Embed Size (px)
Citation preview
RESEARCH REPORT
© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
Addiction,
97
(Suppl 1), 84–97
Blackwell Science, Ltd
Oxford, UK
ADDAddiction
1359-6357© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
97
Supplement 00
Original Article
Michael T. French et al.Cost of outpatient mari-
juana treatment for adolescents
Correspondence to:
Michael T. FrenchMedical University of South CarolinaDepartment of Health Administration and Policy19 Hagwood AvenueSuite 408PO Box 25 0807CharlestonSC 29425Tel:
+
1 843 792 2202Fax:
+
1 843 792 1358
E-mail: [email protected]
RESEARCH REPORT
The economic cost of outpatient marijuana treatment for adolescents: findings from a multi-site field experiment
Michael T. French
1
, M. Christopher Roebuck
2
, Michael L. Dennis
3
, Guy Diamond
4
, Susan H. Godley
3
, Frank Tims
5
, Charles Webb
6
& James M. Herrell
7
Department of Health Administration and Policy, Medical University of South Carolina
1
, AdvancePCS
2
, Chestnut Health Systems
3
, Children’s Hospital of Philadelphia/University of Pennsylvania
4
, Operation PAR, Inc.
5
, University of Connecticut Health Center
6
, Center for Substance Abuse Treatment, Substance Abuse
and Mental Health Services Administration, Rockville, MD, USA
7
ABSTRACT
Aims
Despite recent advances in the economic evaluation of adult substanceabuse treatment, information and basic research is lacking on the cost of ado-lescent substance abuse treatment. The present study conducted an economiccost analysis of several outpatient adolescent treatment approaches.
Design
The Cannabis Youth Treatment (CYT) study evaluated five structuredtreatments for cannabis-using adolescents. One of the approaches was imple-mented by all of the four geographically and institutionally diverse treatmentfacilities collaborating in CYT; each of the other four approaches was imple-mented in two of the sites. Using the Drug Abuse Treatment Cost AnalysisProgram (DATCAP), the economic cost of each site-specific treatment wasdetermined.
Findings
The average economic costs of the five types of outpatient treatmentsranged from $837 to $3334 per episode, and varied by both direct factors (e.g.hours of treatment, treatment retention) and indirect factors (e.g. cost of living,staff level, case-load variation).
Conclusions
These adolescent treatment cost estimates are examined in termsof their calculation, variability by condition, variability by site within conditionand comparability with previous DATCAP results from outpatient drug-free pro-grams for adults. Future research will integrate treatment outcomes and coststo complete cost-effectiveness and benefit–cost analyses of the five therapies.
KEYWORDS
Adolescents, economic cost, marijuana treatment.
INTRODUCTION
National surveys indicate that marijuana has been theillicit drug of choice among adolescents for many yearsand is now the leading primary substance (ahead of alco-hol) mentioned in adolescent substance abuse treatmentadmissions, emergency room admissions, and autopsies(e.g. Dennis & McGeary 1999; Dennis
et al
. 2002a; OAS1997; ISR 1999). Furthermore, the published literaturecontains only data on about 16 experimental and/ornon-experimental adolescent substance abuse treatment
studies with none including analyses of economic costs(Titus & Godley 1999). In response to these persistenttrends and lack of applied research, the Center for Sub-stance Abuse Treatment (CSAT), within the SubstanceAbuse and Mental Health Services Administration,issued GFA no. TI 97–002 to establish the ‘CooperativeAgreement for a Multi-site Study of the Effectiveness ofTreatment for Cannabis (Marijuana) Dependent Youth’in 1997. The purposes of this and the ensuing coopera-tive agreement, The Cannabis Youth Treatment (CYT)study (consisting of a coordinating center, four treatment

Cost of outpatient marijuana treatment for adolescents
85
© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
Addiction,
97
(Suppl 1), 84–97
sites and CSAT), were to identify promising models of out-patient treatment for adolescent cannabis users, evaluatetheir clinical effectiveness, cost and cost-effectiveness,and adapt these models for use in field situations (Dennis
et al
. 2002b).The purpose of this paper is to present the findings of a
cost analysis of the five interventions as implemented inthe CYT sites. In the following section, a brief review ofthe literature indicates a need for this type of cost studyand economic evaluation studies in general. The litera-ture review is followed by a summary of the CYT studydesign and the methodology used for the economic costanalysis. Next, the cost estimates are presented by treat-ment condition (both by site and overall). A regressionanalysis of episode costs by condition reveals several cli-ent and treatment factors that are significantly related tocost. In the Discussion section, the results are interpretedand compared with the existing literature on the eco-nomic costs of adult substance abuse treatment pro-grams. Finally, limitations, future directions, and policyimplications are addressed.
BACKGROUND
Overview of economic evaluations
Although treatment effectiveness may be of greatestinterest to CYT providers and addiction programs overall,economic evaluation is also important. Policymakers lookto cost-effectiveness and benefit–cost analyses to aid indecision making, while treatment providers use theresults to develop more efficient operations and argue forincreased funding. Little is known about the ‘economics’of adolescent substance abuse treatment despite numer-ous published studies on adult programs (e.g. French &Martin 1996; French
et al
. 1996; French & McGeary1997; French
et al
. 1997; Dunlap & French 1998; Salomé& French 2001). Because young adults bring uniqueneeds to the therapeutic process, separate economic eval-uations of adolescent addiction interventions are war-ranted. Such studies are also timely, given the nationaldebate in each state over whether to include adolescentsubstance abuse treatment benefits under the Children’sHealth Insurance Program (CHIP) (see CSAT 1999; Den-nis & McGeary 1999; Dennis, Godley & Titus 1999).
Economic evaluation of substance abuse treatment isan evolving science with a collection of different tech-niques and methodologies (e.g. French 1995, 2000;Drummond
et al
. 1997; Cartwright 1998, 2000). Anyproper, full economic evaluation must include an assess-ment of the costs of treatment delivered. Accounting costsof treatment services typically include money spentto operate a program (e.g. personnel, supplies) and
depreciation of equipment and facilities, whereas eco-nomic costs are the value of all resources used in thetreatment process including resources received either inkind or at below market rates (i.e. opportunity costs)(Salomé & French 2001). It should be noted, however,that reimbursement rates for treatment services are oftenset by government agencies or managed care organiza-tions, and these rates may be unrelated to either account-ing or economic costs at individual programs. In additionto defining costs, it is important to emphasize that theperspective one takes in estimating treatment costs candramatically affect the results. For example, the cost tothe employer (e.g. treatment provider) of an unpaid vol-unteer worker (e.g. graduate student) is zero. However,from the point of view of society, which includes the grad-uate student worker, the opportunity cost is equal to theamount the person could have earned elsewhere (i.e. theresource’s next highest and best use). Since the impact ofdrug abuse is broadly felt, economic evaluation of drugabuse treatment is generally conducted from the compre-hensive societal perspective (Gold
et al
. 1996; Drummond
et al
. 1997; French 2000).The Drug Abuse Treatment Cost Analysis Program
(DATCAP) applies the economic (opportunity cost)approach to determine the cost of treatment for anentire program or modality (French 2001a, 2001b;http://www.DATCAP.com). The DATCAP yields statisticssuch as the total annual opportunity cost of treatmentand the labor cost per client, each pertaining to a singletreatment program during a particular fiscal year. Todate, the DATCAP has been administered at well over 80programs, ranging from intensive residential modalitiesto methadone maintenance and outpatient drug-freeprograms (e.g. Bradley
et al
. 1994; French
et al
. 1994,1996, 1997; Bray
et al
. 1996; French & McGeary 1997;McCollister & French, 2002; Salomé & French 2001). TheDATCAP has made important contributions to the addic-tion treatment evaluation literature by providing reliableand comparable cost estimates for numerous treatmentmodalities and programs.
Once economic costs have been identified, they can bepaired with appropriate outcome data for more advancedanalyses such as cost-effectiveness and benefit–cost stud-ies (Gold
et al
. 1996; Drummond
et al
. 1997; French2000; French
et al
. 2000, 2002). The process of identify-ing the economic costs described here for the CYT studylays the foundation for further analyses that will providecritical economic information of different substanceabuse treatment approaches for adolescents.
Overview of CYT design
As part of the Secretary of Health and Human Service’s‘Youth Initiative’ (HHS 1998), CSAT implemented the

© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
Addiction,
97
(Suppl 1), 84–97
86
Michael T. French
et al.
CYT study to (a) identify promising approaches to treat-ing cannabis use by adolescents from research, best prac-tices and/or expert consensus panels, (b) adapt theseapproaches for use in actual practice, (c) evaluate theireffectiveness, cost, and cost-effectiveness and (d) explorehow well they work with different subgroups of adoles-cents and in different programs/environments (Dennis
et al
. 2002b). The CYT study was one of the largest exper-imental studies of outpatient adolescent treatment to date(
n
=
600 adolescents and their families), representing acollaboration between CSAT, two large adolescent treat-ment providers (Chestnut Health Systems, in Illinois andOperation PAR, in Florida), and two of the nation’s majormedical centers (University of Connecticut Health Centerand Children’s Hospital of Philadelphia). The study man-ualized and evaluated five promising approaches to out-patient treatment for adolescents that use marijuana,alcohol and some limited amount of other drugs. Thesetreatments (described in the next subsection) varied interms of total resources used and approach.
In the ‘incremental’ arm of the study, CYT started witha brief intervention (five sessions over 6 weeks) consistingof two initial individual sessions followed by three groupsessions. CYT examined the impact of adding group ses-sions to the brief intervention (12 weeks total) and, forthe third intervention, adding family treatment to thesecond intervention (12 weeks total).
In the ‘alternative arm’, CYT started with the samebrief intervention. Instead of adding more treatment/resources to the existing dosage, however, 12 weeks of anindividual counseling approach and 12 weeks of an inte-grated family counseling approach were delivered. Whilethis treatment increased the dosage in duration and ses-sions, it involved less weekly contact time and resources,on average, relative to the brief intervention.
In both arms, all three interventions were replicated attwo sites (one of the large adolescent providers and one ofthe medical centers). Within site, eligible adolescentswere randomized to one of the arm’s three conditions.Thus, treatments can be compared experimentally withinarm, or quasi-experimentally across arms (see Dennis
et al
. 2002b, for a further discussion of this issue).Adolescents were recruited from families, schools, the
criminal justice system and from the normal case-flow foroutpatient treatment in these agencies. To be included inCYT, the adolescents had to: (a) be between the ages of 12and 18, (b) meet criteria for current DSM-IV (APA 1994)diagnosis of cannabis abuse or dependence, (c) have usedmarijuana in the past 90 days (or 90 days prior to beingin a controlled environment) and (d) meet ASAM (1996)patient placement criteria for level I (outpatient) or level II(intensive outpatient) under state waiver, where applica-ble. For safety and logistical reasons, participants wereexcluded if they met any of the following criteria: (a) used
alcohol 45 or more days of the 90 days prior to intake (orprior to being in a controlled environment, where rele-vant), (b) used other drugs 13 or more of the 90 daysprior to intake (or prior to being in a controlled environ-ment, where relevant), (c) had an acute medical condi-tion that required immediate treatment or was likely toprohibit full participation in treatment, (d) had an acutepsychological condition that required immediate treat-ment and/or was likely to prohibit full participation intreatment, (e) appeared to have insufficient mentalcapacity to understand the consent and/or participate intreatment, (f) was living outside the program’s catchmentarea or expected to move out within the next 90 days, (g)had a history of violent behavior, severe conduct disorder,predatory crime or criminal justice system involvementthat was likely to prohibit full participation in treatment(e.g. pending incarceration), (h) lacked sufficient abilityto use English to participate in treatment, (i) had a signif-icant other (usually a parent) who lacked sufficient abilityin English to understand the collateral consent form andparticipate in research assessments and potentially intreatment and/or (j) had participated previously in thestudy. Participation was voluntary, under the supervisionof local institutional review boards, and protected undera federal certificate of confidentiality.
The accounting and economic cost data, which arethe focus of this paper, were collected during the middle 6months (1 January 1999–30 June 1999) of the CYTstudy to minimize the impact of start-up or wind-downcosts. While the investigators strived to separate theresearch costs, there are some areas where the cost esti-mates may still be influenced by the research context.Foremost among these concerns is the fact that, underCYT, all treatment costs were covered by the researchstudy (which may have increased attendance at treat-ment sessions). In addition, to provide three differenttypes of treatment over a short period of time, some sites(particularly CHOP and PAR) had to hire a greateramount of personnel than would be required in a normaltreatment setting. These limitations and their implica-tions for the interpretation and replicability of the costestimates are discussed at length after the results arepresented.
Overview of CYT interventions
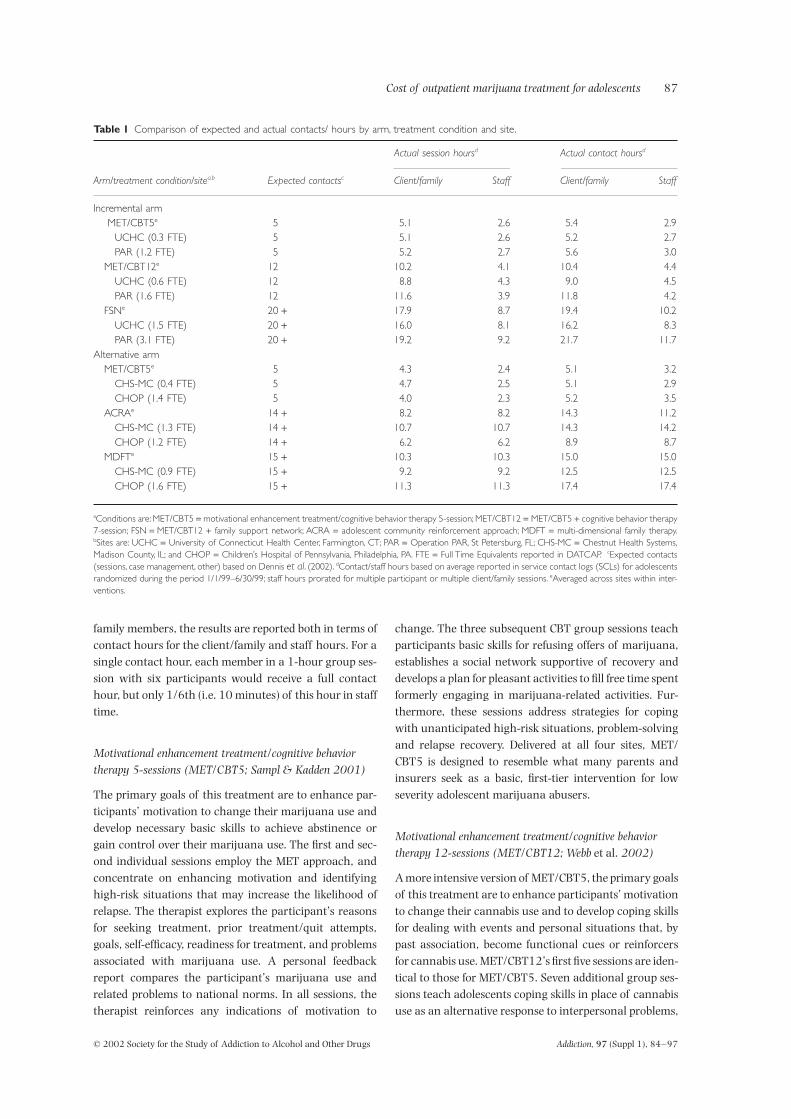
Below is a short description of each of the five interven-tions. In addition, Table 1 contrasts the five interventionsin terms of the total amount (formal sessions and casemanagement) of direct contacts and service hours thetreatment programs were expected to provide and thenumber they actually provided to the average adolescentand his/her family during this 6-month period. Becausesome sessions involved multiple adolescents and/or
Cost of outpatient marijuana treatment for adolescents
87
© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
Addiction,
97
(Suppl 1), 84–97
family members, the results are reported both in terms ofcontact hours for the client/family and staff hours. For asingle contact hour, each member in a 1-hour group ses-sion with six participants would receive a full contacthour, but only 1/6th (i.e. 10 minutes) of this hour in stafftime.
Motivational enhancement treatment/cognitive behavior therapy 5-sessions (MET/CBT5; Sampl & Kadden 2001)
The primary goals of this treatment are to enhance par-ticipants’ motivation to change their marijuana use anddevelop necessary basic skills to achieve abstinence orgain control over their marijuana use. The first and sec-ond individual sessions employ the MET approach, andconcentrate on enhancing motivation and identifyinghigh-risk situations that may increase the likelihood ofrelapse. The therapist explores the participant’s reasonsfor seeking treatment, prior treatment/quit attempts,goals, self-efficacy, readiness for treatment, and problemsassociated with marijuana use. A personal feedbackreport compares the participant’s marijuana use andrelated problems to national norms. In all sessions, thetherapist reinforces any indications of motivation to
change. The three subsequent CBT group sessions teachparticipants basic skills for refusing offers of marijuana,establishes a social network supportive of recovery anddevelops a plan for pleasant activities to fill free time spentformerly engaging in marijuana-related activities. Fur-thermore, these sessions address strategies for copingwith unanticipated high-risk situations, problem-solvingand relapse recovery. Delivered at all four sites, MET/CBT5 is designed to resemble what many parents andinsurers seek as a basic, first-tier intervention for lowseverity adolescent marijuana abusers.
Motivational enhancement treatment/cognitive behavior therapy 12-sessions (MET/CBT12; Webb
et al.
2002)
A more intensive version of MET/CBT5, the primary goalsof this treatment are to enhance participants’ motivationto change their cannabis use and to develop coping skillsfor dealing with events and personal situations that, bypast association, become functional cues or reinforcersfor cannabis use. MET/CBT12’s first five sessions are iden-tical to those for MET/CBT5. Seven additional group ses-sions teach adolescents coping skills in place of cannabisuse as an alternative response to interpersonal problems,
Table 1
Comparison of expected and actual contacts/ hours by arm, treatment condition and site.
Arm/treatment condition/site
a,b
Expected contacts
c
Actual session hours
d
Actual contact hours
d
Client/family Staff Client/family Staff
Incremental arm MET/CBT5
e
5 5.1 2.6 5.4 2.9UCHC (0.3 FTE) 5 5.1 2.6 5.2 2.7PAR (1.2 FTE) 5 5.2 2.7 5.6 3.0
MET/CBT12
e
12 10.2 4.1 10.4 4.4UCHC (0.6 FTE) 12 8.8 4.3 9.0 4.5PAR (1.6 FTE) 12 11.6 3.9 11.8 4.2
FSN
e
20
+
17.9 8.7 19.4 10.2UCHC (1.5 FTE) 20
+
16.0 8.1 16.2 8.3PAR (3.1 FTE) 20
+
19.2 9.2 21.7 11.7Alternative arm
MET/CBT5
e
5 4.3 2.4 5.1 3.2CHS-MC (0.4 FTE) 5 4.7 2.5 5.1 2.9CHOP (1.4 FTE) 5 4.0 2.3 5.2 3.5
ACRA
e
14
+
8.2 8.2 14.3 11.2CHS-MC (1.3 FTE) 14
+
10.7 10.7 14.3 14.2CHOP (1.2 FTE) 14
+
6.2 6.2 8.9 8.7MDFT
e
15
+
10.3 10.3 15.0 15.0CHS-MC (0.9 FTE) 15
+
9.2 9.2 12.5 12.5CHOP (1.6 FTE) 15
+
11.3 11.3 17.4 17.4
a
Conditions are: MET/CBT5
=
motivational enhancement treatment/cognitive behavior therapy 5-session; MET/CBT12
=
MET/CBT5
+
cognitive behavior therapy7-session; FSN
=
MET/CBT12
+
family support network; ACRA
=
adolescent community reinforcement approach; MDFT
=
multi-dimensional family therapy.
b
Sites are: UCHC
=
University of Connecticut Health Center, Farmington, CT; PAR
=
Operation PAR, St Petersburg, FL; CHS-MC
=
Chestnut Health Systems,Madison County, IL; and CHOP
=
Children’s Hospital of Pennsylvania, Philadelphia, PA. FTE
=
Full Time Equivalents reported in DATCAP.
c
Expected contacts(sessions, case management, other) based on Dennis
et al
. (2002).
d
Contact/staff hours based on average reported in service contact logs (SCLs) for adolescentsrandomized during the period 1/1/99–6/30/99; staff hours prorated for multiple participant or multiple client/family sessions.
e
Averaged across sites within inter-ventions.

© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
Addiction,
97
(Suppl 1), 84–97
88
Michael T. French
et al.
negative affect and psychological dependence. Group ses-sions address problem-solving, anger awareness, angermanagement, communication, resistance to craving,depression management and management of thoughtsabout marijuana. With its longer duration and greaterbreadth, MET/CBT12 is closer in process and content tomost adolescent treatment programs.
Family support network (FSN; Hamilton
et al.
2001)
FSN is an intensive and family-focused approachdesigned to improve family cohesion/closeness, parent-ing skills and parental support, which is presumed toincrease the likelihood of both initial and sustainedchange. Designed to wrap these additional servicesaround the MET/CBT12 therapy over a 12-week period,FSN is composed of case management (to promote parentengagement in the treatment process), six parent educa-tion group meetings (to improve parent knowledge andskills relevant to adolescent problems and family func-tioning), four therapeutic home visits and referral to self-help support groups. These additional services aredesigned to impact several external factors, including: (a)helping staff gain a better understanding of the adoles-cent’s home/family environment; (b) providing the par-ent(s) with knowledge about problems and skills andabout how to deal with them; (c) tailoring plans to fit thefamily’s specific home situation; (d) supplying links withon-going groups for providing parents with social/emo-tional support; and (e) helping the family deal with thelogistical issues related to coming to treatment. FSN pro-vides a more comprehensive treatment model in line withCSAT TIPS recommendations (CSAT 1992, 1993).
Adolescent community reinforcement approach (ACRA; Godley
et al.
2002)
ACRA’s primary focus is helping the adolescent identifyreinforcers incompatible with drug use and rearrangingenvironmental contingencies so that abstinence frommarijuana is more rewarding than use. It is a modifica-tion of the community reinforcement approach (CRA)that was initially developed for the treatment of adultalcoholics (Meyers & Smith 1995). The ACRA modifica-tions address the special issues and needs of adolescents.ACRA is composed of 10 individual sessions with the ado-lescent and four meetings with care-givers. Two of thecare-giver sessions are with the care-giver(s) only andtwo include the adolescent and care-giver together. Medi-ating variables targeted by ACRA include: (a) treatmentparticipation; (b) increased motivation to quit; (c) aware-ness of the link between behavior and use; (d) increasedengagement in prosocial activities; (e) improved problemsolving skills; (f) improved communication skills; and (g)
an improved relationship between the adolescent andcare-giver that is more supportive of abstinence. Longer-term outcomes include improved relapse coping,reduced use/problems, decreased illegal activity/arrests,increased days in school/work, decreased affiliation withdrug-using peers, improved family cohesion and reducedfamily conflict.
Multidimensional family therapy (MDFT; Liddle, 2002)
MDFT is an intensive, family-focused, developmental, eco-logical, multiple-systems approach for treating adolescentsubstance abuse. The model targets adolescent and parentindividual functioning, family interaction patterns andthe extended social system (Liddle 1995). MDFT is com-posed of 12–15 family-focused treatment sessions over thecourse of 12 weeks. In addition to family sessions, time isspent alone with the adolescent and parent(s) and sup-plemented with phone contact for the purpose of engage-ment, reworking treatment themes and case/crisismanagement. MDFT attempts to improve the adolescent’scognitive states (e.g. perceived harmfulness of drugs),emotional regulation/distress (e.g. expression of anger,depression), and perceived role in the family/peer net-work. MDFT emphasizes establishing multiple therapeuticalliances with improved communication between the ado-lescent, parent(s), other family members and others out-side the family via several specific tasks (e.g. relationshipformation, agenda establishment, definition of and moti-vation to attempt change, renewal of parents’ connectionto the adolescent or the teenager’s connection to the par-ent, conflict resolution skills, developing authoritativeparenting style). It also targets behavior improvement(e.g. school attendance), peer network (e.g. identificationof prosocial activities), parental distress (e.g. depression ormarital conflict), parenting practices (e.g. behavior man-agement, attachment to the adolescent) and the influ-ences of other social systems (e.g. school, juvenile justice,work). MDFT is a multi-systemic treatment approach tar-geted more broadly at changing the individual’s relation-ships with family, peers and social systems.
Coordinating center and treatment sites
Chestnut Health Systems coordinating center (CHS-CC)
Chestnut Health Systems is a privately held, not-for-profitorganization. Based out of its Bloomington and Chicagooffices, the CYT Coordinating Center was supported bysubcontracts to the University of Connecticut for over-sight of the MET/CBT5 intervention, and to the Univer-sity of Miami to conduct the economic analyses.Additionally, the CHS-CC site was responsible for theoperation of the website, data management, and

Cost of outpatient marijuana treatment for adolescents
89
© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
Addiction,
97
(Suppl 1), 84–97
reporting for the entire CYT consortium. While it did notdirectly deliver treatment in the study, the CC (via the Uni-versity of Connecticut subcontract) was responsible forthe supervision of the MET/CBT5 condition and its asso-ciated costs.
University of Connecticut Health Center (UCHC)
UCHC is located at the University of Connecticut in Farm-ington, Connecticut, 10 miles from the city of Hartford.For over 25 years, UCHC, a large, public, non-profit orga-nization, has been an active center of research and devel-opment for addiction treatment, clinical subtyping andassessment technologies for the treatment of substanceuse disorders. The UCHC CYT treatment site recruits fromjuvenile/adult court-affiliated offices, youth service orga-nizations and schools and families (i.e. via advertising)located within a 20-mile radius of the health center.
Operation PAR, Inc. (PAR)
PAR is the largest community-based treatment providerin the state of Florida and the state’s largest adolescenttreatment provider. Serving participants from the StPetersburg, Florida area and/or recruits from thecounty’s juvenile justice assessment center (also operatedby Operation PAR, Inc.), PAR offers a full range of accred-ited programs for both adolescent and adult outpatientand in-patient care. The organization is operated as a pri-vate, non-profit entity.
Chestnut Health Systems, Madison County, Illinois (CHS-MC)
Operated by Chestnut Health System’s Adolescent Ser-vices Program, CHS-MC serves a catchment area of over800 square miles in the north-east corner of the St Louismetropolitan area that includes all of Madison Countyand East St Louis. Chestnut Health Systems is one of thelargest community-based substance abuse treatmentproviders in Illinois and the state’s largest adolescent pro-vider. It offers a full range of accredited, adolescent sub-stance abuse treatment services including prevention,early intervention, outpatient, intensive outpatient, daytreatment and residential treatment. Due to the ruralnature of the treatment delivery area, staff commutebetween and provide services out of facilities located inboth Granite City and Maryville (30 miles apart). CHS-MC’s financial structure is private, non-profit.
Children’s Hospital of Philadelphia (CHOP)
The Children’s Hospital of Philadelphia (CHOP) primarilyserves participants from Philadelphia’s inner city. CHOP
is a leading pediatric care hospital providing a full rangeof in-patient and outpatient medical and psychiatric ser-vices. The CYT program operated by CHOP was housedwithin the Child, Adolescent and Family Treatment Unit,which is a program in the Department of Psychiatry.Organizationally large, CHOP maintains a private, not-for-profit financial structure.
METHODS
Instrumentation
Drug Abuse Treatment Cost Analysis Program (DATCAP)
The DATCAP is a data collection instrument and inter-view guide designed to measure both the accounting andopportunity costs of a substance abuse treatment pro-gram based upon standard economic principles (French2001a, 2001b; http://www.DATCAP.com). Now usedwidely by different types of service providers, the DATCAPis appropriate for economic cost evaluation of most treat-ment modalities in most social service settings. Theinstrument is intended to collect and organize detailedinformation on resources used in service delivery andtheir associated costs. Resource categories include per-sonnel, supplies and materials, contracted services, build-ings and facilities, equipment and miscellaneous items.Additionally, the DATCAP gathers data on program reve-nues and client caseflows. Administration of the DATCAPis generally a collaborative effort involving an economistand various members of the treatment program’s staff(e.g. administrators, therapist coordinators and account-ing/finance personnel). Despite the growing list of DAT-CAP studies, this project is the first time the instrumenthas been used to estimate the economic cost of adolescentsubstance abuse treatment.
Service Contact Logs (SCLs)
SCLs were developed that were specific to each interven-tion. Each log contained the same basic componentsdescribing who, when, where, and what was donethroughout the interventions. However, codes for inter-vention components were specific to each intervention.SCLs were completed daily by all therapists involved in thestudy to ensure that each session held with a client and/or a family member was documented. These data werecollected and maintained by the Coordinating Center(CHS-CC) on an ongoing basis.
Data collection procedures
Shortly after the start of the CYT study, principal investi-gators and other program personnel were issued copies of

© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
Addiction,
97
(Suppl 1), 84–97
90
Michael T. French
et al.
the DATCAP User’s Manual (French 2001b) and the DAT-CAP Program Instrument (French 2001a). After provid-ing adequate time to review these materials, DATCAPcollaborators participated in several conference calls withhealth economists from the University of Miami to formu-late strategies for preliminary data collection, and answerquestions regarding completion of the DATCAP. Gener-ally, program personnel were offered guidance about thetype and source of information to gather for administra-tion of the DATCAP. When all four treatment sites hadreached a relatively stable point in their client random-ization and treatment processes, they were asked to makean initial attempt at completing a separate DATCAP ques-tionnaire for each of the therapies they were administer-ing at their respective CYT study sites. There were twostudy arms, each with three treatment approaches,which were implemented in two sites. Thus, a total of 12DATCAPs were completed.
Although the DATCAP is intended to cover a full fiscalyear, the 6-month time frame ending 30 June 1999 wasselected as the period of study. This half-year window wasnecessary to minimize the inclusion of costs associatedwith the start-up and wind-down of subject randomiza-tion and other research-specific activities. Furthermore,for comparability with other treatment programs, inves-tigators were also instructed to exclude all costs attrib-uted to the research component of the study. Finally,because some interventions involved shared resourcesacross two or more sites, program personnel wereinstructed to estimate cross-site costs according to howthey were consumed. For example, if the therapist co-ordinator for a certain treatment intervention contrib-uted 20% time (i.e. 8 hours per week) supervising, viatelephone, a counselor at another site, then 20% of thecost of the therapist coordinator would be allocated to theremote site for that therapy. These important qualifica-tions will be explained again later.
After preliminary DATCAPs were completed, a healtheconomist (Mr Roebuck) from the University of Miami’sHealth Services Research Center visited each of the treat-ment sites. The purpose of the site visit was to tour thefacility and observe the intervention processes to insurethat all resources were properly accounted for in the eco-nomic cost analysis. Program personnel were questionedabout their level of effort (i.e. time) on each of the respec-tive therapies. Physical office space was measured andallocated to the intervention it served. Equipment costswere determined based upon the percentage of time a unitwas used by each therapy. In addition, during the sitevisit, the DATCAP administrator reviewed the prelimi-nary DATCAPs for quality and consistency.
Following the site visits, the CYT-CC computed aver-age weekly census and length of stay measures from theSCL database. These measures are critical in determining
the average weekly and episode costs of treatment and toensure consistency across sites. They were calculated asfollows:• Average weekly census (i.e. average active caseload),
calculated as the average number of clients that partic-ipated in treatment during the weeks from 1 January1999 to 30 June 1999.
• Client length of stay (i.e. weeks retained in treatment),calculated as the number of weeks in treatment foreach client from the baseline assessment to the last ser-vice received.After completion of all 12 DATCAPs, hard-copy data
were entered into a Microsoft
®
Excel (version 2000)spreadsheet designed specifically for the DATCAP instru-ment and the cost analysis. This spreadsheet programemploys economic principles and cost calculation tech-niques (e.g. Drummond
et al
. 1997), and generates a two-page Results Summary. The summary document reportsthe total accounting and economic costs, average weeklycost (per client), average cost per treatment episode, andtotal cost distributed across resource categories. A fullinterpretation of the cost findings is presented and dis-cussed in the following section.
RESULTS
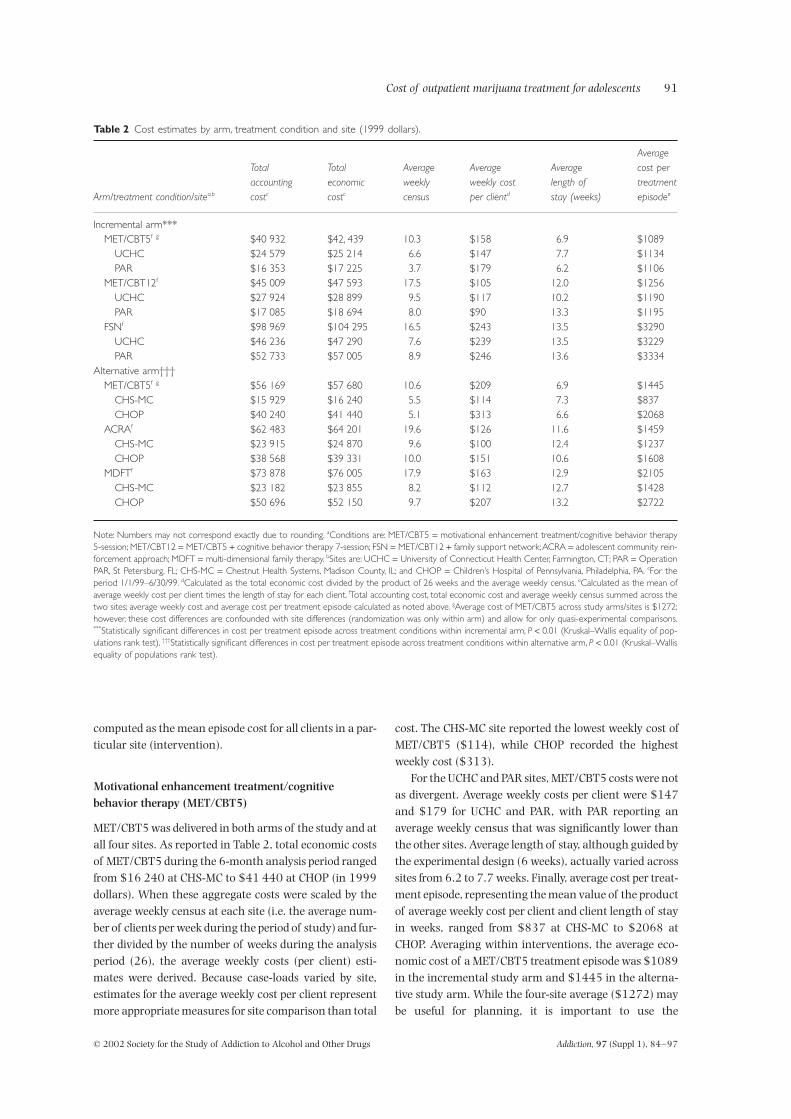
The DATCAP results are presented for each of the CYTinterventions, by treatment delivery site. While account-ing costs are reported along with economic costs inTable 2, only the latter estimates are discussed in the bodyof the article because economic costs are the most impor-tant estimates for the full economic evaluation. Moreover,for these interventions, economic costs were 2–9%higher (4% higher on average) than accounting costs.This small differential was due in part to the short-termnature of the project, whereby minimal opportunitieswere present for in-kind or under-priced resources thatare often employed in longer-running programs.
Cost estimates are presented below by condition andby site. The most likely reasons for and implications of thesignificant site variation in costs are also examined in theregression analysis that follows and the Discussion sec-tion. Table 2 presents the aggregate DATCAP results (byarm) for MET/CBT5, MET/CBT12, FSN, ACRA andMDFT. For each intervention, all aggregate costs weresummed across sites, as were average weekly census esti-mates. Average length of stay estimates, by site and inter-vention, were calculated as the mean length of stay for allclients who were assigned to a particular site and inter-vention. The (economic) cost per treatment episode foreach client was calculated as the product of averageweekly cost and length of stay in treatment (weeks). Aver-age episode costs for each site (intervention) was
Cost of outpatient marijuana treatment for adolescents
91
© 2002 Society for the Study of Addiction to Alcohol and Other Drugs
Addiction,
97
(Suppl 1), 84–97
computed as the mean episode cost for all clients in a par-ticular site (intervention).
Motivational enhancement treatment/cognitive behavior therapy (MET/CBT5)
MET/CBT5 was delivered in both arms of the study and atall four sites. As reported in Table 2, total economic costsof MET/CBT5 during the 6-month analysis period rangedfrom $16 240 at CHS-MC to $41 440 at CHOP (in 1999dollars). When these aggregate costs were scaled by theaverage weekly census at each site (i.e. the average num-ber of clients per week during the period of study) and fur-ther divided by the number of weeks during the analysisperiod (26), the average weekly costs (per client) esti-mates were derived. Because case-loads varied by site,estimates for the average weekly cost per client representmore appropriate measures for site comparison than total
cost. The CHS-MC site reported the lowest weekly cost ofMET/CBT5 ($114), while CHOP recorded the highestweekly cost ($313).
For the UCHC and PAR sites, MET/CBT5 costs were notas divergent. Average weekly costs per client were $147and $179 for UCHC and PAR, with PAR reporting anaverage weekly census that was significantly lower thanthe other sites. Average length of stay, although guided bythe experimental design (6 weeks), actually varied acrosssites from 6.2 to 7.7 weeks. Finally, average cost per treat-ment episode, representing the mean value of the productof average weekly cost per client and client length of stayin weeks, ranged from $837 at CHS-MC to $2068 atCHOP. Averaging within interventions, the average eco-nomic cost of a MET/CBT5 treatment episode was $1089in the incremental study arm and $1445 in the alterna-tive study arm. While the four-site average ($1272) maybe useful for planning, it is important to use the
Table 2
Cost estimates by arm, treatment condition and site (1999 dollars).
Arm/treatment condition/site
a,b
Totalaccountingcost
c
Total
economiccost
c
Averageweeklycensus
Averageweekly costper client
d
Averagelength of
stay (weeks)
Average
cost per
treatmentepisode
e
Incremental arm***MET/CBT5
f
g
$40 932 $42, 439 10.3 $158 6.9 $1089UCHC $24 579 $25 214 6.6 $147 7.7 $1134PAR $16 353 $17 225 3.7 $179 6.2 $1106
MET/CBT12f $45 009 $47 593 17.5 $105 12.0 $1256UCHC $27 924 $28 899 9.5 $117 10.2 $1190PAR $17 085 $18 694 8.0 $90 13.3 $1195
FSNf $98 969 $104 295 16.5 $243 13.5 $3290UCHC $46 236 $47 290 7.6 $239 13.5 $3229PAR $52 733 $57 005 8.9 $246 13.6 $3334
Alternative arm†††MET/CBT5f g $56 169 $57 680 10.6 $209 6.9 $1445
CHS-MC $15 929 $16 240 5.5 $114 7.3 $837CHOP $40 240 $41 440 5.1 $313 6.6 $2068
ACRAf $62 483 $64 201 19.6 $126 11.6 $1459CHS-MC $23 915 $24 870 9.6 $100 12.4 $1237CHOP $38 568 $39 331 10.0 $151 10.6 $1608
MDFTf $73 878 $76 005 17.9 $163 12.9 $2105CHS-MC $23 182 $23 855 8.2 $112 12.7 $1428CHOP $50 696 $52 150 9.7 $207 13.2 $2722
Note: Numbers may not correspond exactly due to rounding. aConditions are: MET/CBT5 = motivational enhancement treatment/cognitive behavior therapy5-session; MET/CBT12 = MET/CBT5 + cognitive behavior therapy 7-session; FSN = MET/CBT12 + family support network; ACRA = adolescent community rein-forcement approach; MDFT = multi-dimensional family therapy. bSites are: UCHC = University of Connecticut Health Center, Farmington, CT; PAR = OperationPAR, St Petersburg, FL; CHS-MC = Chestnut Health Systems, Madison County, IL; and CHOP = Children’s Hospital of Pennsylvania, Philadelphia, PA. cFor theperiod 1/1/99–6/30/99. dCalculated as the total economic cost divided by the product of 26 weeks and the average weekly census. eCalculated as the mean ofaverage weekly cost per client times the length of stay for each client. fTotal accounting cost, total economic cost and average weekly census summed across thetwo sites; average weekly cost and average cost per treatment episode calculated as noted above. gAverage cost of MET/CBT5 across study arms/sites is $1272;however, these cost differences are confounded with site differences (randomization was only within arm) and allow for only quasi-experimental comparisons.***Statistically significant differences in cost per treatment episode across treatment conditions within incremental arm, P < 0.01 (Kruskal–Wallis equality of pop-ulations rank test). †††Statistically significant differences in cost per treatment episode across treatment conditions within alternative arm, P < 0.01 (Kruskal–Wallisequality of populations rank test).

© 2002 Society for the Study of Addiction to Alcohol and Other Drugs Addiction, 97 (Suppl 1), 84–97
92 Michael T. French et al.
appropriate intervention site estimate above to reflect dif-ferences in the local cost of living, organizational struc-ture, and staffing pattern (discussed further below).
MET/CBT12 and all other remaining therapies wereadministered at two of the four treatment sites, as pre-sented below.
Motivational enhancement treatment/cognitive behavior therapy (MET/CBT12)
The total economic cost of delivering MET/CBT12 atUCHC was $28 899, compared with $18 694 at PAR.Although the total cost at UCHC was more than $10 000higher than at PAR, part of this differential was due prob-ably to the larger client case-load at UCHC. Specifically,the average weekly census was 9.5 clients at UCHC com-pared with 8.0 individuals at PAR. For an average client,the weekly cost was $117 at UCHC and $90 at PAR.Patients remained in treatment typically for the 12-weektarget in the MET/CBT12 experimental design. Thus, theaverage cost per MET/CBT12 treatment episode was$1190 at UCHC, $1195 at PAR and $1256 across theincremental study arm.
Family support network (FSN)
Although average weekly and episode cost estimates forthe MET/CBT12 intervention were nearly identical forUCHC and PAR, DATCAP results for the FSN therapy atthe two sites were somewhat similar. Starting at theaggregate level, total economic cost varied by $9715, or21%. Since UCHC had a slightly smaller case-load (7.6)than PAR (8.9), average weekly costs per client were$239 and $246 for UCHC and PAR. Moreover, similaritiesacross sites in the average length of stay in treatmentcaused average costs per treatment episode to have a verynarrow range of only $105. (This may actually be decep-tive since despite similar costs, Table 1 shows they pro-vided fairly different amounts of care because UCHC hadproblems keeping case managers on staff.) Thus, the aver-age cost per FSN treatment episode was $3229 at UCHC,$3334 at PAR and $3290 across the incremental studyarm.
Adolescent community reinforcement approach (ACRA)
Although not as wide as for MET/CBT5, differences in thecost estimates for ACRA therapy between CHS-MC andCHOP were larger than the site differences for FSN. Totaleconomic cost of ACRA was $14 461 higher at CHOPcompared to CHS-MC. The average weekly cost at CHOPfor an adolescent who received ACRA was $151, whilethe average weekly cost for an ACRA client at CHS-MCwas $100. Average client caseloads at CHS-MC and
CHOP were similar (9.6 and 10.0), and average length ofstay at CHS-MC was slightly longer (12.4 weeks) than atCHOP (10.6 weeks). Thus, the average cost per ACRAtreatment episode was $1608 at CHOP, $1237 at CHS-MC and $1459 across the alternative study arm.
Multidimensional family therapy (MDFT)
The DATCAP results to this point suggest that averagecost estimates (weekly and episode) had minor to modestdifferences across sites that delivered the same interven-tions. This pattern did not endure for MDFT, which dis-played the greatest relative cost differentials in the study.Specifically, the estimated total economic cost for CHOPwas $52 150, compared to only $23 855 reported byCHS-MC. Although CHOP treated about 1.5 more clientsper day throughout the study period than CHS-MC, aver-age weekly cost per client was still $95 higher at CHOPthan at CHS-MC. Both sites also reported similar esti-mates for average length of stay in treatment (12.7 weeksat CHS-MC, 13.2 weeks at CHOP). Thus, the average epi-sode costs per MDFT treatment episode was $1428 atCHS-MC, $2722 at CHOP and $2105 across the alterna-tive study arm.
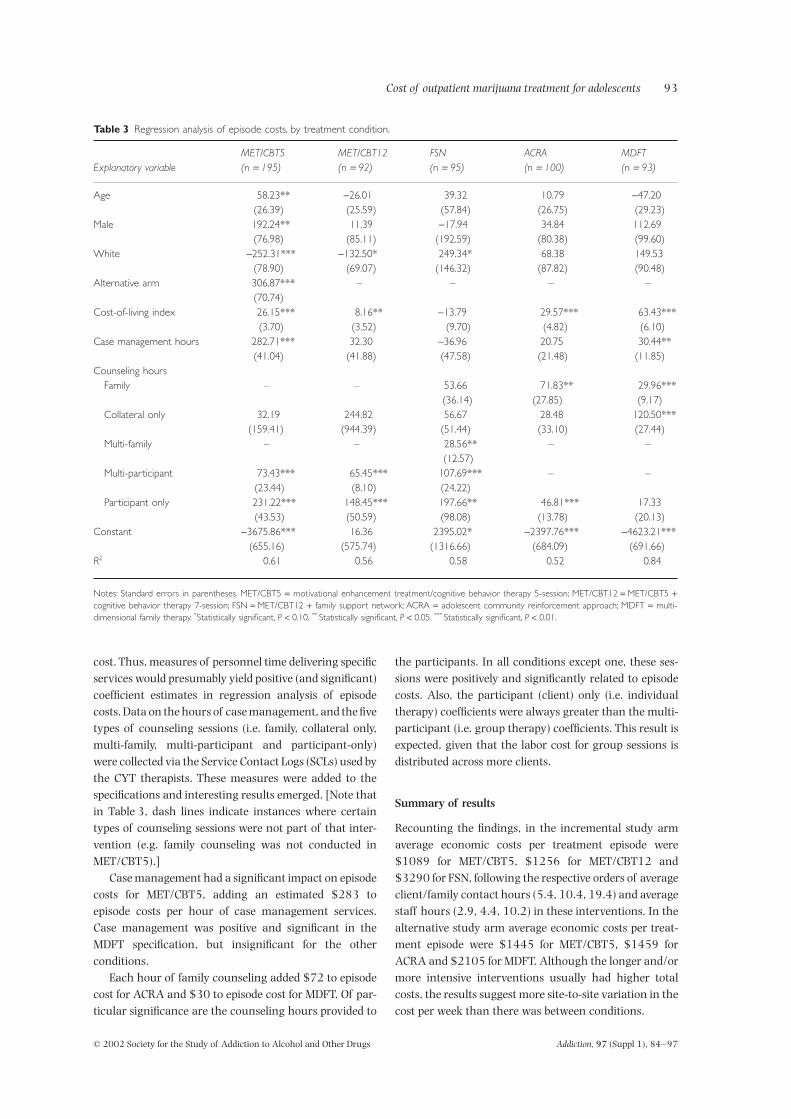
Regression analysis of episode costs
To explore possible sources of variation in episode costsfor clients, a regression analysis using ordinary leastsquares (OLS) was estimated by treatment condition.Table 3 presents the results from these specifications.Minimal demographic controls were included to increasepower in the equations. For MET/CBT5, age was relatedpositively to episode cost and males had significantlyhigher costs than females. White adolescents often hadsignificantly different costs than other races, but thedirection was not always the same. For example, the esti-mated MET/CBT5 episode costs were $252 less forwhites, yet the estimated episode costs were $249 morefor whites in FSN.
Since CYT was randomized within treatment arm, adichotomous measure for the alternative arm wasincluded in the MET/CBT5 regression. Clients whoreceived the MET/CBT5 intervention within the alterna-tive arm had a higher cost than MET/CBT5 clients in theincremental arm, by an estimated $307.
The cost-of-living index prevailing in 1999 for eachsite’s geographical location was obtained from the Amer-ican Chamber of Commerce Researcher’s Association(ACCRA 2000), and this measure was included in all theregressions. This index was significantly related to clientepisode costs in all but one condition (FSN).
Information from the DATCAP at each site and condi-tion showed that labor was the largest component of total
Cost of outpatient marijuana treatment for adolescents 93
© 2002 Society for the Study of Addiction to Alcohol and Other Drugs Addiction, 97 (Suppl 1), 84–97
cost. Thus, measures of personnel time delivering specificservices would presumably yield positive (and significant)coefficient estimates in regression analysis of episodecosts. Data on the hours of case management, and the fivetypes of counseling sessions (i.e. family, collateral only,multi-family, multi-participant and participant-only)were collected via the Service Contact Logs (SCLs) used bythe CYT therapists. These measures were added to thespecifications and interesting results emerged. [Note thatin Table 3, dash lines indicate instances where certaintypes of counseling sessions were not part of that inter-vention (e.g. family counseling was not conducted inMET/CBT5).]
Case management had a significant impact on episodecosts for MET/CBT5, adding an estimated $283 toepisode costs per hour of case management services.Case management was positive and significant in theMDFT specification, but insignificant for the otherconditions.
Each hour of family counseling added $72 to episodecost for ACRA and $30 to episode cost for MDFT. Of par-ticular significance are the counseling hours provided to
the participants. In all conditions except one, these ses-sions were positively and significantly related to episodecosts. Also, the participant (client) only (i.e. individualtherapy) coefficients were always greater than the multi-participant (i.e. group therapy) coefficients. This result isexpected, given that the labor cost for group sessions isdistributed across more clients.
Summary of results
Recounting the findings, in the incremental study armaverage economic costs per treatment episode were$1089 for MET/CBT5, $1256 for MET/CBT12 and$3290 for FSN, following the respective orders of averageclient/family contact hours (5.4, 10.4, 19.4) and averagestaff hours (2.9, 4.4, 10.2) in these interventions. In thealternative study arm average economic costs per treat-ment episode were $1445 for MET/CBT5, $1459 forACRA and $2105 for MDFT. Although the longer and/ormore intensive interventions usually had higher totalcosts, the results suggest more site-to-site variation in thecost per week than there was between conditions.
Table 3 Regression analysis of episode costs, by treatment condition.
Explanatory variableMET/CBT5(n = 195)
MET/CBT12(n = 92)
FSN(n = 95)
ACRA(n = 100)
MDFT (n = 93)
Age 58.23** -26.01 39.32 10.79 -47.20(26.39) (25.59) (57.84) (26.75) (29.23)
Male 192.24** 11.39 -17.94 34.84 112.69(76.98) (85.11) (192.59) (80.38) (99.60)
White -252.31*** -132.50* 249.34* 68.38 149.53(78.90) (69.07) (146.32) (87.82) (90.48)
Alternative arm 306.87*** – – – –(70.74)
Cost-of-living index 26.15*** 8.16** -13.79 29.57*** 63.43***(3.70) (3.52) (9.70) (4.82) (6.10)
Case management hours 282.71*** 32.30 -36.96 20.75 30.44**(41.04) (41.88) (47.58) (21.48) (11.85)
Counseling hoursFamily – – 53.66 71.83** 29.96***
(36.14) (27.85) (9.17)Collateral only 32.19 244.82 56.67 28.48 120.50***
(159.41) (944.39) (51.44) (33.10) (27.44)Multi-family – – 28.56** – –
(12.57)Multi-participant 73.43*** 65.45*** 107.69*** – –
(23.44) (8.10) (24.22)Participant only 231.22*** 148.45*** 197.66** 46.81*** 17.33
(43.53) (50.59) (98.08) (13.78) (20.13)Constant -3675.86*** 16.36 2395.02* -2397.76*** -4623.21***
(655.16) (575.74) (1316.66) (684.09) (691.66)R2 0.61 0.56 0.58 0.52 0.84
Notes: Standard errors in parentheses. MET/CBT5 = motivational enhancement treatment/cognitive behavior therapy 5-session; MET/CBT12 = MET/CBT5 +cognitive behavior therapy 7-session; FSN = MET/CBT12 + family support network; ACRA = adolescent community reinforcement approach; MDFT = multi-dimensional family therapy. *Statistically significant, P < 0.10. ** Statistically significant, P < 0.05. *** Statistically significant, P < 0.01.

© 2002 Society for the Study of Addiction to Alcohol and Other Drugs Addiction, 97 (Suppl 1), 84–97
94 Michael T. French et al.
DISCUSSION
Limitations
Despite the programmatic and policy value of these orig-inal results, certain limitations pertaining to the data col-lection and analysis must be addressed. First, theDATCAP was designed to analyze resource use and costsfor a full fiscal year (French 2001b). Because the DATCAPadministration at the CYT programs covered a 6-monthperiod, seasonal characteristics and unexpected varia-tions in caseflow may have influenced the cost estimates.If present, however, these fluctuations were probablyminor, with only a small impact on the final results (e.g.utilities during winter/spring, tax schedules, employeevacations). More importantly, the half-year approachdampened the start-up and wind-down costs associatedwith the subject randomization process, a potentiallymore serious problem than seasonality.
A second limitation concerned the proper exclusion ofresearch costs. Recall that personnel completing the DAT-CAP were instructed to omit the resources and costs asso-ciated with the research component of the CYT study. Forexample, the cost of a research assistant who was hired tocode and process SCL data was not included in the DAT-CAP calculations. Other research-specific resources (e.g.computer equipment, clerical support, research offices)were excluded from the cost estimation as well. Theseresource exclusions were necessary to calculate the truecosts of service delivery and for comparability with moretraditional treatment programs. However, the allocationof resources across the research and clinical componentsrequired expert judgement on some occasions.
Thirdly, because sites with common interventionsoften shared resources across sites (e.g. clinical supervi-sors, clinical advisors) and/or conditions (e.g. copymachines, office space), the allocation of costs for sharedresources was a difficult and sometimes subjective task.In general, shared resources were allocated to sites andinterventions based on a diary method for personnel anda usage rate technique for equipment and facilities. Nev-ertheless, combining site data to derive intervention-specific cost estimates was appropriate to minimizevariability and potential site-specific biases.
Exploring the variation in costs
Variation in the cost of service delivery among the CYTtherapies and treatment sites was both expected andsomewhat predictable. The five manualized treatmentapproaches offered different services (e.g. group versusindividual sessions), involved different parties (e.g. client,family, guardian, etc.), and were delivered for differentdurations (e.g. 6 weeks versus 12 weeks). Obviously, apriori, cost differences among the therapies were antici-
pated. Cross-site cost variation for common interventionswas also expected. Clinical and administrative staff ateach site faced unique challenges in implementing theCYT study design (e.g. urban versus rural, high versuslow cost of living). These challenges naturally influencedthe nature and extent of the resources hired to deliver theCYT interventions. Indeed, community-based treatmentprograms have similar financial, organizational and clin-ical constraints as the participating organizations in thisresearch study. Therefore, proper interpretation of thecost estimates requires a close inspection of these site-specific factors.
Results from the regression analysis of episode costs byintervention yielded relatively large R2 values, rangingfrom 0.52 to 0.84. This implies that 50% or more of thevariation in costs can be explained by the selected regres-sors. Cost-of-living differences in site location, and to amuch larger extent, actual time spent delivering theinterventions (i.e. case management and counseling),were consistently positive and significantly related toepisode costs.
Site location was probably the most obvious contribu-tor to the cross-site variation in intervention costs.Wages, rents and other resource prices in large metropol-itan cities typically exceed those in rural areas. Becausethe CYT study included geographically diverse treatmentsites, cost-of-living differences in resource costs prevailed.According to the American Chamber of CommerceResearchers Association (ACCRA 2000), Philadelphia,Pennsylvania (where CHOP is located) is approximately19% more expensive than Madison County (part of the StLouis, Missouri metropolitan area and the location ofCHS-MC). This cost-of-living disparity explains a portionof the cost differentials among the interventions that arecommon to CHOP and CHS-MC. Similarly, Farmington,Connecticut (UCHC) had a higher cost-of-living indexthan St Petersburg, Florida (PAR) (ACCRA 2000). Conse-quently, cost differentials between UCHC and PAR canbe attributed partly to geographical cost-of-livingdifferences.
Although not captured in the regression analysis,another factor that probably contributed to cross-site dif-ferences in intervention costs was the composition andassignment of personnel. Because labor accounted for62.2% to 90.1% of the total intervention costs acrosssites, differences in wage rates due to factors other thangeographical location probably affected the cost esti-mates. For example, CHOP mainly hired PhD-level thera-pists rather than therapists with less education. Thisstaffing pattern differed from other sites, which employedmainly master’s-level counselors. Naturally, personnelwith more education, experience and credentials willcommand higher salaries. Hence, cost variationsbetween CHOP and other sites that delivered the same

Cost of outpatient marijuana treatment for adolescents 95
© 2002 Society for the Study of Addiction to Alcohol and Other Drugs Addiction, 97 (Suppl 1), 84–97
interventions were probably influenced by humanresource decisions. It is conceivable that more creden-tialed counselors and other professional labor will gener-ate better treatment outcomes, ceteris paribus, than lesscredentialed personnel. This issue will be addressed insubsequent cost-effectiveness and benefit–cost analyses.
A less obvious, but potentially large influence on thecost findings, is excess human resource capacity. Inadministering DATCAP and evaluating the delivery andcost of substance abuse treatment services at over 70 pro-grams, the under-utilization of resources has been rela-tively rare. In fact, most publicly funded programs seem to‘overextend’ their personnel (i.e. have higher case-loads orlonger hours than counselors feel are appropriate). For theCYT study, however, significant variation occurred incounselor availability (i.e. capacity) for similar case-loadsand hours. For example, in the incremental study arm,MET/CBT5 was provided at UCHC with 0.3 FTEs for anaverage of 6.6 adolescents while PAR used 1.2 FTEs toserve an average of 3.7 adolescents per week. In the alter-native arm, CHS-MC used 0.4 FTEs to serve 5.5 adoles-cents while CHOP used 1.4 FTEs to serve 5.1 adolescentsper week. Case-load differences across sites were duelargely to organizational capacity, human resource allo-cations at each site, and the challenges associated withstaffing a short-term study. Presumably, a continuouslyoperating program would be able to better manage itscapacity by using part-time staff as did UCHC or sharingresources across other programs in the organization as didCHS-MC. In such cases, the corresponding costs of treat-ment services would probably be lower than reported here.
Research and policy significance
We believe the cost estimates presented in this paper arethe first published figures for outpatient adolescent sub-stance abuse treatment using standardized economicmethods. Although the DATCAP has now been used toestimate the economic cost of addiction services innumerous studies, only the CYT project involved inter-ventions that were specifically designed for youth.Because marijuana is largely the drug of choice amongadolescents, and greater than 80% of adolescent treat-ment for cannabis dependence is delivered in outpatientsettings, this cost analysis of the CYT experiment is bothtimely and important (Dennis et al. 1999; 2002a; Dennis& McGeary 1999). As new economic data for adolescentdrug treatment emerges, these results can be further stud-ied and assessed. Meanwhile, it is interesting to see howthe CYT cost estimates compare to the existing literaturefor similar adult programs using standardized measures,as well as unstandardized estimates for adolescents.
Approximately one-quarter of all completed DATCAPswere conducted at adult outpatient drug-free programs.
The average weekly cost of outpatient drug-free treat-ment at these programs was $119 (in 1999 dollars)(French et al. 1996, 1997; French & McGeary 1997;McCollister & French, 2002; Salomé & French 2001). Theaverage weekly cost of adolescent treatment among CYTprograms ranged from $90 to $313. Although the aver-age weekly cost of MET/CBT12 was lower than the aver-age weekly cost for adult treatment, this interventionincluded 7 weeks of group therapy, a low-cost service.
Although it was based on non-standardized self-reported information from program directors, one of thefew sources of treatment cost estimates for adolescents isthe National Treatment Improvement Evaluation Study(NTIES; Gerstein & Johnson 1999). For adolescents inoutpatient treatment, NTIES estimated that for a lengthof stay of 2 months, the median weekly cost of adolescentoutpatient treatment was about $267 (adjusted to 1999dollars). Mean cost estimates were not reported for ado-lescents separately, but mean costs were typically 25%higher (i.e. mean weekly cost of $356, adjusted to 1999dollars) than the median costs in all outpatient treatmentprograms. Thus, the cost estimates reported by NTIES arehigher than the DATCAP estimates reported here for allfive CYT interventions, but considerable caution needs tobe exercised in making such direct comparisons becausethe cost methodologies were different and it is unclearwhether the interventions are comparable in terms of theservices provided.
It is perhaps informative to compare the episode costsof the five CYT interventions to local reimbursement pol-icies (as reported by our participating clinics) that wouldgenerally only pay about $45–55 for an hour of individ-ual counseling, $20–30 per hour for group counselingand $0–55 for case management. Among the CYT inter-ventions the MET/CBT conditions usually had the lowestestimated cost per treatment episode, but these averageepisode costs are more than 200% of the reimbursementamount, based on existing rates at the various sites.While the ACRA and MDFT interventions were morecostly on an episode basis, the episode costs are only 16–39% more than the reimbursement amounts. Finally,FSN cost more than the other interventions for an aver-age episode, but also provided the most comprehensive setof services (e.g. group counseling, in-home therapy, casemanagement), which can draw reimbursement fromnumerous sources.
CONCLUSION
In summary, the economic evaluation of the CYT projectwas planned as a two-stage process. First, data werecollected and the opportunity costs of adolescent treat-ment were estimated and assessed. This paper presentsthe rationale for this initial phase of the economic

© 2002 Society for the Study of Addiction to Alcohol and Other Drugs Addiction, 97 (Suppl 1), 84–97
96 Michael T. French et al.
evaluation along with a description of the methods used,results and implications of the findings. Besides adding tothe growing literature on the costs of outpatient sub-stance abuse treatment, these adolescent treatment costestimates are informative and unique. The second stage ofthe economic analysis of CYT will combine the cost esti-mates with client-specific data on treatment outcomes toconduct cost-effectiveness and benefit-cost analyses.Comprehensive research findings from both phases of theeconomic evaluation will provide CYT investigators, pol-icymakers, substance abuse researchers, and treatmentproviders with the first full set of economic estimates foradolescent programs. This information will facilitate abetter understanding of the economics of addiction per-taining especially to the unique needs and challenges ofadolescent substance abusers.
In general, the CYT interventions with higher episodecosts also provided more services. Understandingwhether this additional investment in treatment servicesis justified economically depends on many factors andwill be the subject of the on-going CYT investigation.Clearly, more research is still needed, but these prelimi-nary cost estimates provide practial financial informationfor delivering adolescent treatment in community-basedprograms.
ACKNOWLEDGEMENTS
Financial assistance for this study was provided by SAM-HSA’s Center for Substance Abuse Treatment (CSAT)(grant nos TI11317, TI11320, TI11321, TI11323 andTI11324) and the National Institute on Drug Abuse(NIDA) (grant nos R01 DA11506 and 3P50 DA07705).The opinions expressed herein are those of the authorsand do not reflect official positions of the government. Theauthors appreciate the valuable work of Allison Angus,Betty Buchan, Tracy Karvinen, Jodi Leckrone, Karen Ret-tick, Zeena Tawfik and James West. The authors are alsograteful for the comments, suggestions and supportoffered by Joe Burleson, Jean Donaldson, Mark Foss,James Fraser, Rodney Funk, Mark Godley, Amelia Goem-bel, Nancy Hamilton, Ron Kadden, Yifrah Kaminer,Howard Liddle, A. Thomas McLellan, Melissa McDermeit,Samia Noursi, Suzie Panichelli-Mindel, Brenda Reis,Susan Sampl, Christy Scott, Manny Tejeda, Janet Titus,Joan Unsicker, Cathy Urmann and Bill White. M. T. F. andM. C. R. were employed at the University of Miami duringthe completion of this research.
REFERENCES
American Chamber of Commerce Researchers Association(ACCRA) (2000) Cost of Living Index. Arlington, VA: ACCRA.
American Psychiatric Association (APA) (1994) American Psy-chiatric Association Diagnostic and Statistical Manual of MentalDisorders, 4th edn. Washington, DC: APA.
American Society of Addiction Medicine (ASAM) (1996) PatientPlacement Criteria for the Treatment of Psychoactive SubstanceDisorders, 2nd edn. Chevy Chase, MD: ASAM.
Bradley, C. J., French, M. T. & Rachal, J. V. (1994) Financing andcost of standard and enhanced methadone treatment. Journalof Substance Abuse Treatment, 11, 433–442.
Bray, J. W., French, M. T., Bowland, B. J. & Dunlap, L. J. (1996)The cost of employee assistance programs (EAPs): findingsfrom seven case studies. Employee Assistance Quarterly, 11, 1–19.
Cartwright, W. S. (1998) Cost–benefit and cost-effectivenessanalysis of drug abuse treatment services. Evaluation Review,22, 609–636.
Cartwright, W. S. (2000) Cost–benefit analysis of drug treat-ment services: review of the literature. Journal of Mental HealthPolicy and Economics, 3, 11–26.
Center for Substance Abuse Treatment (CSAT) (1992) Empow-ering Families, Helping Adolescents: Family-Centered Treatment ofAdolescents with Alcohol, Drug Abuse, and Mental Health Prob-lems. Technical Assistance Publication Series no. 6. Rockville,MD: US Department of Health & Human Services.
Center For Substance Abuse Treatment (CSAT) (1993)Guidelines for the Treatment of Alcohol and Other Drug-AbusingAdolescents. Treatment Improvement Protocol (TIP) Series 4Rockville, MD: US Department of Health & Human Services.
Center for Substance Abuse Treatment (1999) Treatment of Ado-lescents with Substance Use Disorders. Treatment ImprovementProtocol (TIP) series 32. Rockville, MD: Substance Abuse andMental Health Services Administration.
Dennis, M. L., Babor, T. F., Roebuck, M. C. & Donaldson, J.(2002a) Changing the focus: the case for recognizing andtreating cannabis use disorders. Addiction, 97 (Suppl 1), 4–15.
Dennis, M. L., Godley, S. & Titus, J. (1999) Co-occurring psychi-atric problems among adolescents: variations by treatment, level ofcare and gender. TIE Communiqué, pp. 5–8, 16. Rockville, MD:Substance Abuse and Mental Health Services Administration,Center for Substance Abuse Treatment.
Dennis, M. L. & McGeary, K. A. (1999) Adolescent alcohol andmarijuana treatment: kids need it now. TIE Communiqué, pp.10–12. Rockville, MD: Substance Abuse and Mental HealthServices Administration, Center for Substance Abuse Treat-ment.
Dennis, M. L., Titus, J. C., Diamond, G., Donaldson, J., Godley, S.H., Tims, F., Webb, C., Kaminer, Y., Babor, T., Roebuck, M. C.,Godley, M. D., Hamilton, N., Liddle, H., Scott, C. K. & and TheCYT Steering Committee (2002b) The Cannabis Youth Treat-ment (CYT) experiment: rationale, study design and analysisplans. Addiction, 97 (Suppl 1), 16–34.
Drummond, M. F., O’Brien, J. O., Stoddart, G. L. & Torrance, G.W. (1997) Methods for the Economic Evaluation of Health CareProgrammes, 2nd edn. New York: Oxford University Press.
Dunlap, L. J. & French, M. T. (1998) A comparison of two meth-ods for estimating the costs of drug abuse treatment. Journal ofMaintenance in the Addictions, 1, 29–44.
French, M. T. (1995) Economic evaluation of drug abuse treat-ment programs: methodology and findings. American Journalof Drug and Alcohol Abuse, 21, 111–135.
French, M. T. (2000) Economic evaluation of alcohol treatmentservices. Evaluation and Program Planning, 23, 27–39.
French, M. T. (2001a) Drug Abuse Treatment Cost Analysis

Cost of outpatient marijuana treatment for adolescents 97
© 2002 Society for the Study of Addiction to Alcohol and Other Drugs Addiction, 97 (Suppl 1), 84–97
Program (DATCAP): Program Version, 7th edn. Coral Gables,FL: University of Miami. Available at: http://www.DAT-CAP.com.
French, M. T. (2001b) Drug Abuse Treatment Cost Analysis Pro-gram (DATCAP): Program Version User’s Manual, 7th edn. CoralGables, FL: University of Miami. Available at: http://www.DATCAP.com.
French, M. T., Bradley, C. J., Calingaert, B., Dennis, M. L. &Karuntzos, G. T. (1994) Cost Analysis of Training andEmployment Services in Methadone Treatment. Evaluationand Program Planning, 17, 107–120.
French, M. T., Dunlap, L. J., Galinis, D. N., Rachal, J. V. & Zarkin,G. A. (1996) Health care reforms and managed care for sub-stance abuse services: findings from 11 case studies. Journal ofPublic Health Policy, 17, 181–203.
French, M. T., Dunlap, L. J., Zarkin, G. A., McGeary, K. A. &McLellan, A. T. (1997) A structured instrument for estimat-ing the economic cost of drug abuse treatment: the DrugAbuse Treatment Cost Analysis Program (DATCAP). Journal ofSubstance Abuse Treatment, 14, 1–11.
French, M. T. & Martin, R. F. (1996) The costs of drug abuse con-sequences: a summary of research findings. Journal of Sub-stance Abuse Treatment, 13, 453–466.
French, M. T. & McGeary, K. A. (1997) Estimating the economiccost of substance abuse treatment. Health Economics, 6, 539–544.
French, M. T., Salomé, H. J., Krupski, A., McKay, J. R., Donovan,D. M., McLellan, A. T. & Durell, J. (2000) Benefit–cost analysisof residential and outpatient addiction treatment in the Stateof Washington, Evaluation Review, 24, 609–634.
French, M. T., Salomé, H. J., Sindelar, J. L. & McLellan, A. T.(2002) Benefit–cost analysis of addiction treatment. method-ological guidelines and application using the DATCAP andASI. Health Services Research, 37, 433–455.
Gerstein, D. R. & Johnson, R. A. (1999) Adolescents and YoungAdults in the National Treatment Improvement Evaluation Study.Rockville, MD: National Evaluation Data Services, SubstanceAbuse and Mental Health Services Administration, Center forSubstance Abuse Treatment. Available at: http://www.health.org/nties/highlight/highall.htm.
Godley, S. H., Meyers, R. J., Smith, J. E., Godley, M. D., Titus, J.M., Karvinen, T., Dent, G., Passetti, L. & Kelberg, P. (2001) TheAdolescent Community Reinforcement Approach for AdolescentCannabis Users. (DHHS Publication No. (SMA) 01-3489, Can-nabis Youth Treatment (CYT) Series, Volume 4). Rockville,MD: Center for Substance Abuse Treatment, Substance Abuseand Mental Health Services Administration. Available at:http://www.chestnut.org/li/cyt/products/acra_cyt_v4.pdf.
Gold, M. R., Siegel, J. E., Russell, L. B. & Weinstein, M. C., eds(1996) Cost-effectiveness in Health and Medicine. New York:Oxford University Press.
Hamilton, N., Brantley, L., Tims, F., Angelovich, N. &McDougall, B. (2001) Family Support Network (FSN) forAdolescent Cannabis Users. (DHHS Publication No. (SMA)01-3488, Cannabis Youth Treatment (CYT) Manual Series,Volume 3). Rockville, MD: Center for Substance AbuseTreatment, Substance Abuse and Mental Health ServicesAdministration. Available at: http://www.chestnut.org/li/cyt/products/FSN_CYT_v3.pdf.
Health and Human Service (HHS) Press Office (1998) Substance
Abuse—a National Challenge. Prevention, Treatment andResearch at HHS, HHS Fact Sheet, 18 December. Washington,DC: US Government Printing Office. Available at: http://www.hhs.gov/news/press/1998pres/981218b.html.
Institute for Social Research (1999) Monitoring the Future Study.Ann Arbor, MI: University of Michigan.
Liddle, H. A. (1995) Conceptual and clinical dimensions of amultidimensional, multisystems engagement strategy in fam-ily-based adolescent treatment. Psychotherapy: Theory,Research, Practice and Training, 32, 39–58.
Liddle, H. A. (2002) Multidimensional Family Therapy (MDFT) forAdolescent Cannabis Users. (DHHS Publication No. (SMA) 02-3660, Cannabis Youth Treatment (CYT) Manual Series, Vol-ume 5). Rockville, MD: Center for Substance Abuse Treat-ment, Substance Abuse and Mental Health ServicesAdministration. Available at: http://www.chestnut.org/li/cyt/products/MDFT_CYT_v5.pdf.
McCollister, K. E. & French, M. T. (2002) The economic cost ofsubstance abuse treatment in criminal justice settings. In:Leukefeld, C. G., Tims, F. & Farabee, D., eds. Treatment of DrugOffenders: Polices and Issues, pp 22–37. New York: SpringerPublishing Compary.
Meyers, R. J. & Smith, J. E. (1995) Clinical Guide to Alcohol Treat-ment: the Community Reinforcement Approach. New York: Guil-ford Press.
Office of Applied Studies (1997) Preliminary Results from the1996 National Household Survey on Drug Abuse. Rockville, MD:Substance Abuse and Mental Health Services Administra-tion.
Salomé, H. J. & French, M. T. (2001) Using cost and financinginstruments for economic evaluation of substance abusetreatment services. In: Galanter, M., ed. Recent Developments inAlcoholism, Vol. XV. Services Research in the Era of ManagedCare, Section III, Chapter 11, pp. 253–269. New York: KluwerAcademic/Plenum Press.
Sampl, S. & Kadden, R. (2001) Motivational Enhancement Therapyand Cognitive Behavioral Therapy (MET-CBT-5) for AdolescentCannabis Users. (DHHS Publication No. (SMA) 01-3486, Can-nabis Youth Treatment (CYT) Manual Series, Volume 1).Rockville, MD: Center for Substance Abuse Treatment, Sub-stance Abuse and Mental Health Services Administration.Available at: http://www.chestnut.org/li/cyt/products/mcb5_cyt_v1.pdf.
Substance Abuse and Mental Health Services Administration(SAMHSA), Center For Substance Abuse Treatment (CSAT)(1997) Cooperative Agreements for a Multi-Site Study of theEffectiveness of Treatment for Cannabis (Marijuana) DependentYouth. Guidance for Applicants (GFA), No. TI 97–002. Rock-ville, MD: SAMHSA/CSAT.
Titus, J. C. & Godley, M. D. (1999) What research tells us aboutthe treatment of adolescent substance use disorders. Paperpresented at the Governor’s Conference, Chicago, IL.
Webb, C., Scudder, M., Kaminer, Y., Kadden, R. & Tawfik, Z.(2002) The MET/CBT 5 Supplement: 7 Sessions of CognitiveBehavioral Therapy (CBT 7) for Adolescent Cannabis Users.(DHHS Publication No. (SMA) 02-3659, Cannabis YouthTreatment (CYT) Manual Series, Volume 2). Rockville, MD:Center for Substance Abuse Treatment, Substance Abuse andMental Health Services Administration. Available at: http://www.chestnut.org/li/cyt/products/CBT7_CYT_v2.pdf.