond
ition
s ar
e sa
tisfie
d, a
nd it
s at
tract
iven
ess
is m
ater
ially
dim
inis
hed
whe
n co
mpa
red
to o
ther
stra
tegi
es.”
(41)
Conc
lusi
ons
are
acco
mpa
nied
by
the
appr
opria
te c
avea
ts.
Lim
itatio
n of
the
anal
ysis
sho
uld
be re
porte
d.
Lim
itatio
ns s
houl
d be
div
ided
into
qua
lity-
, st
ruct
ural
-, an
d pa
ram
eter
-rela
ted
issu
es.
This
app
lies
to p
atie
nt s
afet
y an
alys
es.
Exam
ple:
“Th
e re
sults
indi
cate
that
pha
rmac
ist-l
ed m
edic
ines
reco
ncili
atio
n is
like
ly to
be
the
mos
t cos
t-effe
ctiv
e in
terv
entio
n, a
lthou
gh it
is d
ifficu
lt to
as
sess
whe
ther
the
mod
el h
as c
aptu
red
all o
f the
rele
vant
nce
rtain
ty.
Ther
e ar
e al
so li
kely
to b
e ot
her i
nter
vent
ions
, par
ticul
arly
IT-b
ased
in
terv
entio
ns, f
or w
hich
evi
denc
e of
effe
ctiv
enes
s w
as n
ot a
vaila
ble.
” (1
03)
*Som
e ex
ampl
es a
re c
hose
n fro
m s
tudi
es th
at w
ere
ultim
atel
y ex
clud
ed fr
om o
ur fi
nal r
epor
t
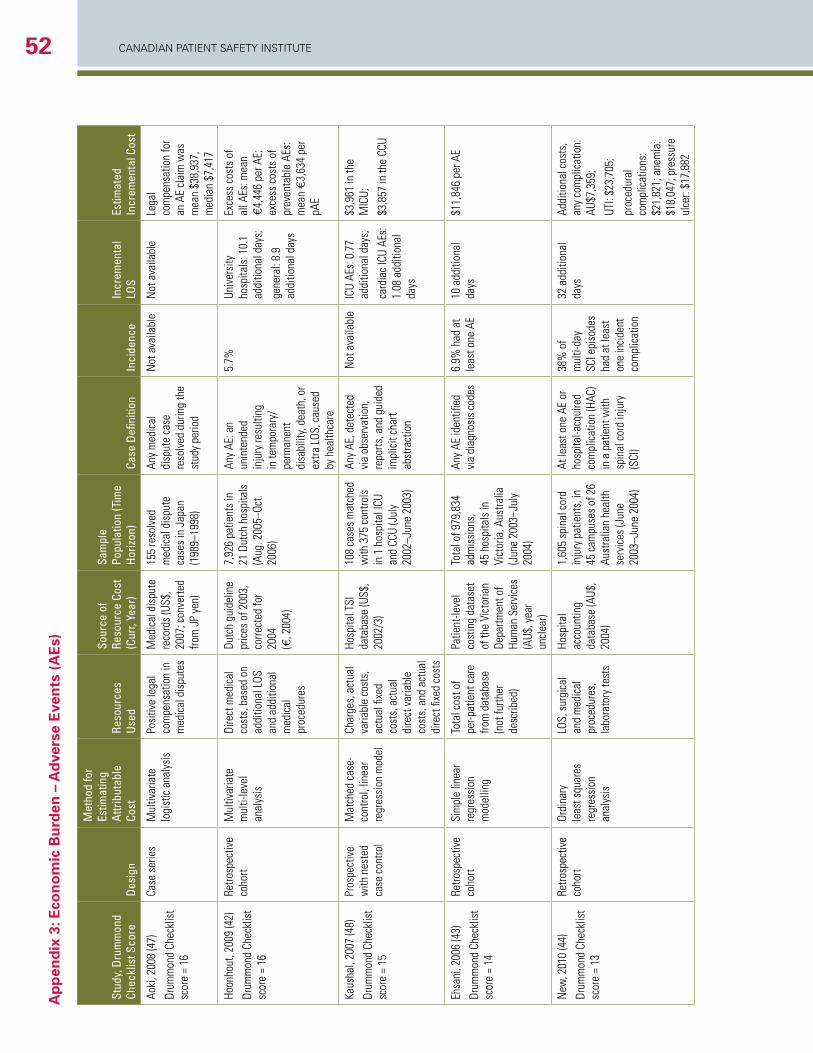
CANADIAN PAtIeNt SAfety INStItUte52a
pp
end
ix 3
: eco
no
mic
Bu
rden
– a
dve
rse
eve
nts
(a
es)
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
Defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Aoki
, 200
8 (4
7)
Drum
mon
d Ch
eckl
ist
scor
e =
16
Case
ser
ies
Mul
tivar
iate
lo
gist
ic a
naly
sis
Posi
tive
lega
l co
mpe
nsat
ion
in
med
ical
dis
pute
s
Med
ical
dis
pute
re
cord
s (U
S$,
2007
; con
verte
d fro
m J
P ye
n)
155
reso
lved
m
edic
al d
ispu
te
case
s in
Jap
an
(198
9–19
98)
Any
med
ical
di
sput
e ca
se
reso
lved
dur
ing
the
stud
y pe
riod
Not
ava
ilabl
eN
ot a
vaila
ble
Lega
l co
mpe
nsat
ion
for
an A
E cl
aim
was
m
ean
$38,
937,
m
edia
n $7
,417
Hoon
hout
, 200
9 (4
2)
Drum
mon
d Ch
eckl
ist
scor
e =
16
Retro
spec
tive
coho
rtM
ultiv
aria
te
mul
ti-le
vel
anal
ysis
Dire
ct m
edic
al
cost
s, b
ased
on
addi
tiona
l LOS
an
d ad
ditio
nal
med
ical
pr
oced
ures
Dutc
h gu
idel
ine
pric
es o
f 200
3,
corre
cted
for
2004
(€
, 200
4)
7,92
6 pa
tient
s in
21
Dut
ch h
ospi
tals
(A
ug. 2
005–
Oct.
2006
)
Any
AE: a
n un
inte
nded
in
jury
resu
lting
in
tem
pora
ry/
perm
anen
t di
sabi
lity,
deat
h, o
r ex
tra L
OS, c
ause
d by
hea
lthca
re
5.7%
Un
iver
sity
ho
spita
ls: 1
0.1
addi
tiona
l day
s;
gene
ral:
8.9
addi
tiona
l day
s
Exce
ss c
osts
of
all A
Es: m
ean
€4,4
46 p
er A
E;
exce
ss c
osts
of
prev
enta
ble
AEs:
m
ean
€3,6
34 p
er
pAE
Kaus
hal,
2007
(48)
Drum
mon
d Ch
eckl
ist
scor
e =
15
Pros
pect
ive
with
nes
ted
case
con
trol
Mat
ched
cas
e-co
ntro
l, lin
ear
regr
essi
on m
odel
Char
ges,
act
ual
varia
ble
cost
s,
actu
al fi
xed
cost
s, a
ctua
l di
rect
var
iabl
e co
sts,
and
act
ual
dire
ct fi
xed
cost
s
Hosp
ital T
SI
data
base
(US$
, 20
02/3
)
108
case
s m
atch
ed
with
375
con
trols
in
1 h
ospi
tal I
CU
and
CCU
(Jul
y 20
02–J
une
2003
)
Any
AE, d
etec
ted
via
obse
rvat
ion,
re
ports
, and
gui
ded
impl
icit
char
t ab
stra
ctio
n
Not
ava
ilabl
eIC
U AE
s: 0
.77
addi
tiona
l day
s;
card
iac
ICU
AEs:
1.
08 a
dditi
onal
da
ys
$3,9
61 in
the
MIC
U;
$3,8
57 in
the
CCU
Ehsa
ni, 2
006
(43)
Drum
mon
d Ch
eckl
ist
scor
e =
14
Retro
spec
tive
coho
rtSi
mpl
e lin
ear
regr
essi
on
mod
ellin
g
Tota
l cos
t of
per-p
atie
nt c
are
from
dat
abas
e (n
ot fu
rther
de
scrib
ed)
Patie
nt-le
vel
cost
ing
data
set
of th
e Vi
ctor
ian
Depa
rtmen
t of
Hum
an S
ervi
ces
(AU$
, yea
r un
clea
r)
Tota
l of 9
79,8
34
adm
issi
ons,
45
hos
pita
ls in
Vi
ctor
ia, A
ustra
lia
(Jun
e 20
03–J
uly
2004
)
Any
AE id
entifi
ed
via
diag
nosi
s co
des
6.9%
had
at
leas
t one
AE
10 a
dditi
onal
da
ys
$11,
846
per A
E
New
, 201
0 (4
4)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Retro
spec
tive
coho
rtOr
dina
ry
leas
t squ
ares
re
gres
sion
an
alys
is
LOS,
sur
gica
l an
d m
edic
al
proc
edur
es,
labo
rato
ry te
sts
Hosp
ital
acco
untin
g da
taba
se (A
U$,
2004
)
1,60
5 sp
inal
cor
d in
jury
pat
ient
s, in
45
cam
puse
s of
26
Aust
ralia
n he
alth
se
rvic
es (J
une
2003
–Jun
e 20
04)
At le
ast o
ne A
E or
ho
spita
l-acq
uire
d co
mpl
icat
ion
(HAC
) in
a p
atie
nt w
ith
spin
al c
ord
inju
ry
(SCI
)
38%
of
mul
ti-da
y SC
I epi
sode
s ha
d at
leas
t on
e in
cide
nt
com
plic
atio
n
32 a
dditi
onal
da
ys
Addi
tiona
l cos
ts,
any
com
plic
atio
n:
AU$7
,359
;
UTI:
$23,
705;
proc
edur
al
com
plic
atio
ns:
$21,
821;
ane
mia
: $1
8,04
7; p
ress
ure
ulce
r: $1
7,88
2
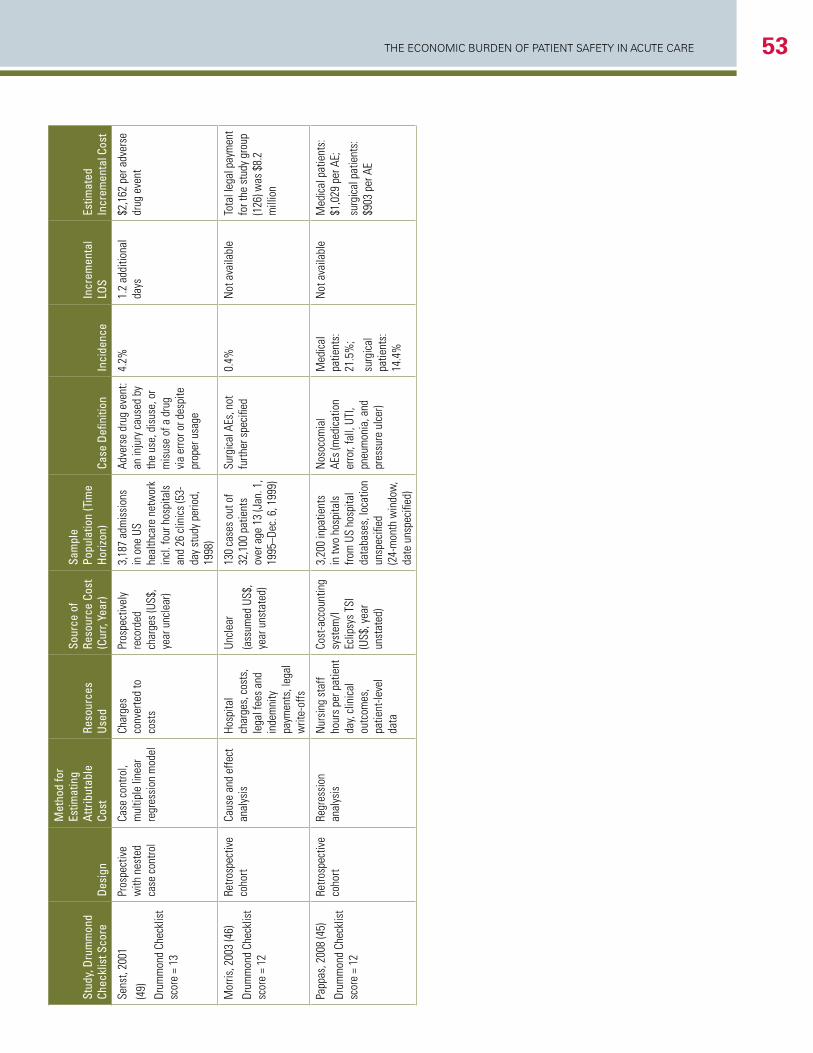
The economic Burden of PaTienT SafeTy in acuTe care 53
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
Defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Sens
t, 20
01
(49)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Pros
pect
ive
with
nes
ted
case
con
trol
Case
con
trol,
mul
tiple
line
ar
regr
essi
on m
odel
Char
ges
conv
erte
d to
co
sts
Pros
pect
ivel
y re
cord
ed
char
ges
(US$
, ye
ar u
ncle
ar)
3,18
7 ad
mis
sion
s in
one
US
heal
thca
re n
etw
ork
incl
. fou
r hos
pita
ls
and
26 c
linic
s (5
3-da
y st
udy
perio
d,
1998
)
Adve
rse
drug
eve
nt:
an in
jury
cau
sed
by
the
use,
dis
use,
or
mis
use
of a
dru
g vi
a er
ror o
r des
pite
pr
oper
usa
ge
4.2%
1.2
addi
tiona
l da
ys$2
,162
per
adv
erse
dr
ug e
vent
Mor
ris, 2
003
(46)
Drum
mon
d Ch
eckl
ist
scor
e =
12
Retro
spec
tive
coho
rtCa
use
and
effe
ct
anal
ysis
Hosp
ital
char
ges,
cos
ts,
lega
l fee
s an
d in
dem
nity
pa
ymen
ts, l
egal
w
rite-
offs
Uncl
ear
(ass
umed
US$
, ye
ar u
nsta
ted)
130
case
s ou
t of
32,1
00 p
atie
nts
over
age
13
(Jan
. 1,
1995
–Dec
. 6, 1
999)
Surg
ical
AEs
, not
fu
rther
spe
cifie
d0.
4%
Not
ava
ilabl
eTo
tal l
egal
pay
men
t fo
r the
stu
dy g
roup
(1
26) w
as $
8.2
mill
ion
Papp
as, 2
008
(45)
Drum
mon
d Ch
eckl
ist
scor
e =
12
Retro
spec
tive
coho
rtRe
gres
sion
an
alys
isN
ursi
ng s
taff
hour
s pe
r pat
ient
da
y, cl
inic
al
outc
omes
, pa
tient
-leve
l da
ta
Cost
-acc
ount
ing
syst
em/l
Eclip
sys
TSI
(US$
, yea
r un
stat
ed)
3,20
0 in
patie
nts
in tw
o ho
spita
ls
from
US
hosp
ital
data
base
s, lo
catio
n un
spec
ified
(2
4-m
onth
win
dow
, da
te u
nspe
cifie
d)
Nos
ocom
ial
AEs
(med
icat
ion
erro
r, fa
ll, U
TI,
pneu
mon
ia, a
nd
pres
sure
ulc
er)
Med
ical
pa
tient
s:
21.5
%;
surg
ical
pa
tient
s:
14.4
%
Not
ava
ilabl
eM
edic
al p
atie
nts:
$1
,029
per
AE;
surg
ical
pat
ient
s:
$903
per
AE
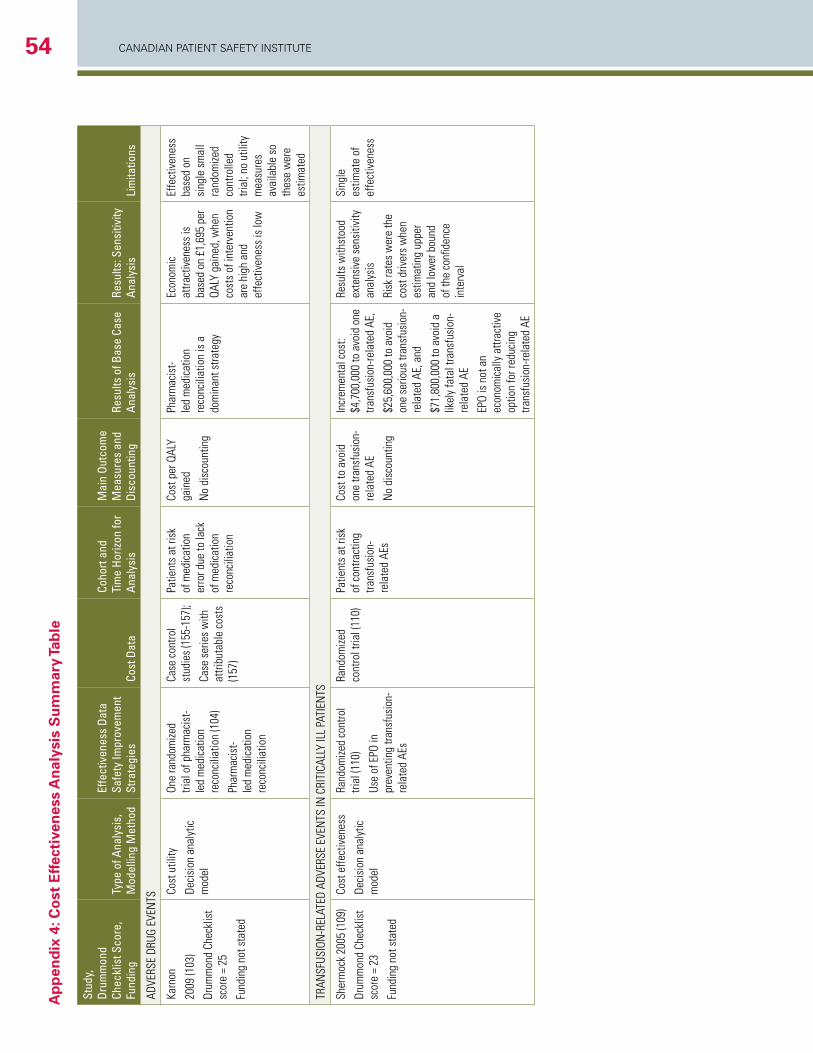
CANADIAN PAtIeNt SAfety INStItUte54a
pp
end
ix 4
: co
st e
ffect
iven
ess
an
alys
is s
um
mar
y Ta
ble
Stud
y,Dr
umm
ond
Chec
klis
t Sco
re,
Fund
ing
Type
of A
naly
sis,
M
odel
ling
Met
hod
Effe
ctiv
enes
s Da
ta
Safe
ty Im
prov
emen
t St
rate
gies
Cost
Dat
a
Coho
rt an
d Ti
me
Horiz
on fo
r An
alys
is
Mai
n Ou
tcom
e M
easu
res
and
Disc
ount
ing
Resu
lts o
f Bas
e Ca
se
Anal
ysis
Re
sults
: Sen
sitiv
ity
Anal
ysis
Lim
itatio
ns
ADVE
RSE
DRUG
EVE
NTS
Karn
on
2009
(103
)
Drum
mon
d Ch
eckl
ist
scor
e =
25
Fund
ing
not s
tate
d
Cost
util
ity
Deci
sion
ana
lytic
m
odel
One
rand
omize
d tri
al o
f pha
rmac
ist-
led
med
icat
ion
reco
ncili
atio
n (1
04)
Phar
mac
ist-
led
med
icat
ion
reco
ncili
atio
n
Case
con
trol
stud
ies
(155
-157
);
Case
ser
ies
with
at
tribu
tabl
e co
sts
(157
)
Patie
nts
at ri
sk
of m
edic
atio
n er
ror d
ue to
lack
of
med
icat
ion
reco
ncili
atio
n
Cost
per
QAL
Y ga
ined
No
disc
ount
ing
Phar
mac
ist-
led
med
icat
ion
reco
ncili
atio
n is
a
dom
inan
t stra
tegy
Econ
omic
at
tract
iven
ess
is
base
d on
£1,
695
per
QALY
gai
ned,
whe
n co
sts
of in
terv
entio
n ar
e hi
gh a
nd
effe
ctiv
enes
s is
low
Effe
ctiv
enes
s ba
sed
on
sing
le s
mal
l ra
ndom
ized
cont
rolle
d tri
al; n
o ut
ility
m
easu
res
avai
labl
e so
th
ese
wer
e es
timat
ed
TRAN
SFUS
ION
-REL
ATED
ADV
ERSE
EVE
NTS
IN C
RITI
CALL
Y IL
L PA
TIEN
TS
Sher
moc
k 20
05 (1
09)
Drum
mon
d Ch
eckl
ist
scor
e =
23
Fund
ing
not s
tate
d
Cost
effe
ctiv
enes
s
Deci
sion
ana
lytic
m
odel
Rand
omize
d co
ntro
l tri
al (1
10)
Use
of E
PO in
pr
even
ting
trans
fusi
on-
rela
ted
AEs
Rand
omize
d co
ntro
l tria
l (11
0)Pa
tient
s at
risk
of
con
tract
ing
trans
fusi
on-
rela
ted
AEs
Cost
to a
void
on
e tra
nsfu
sion
-re
late
d AE
No
disc
ount
ing
Incr
emen
tal c
ost:
$4,7
00,0
00 to
avo
id o
ne
trans
fusi
on-re
late
d AE
,
$25,
600,
000
to a
void
on
e se
rious
tran
sfus
ion-
rela
ted
AE, a
nd
$71,
800,
000
to a
void
a
likel
y fa
tal t
rans
fusi
on-
rela
ted
AE
EPO
is n
ot a
n ec
onom
ical
ly a
ttrac
tive
optio
n fo
r red
ucin
g tra
nsfu
sion
-rela
ted
AE
Resu
lts w
ithst
ood
exte
nsiv
e se
nsiti
vity
an
alys
is
Risk
rate
s w
ere
the
cost
driv
ers
whe
n es
timat
ing
uppe
r an
d lo
wer
bou
nd
of th
e co
nfide
nce
inte
rval
Sing
le
estim
ate
of
effe
ctiv
enes
s
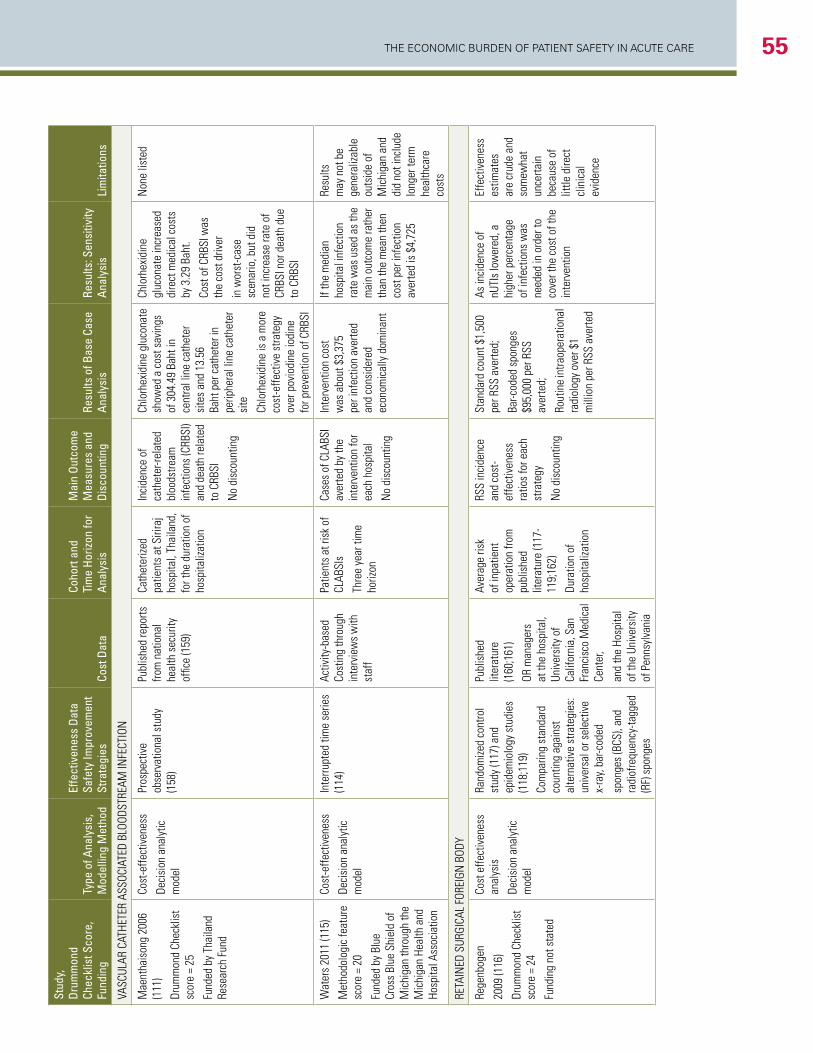
The economic Burden of PaTienT SafeTy in acuTe care 55St
udy,
Drum
mon
d Ch
eckl
ist S
core
,Fu
ndin
gTy
pe o
f Ana
lysi
s,
Mod
ellin
g M
etho
d
Effe
ctiv
enes
s Da
ta
Safe
ty Im
prov
emen
t St
rate
gies
Cost
Dat
a
Coho
rt an
d Ti
me
Horiz
on fo
r An
alys
is
Mai
n Ou
tcom
e M
easu
res
and
Disc
ount
ing
Resu
lts o
f Bas
e Ca
se
Anal
ysis
Re
sults
: Sen
sitiv
ity
Anal
ysis
Lim
itatio
ns
VASC
ULAR
CAT
HETE
R AS
SOCI
ATED
BLO
ODST
REAM
INFE
CTIO
N
Mae
ntha
ison
g 20
06
(111
)
Drum
mon
d Ch
eckl
ist
scor
e =
25
Fund
ed b
y Th
aila
nd
Rese
arch
Fun
d
Cost
-effe
ctiv
enes
s
Deci
sion
ana
lytic
m
odel
Pros
pect
ive
obse
rvat
iona
l stu
dy
(158
)
Publ
ishe
d re
ports
fro
m n
atio
nal
heal
th s
ecur
ity
offic
e (1
59)
Cath
eter
ized
patie
nts
at S
irira
j ho
spita
l, Th
aila
nd,
for t
he d
urat
ion
of
hosp
italiz
atio
n
Inci
denc
e of
ca
thet
er-re
late
d bl
oods
tream
in
fect
ions
(CRB
SI)
and
deat
h re
late
d to
CRB
SI
No
disc
ount
ing
Chlo
rhex
idin
e gl
ucon
ate
show
ed a
cos
t sav
ings
of
304
.49
Baht
in
cent
ral l
ine
cath
eter
si
tes
and
13.5
6 Ba
ht p
er c
athe
ter i
n pe
riphe
ral l
ine
cath
eter
si
te
Chlo
rhex
idin
e is
a m
ore
cost
-effe
ctiv
e st
rate
gy
over
pov
iodi
ne io
dine
fo
r pre
vent
ion
of C
RBSI
Chlo
rhex
idin
e gl
ucon
ate
incr
ease
d di
rect
med
ical
cos
ts
by 3
.29
Baht
.
Cost
of C
RBSI
was
th
e co
st d
river
in w
orst
-cas
e sc
enar
io, b
ut d
id
not i
ncre
ase
rate
of
CRBS
I nor
dea
th d
ue
to C
RBSI
Non
e lis
ted
Wat
ers
2011
(115
)
Met
hodo
logi
c fe
atur
e sc
ore
= 20
Fund
ed b
y Bl
ue
Cros
s Bl
ue S
hiel
d of
M
ichi
gan
thro
ugh
the
Mic
higa
n He
alth
and
Ho
spita
l Ass
ocia
tion
Cost
-effe
ctiv
enes
s
Deci
sion
ana
lytic
m
odel
Inte
rrupt
ed ti
me
serie
s (1
14)
Activ
ity-b
ased
Co
stin
g th
roug
h in
terv
iew
s w
ith
staf
f
Patie
nts
at ri
sk o
f CL
ABSI
s
Thre
e ye
ar ti
me
horiz
on
Case
s of
CLA
BSI
aver
ted
by th
e in
terv
entio
n fo
r ea
ch h
ospi
tal
No
disc
ount
ing
Inte
rven
tion
cost
w
as a
bout
$3,
375
per i
nfec
tion
aver
ted
and
cons
ider
ed
econ
omic
ally
dom
inan
t
If th
e m
edia
n ho
spita
l inf
ectio
n ra
te w
as u
sed
as th
e m
ain
outc
ome
rath
er
than
the
mea
n th
en
cost
per
infe
ctio
n av
erte
d is
$4,
725
Resu
lts
may
not
be
gene
raliz
able
ou
tsid
e of
M
ichi
gan
and
did
not i
nclu
de
long
er te
rm
heal
thca
re
cost
s
RETA
INED
SUR
GICA
L FO
REIG
N B
ODY
Rege
nbog
en
2009
(116
)
Drum
mon
d Ch
eckl
ist
scor
e =
24
Fund
ing
not s
tate
d
Cost
effe
ctiv
enes
s an
alys
is
Deci
sion
ana
lytic
m
odel
Rand
omize
d co
ntro
l st
udy
(117
) and
ep
idem
iolo
gy s
tudi
es
(118
;119
)
Com
parin
g st
anda
rd
coun
ting
agai
nst
alte
rnat
ive
stra
tegi
es:
univ
ersa
l or s
elec
tive
x-ra
y, ba
r-cod
ed
spon
ges
(BCS
), an
d ra
diof
requ
ency
-tagg
ed
(RF)
spo
nges
Publ
ishe
d lit
erat
ure
(160
;161
)
OR m
anag
ers
at th
e ho
spita
l, Un
iver
sity
of
Calif
orni
a, S
an
Fran
cisc
o M
edic
al
Cent
er,
and
the
Hosp
ital
of th
e Un
iver
sity
of
Pen
nsyl
vani
a
Aver
age
risk
of in
patie
nt
oper
atio
n fro
m
publ
ishe
d lit
erat
ure
(117
-11
9;16
2)
Dura
tion
of
hosp
italiz
atio
n
RSS
inci
denc
e an
d co
st-
effe
ctiv
enes
s ra
tios
for e
ach
stra
tegy
No
disc
ount
ing
Stan
dard
cou
nt $
1,50
0 pe
r RSS
ave
rted;
Bar-c
oded
spo
nges
$9
5,00
0 pe
r RSS
av
erte
d;
Rout
ine
intra
oper
atio
nal
radi
olog
y ov
er $
1 m
illio
n pe
r RSS
ave
rted
As in
cide
nce
of
nUTI
s lo
wer
ed, a
hi
gher
per
cent
age
of in
fect
ions
was
ne
eded
in o
rder
to
cove
r the
cos
t of t
he
inte
rven
tion
Effe
ctiv
enes
s es
timat
es
are
crud
e an
d so
mew
hat
unce
rtain
be
caus
e of
lit
tle d
irect
cl
inic
al
evid
ence
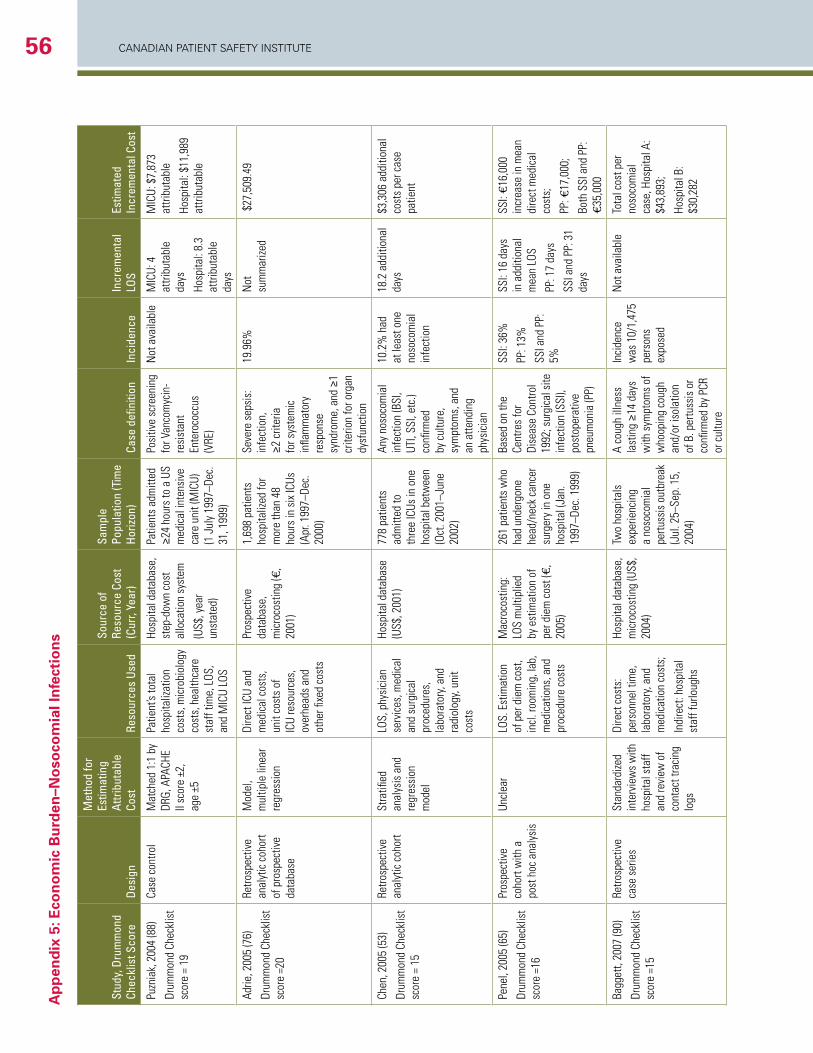
CANADIAN PAtIeNt SAfety INStItUte56a
pp
end
ix 5
: eco
no
mic
Bu
rden
–no
soco
mia
l in
fect
ion
s
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Puzn
iak,
200
4 (8
8)
Drum
mon
d Ch
eckl
ist
scor
e =
19
Case
con
trol
Mat
ched
1:1
by
DRG,
APA
CHE
II sc
ore
±2,
age
±5
Patie
nt’s
tota
l ho
spita
lizat
ion
cost
s, m
icro
biol
ogy
cost
s, h
ealth
care
st
aff t
ime,
LOS
, an
d M
ICU
LOS
Hosp
ital d
atab
ase,
st
ep-d
own
cost
al
loca
tion
syst
em
(US$
, yea
r un
stat
ed)
Patie
nts
adm
itted
≥2
4 ho
urs
to a
US
med
ical
inte
nsiv
e ca
re u
nit (
MIC
U)
(1 J
uly
1997
–Dec
. 31
, 199
9)
Posi
tive
scre
enin
g fo
r Van
com
ycin
-re
sist
ant
Ente
roco
ccus
(V
RE)
Not
ava
ilabl
eM
ICU:
4
attri
buta
ble
days
Hosp
ital:
8.3
attri
buta
ble
days
MIC
U: $
7,87
3 at
tribu
tabl
e
Hosp
ital:
$11,
989
attri
buta
ble
Adrie
, 200
5 (7
6)
Drum
mon
d Ch
eckl
ist
scor
e =2
0
Retro
spec
tive
anal
ytic
coh
ort
of p
rosp
ectiv
e da
taba
se
Mod
el,
mul
tiple
line
ar
regr
essi
on
Dire
ct IC
U an
d m
edic
al c
osts
, un
it co
sts
of
ICU
reso
urce
s,
over
head
s an
d ot
her fi
xed
cost
s
Pros
pect
ive
data
base
, m
icro
cost
ing
(€,
2001
)
1,69
8 pa
tient
s ho
spita
lized
for
mor
e th
an 4
8 ho
urs
in s
ix IC
Us
(Apr
. 199
7–De
c.
2000
)
Seve
re s
epsi
s:
infe
ctio
n,
≥2 c
riter
ia
for s
yste
mic
in
flam
mat
ory
resp
onse
sy
ndro
me,
and
≥1
crite
rion
for o
rgan
dy
sfun
ctio
n
19.9
6%
Not
su
mm
arize
d $
27,5
09.4
9
Chen
, 200
5 (5
3)
Drum
mon
d Ch
eckl
ist
scor
e =
15
Retro
spec
tive
anal
ytic
coh
ort
Stra
tified
an
alys
is a
nd
regr
essi
on
mod
el
LOS,
phy
sici
an
serv
ices
, med
ical
an
d su
rgic
al
proc
edur
es,
labo
rato
ry, a
nd
radi
olog
y, un
it co
sts
Hosp
ital d
atab
ase
(US$
, 200
1)77
8 pa
tient
s ad
mitt
ed to
th
ree
ICUs
in o
ne
hosp
ital b
etw
een
(Oct
. 200
1–Ju
ne
2002
)
Any
noso
com
ial
infe
ctio
n (B
SI,
UTI,
SSI,
etc.
) co
nfirm
ed
by c
ultu
re,
sym
ptom
s, a
nd
an a
ttend
ing
phys
icia
n
10.2
% h
ad
at le
ast o
ne
noso
com
ial
infe
ctio
n
18.2
add
ition
al
days
$3
,306
add
ition
al
cost
s pe
r cas
e pa
tient
Pene
l, 20
05 (6
5)
Drum
mon
d Ch
eckl
ist
scor
e =1
6
Pros
pect
ive
coho
rt w
ith a
po
st h
oc a
naly
sis
Uncl
ear
LOS.
Est
imat
ion
of p
er d
iem
cos
t, in
cl. r
oom
ing,
lab,
m
edic
atio
ns, a
nd
proc
edur
e co
sts
Mac
roco
stin
g:
LOS
mul
tiplie
d by
est
imat
ion
of
per d
iem
cos
t (€,
20
05)
261
patie
nts
who
ha
d un
derg
one
head
/nec
k ca
ncer
su
rger
y in
one
ho
spita
l (Ja
n.
1997
–Dec
. 199
9)
Base
d on
the
Cent
res
for
Dise
ase
Cont
rol
1992
; sur
gica
l site
in
fect
ion
(SSI
), po
stop
erat
ive
pneu
mon
ia (P
P)
SSI:
36%
PP: 1
3%
SSI a
nd P
P:
5%
SSI:
16 d
ays
in a
dditi
onal
m
ean
LOS
PP: 1
7 da
ys
SSI a
nd P
P: 3
1 da
ys
SSI:
€16,
000
incr
ease
in m
ean
dire
ct m
edic
al
cost
s;
PP: €
17,0
00;
Both
SSI
and
PP:
€3
5,00
0
Bagg
ett,
2007
(90)
Drum
mon
d Ch
eckl
ist
scor
e =1
5
Retro
spec
tive
case
ser
ies
Stan
dard
ized
inte
rvie
ws
with
ho
spita
l sta
ff an
d re
view
of
cont
act t
raci
ng
logs
Dire
ct c
osts
: pe
rson
nel t
ime,
la
bora
tory
, and
m
edic
atio
n co
sts;
Indi
rect
: hos
pita
l st
aff f
urlo
ughs
Hosp
ital d
atab
ase,
m
icro
cost
ing
(US$
, 20
04)
Two
hosp
itals
ex
perie
ncin
g a
noso
com
ial
pertu
ssis
out
brea
k (J
ul. 2
5–Se
p. 1
5,
2004
)
A co
ugh
illne
ss
last
ing
≥14
days
w
ith s
ympt
oms
of
who
opin
g co
ugh
and/
or is
olat
ion
of B
. per
tuss
is o
r co
nfirm
ed b
y PC
R or
cul
ture
Inci
denc
e w
as 1
0/1,
475
pers
ons
expo
sed
Not
ava
ilabl
eTo
tal c
ost p
er
noso
com
ial
case
, Hos
pita
l A:
$43,
893;
Hosp
ital B
: $3
0,28
2
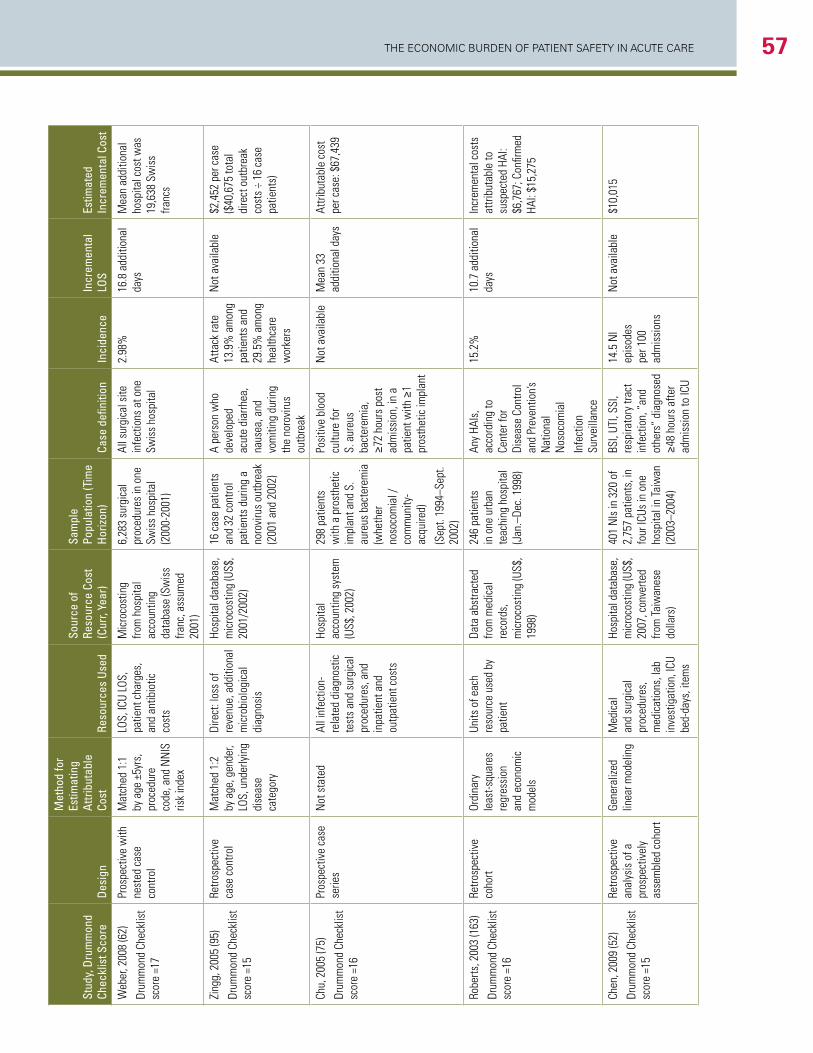
The economic Burden of PaTienT SafeTy in acuTe care 57
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Web
er, 2
008
(62)
Drum
mon
d Ch
eckl
ist
scor
e =1
7
Pros
pect
ive
with
ne
sted
cas
e co
ntro
l
Mat
ched
1:1
by
age
±5y
rs,
proc
edur
e co
de, a
nd N
NIS
ris
k in
dex
LOS,
ICU
LOS,
pa
tient
cha
rges
, an
d an
tibio
tic
cost
s
Mic
roco
stin
g fro
m h
ospi
tal
acco
untin
g da
taba
se (S
wis
s fra
nc, a
ssum
ed
2001
)
6,28
3 su
rgic
al
proc
edur
es in
one
Sw
iss
hosp
ital
(200
0-20
01)
All s
urgi
cal s
ite
infe
ctio
ns a
t one
Sw
iss
hosp
ital
2.98
%16
.8 a
dditi
onal
da
ysM
ean
addi
tiona
l ho
spita
l cos
t was
19
,638
Sw
iss
franc
s
Zing
g, 2
005
(95)
Drum
mon
d Ch
eckl
ist
scor
e =1
5
Retro
spec
tive
case
con
trol
Mat
ched
1:2
by
age
, gen
der,
LOS,
und
erly
ing
dise
ase
cate
gory
Dire
ct: l
oss
of
reve
nue,
add
ition
al
mic
robi
olog
ical
di
agno
sis
Hosp
ital d
atab
ase,
m
icro
cost
ing
(US$
, 20
01/2
002)
16 c
ase
patie
nts
and
32 c
ontro
l pa
tient
s du
ring
a no
rovi
rus
outb
reak
(2
001
and
2002
)
A pe
rson
who
de
velo
ped
acut
e di
arrh
ea,
naus
ea, a
nd
vom
iting
dur
ing
the
noro
viru
s ou
tbre
ak
Atta
ck ra
te
13.9
% a
mon
g pa
tient
s an
d 29
.5%
am
ong
heal
thca
re
wor
kers
Not
ava
ilabl
e$2
,452
per
cas
e ($
40,6
75 to
tal
dire
ct o
utbr
eak
cost
s ÷
16 c
ase
patie
nts)
Chu,
200
5 (7
5)
Drum
mon
d Ch
eckl
ist
scor
e =1
6
Pros
pect
ive
case
se
ries
Not
sta
ted
All i
nfec
tion-
rela
ted
diag
nost
ic
test
s an
d su
rgic
al
proc
edur
es, a
nd
inpa
tient
and
ou
tpat
ient
cos
ts
Hosp
ital
acco
untin
g sy
stem
(U
S$, 2
002)
298
patie
nts
with
a p
rost
hetic
im
plan
t and
S.
aure
us b
acte
rem
ia
(whe
ther
no
soco
mia
l /
com
mun
ity-
acqu
ired)
(Sep
t. 19
94–S
ept.
2002
)
Posi
tive
bloo
d cu
lture
for
S. a
ureu
s ba
cter
emia
, ≥7
2 ho
urs
post
ad
mis
sion
, in
a pa
tient
with
≥1
pros
thet
ic im
plan
t
Not
ava
ilabl
eM
ean
33
addi
tiona
l day
s
Attri
buta
ble
cost
pe
r cas
e: $
67,4
39
Robe
rts, 2
003
(163
)
Drum
mon
d Ch
eckl
ist
scor
e =1
6
Retro
spec
tive
coho
rtOr
dina
ry
leas
t-squ
ares
re
gres
sion
an
d ec
onom
ic
mod
els
Units
of e
ach
reso
urce
use
d by
pa
tient
Data
abs
tract
ed
from
med
ical
re
cord
s,
mic
roco
stin
g (U
S$,
1998
)
246
patie
nts
in o
ne u
rban
te
achi
ng h
ospi
tal
(Jan
.–De
c. 1
998)
Any
HAIs
, ac
cord
ing
to
Cent
er fo
r Di
seas
e Co
ntro
l an
d Pr
even
tion’s
N
atio
nal
Nos
ocom
ial
Infe
ctio
n Su
rvei
llanc
e
15.2
%10
.7 a
dditi
onal
da
ysIn
crem
enta
l cos
ts
attri
buta
ble
to
susp
ecte
d HA
I: $6
,767
; Con
firm
ed
HAI:
$15,
275
Chen
, 200
9 (5
2)
Drum
mon
d Ch
eckl
ist
scor
e =1
5
Retro
spec
tive
anal
ysis
of a
pr
ospe
ctiv
ely
asse
mbl
ed c
ohor
t
Gene
raliz
ed
linea
r mod
elin
gM
edic
al
and
surg
ical
pr
oced
ures
, m
edic
atio
ns, l
ab
inve
stig
atio
n, IC
U be
d-da
ys, i
tem
s
Hosp
ital d
atab
ase,
m
icro
cost
ing
(US$
, 20
07, c
onve
rted
from
Taiw
anes
e do
llars
)
401
NIs
in 3
20 o
f 2,
757
patie
nts,
in
four
ICUs
in o
ne
hosp
ital i
n Ta
iwan
(2
003–
2004
)
BSI,
UTI,
SSI,
resp
irato
ry tr
act
infe
ctio
n, “
and
othe
rs”
diag
nose
d ≥4
8 ho
urs
afte
r ad
mis
sion
to IC
U
14.5
NI
epis
odes
pe
r 100
ad
mis
sion
s
Not
ava
ilabl
e$1
0,01
5
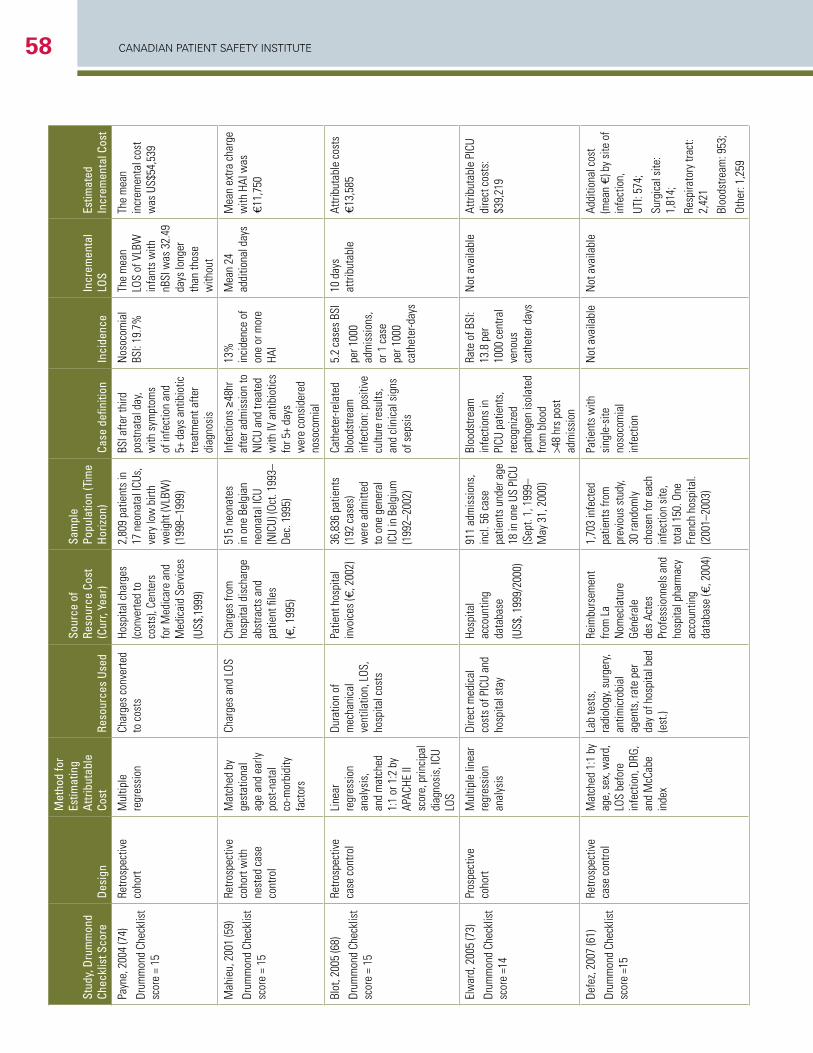
CANADIAN PAtIeNt SAfety INStItUte58
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Payn
e, 2
004
(74)
Drum
mon
d Ch
eckl
ist
scor
e =
15
Retro
spec
tive
coho
rt
Mul
tiple
re
gres
sion
Char
ges
conv
erte
d to
cos
tsHo
spita
l cha
rges
(c
onve
rted
to
cost
s), C
ente
rs
for M
edic
are
and
Med
icai
d Se
rvic
es
(US$
,199
9)
2,80
9 pa
tient
s in
17
neo
nata
l ICU
s,
very
low
birt
h w
eigh
t (VL
BW)
(199
8–19
99)
BSI a
fter t
hird
po
stna
tal d
ay,
with
sym
ptom
s of
infe
ctio
n an
d 5+
day
s an
tibio
tic
treat
men
t afte
r di
agno
sis
Nos
ocom
ial
BSI:
19.7
%
The
mea
n LO
S of
VLB
W
infa
nts
with
nB
SI w
as 3
2.49
da
ys lo
nger
th
an th
ose
with
out
The
mea
n in
crem
enta
l cos
t w
as U
S$54
,539
Mah
ieu,
200
1 (5
9)
Drum
mon
d Ch
eckl
ist
scor
e =
15
Retro
spec
tive
coho
rt w
ith
nest
ed c
ase
cont
rol
Mat
ched
by
gest
atio
nal
age
and
early
po
st-n
atal
co
-mor
bidi
ty
fact
ors
Char
ges
and
LOS
Char
ges
from
ho
spita
l dis
char
ge
abst
ract
s an
d pa
tient
file
s
(€, 1
995)
515
neon
ates
in
one
Bel
gian
ne
onat
al IC
U (N
ICU)
(Oct
. 199
3–De
c. 1
995)
Infe
ctio
ns ≥
48hr
af
ter a
dmis
sion
to
NIC
U an
d tre
ated
w
ith IV
ant
ibio
tics
for 5
+ da
ys
wer
e co
nsid
ered
no
soco
mia
l
13%
in
cide
nce
of
one
or m
ore
HAI
Mea
n 24
ad
ditio
nal d
ays
Mea
n ex
tra c
harg
e w
ith H
AI w
as
€11,
750
Blot
, 200
5 (6
8)
Drum
mon
d Ch
eckl
ist
scor
e =
15
Retro
spec
tive
case
con
trol
Line
ar
regr
essi
on
anal
ysis
, an
d m
atch
ed
1:1
or 1
:2 b
y AP
ACHE
II
scor
e, p
rinci
pal
diag
nosi
s, IC
U LO
S
Dura
tion
of
mec
hani
cal
vent
ilatio
n, L
OS,
hosp
ital c
osts
Patie
nt h
ospi
tal
invo
ices
(€, 2
002)
36,8
36 p
atie
nts
(192
cas
es)
wer
e ad
mitt
ed
to o
ne g
ener
al
ICU
in B
elgi
um
(199
2–20
02)
Cath
eter
-rela
ted
bloo
dstre
am
infe
ctio
n: p
ositi
ve
cultu
re re
sults
, an
d cl
inic
al s
igns
of
sep
sis
5.2
case
s BS
I
per 1
000
adm
issi
ons,
or
1 c
ase
per 1
000
cath
eter
-day
s
10 d
ays
attri
buta
ble
Attri
buta
ble
cost
s €1
3,58
5
Elw
ard,
200
5 (7
3)
Drum
mon
d Ch
eckl
ist
scor
e =1
4
Pros
pect
ive
coho
rtM
ultip
le li
near
re
gres
sion
an
alys
is
Dire
ct m
edic
al
cost
s of
PIC
U an
d ho
spita
l sta
y
Hosp
ital
acco
untin
g da
taba
se
(US$
, 199
9/20
00)
911
adm
issi
ons,
in
cl. 5
6 ca
se
patie
nts u
nder
age
18
in o
ne U
S PI
CU
(Sep
t. 1,
199
9–M
ay 3
1, 2
000)
Bloo
dstre
am
infe
ctio
ns in
PI
CU p
atie
nts,
re
cogn
ized
path
ogen
isol
ated
fro
m b
lood
>4
8 hr
s po
st
adm
issi
on
Rate
of B
SI:
13.8
per
10
00 c
entra
l ve
nous
ca
thet
er d
ays
Not
ava
ilabl
eAt
tribu
tabl
e PI
CU
dire
ct c
osts
: $3
9,21
9
Defe
z, 20
07 (6
1)
Drum
mon
d Ch
eckl
ist
scor
e =1
5
Retro
spec
tive
case
con
trol
Mat
ched
1:1
by
age,
sex
, war
d,
LOS
befo
re
infe
ctio
n, D
RG,
and
McC
abe
inde
x
Lab
test
s,
radi
olog
y, su
rger
y, an
timic
robi
al
agen
ts, r
ate
per
day
of h
ospi
tal b
ed
(est
.)
Reim
burs
emen
t fro
m L
a N
omec
latu
re
Géné
rale
de
s Ac
tes
Prof
essi
onne
ls a
nd
hosp
ital p
harm
acy
acco
untin
g da
taba
se (€
, 200
4)
1,70
3 in
fect
ed
patie
nts
from
pr
evio
us s
tudy
, 30
rand
omly
ch
osen
for e
ach
infe
ctio
n si
te,
tota
l 150
. One
Fr
ench
hos
pita
l. (2
001–
2003
)
Patie
nts
with
si
ngle
-site
no
soco
mia
l in
fect
ion
Not
ava
ilabl
eN
ot a
vaila
ble
Addi
tiona
l cos
t (m
ean
€) b
y si
te o
f in
fect
ion,
UTI:
574;
Surg
ical
site
: 1,
814;
Resp
irato
ry tr
act:
2,42
1
Bloo
dstre
am: 9
53;
Othe
r: 1,
259
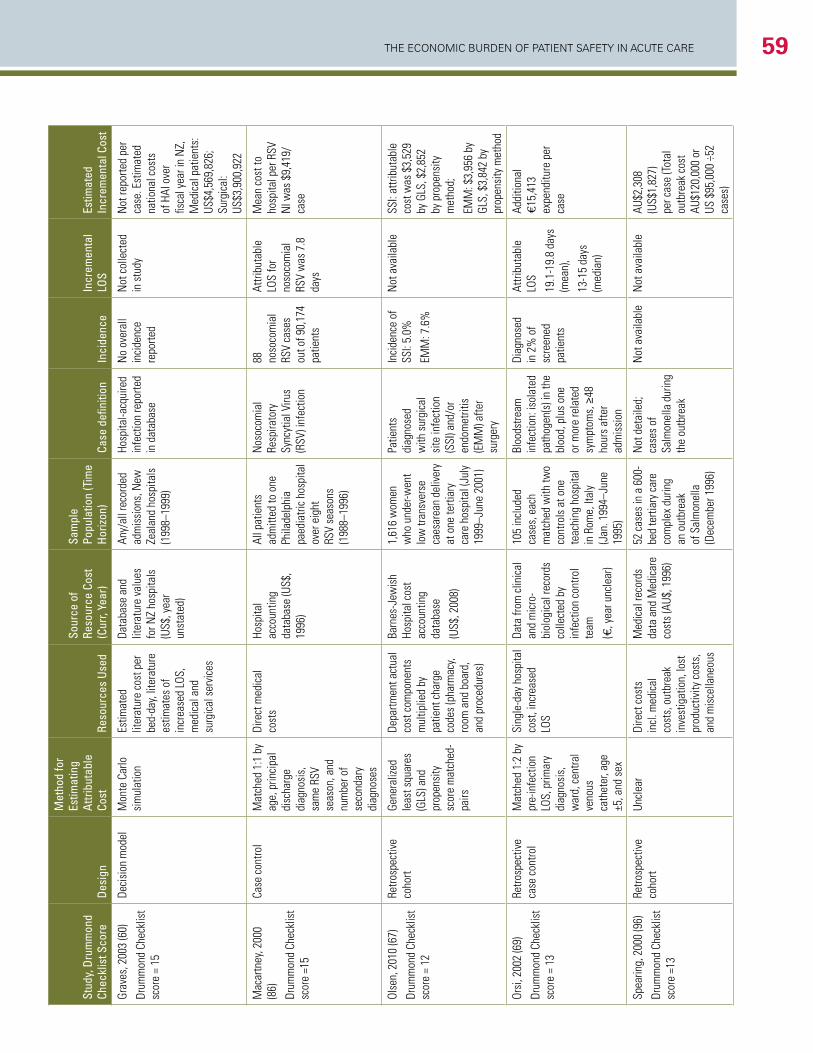
The economic Burden of PaTienT SafeTy in acuTe care 59
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Grav
es, 2
003
(60)
Drum
mon
d Ch
eckl
ist
scor
e =
15
Deci
sion
mod
elM
onte
Car
lo
sim
ulat
ion
Estim
ated
lit
erat
ure
cost
per
be
d-da
y, lit
erat
ure
estim
ates
of
incr
ease
d LO
S,
med
ical
and
su
rgic
al s
ervi
ces
Data
base
and
lit
erat
ure
valu
es
for N
Z ho
spita
ls
(US$
, yea
r un
stat
ed)
Any/
all r
ecor
ded
adm
issi
ons,
New
Ze
alan
d ho
spita
ls
(199
8–19
99)
Hosp
ital-a
cqui
red
infe
ctio
n re
porte
d in
dat
abas
e
No
over
all
inci
denc
e re
porte
d
Not
col
lect
ed
in s
tudy
Not
repo
rted
per
case
. Est
imat
ed
natio
nal c
osts
of
HAI
ove
r fis
cal y
ear i
n N
Z,
Med
ical
pat
ient
s:
US$4
,569
,826
; Su
rgic
al:
US$3
,900
,922
Mac
artn
ey, 2
000
(86)
Drum
mon
d Ch
eckl
ist
scor
e =1
5
Case
con
trol
Mat
ched
1:1
by
age,
prin
cipa
l di
scha
rge
diag
nosi
s,
sam
e RS
V se
ason
, and
nu
mbe
r of
seco
ndar
y di
agno
ses
Dire
ct m
edic
al
cost
sHo
spita
l ac
coun
ting
data
base
(US$
, 19
96)
All p
atie
nts
adm
itted
to o
ne
Phila
delp
hia
paed
iatri
c ho
spita
l ov
er e
ight
RS
V se
ason
s (1
988–
1996
)
Nos
ocom
ial
Resp
irato
ry
Sync
ytia
l Viru
s (R
SV) i
nfec
tion
88
noso
com
ial
RSV
case
s ou
t of 9
0,17
4 pa
tient
s
Attri
buta
ble
LOS
for
noso
com
ial
RSV
was
7.8
da
ys
Mea
n co
st to
ho
spita
l per
RSV
N
I was
$9,
419/
case
Olse
n, 2
010
(67)
Drum
mon
d Ch
eckl
ist
scor
e =
12
Retro
spec
tive
coho
rtGe
nera
lized
le
ast s
quar
es
(GLS
) and
pr
open
sity
sc
ore
mat
ched
-pa
irs
Depa
rtmen
t act
ual
cost
com
pone
nts
mul
tiplie
d by
pa
tient
cha
rge
code
s (p
harm
acy,
room
and
boa
rd,
and
proc
edur
es)
Barn
es-J
ewis
h Ho
spita
l cos
t ac
coun
ting
data
base
(US$
, 200
8)
1,61
6 w
omen
w
ho u
nder
-wen
t lo
w tr
ansv
erse
ca
esar
ean
deliv
ery
at o
ne te
rtiar
y ca
re h
ospi
tal (
July
19
99–J
une
2001
)
Patie
nts
diag
nose
d w
ith s
urgi
cal
site
infe
ctio
n (S
SI) a
nd/o
r en
dom
etrit
is
(EM
M) a
fter
surg
ery
Inci
denc
e of
SS
I: 5.
0%
EMM
: 7.6
%
Not
ava
ilabl
eSS
I: at
tribu
tabl
e co
st w
as $
3,52
9 by
GLS
, $2,
852
by p
rope
nsity
m
etho
d;
EMM
: $3,
956
by
GLS,
$3,
842
by
prop
ensi
ty m
etho
d
Orsi
, 200
2 (6
9)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Retro
spec
tive
case
con
trol
Mat
ched
1:2
by
pre-
infe
ctio
n LO
S, p
rimar
y di
agno
sis,
w
ard,
cen
tral
veno
us
cath
eter
, age
±5
, and
sex
Sing
le-d
ay h
ospi
tal
cost
, inc
reas
ed
LOS
Data
from
clin
ical
an
d m
icro
-bi
olog
ical
reco
rds
colle
cted
by
infe
ctio
n co
ntro
l te
am
(€, y
ear u
ncle
ar)
105
incl
uded
ca
ses,
eac
h m
atch
ed w
ith tw
o co
ntro
ls a
t one
te
achi
ng h
ospi
tal
in R
ome,
Ital
y (J
an. 1
994–
June
19
95)
Bloo
dstre
am
infe
ctio
n: is
olat
ed
path
ogen
(s) i
n th
e bl
ood,
plu
s on
e or
mor
e re
late
d sy
mpt
oms,
≥48
ho
urs
afte
r ad
mis
sion
Diag
nose
d in
2%
of
scre
ened
pa
tient
s
Attri
buta
ble
LOS
19.1
-19.
8 da
ys
(mea
n),
13-1
5 da
ys
(med
ian)
Addi
tiona
l €1
5,41
3 ex
pend
iture
per
ca
se
Spea
ring,
200
0 (9
6)
Drum
mon
d Ch
eckl
ist
scor
e =1
3
Retro
spec
tive
coho
rtUn
clea
rDi
rect
cos
ts
incl
. med
ical
co
sts,
out
brea
k in
vest
igat
ion,
lost
pr
oduc
tivity
cos
ts,
and
mis
cella
neou
s
Med
ical
reco
rds
data
and
Med
icar
e co
sts
(AU$
, 199
6)
52 c
ases
in a
600
-be
d te
rtiar
y ca
re
com
plex
dur
ing
an o
utbr
eak
of S
alm
onel
la
(Dec
embe
r 199
6)
Not
det
aile
d;
case
s of
Sa
lmon
ella
dur
ing
the
outb
reak
Not
ava
ilabl
eN
ot a
vaila
ble
AU$2
,308
(U
S$1,
827)
pe
r cas
e (To
tal
outb
reak
cos
t AU
$120
,000
or
US $
95,0
00 ÷
52
case
s)
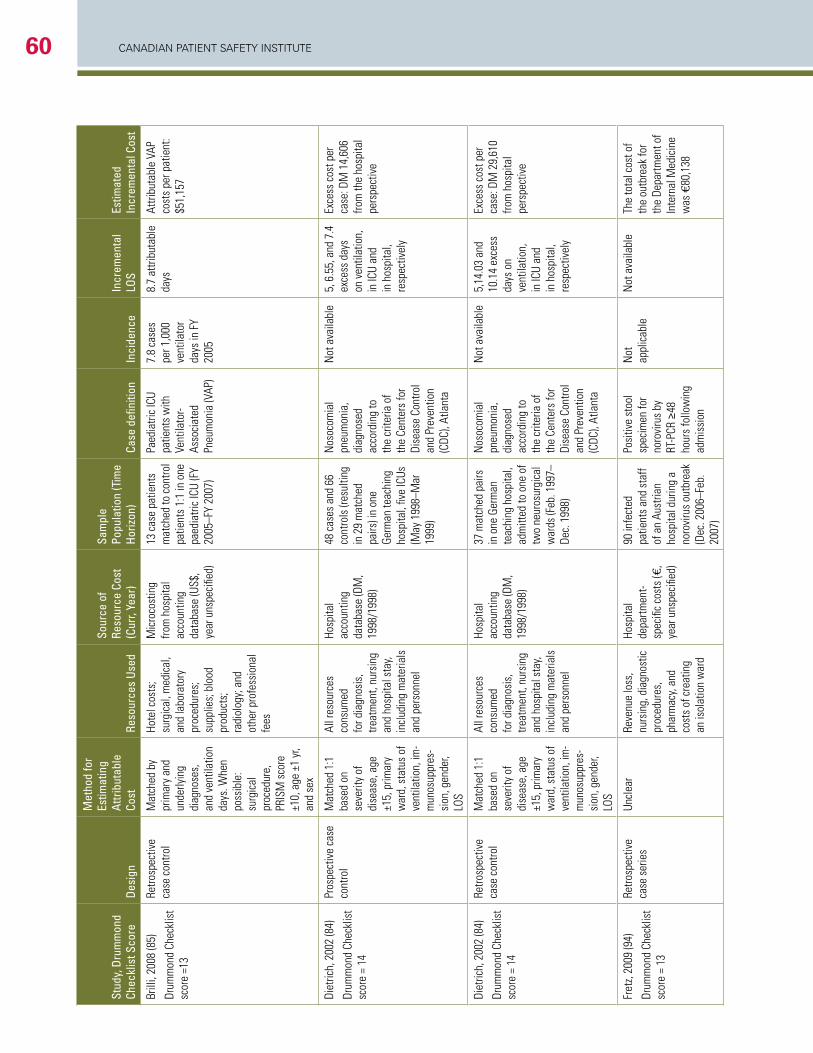
CANADIAN PAtIeNt SAfety INStItUte60
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Brill
i, 20
08 (8
5)
Drum
mon
d Ch
eckl
ist
scor
e =1
3
Retro
spec
tive
case
con
trol
Mat
ched
by
prim
ary
and
unde
rlyin
g di
agno
ses,
an
d ve
ntila
tion
days
. Whe
n po
ssib
le:
surg
ical
pr
oced
ure,
PR
ISM
sco
re
±10,
age
±1
yr,
and
sex
Hote
l cos
ts;
surg
ical
, med
ical
, an
d la
bora
tory
pr
oced
ures
; su
pplie
s; b
lood
pr
oduc
ts;
radi
olog
y; a
nd
othe
r pro
fess
iona
l fe
es
Mic
roco
stin
g fro
m h
ospi
tal
acco
untin
g da
taba
se (U
S$,
year
uns
peci
fied)
13 c
ase
patie
nts
mat
ched
to co
ntro
l pa
tient
s 1:
1 in
one
pa
edia
tric
ICU
(FY
2005
–FY
2007
)
Paed
iatri
c IC
U pa
tient
s w
ith
Vent
ilato
r-As
soci
ated
Pn
eum
onia
(VAP
)
7.8
case
s pe
r 1,0
00
vent
ilato
r da
ys in
FY
2005
8.7
attri
buta
ble
days
At
tribu
tabl
e VA
P co
sts
per p
atie
nt:
$51,
157
Diet
rich,
200
2 (8
4)
Drum
mon
d Ch
eckl
ist
scor
e =
14
Pros
pect
ive
case
co
ntro
lM
atch
ed 1
:1
base
d on
se
verit
y of
di
seas
e, a
ge
±15,
prim
ary
war
d, s
tatu
s of
ve
ntila
tion,
im-
mun
osup
pres
-si
on, g
ende
r, LO
S
All r
esou
rces
co
nsum
ed
for d
iagn
osis
, tre
atm
ent,
nurs
ing
and
hosp
ital s
tay,
incl
udin
g m
ater
ials
an
d pe
rson
nel
Hosp
ital
acco
untin
g da
taba
se (D
M,
1998
/199
8)
48 c
ases
and
66
cont
rols
(res
ultin
g in
29
mat
ched
pa
irs) i
n on
e Ge
rman
teac
hing
ho
spita
l, fiv
e IC
Us
(May
199
8–M
ar
1999
)
Nos
ocom
ial
pneu
mon
ia,
diag
nose
d ac
cord
ing
to
the
crite
ria o
f th
e Ce
nter
s fo
r Di
seas
e Co
ntro
l an
d Pr
even
tion
(CDC
), At
lant
a
Not
ava
ilabl
e5,
6.5
5, a
nd 7
.4
exce
ss d
ays
on v
entil
atio
n,
in IC
U an
d in
hos
pita
l, re
spec
tivel
y
Exce
ss c
ost p
er
case
: DM
14,
606
from
the
hosp
ital
pers
pect
ive
Diet
rich,
200
2 (8
4)
Drum
mon
d Ch
eckl
ist
scor
e =
14
Retro
spec
tive
case
con
trol
Mat
ched
1:1
ba
sed
on
seve
rity
of
dise
ase,
age
±1
5, p
rimar
y w
ard,
sta
tus
of
vent
ilatio
n, im
-m
unos
uppr
es-
sion
, gen
der,
LOS
All r
esou
rces
co
nsum
ed
for d
iagn
osis
, tre
atm
ent,
nurs
ing
and
hosp
ital s
tay,
incl
udin
g m
ater
ials
an
d pe
rson
nel
Hosp
ital
acco
untin
g da
taba
se (D
M,
1998
/199
8)
37 m
atch
ed p
airs
in
one
Ger
man
te
achi
ng h
ospi
tal,
adm
itted
to o
ne o
f tw
o ne
uros
urgi
cal
war
ds (F
eb. 1
997–
Dec.
199
8)
Nos
ocom
ial
pneu
mon
ia,
diag
nose
d ac
cord
ing
to
the
crite
ria o
f th
e Ce
nter
s fo
r Di
seas
e Co
ntro
l an
d Pr
even
tion
(CDC
), At
lant
a
Not
ava
ilabl
e5,
14.0
3 an
d 10
.14
exce
ss
days
on
vent
ilatio
n,
in IC
U an
d in
hos
pita
l, re
spec
tivel
y
Exce
ss c
ost p
er
case
: DM
29,
610
from
hos
pita
l pe
rspe
ctiv
e
Fret
z, 20
09 (9
4)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Retro
spec
tive
case
ser
ies
Uncl
ear
Reve
nue
loss
, nu
rsin
g, d
iagn
ostic
pr
oced
ures
, ph
arm
acy,
and
cost
s of
cre
atin
g an
isol
atio
n w
ard
Hosp
ital
depa
rtmen
t-sp
ecifi
c co
sts
(€,
year
uns
peci
fied)
90 in
fect
ed
patie
nts
and
staf
f of
an
Aust
rian
hosp
ital d
urin
g a
noro
viru
s ou
tbre
ak
(Dec
. 200
6–Fe
b.
2007
)
Posi
tive
stoo
l sp
ecim
en fo
r no
rovi
rus
by
RT-P
CR ≥
48
hour
s fo
llow
ing
adm
issi
on
Not
ap
plic
able
Not
ava
ilabl
eTh
e to
tal c
ost o
f th
e ou
tbre
ak fo
r th
e De
partm
ent o
f In
tern
al M
edic
ine
was
€80
,138
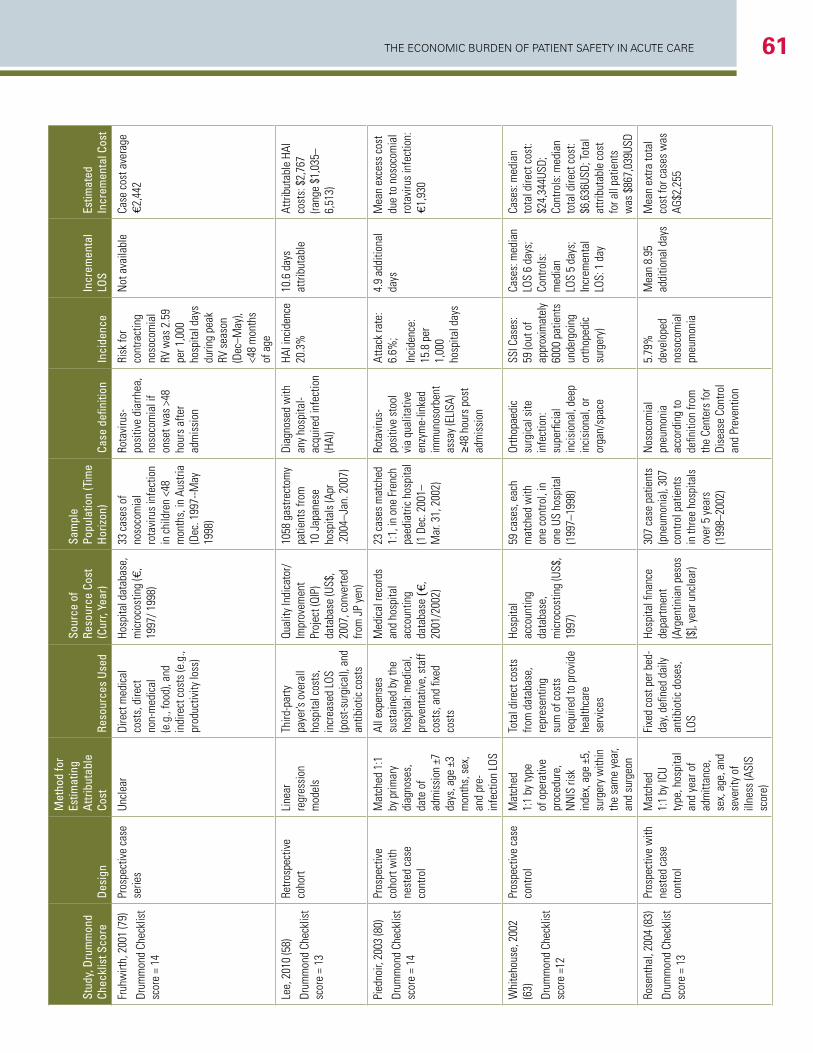
The economic Burden of PaTienT SafeTy in acuTe care 61
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Fruh
wirt
h, 2
001
(79)
Drum
mon
d Ch
eckl
ist
scor
e =
14
Pros
pect
ive
case
se
ries
Uncl
ear
Dire
ct m
edic
al
cost
s, d
irect
no
n-m
edic
al
(e.g
., fo
od),
and
indi
rect
cos
ts (e
.g.,
prod
uctiv
ity lo
ss)
Hosp
ital d
atab
ase,
m
icro
cost
ing
(€,
1997
/ 199
8)
33 c
ases
of
noso
com
ial
rota
viru
s in
fect
ion
in c
hild
ren
<48
mon
ths,
in A
ustri
a (D
ec. 1
997-
-May
19
98)
Rota
viru
s-po
sitiv
e di
arrh
ea,
noso
com
ial i
f on
set w
as >
48
hour
s af
ter
adm
issi
on
Risk
for
cont
ract
ing
noso
com
ial
RV w
as 2
.59
per 1
,000
ho
spita
l day
s du
ring
peak
RV
sea
son
(Dec
–May
), <4
8 m
onth
s of
age
Not
ava
ilabl
eCa
se c
ost a
vera
ge
€2,4
42
Lee,
201
0 (5
8)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Retro
spec
tive
coho
rtLi
near
re
gres
sion
m
odel
s
Third
-par
ty
paye
r’s o
vera
ll ho
spita
l cos
ts,
incr
ease
d LO
S (p
ost-s
urgi
cal),
and
an
tibio
tic c
osts
Qual
ity In
dica
tor/
Im
prov
emen
t Pr
ojec
t (QI
P)
data
base
(US$
, 20
07, c
onve
rted
from
JP
yen)
1058
gas
trect
omy
patie
nts
from
10
Jap
anes
e ho
spita
ls (A
pr
.200
4–Ja
n. 2
007)
Diag
nose
d w
ith
any
hosp
ital-
acqu
ired
infe
ctio
n (H
AI)
HAI i
ncid
ence
20
.3%
10
.6 d
ays
attri
buta
ble
Attri
buta
ble
HAI
cost
s: $
2,76
7 (ra
nge
$1,0
35–
6,51
3)
Pied
noir,
200
3 (8
0)
Drum
mon
d Ch
eckl
ist
scor
e =
14
Pros
pect
ive
coho
rt w
ith
nest
ed c
ase
cont
rol
Mat
ched
1:1
by
prim
ary
diag
nose
s,
date
of
adm
issi
on ±
7 da
ys, a
ge ±
3 m
onth
s, s
ex,
and
pre-
infe
ctio
n LO
S
All e
xpen
ses
sust
aine
d by
the
hosp
ital:
med
ical
, pr
even
tativ
e, s
taff
cost
s, a
nd fi
xed
cost
s
Med
ical
reco
rds
and
hosp
ital
acco
untin
g da
taba
se (€
, 20
01/2
002)
23 c
ases
mat
ched
1:
1, in
one
Fre
nch
paed
iatri
c ho
spita
l (1
Dec
. 200
1–
Mar
. 31,
200
2)
Rota
viru
s-po
sitiv
e st
ool
via
qual
itativ
e en
zym
e-lin
ked
imm
unos
orbe
nt
assa
y (E
LISA
) ≥4
8 ho
urs
post
ad
mis
sion
Atta
ck ra
te:
6.6%
;
Inci
denc
e:
15.8
per
1,
000
hosp
ital d
ays
4.9
addi
tiona
l da
ysM
ean
exce
ss c
ost
due
to n
osoc
omia
l ro
tavi
rus
infe
ctio
n:
€1,9
30
Whi
teho
use,
200
2 (6
3)
Drum
mon
d Ch
eckl
ist
scor
e =1
2
Pros
pect
ive
case
co
ntro
lM
atch
ed
1:1
by ty
pe
of o
pera
tive
proc
edur
e,
NN
IS ri
sk
inde
x, a
ge ±
5,
surg
ery
with
in
the
sam
e ye
ar,
and
surg
eon
Tota
l dire
ct c
osts
fro
m d
atab
ase,
re
pres
entin
g su
m o
f cos
ts
requ
ired
to p
rovi
de
heal
thca
re
serv
ices
Hosp
ital
acco
untin
g da
taba
se,
mic
roco
stin
g (U
S$,
1997
)
59 c
ases
, eac
h m
atch
ed w
ith
one
cont
rol,
in
one
US h
ospi
tal
(199
7–19
98)
Orth
opae
dic
surg
ical
site
in
fect
ion:
su
perfi
cial
in
cisi
onal
, dee
p in
cisi
onal
, or
orga
n/sp
ace
SSI C
ases
: 59
(out
of
appr
oxim
atel
y 60
00 p
atie
nts
unde
rgoi
ng
orth
oped
ic
surg
ery)
Case
s: m
edia
n LO
S 6
days
; Co
ntro
ls:
med
ian
LOS
5 da
ys;
Incr
emen
tal
LOS:
1 d
ay
Case
s: m
edia
n to
tal d
irect
cos
t: $2
4,34
4USD
; Co
ntro
ls: m
edia
n to
tal d
irect
cos
t: $6
,636
USD;
Tota
l at
tribu
tabl
e co
st
for a
ll pa
tient
s w
as $
867,
039U
SD
Rose
ntha
l, 20
04 (8
3)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Pros
pect
ive
with
ne
sted
cas
e co
ntro
l
Mat
ched
1:
1 by
ICU
type
, hos
pita
l an
d ye
ar o
f ad
mitt
ance
, se
x, a
ge, a
nd
seve
rity
of
illne
ss (A
SIS
scor
e)
Fixe
d co
st p
er b
ed-
day,
defin
ed d
aily
an
tibio
tic d
oses
, LO
S
Hosp
ital fi
nanc
e de
partm
ent
(Arg
entin
ian
peso
s [$
], ye
ar u
ncle
ar)
307
case
pat
ient
s (p
neum
onia
), 30
7 co
ntro
l pat
ient
s in
thre
e ho
spita
ls
over
5 y
ears
(1
998–
2002
)
Nos
ocom
ial
pneu
mon
ia
acco
rdin
g to
de
finiti
on fr
om
the
Cent
ers
for
Dise
ase
Cont
rol
and
Prev
entio
n
5.79
%
deve
lope
d no
soco
mia
l pn
eum
onia
Mea
n 8.
95
addi
tiona
l day
sM
ean
extra
tota
l co
st fo
r cas
es w
as
AG$2
,255
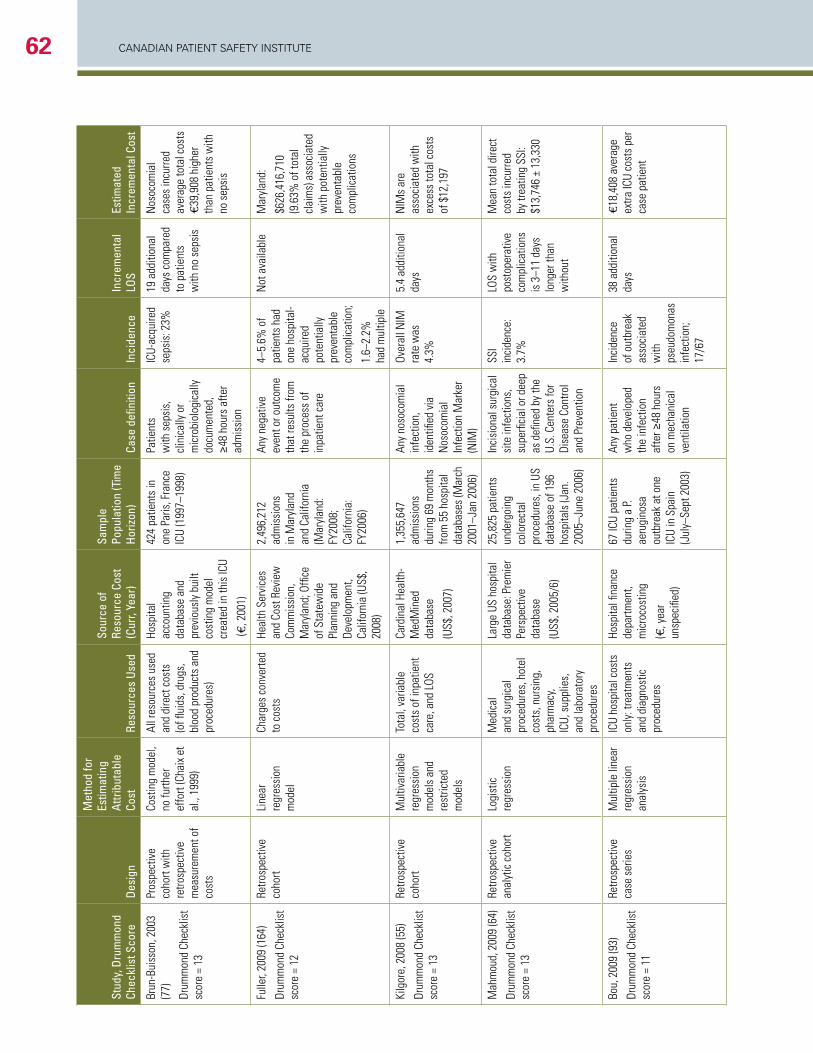
CANADIAN PAtIeNt SAfety INStItUte62
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Brun
-Bui
sson
, 200
3 (7
7)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Pros
pect
ive
coho
rt w
ith
retro
spec
tive
mea
sure
men
t of
cost
s
Cost
ing
mod
el,
no fu
rther
ef
fort
(Cha
ix e
t al
., 19
99)
All r
esou
rces
use
d an
d di
rect
cos
ts
(of fl
uids
, dru
gs,
bloo
d pr
oduc
ts a
nd
proc
edur
es)
Hosp
ital
acco
untin
g da
taba
se a
nd
prev
ious
ly b
uilt
cost
ing
mod
el
crea
ted
in th
is IC
U
(€, 2
001)
424
patie
nts
in
one
Paris
, Fra
nce
ICU
(199
7–19
98)
Patie
nts
with
sep
sis,
cl
inic
ally
or
mic
robi
olog
ical
ly
docu
men
ted,
≥4
8 ho
urs
afte
r ad
mis
sion
ICU-
acqu
ired
seps
is: 2
3%
19 a
dditi
onal
da
ys c
ompa
red
to p
atie
nts
with
no
seps
is
Nos
ocom
ial
case
s in
curre
d av
erag
e to
tal c
osts
€3
9,90
8 hi
gher
th
an p
atie
nts
with
no
sep
sis
Fulle
r, 20
09 (1
64)
Drum
mon
d Ch
eckl
ist
scor
e =
12
Retro
spec
tive
coho
rtLi
near
re
gres
sion
m
odel
Char
ges
conv
erte
d to
cos
tsHe
alth
Ser
vice
s an
d Co
st R
evie
w
Com
mis
sion
, M
aryl
and;
Offi
ce
of S
tate
wid
e Pl
anni
ng a
nd
Deve
lopm
ent,
Calif
orni
a (U
S$,
2008
)
2,49
6,21
2 ad
mis
sion
s in
Mar
ylan
d an
d Ca
lifor
nia
(Mar
ylan
d:
FY20
08;
Calif
orni
a:
FY20
06)
Any
nega
tive
even
t or o
utco
me
that
resu
lts fr
om
the
proc
ess
of
inpa
tient
car
e
4–5.
6% o
f pa
tient
s ha
d on
e ho
spita
l-ac
quire
d po
tent
ially
pr
even
tabl
e co
mpl
icat
ion;
1.6–
2.2%
ha
d m
ultip
le
Not
ava
ilabl
eM
aryl
and:
$626
,416
,710
(9
.63%
of t
otal
cl
aim
s) a
ssoc
iate
d w
ith p
oten
tially
pr
even
tabl
e co
mpl
icat
ions
Kilg
ore,
200
8 (5
5)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Retro
spec
tive
coho
rtM
ultiv
aria
ble
regr
essi
on
mod
els
and
rest
ricte
d m
odel
s
Tota
l, va
riabl
e co
sts
of in
patie
nt
care
, and
LOS
Card
inal
Hea
lth-
Med
Min
ed
data
base
(US$
, 200
7)
1,35
5,64
7 ad
mis
sion
s du
ring
69 m
onth
s fro
m 5
5 ho
spita
l da
taba
ses
(Mar
ch
2001
–Jan
200
6)
Any
noso
com
ial
infe
ctio
n,
iden
tified
via
N
osoc
omia
l In
fect
ion
Mar
ker
(NIM
)
Over
all N
IM
rate
was
4.
3%
5.4
addi
tiona
l da
ys
NIM
s ar
e as
soci
ated
with
ex
cess
tota
l cos
ts
of $
12,1
97
Mah
mou
d, 2
009
(64)
Drum
mon
d Ch
eckl
ist
scor
e =
13
Retro
spec
tive
anal
ytic
coh
ort
Logi
stic
re
gres
sion
Med
ical
an
d su
rgic
al
proc
edur
es, h
otel
co
sts,
nur
sing
, ph
arm
acy,
ICU,
sup
plie
s,
and
labo
rato
ry
proc
edur
es
Larg
e US
hos
pita
l da
taba
se: P
rem
ier
Pers
pect
ive
data
base
(US$
, 200
5/6)
25,8
25 p
atie
nts
unde
rgoi
ng
colo
rect
al
proc
edur
es, i
n US
da
taba
se o
f 196
ho
spita
ls (J
an.
2005
–Jun
e 20
06)
Inci
sion
al s
urgi
cal
site
infe
ctio
ns,
supe
rfici
al o
r dee
p as
defi
ned
by th
e U.
S. C
ente
rs fo
r Di
seas
e Co
ntro
l an
d Pr
even
tion
SSI
inci
denc
e:
3.7%
LOS
with
po
stop
erat
ive
com
plic
atio
ns
is 3
–11
days
lo
nger
than
w
ithou
t
Mea
n to
tal d
irect
co
sts
incu
rred
by tr
eatin
g SS
I: $1
3,74
6 ±
13,3
30
Bou,
200
9 (9
3)
Drum
mon
d Ch
eckl
ist
scor
e =
11
Retro
spec
tive
case
ser
ies
Mul
tiple
line
ar
regr
essi
on
anal
ysis
ICU
hosp
ital c
osts
on
ly: t
reat
men
ts
and
diag
nost
ic
proc
edur
es
Hosp
ital fi
nanc
e de
partm
ent,
mic
roco
stin
g
(€, y
ear
unsp
ecifi
ed)
67 IC
U pa
tient
s du
ring
a P.
aeru
gino
sa
outb
reak
at o
ne
ICU
in S
pain
(J
uly–
Sept
200
3)
Any
patie
nt
who
dev
elop
ed
the
infe
ctio
n af
ter ≥
48 h
ours
on
mec
hani
cal
vent
ilatio
n
Inci
denc
e of
out
brea
k as
soci
ated
w
ith
pseu
dom
onas
in
fect
ion;
17
/67
38 a
dditi
onal
da
ys€1
8,40
8 av
erag
e ex
tra IC
U co
sts
per
case
pat
ient
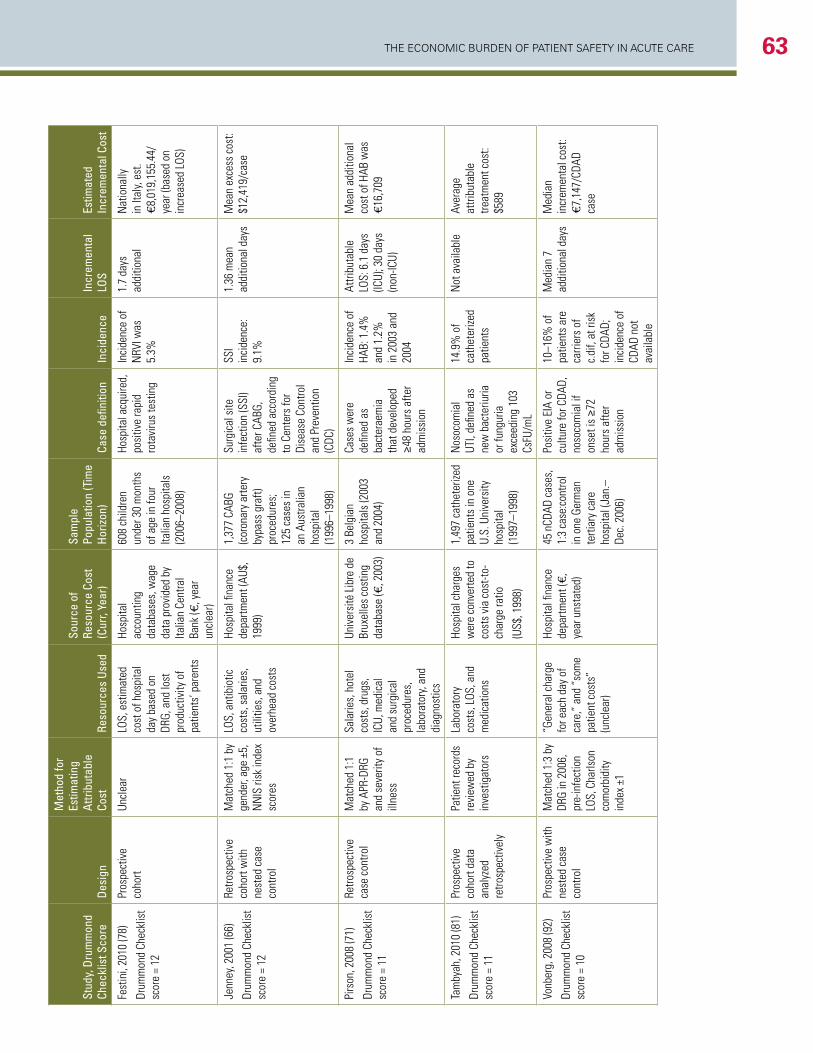
The economic Burden of PaTienT SafeTy in acuTe care 63
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Fest
ini,
2010
(78)
Drum
mon
d Ch
eckl
ist
scor
e =
12
Pros
pect
ive
coho
rtUn
clea
rLO
S, e
stim
ated
co
st o
f hos
pita
l da
y ba
sed
on
DRG,
and
lost
pr
oduc
tivity
of
patie
nts’
par
ents
Hosp
ital
acco
untin
g da
taba
ses,
wag
e da
ta p
rovi
ded
by
Italia
n Ce
ntra
l Ba
nk (€
, yea
r un
clea
r)
608
child
ren
unde
r 30
mon
ths
of a
ge in
four
Ita
lian
hosp
itals
(2
006–
2008
)
Hosp
ital a
cqui
red,
po
sitiv
e ra
pid
rota
viru
s te
stin
g
Inci
denc
e of
N
RVI w
as
5.3%
1.7
days
ad
ditio
nal
Nat
iona
lly
in It
aly,
est.
€8,0
19,1
55.4
4/ye
ar (b
ased
on
incr
ease
d LO
S)
Jenn
ey, 2
001
(66)
Drum
mon
d Ch
eckl
ist
scor
e =
12
Retro
spec
tive
coho
rt w
ith
nest
ed c
ase
cont
rol
Mat
ched
1:1
by
gend
er, a
ge ±
5,
NN
IS ri
sk in
dex
scor
es
LOS,
ant
ibio
tic
cost
s, s
alar
ies,
ut
ilitie
s, a
nd
over
head
cos
ts
Hosp
ital fi
nanc
e de
partm
ent (
AU$,
19
99)
1,37
7 CA
BG
(cor
onar
y ar
tery
by
pass
gra
ft)
proc
edur
es;
125
case
s in
an
Aus
tralia
n ho
spita
l (1
996–
1998
)
Surg
ical
site
in
fect
ion
(SSI
) af
ter C
ABG,
de
fined
acc
ordi
ng
to C
ente
rs fo
r Di
seas
e Co
ntro
l an
d Pr
even
tion
(CDC
)
SSI
inci
denc
e:
9.1%
1.36
mea
n ad
ditio
nal d
ays
Mea
n ex
cess
cos
t: $1
2,41
9/ca
se
Pirs
on, 2
008
(71)
Drum
mon
d Ch
eckl
ist
scor
e =
11
Retro
spec
tive
case
con
trol
Mat
ched
1:1
by
APR
-DRG
an
d se
verit
y of
ill
ness
Sala
ries,
hot
el
cost
s, d
rugs
, IC
U, m
edic
al
and
surg
ical
pr
oced
ures
, la
bora
tory
, and
di
agno
stic
s
Univ
ersi
té L
ibre
de
Brux
elle
s co
stin
g da
taba
se (€
, 200
3)
3 Be
lgia
n ho
spita
ls (2
003
and
2004
)
Case
s w
ere
defin
ed a
s ba
cter
aem
ia
that
dev
elop
ed
≥48
hour
s af
ter
adm
issi
on
Inci
denc
e of
HA
B: 1
.4%
an
d 1.
2%
in 2
003
and
2004
Attri
buta
ble
LOS:
6.1
day
s (IC
U); 3
0 da
ys
(non
-ICU)
Mea
n ad
ditio
nal
cost
of H
AB w
as
€16,
709
Tam
byah
, 201
0 (8
1)
Drum
mon
d Ch
eckl
ist
scor
e =
11
Pros
pect
ive
coho
rt da
ta
anal
yzed
re
trosp
ectiv
ely
Patie
nt re
cord
s re
view
ed b
y in
vest
igat
ors
Labo
rato
ry
cost
s, L
OS, a
nd
med
icat
ions
Hosp
ital c
harg
es
wer
e co
nver
ted
to
cost
s vi
a co
st-to
-ch
arge
ratio
(US$
, 199
8)
1,49
7 ca
thet
erize
d pa
tient
s in
one
U.
S. U
nive
rsity
ho
spita
l (1
997–
1998
)
Nos
ocom
ial
UTI,
defin
ed a
s ne
w b
acte
riuria
or
fung
uria
ex
ceed
ing
103
CsFU
/mL
14.9
% o
f ca
thet
erize
d pa
tient
s
Not
ava
ilabl
eAv
erag
e at
tribu
tabl
e tre
atm
ent c
ost:
$589
Vonb
erg,
200
8 (9
2)
Drum
mon
d Ch
eckl
ist
scor
e =
10
Pros
pect
ive
with
ne
sted
cas
e co
ntro
l
Mat
ched
1:3
by
DRG
in 2
006,
pr
e-in
fect
ion
LOS,
Cha
rlson
co
mor
bidi
ty
inde
x ±1
“Gen
eral
cha
rge
for e
ach
day
of
care
,” a
nd “
som
e pa
tient
cos
ts”
(unc
lear
)
Hosp
ital fi
nanc
e de
partm
ent (
€,
year
uns
tate
d)
45 n
CDAD
cas
es,
1:3
case
:con
trol
in o
ne G
erm
an
terti
ary
care
ho
spita
l (Ja
n.–
Dec.
200
6)
Posi
tive
EIA
or
cultu
re fo
r CDA
D,
noso
com
ial i
f on
set i
s ≥7
2 ho
urs
afte
r ad
mis
sion
10–1
6% o
f pa
tient
s ar
e ca
rrier
s of
c.
dif,
at ri
sk
for C
DAD;
in
cide
nce
of
CDAD
not
av
aila
ble
Med
ian
7 ad
ditio
nal d
ays
Med
ian
incr
emen
tal c
ost:
€7,1
47/C
DAD
case
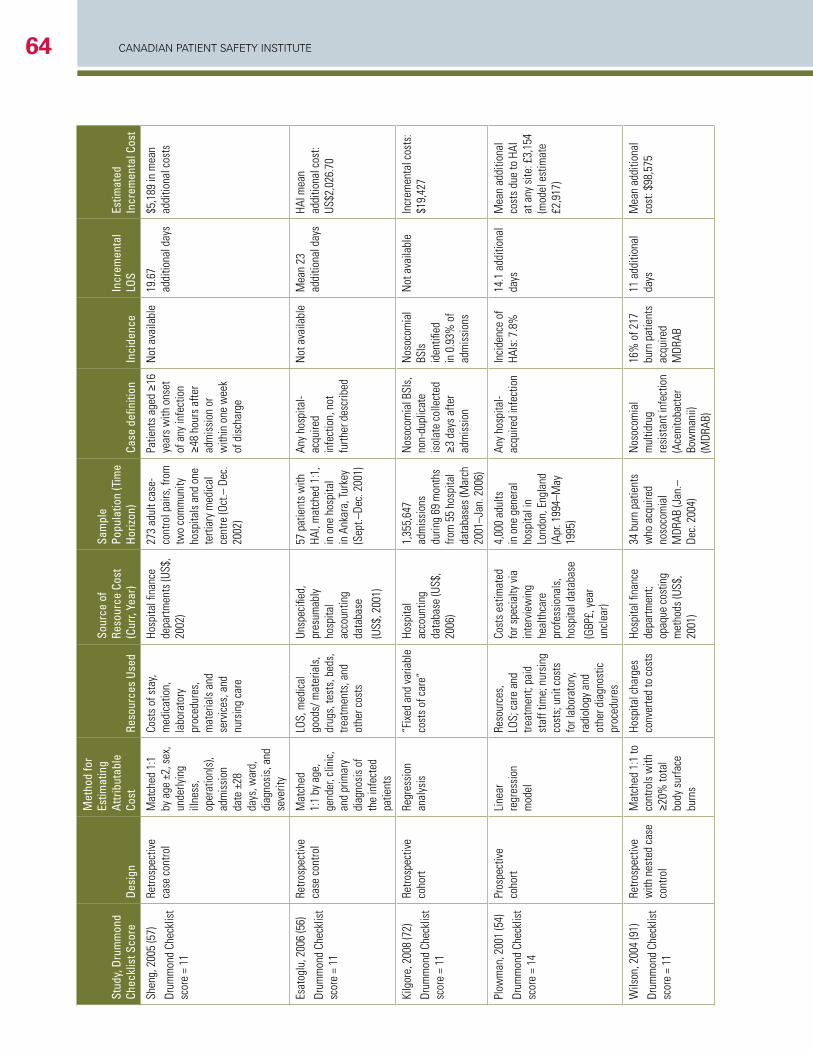
CANADIAN PAtIeNt SAfety INStItUte64
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Shen
g, 2
005
(57)
Drum
mon
d Ch
eckl
ist
scor
e =
11
Retro
spec
tive
case
con
trol
Mat
ched
1:1
by
age
±2,
sex
, un
derly
ing
illne
ss,
oper
atio
n(s)
, ad
mis
sion
da
te ±
28
days
, war
d,
diag
nosi
s, a
nd
seve
rity
Cost
s of
sta
y, m
edic
atio
n,
labo
rato
ry
proc
edur
es,
mat
eria
ls a
nd
serv
ices
, and
nu
rsin
g ca
re
Hosp
ital fi
nanc
e de
partm
ents
(US$
, 20
02)
273
adul
t cas
e-co
ntro
l pai
rs, f
rom
tw
o co
mm
unity
ho
spita
ls a
nd o
ne
terti
ary
med
ical
ce
ntre
(Oct
.– D
ec.
2002
)
Patie
nts
aged
≥16
ye
ars
with
ons
et
of a
ny in
fect
ion
≥48
hour
s af
ter
adm
issi
on o
r w
ithin
one
wee
k of
dis
char
ge
Not
ava
ilabl
e19
.67
addi
tiona
l day
s$5
,189
in m
ean
addi
tiona
l cos
ts
Esat
oglu
, 200
6 (5
6)
Drum
mon
d Ch
eckl
ist
scor
e =
11
Retro
spec
tive
case
con
trol
Mat
ched
1:
1 by
age
, ge
nder
, clin
ic,
and
prim
ary
diag
nosi
s of
th
e in
fect
ed
patie
nts
LOS,
med
ical
go
ods/
mat
eria
ls,
drug
s, te
sts,
bed
s,
treat
men
ts, a
nd
othe
r cos
ts
Unsp
ecifi
ed,
pres
umab
ly
hosp
ital
acco
untin
g da
taba
se
(US$
, 200
1)
57 p
atie
nts
with
HA
I, m
atch
ed 1
:1,
in o
ne h
ospi
tal
in A
nkar
a, Tu
rkey
(S
ept.–
Dec.
200
1)
Any
hosp
ital-
acqu
ired
infe
ctio
n, n
ot
furth
er d
escr
ibed
Not
ava
ilabl
eM
ean
23
addi
tiona
l day
s HA
I mea
n ad
ditio
nal c
ost:
US$2
,026
.70
Kilg
ore,
200
8 (7
2)
Drum
mon
d Ch
eckl
ist
scor
e =
11
Retro
spec
tive
coho
rtRe
gres
sion
an
alys
is
“Fix
ed a
nd v
aria
ble
cost
s of
car
e”Ho
spita
l ac
coun
ting
data
base
(US$
, 20
06)
1,35
5,64
7 ad
mis
sion
s du
ring
69 m
onth
s fro
m 5
5 ho
spita
l da
taba
ses
(Mar
ch
2001
–Jan
. 200
6)
Nos
ocom
ial B
SIs,
no
n-du
plic
ate
isol
ate
colle
cted
≥3
day
s af
ter
adm
issi
on
Nos
ocom
ial
BSIs
id
entifi
ed
in 0
.93%
of
adm
issi
ons
Not
ava
ilabl
eIn
crem
enta
l cos
ts:
$19,
427
Plow
man
, 200
1 (5
4)
Drum
mon
d Ch
eckl
ist
scor
e =
14
Pros
pect
ive
coho
rtLi
near
re
gres
sion
m
odel
Reso
urce
s,
LOS;
car
e an
d tre
atm
ent;
paid
st
aff t
ime;
nur
sing
co
sts;
uni
t cos
ts
for l
abor
ator
y, ra
diol
ogy
and
othe
r dia
gnos
tic
proc
edur
es
Cost
s es
timat
ed
for s
peci
alty
via
in
terv
iew
ing
heal
thca
re
prof
essi
onal
s,
hosp
ital d
atab
ase
(GBP
£, y
ear
uncl
ear)
4,00
0 ad
ults
in
one
gen
eral
ho
spita
l in
Lond
on, E
ngla
nd
(Apr
. 199
4–M
ay
1995
)
Any
hosp
ital-
acqu
ired
infe
ctio
nIn
cide
nce
of
HAIs
: 7.8
%14
.1 a
dditi
onal
da
ysM
ean
addi
tiona
l co
sts
due
to H
AI
at a
ny s
ite: £
3,15
4 (m
odel
est
imat
e £2
,917
)
Wils
on, 2
004
(91)
Drum
mon
d Ch
eckl
ist
scor
e =
11
Retro
spec
tive
with
nes
ted
case
co
ntro
l
Mat
ched
1:1
to
cont
rols
with
≥2
0% to
tal
body
sur
face
bu
rns
Hosp
ital c
harg
es
conv
erte
d to
cos
tsHo
spita
l fina
nce
depa
rtmen
t; op
aque
cos
ting
met
hods
(US$
, 20
01)
34 b
urn
patie
nts
who
acq
uire
d no
soco
mia
l M
DRAB
(Jan
.–De
c. 2
004)
Nos
ocom
ial
mul
tidru
g re
sist
ant i
nfec
tion
(Ace
nito
bact
er
Bow
man
ii)
(MDR
AB)
16%
of 2
17
burn
pat
ient
s ac
quire
d M
DRAB
11 a
dditi
onal
da
ysM
ean
addi
tiona
l co
st: $
98,5
75
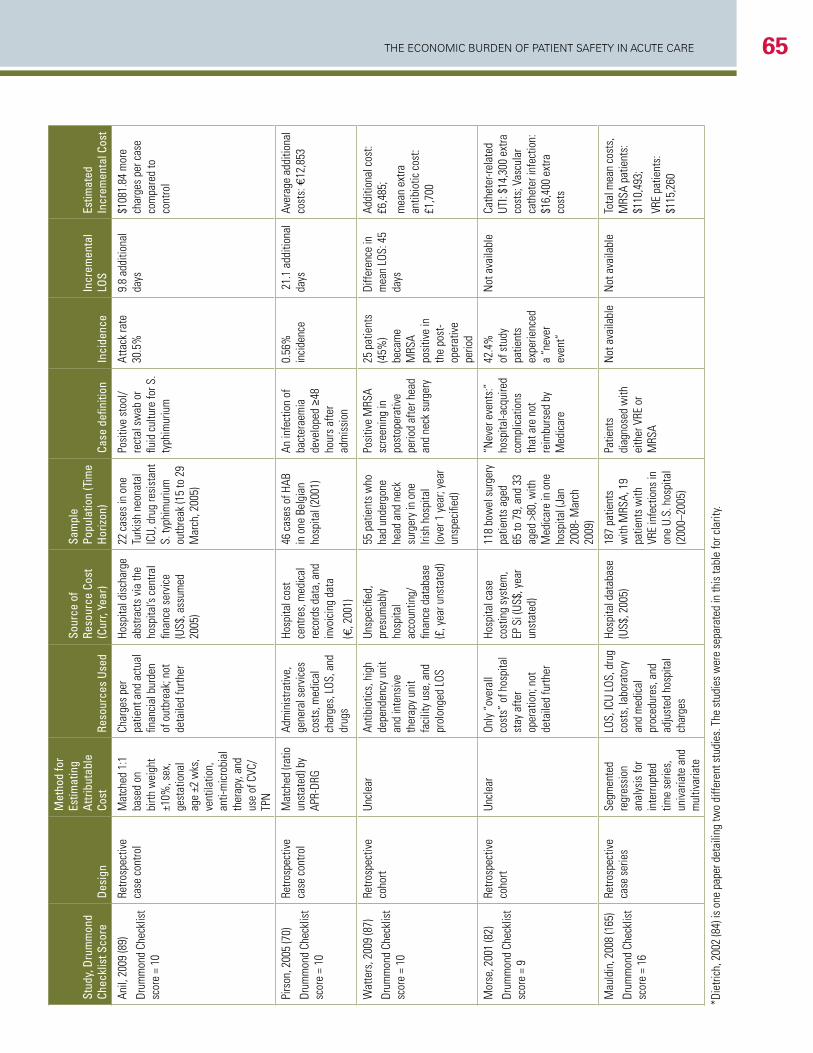
The economic Burden of PaTienT SafeTy in acuTe care 65
Stud
y, D
rum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Anil,
200
9 (8
9)
Drum
mon
d Ch
eckl
ist
scor
e =
10
Retro
spec
tive
case
con
trol
Mat
ched
1:1
ba
sed
on
birth
wei
ght
±10%
, sex
, ge
stat
iona
l ag
e ±2
wks
, ve
ntila
tion,
an
ti-m
icro
bial
th
erap
y, an
d us
e of
CVC
/TP
N
Char
ges
per
patie
nt a
nd a
ctua
l fin
anci
al b
urde
n of
out
brea
k; n
ot
deta
iled
furth
er
Hosp
ital d
isch
arge
ab
stra
cts
via
the
hosp
ital’s
cen
tral
finan
ce s
ervi
ce
(US$
, ass
umed
20
05)
22 c
ases
in o
ne
Turk
ish
neon
atal
IC
U, d
rug
resi
stan
t S.
typh
imur
ium
ou
tbre
ak (1
5 to
29
Mar
ch, 2
005)
Posi
tive
stoo
l/re
ctal
sw
ab o
r flu
id c
ultu
re fo
r S.
typh
imur
ium
Atta
ck ra
te
30.5
%9.
8 ad
ditio
nal
days
$1
081.
84 m
ore
char
ges
per c
ase
com
pare
d to
co
ntro
l
Pirs
on, 2
005
(70)
Drum
mon
d Ch
eckl
ist
scor
e =
10
Retro
spec
tive
case
con
trol
Mat
ched
(rat
io
unst
ated
) by
APR-
DRG
Adm
inis
trativ
e,
gene
ral s
ervi
ces
cost
s, m
edic
al
char
ges,
LOS
, and
dr
ugs
Hosp
ital c
ost
cent
res,
med
ical
re
cord
s da
ta, a
nd
invo
icin
g da
ta
(€, 2
001)
46 c
ases
of H
AB
in o
ne B
elgi
an
hosp
ital (
2001
)
An in
fect
ion
of
bact
erae
mia
de
velo
ped
≥48
hour
s af
ter
adm
issi
on
0.56
%
inci
denc
e 2
1.1
addi
tiona
l da
ysAv
erag
e ad
ditio
nal
cost
s: €
12,8
53
Wat
ters
, 200
9 (8
7)
Drum
mon
d Ch
eckl
ist
scor
e =
10
Retro
spec
tive
coho
rtUn
clea
rAn
tibio
tics,
hig
h de
pend
ency
uni
t an
d in
tens
ive
ther
apy
unit
faci
lity
use,
and
pr
olon
ged
LOS
Unsp
ecifi
ed,
pres
umab
ly
hosp
ital
acco
untin
g/
finan
ce d
atab
ase
(£, y
ear u
nsta
ted)
55 p
atie
nts
who
ha
d un
derg
one
head
and
nec
k su
rger
y in
one
Iri
sh h
ospi
tal
(ove
r 1 y
ear;
year
un
spec
ified
)
Posi
tive
MRS
A sc
reen
ing
in
post
oper
ativ
e pe
riod
afte
r hea
d an
d ne
ck s
urge
ry
25 p
atie
nts
(45%
) be
cam
e M
RSA
posi
tive
in
the
post
-op
erat
ive
perio
d
Diffe
renc
e in
m
ean
LOS:
45
days
Addi
tiona
l cos
t: £6
,485
;
mea
n ex
tra
antib
iotic
cos
t: £1
,700
Mor
se, 2
001
(82)
Drum
mon
d Ch
eckl
ist
scor
e =
9
Retro
spec
tive
coho
rtUn
clea
r On
ly “
over
all
cost
s” o
f hos
pita
l st
ay a
fter
oper
atio
n; n
ot
deta
iled
furth
er
Hosp
ital c
ase
cost
ing
syst
em,
EP S
i (US
$, y
ear
unst
ated
)
118
bow
el s
urge
ry
patie
nts
aged
65
to 7
9, a
nd 3
3 ag
ed >
80, w
ith
Med
icar
e in
one
ho
spita
l (Ja
n 20
08- M
arch
20
09)
“Nev
er e
vent
s:”
hosp
ital-a
cqui
red
com
plic
atio
ns
that
are
not
re
imbu
rsed
by
Med
icar
e
42.4
%
of s
tudy
pa
tient
s ex
perie
nced
a
“nev
er
even
t”
Not
ava
ilabl
eCa
thet
er-re
late
d UT
I: $1
4,30
0 ex
tra
cost
s; V
ascu
lar
cath
eter
infe
ctio
n:
$16,
400
extra
co
sts
Mau
ldin
, 200
8 (1
65)
Drum
mon
d Ch
eckl
ist
scor
e =
16
Retro
spec
tive
case
ser
ies
Segm
ente
d re
gres
sion
an
alys
is fo
r in
terru
pted
tim
e se
ries,
un
ivar
iate
and
m
ultiv
aria
te
LOS,
ICU
LOS,
dru
g co
sts,
labo
rato
ry
and
med
ical
pr
oced
ures
, and
ad
just
ed h
ospi
tal
char
ges
Hosp
ital d
atab
ase
(US$
, 200
5)18
7 pa
tient
s w
ith M
RSA,
19
patie
nts
with
VR
E in
fect
ions
in
one
U.S.
hos
pita
l (2
000–
2005
)
Patie
nts
diag
nose
d w
ith
eith
er V
RE o
r M
RSA
Not
ava
ilabl
eN
ot a
vaila
ble
Tota
l mea
n co
sts,
M
RSA
patie
nts:
$1
10,4
93;
VRE
patie
nts:
$1
15,2
60
*Die
trich
, 200
2 (8
4) is
one
pap
er d
etai
ling
two
diffe
rent
stu
dies
. The
stu
dies
wer
e se
para
ted
in th
is ta
ble
for c
larit
y.
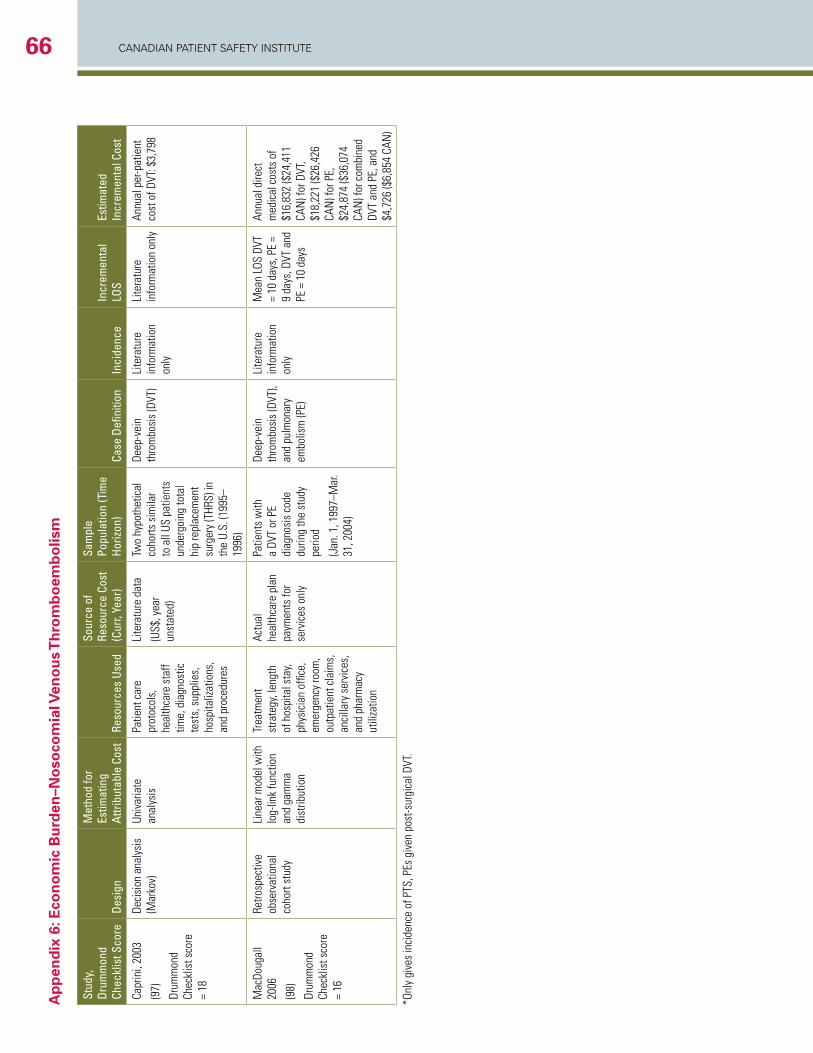
CANADIAN PAtIeNt SAfety INStItUte66a
pp
end
ix 6
: eco
no
mic
Bu
rden
–no
soco
mia
l ven
ou
s T
hro
mb
oem
bo
lism
Stud
y,
Drum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
Defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Capr
ini,
2003
(97)
Drum
mon
d Ch
eckl
ist s
core
=
18
Deci
sion
ana
lysi
s (M
arko
v)Un
ivar
iate
an
alys
is
Patie
nt c
are
prot
ocol
s,
heal
thca
re s
taff
time,
dia
gnos
tic
test
s, s
uppl
ies,
ho
spita
lizat
ions
, an
d pr
oced
ures
Lite
ratu
re d
ata
(US$
, yea
r un
stat
ed)
Two
hypo
thet
ical
co
horts
sim
ilar
to a
ll US
pat
ient
s un
derg
oing
tota
l hi
p re
plac
emen
t su
rger
y (T
HRS)
in
the
U.S.
(199
5–19
96)
Deep
-vei
n th
rom
bosi
s (D
VT)
Lite
ratu
re
info
rmat
ion
only
Lite
ratu
re
info
rmat
ion
only
Annu
al p
er-p
atie
nt
cost
of D
VT: $
3,79
8
Mac
Doug
all
2006
(98)
Drum
mon
d Ch
eckl
ist s
core
=
16
Retro
spec
tive
obse
rvat
iona
l co
hort
stud
y
Line
ar m
odel
with
lo
g-lin
k fu
nctio
n an
d ga
mm
a di
strib
utio
n
Trea
tmen
t st
rate
gy, l
engt
h of
hos
pita
l sta
y, ph
ysic
ian
offic
e,
emer
genc
y ro
om,
outp
atie
nt c
laim
s,
anci
llary
ser
vice
s,
and
phar
mac
y ut
iliza
tion
Actu
al
heal
thca
re p
lan
paym
ents
for
serv
ices
onl
y
Patie
nts
with
a
DVT
or P
E di
agno
sis
code
du
ring
the
stud
y pe
riod
(Jan
. 1, 1
997–
Mar
. 31
, 200
4)
Deep
-vei
n th
rom
bosi
s (D
VT),
and
pulm
onar
y em
bolis
m (P
E)
Lite
ratu
re
info
rmat
ion
only
Mea
n LO
S DV
T =
10 d
ays,
PE
= 9
days
, DVT
and
PE
= 1
0 da
ys
Annu
al d
irect
m
edic
al c
osts
of
$16,
832
($24
,411
CA
N) f
or D
VT,
$18,
221
($26
,426
CA
N) f
or P
E,
$24,
874
($36
,074
CA
N) f
or c
ombi
ned
DVT
and
PE, a
nd
$4,7
26 ($
6,85
4 CA
N)
*Onl
y gi
ves
inci
denc
e of
PTS
, PEs
giv
en p
ost-s
urgi
cal D
VT.
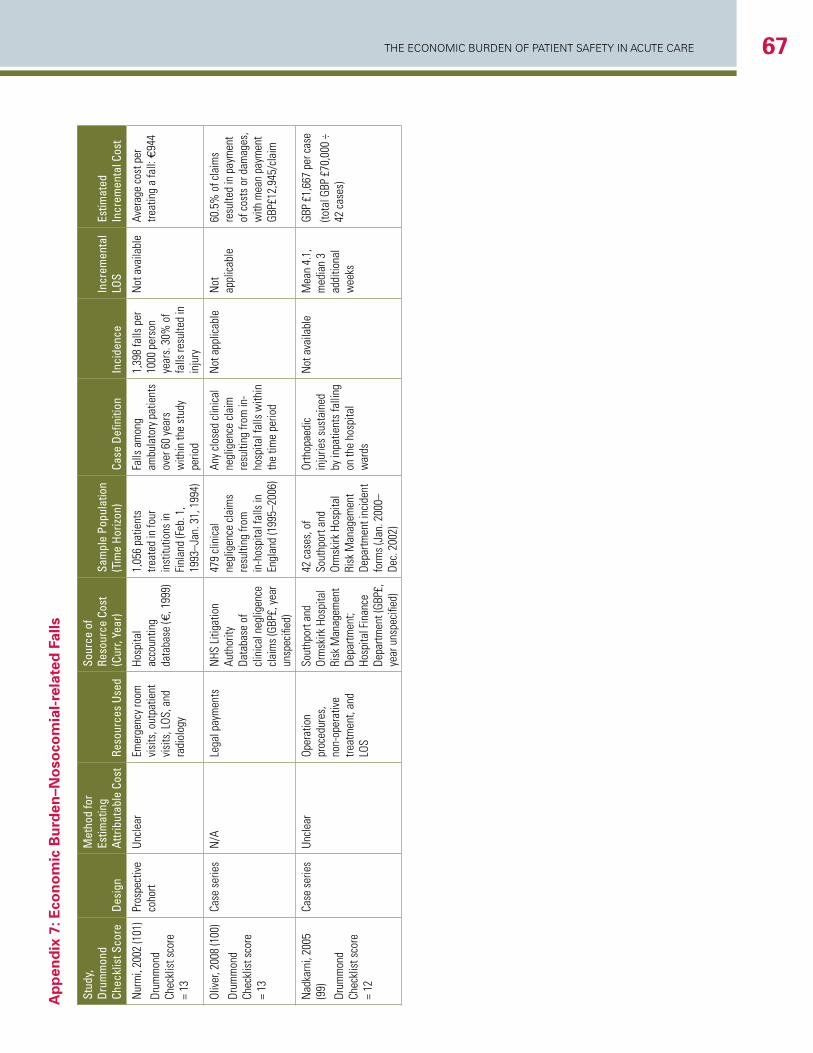
The economic Burden of PaTienT SafeTy in acuTe care 67A
pp
end
ix 7
: Eco
no
mic
Bu
rden
–No
soco
mia
l-re
late
d F
alls
Stud
y,
Drum
mon
d Ch
eckl
ist S
core
Desi
gn
Met
hod
for
Estim
atin
g At
tribu
tabl
e Co
stRe
sour
ces
Used
Sour
ce o
f Re
sour
ce C
ost
(Cur
r, Ye
ar)
Sam
ple
Popu
latio
n (T
ime
Horiz
on)
Case
Defi
nitio
nIn
cide
nce
Incr
emen
tal
LOS
Estim
ated
In
crem
enta
l Cos
t
Nur
mi,
2002
(101
)
Drum
mon
d Ch
eckl
ist s
core
=
13
Pros
pect
ive
coho
rtUn
clea
rEm
erge
ncy
room
vi
sits
, out
patie
nt
visi
ts, L
OS, a
nd
radi
olog
y
Hosp
ital
acco
untin
g da
taba
se (€
, 199
9)
1,05
6 pa
tient
s tre
ated
in fo
ur
inst
itutio
ns in
Fi
nlan
d (F
eb. 1
, 19
93–J
an. 3
1, 1
994)
Falls
am
ong
ambu
lato
ry p
atie
nts
over
60
year
s w
ithin
the
stud
y pe
riod
1,39
8 fa
lls p
er
1000
per
son
year
s. 3
0% o
f fa
lls re
sulte
d in
in
jury
Not
ava
ilabl
eAv
erag
e co
st p
er
treat
ing
a fa
ll: €
944
Oliv
er, 2
008
(100
)
Drum
mon
d Ch
eckl
ist s
core
=
13
Case
ser
ies
N/A
Lega
l pay
men
tsN
HS L
itiga
tion
Auth
ority
Da
taba
se o
f cl
inic
al n
eglig
ence
cl
aim
s (G
BP£,
yea
r un
spec
ified
)
479
clin
ical
ne
glig
ence
cla
ims
resu
lting
from
in
-hos
pita
l fal
ls in
En
glan
d (1
995–
2006
)
Any
clos
ed c
linic
al
negl
igen
ce c
laim
re
sulti
ng fr
om in
-ho
spita
l fal
ls w
ithin
th
e tim
e pe
riod
Not
app
licab
leN
ot
appl
icab
le60
.5%
of c
laim
s re
sulte
d in
pay
men
t of
cos
ts o
r dam
ages
, w
ith m
ean
paym
ent
GBP£
12,9
45/c
laim
Nad
karn
i, 20
05
(99)
Drum
mon
d Ch
eckl
ist s
core
=
12
Case
ser
ies
Uncl
ear
Oper
atio
n pr
oced
ures
, no
n-op
erat
ive
treat
men
t, an
d LO
S
Sout
hpor
t and
Or
msk
irk H
ospi
tal
Risk
Man
agem
ent
Depa
rtmen
t; Ho
spita
l Fin
ance
De
partm
ent (
GBP£
, ye
ar u
nspe
cifie
d)
42 c
ases
, of
Sout
hpor
t and
Or
msk
irk H
ospi
tal
Risk
Man
agem
ent
Depa
rtmen
t inc
iden
t fo
rms
(Jan
. 200
0–De
c. 2
002)
Orth
opae
dic
inju
ries
sust
aine
d by
inpa
tient
s fa
lling
on
the
hosp
ital
war
ds
Not
ava
ilabl
e M
ean
4.1,
m
edia
n 3
addi
tiona
l w
eeks
GBP
£1,6
67 p
er c
ase
(tota
l GBP
£70
,000
÷
42 c
ases
)
Safe care... accepting no less





























