-
ARTICLE IN PRESS
Health & Place 12 (2006) 1937
in London, 760 electoral wards as dened in 1998. The analysis
controls for age and sex composition and, as a proxy for
www.elsevier.com/locate/healthplace
1353-8292/$ - see front matter r 2004 Elsevier Ltd. All rights
reserved.
doi:10.1016/j.healthplace.2004.07.002
Corresponding author. Tel.: +44-171-975-5400; fax:
+44-207-975-5500.
E-mail address: [email protected] (S. Curtis).access to care,
spatial proximity to hospitals with psychiatric beds. Poisson
regression modeling incorporating random
effects was used to control for both overdispersion in the
counts of admissions and for the effects of spatial
autocorrelation. The results for NYC and London showed that
local admission rates for all types of condition were
positively and signicantly associated with deprivation and the
association is independent of demographic composition
or access to beds. In NYC, social fragmentation showed a
signicant association with admissions due to affective
disorders and schizophrenia, and for drug dependency among
females. Racial minority concentration was signicantly
and positively associated with admissions for schizophrenia. In
London, social fragmentation was associated positively
with admissions for men and women due to schizophrenia and
affective disorders. The variable measuring racial/ethnic
minority concentration for London wards showed a negative
association with admission rates for drug dependency and
for affective disorders. We discuss the interpretation of these
results and the issues they raise in terms of the potential
and limitations of international comparison.
r 2004 Elsevier Ltd. All rights reserved.
Keywords: Psychiatric inpatient admissions; New York; London;
Ecological analysis; Deprivation indicesThe ecological relationship
between deprivation, socialisolation and rates of hospital
admission for acute psychiatric
care: a comparison of London and New York City
Sarah Curtisa,, Alison Copelanda, James Fagga, Peter
Congdona,Michael Almogb, Justine Fitzpatrickc
aDepartment of Geography, Health Research Group, Queen Mary
College, University of London, London, UKbWagner Graduate School of
Public Service, New York University, USA
cLondon Health Observatory, London, UK
Received in revised form 28 June 2004
Abstract
We report on comparative analyses of small area variation in
rates of acute hospital admissions for psychiatric
conditions in Greater London around the year 1998 and in New
York City (NYC) in 2000. Based on a theoretical
model of the factors likely to inuence psychiatric admission
rates, and using data from the most recent population
censuses and other sources, we examine the association with area
indicators designed to measure access to hospital beds,
socio-economic deprivation, social fragmentation and
ethnic/racial composition. We report results on admissions for
men and women aged 1564 for all psychiatric conditions
(excluding self-harm), drug-related substance abuse/
addiction, schizophrenia and affective disorders. The units of
analysis in NYC were 165 ve-digit Zip Code Areas and,
-
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
193720Introduction: background to the analysis
In the USA and the UK, mental health care for most
patients is provided according to a model emphasising
care in the community, rather than long-term care in
residential institutions. Nevertheless, inpatient psychia-
tric care in acute hospitals continues to play an
important role in community-based systems and con-
sumes signicant health care resources to meet the costs.
Policy making and nancial planning for mental health
services therefore require information on the factors
associated with use of psychiatric inpatient care.
In this paper, we discuss the signicance of ecological
analyses for mental healthcare planning. By means of a
comparative study of small area variations in the rate of
psychiatric inpatient use by local populations, we
illustrate the ecological factors that relate to psychiatric
inpatient use in New York City (NYC), USA, and
London, UK. While their health systems vary signi-
cantly and there are some differences in their social
geographies, these cities have several features that justify
an international comparative study, considering them
separately from the rest of the country as a whole. They
are both global cities, they are atypical of average
conditions prevailing in the rest of the country, they
show considerable internal diversity and they have
complex healthcare systems. Both cities face challenges
in providing services for seriously mentally ill people.
Both have health information systems providing routine
data on admissions, as well as other sources of small
area data on socio-economic conditions, that allow a
similar approach to ecological variation in psychiatric
hospital use.
The ecological analyses presented here concern
patterns of health care use by geographically dened
populations. This approach does not aim to explain or
predict service use by individual patients and one should
not assume that individual mental health care users have
characteristics like the population average in their area
of residence. On the other hand, there is a large body of
evidence from health geography demonstrating that
individual and ecological characteristics may interact,
such that conditions in small areas may have signicance
for individual experience of illness and health services
use (Macintyre et al., 1993; Kearns and Joseph, 1993;
Jones and Moon, 1993; Duncan et al., 1996; Curtis and
Jones, 1998, Diez-Roux, 1998).
Ecological studies may also illustrate differences
between local communities in service use, which are
signicant for the organization and nancing of mental
health services. In the UK, most psychiatric services
used by the population are provided by the National
Health Service (NHS), a comprehensive, integrated
system in which local NHS trusts use budgets allocated
by central government to commission services for the
population in a specic area. Access to health care issignicantly
affected both by the amount of NHS
resource allocated for a local population and by the
ways that this resource is managed at the local level to
commission services. A founding principle of the NHS is
that services should be provided equitably in proportion
to need for populations in all parts of the country. The
information produced in geographical analyses therefore
can help target mental health care resources or inter-
ventions to areas where they are most needed (e.g.,
Smith et al., 1996; Glover et al., 1998; DH, 2003).
The organization of US health care system is more
diversied and care of individual patients may be funded
by one or more of a range of different, independent
private insurance schemes, or publicly funded by
Medicaid or Medicare (McAlpine and Mechanic,
2000). Access to services is therefore largely dependent
on the health care plan providing coverage for the
patient and the system does not allow for national
control of resource allocation to different areas. Never-
theless, there is constant emphasis in health policy on
the requirement to manage health care in order to make
it more cost-effective. Therefore, a focus on small area
variations in mental health care use may have relevance
for mental health service planning in the US situation.
For example, recommendation 2.4 of the Presidents
New Freedom Commission on Mental Health (2003: p. 8,
44) proposes the production of comprehensive State
Mental Health Plans to increase exibility of resource
use, expand options and arrays of services and supports,
and encourage states and localities to develop compre-
hensive health care strategies. It seems likely that, in
order to produce these plans, States and local govern-
ments will need to be informed about local variations in
current mental health care resource use and to judge
whether these variations appear to be justied on
grounds of cost-effectiveness in meeting the needs of
patients with mental illness.
Whereas ecological associations do not necessarily
provide explanations for differences in use of health
services between areas, they can be used to predict local
differences in use of psychiatric care and, as argued
above, they may help to inform service planning and
provision in different urban settings. A large body of
theoretical and empirical evidence from the UK, the
USA and elsewhere suggests that several types of
ecological factors are associated with varying use of
psychiatric care at the small area level. It may be
possible to argue that such associations are suggestive of
direct or indirect causal processes producing variation
among populations in different places in need for, and
access to psychiatric care. In North America these
relationships were discussed by Dear and Wolch (1987),
who proposed a general model of the service-dependent
ghetto, describing the typical geographical concentra-
tion of mental health service users. In NYC, Schweitzer
and Kierszenbaum (1978) examined variations in
-
admission rates in Brooklyn (Kings County) and Almog
et al. (2004) reported time trends in small area variation
in NYC during the 1990s. In the UK, hospital admission
rates have been examined using ecological analysis by
Giggs (1986) in Nottingham, by Dean and James (1981)
in Plymouth, and by several groups of authors in
London and the surrounding area (Thornicroft, 1991;
Harvey et al., 1996; Glover et al., 1998; Johnson et al.,
1998). Congdon et al. (1998) also found associations
between socio-economic conditions and small area
variation in rates of use of community services for
serious mental illness in London. Nationwide analysis of
small area variation in psychiatric hospital use was also
reported by Carr-Hill et al. (1994) and Smith et al.
(1996). There are examples of similar studies in cities in
other parts of Europe (Dekker et al., 1997 for
Amsterdam; Driessen et al., 1998 for Maastricht;
Maylath et al., 1999, 2000 for Hamburg; Thornicroft
et al., 1993 for Verona).
There is some variability in the ndings reported, and
this may be partly due to differences among these studies
an
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
1937 21in the type of urban setting, the type of statistical
approach used to test for ecological associations and the
measures of social conditions and of hospital use
examined. Some studies have shown that in the same
setting, admission rates for different types of psychiatric
condition have different ecological relationships with
social indicators (Thornicroft et al., 1993; Tansella et
al.,
1993; Harrison et al., 1995; Boardman et al., 1997;
Koppel and McGufn, 1999). For example, hospitaliza-
tion rates due to disorders related to schizophrenia or
substance abuse are more consistently associated with
socio-economic deprivation than affective or neurotic
disorders1.
1For example, in Verona, Italy, Thornicroft et al. (1993)
and
Tansella et al. (1993) showed that while indicators of area
deprivation predicted rates of mental health service use for
schizophrenic conditions, these associations were not
consis-
tently related with use of services for neurotic disorders.
Harrison et al. (1995) showed that for districts in North
West
England, deprivation was more strongly associated with area
variation in admission for psychotic disorders than for non-
psychotic conditons. In North Staffordshire, Boardman et al.
(1997) analysed the ecological relationship at ward level
between deprivation indicators and standardized admission
rates for schizophrenic, affective, neurotic, substance
abuse
disorders and found that both psychotic and non-psychotic
conditions were signicantly and positively associated with
deprivation indicators. The correlations were weaker for
affective disorders than for other causes of admission. A
study
in Cardiff by Koppel and McGufn (1999) found associations
between psychiatric admission rates at ward level and
composite measures of deprivation as well as with specic
poverty measures like unemployment. These varied by cause of
admission in that drug related disorders and schizophrenia
showed stronger associations than affective and neurotic
disorders.affordable accommodation and where some specialist
psychiatric and social support services are available.
Breeder and drift effects operating together are thought
to cause greater concentrations of people with severe
mental illness in areas where on average the population
is relatively poor, accommodation is cheap or where
communities lack strong social support systems and
social cohesion.
Varying access to care may also affect the pattern.
This is supported by the nding that populations living
close to hospitals are more likely to use them than
populations living at a greater distance (the distance
decay effect in hospital use). Thus some local popula-
tions within a city may have higher levels of hospitaliza-
tion just because they are closer to the supply of beds.
Historically, large hospitals in major cities like London
and New York were established in inner city areas, andwe
(usople tend to be excluded from some (usually
althier) parts of the city and will move towards other
ually poor inner city) areas where they can ndtor
peereby deprived environments with high levels of
omie cause or exacerbate mental illness. Commenta-
s also refer to drift effects, by which mentally illcau
whsal pathways may operate through breeder effects,LaSome
researchers have also compared the predictive
power of different social indicators. For example,
Thornicroft (1991) and Koppel and McGufn (1999)
demonstrated that certain specic area indicators that
are updated annually, such as small area unemployment
rates, predict psychiatric admissions as effectively as
composite socio-economic indicators that require de-
cennial census data. This may be important for service
planning because during the period between censuses,
social indicators that can be regularly updated may
more accurately reect changing socio-economic condi-
tions at the local level.
Taken together, these empirical studies suggest that at
the local level, within cities, several groups of ecologi-
cal factors are often positively associated with higher
levels of psychiatric hospital use. These are:
relatively high levels of poverty and socio-economicdeprivation
in the local population; relatively high levels of social
fragmentation andindividual isolation in the local community
(also
described by Durkheim (1897) as anomie); locally high
concentrations of minority ethnic groups; close spatial proximity
of the area to hospitals withpsychiatric beds.
Explanations for these associations are thought to be
complex, and they may be summarized as a combination
of different processes (as discussed for example by Smith
and Hanham, 1981; Giggs, 1988, Dear and Wolch, 1987;
Dohwenrend et al., 1992; Takahashi and Gaber, 1998;
mont et al., 2000; Almog et al., 2004). One set of
-
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
193722they are now often located in relatively deprived areas,
so that socio-economic factors and proximity to beds
may be spatially correlated. Some ecological studies of
varying hospitalization rates therefore include indicators
of spatial proximity to services (eg Carr-Hill et al., 1994;
Smith et al., 1996; Almog et al., 2004; Maylath et al.,
1999) and try to establish whether associations with
socio-economic conditions are independent of spatial
proximity to the supply of beds.
Access to primary and ambulatory services may also
be variable for the populations of small areas, which
may affect their use of hospitals. The Commission on
Mental Health in the US observed that:
Too often the short term inpatient care and
emergency services in hospitals are used as the rst
contact for uninsured and underinsured populations.
(Commission on Mental Health, 2003, p. 71).
The comments by the commission seem to conrm that
emergency inpatient hospital care is being used as a rst
response service for some people with mental illness
because of lack of access to ambulatory care alternatives.
This may occur in the event of crises arising when mental
illness has not been managed effectively in the commu-
nity. It raises questions about whether such use of
inpatient care is effective or efcient in a mental health
system based on a model of care in the community.
Commentators from European countries have also
commented that community mental health services need
to be better developed and that high levels of hospitaliza-
tion in some areas may be compensating for a lack of
access to other forms of social or community support
(Johnson et al., 1998; Maylath et al., 1999).
This is all the more important because it seems that
such variation in use of inpatient and outpatient care
relates to poverty and to race or ethnic group. Several
observers have criticized the US mental health care
system for what is apparently a lack of access to good
ambulatory mental health care for poor patients without
insurance cover (e.g. Frank and Morlock, 1997; Grob,
1994). This is reported especially for black Americans,
and may be partly related to differences in the way that
health services diagnose and treat patients from this
racial group. Jones and Gray (1986) suggested that there
are discrepancies in the pattern of psychiatric diagnoses
for black and white patients such that there may be
relative overdiagnosis for black patients of schizophre-
nia-related disorders, and an overdiagnosis of whites
for personality and affective disorders. This seems to be
associated with relatively low usage of outpatient care
and high rates of use of inpatient services by black
populations, often funded by the Medicaid program
(Snowden, 1999; Dixon et al., 2001; Wang & Demler,
2002). For example, Dixon et al. (2001) report a large
study of service use for schizophrenia in the populationunder 65
years of age, and found that, although
incidence of diagnosed schizophrenia and associated
use of hospital care were relatively high among black
Americans, whites were about 1.5 times as likely as
blacks to have received outpatient care and 1.3 times as
likely to have received individual therapy. Reports of
relatively high rates of psychiatric illness requiring
hospital treatment among African-Carribean British
men include: Van Os et al., (1996), Callan (1996),
Harrison et al. (1997), Bhui and Bhugra (2001).
Thus if ecological studies reveal that in certain areas
the rate of acute hospital use is relatively high, this
could
be open to different interpretations. Such variations
might be appropriate if the prevalence, nature and
severity of mental illness in some areas necessitate higher
rates of inpatient care to provide effective medical
treatment. On the other hand, they might reect varying
access to hospital beds and to effective primary and
ambulatory care which might prevent admission. The
latter scenario suggests that there may be some inap-
propriate use of inpatient services as a rst resort and as
an alternative to ambulatory, community-based-care.
Method to compare geographical differences in
hospitalization rates in New York City and London
We aimed to make a comparative empirical study to
investigate the relationships discussed above in NYC
and London. We analysed small area data, for both
cities, on acute admissions of men and women aged
1564, collated for selected psychiatric conditions, which
we have dened as far as possible in similar terms for
both cities. We have examined the relationship between
local admission rates and a set of predictor variables,
which we also attempted to dene in similar ways for
both cities.
Hospitalization data for NYC were derived from
administrative data in the Statewide Planning and
Research Co-operative System (SPARCS) produced by
the New York State Department of Health. The data
used here represent almost all psychiatric admissions of
NYC residents to non-federal public, non-prot and
proprietary general hospitals in New York State
included in the SPARCS system. Admissions to
Veterans Administration hospitalizations as well as
those outside of New York State are not included in
this analysis. For London, the data were derived from
the Hospital Episode Statistics (HES), which are
compiled for all parts of the country and record all
episodes of inpatient psychiatric care funded by the
National Health Service. The relatively small proportion
of hospital use that is privately funded is excluded
because suitable data are not available. The HES data
used here were for residents of Greater London.
We focus on acute admissions (lasting less than 90
days) for which the main cause of admission is classied
-
as one of categories 290319 inclusive of the World
Health Organization (WHO, 1978) International Classi-
fication of Diseases Version 9 (ICD-9), three-digit
classication. We refer to these here as all psychiatric
conditions (though they exclude, for example, self-harm
categories associated with para-suicide). All psychiatric
conditions are therefore a broad category, including
admissions due to drug and alcohol dependency, organic
problems such as Alzheimers disease, mental retarda-
tion and developmental disorders, as well as illness due
to schizophrenia and affective disorders. We have also
psychiatric beds and socio-economic conditions within
the area. These data were derived from the most recent
population censuses (for the year 2000 in US and 2001 in
UK) and also from other UK sources discussed below.
The demographic data for NYC ZCAs were derived
from the 2000 population census giving the numbers of
males and females in 5-year age groups. For London,
ward level population estimates for 1998 produced by
the London Research Centre were used to estimate
person-years for the relevant period. These population
data were used in combination with the admissions data
to calculate expected numbers of admissions for each
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
1937 23examined the pattern for selected, more specic causes
of mental illness: schizophrenic conditions (coded 295 in
the ICD-9 3 digit classication), affective disorders
(coded 296), and drug dependency (coded 304). We have
selected these because other ecological studies (reviewed
above) found that while they were all correlated with
small area social structure, the different diagnoses
showed varying associations with socio-economic vari-
ables. Although we aimed for consistency in diagnostic
cause of admission there is some difculty due to
changes in classication between ICD version 9, used in
the NYC data, and ICD version 10 (WHO, 1992), used
in the London data2.
In NYC data were collated for 165 ve-digit Zip Code
Areas (ZCAs). Total population size ranges from 4226
to 106,154. In London the spatial units were 760
electoral wards (as dened in 1998) population ranges
from 2257 to 21,162. We examined admissions for men
and women separately in the age groups 1564. Hospital
stays/episodes exceeding 90 days were excluded from the
analysis because we are interested in acute psychiatric
care (which can be seen as part of the spectrum of care
provided in a community based care model involving
ambulatory services and relatively brief inpatient stays
when necessary). The data for NYC are for the 12-
month period April 1999March 2000. In London
hospitalization rates are lower than in New York and
the spatial units are smaller, and as a consequence the
counts of admissions are fewer, so we combined data for
the 3-year period: April 1996March 1999.
Admissions data for small areas were linked to
information relating to the demographic prole of area
populations, the proximity of areas to hospitals with
2The following ICD-10 codes were used, in the London
admissions data, to approximate ICD-9 categories in the NYC
data. This conversion was based on: NHSCCC (2000).
All psychiatric causes: ICD-10 categories F00-99 (approx-
imating to 290-319 of ICD-9).
Schizophrenic disorders ICD-10 codes F20, F21X, F23,
F25, F25x (approximating to ICD-9 295).
Affective psychoses:ICD-10 codes F30-F39 (approximating
to ICD-9 296).
Drug dependency: ICD-10, F11F16, F18, F19 (approx-
imating for ICD-9 304).New York ZCA or London ward. This is the
number
that would occur if the annual rate of admissions for
each sex and age group in the small area were the same
as in the general population of the whole city where it is
situated. This information is used to produce age
standardized admission ratios (SARs) for men and
women (comparing the observed and expected admis-
sions to show whether small area rates of admission are
higher or lower than expected given their demographic
prole). The reference population for SARs of NYC
ZCAs is therefore the general population of the ve
NYC counties, while for London the reference is the
population of Greater London.
To measure spatial proximity to psychiatric beds we
used data on the location and number of psychiatric
beds in hospitals. These were supplied for NYC by New
York State Department of Health and for London by
the Adult Mental Health Service Mapping project,
University of Durham, UK (http://www.dur.ac.uk/
service.mapping/). We used the postcode of individual
hospitals to derive an approximate estimate of geo-
graphic location (based on the centroid of the small area
in which it was situated). This information was used to
generate two measures of spatial proximity to psychia-
tric beds for each small area. One indicator shows
whether or not there is a hospital with psychiatric beds
located within the small area (this measures proximity to
psychiatric beds for the population located in the
immediate vicinity of the hospital). The second is a
general measure of spatial access opportunity3 to all
beds in the city, based on a gravity model (Carr-Hill
3The access opportunity measure used here was calculated
as follows:
Ai SkBkgdik=SmPmgdmk;where Ai is the access score for ith Zip
Code Area; Bk the no. of
psychiatric beds at kth hospital; dik and dmk the distances
from
kth hospital to ith and mth Zip Code Areas, respectively; Pm
the
population in mth Zip Code Area; and g is a function of
distance. An inverse function of distance is used to reect
the
distance decay effect on access. Following Carr-Hill et al.
(1994) the function used is g(d)=e0.2d.For further discussion of
gravity models in the analysis of
hospital distribution, see (Congdon, 1996b).
-
et al., 1994). This assumes that the population of every
area competes for access to all the available beds in the
city, and that in each area, mentally ill people are more
likely to use beds which are geographically closer than
beds which are further away. As discussed above, it was
important to examine local variations in the supply of
psychiatric beds because in both London and NYC many
hospitals have been located in what are now poorer inner
city areas and, as discussed above, this may confound the
association with social and economic variables.
We would have liked to include information on use of
outpatient services, which might have been indicative of
use of alternatives to inpatient care, but these data were
not available for this research. This limitation is
considered in the discussion that concludes this paper.
We used three composite indicators of socio-economic
conditions to reect deprivation, anomie and concentra-
tion of racial/ethnic minority groups. As shown in the
theoretical and empirical evidence summarized above,
these represent different population factors likely to be
independently associated with psychiatric admissions.
The deprivation indicators for NYC and London
were based on components4 dened in similar ways.
Most previous analyses of socio-economic factors
associated with psychiatric hospital use in Britain (e.g.
Glover, 1998; Carr-Hill et al., 1994) have used census-
based socio-economic indicators. For our analysis of
London wards, we employed the Index of Multiple
Deprivation (IMD) which is disseminated by the Ofce
of the Deputy Prime Minister (ODPM) and is widely
used to measure local variation in deprivation and to
inform area-based social policy (DETR, 2000). Several
of the elements of this indicator are derived from sources
that do not depend on the decennial census and can be
compiled on an annual basis for wards throughout the
country. Moreover, unlike the population census (which
does not provide direct information on income poverty),
the IMD indicator includes several measures of relative
numbers of the population qualifying for welfare
benets because of low income, disability or unemploy-
ment. It also includes detailed measures of educational
qualications of the local population, housing depriva-
tion, morbidity and disability and access to essential
services. However, the IMD does not include data on
racial/ethnic composition of the population or variables
relating to anomie. The following analysis shows the
ARTICLE IN PRESS
4The indicator of deprivation for London wards which we
have adopted here was compiled for the Ofce of the Deputy
Prime Minister from a variety of sources and includes
components relating to several different domains. These are
dened as follows (IMD, 2000):
Income domain:
Adults (and children) in income support households, 1998.
Adults (and children) in income-based job seekers allowance
(footnote continued)
HE, 1997-8.
KS2 primary school performance indicators, 1998.
Primary school children with English as an additional
language, 1998.
Absenteeism at primary school, 1998.
Housing domain:
S. Curtis et al. / Health & Place 12 (2006)
193724households, 1998.
Adults (and children) in family credit households, 1999.
Adults (and children) in disability working allowance
households, 1999.
Non-earning, non-IS pensioner and disabled Council Tax
Benet recipients, 1998.
Employment domain:
Unemployment claimant counts, 199899.
People out of work but in TEC government supported
training.
People aged 1824 on New Deal options.
Incapacity benet recipients aged 1659, 1998.
Severe disablement allowance claimants aged 1659, 1999.
Health deprivation and disability domain
Mortality ratios under 65, 199798
Proportion of population receiving attendance allowance or
disability living allowance, 1998.
People of working age receiving incapacity benet or severe
disablement allowance, 199899.
Age/sex standardized morbidity ratio (self reported long
term limiting illness), 1991 census.
Proportion of births with birthweight o2500 g, 199397.Education
skills and training domain:
Working age adults with no qualications, 199598.
Children aged 16+ not in full time education, 1999.
Proportions of 17-19 year olds not successfully applied
forHomeless households in temporary accommodation,
19978.
Houshold overcrowding 1991 census.
Poor private sector housing.
Access domain:
Access to a post ofce.
Access to food shops.
Access to a GP.
Access to a primary school.
To produce an indicator of deprivation for ZCAs NYC
(data from 2000 census), z-score transformations of the
following variables were used:
% population over 16 years old unemployed.
% with income less than $10,000.
inverse of median income in 1999.
% of households qualifying for social security payments.
% households with supplemental income.
% households with public assistance income.
% population over 25 years of age with less than 9th grade
educational level.
% population aged 2164 with a disability.
% individuals over 18 years below poverty level.
% housing units with more than 1 person per room.
% housing lacking complete plumbing facilities.
% housing lacking kitchen facilities.
-
value of the IMD measure as predictor of admissions
and whether better prediction can be obtained by using
social isolation and ethnicity indicators in addition to
the IMD measure. Another advantage of the IMD
measure, for the purposes of this study, is that several of
the components are dened in a similar way to variables
in the US census for 2000. Footnote 4 lists the census
data selected for NYC ZCAs to approximate, as far as
possible, the IMD index. In the IMD index the
component variables are standardized and weighted
according to the results of a factorial analysis. For the
NYC deprivation measure we standardized the variables
(z-scores) and combined the resulting components
without weighting them.
The indicators of anomie used in London and
NYC5 were previously employed in ecological
studies of variation in suicide rates in London by
themselves as belonging to the white racial/ethnic
category, because there may be other minority groups
with distinctive patterns of use of mental health care,
which are not as frequently reported in the literature
(Burr, 2002; Lu et al., 2002).
Poisson regression modeling incorporating random
effects was used to control for both overdispersion in the
counts of admissions and for the effects of spatial
autocorrelation6. The analysis was carried out in the
WINBUGS analysis package (Spiegelhalter et al., 2000).
This employs Bayesian modeling, which is more suitable
than conventional Poisson modeling for data from small
areas that includes small counts. The dependent variable
in these models was the count of the observed number of
inpatient events (admissions). The expected number of
events was included as an offset term to standardize for
the effect of age and sex. This means that the outcome
variable can be interpreted as the ratio of observed to
expected events (the Standardized Admission Ratios
described above). The deviance was examined in relation
to the number of units in the analysis to check for
overdispersion7.
The analysis produced mean values for beta coef-
cients for the predictor variables in the model. These
were used to assess the signicance of association
ARTICLE IN PRESS
6We have chosen to use a regression model that takes spatial
auto-correlation into account, in preference to a more
conven-
tional Poisson regression model. The Poisson model is often
S. Curtis et al. / Health & Place 12 (2006) 1937 25Congdon
(1996a, 1997, 2001) and in Britain by Whitley
et al. (1999). We have included components which
separately measure the proportions of the population
who live alone, who are not married (which at the
population level we take to represent household level
isolation), who live in privately rented accommodation
or who had moved in the 12 months preceding the
census (reecting residentially mobile populations that
may generally be less likely to form stable neighbour-
hood ties).
We included a variable labelled race, to reect the
concentration of minority racial/ethnic populations. For
this we used census data for London and NYC on self-
dened racial or ethnic category. We used data on the
proportion of the population who identied themselves
in the census as belonging to black or African racial/
ethnic groups (which we have selected because of the
large literature suggesting that this group tend to have
particularly high rates of hospital admission for some
psychiatric disorders). In addition, we have included the
proportion of the population who did not identify
5Indicators of social isolation or social fragmentation were
calculated by combining standardized (z-score)
transformations
of the following components:
For ZCAs in New York City (data from 2000 population
census):
% population living alone.
% population not unmarried or separated.
% population in rented accommodation.
% population who moved house in the previous year.
For wards in London (data from 2001 population census):
% population living alone.
% population not unmarried or separated.
% population in rented accommodation.
Measure of racial composition, NYC:
% of population in households with people of Black or
African American race (alone or in combination)
% of population in households with people of white race
(alone or in combination).suitable for data made up of counts,
but here there are possible
problems of overdispersion in the count data (Cameron and
Trivedi, 1990). With spatially dened units there are likely to
be
issues of spatial correlation in the extraneous variation
(e.g.
Cliff and Ord, 1981). This was apparent in this analysis,
because
we found that a conventional Poisson model gave deviances
considerably exceeding the degrees of freedom, indicating
that
the signicance of the regression coefcients of independent
variables may be overstated. Solutions may be to introduce
the
random effects either multiplicatively (e.g. leading to a
negative
binomial) or to additively in the regression link. Here we
have
adopted the mixed model of Besag et al. (1991) which adds
two
kinds of random effects in the regression link, one
spatially
structured, the other being spatially unstructured effects.
Our
approach differed from the Besag et al. model because
spatial
effects were modelled via the specication of Sun et al.
(1999),
which involves a specic spatial correlation parameter.7To conrm
that the model is appropriate to the data
structure we have examined the size of the deviance at the
posterior mean of the coefcients, which should be similar to
the number of degrees of freedom in the model. The degrees
of
freedom in a model without random effects is Np where
N=165 and p is the number of independent variables (constant
included). In a model with random effects the degrees of
freedom is problematic because the number of parameters has
to be estimated. Here we have estimated the effective number
of
parameters in deriving the Deviance Information Criterion
(Spiegelhalter et al., 2002) which indicates the goodness of t
of
the model.
-
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
193726between the predictor variable and the rate of admission
(dependent variable). The ratio of the mean beta value
to the standard deviation indicates the signicance of the
association. Where the mean of the beta coefcient has a
value more than 1.96 the standard deviation, and where
the 95% credible interval (the condence interval in
Bayesian analysis) does not include zero, the association
is signicant (indicated by in the tables of results).The sign of
the coefcient shows whether the correlation
is positive or negative. Relatively high ratios of mean to
standard deviation indicate that there is a relatively large
variability in admission ratios associated with variation
in the predictor variable. We also report the deviance at
posterior mean and the deviance information criterion
(DIC), which are indicators of the goodness of t of the
model and the rho coefcient, indicating the degree of
spatial auto-correlation in the regression errors (Sun
et al., 1999).
Results: local variation in hospitalization for psychiatric
conditions in NYC and London
The patterns of admissions show some variation
between New York and London. For example, crude
Fig. 1. ODPM index of deprivarates of admission per 1000 men
aged 1564 are much
higher in New York than in London (25/1000 compared
with 11/1000). Admission rates for women are more
similar between the two cities (11/1000 in NYC and 8/
1000 in London). The large differential between male
and female rates of admission in NYC is most evident
for admissions due to conditions such as drug depen-
dency. (Male admission rates for ICD-9 304 are three
times those for women). These results suggest differences
between the two cities in treatment of some psychiatric
conditions, or possibly variations in prevalence of these
conditions in the population.
Fig. 1 shows a ward level map for London of
variation in the deprivation indicator, showing more
deprived areas (shaded darker) especially in central and
in eastern areas, as well as in some western areas. Ward
level SARs for all psychiatric causes for males aged
1564 in London are shown in Fig. 2, and the higher
levels of admission follow a broadly similar spatial
pattern to that for higher levels of deprivation. Almog et
al. (2004) reported a similar spatial association between
poverty and admission rates in NYC. Figs. 3 and 4,
which show patterns for admissions in London due to
affective disorders and for schizophrenia, demonstrate
that there are some differences in the geographical
tion 2000; London wards.
-
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
1937 27pattern of admission rates according to the type of
diagnosis considered.
Tables 1 to 4 record the results from the regression
analyses for each city and for males and females,
respectively.
The regression analyses of male admission rates for
NYC are shown in Table 1. In most of the models, the
measure of access showing that there was a hospital
located in the same ZCA had a positive and signicant
association with admission rates. Admissions due to
drug dependency, however, were positively associated
with the alternative indicator measuring spatial access to
beds across the city as a whole. After controlling for the
access indicators, deprivation was signicantly and
positively associated with all the causes of admission
considered here for males in NYC. The association with
deprivation was stronger (larger beta coefcient) for
admissions due to drug dependency than for affective
disorders or schizophrenia. For males in NYC, anomie
(social fragmentation) showed a signicant association
with admissions due to all causes and admissions due to
affective disorders and schizophrenia but not for drug
dependency. Racial minority concentration was signi-
cantly and positively associated with admissions for
Fig. 2. SARs for all psychiatric causes;schizophrenia but not
for affective disorders or drug
dependency admissions for males.
Admissions for women in NYC (Table 2) showed
similar associations with predictor variables, except that
beta coefcients for the access variables show weaker
associations which are not always signicant. Also the
anomie indicator was signicantly and positively related
to admissions for drug dependency, which was not the
case for male admissions.
Results for London (Tables 3 and 4) showed variable
associations with the measure of access opportunity.
Most of the signicant associations were positive,
especially for admissions due to schizophrenia and drug
dependency, reecting relatively high rates for wards
which are closer to the overall supply of hospitals with
psychiatric beds across the city. However, for affective
disorders, there was no important association with the
overall access opportunity measure, and female admis-
sion rates for affective disorders were signicantly lower
in wards within which psychiatric hospital beds are
located.
Independently of the measures of access, deprivation
was positively associated with admission rates in
London for all the types of psychiatric conditions
London, males 1564, 19961999.
-
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
193728considered here and for both males and females. Anomie
was associated positively with admissions for men and
women due to schizophrenia and affective disorders, and
for all psychiatric conditions, including these. How-
ever, for drug dependency the association was insignif-
icant. When controlling for deprivation and anomie, the
variable measuring racial/ethnic minority concentration
for London wards showed a negative association with
admission rates for drug dependency and for affective
disorders. For schizophrenia the association showed no
signicant association independent of deprivation and
social fragmentation. This was unexpected, given the
evidence from the UK reviewed above concerning
relatively high rates of admission for African and
Carribean Black men due to conditions such as
schizophrenia. In our data, the association between
racial composition and deprivation in London wards is
quite strong (Pearsons R=0.46), so it is possible that
the strong association with deprivation is masking a
positive link with ethnic composition in these data.
Alternative variables relating to ethnicity were also
tested in the model (e.g. a variable which specically
indicated the proportion of the population belonging to
Black African and Caribbean groups), and they gave
similar results. We discuss the interpretation of this
nding below.
Fig. 3. Standardized admission ratios: acute psychiatric
admissioDiscussion
There are other examples of international compara-
tive studies of psychiatric care in urban settings (e.g.,
Goldberg and Thornicroft, 1998) and some have
employed a standardized methodology to improve the
potential for comparative measurement of variations in
psychiatric care (e.g., Becker et al., 1999). However, we
are not aware of other studies that have taken such a
standardized approach to comparison of psychiatric
hospitalization in NYC and London. This paper
demonstrates that there are some limits to the scope
for direct statistical comparisons using a common
approach to ecological analysis of hospitalization for
these two cities. For example, there are differences
between the two cities in: the average size of the small
areas for which analysis is feasible; the ways in which
causes of admission are coded (using different versions
of the ICD); and the inclusion of data on hospitaliza-
tions paid by commercial insurance in NYC, which is
not provided by HES data for London. There are slight
differences in the years for which data have been
collected (though we do not consider this large enough
to affect the comparison). Also, the socio-economic data
available from sources like the census are similar, but
not dened in exactly the same way. Furthermore, some
ns, London wards c. 1998: males 1564, affective disorders.
-
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
1937 29socio-economic variables may have different social
meaning in the two cities, even though they appear to
be dened in rather similar ways. For example, the
ethnic/racial categories do not relate to groups with
exactly the same origins.
It is also important to note that this analysis has
considered data on hospital admissions. Some of these
will be repeat admissions of the same patients for
ongoing mental health problems and they are therefore
not indications of the incidence or prevalence of mental
illness in the population. Furthermore, service use is not
a very reliable indication of the pattern of mental illness
in the population, and this is not an aetiological study of
factors that may be causing psychiatric conditions. We
have not reported here analyses which take into account
variations in length of stay in hospital which are also
relevant in assessing the health care burden associated
with different patient groups. However, in a separate
paper we show that local variation in the volume of
hospital use (beddays) in NYC shows associations with
socio-economic conditions and proximity to services
that are broadly similar to those found for admissions
(Almog et al., 2004). For this analysis we only had
inpatient data available and we were not able to include
data on rates of use of outpatient hospital services or
other forms of ambulatory psychiatric care. The
Fig. 4. Standardized admission ratios: acute psychiatric
admissaddition of such data would give a clearer impression
of the spectrum of mental health services consumed by
local populations and we plan further research to derive
this information from other sources and include these in
later analyses. It is also important to note that, as this
study relies on routine data sources, any biases in data
recording will affect the results. One possible problem
here concerns the possible under-enumeration of resi-
dent populations in some areas of large cities, which
would tend to result in inated calculations of admission
rates. Under-enumeration may be particularly proble-
matic in areas with large numbers of marginalized and
highly mobile populations, so this might partly explain
our ndings of higher admission rates in deprived areas.
On the other hand, the rates of under-enumeration
would need to be very large (well in excess of 30%) to
fully account for the differences we report here between
observed and expected rates of admission.
Allowing for these caveats about the comprehensive-
ness and comparability of the data, some interesting
observations can be made about the results of the
analyses reported here.
For admissions of men due to schizophrenia and drug
dependency (in London and in NYC), we found that the
rate of hospitalization is partly determined by supply of
hospital beds. This is consistent with commentaries on
ions, London wards c.1998: males 1564, Schizophrenia.
-
ARTIC
LEIN
PRESS
Table 1
Regression results for males 1564 in NYC (controlling spatial
autocorrelation)
Dependent variable
(cause of
admission)
Deviance at
posterior mean
DIC rho Variable *Signicant b-coeff; mean Standard
deviation
Credible interval
0.025 0.975
All psychiatric 163.5 320.6 0.944 Constant 0.420 0.067 0.540
0.283Access opportunity 0.092 0.061 0.029 0.205Whether hospital
in
area
* 0.258 0.058 0.134 0.378
Deprivation * 0.051 0.005 0.041 0.062
Anomie * 0.050 0.017 0.017 0.081
Race * 0.049 0.023 0.007 0.092
ICD-9 304 162.2 304.9 0.956 Constant 0.529 0.129 0.773 0.274Drug
dependence Access opportunity * 0.237 0.095 0.039 0.418
Whether hospital in
area
0.054 0.086 0.120 0.230
Deprivation * 0.072 0.008 0.056 0.088
Anomie 0.041 0.029 0.019 0.094Race 0.034 0.031 0.030 0.094
ICD-9 295 161.0 301.5 0.816 Constant 0.353 0.077 0.500
0.186Schizophrenia Access opportunity 0.007 0.101 0.180 0.196
Whether hospital in
area
* 0.267 0.098 0.083 0.464
Deprivation * 0.028 0.007 0.015 0.041
Anomie * 0.065 0.024 0.015 0.110
Race * 0.153 0.028 0.094 0.203
ICD-9 296 162.5 280.6 0.844 Constant 0.191 0.047 0.286
0.099Affective disorders Access opportunity 0.081 0.054 0.186
0.027
Whether hospital in
area
* 0.212 0.067 0.088 0.353
Deprivation * 0.025 0.005 0.016 0.035
Anomie * 0.075 0.020 0.033 0.110
Race 0.030 0.019 0.007 0.067
S.
Cu
rtiset
al.
/H
ealth
&P
lace
12
(2
00
6)
19
3
730
-
ARTIC
LEIN
PRESS
Table 2
Regression results for females 1564 in NYC
Dependent variable
(cause of
admission)
Deviance at
posterior mean
DIC rho Predictor variable *Signicant b-coeff; mean Standard
deviation
Credible interval
0.025 0.975
All psychiatric 166.20 308.69 0.96 Constant 0.211 0.080 0.381
0.075Access opportunity 0.015 0.056 0.104 0.121Whether hospital
in
area
0.090 0.052 0.014 0.197
Deprivation * 0.041 0.005 0.031 0.049
Anomie * 0.065 0.015 0.037 0.098
Race * 0.034 0.017 0.000 0.069
ICD-9 304 165.90 290.89 0.92 Constant 0.572 0.161 0.888
0.270Drug dependence Access opportunity 0.144 0.105 0.080 0.334
Whether hospital in
area
0.021 0.098 0.172 0.209
Deprivation * 0.066 0.009 0.049 0.084
Anomie * 0.065 0.029 0.010 0.121
Race 0.062 0.037 0.004 0.137ICD-9 295 165.20 297.78 0.78
Constant 0.231 0.061 0.348 0.105Schizophrenia Access opportunity
0.075 0.088 0.225 0.123
Whether hospital in
area
0.177 0.106 0.025 0.392
Deprivation * 0.027 0.007 0.013 0.041
Anomie * 0.070 0.024 0.023 0.118
Race * 0.070 0.028 0.017 0.125
ICD-9 296 164.90 278.02 0.93 Constant 0.148 0.040 0.226
0.067Affective disorders Access opportunity 0.051 0.048 0.141
0.048
Whether hospital in
area
0.077 0.060 0.035 0.203
Deprivation * 0.028 0.004 0.021 0.036
Anomie * 0.066 0.015 0.036 0.095
Race 0.011 0.016 0.042 0.020
S.
Cu
rtiset
al.
/H
ealth
&P
lace
12
(2
00
6)
19
3
731
-
ARTIC
LEIN
PRESS
Table 3
Regression results for males 1564 in London
Dependent variable
cause of admission
Deviance at
posterior mean
DIC rho Predictor variable *Signicant Mean Standard
deviation
Credible interval
0.025 97.5%
All psychiatric 754 1366 0.95 Constant 0.201 0.026 0.254
0.148Access opportunity 0.052 0.030 0.005 0.111Whether hospital
in
area
0.035 0.041 0.047 0.114
Deprivation * 0.594 0.032 0.533 0.655
Anomie * 0.151 0.026 0.098 0.199
Race * 0.148 0.030 0.209 0.093ICD-9 304 630 932 0.92 Constant
0.311 0.051 0.411 0.208Drug dependence Access opportunity * 0.266
0.057 0.146 0.372
Whether hospital in
area
0.086 0.062 0.031 0.211
Deprivation * 0.444 0.085 0.306 0.628
Anomie 0.051 0.057 0.153 0.063Race * 0.128 0.053 0.231 0.023
ICD-9 295 718 1185 0.83 Constant 0.495 0.064 0.657
0.390Schizophrenia Access opportunity * 0.131 0.067 0.017 0.297
Whether hospital in
area
0.058 0.084 0.225 0.104
Deprivation * 0.731 0.061 0.612 0.846
Anomie * 0.338 0.069 0.190 0.450
Race 0.096 0.059 0.202 0.037ICD-9 296 723 1141 0.89 Constant
0.321 0.051 0.430 0.215Affective disorders Access opportunity 0.014
0.074 0.100 0.194
Whether hospital in
area
0.023 0.076 0.177 0.121
Deprivation * 0.694 0.086 0.515 0.836
Anomie * 0.211 0.059 0.091 0.312
Race * 0.267 0.052 0.365 0.159
S.
Cu
rtiset
al.
/H
ealth
&P
lace
12
(2
00
6)
19
3
732
-
ARTIC
LEIN
PRESS
Table 4
Regression results for females 1564 in London
Dependent variable
(cause of
admission)
Deviance at
posterior mean
DIC rho Predictor variable *Signicant b-coeff; mean Standard
deviation
Credible interval
0.025 0.975
All psychiatric 751 1346 0.95 Constant 0.214 0.052 0.350
0.113Access opportunity * 0.099 0.058 0.006 0.252
Whether hospital in
area
0.023 0.049 0.122 0.072
Deprivation * 0.552 0.046 0.465 0.642
Anomie 0.081 0.046 0.007 0.164Race * 0.239 0.037 0.311 0.170
ICD-9 304 466 662 0.92 Constant 0.432 0.098 0.657 0.248Drug
dependence Access opportunity * 0.374 0.100 0.176 0.559
Whether hospital in
area
0.091 0.097 0.294 0.095
Deprivation * 0.500 0.139 0.237 0.751
Anomie 0.062 0.097 0.256 0.117Race * 0.278 0.082 0.446 0.126
ICD-9 295 687 1086 0.90 Constant 0.424 0.070 0.579
0.281Schizophrenia Access opportunity * 0.163 0.082 0.035 0.374
Whether hospital in
area
0.061 0.083 0.228 0.097
Deprivation * 0.611 0.067 0.474 0.739
Anomie * 0.202 0.073 0.060 0.331
Race 0.080 0.053 0.186 0.022ICD-9 296 755 1209 0.92 Constant
0.251 0.042 0.329 0.158Affective disorders Access opportunity 0.035
0.063 0.076 0.175
Whether hospital in
area
* 0.186 0.087 0.365 0.029
Deprivation * 0.604 0.076 0.464 0.751
Anomie * 0.135 0.052 0.035 0.235
Race * 0.268 0.047 0.359 0.180
S.
Cu
rtiset
al.
/H
ealth
&P
lace
12
(2
00
6)
19
3
733
-
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
193734hospital service use in London (Smith et al., 1996;
Johston et al., 1998) and also agrees with ndings by
Maylath et al. (1999) for Hamburg. We also found that
this does not apply equally to all types of condition
because for affective disorders in London (and also for
females in NYC) the indicators of spatial access do not
show a positive relationship with rates of hospitalization
when socio-economic factors are included in the model.
In this respect our ndings differ from those of Maylath
et al. (1999). This raises a question about whether
proximity to supply is really an important factor for all
types of hospital use, or only for certain mental illnesses
such as schizophrenia and drug dependency.
Another key point from our analysis is that there are
signicant independent associations between the socio-
economic characteristics of the local population and the
rate of hospitalization. These associations are indepen-
dent of variations in the local supply of beds. It seems
possible that poverty and anomie are rather consistently
related to psychiatric hospital use in large cities around
the world. However the signicance of relationships with
socio-economic variables differs according to the cause
of admission. This might be partly because some
diagnoses tend to give rise to more admissions than
others, which might affect the statistical signicance of
results based on larger or smaller counts. However, our
results may reect real differences in the geography of
admissions for different conditions. Such differences
might be due to admissions policy, bed availability and
treatment of different conditions, or variations in the
aetiology of different types of mental illness (or at least
the social conditions which precipitate admission). The
results suggest that poverty is more predictive for drug
dependency while anomie (social fragmentation) is more
strongly associated with affective disorders. These
ndings are broadly similar in both cities and are fairly
consistent with research from other cities, reviewed in
the introduction.
Ethnic/racial composition of the population also has
an independent association for schizophrenia admis-
sions in New York City, but not in London. Our results
for New York City are consistent with other research
that has highlighted high rates of diagnosed schizo-
phrenia and associated hospital use among Black and
African populations. Also, we have shown that the
variables representing the racial composition of the local
population are particularly important for admissions
due to schizophrenia in New York, but less so for other
conditions. However, our results for the race variable in
London, showing that Schizophrenia SARs are not
signicantly higher in areas with large Black and African
populations, seem contrary to some other studies which
have indicated high rates of hospitalization for African
Caribbean populations in Britain. We also found that
SARs for drug-related and affective disorders are
negatively associated with populations with largeminority
groups. It is possible that the ecological data
in London do not pick out Black Carribean and African
populations very effectively. For example, census data
for London do not show such extreme concentrations of
Black and African populations as are found in NYC.
In the data we have used for London wards, the
proportion of Black and African residents does not
exceed 62%, however 15% of NYC ZCAs have
concentrations in excess of this gure, and in some
ZCAs, concentrations occur of over 80% or even 90%,
so it may be easier to detect the experience of Black and
African populations using ecological data in New York.
Our results for London may also be due to intercorrela-
tions between poverty and race at the ecological level,
so that higher rates of admission among individuals of
Black Caribbean or African origin is not detectable
once poverty, proximity to hospitals and spatial
auto-correlation effects are taken fully into account.
Most of the previous ecological studies in London
showing high rates of admission in areas with
greater concentration of minority ethnic groups were
based on older data and so it is also possible that there
has been some change in the pattern of admissions
over time. Our results suggest that areas with
large populations from Black, African and Asian
minority ethnic groups are now more distinguished
from the White majority population by their relatively
low use of hospital care for affective disorders and drug
dependency (especially among women). Our results
suggest that relationships between ethnic composition
of the population and use of psychiatric hospitals may
be continguent on other factors and variable between
cities.
The ecological relationships shown here show broadly
similar associations for admissions for males and
females. However, there are some differences in the
strength of the associations with some variables.
Because we have examined cause specic admissions, it
seems unlikely that these differences are simply due to
variations in the types of mental illness for which men or
women are hospitalized. For example, deprivation
appears to be more strongly associated with male
admissions generally and in New York this is most
evident for drug-related diagnoses, while in London the
difference is more apparent for schizophrenia and for
affective disorders.
The application of these results for service planning
would probably be interpreted somewhat differently in
London and in NYC. In Britain, ecological models of
the type we have discussed here are used to predict the
demand for psychiatric inpatient care and to direct NHS
resources for mental health services. Differences in
relative levels of poverty seem to have the biggest
impact on admission rates and we have shown that, for
London, it is possible to predict local rates of admission
using the IMD measures of poverty and deprivation that
-
the introduction.
UK.
issue. Science NS 255, 946952.
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
1937 35References
Almog, M., Curtis, S., Copeland, A., Congdon, P., 2004.
Geographical variation in acute psychiatric admissions
within New York City 19902000: growing inequalities in
service use? Social Science and Medicine, in press.
Becker, T., Knapp, M., Knudsen, H., Schene, A., Tansella,
M.,
Thornicroft, G., Vazquez-Barquero, J., 1999. The EPSI-
LON study of schizophrenia in ve European countries
design and methodology for standardising outcome mea-
sures and comparing patterns of care and service costs.
British Journal of Psychiatry 175, 514521.
Besag, J., York, J., Mollie, A., 1991. Bayesian image
restora-
tion, with two applications in spatial statistics (with
discussion). Annals of the Institute of Statistical Mathe-
matics 43, 159.
Bhui, K., Bhugra, D., 2001. Transcultural psychiatry: some
social and epidemiological research issues. International
Journal of Social Psychiatry 47 (3), 19.
Boardman, A., Hodgson, R., Lewis, M., Allen, K., 1997.
Social
indicators and the prediction of psychiatric admission in
different diagnostic groups. British Journal of Psychiatry
171, 457462.Acknowledgement
We would like to thank, Prof Giles Glover, University
of Durham, UK, and Dr. Fancis Boscoe, New York
State Department of Health, for providing data on the
location of pscyhiatric inpatient facilities in London and
New York City; Lori Kohn for secretarial assistance.
This research was funded by the Nufeld Foundation,are based on
data available between census years. Our
results suggest, however, that different congurations of
ecological measures are associated with service use for
different types of condition, so that a model for
psychiatric admissions generally might not be applicable
to predicting resource requirements for hospital care of
more specic mental illnesses. Additional information
on social fragmentation and ethnic composition, which
is not included in the IMD, is also signicant for
variation in psychiatric hospitalization rates in London.
In New York City, census-based indicators of poverty
also have relevance for varying patterns of use of
psychiatric hospitals. The fact that hospital use is
geographically variable and associated with differences
in the socio-economic and racial composition of the
population supports other commentaries on the need to
consider why the mental health system in the US
appears to treat different groups of patients so
differently. The information may also be relevant for
production of local service plans proposed in the
Commission for Mental Health (2003), as discussed inBurr, J.,
2002. Cultural stereotypes of women from South Asian
communities: mental health care professionals explanations
for patterns of suicide and depression. Social Science and
Medicine 55 (5), 835845.
Callan, A., 1996. Schizophrenia in Afro-Caribbean
immigrants.
Journal of the Royal Society of Medicine 89 (5),
253256.
Cameron, A., Trivedi, P., 1990. Regression-based tests for
over
dispersion in the poisson model. Journal of Econometrics 46
(3), 347364.
Carr-Hill, R., Hardman, G., Martin, S., Peacock, S.,
Sheldon,
T., Smith, P., 1994. A Formula for Distributing NHS
Revenues Based on Small Area use of Hospital
Beds. University of York, Centre for Heath Economics,
York.
Cliff, A., Ord, J., 1981. Spatial Processes: Models and
Applications. Pion, London.
Commission on Mental Health, 2003. Presidents New Freedom
Commission on Mental Health. New Freedom Commission
on Mental Health, Park Lawn Building, 5600 Fischers
Lane, suite 13c-26. Rockeville, Maryland US.
Congdon, P., 1996a. The epidemiology of suicide in London.
Journal of Royal Statistical Society, Series A 159, 515533.
Congdon, P., 1996b. General linear gravity models for the
impact of casualty unit closures. Urban Studies 33,
17071728.
Congdon, P., 1997. Bayesian models for the spatial structure
of
rare health outcomes: a study of suicide using the BUGS
program. Journal of Health and Place 3 (4), 229247.
Congdon, P., 2001. Bayesian models for suicide monitoring.
European Journal of Population 16, 251284.
Congdon, P., Smith, A., Dean, C., 1998. Assessing
psychiatric
morbidity from a community register: methods for Bayesian
adjustment. Urban Studies 35 (12), 23232352.
Curtis, S., Jones, I.R., 1998. Is there a place for
Geography
geography in the analysis of health inequality? Sociology of
Health and Illness 20 (5 Special Issue), 645672.
Dean, K., James, H., 1981. Social factors and admission to
psychiatric hospital: schizophrenia in Plymouth. Transac-
tions of Institute of British Geographers NS 6, 3952.
Dear, M., Wolch, J., 1987. Landscapes of Despair: From
Institutionalization to Homelessness. Polity Press, Oxford.
Dekker, J., Peen, J., Goris, A., Heijnen, H., Kwakman, H.,
1997. Social deprivation and psychiatric admission rates in
Amsterdam. Social Psychiatry and Psychiatric Epidemiol-
ogy 32 (8), 485492.
DETR, 2000. Indices of Deprivation 2000. Regeneration
Research Summary, 31. Department of Environment
Transport and the Regions, London.
DH, 2003. Resource Allocation; Weighted Capitation. London,
Department of Health.
Diez-Roux, A., 1998. Bringing context back into
epidemiology:
variables and fallacies in multilevel analysis. American
Journal of Public Health 88 (2), 216222.
Dixon, L., Lyles, A., Smith, C., 2001. Use and costs of
ambulatory care services among Medicare enrollees with
schizophrenia. Psychiatric Services 52 (6), 786792.
Dohwenrend, B., Levav, I., Shrout, P., Schwartz, S., Naveh,
G.,
Link, B., Skodol, A., Stueve, A., 1992. Socioeconomic
status and psychiatric disorders: the causation-selection
-
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
193736Driessen, G., Gunther, N., Van Os, J., 1998. Shared
social
environmentand psychiatric disorder: a multilevel analysis
of individual and ecological effects. Social Psychiatry and
Psychiatric Epidemiology 33 (12), 606612.
Duncan, C., Jones, K., Moon, G., 1996. Health-related
behaviour in context: a multilevel modelling approach.
Social Science and Medicine 42 (6), 817830.
Durkheim, E., 1963 (Original in 1897). Suicide: A
Sociological
Study. Routledge and Kegan Paul, London.
Frank, R., Morlock, L., 1997. In: Richard, C.S. (Ed.),
Managing Fragmented Public Mental Health Services.
With an Introduction. Milbank Memorial Fund,
New York City.
Giggs, J., 1986. Schizophrenia and affective psychosis In
Nottingham. Social Sciene and Medicine 23, 945961.
Giggs, J., 1988. The spatial ecology of mental illness. In:
Smith,
C.J., Giggs, J. (Eds.), Location And Stigma: Contemporary
Perspectives On Mental Health And Mental Health Care.
Unwin Hyman, London, pp. 103133.
Glover, G., Robin, E., Emami, J., et al., 1998. A needs index
for
mental health care. Social Psychology and Psych Epide-
miology 33 (2), 8996.
Goldberg, D., Thornicroft, G., 1998. Mental Health in our
Future Cities. Psychology Press, London.
Grob, G., 1994. Government and mental health policya
structural analysis. Milbank Quarterly 72 (3), 471500.
Harrison, G., Glazebrook, C., Brewin, J., Cantwell, R.,
Dalkin,
T., Fox, R., Jones, P., Medley, I., 1997. Increased
incidence
of psychotic disorders in migrants from the Caribbean to
the United Kingdom. Psychological Medicine 27 (4),
799806.
Harrison, J., Barrow, S., Creed, F., 1995. Social
deprivation
and psychotic admission rates among different diagnostic
groups. British Journal of Psychiatry 167, 456462.
Harvey, C., Pantelis, C., Taylor, J., et al., 1996. The
Camden
Schizophrenia Study Surveys 2: High prevalence of schizo-
phrenia in an inner London borough and its relationship to
socio-demographic factors. British Journal of Psychiatry
169 (4), 418426.
Johnson, S., Ramsay, R., Thornicroft, G., 1998. Londoners
mental health needs: the sociodemographic context. In:
Johnson, S., Ramsay, R., Thornicroft, G., Brooks, L.,
Lelliott, P., Peck, E., Smith, H., Chisholm, D., Audini, B.,
Knapp, M., Goldberg, D. (Eds.), Londons Mental
Health. Kings Fund Publishing, London, pp. 1532
(Chapter 3).
Jones, B.E., Gray, M.A., 1986. Problems in diagnosing
schizophrenia and affective disorders among blacks. Hospi-
tal and Community Psychiatry 37, 6165.
Jones, K., Moon, G., 1993. Medical geography: taking space
seriously. Progress in Human Geography 17 (4), 515524.
Kearns, R., Joseph, A., 1993. Space in its place: developing
the
link in medical geography. Social Science and Medicine 37
(6), 711717.
Koppel, S., McGufn, P., 1999. Socio-economic factors that
predict psychiatric admissions at a local level.
Psychological
Medicine 29, 12351241.
Lamont, A., Ukoumunne, O., Tyrer, P., Thornicroft, G.,
Slaughter, J., 2000. The geographical mobility of severely
mentally ill residents in London. Social Psychiatry
andPsychiatric Epidemiology 35 (4), 164169.Lu, F., Du, N., Gaw, A.,
Lin, K., 2002. A psychiatric residency
curriculum about Asian-American issues. Academic Psy-
chiatry 26 (4), 225236.
Macintyre, S., Maciver, S., Soomans, A., 1993. Area, class
and
health: should we be focusing in places or people. Journal
of
Social Policy 22 (2), 213234.
Maylath, E., Seidel, J., Werner, B., et al., 1999.
Geographical
analysis of the risk of psychiatric hopsitalization in
Hamburg from 19881994. European Psychiatry 14 (8),
414425.
Maylath, E., Seidel, J., Schlattmann, P., 2000. Inequity in
the
hospital care of patients with alcoholism and medication
addiction. European Addition Research 6 (2), 7983.
McAlpine, D.D., Mechanic, D., 2000. Utilization of specialty
mental health care among persons with severe mental
illness: the roles of demographics, need, insurance, and
risk. Health Services Research 35 (1), 277292.
NHSCCC (National Health Service Clinical Coding Centre),
2000. Clinical Coding Guidance for Users of HES Data
(version 2). NHSCCC, London.
Schweitzer, L., Kierszenbaum, H., 1978. Community charac-
teristics that affect hospitalization and rehospitalization
rates in a municipal psychiatric hospital. Community
Mental Health Journal 14 (1), 6373.
Smith, C., Hanham, R., 1981. Proximity and the formation of
public attitudes towards mental illness. Environment and
Planning A 13, 147165.
Smith, P., Sheldon, T., Martin, S., 1996. An index of need
for
psychiatric services based on in-patient utilisation.
British
Journal of Psychiatry 169 (3), 308316.
Snowden, L., 1999. African American service use for mental
health problems. Journal of Community Psychology 27 (3),
303313.
Spiegelhalter, D., Thomas, A., Best, N., 2000. Winbugs
Manual: Version 1.3; http://www.mrc-bsu.cam.ac.uk/bugs.
Spiegelhalter, D., Best, N., Carlin, B., van der Linde, A.,
2002.
Bayesian measures of model complexity and t. Journal of
the Royal Statistical Society. Series B 64 (3), 583639.
Sun, D., Tsutakawa, R., Speckman, P., 1999. Posterior
distribution of hierarchical models using CAR(1) distribu-
tions. Biometrika 86, 341350.
Takahashi, L., Gaber, S., 1998. Controversial facility siting
in
the urban environmentresident and planner perceptions
in the United States. Environment and Behaviour 30 (2),
184215.
Tansella, M., Bisof, G., Thornicroft, G., 1993. Are social
deprivation and psychiatric service utilisation associated
in
neurotic disorders? Social Psychiatry and Psychiatric
Epidemiology 28, 225230.
Thornicroft, G., 1991. Social deprivation and rates of
treated
mental disorder: developing statistical models to predict
service utilisation. British Journal of Psychiatry 158,
475484.
Thornicroft, G., Bisof, G., De Salvia, D., Tansella, M.,
1993.
Urbanrural differences in the associations between social
deprivation and psychiatric services utiliation in schizo-
phrenia and all diagnoses; a case register study in Northern
Italy. Psychological Medicine 23, 487496.
Van Os, J., Castle, D., Takei, N., Der, G., Murray, R.,
1996.
Psychotic illness in ethnic minorities; clarication from the1991
census. Psychological Medicine 26 (1), 203208.
-
Wang, P.S., Demler, O., et al., 2002. Adequacy of treatment
for
serious mental illness in the United States. American
Journal of Public Health 92 (1), 9298.
Whitley, E., Gunnell, D., Dorling, D., Davey Smith, G.,
1999.
Ecological study of social fragmentation, poverty, and
suicide. British Medical Journal 319 (7216), 10341037.
WHO, 1978. Manual of the International Statistical Classica-
tion of Diseases, Injuries and Causes of Death, 9th Edition
revised. World Health Organization, Geneva.
WHO, 1992. The International Statistical Classication of
Diseases and Related Health Problems, tenth revision.
World Health Organization, Geneva.
ARTICLE IN PRESSS. Curtis et al. / Health & Place 12 (2006)
1937 37
The ecological relationship between deprivation, social
isolation and rates of hospital admission for acute psychiatric
care: a comparison of London and New York CityIntroduction:
background to the analysisMethod to compare geographical
differences in hospitalization rates in New York City and
LondonResults: local variation in hospitalization for psychiatric
conditions in NYC and LondonDiscussionAcknowledgementReferences





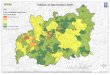







![Taylor Swift August ‘09 [justice, Chinada prison certainty] · Selena Gomez June 16, ‘10 [Chinada prison certainty] Eva Mendes June 17, ‘10 [China, isolation-deprivation (romance)]](https://img.pdfslide.us/doc/110x75/5e52817195a65a63ad383548/taylor-swift-august-a09-justice-chinada-prison-certainty-selena-gomez-june.jpg)














