Embed Size (px)
DESCRIPTION
The Diabetic Retinopathy Clinical Research Network. Dedicated to multicenter clinical research of diabetic retinopathy, macular edema and associated conditions Carl W. Baker, MD for the Diabetic Retinopathy Clinical Research Network - PowerPoint PPT Presentation
Citation preview
The Diabetic Retinopathy Clinical Research Network
The Diabetic Retinopathy Clinical Research Network
Dedicated to multicenter clinical research of diabetic
retinopathy, macular edema and associated conditions
Carl W. Baker, MD for the Diabetic Retinopathy Clinical Research Network
Supported through a cooperative agreement from the National Eye Institute and the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Department of Health and
Human Services EY14231, EY018817
Financial DisclosuresFinancial Disclosures Carl Baker:
22
Bausch and Lomb 25 Jan 2012 25 Jan 2013Consultancy, Payment for lectures
Alimera Sciences 25 Jan 2012 25 Jan 2013Clinical or lab research grants
ArcticDx Inc. 25 Jan 2012 25 Jan 2013 Employment
GlaxoSmithKline 25 Jan 2012 25 Jan 2013Clinical or lab research grants
Allergan 25 Jan 2012 25 Jan 2013Clinical or lab research grants
Genentech 25 Jan 2012 25 Jan 2013Clinical or lab research grants
Neovista 25 Jan 2012 25 Jan 2013Clinical or lab research grants
Course OutlineCourse Outline
33
1. DRCR.net Overview. Carl W. Baker, MD 2. DRCR.net recent trial results
Intravitreal Anti-VEGF vs. Saline for Diabetic Vitreous Hemorrhage. Abdhish R. Bhavsar, MD
3. Rationale for ongoing trials Comparison of aflibercept, ranibizumab, and bevacizumab
for DME. Jack Wells, MD Ranibizumab vs. PRP for Proliferative diabetic retinopathy.
Jennifer K. Sun, MD
Course OutlineCourse Outline4. Common Topics for Clinical case review/discussion Incomplete response of DME to
anti-VEGF treatment.
Susan B Bressler, MD
Asymptomatic 20/20 VA with central-involved DME.
Neil M Bressler, MD
Role of laser in DME. Lee Jampol, MD
44
Managing DME and PDR when both present in the same eye.
John A Wells, III MD
Standard vs wide-field fundus photographs and fluorescine angiography in the management of DME and PDR.
Jennifer K Sun, MD
DME treatment in Pseudophakic Eyes.
Scott M Friedman, MD
DRCR.net OverviewDRCR.net Overview Objective:
• The development of a collaborative network to facilitate multicenter clinical research on diabetic retinopathy, DME and associated conditions.
Funding:• National Eye Institute (NEI) and The National Institute of
Diabetes and Digestive and Kidney Diseases (NIDDK)-sponsored cooperative agreement initiated September 2002.
o Current award 2009-2013
55
DRCR.net OverviewDRCR.net Overview Network Chair: Neil M.
Bressler, M.D.Wilmer Ophthalmological Institute at
Johns Hopkins, Baltimore, MD Network Chair elect:
Lee M. Jampol, M.D.Northwestern University Medical School, Department of Ophthalmology, Chicago, IL
Director of the Coordinating Center:
Adam R. Glassman, M.S. (Jaeb Center for Health Research) 66
National Eye Institute Project Officer: Eleanor B. Schron, Ph.D., R.N.
Vice-Chairs (2013): Carl W. Baker, M.D., Paducah
Retinal Center, Scott M. Friedman, M.D., Florida
Retina ConsultantsJennifer K. Sun, M.D., M.P.H.,
Joslin Diabetes Center

Priority InitiativesPriority Initiatives Involvement of community-based practices, as Involvement of community-based practices, as
well as “academic” or university-based centers. well as “academic” or university-based centers.
Collaborate with industryCollaborate with industry to facilitate to facilitate investigations and pursue opportunities otherwise investigations and pursue opportunities otherwise not possible and to do so in a manner consistent not possible and to do so in a manner consistent with the Network’s dedication to academic with the Network’s dedication to academic integrity and optimal clinical trial performance.integrity and optimal clinical trial performance.
77
Organization: Clinical Sites of the Network
Organization: Clinical Sites of the Network
Overall Network Participation (as of 10/07/13)• 285 sites submitted application for Network • 1017 total Investigators; 3261 additional personnel
Network is open and continually solicits participation of new sites and investigators
88
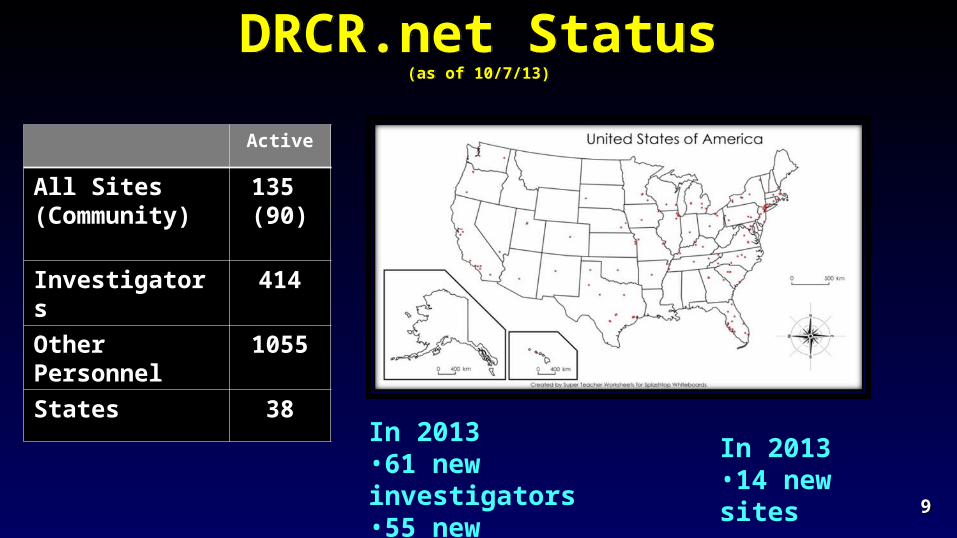
DRCR.net Status(as of 10/7/13)
DRCR.net Status(as of 10/7/13)
Active
All Sites (Community)
135 (90)
Investigators 414
Other Personnel
1055
States 38
99
In 2013•14 new sites
In 2013•61 new investigators•55 new coordinators
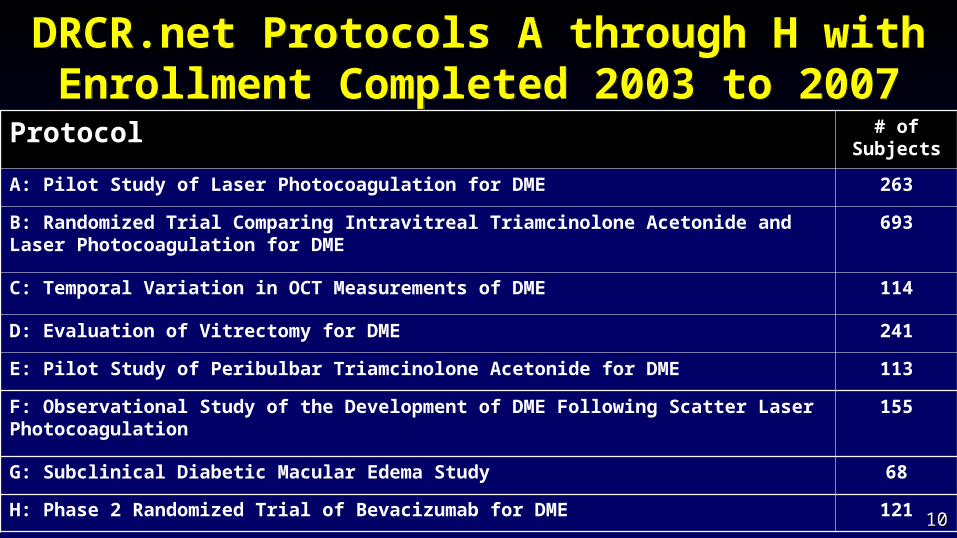
DRCR.net Protocols A through H with Enrollment Completed 2003 to 2007
DRCR.net Protocols A through H with Enrollment Completed 2003 to 2007
1010
Protocol # of Subjects
A: Pilot Study of Laser Photocoagulation for DME 263
B: Randomized Trial Comparing Intravitreal Triamcinolone Acetonide and Laser Photocoagulation for DME
693
C: Temporal Variation in OCT Measurements of DME 114
D: Evaluation of Vitrectomy for DME 241
E: Pilot Study of Peribulbar Triamcinolone Acetonide for DME 113
F: Observational Study of the Development of DME Following Scatter Laser Photocoagulation
155
G: Subclinical Diabetic Macular Edema Study 68
H: Phase 2 Randomized Trial of Bevacizumab for DME 1211010
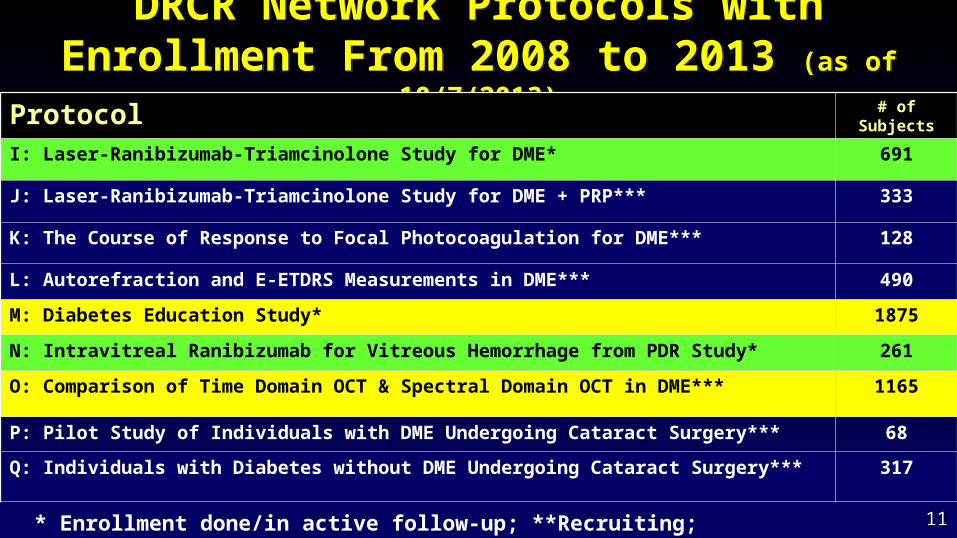
DRCR Network Protocols with Enrollment From 2008 to 2013 (as of 10/7/2013)
DRCR Network Protocols with Enrollment From 2008 to 2013 (as of 10/7/2013)
1111
Protocol # of Subjects
I: Laser-Ranibizumab-Triamcinolone Study for DME* 691
J: Laser-Ranibizumab-Triamcinolone Study for DME + PRP*** 333
K: The Course of Response to Focal Photocoagulation for DME*** 128
L: Autorefraction and E-ETDRS Measurements in DME*** 490
M: Diabetes Education Study* 1875
N: Intravitreal Ranibizumab for Vitreous Hemorrhage from PDR Study* 261
O: Comparison of Time Domain OCT & Spectral Domain OCT in DME*** 1165
P: Pilot Study of Individuals with DME Undergoing Cataract Surgery*** 68
Q: Individuals with Diabetes without DME Undergoing Cataract Surgery*** 317
* Enrollment done/in active follow-up; **Recruiting; ***Enrollment/follow-up done
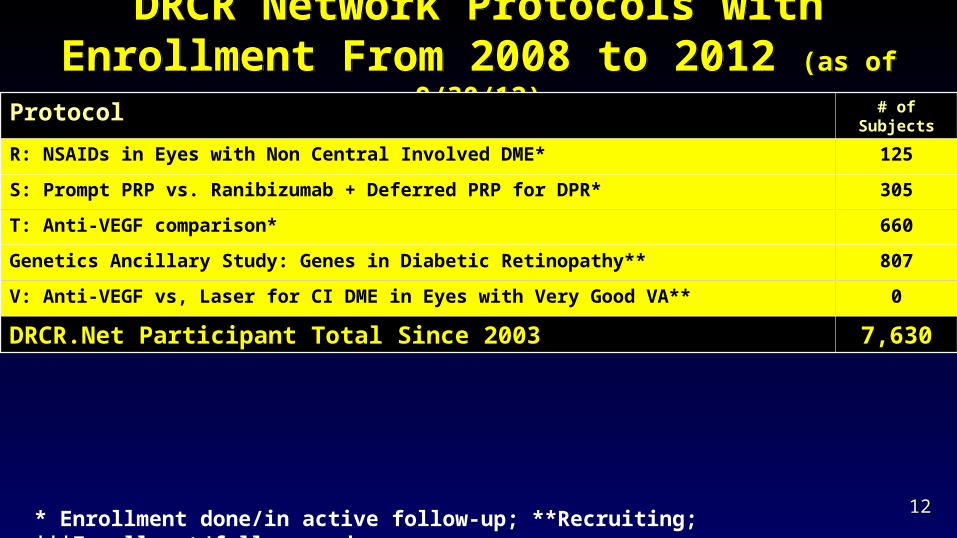
DRCR Network Protocols with Enrollment From 2008 to 2012 (as of 9/30/12)
DRCR Network Protocols with Enrollment From 2008 to 2012 (as of 9/30/12)
Protocol # of Subjects
R: NSAIDs in Eyes with Non Central Involved DME* 125
S: Prompt PRP vs. Ranibizumab + Deferred PRP for DPR* 305
T: Anti-VEGF comparison* 660
Genetics Ancillary Study: Genes in Diabetic Retinopathy** 807
V: Anti-VEGF vs, Laser for CI DME in Eyes with Very Good VA** 0
DRCR.Net Participant Total Since 2003 7,630
* Enrollment done/in active follow-up; **Recruiting; ***Enrollment/follow-up done 1212
What Has Been Learned?Diabetic Macular Edema Treatment
What Has Been Learned?Diabetic Macular Edema Treatment Protocol B: Over 2 years, focal/grid photocoagulation is more
effective and has fewer side effects than 1 mg or 4 mg doses of preservative-free intravitreal triamcinolone.
Protocol E: In cases of DME with good visual acuity, peribulbar triamcinolone, with or without focal photocoagulation, is unlikely to be of substantial benefit.
Protocol H: The results demonstrated that intravitreal bevacizumab can reduce DME in some eyes, but the study was not designed to determine whether the treatment was beneficial.
1313
What Has Been Learned?Diabetic Macular Edema Treatment
What Has Been Learned?Diabetic Macular Edema Treatment
Protocol I: Intravitreal ranibizumab with prompt or deferred (≥24 weeks) focal/grid laser is more effective through 2 years in increasing visual acuity compared with focal/grid laser treatment alone for the treatment of DME involving the central macula. Ranibizumab should be considered for patients with DME and decreased visual acuity.
Protocol K: Sixteen weeks after focal/grid laser for diabetic macular edema in eyes with a definite reduction, but not resolution, of central edema, 23% to 63% likely will continue to improve without additional treatment.
1414
What Has Been Learned?Diabetic Retinopathy Treatment
What Has Been Learned?Diabetic Retinopathy Treatment
Protocol F: Clinically meaningful differences are unlikely in OCT thickness or visual acuity following application of PRP in 1 sitting compared with 4 sittings. These results suggest PRP costs to some patients in terms of travel and lost productivity as well as to eye care providers could be reduced.
Protocol J: The addition of 1 or 2 intravitreal triamcinolone injections in eyes receiving focal/grid laser for DME and PRP is associated with better visual acuity and decreased macular edema by 14 weeks. Whether continued long-term intravitreal treatment is beneficial cannot be determined from this study.
1515
What Has Been Learned?OCT and Retinal Thickening
What Has Been Learned?OCT and Retinal Thickening
Protocol C: Although on average there are slight decreases in retinal thickening during the day, most eyes with DME have little meaningful change in OCT CSF thickening or VA between 8 AM and 4 PM.
Protocol C: Reproducibility of retinal thickness in DME was better for CSF thickness than for center point measurements. A change in CSF thickness exceeding 11% is likely to be real.
Protocol G: While subclinical DME may be uncommon, this study suggests that between ~25% and 50% of eyes with subclinical DME will progress to more definite thickening or be judged to need treatment for DME within 2 years after its identification.
1616
What Has Been Learned?Optical Coherence Tomography
What Has Been Learned?Optical Coherence Tomography
Protocol G: CSF thickness on Stratus OCT™ in people with diabetes and minimal or no retinopathy are similar to a normative database of people without diabetes. CSF thickness is greater in men than in women. Studies involving comparisons of retinal thickness to expected norms should consider different mean values for women and men.
Protocol O: Mean CSF thickness is ~70 µm thicker when measured with Heidelberg Spectralis OCT as compared with Stratus OCT among individuals with diabetes in the absence of retinopathy or with minimal non-proliferative retinopathy and a normal macular architecture. CSF thickness values ≥320 µm for men and 305 µm for women are proposed as gender-specific thickness levels.
1717
1818Image: National Eye Institute, National Institutes of Health
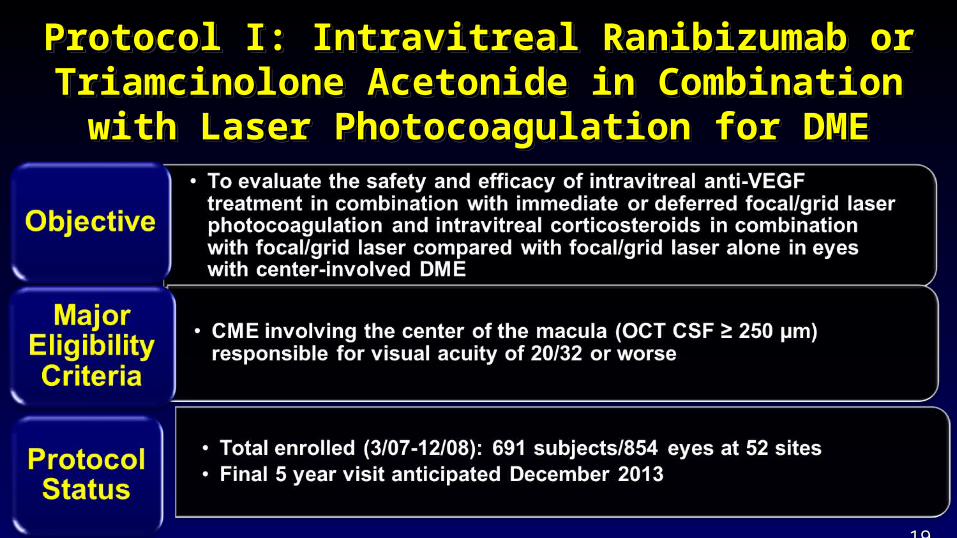
Protocol I: Intravitreal Ranibizumab or Protocol I: Intravitreal Ranibizumab or Triamcinolone Acetonide in Combination with Laser Triamcinolone Acetonide in Combination with Laser
Photocoagulation for DMEPhotocoagulation for DME
Protocol I: Intravitreal Ranibizumab or Protocol I: Intravitreal Ranibizumab or Triamcinolone Acetonide in Combination with Laser Triamcinolone Acetonide in Combination with Laser
Photocoagulation for DMEPhotocoagulation for DME
1919
Protocol M: Effect of Diabetes Education Protocol M: Effect of Diabetes Education during Ophthalmology Visits on Diabetes during Ophthalmology Visits on Diabetes
ControlControl
Protocol M: Effect of Diabetes Education Protocol M: Effect of Diabetes Education during Ophthalmology Visits on Diabetes during Ophthalmology Visits on Diabetes
ControlControl Objective
• To assess whether glycemic control (assessed with HbA1c measurement) in individuals with type 1 or type 2 diabetes can be improved with a point-of-care measurement of HbA1c in the ophthalmologist’s office combined with a personalized risk assessment for diabetic retinopathy and other complications of diabetes
2020
Protocol M: Effect of Diabetes Education Protocol M: Effect of Diabetes Education during Ophthalmology Visits on Diabetes during Ophthalmology Visits on Diabetes
ControlControl
Protocol M: Effect of Diabetes Education Protocol M: Effect of Diabetes Education during Ophthalmology Visits on Diabetes during Ophthalmology Visits on Diabetes
ControlControl Major Eligibility Criteria
• Diagnosis of diabetes mellitus (type 1 or type 2)
• Patient is not eligible if patient has a known HbA1c <7.5% within prior 6 months
Enrollment (Complete)• Total enrolled: 1875 participants at
43 sites
2121
Protocol N: An Evaluation of Intravitreal Protocol N: An Evaluation of Intravitreal Ranibizumab for Vitreous Hemorrhage Due Ranibizumab for Vitreous Hemorrhage Due
to Proliferative Diabetic Retinopathyto Proliferative Diabetic Retinopathy
Protocol N: An Evaluation of Intravitreal Protocol N: An Evaluation of Intravitreal Ranibizumab for Vitreous Hemorrhage Due Ranibizumab for Vitreous Hemorrhage Due
to Proliferative Diabetic Retinopathyto Proliferative Diabetic Retinopathy Objective
• To determine if intravitreal injections of ranibizumab decrease the proportion of eyes in which vitrectomy is performed compared with saline injections in eyes presenting with vitreous hemorrhage from proliferative diabetic retinopathy
2222
Protocol N: An Evaluation of Intravitreal Protocol N: An Evaluation of Intravitreal Ranibizumab for Vitreous Hemorrhage Due Ranibizumab for Vitreous Hemorrhage Due
to PDRto PDR
Protocol N: An Evaluation of Intravitreal Protocol N: An Evaluation of Intravitreal Ranibizumab for Vitreous Hemorrhage Due Ranibizumab for Vitreous Hemorrhage Due
to PDRto PDR Major Eligibility Criteria
• Study eye witho Vitreous hemorrhage
causing vision impairment, presumed to be from PDR, and precluding completion of PRP
o Immediate vitrectomy not required
2323
Protocol Status • Total enrolled (6/10-
10/11): 261 subjects at 61 sites
• Final visit November 2012
Protocol O: Comparison of Time Domain OCT Protocol O: Comparison of Time Domain OCT and Spectral Domain OCT Retinal Thickness and Spectral Domain OCT Retinal Thickness
Measurement in DMEMeasurement in DME
Protocol O: Comparison of Time Domain OCT Protocol O: Comparison of Time Domain OCT and Spectral Domain OCT Retinal Thickness and Spectral Domain OCT Retinal Thickness
Measurement in DMEMeasurement in DME Objective
• Compare thickness measurements between Zeiss TD Stratus OCT and selected SD OCT machines (Zeiss Cirrus, Heidelberg Spectralis, Topcon 3D-OCT, and Optovue RTVue), estimating a conversion factor between TD OCT and SD OCT
• To assess and compare the reproducibility of the selected SD OCT machines utilizing their respective software analysis algorithms
Major Eligibility Criteria• DME in at least one eye (OCT CSF ≥250 µm)
Enrollment (Ongoing)• Total enrolled: 1165 participants at 39 sites (as of 9/30/12)
2424
Protocol R: A Phase II Evaluation of Topical Protocol R: A Phase II Evaluation of Topical NSAIDs in Eyes with Non Central Involved NSAIDs in Eyes with Non Central Involved
DMEDME
Protocol R: A Phase II Evaluation of Topical Protocol R: A Phase II Evaluation of Topical NSAIDs in Eyes with Non Central Involved NSAIDs in Eyes with Non Central Involved
DMEDME Objective
• To assess the effects of topical NSAIDs on macular retina volume compared with placebo in eyes with non-central DME
• To assess the effects of topical NSAIDs on central subfield thickness and to compare the progression of non-central DME to central DME as determined by OCT and stereoscopic fundus photographs
2525
Protocol R continuedProtocol R continued Major Eligibility Criteria
• Best corrected E-ETDRS VA letter score ≥74 (20/25 or better)
• Definite retinal thickening due to DME within 3000 µm of the center of the macula but not involving the central subfield
• No focal/grid laser within the last 6 months or other treatment for DME within the last 4 months
Enrollment • Total enrolled: 125 subjects randomized at 40 sites (as of
10/7/13)2626
Protocol S: Prompt PRP versus Intravitreal Protocol S: Prompt PRP versus Intravitreal Ranibizumab with Deferred PRP for PDRRanibizumab with Deferred PRP for PDR
Protocol S: Prompt PRP versus Intravitreal Protocol S: Prompt PRP versus Intravitreal Ranibizumab with Deferred PRP for PDRRanibizumab with Deferred PRP for PDR
Objective• To determine if visual acuity outcomes at 2
years in eyes with PDR that receive anti-VEGF therapy with deferred PRP are non-inferior to those in eyes that receive standard prompt PRP therapy.
2727
Protocol S: Prompt PRP versus Intravitreal Protocol S: Prompt PRP versus Intravitreal Ranibizumab with Deferred PRP for PDRRanibizumab with Deferred PRP for PDR
Protocol S: Prompt PRP versus Intravitreal Protocol S: Prompt PRP versus Intravitreal Ranibizumab with Deferred PRP for PDRRanibizumab with Deferred PRP for PDR
Major Eligibility Criteria• Study eye with
o PDR for which PRP can be safely deferred for at least 4 weeks in the investigator’s judgment.
o No prior PRPo Visual acuity letter score in the study eye > 24
(~ Snellen equivalent of 20/320 or better) Enrollment (Complete)
• Total enrolled: 305 participants and 394 study eyes at 56 sites
2828
Protocol T: A Comparative Effectiveness Protocol T: A Comparative Effectiveness Study of Intravitreal Aflibercept, Bevacizumab Study of Intravitreal Aflibercept, Bevacizumab
and Ranibizumab for DMEand Ranibizumab for DME
Protocol T: A Comparative Effectiveness Protocol T: A Comparative Effectiveness Study of Intravitreal Aflibercept, Bevacizumab Study of Intravitreal Aflibercept, Bevacizumab
and Ranibizumab for DMEand Ranibizumab for DME Objective
• To compare the efficacy and safety of intravitreal (1) aflibercept, (2) bevacizumab, and (3) ranibizumab when given to treat central-involved DME
o Specifically, the primary outcome is to assess if either of these three anti-VEGF products is superior to the other with respect to mean changes in visual acuity.
2929
Protocol T: A Comparative Effectiveness Protocol T: A Comparative Effectiveness Study of Intravitreal Aflibercept, Bevacizumab Study of Intravitreal Aflibercept, Bevacizumab
and Ranibizumab for DMEand Ranibizumab for DME
Protocol T: A Comparative Effectiveness Protocol T: A Comparative Effectiveness Study of Intravitreal Aflibercept, Bevacizumab Study of Intravitreal Aflibercept, Bevacizumab
and Ranibizumab for DMEand Ranibizumab for DME Major Eligibility Criteria
• Study eye witho Central-involved DME (OCT CSF ≥250 µm on Zeiss
Stratus or equivalent on spectral domain OCT).o Visual acuity letter score ≤ 78 and >24 (≈ Snellen
20/32 to 20/320) within eight days of randomization.o No prior intravitreal anti-VEG within prior 12 months
Enrollment (complete)• Total enrolled: 660 subjects at 89 sites 3030
Genes in Diabetic Retinopathy ProjectGenes in Diabetic Retinopathy Project Objective
• To create a repository of genetic material and clinical phenotype information as a resource for the research community
• The database may provide the opportunity to assess genetic susceptibility and resistance to DR and also variants impacting visually-important biomarkers for ME and neovascularization.
Major Eligibility Criteria• Previous or current participant in a DRCR.net study
Enrollment (Ongoing)• Total enrolled: 807 subjects
3131
Protocol V: Treatment for Central-Involved DME in Eyes with Very Good Visual AcuityProtocol V: Treatment for Central-Involved DME in Eyes with Very Good Visual Acuity
Objective: To compare the safety and efficacy of prompt focal/grid photocoagulation + deferred intravitreal anti-VEGF, observation + deferred intravitreal anti-VEGF, and prompt intravitreal anti-VEGF in eyes with central-involved DME and good visual acuity.
• Good VA defined as a Snellen equivalent of 20/25 or better (electronic-ETDRS letter score of 79 or better).
3232
Protocol V: Treatment for Central-Involved DME in Eyes with Very Good Visual AcuityProtocol V: Treatment for Central-Involved DME in Eyes with Very Good Visual Acuity
Major Eligibility Criteria:• Must be at two consecutive visits within 1 to 28 days:
o Ophthalmoscopic evidence of CI DME in study eye confirmed on OCT at two consecutive visits within 1 to 28 days; defined by OCT CSF thickness on Zeiss Cirrus or Heidelberg Spectralis OCT.
o VA letter score in study eye ≥ 79 (~Snellen equivalent 20/25 or better) at two consecutive visits within 1 to 28 days
• No history of prior laser or other surgical, intravitreal, or peribulbar treatment for DME in the study eye
• Enrollment Begins November 2013
3333
Protocols In Development Protocols In Development Protocol U – Fall 2013Protocol U – Fall 2013
• Short-term Evaluation of Combination Corticosteroid+Anti-VEGF Treatment for Persistent Central-Involved Diabetic Macular Edema Following Anti-VEGF Therapy in Pseudophakic Eyes
New Protocols New Protocols • Peripheral DR Lesions on Ultrawide-field Fundus Images and Risk of
DR Worsening Over Time• Short-term Evaluation of Using a Different Anti-VEGF Drug Compared
with Continuing on Bevacizumab in Eyes with Persistent Central-Involved Diabetic Macular Edema with Prior Bevacizumab Therapy
3434

Thank you for attending! Your feedback is very important. Scanning this QR code will take you
directly to the evaluation for this course.
Thank you for attending! Your feedback is very important. Scanning this QR code will take you
directly to the evaluation for this course.
3535
186: Update on Treatments for Diabetic Retinopathy: Clinically Relevant Results from the Diabetic Retinopathy Clinical
Research Network

















![The Guide - Diabetic Retinopathy - Vision Lossvisionloss.org.au/wp-content/uploads/2016/05/The... · the guide [diabetic retinopathy] What is Diabetic Retinopathy? Diabetic Retinopathy](https://img.pdfslide.us/doc/110x75/5e3ed00bf9c32e41ea6578a8/the-guide-diabetic-retinopathy-vision-the-guide-diabetic-retinopathy-what.jpg)