Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
Journal of the Chinese Medical Association 75 (2012) 384e388www.jcma-online.com
Original Article
The diameter of the common bile duct in an asymptomatic Taiwanesepopulation: Measurement by magnetic resonance cholangiopancreatography
Tom Chen a, Ching-Ruei Hung b, Ay-Chiao Huang a, Jiunn-Ming Lii a, Ran-Chou Chen b,*
aDepartment of Radiology, Taipei City Hospital, Taipei, Taiwan, ROCbDepartment of Biomedical Imaging and Radiological Sciences, National Yang-Ming University, Taipei, Taiwan, ROC
Received September 26, 2011; accepted February 26, 2012
Abstract
Background: Magnetic resonance cholangiopancreatography (MRCP) is a popular modality for evaluation of the biliary tract, yet there is no dataon the normal common bile duct (CBD) size of the average Taiwanese adult. This study attempts to establish a reference range for CBD diameterfor the Taiwanese population.Methods: Over a 2-year period, all adults who underwent abdominal magnetic resonance imaging for health screening were recruited into thestudy. Patients with a prior history of hepatobiliary surgery and other significant morbidity were not included. Patients who were found to haveabnormal liver function test results or abnormal imaging findings were also excluded from the study. After the patients fasted for a minimum of 8hours, MR imaging was performed with a 1.5 T MR imager using a phased-array coil. Breath-hold thick slab single-shot turbo spin echo (ssTSEBH) projections were obtained, and these were used for CBD and portal vein diameter (PVD) measurement by workstation software. Initialrecruitment included 265 patients, of which 66 were excluded due to abnormal liver function tests, seven more were excluded due to excessimaging artifacts or incomplete CBD visualization, and five were excluded due to other abnormal blood tests. This yielded a final study group of187 patients between the ages of 21 and 78 years, which comprised 69 women and 118 men.Results: The mean CBD diameter is 4.6 mm, with a range from 1.76 to 10.49 mm. CBD diameters are significantly different in patients bothyounger and older than 65 years of age ( p < 0.05), and are not significantly related to gender, serum glucose level, cholesterol level, hepatitisstatus and PVD.Conclusion: Our study showed that the average CBD diameter for an asymptomatic Taiwanese adult is 4.6 mm, with an upper limit of 10.49 mm.CBD diameter is only significantly correlated with age. This is a useful reference in today’s clinical setting where MRCP are commonlyperformed for evaluation of suspected biliary tract disease.Copyright � 2012 Elsevier Taiwan LLC and the Chinese Medical Association. All rights reserved.
Keywords: adult; biliary tract; common bile duct; MRI; Taiwan
1. Introduction
Over the years, modern medical imaging technology hashelped medical practitioners become proficient in the assess-ment of biliary pathology, thereby better enabling moreprecise measurement of the biliary tract. Because a dilated
* Corresponding author. Dr. Ran-Chou Chen, Department of Radiology,
Taipei City Hospital Heping Branch, 33, Section 2, Chun Hua Road, Taipei
100, Taiwan, ROC.
E-mail address: [email protected] (R.-C. Chen).
1726-4901/$ - see front matter Copyright � 2012 Elsevier Taiwan LLC and the C
http://dx.doi.org/10.1016/j.jcma.2012.06.002
common bile duct suggests obstructive causes which mayrequire invasive imaging or remedial procedures, an accurateCBD size reference range should be available. A plethora ofpublished literature exists regarding the normal size of thecommon bile duct (CBD),1e7 and these range from thecadaveric measurements, operative cholangiograms, andendoscopic retrograde cholangio-pancreatography (ERCP) tosonography, and, more recently, multi-detector-row computedtomography (MDCT).
Since its introduction in 1991, MR imaging of the biliarytract has underwent a progressive evolution.8 Today, magnetic
hinese Medical Association. All rights reserved.

385T. Chen et al. / Journal of the Chinese Medical Association 75 (2012) 384e388
resonance cholangiopancreatography (MRCP) is one of thediagnostic mainstays for assessment of biliary tract abnor-malitydespecially those involving obstruction. Manyconsider MR imaging to be the non-invasive “gold standard”imaging for evaluation of biliary pathology,9,10 and it iscommonly performed first to determine the necessity ofsubsequent invasive procedures such as ERCP.
Despite the prevalence of MRCP as a first-line modality ofbiliary pathology,9 a search of the literature available revealedno formal study that specifically documented normal CBDdiameter as measured by MRCP. Consequently, the lack ofa reference range may lead to over- or underdiagnosis ofbiliary dilatation.
The purpose of this study was to evaluate the diameters ofCBD in asymptomatic Taiwanese patients using MRCP, anddetermine the normal size range for this population. In addi-tion, we also attempted to evaluate the relationship betweenCBD diameter and other variables, in order to see if there isa significant relationship between them.
2. Methods
2.1. Patients
During the period of January 2005 to December 2006, werecruited for our study all asymptomatic individuals whounderwent abdominal MRI for health screening and who hadnot undergone prior hepatobiliary surgery. The institutionalreview board approved this retrospective study and theinformed consent requirement was waived.
We recorded the patients’ age, sex, medical history, list ofmedications including substances of abuse, fasting blood sugarlevel, total serum cholesterol, liver function tests, and hepatitisstatus. Any positive history of myocardial infarction, cerebro-vascular accident, biliary disease, pancreatic disease, hepaticdisease, or substance abuse precluded the individual fromjoining the study group. Individualswith abnormal liver functiontests (total bilirubin, AST, ALT) or abnormal MRI findings suchas biliary stones or chronic cholecystitis were also subsequentlyexcluded from the study, thus preventing any individuals withknown potential biliary pathology from joining the study.
The initial recruitment group included 265 participants.Seven were excluded due to excess image artifacts orincomplete CBD visualization, five due to incomplete bloodtest results, and 66 due to abnormal liver function tests. Nonewere excluded due to actual biliary abnormality found byMRI. The final study population consisted of 187 patientsbetween 21 and 78 years of age (mean age of 51 years) andincluded 69 (37%) women and 118 (63%) men.
2.2. Imaging
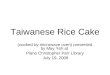
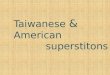
Fig. 1. Measurement of CBD diameter by placing electronic caliper at the
widest visible portion of CBD.
MR imaging was performed on patients after an overnightfast, which translated to at least 8 hours prior to the MRexamination. Abdominal MR imaging was performed with 1.5T MR imagers (GyroScan, Philips Medical Systems, theNetherlands) using phased-array coils. Axial and coronal turbo
spin-echo (TSE) T2-weighted images were acquired using thefollowing parameters without and with fat saturation: TR,2500 ms; TE, 100 ms; TSE factor, 23; matrix, 256 � 256. Dualphase T1-weighted images were obtained within one breathhold using: TR, 210 ms; TE ¼ 2.3 and 4.6 ms; slices thickness,8 mm; gap, 0.8 mm; flip. Breath-hold thick slab single-shotturbo spin echo (ssTSE BH) projections were also acquired,and these were used for the actual CBD measurement. Theparameters of the ssTSE BH sequence were as follows: TR,8000 ms; effective TE, 850 ms; turbo factor, 128; flip angle,90�; slice thickness, 30e40 mm; field of view, 250 mm;matrix, 256 � 205; acquisition time, 8 seconds. The entirepancreaticobiliary tree was included in all images. The samepulse sequence was repeated to acquire four to six projectionsof the pancreaticobiliary system from different angles.
Measurements of the CBD diameters were performedindependently by an experienced radiological technologist(with 11 years of experience with MR techniques, A.C.H.) andan experienced radiologist (7 years of experience, T.C.).Coronal ssTSE BH images at 4-6 different angular planes werereviewed, and the one with well-demonstrated CBD and mainpancreatic duct with the least superimposed artifacts was usedfor measurement. A magnification factor of 2.0 was used toensure precise delineation of the biliary duct margins. Thewidest diameter of CBD was measured perpendicular to theirlong axis using the electronic caliper provided by the picturearchiving and communications system (Centricity PACS, RA600 v6.1, GE Medical Systems, Milwaukee, Wisconsin, USA)(Fig. 1). Portions of CBD with superimposed artifacts from thestomach, small intestines, and cystic ducts were avoided. Theanteroposterior diameters of portal vein anterior to inferiorvena cava were measured using the same method with PACSelectronic caliper, in T2-weighted images.
2.3. Statistical analysis
Statistical analysis was performed using SPSS (SPSS forWindows, version 15.0, SPSS Inc, Chicago, IL, USA). The

386 T. Chen et al. / Journal of the Chinese Medical Association 75 (2012) 384e388
recorded maximal CBD diameters were then analyzed againstage, gender, blood sugar, and cholesterol using Student t-test.The CBD diameters were also analyzed against the presenceof hepatitis B and C antigens using ANOVA. CBD diameterswere analyzed against portal vein diameters using the Pearsoncorrelation.
Interobserver agreement was assessed with Pearson’scorrelation coefficient and paired t-test. Multiple linearregressions were used to confirm the relationships betweenCBD diameters and these variables. A p value < 0.05 wasconsidered statistically significant.
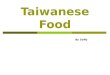
Fig. 2. CBD diameter versus patient age.
3. Results
The mean CBD diameter of 187 patients obtained byReader 1 was 4.6 mm (�1.8 mm), with a range of1.76e10.49 mm. The mean CBD diameter observed byReader 2 is 5.0 mm (�1.7 mm), with a range of2.42e11.65 mm. The mean portal vein diameters obtained byReader 1 and 2 are 8.13 mm (�1.8 mm) and 8.14 mm(�1.8 mm), respectively (Table 1). There was excellentinterobserver agreement between Reader 1 and Reader 2’smeasurements of CBD and portal vein diameter (Pearsoncorrelation coefficients ¼ 0.89 and 0.90, p < 0.0001).
The mean CBD diameter for females was slightly largerthan that of males (4.8 � 1.7 mm vs. 4.5 � 1.8 mm), althoughthis lacks statistical significance ( p < 0.05). CBD diameter isdirectly proportion to age ( p < 0.05), when patients aredivided into two groups using 65 years as the cut-off age.When patient age is subdivided into decades, further analysisreveals that there is a somewhat linear relationship betweenCBD size and age in decades (R2 ¼ 0.62, Fig. 2). Howeverother variables such as fasting blood sugar levels, serumcholesterol, presence of hepatitis B or C, and portal veindiameters show no statistically significant effect on the CBDdiameter. The results are summarized in Table 1.
Table 1
CBD diameters and its relations with different parameters.
Number
Patient CBD diameter Reader 1 187
Reader 2
Gender* Female 69
Male 118
Age* (y) <65 176
S65 11
Serum glucose* (mg/dL) &110 167
>110 20
Total
cholesterol* (mg/dL)
&200 100
>200 87
Hepatitis status** Negative 157
HBVþ 25
HCVþ 5
Portal vein diameter*** Continuous
variable
187
*Student t-test.
**ANOVA.
***Pearson Correlation Coefficient.
CBD ¼ common bile duct.
4. Discussion
Most recently, MRCP is the principle diagnostic modalitythat determines if ERCP is neededdespecially when ultra-sound findings are equivocal.9 The decision to perform ERCPdepends on whether an organic abnormality or an abnormaldilation could be demonstrated. To prove the presence ofabnormal dilatation there needs to be a reference range, withdiameters exceeding its upper limit deemed abnormal.
Our results show that the average CBD diameter asmeasured by MRCP is 4.6 mm � 1.8 mm, with a range of1.97e10.49 mm. Compared to the results of available researchpapers using other imaging modalities, it is well within thereported range. Jonson et al11 showed that the average diam-eter in patients with normal cholangiography was 5.9 mm. Byusing ultrasound measurement, Kaim et al12 found that
Mean (mm) Standard deviation p
4.6 �1.8
5.0 �1.7
4.8 �1.7 0.226
4.5 �1.8
4.4 �1.7 0.008
6.0 �2.6
4.6 �1.8 0.855
4.5 �1.5
4.5 �1.6 0.512
4.7 �2
4.5 �1.8 0.909
4.5 �2
4.8 �1.8
8.13 �1.8 0.785

387T. Chen et al. / Journal of the Chinese Medical Association 75 (2012) 384e388
asymptomatic patients without prior biliary surgery hada mean CBD diameter of 6.2 mm. Horrow et al13 also analyzed258 asymptomatic patients’ routine ultrasounds, and foundmean CBD diameters are 3.9 mm. The sonographic analysis ofthe Iranian population presented by Adibi’ et al14 revealed anaverage CBD diameter of 3.72 mm. Park et al15 measured 398Koreans’ CBD diameter using multi-detector row CT, andfound the average diameter to be 6.7 mm. Our finding that theaverage Taiwanese patients’ CBD of 4.6 mm as measured byMRI is well within the range of currently reported range-values of normal CBD diameter, and appears to be unrelatedto the race of the patients. It is also unique in that this is theonly study that used MRCP to measure the CBD range ofhealthy individuals.
The reason that average CBD diameter reported in avail-able medical literature varies is complex, and, most likely,multi-factorial. One possible source of this discrepancy is thefact that the CBD cross-section is oval in shape when dis-tended,16 which can affect its measurement when usingdifferent modalities. For example, ultrasound measurement ofCBD measures anterioreposteriorly (AP), whereas othercross-sectional imaging such as CT or MR enable measure-ment of the largest diameter. Another source of variation is thedepth of inspiration, which Wachsberg found can result inchanges of CBD diameter.17
Other factors that may have affected CBD diameters havebeen investigated. However, few factors except for age haveproven to consistently affect CBD measurements. Kialianet al.18 observed that the longitudinal smooth muscle bandsand its intervening connective tissues fragments withincreasing age are accompanied by loss of reticulo-endothelialnetwork of the ductal wall, and suggest this may be themechanism behind the age-related biliary dilatation. Mostauthors support the proposition that age is significantly relatedto CBD diameter,19e21 although the nature of the relationshipis still debated. Some believe that there is a linear relationshipbetween CBD diameter and gradual advancement in age,19,20
while others consider the relationship indirect,15 or that itonly dilates after the age of 65.22 Our findings also suggestthat there is a significant difference ( p ¼ 0.008) between CBDdiameters of patients younger and older than 65 years of age,with patients older than 65 years having significantly largerCBD diameter. When patients’ age is further divided intodecades, a trend becomes apparent: as patients’ age increasesfrom the third to the eighth decade of life, the average CBDdiameters also increase in an approximately linear fashion.This trend can be summarized by the equation CBDsize ¼ 0.65 � age (in decades) þ 1.52, with R2 ¼ 0.62. Thiscorresponds closely to what Wu et al.19 proposed: that CBDdiameter increase by 1 mm per decade.
Previous studies suggest that gender has no significanteffect on CBD diameter,6 and our studies also support thisobservation ( p ¼ 0.23). Elevated blood sugar and cholesterollevels are known to be risk factors for saturated bile andgallstone formation,23 and although viral hepatitis in general isnot directly related to biliary dilatation, in rare circumstancesit can result in cholestasis and biliary dilatation.24 Hepatitis B
and C are also endemic in Taiwan with a high prevalence rate.However, our results suggest that none of these are signifi-cantly related to CBD diameter ( p ¼ 0.86, 0.51 and 0.91,respectively). Adibi et al.14 assert that there is a statisticallysignificant relationship between portal vein and CBD diam-eter, although our results suggest the opposite. This couldeither be due to the intrinsic differences between MR andsonography measurements or variances in the studypopulations.
There are some limitations to this retrospective study. First,medications such as morphine, calcium antagonists, andnitroglycerine can cause CBD dilatation.25 Although ourscreening questionnaires did specifically ask for list of medi-cations from the study participants, including substances ofabuse such as alcohol and other drugs, patients may haveintentionally omitted drugs of abuse such as heroin. While thisstudy cohort does contain a wide range of patient age, there isan insufficient number of patients at either end of the spec-trum, which may lead to some statistical bias.
In conclusion, our study shows that the average CBDdiameter of the Taiwanese population measured by MRCP is4.6 mm, with an upper limit of 10.5 mm. CBD diameter issignificantly larger in patients older than 65 years of age, andincreases proportionally by age for each subsequent decade oflife. Otherwise no significant association was found withgender, blood sugar level, cholesterol level, viral hepatitis, andportal vein diameter. This can serve as a useful reference toolwhen medical professionals are faced with clinical decisionsinvolving biliary obstruction and the need for further investi-gation or intervention.
References
1. Co CS, Shea Jr WJ, Goldberg HI. Evaluation of common bile duct
diameter using high resolution computed tomography. J Comput Assist
Tomogr 1986;10:424e7.
2. Niederau C, Muller J, Sonnenberg A, Scholten T, Erckenbrecht J,
Fritsch WP, et al. Extrahepatic bile ducts in healthy subjects, in patients
with cholelithiasis, and in postcholecystectomy patients: a prospective
ultrasonic study. J Clin Ultrasound 1983;11:23e7.
3. Burrell MI, Zeman RK, Simeone JF, Dachman AH, McGahan JP,
VanSonnenberg E, et al. The biliary tract: imaging for the 1990s. AJR Am
J Roentgenol 1991;157:223e33.
4. Cohen SM, Kurtz AB. Biliary sonography. Radiol Clin North Am
1991;29:1171e98.5. Parulekar SG. Ultrasound evaluation of common bile duct size. Radiology
1979;133:703e7.
6. Mahour GH, Wakim KG, Ferris DO. The common bile duct in man: its
diameter and circumference. Ann Surg 1967;165:415e9.7. Karvonen J, Kairisto V, Gronroos JM. The diameter of common bile duct
does not predict the cause of extrahepatic cholestasis. Surg Laparosc
Endosc Percutan Tech 2009;19:25e8.
8. Sodickson A, Mortele KJ, Barish MA, Zou KH, Thibodeau S,
Tempany CM. Three-dimensional fast-recovery fast spin-echo MRCP:
comparison with two-dimensional single-shot fast spin-echo techniques.
Radiology 2006;238:549e59.
9. Shanmugam V, Beattie GC, Yule SR, Reid W, Loudon MA. Is magnetic
resonance cholangiopancreatography the new gold standard in biliary
imaging? Br J Radiol 2005;78:888e93.
10. Park MS, Kim TK, Kim KW, Park SW, Lee JK, Kim JS, et al.
Differentiation of extrahepatic bile duct cholangiocarcinoma from

388 T. Chen et al. / Journal of the Chinese Medical Association 75 (2012) 384e388
benign stricture: findings at MRCP versus ERCP. Radiology
2004;233:234e40.
11. Jonson M. Width of the common bile duct before and after morphine
studied by cholegraphy. Acta radiol 1960;53:345e52.
12. Kaim A, Steinke K, Frank M, Enriquez R, Kirsch E, Bongartz G, et al.
Diameter of the common bile duct in the elderly patient: measurement by
ultrasound. Eur Radiol 1998;8:1413e5.
13. Horrow MM, Horrow JC, Niakosari A, Kirby CL, Rosenberg HK. Is age
associated with size of adult extrahepatic bile duct: sonographic study.
Radiology 2001;221:411e4.
14. Adibi A, Givechian B. Diameter of common bile duct: what are the
predicting factors? J Res Med Sci 2007;12:121e4.15. Park JS, Lee DH, Jeong S, Cho SG. Determination of diameter and
angulation of the normal common bile duct using multidetector computed
tomography. Gut Liver 2009;3:306e10.
16. Wachsberg RH, Kim KH, Sundaram K. Sonographic versus endoscopic
retrograde cholangiographic measurements of the bile duct revisited:
importance of the transverse diameter. AJR Am J Roentgenol
1998;170:669e74.17. Wachsberg RH. Respiratory variation of extrahepatic bile duct diameter
during ultrasonography. J Ultrasound Med 1994;13:617e21.
18. Kialian GP, Aznaurian AV. The age-related characteristics of the muscular
layer of the common bile duct in man. Morfologiia 1995;108:10e2.
19. Wu CC, Ho YH, Chen CY. Effect of aging on common bile duct diameter:
a real-time ultrasonographic study. J Clin Ultrasound 1984;12:473e8.
20. Bachar GN, Cohen M, Belenky A, Atar E, Gideon S. Effect of aging on
the adult extrahepatic bile duct: a sonographic study. J Ultrasound Med
2003;22:879e82. quiz 83e5.
21. Kim HJ, Kim MH, Lee SK, Seo DW, Kim YT, Lee DK, et al. Normal
structure, variations, and anomalies of the pancreaticobiliary ducts of
Koreans: a nationwide cooperative prospective study. Gastrointest Endosc
2002;55:889e96.
22. Weinstein BJ, Weinstein DP. Biliary tract dilatation in the nonjaundiced
patient. AJR Am J Roentgenol 1980;134:899e906.
23. Stokes CS, Krawczyk M, Lammert F. Gallstones: environment, lifestyle
and genes. Dig Dis 2011;29:191e201.
24. Lim HL, Lau GK, Davis GL, Dolson DJ, Lau JY. Cholestatic hepatitis
leading to hepatic failure in a patient with organ-transmitted hepatitis C
virus infection. Gastroenterology 1994;106:248e51.
25. Economou G, Ward-McQuaid JN. A cross-over comparison of the effect
of morphine, pethidine, pentazocine, and phenazocine on biliary pressure.
Gut 1971;12:218e21.