Embed Size (px)
Citation preview
THE CORE STUDY COMPARING TWO STRATEGIES FOR ENROLLING HIV-INFECTED PREGNANT WOMEN FROM ANTENATAL CARE TO CARE AND TREATMENT SERVICES IN CAMEROON: CONTINUUM OF CARE OPERATIONS RESEARCH (CORE) STUDY P Tih1, E Nshom1, E Onyoh1, C Harrington1, Z Fox2, J Nkfusai1, E Kuni1, E Mboh1,D Palmer1, T Welty1
1AIDS Care and Prevention Program, Cameroon Baptist Convention Health Board (CBCHB) North West Region, Cameroon; 2Research Department of Infection and Population Health, University College London, United Kingdom
1

Background2
The Cameroon Baptist Convention Health Board (CBCHB): Faith-based health-
focused organization Owns 5 hospitals and
25 integrated health centers
Operates in 6/10 regions of Cameroon
Supports services to prevent mother-to-child HIV transmission of HIV (PMTCT) in 450 sites

Background Continued3
Prior to 2007, single dose nevirapine was the most widely utilized PMTCT drug in Cameroon
In 2008, mother-to-child HIV transmission rates ranged between 13.8-14.5% in PMTCT facilities in Cameroon
In 2008, a lower level of vertical transmission was observed at CBCHB’s Care and Treatment centres (6.0-7.6%) when multi-drug ARV prophylaxis was initiated.
Challenge: Many women diagnosed with HIV at PMTCT sites do not comply with referral to C&T facilities

Objectives4
In January 2009, CBCHB initiated the CORE Study to investigate:1. The proportion of HIV-positive mothers enrolled
into C&T through two PMTCT-C&T referral systems
2. Uptake of combined antiretroviral therapy (i.e. multidrug ARV regimens containing SD-NVP+AZT and SD-NVP+AZT+3TC) for PMTCT was assessed
3. Vertical transmission rates according to the system of care used.
Ethical Issues5
CBCHB Institutional Review Board approved the study
Verbal informed consent was obtained prior to HIV testing Blood sample collection Home visitation

Methods6
PMTCT sites within 50km from each of the CBCHB’s five C&T centres located in five geographical areas (Banso, Mbingo, Bamenda, Mutengene and Douala) were placed in alphabetical order within each geographical area and assigned a number.
Odd-numbered sites were assigned to System I and even-numbered sites were assigned to System II
System I: Referred HIV-positive women from PMTCT sites to a C&T centre on the day of
HIV diagnosis. Linkage nurses followed up women who did not comply with enrolment at the
C&T centre, drew blood for CD4 testing and referred them again to a C&T centre, irrespective of the results of the CD4 test
System II: Referred HIV-positive women from PMTCT sites to a C&T centre depending on
the results of a CD4 test. Linkage nurses drew blood from HIV-positive women on the day of their HIV
diagnosis and transported it to the nearest C&T centre for CD4 testing. Women with CD4≤350 cells/mm3 were referred to a C&T centre for immediate
ART initiation whereas women with CD4>350 cells/mm3 were given bi-therapy at the PMTCT site, and recommended to enrol at C&T centre.

Methods Continued... 7
Data was collected from January 2009 to August 2010 Medians and interquartile ranges (IQRs) were calculated for
continuous variables and percentages for categorical variables respectively
Mixed effect models were used to: Compare baseline characteristics between the systems of care Compare the follow-up characteristics between the systems of care Estimate the adjusted odd ratios and 95% confidence intervals for
determinants of enrolment at C&T centre. The following factors were adjusted for in the multivariable model:
Category of CD4 count value, WHO stage, Travel time to care and treatment site, Possession of cell phone, Employment status, Gestation age and Maternal age.
Summary Results of CORE Study8
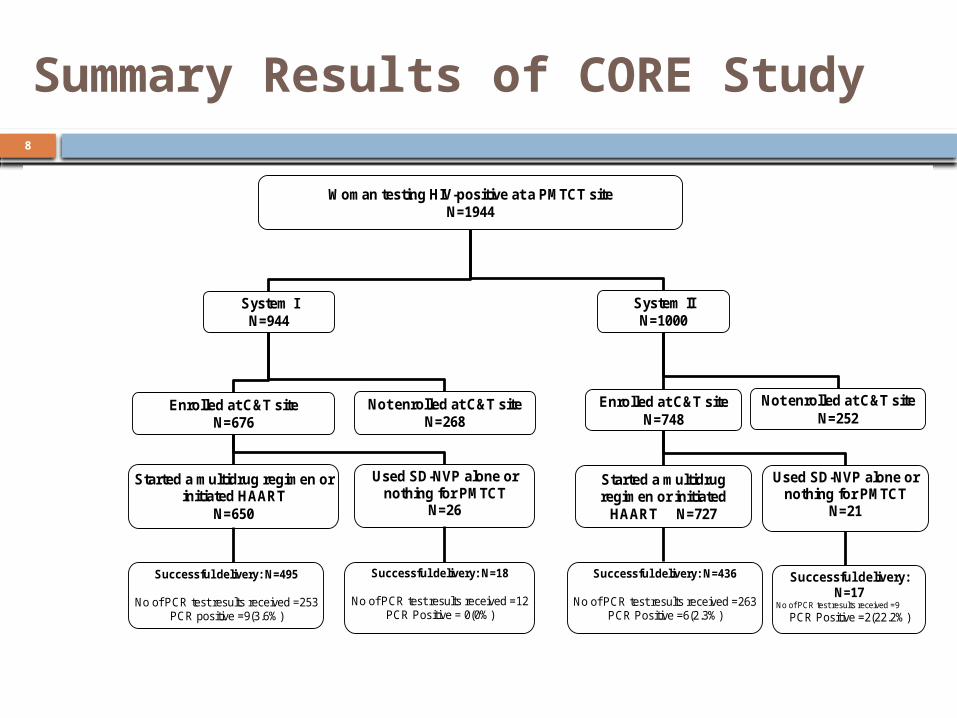
Woman testing HIV-positive at a PMTCT site N=1944
System I N=944
System II N=1000
Enrolled at C&T site N=676
Not enrolled at C&T site N=268
Started a multidrug regimen or initiated HAART
N=650
Used SD-NVP alone or nothing for PMTCT
N=26
Enrolled at C&T site N=748
Not enrolled at C&T site N=252
Successful delivery: N=495
No of PCR test results received =253 PCR positive =9(3.6%)
Successful delivery: N=18
No of PCR test results received =12 PCR Positive = 0(0%)
Started a multidrug regimen or initiated
HAART N=727
Used SD-NVP alone or nothing for PMTCT
N=21
Successful delivery: N=436
No of PCR test results received =263 PCR Positive =6(2.3%)
Successful delivery: N=17
No of PCR test results received =9
PCR Positive =2(22.2%)

Baseline Characteristics of Women Diagnosed HIV-positive at Antenatal Clinics
9
129 facilities (68 System I; 61 System II) HIV disease more advanced by WHO staging in
System II vs System I (p=0.03) CD4 results:
System I ≤350 36.1%; missing 9.2% System II ≤350 40.6%; missing 4.0% p value: 0.045 <0.001
No significant baseline differences between the two systems in: Maternal age Gestational age at first visit Employment status Owning a cell phone Time to C&T site

Treatment, prophylaxis and early infant diagnosis
10
Over 70% of mothers were enrolled in C&T (System I 71.6%, System II 74.8% p=0.97)
CD4 ≤ 350 in 38.5% overall of 699 tested Of those, 59.5 % in System I and 67.9 % in
System II were on HAART (p=0.02) More of System I women than System II had
missing data on prophylaxis/treatment (22.0% vs 16.8% p=0.001)
Of the 849 live born babies, 85% received AZT/NVP prophylaxis with similar rates in both systems.
Of 515 babies tested by PCR, 9 System I babies (3.5%) vs 7 System II babies (2.7%) were positive (p=0.60)

Determinants for Enrollment in Care and Treatment
11
System of care not significant predictor of enrollment
Women with WHO stages III or IV were 2.6 times more likely to be enrolled than those with Stages I or II (p=0.02)
The longer the travel time, the lower the enrollment rate
Women who had cell phones were 2.3 times more likely to be enrolled than those without (p<0.01)
Employed women were 1.4 times more likely to be enrolled than unemployed women (p=0.01)

Pregnant Women listening to ANC Lecture
12
Pregnant Women listening to ANC Lecture
13

Challenges/Study Limitations
14
Transport cost for staff and patient movement between PMTCT and C&T sites
Many staff needed to reinforce referral Refusal to participate (clients & PMTCT
sites) High rates of missing data for
prophylaxis and treatment regimens Lack of funding to follow up all women
and their babies after delivery

Conclusion15
Overall, over 70% of HIV-positive mothers were enrolled into C&T (71.6% in system I and 74.8% in system II p=0.97)
Of the women with CD4 ≤350, 59.5% of System I and 67.9% of System II were on HAART (p=0.02)
Vertical transmission rates were 3.5% in System I and 2.7% in System II (p=0.60)
In System II, women had blood drawn at first ANC and were sent to referral labs for testing. This strategy resulted in significantly more women having CD4 test results, and higher proportion of those with CD4 ≤350 on HAART
The use of referral staff to promote PMTCT-C&T linkages and to provide optimal PMTCT prophylaxis is feasible.

Acknowledgements
Elizabeth Glaser Pediatric AIDS Foundation (EGPAF)
Ministry of Public Health Cameroon University of North Carolina HIV Research Trust HIV-Positive mothers who participated Staff at C&T facilities PMTCT staff at all participating facilities Regional AIDS coordinators, North West,
South West and Littoral Regions
16