Embed Size (px)
Citation preview
POSTGRAD. MDI). J., (1966), 42, 74
THE DIAGNOSIS OF ACUTE OSTEOMYELITISOF THE PELVIS
ALAN MORGAN, ALAN K. YATES,M.B., Ch.B. (Brist.), F.R.C.S. Eng.* M.B., Ch.B. (Sheff.), F.R.C.S. Eng.**
The Royal Infirmary and Children's Hospital, Sheffield.OSTEOMYELITIS of the pelvis has a sparse biblio-graphy, probably because of its relativeinfrequency in general orthopaedics.
Froener (1889) istated that less than 10%/ ofcases occured in the pelvis in a series of 545cases of acute osteomyelitis; Butler (1940)gives an incidence of 8% in 500 cases of acuteosteomyelitis seen at the London Hospital.Von Bergmann (1906) found 63 cases of
osteomyelitis of the ilium in 71 cases of osteo-myelitis of the pelvis. Krasnobajiv (1925),Simmons (1915), Bearse (1923), Flickinger(1927) and Buosanti (1924) each give an in-cidence of osteomyelitis of the ilium of bet-ween 2% and 7%. Young (1934), in his reviewof osteomyelitis of the ilium, to which headded three cases of his own, stated that "acuteosteomyelitis of the pubis and ischium is so rareit is hardly necessary to give it consideration".His paper is the last comprehensive review ofpelvic osteomyelitis, but referred only to theilium.
This paper concerns the diagnosis of acuteosteomyelitis of the pelvis lin 18 patients seenin the Orthopaedic Departments of the RoyalInfirmary and Childrens' Hospital in Sheffieldbetween 1948 and 1964. Thirty case recordsof pelvic osteomyelitis were found among 616cases of acute osteomyeliltis of all bones seenduring this period, but only 18 were documentedsufficiently well for study. This gives an in-cidence of 5% of osteomyelitis occurring in thepelvis. Osteitis pubis due to surgery or traumahas not been included. Although this conditionis more common than acute haematogenousosteomyelitis of the pelvis it is a separate en-tity. The principles of treatment of pelvicosteomyelitis do not differ from those of osteo-myeitis in other bones and will not bediscussed.
AnatomyThe incidence of involvement of individual
bones of the pelvic ring in this series of 18cases is as follows: Ilium, 14; Ischium, 4;Pubis, 0; Total, 18. This refers to the initial
Present address:*United Cardiff Hospitals, Llandouigh Hospital,Cardiff.
**Guy's Hospital, London, S.E.I.
bone involved and does not include otherbones of ithe pelvis involved by subsequentspread of the disease.
In agreement with other authors we findthat the ilium is most commonly affected. Theilium forms the largest portion of the bonypelvis. lits blade has an abundant blood supplywith a large nutrient artery entering its innersurface, and in the adult it is the only bone ofthe pelvis containing haemopoetic marrow.The ischium was more commonly involved
than in other series, but i,n no patient was thepubis primarily infected, although it was in-volved by extension in several cases. (Fig. 1).Clinical PresentationAlthough the correct diagnosis was made
ultimately the condition often eluded diagnosisduring weeks or even months of investigation.On studying ,the case reports it became
evident ,that certain features could be groupedinto clinical syndromes which were related ingeneral to the anatomical site of infection.Most patients initially had symptoms and
signs of toxaemia but dlid not come to hospitaluntil localising signs, such as a limp, appearedsome days later. A few patients suffered fromsepticaemia for a long period while the infectivenidus remained hidden.The following is a suggested classification
based on our observations:1. Septicaemic2. Clinical Syndromes
(a) Hip joint Syndrome.(b) Abdominal Syndrome.(c) Buttock Syndrome.(d) Sciatic Syndrome.
SepticaemicThese patients have symptoms and signs of
toxaemia, usually with a positive blood culture,but with no obvious infective nidus. Carefulexamination of the skeleton is essential in allcases of unexplained septicaemia. It is pertinentthat eight of our patients had initial septicaemicsymptoms on admission.The following case history is illustrative.Case no. 1. J.S. aged 31 years. Admitted initiallyunder medical care with a pyrexia of unknown
origin. He had been ill for one week with malaise,pyrexia and rigors. There was no relevant antecedent
by copyright. on 22 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.484.74 on 1 F
ebruary 1966. Dow
nloaded from
MORGAN and YATES: Osteomyelitis of the Pelvis
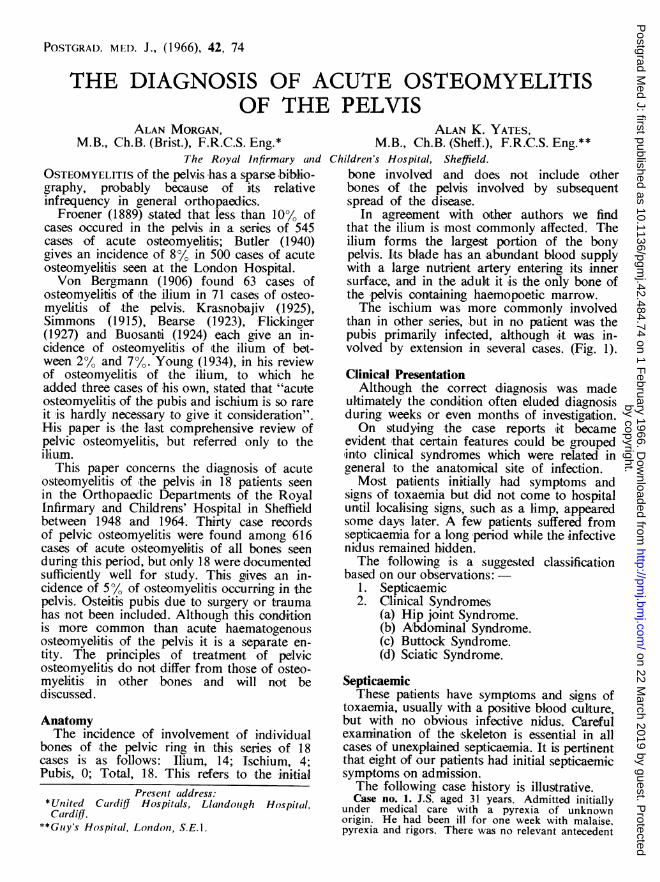
FIG. 1.-Radiograph of case J.S. showing bonedestruction in !the ilium at the anterior inferioriliac spine spreading to the acetabular roof,pubis and ischium.
history and no abnormal physical signs were noted.Initial investigations showed a white cell count of19,500/cu. mm.; 86 % polys. Blood culture grew apure growth of staphylococcus pyogenes.
Antibiotic treatment was commenced and wascontinued for eight weeks with varying combinationsof drugs without success. Blood cultures remainedpositive with increasing resistance of the staphy-lococcus. Extensive investigations were carried outin an unsuccessful attempt to find the source of theinfection. It is interesting to niote that an intravenouspyelogram performed at this time would haverevealed the osteomyelitic focus in the left ischiumif this area had not been obscured by a gonadalradiation screen. Nine weeks after admission thepatient started to complain of pain in the left hipand groin. Radiography showed an osteomyeliticle3ion in the left ischium. A deep buttock abscessdeveloped and he was transferred to orthopaediccare. The abscess was drained and a hip spicaapplied. However,,the infection progressed and Fig. 1shows the extensive bony destruction spreading intothe pubis and acetabular roof. The hip is fusings;pontaneously.
Clinical SyndromesPatients may present certain clinical features
which indicate the diagnosis and the site of theosteomyelitis. Four syndromes can be defined.(a) Hip Joint Syndrome
This syndrome has clinical features like thoseof septic arthritis of the hip but with certainexceptions. The pain is felt in the hip and in
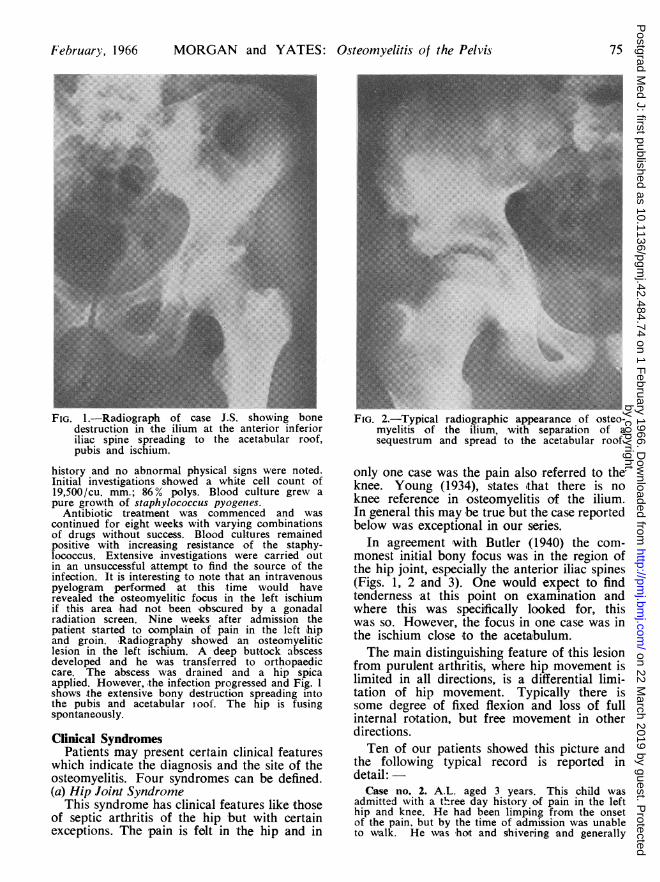
FIG. 2.-Typical radiographic appearance of osteo-myelitis of the ilium, with separation of asequestrum and spread to the acetabular roof.
only one case was the pain also referred to theknee. Young (1934), states ithat there is noknee reference in osteomyelitis of the ilium.In general this may be true but the case reportedbelow was exceptional in our series.
In agreement with Butler (1940) the com-monest initial bony focus was in the region ofthe hip joint, especially the anterior iliac spines(Figs. 1, 2 and 3). One would expect to findtenderness at this point on examination andwhere this was specifically looked for, thiswas so. However, the focus in one case was inthe ischium close to the acetabulum.The main distinguishing feature of this lesion
from purulent arthritis, where hip movement islimited in all directions, is a differential limi-tation of hip movement. Typically there issome degree of fixed flexion and loss of fullinternal rotation, but free movement in otherdirections.Ten of our patients showed this picture and
the following typical record is reported indetail:
Case no. 2. A.L. aged 3 years. This child wasadmitted with a three day history of pain in the lefthip and knee. He had been limping from the onsetof the pain, but by the time of,admission was unableto walk. He was hot and shivering and generally
February, 1966 75by copyright.
on 22 March 2019 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.484.74 on 1 February 1966. D
ownloaded from
POSTGRAiDUATE ME
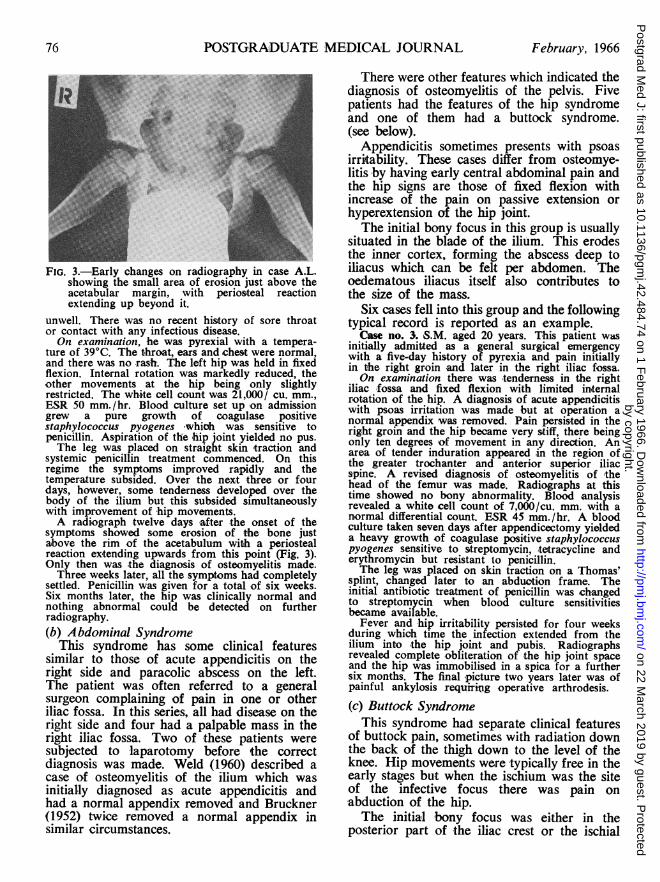
FIG. 3.-Early changes on radiography in case A.L.showing the small area of erosion just above theacetabular margin, with periosteal reactionextending up beyond it.
unwell. There was no recent history of sore throator contact with any infectious disease.On examination, he was pyrexial with a tempera-
ture of 39°C. The throat, ears and chest were normal,and there was no rash. The left hip was held in fixedflexion. Internal rotation was markedly reduced, theother movements at the hip being only slightlyrestricted. The white cell count was 21,000/ cu. mm.,ESR 50 mm./hr. Blood culture set up on admissiongrew a pure growth of coagulase positivestaphylococcus pyogenes which was sensitive topenicillin. Aspiration of the hip joint yielded no pus.The leg was placed on straight skin traction and
systemic penicillin treatment commenced. On thisregime the symptoms improved rapidly and thetemperature subsided. Over the next three or fourdays, however, some tenderness developed over thebody of the ilium but this subsided simultaneouslywith improvement of hip movements.A radiograph twelve days after the onset of the
symptoms showed some erosion of the bone justabove the rim of the acetabulum with a periostealreaction extending upwards from this point (Fig. 3).Only then was the diagnosis of ostoomyelitis made.Three weeks later, all the symptoms had completely
settled. Penicillin was given for a total of six weeks.Six months later, the hip was clinically normal andnothing abnormal could be detected on furtherradiography.(b) Abdominal Syndrome
This syndrome has some clinical featuressimilar to those of acute appendicitis on theright side and paracolic abscess on the left.The patient was often referred to a generalsurgeon complaining of pain in one or otheriliac fossa. In this series, all had disease on theright side and four had a palpable mass in theright iliac fossa. Two of these patients weresubjected to laparotomy before the correctdiagnosis was made. Weld (1960) described acase of osteomyelitis of the ilium which wasinitially diagnosed as acute appendicitis andhad a normal appendix removed and Bruckner(1952) twice removed a normal appendix insimilar circumstances.
DICA,L JOURNAL February, 1966
There were other features which indicated thediagnosis of osteomyelitis of the pelvis. Fivepatients had the features of the hip syndromeand one of them had a buttock syndrome.(see below).
Appendicitis sometimes presents with psoasirritability. These cases differ from osteomye-litis by having early central abdominal pain andthe hip signs are those of fixed flexion withincrease of the pain on passive extension orhyperextension of the hip joint.The initial bony focus in this group is usually
situated in the blade of the ilium. This erodesthe inner cortex, forming the abscess deep toiliacus which can be felt per abdomen. Theoedematous iliacus itself also contributes tothe size of the mass.
Six cases fell into this group and the followingtypical record is reported as an example.
Case no. 3. S.M. aged 20 years. This patient wasinitially admitted as a general surgical emergencywith a five-day history of pyrexia and pain initiallyin the right groin and later in the right iliac fossa.On examination there was tenderness in the right
iliac ifossa and fixed flexion with limited internalrotation of the hip. A diagnosis of acute appendicitiswith psoas irritation was made but at operation anormal appendix was removed. Pain persisted in theright groin and the hip became very stiff, there beingonly ten degrees of movement in any direction. Anarea of tender induration appeared -in the region ofthe greater trochanter and anterior superior iliacspine. A revised diagnosis of osteomyelitis of thehead of the femur was made. Radiographs at thistime showed no bony abnormality. Blood analysisrevealed a white cell count of 7,000/cu. mm. with anormal differential count. ESR 45 mm./hr. A bloodculture taken seven days after appendicectomy yieldeda heavy growth of coagulase positive staphylococcuspyogenes sensitive to streptomycin, tetracycline anderythromycin but resistant to penicillin.The leg was placed on skin traction on a Thomas'
splint, changed later to an abducti,on frame. Theinitial antibiotic treatment of penicillin was changedto streptomycin when blood culture sensitivitiesbecame available.Fever and hip irritability persisted for four weeks
during which time the infection extended from theilium into the hip joint and pubis. Radiographsrevealed complete obliteration of the hip joint spaceand the hip was immobilised in a spica for a furthersix months. The final picture two years later was ofpainful ankylosis requiring operative arthrodesis.
(c) Buttock SyndromeThis syndrome had separate clinical features
of buttock pain, sometimes with radiation downthe back of the thigh down to the level of theknee. Hip movements were typically free in theearly stages but when the ischium was the siteof the infective focus there was pain onabduction of the hip.The initial b-ony focus was either in the
posterior part of the iliac crest or the ischial
76by copyright.
on 22 March 2019 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.484.74 on 1 February 1966. D
ownloaded from
MORGAN and YATES: Osteoniyelitis of the Pelvis
tuberosity and the outer cortex of bone waseroded with an abscess enlarging into theoverlying soft tissues.
Physical examination revealed a localisedarea of tenderness often with a palpable massin the region of the infection. These findingsmade early diagnosis with accurate localisationof the infective focus possible. In our seriesthese cases were correctly diagnosed at the timeof first examination.
Six cases had clinical features of this group,aind the following is a typical record.
Case no. 4. J.H. aged 15 years. The patientcomplained of increasing right buttock pain for sixdays with general malaise. There was no 'history ofrecent trauma.On examination, the patient had a fever of 38.60C.
There was free movement of the hips but somediscomfort was experienced on flexion and abductionof the right hip and exquisite tenderness was presentover the ischial tuberosity. Laboratory investigationsrevealed: !a normal haemoglobin; WBC normal 'butwith a relative polymorphonucleocytosis. ESR 43mm./hr. Blood culture revealed a heavy growth ofcoagulase positive staphylococcus pyogenes sensi,tiveto penicillin.Treatment was by leg traction and intramuscular
penicillin. The patient was afebrile in seven daysand the local symptoms and signs had completelyresolved in eleven days. The patient was dischargedhome on the sixteenth day with no abnormal signs.Radiographs had appeared normal and a provendiagnosis ;had not been established.Four months later a sinus developed in relation to
the ischial tuberosity which now showed signs ofbony infection on radiography. T'he patient persist-antly refused oper-ative treatment and after aprolonged course of anitibiotics the sinus permanentlyhealed with no residual disability one year later.
(d) Sciatic SyndromeOnly one case occurred in this series, but
similar cases have been described in theliterature. The syndrome is characterised bypain along the distribution of the sciatic nerveassociated with the systemic signs of a purulentinfection and localised tenderness over theregion of the sacro-iliac joint. This is indicativeof suppurative artihritis of the sacro-iliac joint.Avila (1941) described seven cases in whomthese features were constant. Riendle Short(1931) described a similar case.
Suppurative arthritis of the sacro-iliac jointis probably secondary to osteomyelitis situatedposteriorly in the blade of the ilium, theinfection spreading later into the joint. Thehistories of some of the reported cases wouldappear to confirm this. Among the accountsin the literature of cases of suppurative sacro-iliitis, a number occurred shortly after childbirthor abortion. This case appears to be the onlyone occurring antenatally.
Case no. 5. J.S. aged 22 years. The patient was36 weeks pregnant. It was her first pregnancy whichhas proceeded normally to date. She was ladmittedcomplaining of backache associated with malaise offour to five days duration. The symptoms hadbecome more severe during the preceding twenty-fourhours and the pain had moved into the buttock withradiation down the back of the thigh, 'the outeraspect of the calf and lateral side of the foot.On examination, she looked ill with a temperature
of 39.2°IC. Although the sciatic pain was very severe,the straight leg raising was normal and there wereno abnormal neurological signs in the legs.
Investigations revealed a white cell count of25,000/cu. mm. with a polymorphonucleocytosis.Intramuscular penicillin was commenced after a bloodculture had been taken. In the next forty-eight hoursthe pain became more severe, 'there being localisedtenderness over the sacro-iliac joint. Tihe temperatureremained high.At this time the decision was taken to aspirate the
joint and simultaneously perform a 'Caesarian section.The joint contained a large amount of pus whichon culture grew a coagulase positive staphylococcuspyogenes as did the blood culture. As a result ofthe culture sensitivities, erythromycin being the drugof choice, was commenced. Subsequently the patientmade a rapid recovery and her baby thrived. Aradiograph taken three weeks later showed an areaof sclerosis in the ilium just anterior to the sacro-iliacjoint which was regarded as the initial focus ofinfection. A year later the joint had spontaneouslyfused.
DiscussionThe classification of osteomyelitis of the
pelvis into clinical syndromes clarifies a con-dition of recognised diagnostic difficulty.Osteomyelitis of the spine presents a similarproblem, and Puig (1946) clarified diagnosisin a like manner, with his classification intomeningeal, abdominal and hip syndromes.The clinical features in patients with
osteomyelitis of the pelvis vary to such anextent that they may be referred to one ofseveral hospital departments, e.g. generalmedicine i(septicaemic syndrome), generalsurgery (abdominal syndrome), paediatric(limping child), or even orthopaedic. Theincidence of this disease is low and unless pelvicosteomyelitis is borne in mind by the examiningdoctor the correct diagnosis may be missedduring the early stage when the correct treat-ment would be most beneficial.As the infective lesion progresses the clinical
features multiply and syndromes emerge. Mostof our patients had features of two syndromesbut one syndrome predominated, preceded theother and was related to the site of the initialfocus of infection. Stress has to be laid onthese clinical features as early diagnosis isonly possible by considering them. Radio-graphic changes are late in appearing and the
February, 1966 77
by copyright. on 22 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.484.74 on 1 F
ebruary 1966. Dow
nloaded from
78 POSTGRADUATE MEDICAL JOURNAL February, 1966
infection may be well established and involvea large area of bone before radiographicchanges are recognisable.Among the initial routine investigations the
white blood cell count was of no diagnostichelp, as a raised count was found in onlyapproximately half of our cases. The erythro-cyte sedimentation rate was raised in all cases,suggesting that a normal value would be againsta diagnosis of acute osteomyelitis. Blood culturewas positive in two-thirds of the patients, andthe value of isolating and obtaining the sen-sitivity of the causative organism at an earlystage is obvious.
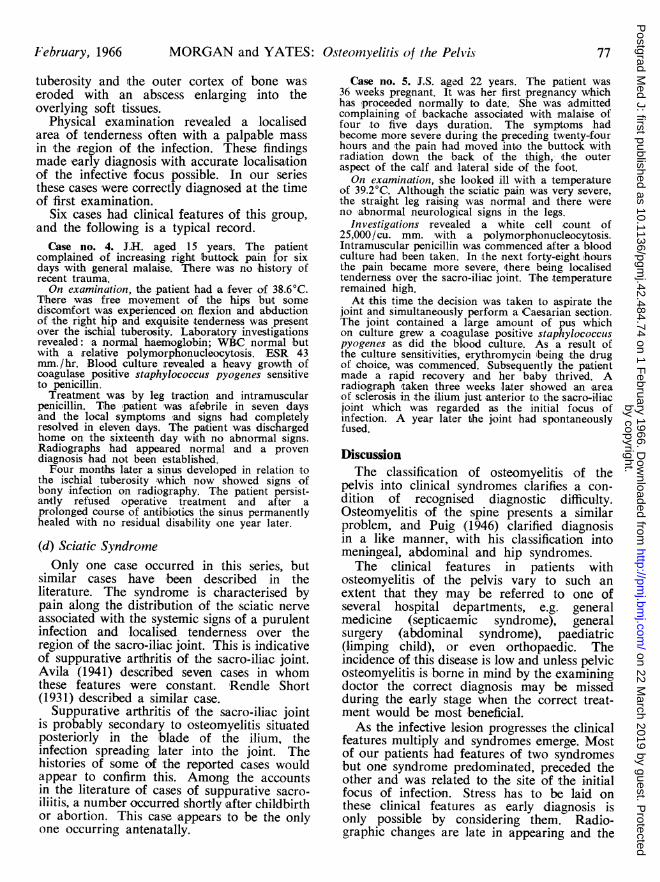
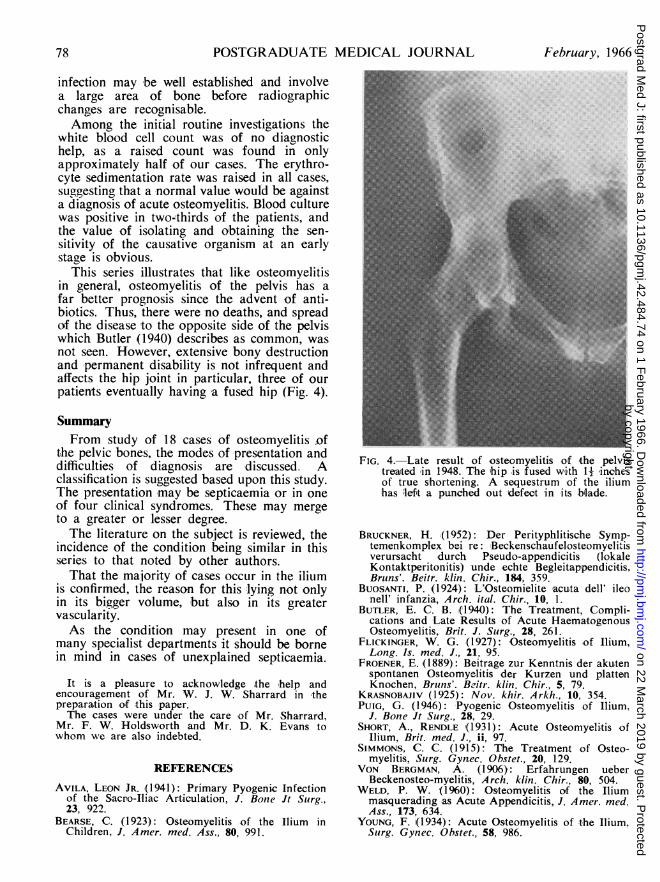
This series illustrates that like osteomyelitisin general, osteomyelitis of the pelvis has afar better prognosis since the advent of anti-biotics. Thus, there were no deaths, and spreadof the disease to the opposite side of the pelviswhich Butler (1940) describes as common, wasnot seen. However, extensive bony destructionand permanent disability is not infrequent andaffects the hip joint in particular, three of ourpatients eventually having a fused hip (Fig. 4).
SummaryFrom study of 18 cases of osteomyelitis of
the pelvic bones, the modes of presentation anddifficulties of diagnosis are discussed. Aclassification is suggested based upon this study.The presentation may be septicaemia or in oneof four clinical syndromes. These may mergeto a greater or lesser degree.The literature on the subject is reviewed, the
incidence of the condition being similar in thisseries to that noted by other authors.That the majority of cases occur in the ilium
is confirmed, the reason for this lying not onlyin its bigger volume, but also in its greatervascularity.As the condition may present in one of
many specialist departments it should be bornein mind in cases of unexplained septicaemia.
It is a pleasure to acknowledge the help andencouragement of Mr. W. J. W. Sharrard in thepreparation of this paper.The cases were under the care of Mr. Sharrard,
Mr. F. W. Holdsworth and Mr. D. K. Evans towhom we are also indebted.
FIG. 4.-Late result of .osteomyelitis of the pelvistreated iin 1948. T_hehip is fused with 1 -inchesof true shortening. A sequestrum of the iliumhas left a punched out defect in its blade.
REFERENCES
AVILA, LEON JR. (1941): Primary Pyogenic Infectionof the Sacro-Iliac Articulation, J. Bone Jt Surg.,23, 922.
BEARSE, C. (1923): Osteomyelitis of the Ilium inChildren, J. Amer. med. Ass., 80, 991.
BRUCKNER, H. (1952): Der Perityphlitische Symp-temenkomplex bei re: Beckenschaufelosteomyelitisverursacht durch Pseudo-appendicitis (lokaleKontaktperitonitis) unde echte Begleitappendicitis.Bruns'. Beitr. klin. Chir., 184, 359.
BUOSANTI, P. (1924): L'Osteomielite acuta dell' ileonell' infanzia, Arch. ital. Chir., 10, 1.
BUTLER, E. C. B. (1940): The Treatment, Compli-cations and Late Results of Acute HaematogenousOsteomyelitis, Brit. J. Surg., 28, 261.
FLICKINGER, W. G. (1927): Osteomyelitis of Ilium,Long. Is. med. J., 21, 95.
FROENER, E. (1889): Beitrage zur Kenntnis der akutenspontanen Osteomyelitis der Kurzen und plattenKnochen, Bruns'. Beitr. klin. Chir., 5, 79.
KRASNOBAJIV (1925): Nov. khir. Arkh., 10, 354.PUIG, G. (1946): Pyogenic Osteomyelitis of Ilium,
J. Bone Jt Surg., 28, 29.SHORT, A., RENDLE ,(1931): Acute Osteomyelitis of
Ilium, Brit. med. J., ii, 97.SIMMONS, C. C. (1915): The Treatment of Osteo-
myelitis, Surg. Gynec. Obstet., 20, 129.VON BERGMAN, A. (1906): Erfahrungen ueber
Beckenosteo-myelitis, Arch. klin. Chir., 80, 504.WELD, P. W. (1960): Osteomyelitis of the Ilium
masquerading as Acute Appendicitis, J. Amer. med.Ass., 173, 634.
YOUNG, F. (1934): Acute Osteomyelitis of the Ilium,Surg. Gynec. Obstet., 58, 986.
by copyright. on 22 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.484.74 on 1 F
ebruary 1966. Dow
nloaded from





























