Embed Size (px)
Citation preview
The Conservative Management of Chronic Kidney Disease
Panduranga S Rao MD DNB MSAssociate Professor,
Division of NephrologyDepartment of Medicine
University of Michigan
1
Definition of Chronic Kidney Disease
• Kidney damage for >3 months with or without decreased glomerular filtration rate as manifest by:
Markers of kidney damage including abnormalities in the composition of blood or urine or imaging
2
What is the extent of the problem?
3
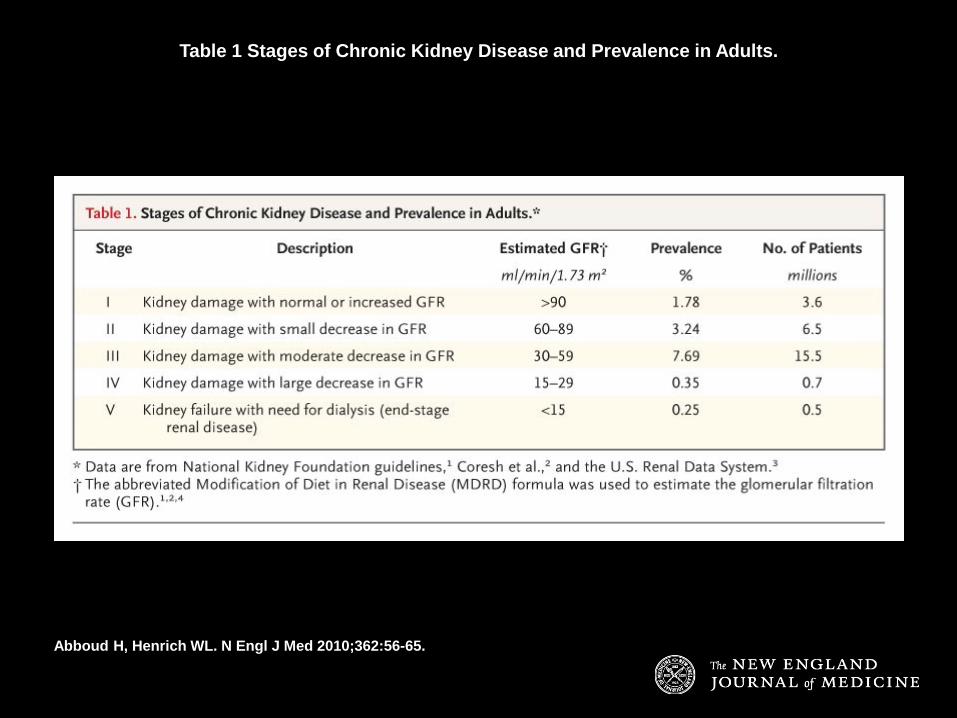
Table 1 Stages of Chronic Kidney Disease and Prevalence in Adults.
Abboud H, Henrich WL. N Engl J Med 2010;362:56-65.

So why worry?
5
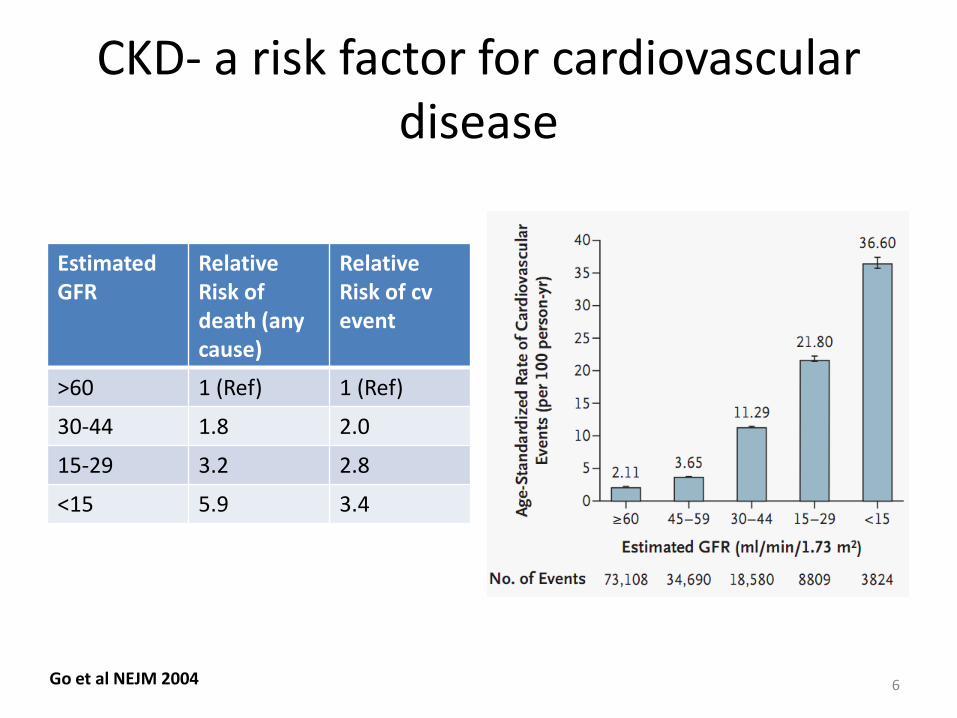
CKD- a risk factor for cardiovascular disease
Estimated GFR
Relative Risk of death (any cause)
Relative Risk of cvevent
>60 1 (Ref) 1 (Ref)
30-44 1.8 2.0
15-29 3.2 2.8
<15 5.9 3.4
Go et al NEJM 2004 6
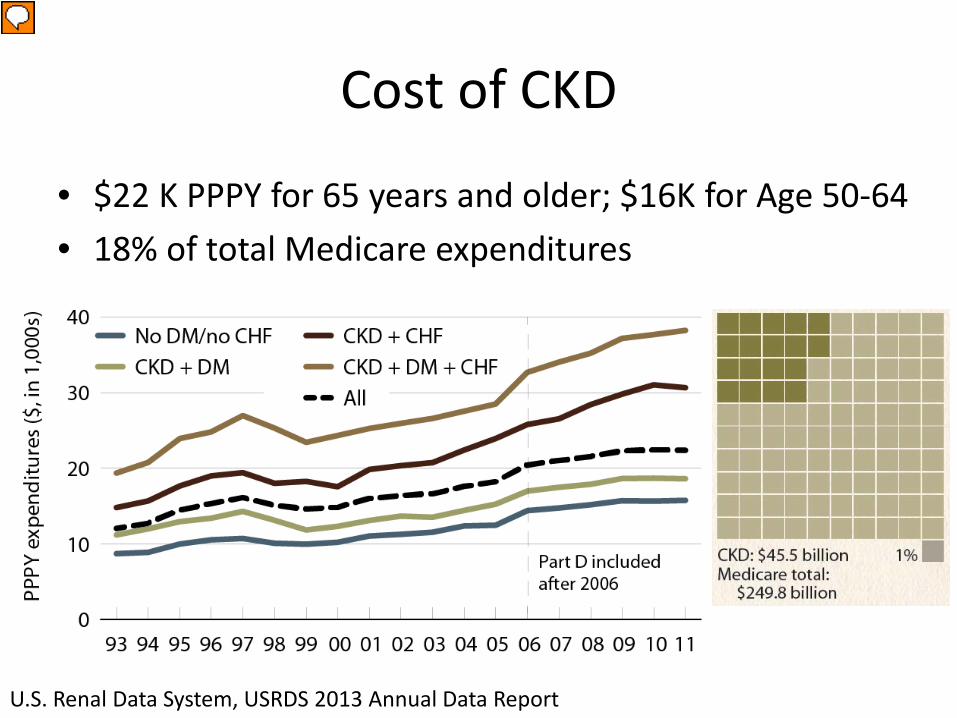
Cost of CKD
• $22 K PPPY for 65 years and older; $16K for Age 50-64• 18% of total Medicare expenditures
U.S. Renal Data System, USRDS 2013 Annual Data Report
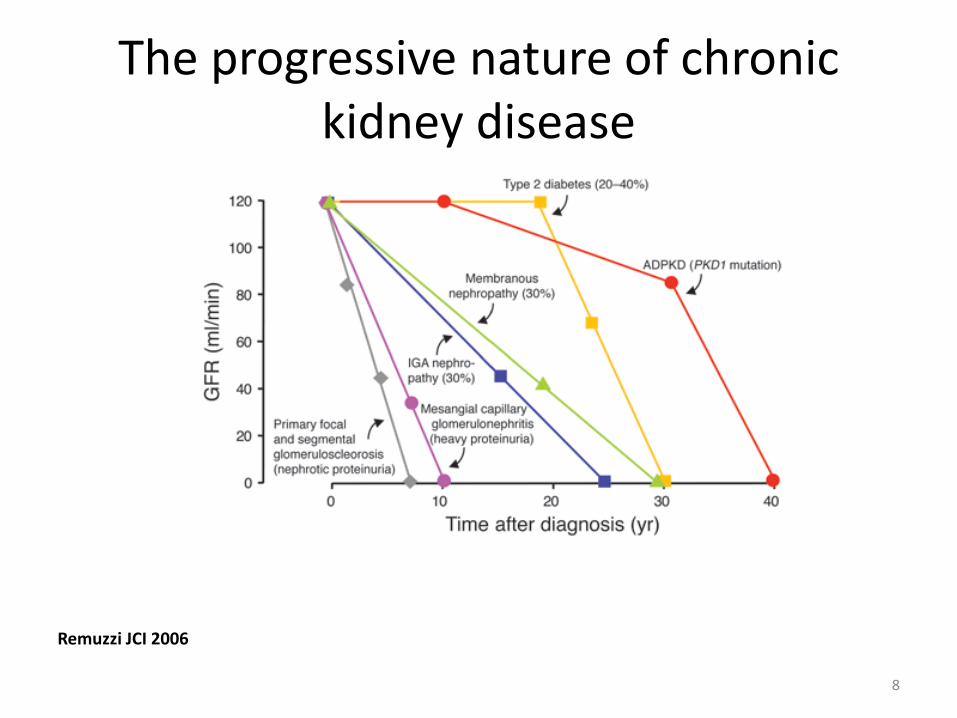
The progressive nature of chronic kidney disease
Remuzzi JCI 2006
8
ATTEMPTS AT SLOWING THE PROGRESSION OF KIDNEY DISEASE IS A WORTHY GOAL
Prevention is key, but failing that…….
9
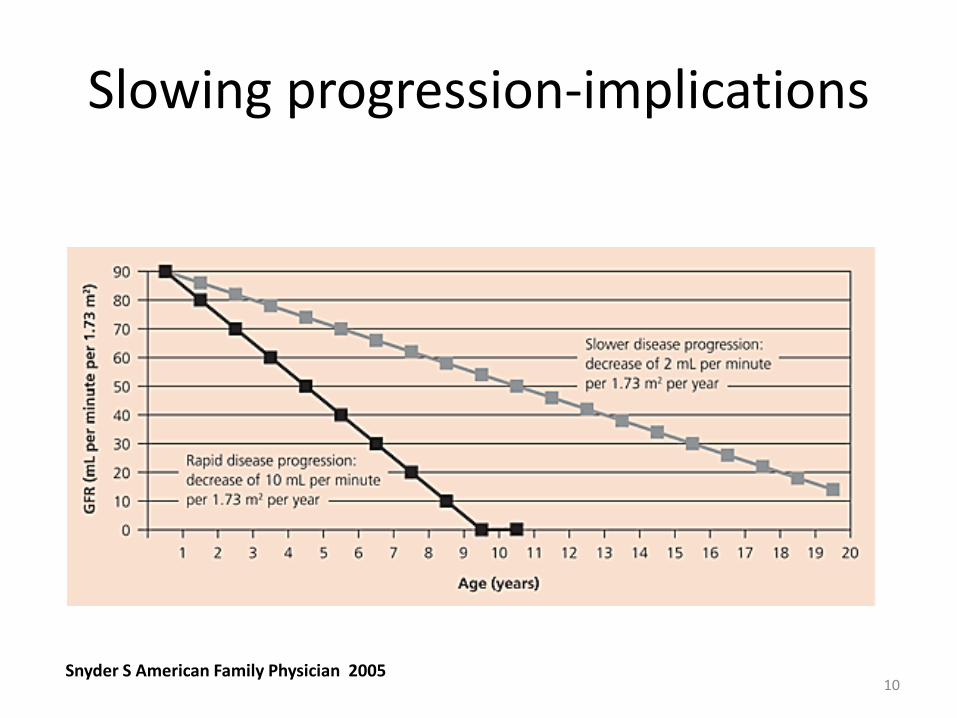
Slowing progression-implications
Snyder S American Family Physician 200510
What does CKD progress?
…and how is it relevant in day to day practice?
11
HYPERFILTRATION
• When the nephron numbers are reduced, the remaining nephrons ‘hyperfilter.’
• An important mediator is Angiotensin 2.
12
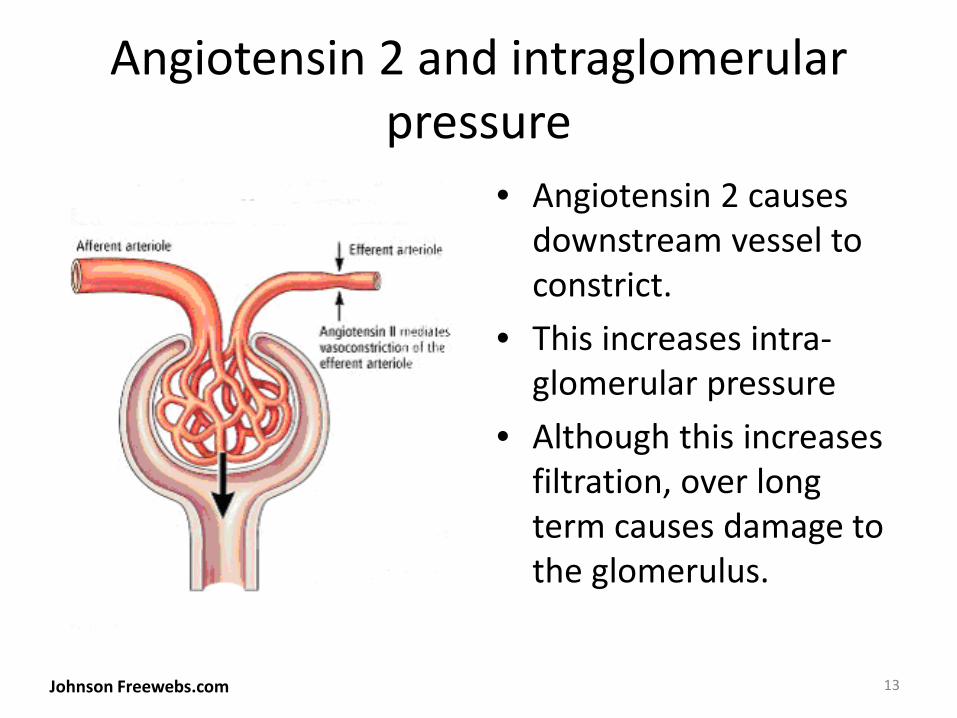
Angiotensin 2 and intraglomerularpressure
• Angiotensin 2 causes downstream vessel to constrict.
• This increases intra-glomerular pressure
• Although this increases filtration, over long term causes damage to the glomerulus.
Johnson Freewebs.com 13
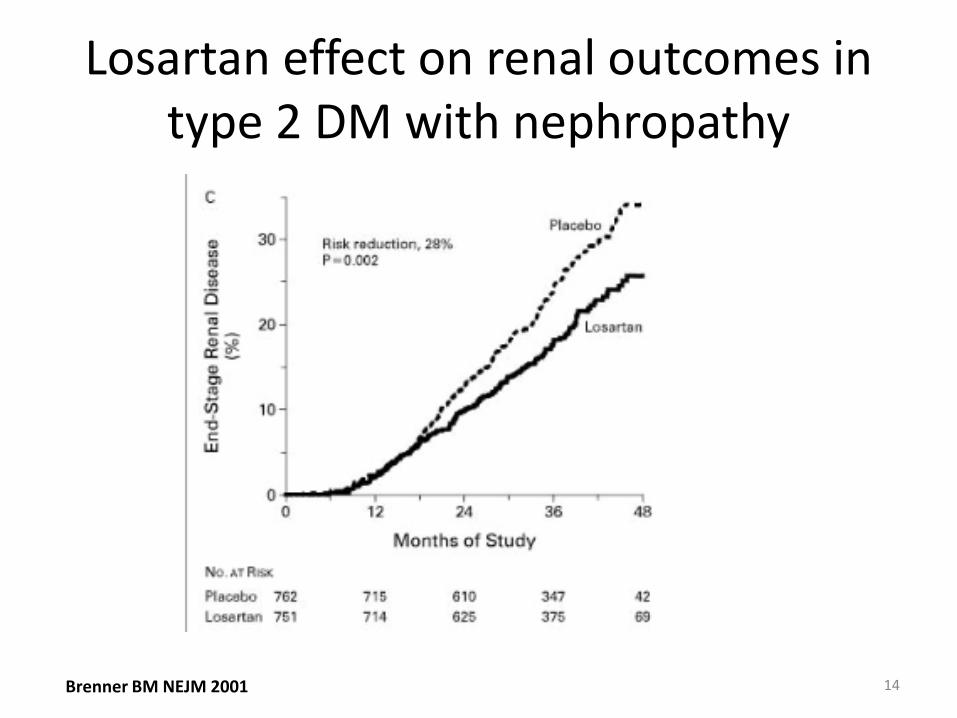
Losartan effect on renal outcomes in type 2 DM with nephropathy
Brenner BM NEJM 2001 14
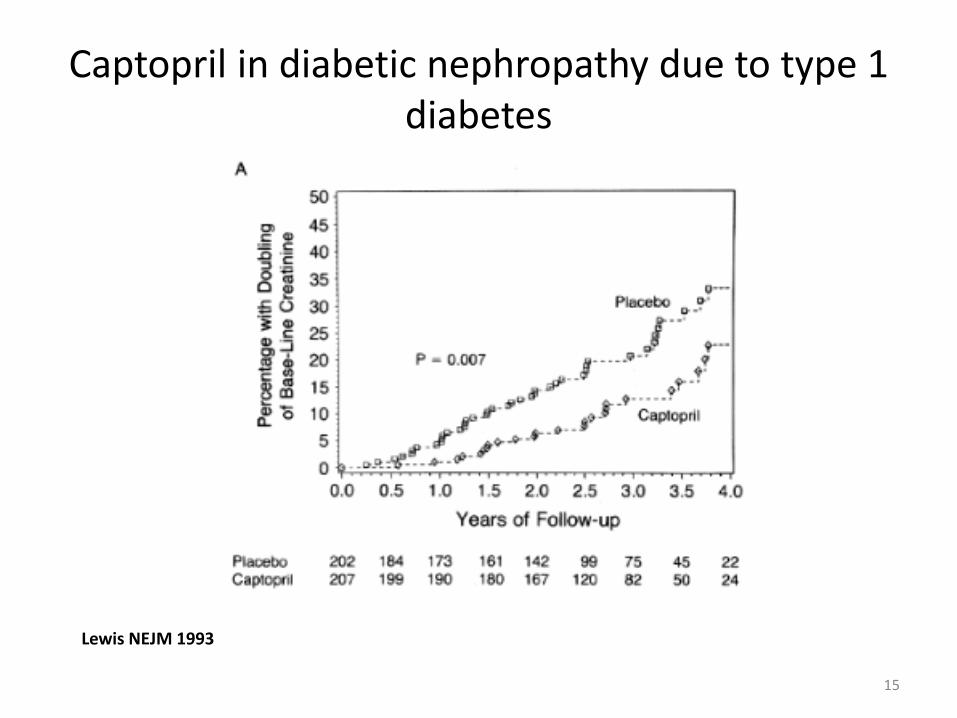
Captopril in diabetic nephropathy due to type 1 diabetes
Lewis NEJM 1993
15
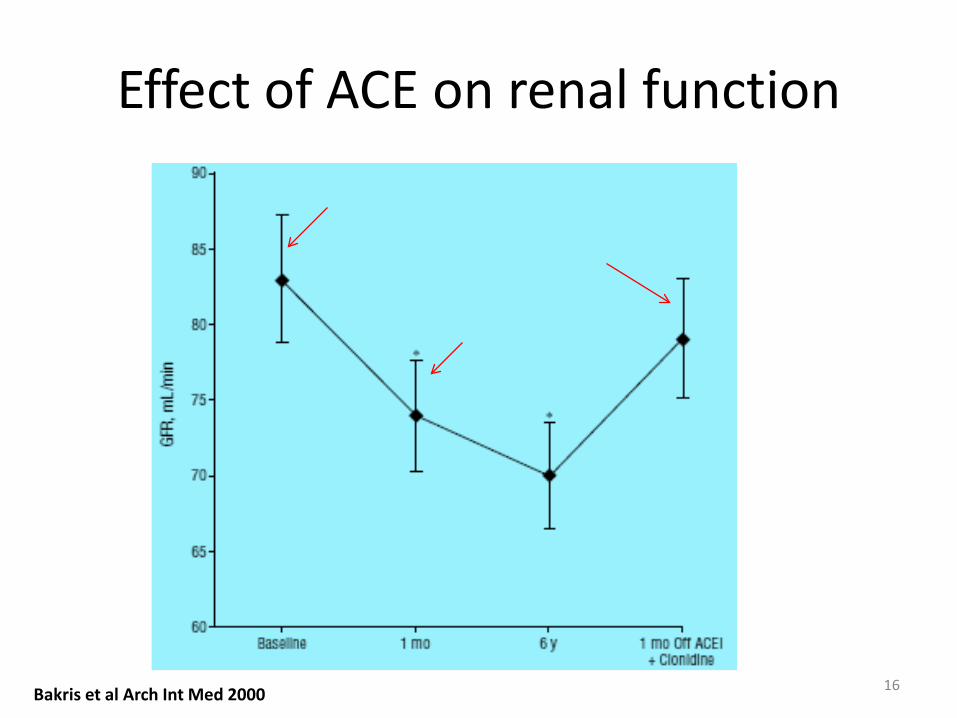
Effect of ACE on renal function
Bakris et al Arch Int Med 2000 16
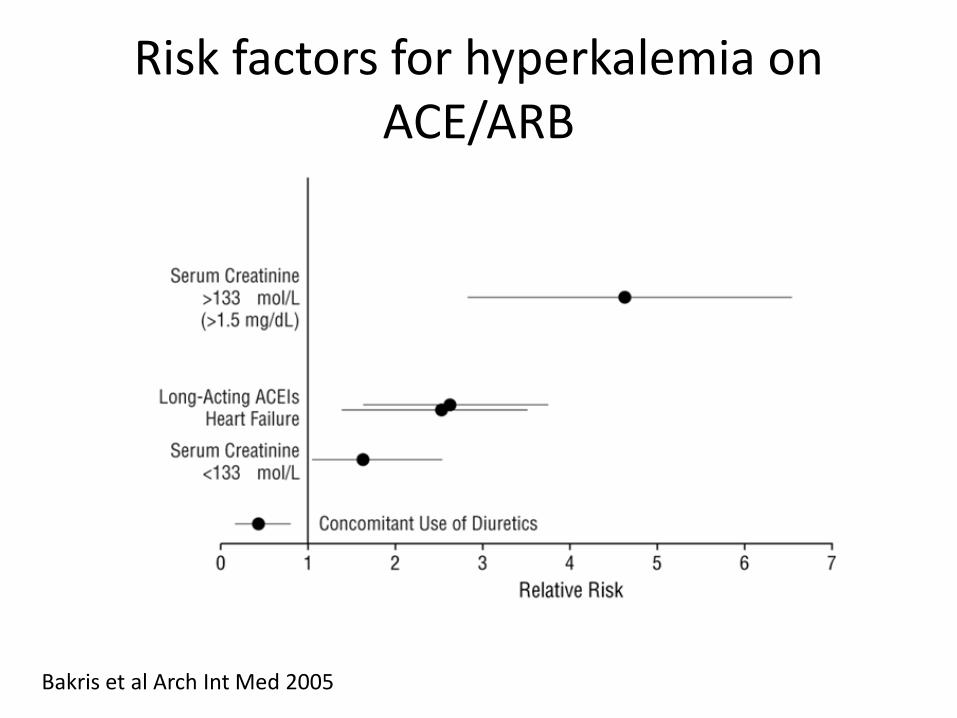
Risk factors for hyperkalemia on ACE/ARB
Bakris et al Arch Int Med 2005
Management
• Review diet, if persisting problem get dietary input
• Beware of salt substitute!• Review drugs ( look for NASIDS)• Diuretics
18
A LOT OF k!
Can 1+ 1=3?
If ACE works well and ARB works well, would ACE+ ARB work even
better?
19
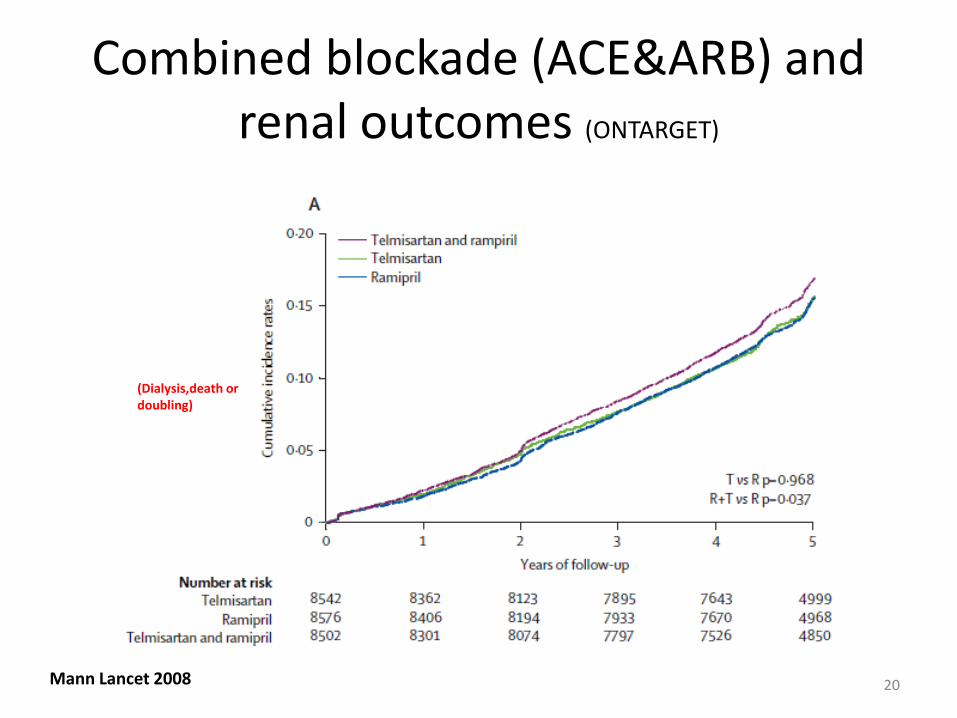
Combined blockade (ACE&ARB) and renal outcomes (ONTARGET)
Mann Lancet 2008 20
(Dialysis,death or doubling)
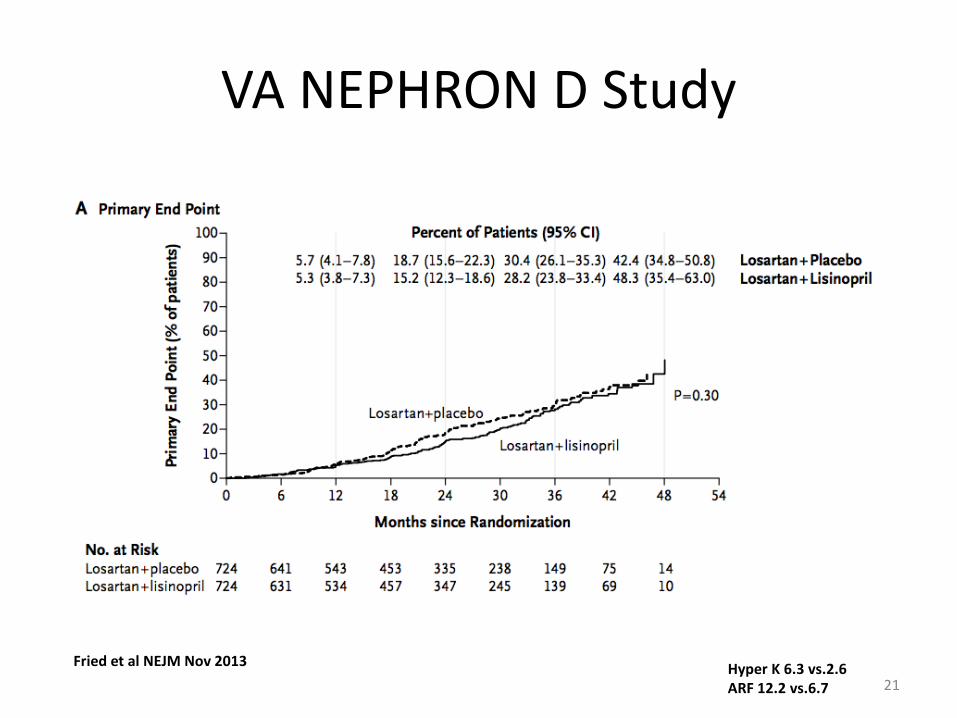
VA NEPHRON D Study
21Fried et al NEJM Nov 2013 Hyper K 6.3 vs.2.6
ARF 12.2 vs.6.7
Role of proteinuria
Why is control important?
22
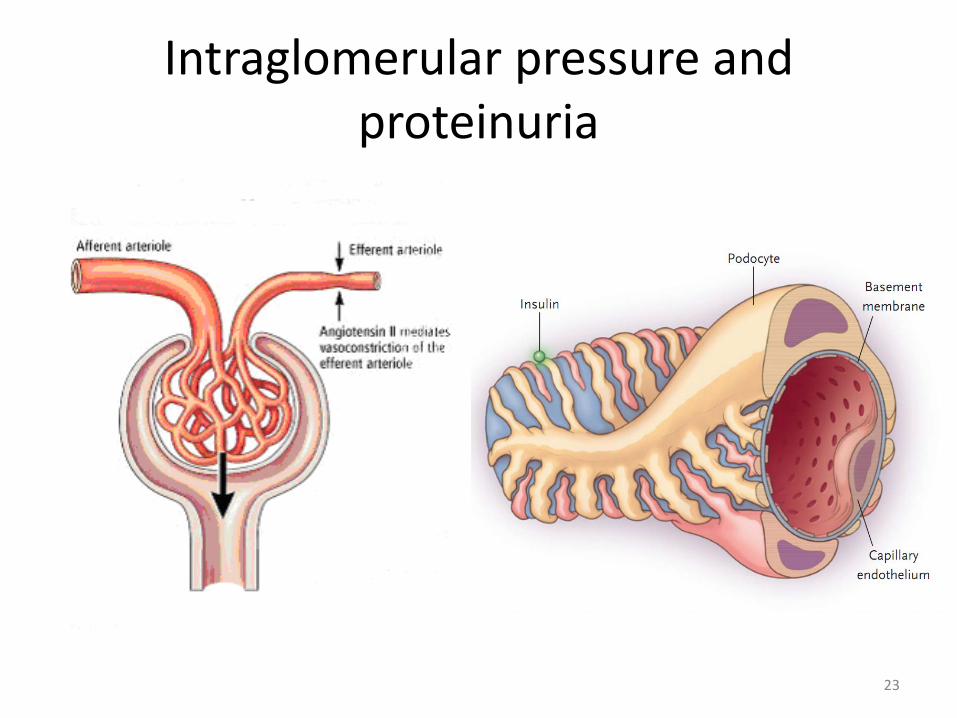
Intraglomerular pressure and proteinuria
23
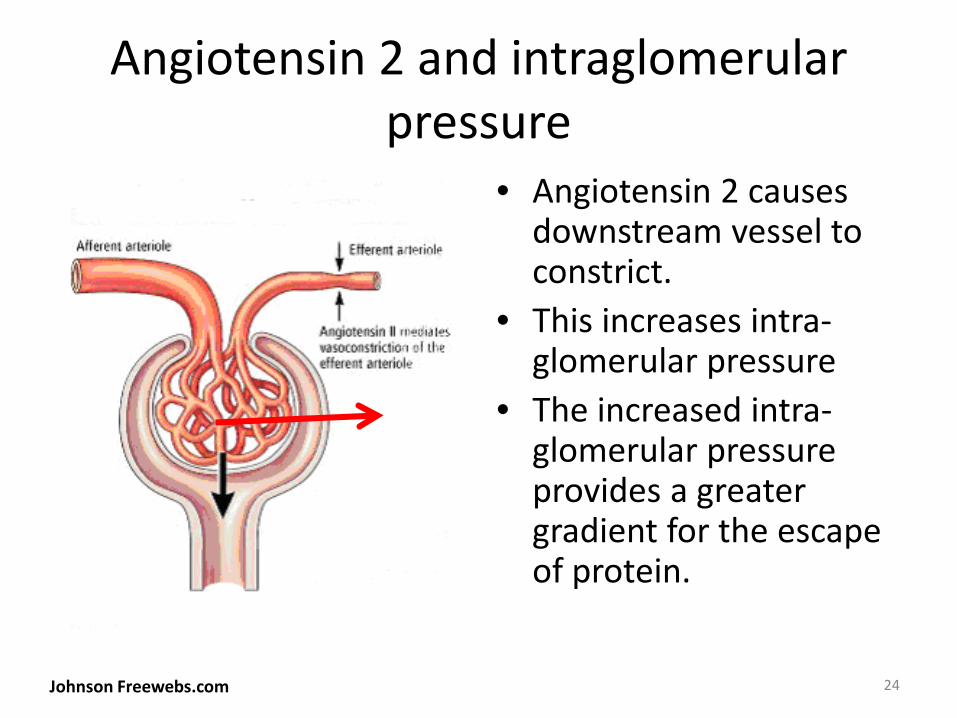
Angiotensin 2 and intraglomerularpressure
• Angiotensin 2 causes downstream vessel to constrict.
• This increases intra-glomerular pressure
• The increased intra-glomerular pressure provides a greater gradient for the escape of protein.
Johnson Freewebs.com 24
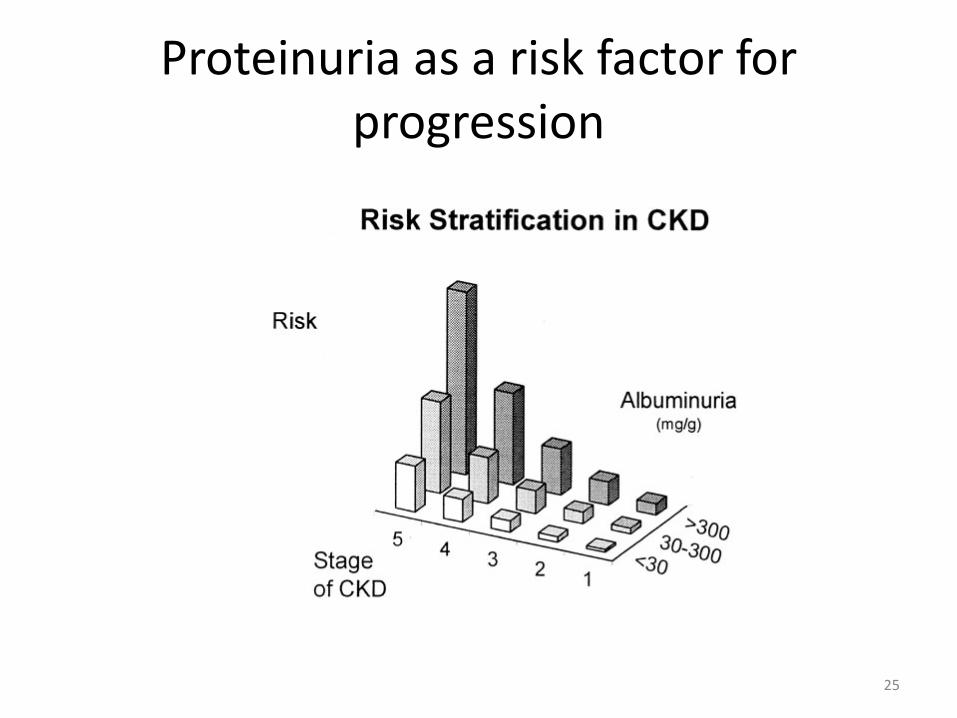
Proteinuria as a risk factor for progression
25
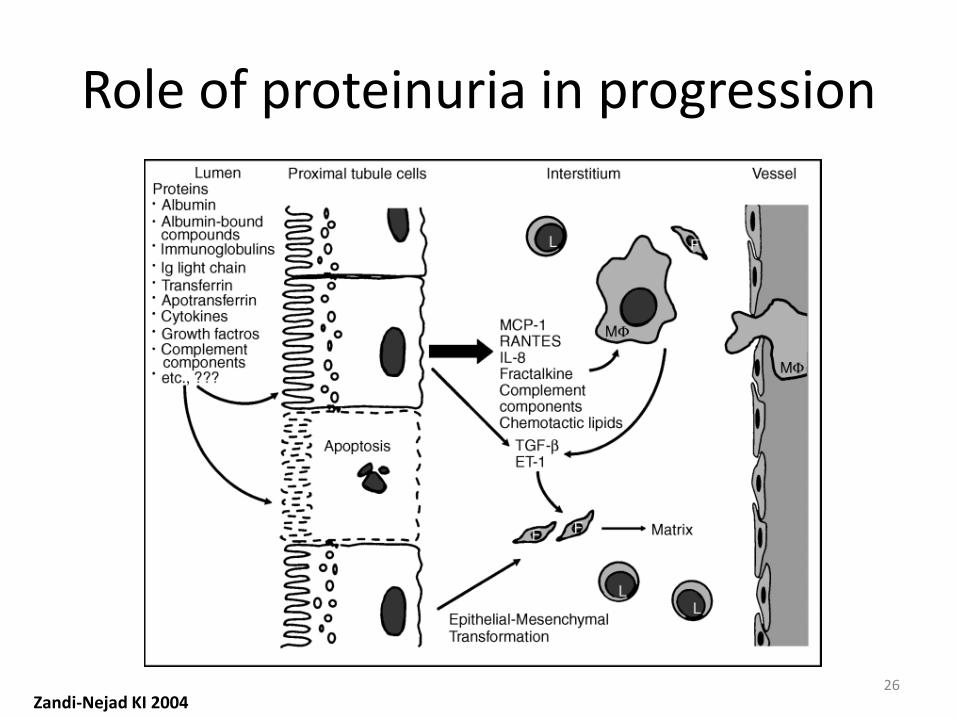
Role of proteinuria in progression
Zandi-Nejad KI 200426
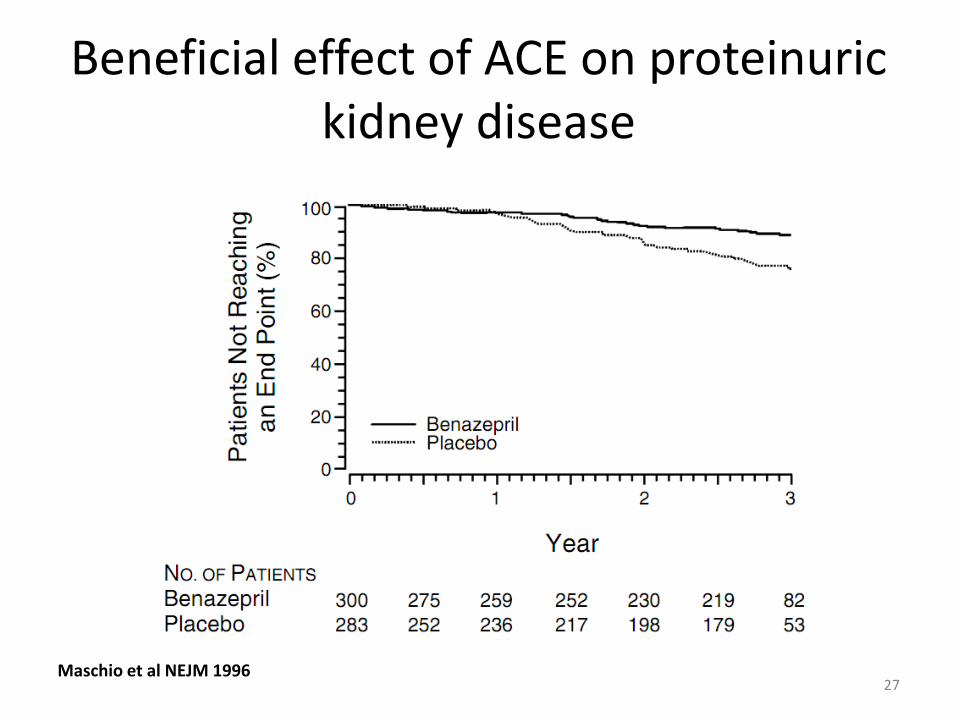
Beneficial effect of ACE on proteinurickidney disease
Maschio et al NEJM 199627
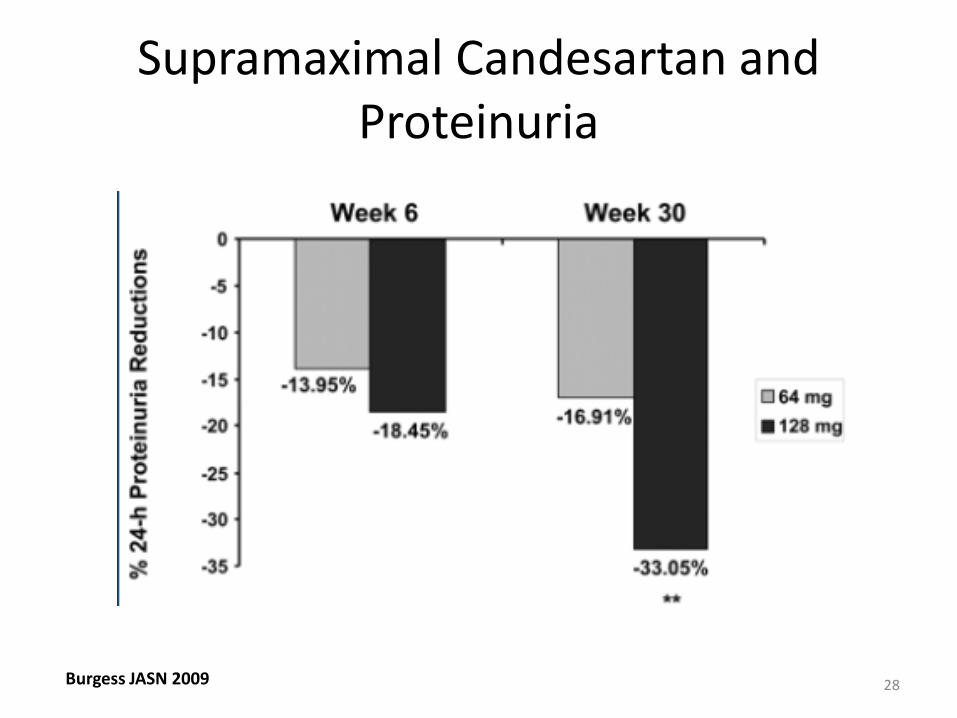
Supramaximal Candesartan and Proteinuria
Burgess JASN 2009 28
Insult to injury (or injury to insult?)
Blood pressure control and progression of kidney disease
29
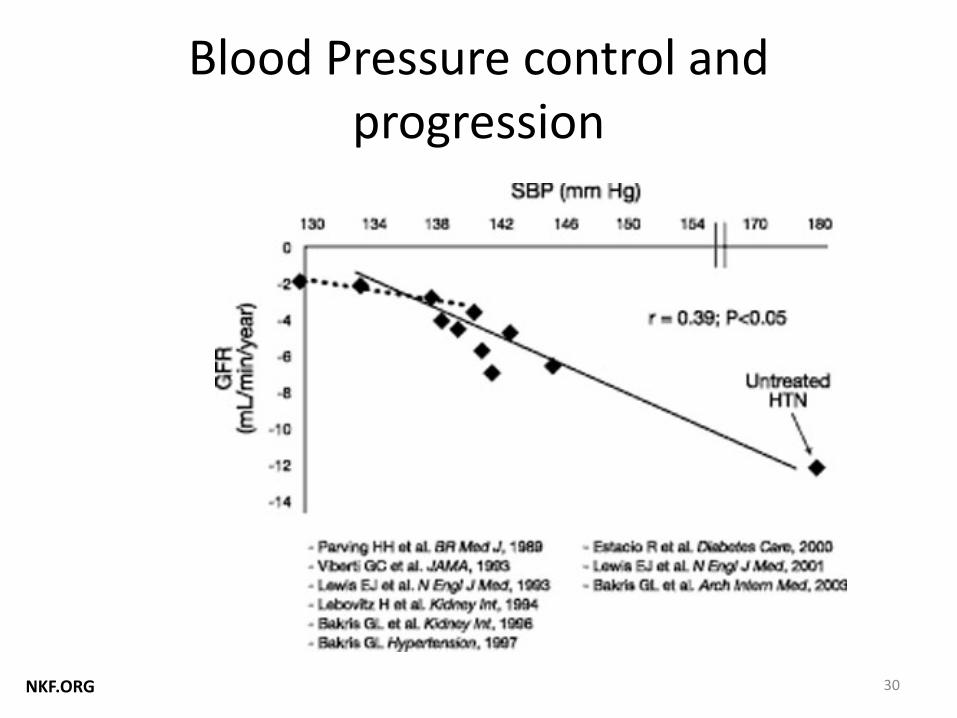
Blood Pressure control and progression
NKF.ORG 30
Hypertension
• Unclear whether <130/80 slows progression of CKD compared with < 140/90 – Especially in patients with protein < 300 mg/day
• SPRINT: RCT comparing <120 vs. <140 in delaying progression of CKD in patients age > 50 years.
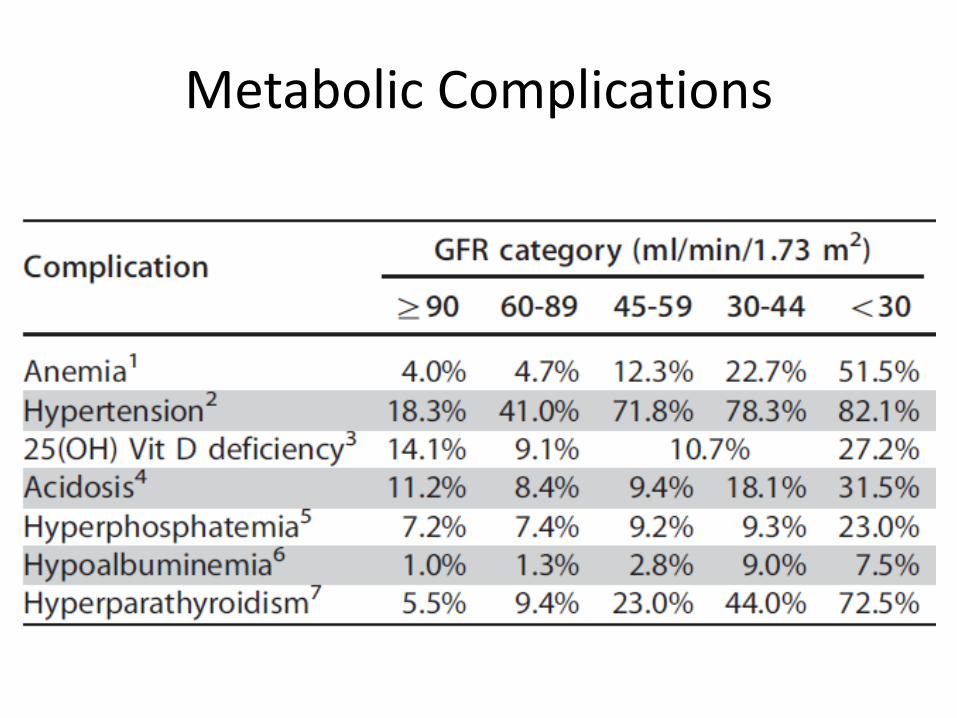
Metabolic Complications
Other issues
• Lipids• Control of diabetes • Salt and water retention• Obesity• Smoking
33
ANEMIA MANAGEMENT IN CKDWITH EPO
Too much of a good thing?
34
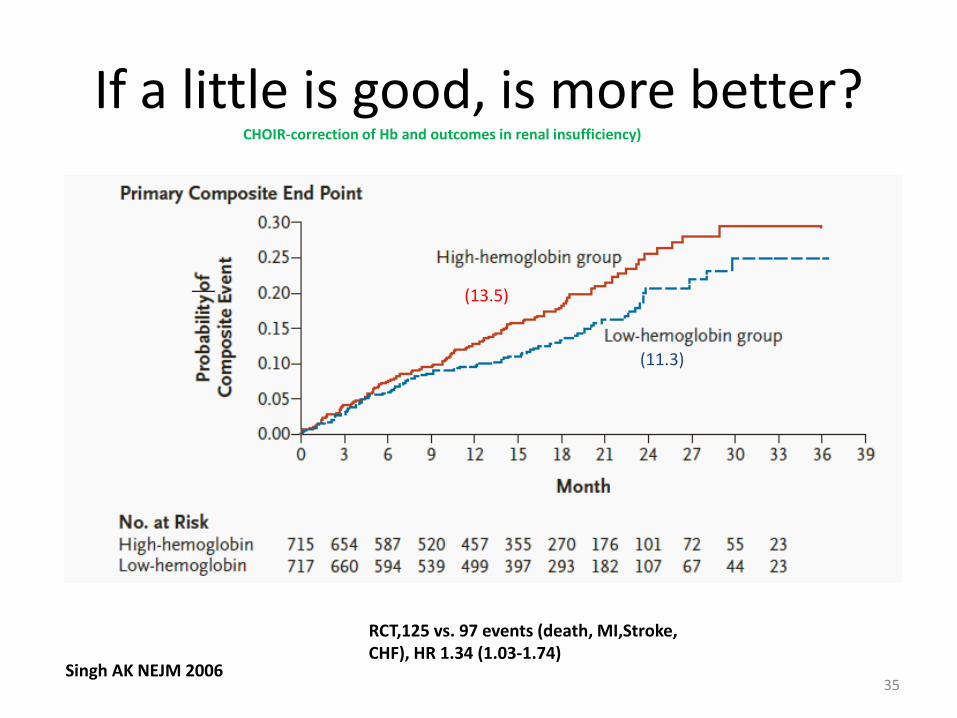
If a little is good, is more better?
35Singh AK NEJM 2006
(13.5)
(11.3)
RCT,125 vs. 97 events (death, MI,Stroke, CHF), HR 1.34 (1.03-1.74)
CHOIR-correction of Hb and outcomes in renal insufficiency)
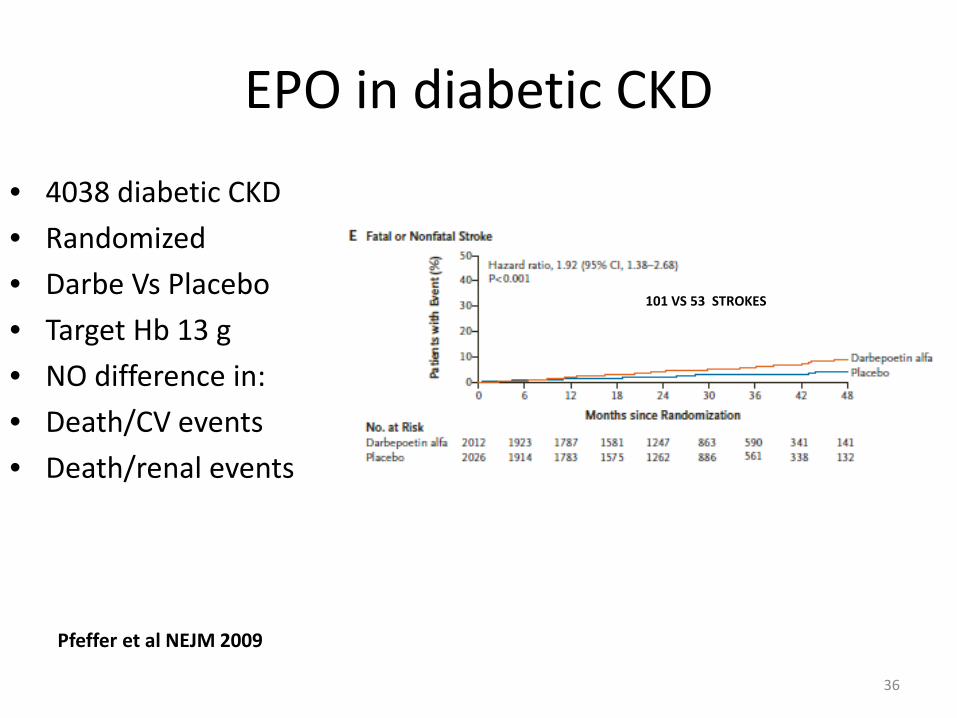
EPO in diabetic CKD
36
• 4038 diabetic CKD• Randomized• Darbe Vs Placebo• Target Hb 13 g• NO difference in:• Death/CV events• Death/renal events
Pfeffer et al NEJM 2009
101 VS 53 STROKES
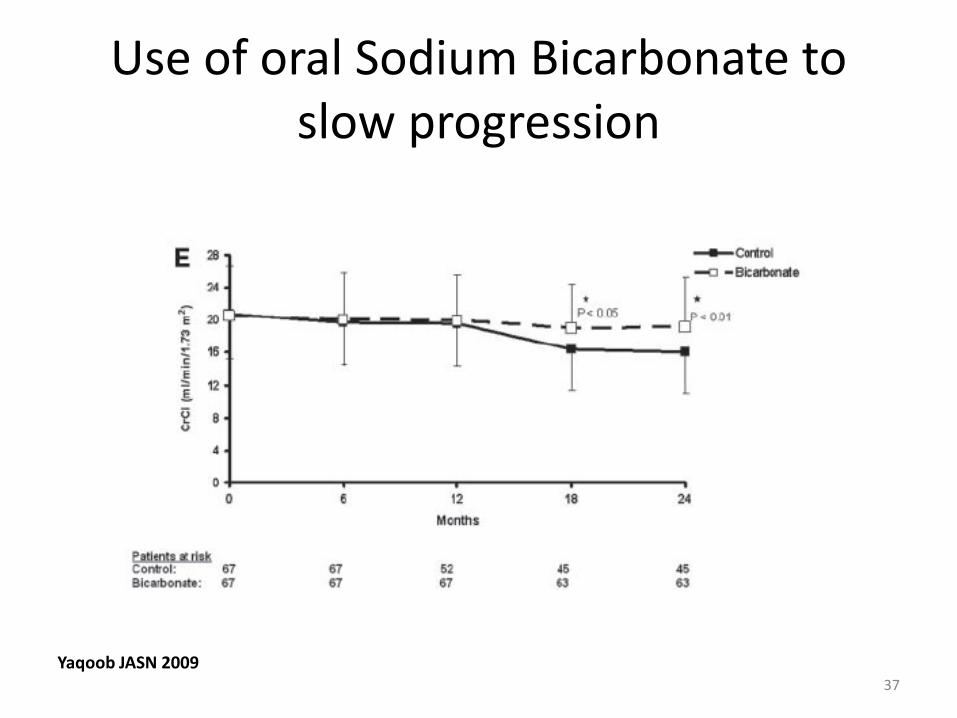
Use of oral Sodium Bicarbonate to slow progression
Yaqoob JASN 200937
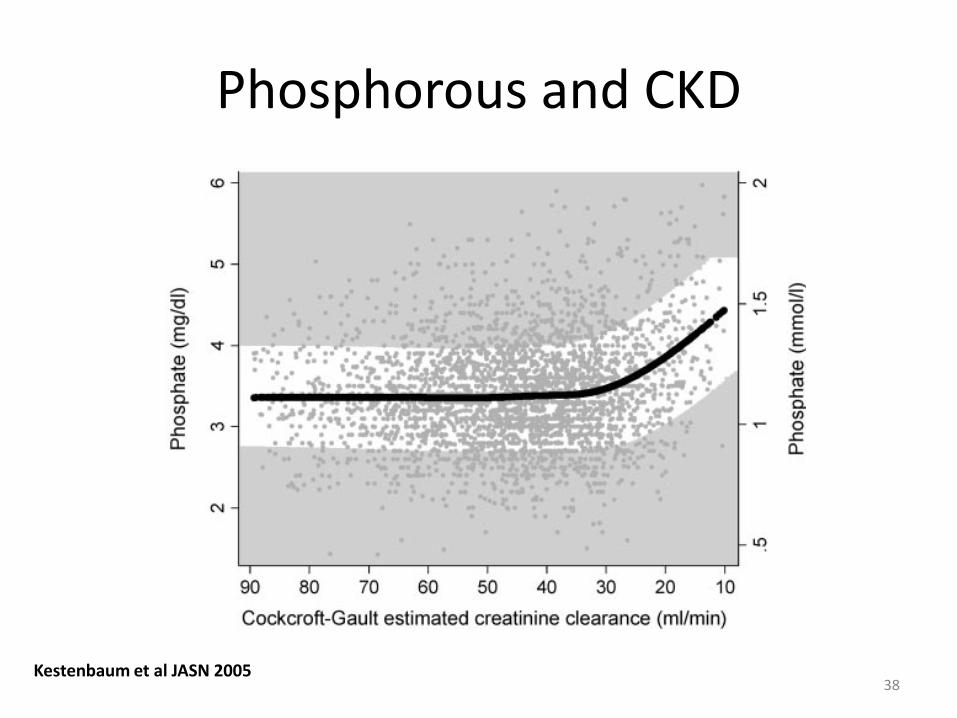
Phosphorous and CKD
38Kestenbaum et al JASN 2005
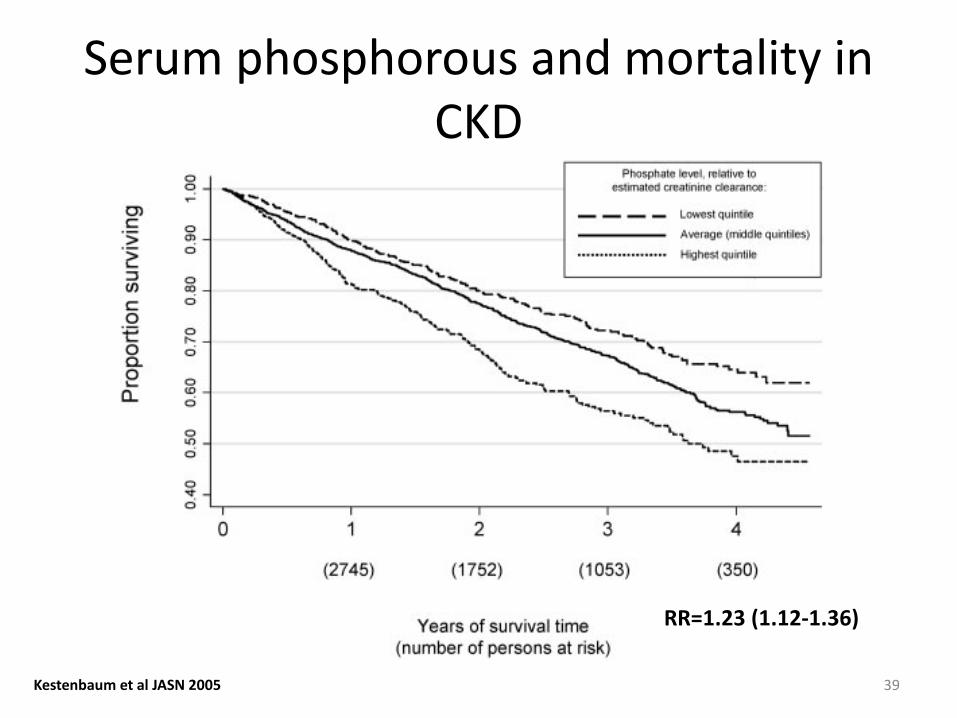
Serum phosphorous and mortality in CKD
39Kestenbaum et al JASN 2005
RR=1.23 (1.12-1.36)
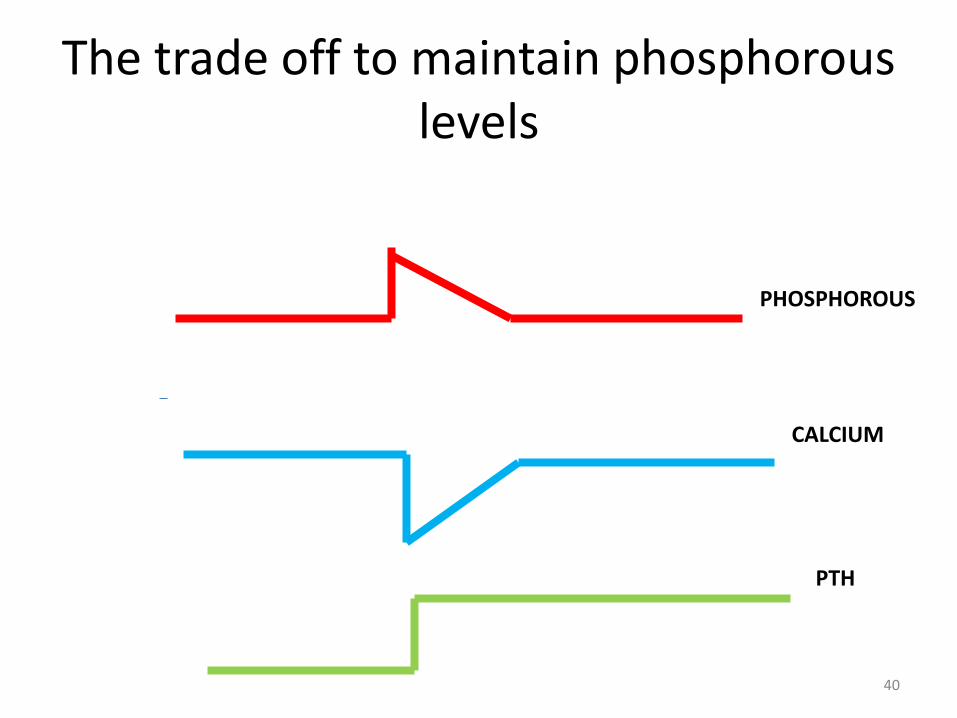
The trade off to maintain phosphorous levels
40
PTH
CALCIUM
PHOSPHOROUS
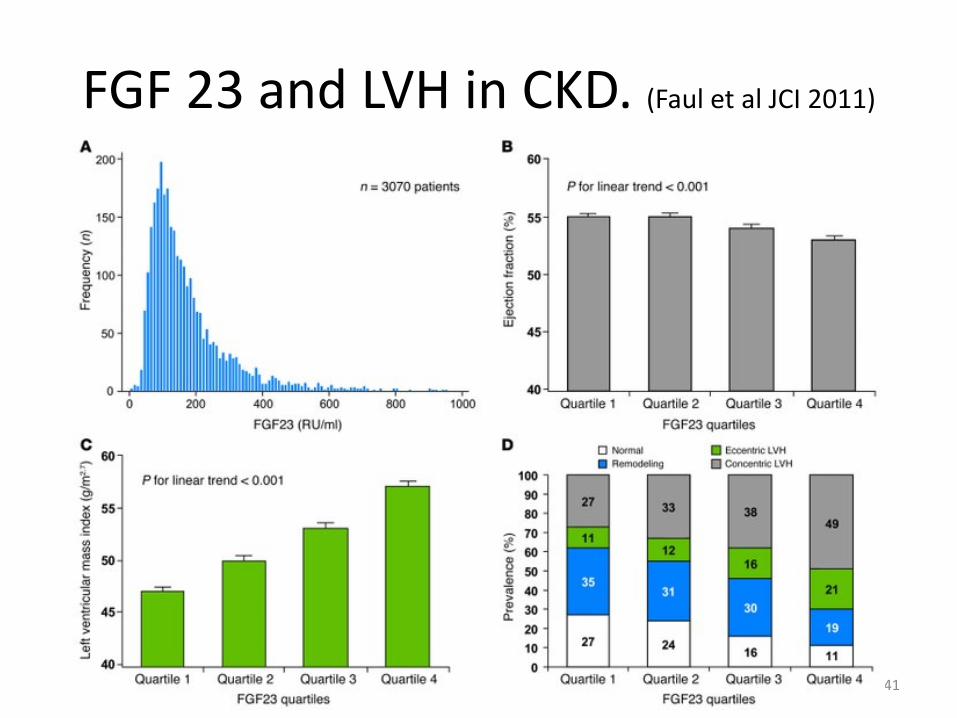
FGF 23 and LVH in CKD. (Faul et al JCI 2011)
41
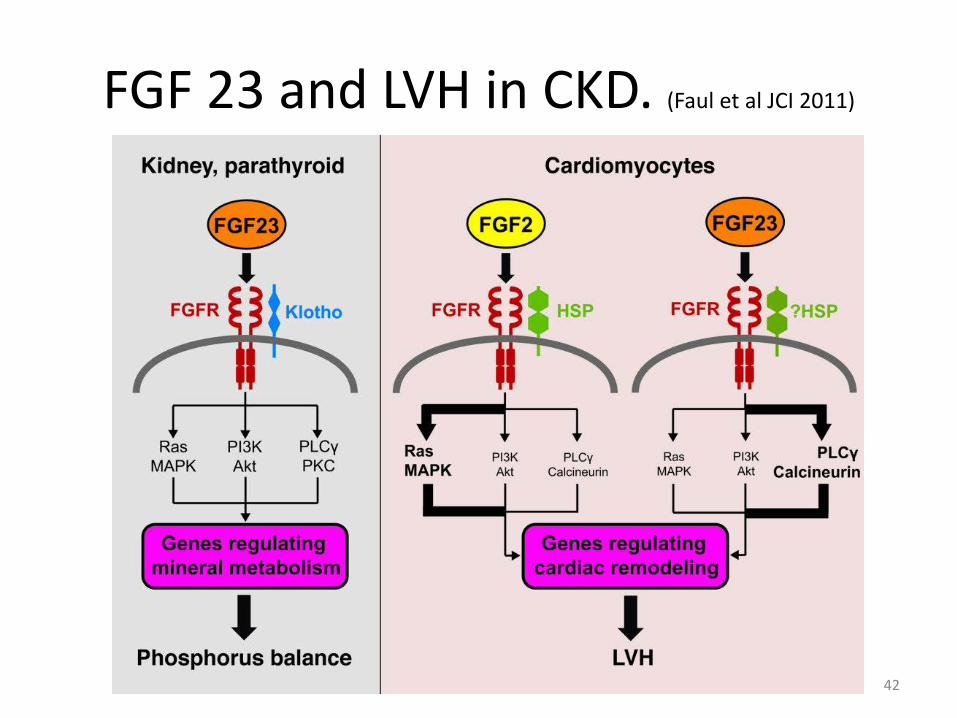
FGF 23 and LVH in CKD. (Faul et al JCI 2011)
42
Control of phosphorous
• Diet ( protein is the most important source). Watch out for processed food, cola products
Phosphorous binders (with food!)• Aluminum hydroxide• Ca carbonate or acetate• Sevelamer carbonate• Lanthanum
43
CONTROL OF AN IMPORTANT CV RISK FACTOR-LIPIDS
If statins are is good for everybody, is it good for everybody with Chronic Kidney Disease?
44
0 1 2 3 4 5 Years of follow-up
0
5
10
15
20
25
Prop
ortio
n su
fferin
g ev
ent (
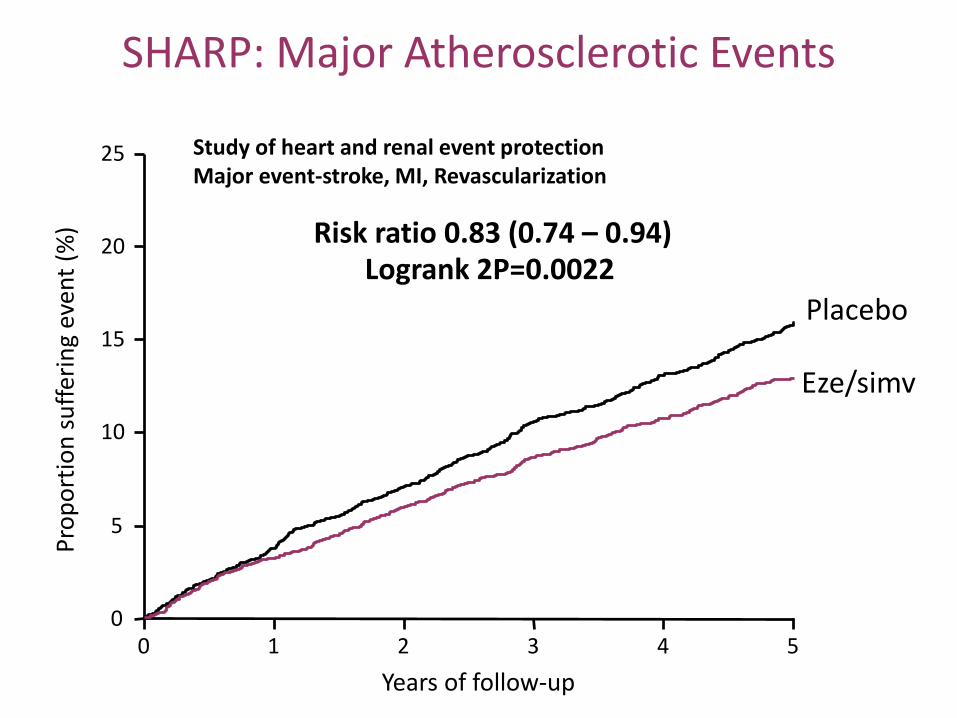
%) Risk ratio 0.83 (0.74 – 0.94)
Logrank 2P=0.0022 Placebo
Eze/simv
SHARP: Major Atherosclerotic Events
Study of heart and renal event protectionMajor event-stroke, MI, Revascularization
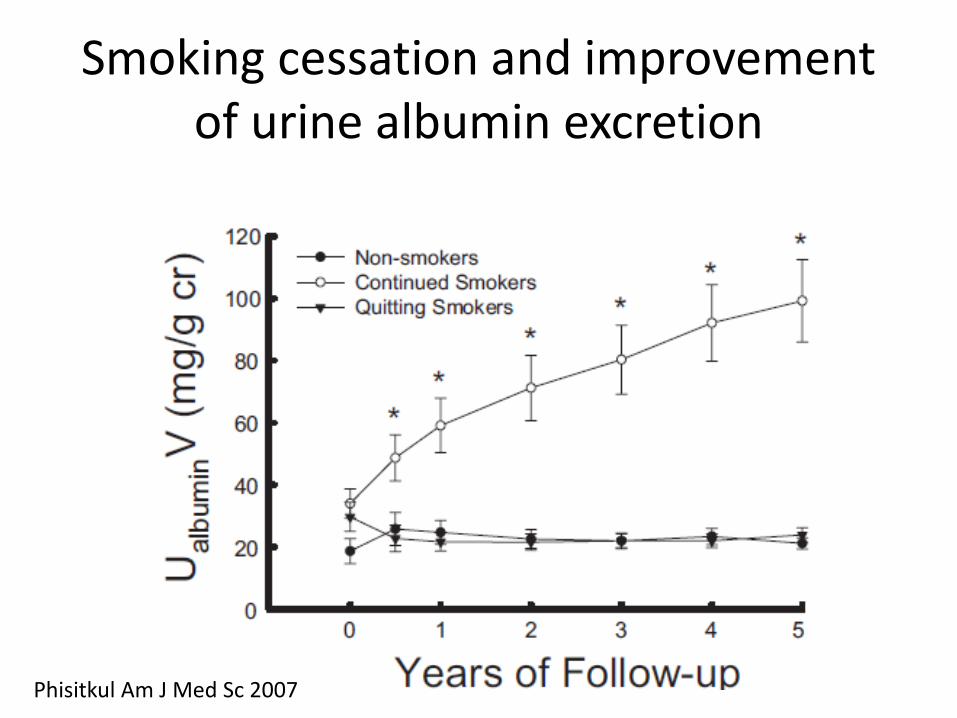
Smoking cessation and improvement of urine albumin excretion
Phisitkul Am J Med Sc 2007
Salt
• Volume management critical• Likely contributes to high CV morbidity• Edema and high blood pressure dictates need
for salt restriction• Emphasize of avoiding processed foods.• Remember it is the salt which is the culprit,
not the water!
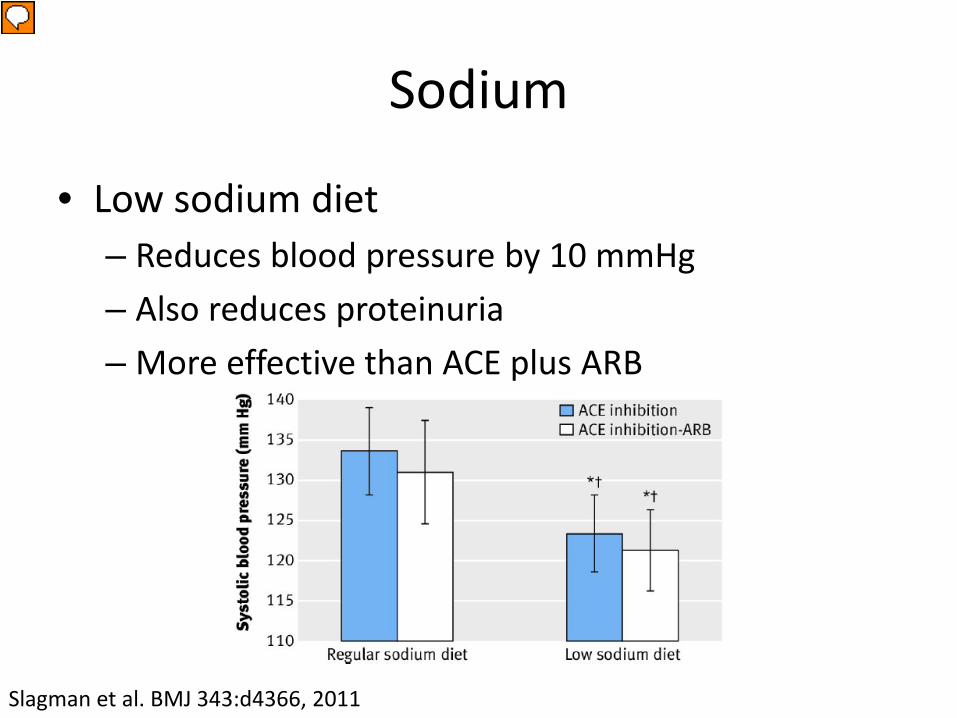
Sodium
• Low sodium diet– Reduces blood pressure by 10 mmHg – Also reduces proteinuria– More effective than ACE plus ARB
Slagman et al. BMJ 343:d4366, 2011
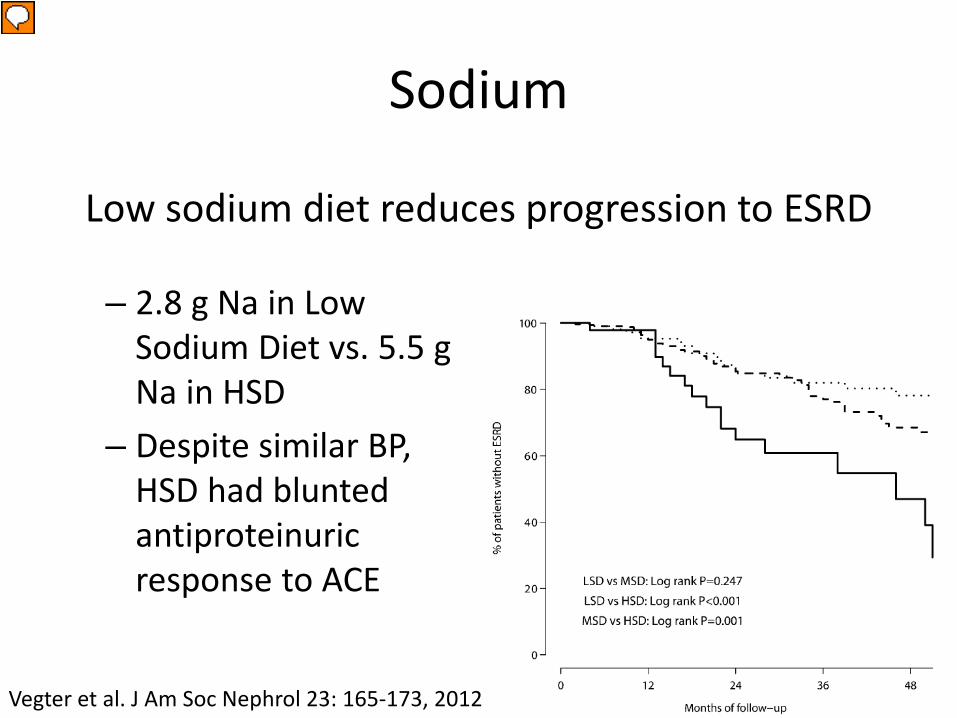
Sodium
– 2.8 g Na in Low Sodium Diet vs. 5.5 g Na in HSD
– Despite similar BP, HSD had blunted antiproteinuricresponse to ACE
Vegter et al. J Am Soc Nephrol 23: 165-173, 2012
Low sodium diet reduces progression to ESRD
Protein Intake
• Quantity– Low protein diet may slow progression of CKD– 0.7 g/kg/day: 86 kg = 60 grams = 2 oz!
• Source– Vegetable sources of protein
• Decreased production of uremic toxins: p-cresyl sulfate and indoxyl sulfate (implicated in progression)
• Low in phosphorus• Lower endogenous acid production
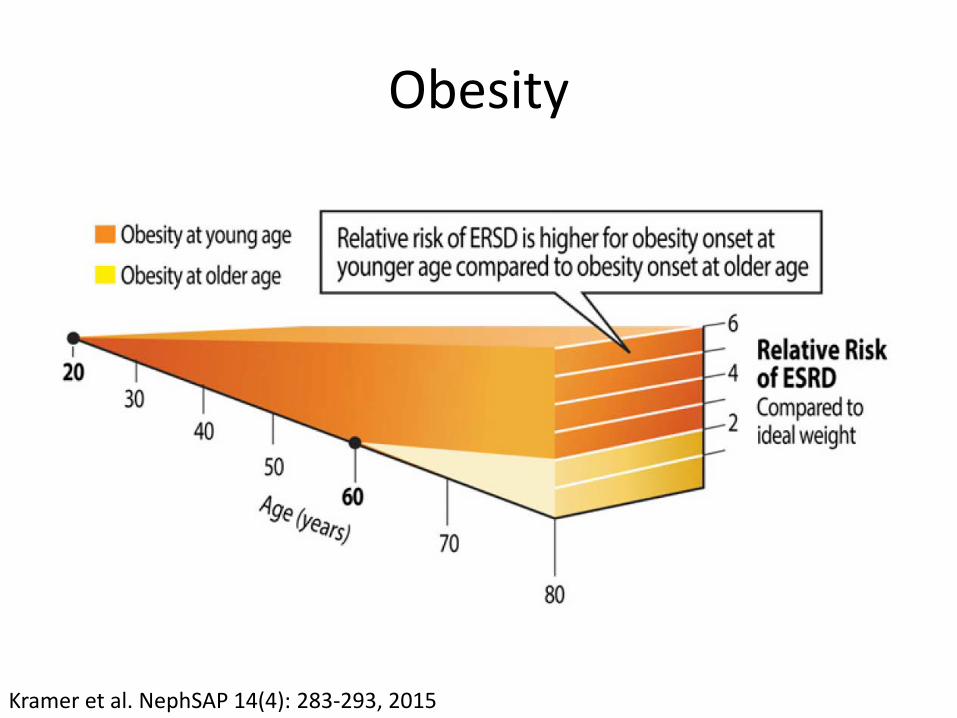
Obesity
Kramer et al. NephSAP 14(4): 283-293, 2015
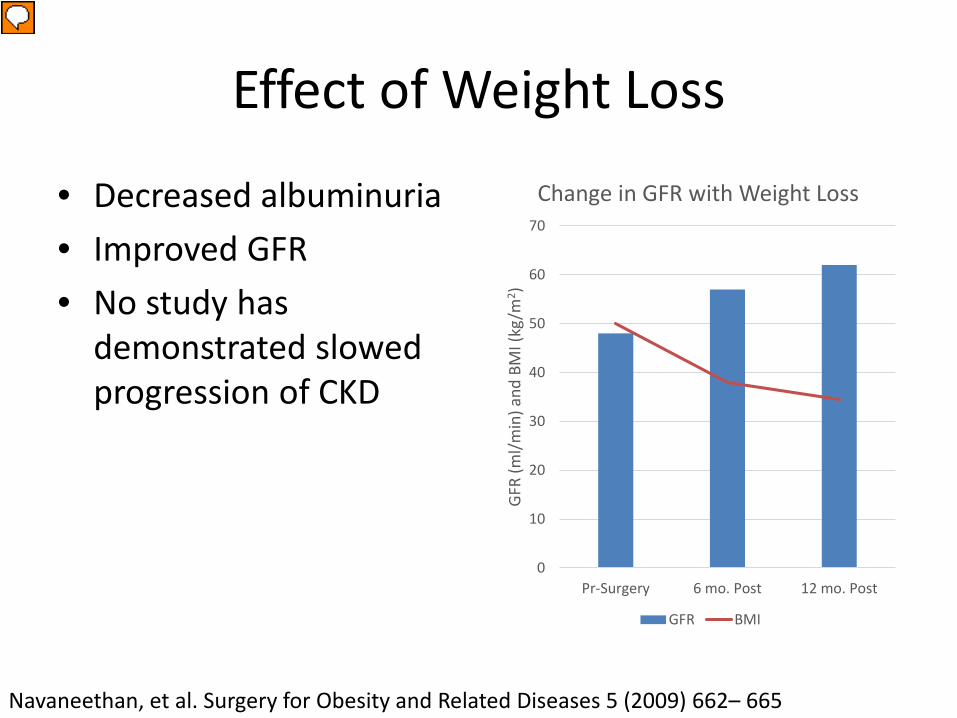
Effect of Weight Loss
• Decreased albuminuria• Improved GFR• No study has
demonstrated slowed progression of CKD
0
10
20
30
40
50
60
70
Pr-Surgery 6 mo. Post 12 mo. Post
GFR
(ml/m
in) a
nd B
MI (
kg/m
2 )
Change in GFR with Weight Loss
GFR BMI
Navaneethan, et al. Surgery for Obesity and Related Diseases 5 (2009) 662– 665
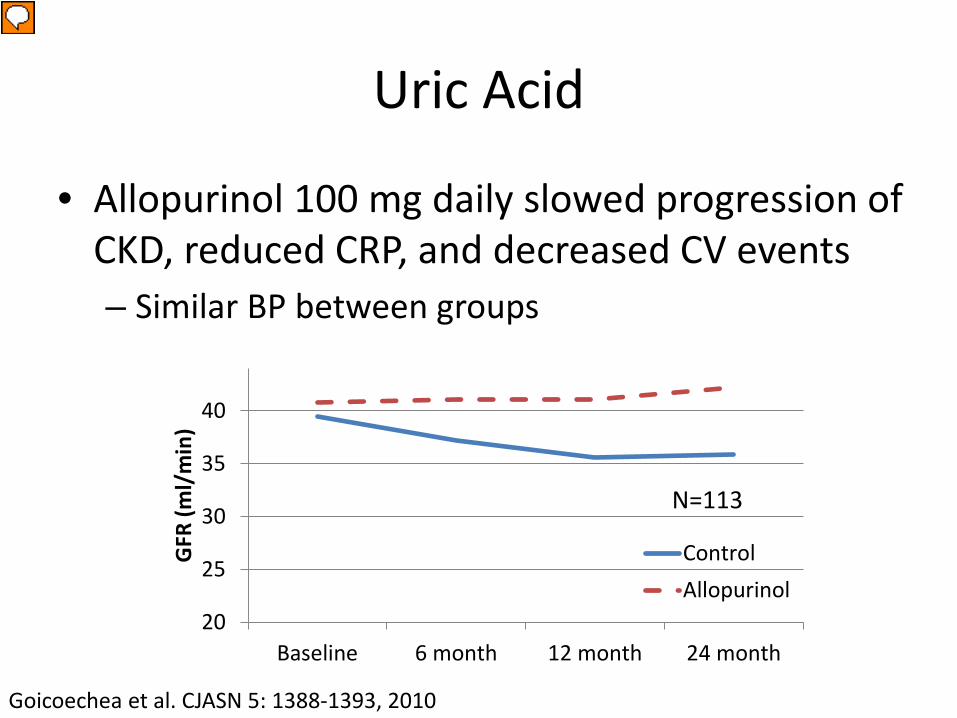
Uric Acid
• Elevated uric acid levels are associated with CKD, hypertension, and CV disease
• Hyperuricemia associated with increased mortality and higher cardiovascular events
• Not clear that elevated uric acid leads to CKD progression. Proposed mechanisms: – hypertension with activation of RAS– increased glomerular hydrostatic pressure– fibrosis
Uric Acid
20
25
30
35
40
Baseline 6 month 12 month 24 month
GFR
(ml/
min
)
ControlAllopurinol
N=113
• Allopurinol 100 mg daily slowed progression of CKD, reduced CRP, and decreased CV events– Similar BP between groups
Goicoechea et al. CJASN 5: 1388-1393, 2010
Nocturnal Hypoxemia
• Sleep Disordered Breathing: up to 65% in CKD vs. 20% in general population– OSA vs. CSA
• Nocturnal Hypoxemia– Oxidative stress, sympathetic and RAS activation– Endothelial dysfunction → CV disease– Tubulointerstitial disease → ESRD
Sakaguchi et al. Clin J Am Soc Nephrol 8: 1502–1507, 2013
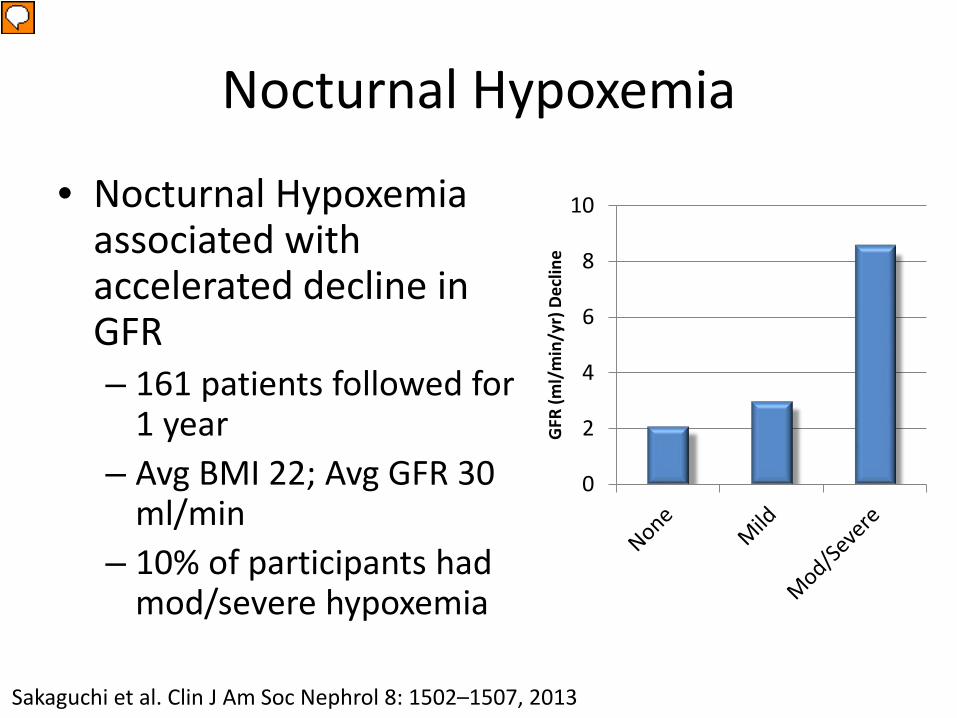
Nocturnal Hypoxemia
• Nocturnal Hypoxemia associated with accelerated decline in GFR– 161 patients followed for
1 year– Avg BMI 22; Avg GFR 30
ml/min– 10% of participants had
mod/severe hypoxemia
0
2
4
6
8
10
GFR
(ml/
min
/yr)
Dec
line
Sakaguchi et al. Clin J Am Soc Nephrol 8: 1502–1507, 2013
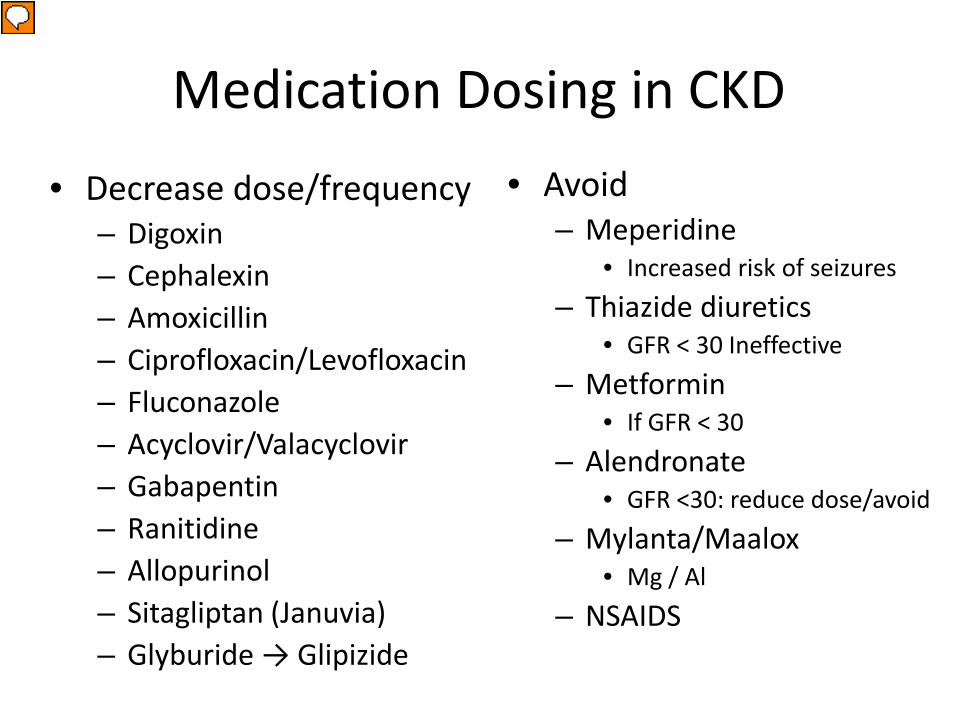
Medication Dosing in CKD• Avoid
– Meperidine• Increased risk of seizures
– Thiazide diuretics• GFR < 30 Ineffective
– Metformin• If GFR < 30
– Alendronate• GFR <30: reduce dose/avoid
– Mylanta/Maalox• Mg / Al
– NSAIDS
• Decrease dose/frequency– Digoxin– Cephalexin– Amoxicillin– Ciprofloxacin/Levofloxacin– Fluconazole– Acyclovir/Valacyclovir– Gabapentin– Ranitidine– Allopurinol– Sitagliptan (Januvia)– Glyburide → Glipizide
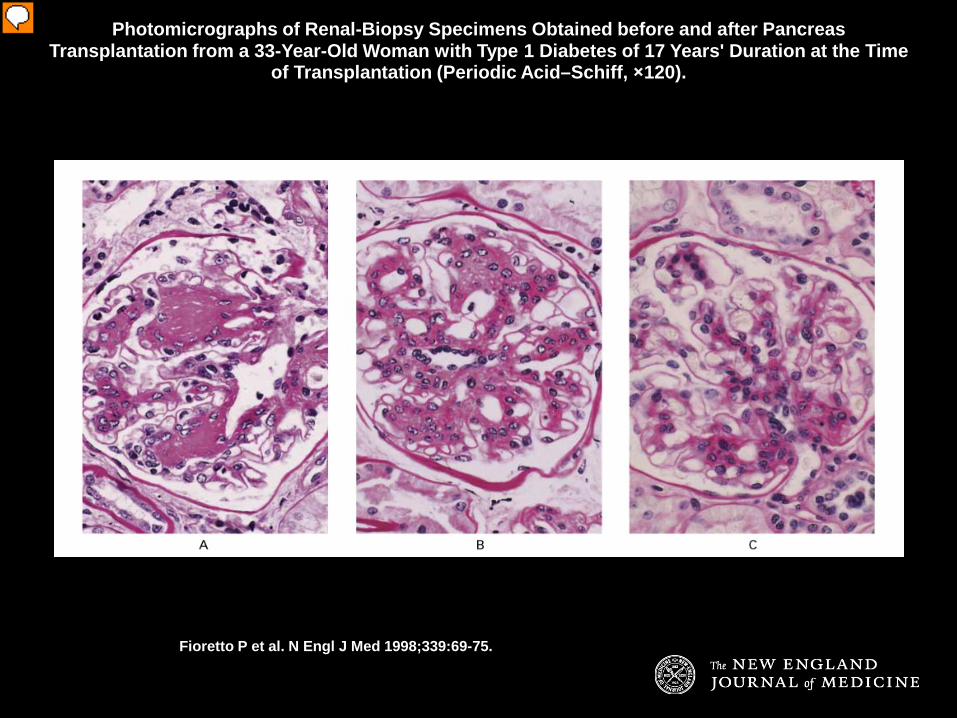
Photomicrographs of Renal-Biopsy Specimens Obtained before and after Pancreas Transplantation from a 33-Year-Old Woman with Type 1 Diabetes of 17 Years' Duration at the Time
of Transplantation (Periodic Acid–Schiff, ×120).
Fioretto P et al. N Engl J Med 1998;339:69-75.
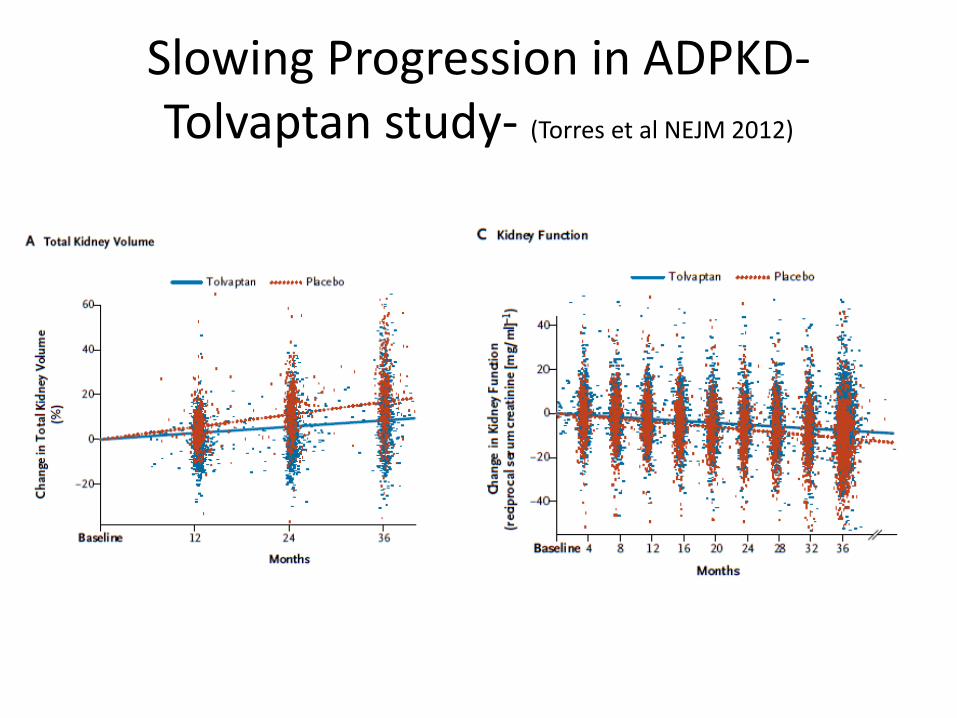
Slowing Progression in ADPKD-Tolvaptan study- (Torres et al NEJM 2012)
Summary• Chronic kidney disease is common.• Many of the CKD progresses over time• Blood pressure control, angiotensin blockade, and
control of proteinuria slows progression• Renal anemia treatment with EPO needs a careful
approach.• Control phosphorous• Always be vigilant of drugs (both OTC and prescribed)
which could make CKD more difficult to manage.• Good medical management of risk factors like lipids,
obesity, salt intake and smoking reduce morbidity
60












