Embed Size (px)
Citation preview

lable at ScienceDirect
Clinical Radiology 69 (2014) e291ee297
Contents lists avai
Clinical Radiology
journal homepage: www.cl inicalradiologyonl ine.net
The diagnosis of hemimegalencephaly using inutero MRIF. Williams a,*, P.D. Griffiths b
aDepartment of Neuroradiology, Royal Hallamshire Hospital, Sheffield, UKbAcademic Unit of Radiology, University of Sheffield, Sheffield, UK
article information
Article history:Received 27 November 2013Received in revised form29 January 2014Accepted 31 January 2014
* Guarantor and correspondent: F. Williams,ology, Royal Hallamshire Hospital, Glossop RoTel.: þ44 7525449964.
E-mail address: [email protected] (F. W
0009-9260/$ e see front matter � 2014 The Royal Cohttp://dx.doi.org/10.1016/j.crad.2014.01.026
AIM: To review our experience of diagnosing hemimegalencephaly (HME) using in uteromagnetic resonance imaging (MRI).MATERIALS AND METHODS: The MRI database in the Academic Unit of Radiology, University
of Sheffield was searched using “hemimegalencephaly” and “in utero MR” as search terms. Theantenatal histories and reports of ultrasound imaging were reviewed as well as the in uteroMRI images.RESULTS: Nine cases of foetal HME were located. One case was referred after ultrasound with
the diagnosis of HME, one as a “complex brain malformation”, and one as a “mass lesion”. Theother six were referred as “unilateral ventriculomegaly”. A common finding in foetuses imagedin the second trimester was disruption of the normal “transient structures” found in thedeveloping cerebral hemispheres.CONCLUSION: HME is a difficult diagnosis to make using antenatal ultrasound and in utero
MRI should be considered in cases of unilateral ventriculomegaly diagnosed at ultrasound.Disruption of the transient structures of the cerebral hemispheres is a common finding on inutero MRI and can sometimes produce mass-like appearances in the region of the germinalmatrix/ganglionic eminence.
� 2014 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Introduction
Hemimegalencephaly (HME) is a rare brain disordercharacterized by hamartomatous overgrowth of one cere-bral hemisphere. HME is also known as unilateral mega-lencephaly and the term “focal megalencephaly” isfrequently used if only part of the hemisphere is involved.Secondary effects of the brain overgrowth include ipsilat-eral enlargement of the cranium and lateral ventricle, but itis the abnormalities of cortical formation that define thepathology. A wide range of different abnormalities of
Department of Neuroradi-ad, Sheffield S10 2JF, UK.
illiams).
llege of Radiologists. Published by
cortical formation may be found in hemispheres affected byHME including pachygyria, heterotopia, and poly-microgyria, often in combination.1 Although the clinicalsequelae are difficult to predict, children born with HMEtend to be severely disabled with intractable seizures,hemiparesis, and developmental delay.2 HME is mostcommonly an isolated abnormality, but is found inconjunction with a wide range of clinical syndromesincluding epidermal nevus syndrome, Proteus syndrome,hypomelanosis of Ito, neurofibromatosis type, 1 and tuber-ous sclerosis.1,3,4
It is possible to make the diagnosis of HME using ante-natal ultrasound, but it was the impression of the presentauthors, prior to performing this review, that it can be adifficult diagnosis to make using ultrasound. The purpose ofthis paper was to investigate that supposition by reviewingthe authors’ experience of diagnosing HME using in utero
Elsevier Ltd. All rights reserved.

F. Williams, P.D. Griffiths / Clinical Radiology 69 (2014) e291ee297e292
magnetic resonance imaging (iuMRI) to supplement ante-natal ultrasound.
Material and methods
Participants
The pregnant women included in this retrospective,observational study underwent iuMRI at the University ofSheffield from 2000 to 2012 inclusive. The women werereferred from several hospitals in Britain when brain ab-normalities were known or suspected at antenatal ultra-sound. All of the cases came from foeto-maternal expertsworking in tertiary-referral centres, either an obstetricianor a radiologist. Cases were entered into this from one oftwo sources: either recruited as research cases under theguidance of the South Sheffield Research Ethics Committee,in which case they provided written consent after fullexplanation. Those women were not paid for theirinvolvement in the study but travel expenses were offeredfor themselves and a companion. The other cases wereperformed as clinical studies and relevant review andapproval was sought and obtained from the InstitutionalClinical Effectiveness Unit and Research Department in or-der to include those cases in this report.
iuMRI protocol
iuMRI was performed on one of two 1.5 T super-conducting systems (before 2008: Infineon, Philips MedicalSystems, Best, The Netherlands; 2008 and after HDx, GEHealthcare, Milwaukee, WI, USA). A range of sequenceswere performed but all included single-shot fast spin echo
Table 1Summary of ultrasound referral data, in utero magnetic resonance imaging findin
Case Ultrasound findings Gestationalage at iuMRI(weeks)
*DWI performed (he
1 HME 23 *(1.7) Focal megalencwith CFA and disrupventricular layer
2 Complex brain malformation 21 *(2.6) HME with comand widespread CFA
3 Unilateral VM 33 (1.6) HME with wideabnormal hemispher
4 Unilateral VM 23 (1.3) Focal megalenc
5 Unilateral VM 33 (1.2) HME with front
6 Unilateral VM 32 *(1.4) HME with fronin frontal and ganglio
7 Unilateral VM 25 (1.2) Focal megalenc
8 Asymmetric brain and mass lesion 21 *(1.3) HME with wid9 Unilateral VM 21 *(1.3) Focal megalenc
transient structures.
iuMRI, in utero magnetic resonance imaging; DWI, diffusion-weighted imagintriculomegaly; CFA, cortical formation abnormality.*The asterisk refers to the cases where it was possible to perform DWI.
(ssFSE) sequences (5 mm thick sections in all threeorthogonal planes and 3 mm thick sections in at least twoorthogonal planes). The exact parameters varied form caseto case but sample parameters for the ssFSE sequence usedat the time of writing were 1782 ms repetition time (TR),91.4 ms echo time (TE effective), 5 mm slice thickness, andecho train length of 184. From 2005 echo planar diffusion-weighted imaging in the axial plane was included in theroutine iuMRI protocol. The parameters of the sequenceused at the time of writing were 4000 ms TR, 108 ms TE(minimum), b ¼ 700 s/mm, and 5 mm section thickness.
iuMRI analysis
All of the iuMRI studies were reported clinically at thetime of the iuMRI examination but were reviewed retro-spectively by two radiologists experienced in foetal neuro-imaging (P.D.G., F.W.) for the purposes of this study. Thereview consisted of an estimate of the increased hemi-spheric size (using the ratio of maximum transverse widthof the hemisphere e abnormal/normal); the presence orabsence of a definable cortical malformation in the affectedhemisphere; any disruption to the usual transient struc-tures of the hemisphere; and the presence or absence ofother brain abnormalities.
Results
Approximately 1800 iuMRI studies of the foetal brainwere performed during the 12 years of this review and nineof those cases met the diagnostic criteria for HME, a sum-mary of their details is presented in Table 1. Three examplesare shown in Figs 1e3. HME was given as the specific
gs and outcome of pregnancy in nine cases of foetal hemimegalencephaly.
misphere ratio) MRI findings Outcome of pregnancy
ephaly (frontal and ganglionic)ted transient structures. Mass-like
Delivered 39 weeks.Confirmed at post-natalMRI
plete disruption of transient structures. Central mass-like ventricular layer
TOP at 22 weeks.No autopsy
spread CFA. Extensive low signal ine on ssFSE images.
Delivered 34 weeks.Confirmed at post-natalMRI
ephaly (frontal) with CFA TOP at 23 weeksNo autopsy
al CFA Delivered 36 weeks.Confirmed at post-natalMRI
tal CFA. Generalized increased diffusionnic regions
Stillborn 33 weeks.No autopsy.
ephaly (occipital and parietal) with CFA Delivered 39 weeks.No follow-up available
espread CFA. Central mass-like ventricular layer TOP at 21 weeksephaly (frontal and ganglionic) with disruptedMass-like ventricular layer
Current case at the timeof writing
g; HME, hemimegalencephaly; TOP, termination of pregnancy; VM, ven-

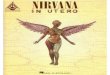
Figure 1 iuMRI of a foetus at 21 weeks gestational age with hemi-megalencephaly (case 2). ssFSE images in the coronal (a) and axialplane (b) show gross asymmetry of the hemispheres of the affectedbrain with a mass-like overgrowth of the ventricular zone (germinalmatrix).
F. Williams, P.D. Griffiths / Clinical Radiology 69 (2014) e291ee297 e293
diagnosis on antenatal ultrasound in one of the nine cases,“complex brain malformation” in one case, and “brainasymmetry and mass lesion” in one case. In the other sixcases, the ultrasound diagnosis was unilateral ven-triculomegaly. The abnormality shown on iuMRI involvedall, or most of, the affected hemisphere sufficient to make adiagnosis of HME in five cases and in four cases the mal-formation involved only part of the hemisphere consistent
with a diagnosis of focal megalencephaly (frontal in threeand occipital in one).
A prominent feature of the foetuses imaged in the secondtrimester of pregnancy was disruption of the normal“transient structures” of the developing cerebral hemi-sphere. Although this feature could be shown on ssFSE se-quences, it was much better appreciated on the diffusion-weighted imaging when that type of study was per-formed. In four of those cases, the disrupted transientstructures produced a mass-like abnormality, particularlyinvolving the ventricular region (Figs 1 and 2). In two of thefoetuses imaged in the third trimester, there was a uniformlower signal in the involved hemisphere on ssFSE images,and in the one case that underwent diffusion-weightedimaging, restricted diffusion of water was demonstrated.The significance of these findings is discussed below.
Discussion
HME is classified as a malformation of cortical formation.The grey-matter structures of the cerebral hemispheresoriginate from the ventricular layer (germinal matrix) of thedeveloping hemisphere, and the neurons and glia mustmigrate outwards to their final position in either the cere-bral cortex or the deep grey structures. Barkovich and col-leagues5 subclassified such disorders depending on thefailure of the temporal sequence of formation of the cere-bral cortex, i.e., failure of neuronal/glial proliferation in theventricular zone, failure of migration, and failure of corticalorganisation. The classification is more complicatedbecause an abnormality in an earlier process is highly likelyto interfere with the related later process, e.g., abnormalneuronal formation is likely to have a deleterious impact onboth neuronal migration and cortical formation. Abnor-malities of cortical formation, therefore, are classified by thedevelopmentally earliest event that is known to be defec-tive. Using that approach, HME is classified as a focal, non-neoplastic failure of neuronal/glial proliferation. As such,there is a unilateral overproduction of neurons and glia,which produces the increased volume of the affected ce-rebral hemisphere. The cells are embryologically immatureand so migration and cortical organisation are necessarilyfaulty, explaining the pachygyria, polymicrogyria, and het-erotopia that are found as part of the pathological process.
Although rare, the post-natal imaging appearances ofHME are well described in peer reviewed publications andtextbooks, as is the growing number of rare syndromeswithwhich HME has been found in association. The commonestimaging findings involve some combination of corticalmalformation (broad gyri, shallow sulci, and/or thick cor-tex) and white matter abnormalities (gliosis and hetero-topia). There are fewer published reports of HME diagnosedin utero, consisting of a case report6 or cases of HME foundin wider studies of iuMRI as a technique for diagnosingfoetal brain abnormalities.7e9 It should be noted that four ofthe cases reported in the present paper were included in theanalyses of two previous papers,8,9 but were not discussedindividually. One of the characteristic features of the foetal

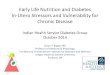
Figure 2 iuMRI of a foetus at 23 weeks gestational age with focal megalencephaly involving the left frontal lobe (case 1). ssFSE images in thecoronal (a) and axial plane (b) show asymmetry of the frontal lobes of the affected brain with a mass-like overgrowth of the ventricular zone(germinal matrix). Disruption of the normal transient structures in the affected part of the brain is well shown on axial diffusion-weightedimaging (c).
F. Williams, P.D. Griffiths / Clinical Radiology 69 (2014) e291ee297e294
brain, particularly in the second trimester is the presence of“transient structures” that occur in a laminar pattern in thedeveloping hemispheres. Histologically, six layers can bedemonstrated and five of those are visible macroscopicallyon tissue sections. From the ventricular surface outwards,they are the ventricular zone (germinal matrix), sub-ventricular zone, intermediate zone, subplate, and corticalplate (Fig 4a). Of those, the ventricular zone, intermediatezone, and cortical plate are cell-dense, whereas the peri-ventricular and subplate zones are cell-sparse/fluid-rich(and without myelin). As such, they have different signalcharacteristics that produce discrete layers visible on T2-weighted images, particularly well-shown on post-mortem MRI (Fig 4b), but they can also be delineated tosome degree of ssFSE T2-weighted images used at iuMRI(Fig 4c). They are not shown as well on the ultrafast iuMRIexaminations due to constraints in both anatomical andcontrast resolution, brought about by the wide range of TEsfrom multiple echoes used to create the image.
Diffusion-weighted imaging usually delineates thetransient structures better than ssFSE sequences and isoften used for that purpose, although it is highly sensitive tofoetal movement. Diffusion imaging is used to look forrestricted diffusion of water, which shows as high signal ondiffusion-weighted imaging and as low signal on para-metric maps of apparent diffusion coefficients. In routineclinical neuroimaging, diffusion-weighted imaging is usedas the most sensitive indicator of acute/subacute stroke bydetecting restricted diffusion in areas of cytotoxic oedema.In the foetal brain, the cell-rich and cell-sparse transientstructures have different diffusion characteristics, with highdiffusion coefficients in the cell-sparse zones and restricteddiffusion in the cell-rich regions (as is seen in tissues withsmall cells with high nuclear/cytoplasmic ratios; Fig 4d). Intheory, the detection of the transient layers should be avaluable assistance in trying to detect some forms ofabnormal cortical formation in utero. The intermediate, cell-rich layer for example contains primarily neurons and glia

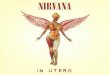
Figure 3 iuMRI of a foetus at 32 weeks gestational age with hemimegalencephaly (case 6). ssFSE images in the coronal (a) and axial plane (bec)show increased size of the right hemisphere and heterotopia in the frontal lobe. Axial diffusion-weighted imaging (d) shows mild restricteddiffusion in the central portion of the right hemisphere.
F. Williams, P.D. Griffiths / Clinical Radiology 69 (2014) e291ee297 e295
that are en route to the future cerebral cortex and anydisruption in that structure might be an indication of dis-rupted proliferation or migration. The transient layersdescribed above disappear quite quickly after the end of thesecond trimester, with only the remnants of the ventricularzone (germinal matrix) demonstrable on iuMRI after 30weeks (Fig 4e and f). As such, the possible use of transientlayers as an indicator of abnormal cortical formationmay beof progressively less value after 24 weeks.
Disruption of the transient layers was a consistentfinding in second trimester foetuses with HME whendiffusion-weighted imaging was performed. The secondtrimester cases performed in the early part of the study didnot have diffusion-weighted imaging and the quality of thessFSE was lower, inasmuch as it was difficult to see thelaminar form of the transient structures consistently innormal cases. A feature that is of interest is that in four casesthere was such hyperplasia of the ventricular zone that it
appeared mass-like. It is possible that this could be mis-interpreted as a haemorrhagic tumour because of the lowsignal of that structure on ssFSE weighted images. A betterquality ssFSE and diffusion-weighted imaging was per-formed in only one-third trimester foetus, and although thetransient layers have predominantly disappeared at thattime, there remained uniform restricted diffusion in theaffected hemisphere. The case report of Agid et al.6 was of a32-week-old foetus whose iuMRI protocol includeddiffusion-weighted imaging. The authors describe that thewoman was referred with a diagnosis of severe, unilateralventriculomegaly at ultrasonography, as were six of thenine cases in the present report. The findings at diffusion-weighted imaging in the case reported by Agid et al.6
were very similar to those in the third trimester case inthe present study, showing an extensive area of restricteddiffusion. Similar to those authors, the restricted diffusion ismost likely to be due to increased cellularity in the white

Figure 4 (a) A coronal tissue section of a foetus at 22 weeks gestational age demonstrates the normal transient structures in the secondtrimester cerebral hemisphere (see Discussion). Those features are well shown on high-resolution MRI of a 22-week-old foetus post-mortem (b).The transient laminar structures are demonstrated to a limited extent on SSFSE T2-weighted images of a 22-week-old foetus in utero (c), but aremore clearly seen on diffusion-weighted imaging (d). The transient nature of those structures is appreciated by the virtual disappearance of thelaminar pattern in a 31-week-old foetus in utero (eef).
F. Williams, P.D. Griffiths / Clinical Radiology 69 (2014) e291ee297e296

F. Williams, P.D. Griffiths / Clinical Radiology 69 (2014) e291ee297 e297
matter of the developing, non-myelinated cerebral hemi-sphere, as it is known histologically that there is an excess ofglial cells and abnormal neurons in the white matter ofHME. Also noted is the suggestion made by Agid et al.6 thatthe restricted diffusion could be due to advanced myelina-tion in the hemisphere.
In conclusion, hemimegalencephaly appears to be adifficult diagnosis to make at antenatal ultrasound andiuMRI should be considered in cases of unilateral ven-triculomegaly diagnosed at ultrasound, especially whenassociated with any suspicion of asymmetry or midlineshift. A useful feature to aid the diagnosis of HME at iuMRIin the second trimester is disruption of the transientstructures of the cerebral hemispheres, particularly ondiffusion-weighted imaging. It should also be appreciatedthat the disrupted transient structures may have mass-likeappearances.
Acknowledgements
P.D.G. is a member of a medical advisory board for GEhealthcare and is in receipt of research funding from GEHealthcare.
References
1. Barkovich AJ, Raybaud CA. Congenital malformations of the brain andskull. Chapter 5. In: Barkovich AJ, Raybaud CA, editors. Pediatric neuro-imaging. 5th ed. Philadephia: Lippincott, Williams and Wilkins; 2012.pp. 367e568.
2. Sasaki M, Hashimoto T, Furushima W, et al. Clinical aspects of hemi-megalencephaly by means of a nationwide survey. J Child Neurol2005;20:337e41.
3. Griffiths PD, Welch RJ, Gardner-Medwin D, et al. The radiological featuresof hemimegalencephaly. Neuropediatrics 1994;25:140e4.
4. Griffiths PD, Gardner S, Smith M, et al. Cortical malformations in tuberoussclerosis complex: reports of associated hemimegalencephaly and focalmegalencephaly. AJNR Am J Neuroradiol 1998;19:1935e8.
5. Barkovich AJ, Kuzniecky RI, Dobyns WB, et al. A classification schemefor malformations of cortical development. Neuropediatrics 1996;27:59e63.
6. Agid R, Lieberman S, Nadjari M, et al. Prenatal MR diffusion weightedimaging in a fetus with hemimegalencephaly. Pediatr Radiol 2006;36:138e40.
7. Yuh WT, Nguyen HD, Fisher DJ, et al. MR of fetal CNS abnormalities. AJNRAm J Neuroradiol 1994;15:459e64.
8. Whitby EH, Paley MNJ, Sprigg A, et al. Outcome of 100 singleton preg-nancies with suspected brain abnormalities diagnosed on ultrasound andinvestigated by in utero MR imaging. Br J Obstet Gynaecol 2004;111:784e92.
9. Griffiths PD, Reeves MJ, Morris JE, et al. A prospective study of fetuseswith isolated ventriculomegaly investigated by antenatal ultrasound andin utero MR. AJNR Am J Neuroradiol 2010;31:106e11.












![Nirvana - [Book] in Utero - Guitar Songbook 3](https://img.pdfslide.us/doc/110x75/5695cff41a28ab9b02904a8a/nirvana-book-in-utero-guitar-songbook-3.jpg)