Embed Size (px)
Citation preview

The Comprehensive Pediatric Health Assessment
What do I need to know?
Jessica Keester, MSN, C-PNP, RN

Objectives 1. Review the pediatric-focused assessment:
2. To understand the components of a
comprehensive assessment
3. Discuss system-specific focused assessments;
that vary most significantly in pediatric
4. To be able to demonstrate complete
documentation of patient assessment
5. Handouts- tools to use in practice

Components of a Comprehensive Assessment 1. Patient History: (Subjective information)
Obtained from..
a. The client/ parent interview
b. Chart, Medical Records
Includes:
c. Family History
d. Past Medical History; medications; allergies
e. History related to current need for care or treatment
f. Chief Complaint
- Current issue being cared for Do I need to ask this
every shift?! Where o I find it if I am
new to the case?!

Components of a Comprehensive Assessment
2. Physical Exam (mostly objective
information)
a. Objective Information:
a. Vital Signs, ht, wt (if applicable)
b. Head to Toe assessment
a. Should include focused exams by
system: Inspection, Auscultation,
Percussion, palpation
c. Focused Assessments
a. What systems? How often?
b. Subjective information:
a. Symptoms r/t system assessing
(Ie. pain, tenderness)

Medical History?
Subjective
Medications?Subjective
Pain?
Subjective
Skin Breakdown?Heart Rate?
Both! Objective
Subjective vs. Objective
Nausea?Subjective

Where do I start?

Client history …AS important as the physical exam

Client History: Obtaining The Initial History
Preparation: Review information do we have before the client interview:
1. Any Previous medical records
available on the patient 2. Order set/ plan of care
1. Medication List 2. Treatment schedule
Interview: The complete health history is an opportunity to establish a relationship with the patient/family, gain insight into the family environment and dynamic, as well obtain health information
(Richardson, 2013)

Client History: Obtaining The Initial History
Obtaining the initial History
When you are the first person in your organization to assume care for this patient
Subjective information:
1. Family history
For example: Incidence of chronic conditions/ disability/ psychosocial diagnoses, serious illness, early death
-Maternal history of high risk pregnancy, drug/ alcohol use, prenatal history(s)
-Social History
2. Past Medical History of Patient
a) Diagnoses (chronic and acute)
b) Medical/ Surgical (ED visits, hospitalizations, etc)
c) Allergies; Medication List
3. Dynamic family situation
4. What their goal is for your services(Richardson, 2013)

Client History: The Interval History
Re-admission/ Re-cert When your organization is RE-assuming care of this patient/ OR 60 day update
on plan of care
Subjective: 1. Any information above that is not previously documented in chart, or
unable to obtain. *Who did the previous assessment? Is it as detailed as you would make it?
* “To get started I’m just going to review some information with you that we already have in your chart”
2. Any Changes since last Comp Assessment was done 1. ED Visits, Hospitalizations2. Office Visits: Changes to Plan of care or Medications3. Significant Growth, changes in Developmental Status4. Changes to Plan of Care
(Richardson, 2013)

“Other” Subjective information Some examples from Devero:
1. Home Assessment (layout, sanitary, electrical)2. Language 3. Psychosocial 4. Spiritual/ cultural 5. Neurological status 6. Emergency/ safety measures; Supplies7. Advanced Directives 8. Neurological status 9. Supplies
Ultimately the goal is to work these answers into a narrative; guide the conversation without reading question by question. Answer as much as you can by observation

Tips for the interview 1. The first impression can set a precedence for the duration of care;
approach accordingly *What impression is given if you have not read their chart/ medical
record yet?2. Be fully present with the client/ family during this time: Active Listening
1. Greet the patient/ family by name2. Sit3. Maintain eye contact with historian 4. Do NOT babysit the EMR
3. Allow time for the historian to recall, or decide how to word things*Silence is ok!
4. Take the history in chronological order1. prenatal Infant toddler pre-school/ school age adolescent
5. Clarify when needed! 1. It’s better to do this immediately than to go back later
6. “Is there anything else I have not addressed that you would like to discuss?”
7. Use your instincts! (Henderson, Tierney, and Smetana, 2012.)

The interview helps establish a
relationship with the client before
moving into the invasive physical
exam

Physical Assessment
…It’s a big deal too.

Vitals: a) Pulse/ hr b) Respirationsc) Blood pressure (?)d) Pulse ox (?) e) **PAIN
1. Exam by system a) General (……?) b) Skin (throughout whole exam) c) “HEENT” (+Mouth)d) Neurological (reflexes?, developmental status..) e) Respiratory f) Gastrointestinal g) MSK (motor skills, some neuro) h) Genitalia (often PD for therapists..Nurses should NOT defer
this if possible…) Subjective Data
**Be aware for MIX of subjective and OBJECTIVE data: For example: endocrine section- you as a therapist or nurse can not “assess” hypothyroid. That is a Medical Diagnosis. Devero groups together relative subjective findings of ROS and exam .
Components of the Physical Assessment:

Physical “Exam” vs. “Assessment”…..“Assessment” data is information you can gather. Subtle differences between fields. You can “assess” data that is given to you as a subjective assessment; or you can assess data that you collect based on your training and scope of practice
“Exam” data includes only the information you can collect independently; based on training and scope of practice.
Ie….. MEDICAL Practice/ Diagnosis NURSING Practice/ Diagnosis THERAPY Practice/ Diagnosis “MID- LEVEL” Practice/ Diagnosis

Moving on.

•Gathering information
•Explanation of procedure
•Cooperation during the exam
•Concept of invasive vs. non-invasive
•Relationship with the family is as important as the client themselves.
•….. Medications, compensating, anatomy changes with phase of development, etc. …..
What makes a pediatric patient different than an adult?

Developmentally AppropriateCare

Development: Dependent to parent, will look to parents for security, reacts to parents anxiety levels
Interview: Full interview taken with parent. “white coat” anxiety less of a factor, Least invasive first is most important (you never when they will get irritated with being touched!)
Position: Before 4-6 months: can be on table, make sure parent is in view After 6 months: Best in parent arms, or laying on parent lap encourage parents to be an active part of the exam *great time to assess parent attachment to infant
Sequence: If quiet, auscultate heart, lungs, abdomen. Heart and respiratory rates. Perform traumatic procedures last (eyes, ears, mouth [while infant is crying]). Elicit reflexes as body part examined.
Infant: Birth – 12 months
(Richardson, 2013; Duderstadt, 2006)

Provider Tip:
What is “invasive” to
infants/ kids??Thermometers
Mouth, nose, ears…think orrifaces
Under their clothes
COLD

Development:
Still utilizes parent as safety; but begins to explore in
sight of parent
Interview:
Full interview taken with parent. Should have some
anxiety to new faces/ caregivers. Begin communication
with child based on their growing vocabulary
Position:
Best to begin in parent arms, or on parent’s lap. A good
approach is to assess on parent first than the child
Sequence:
Attempt to warm child up to you first, involving toys/
play, let them touch equipment before use. Attempt to
auscultate heart, lung, abdomen first, get RR heart rate
they may cooperate very well at first related to
curiosity..this will not last long! Invasive assessments
LAST!
Toddlers: (12mo-3yo)
(Richardson, 2013; Duderstadt, 2006)

Development:
Increased exploring; intentional limit pushing
Interview:
Full interview taken with parent. Should have some anxiety to new faces/ caregivers. Begin communication with child based on their growing vocabulary; If they are timid try averting eye contact
Position:
Child may want to begin on parent’s lap or holding parents hand, A successful approach is to assess on parent first than the child
Sequence:
Use play and toys to become acquainted and non-threatening; Inspect body through counting fingers; using minimal contact initially. Introduce equipment through play, let them feel and touch equipment. Auscultate as soon as possible–busy age group!
Preschool: 3 yo-5yo
(Richardson, 2013; Duderstadt, 2006)

Development: Seeking autonomy; exploring (self-exploration/ stimulation common) Still prefers parent closenessInterview:Include child in interview/ subjective information. Children this age generally like to answer questions about themselves; Provider lead style of interview Position: Sitting alone Sequence: In this time period it is appropriate to begin proceeding through head to toe assessment; examine genitalia last assessment, should notice discomfort or resistance with genital assessment. (Richardson, 2013; Duderstadt, 2006)
School age: (5yo-12yo)

Development: Autonomy is very important to this age *
specific struggle for patient who are
medically dependent
Interview:Let the adolescent patient speak for themselves; Patient-lead style of interview. Clarify questions you still have at the end, allow parents to add at the end.
Position: Sitting/ Alone, may want parent to leave room during physical assessment *without developmental delay- allowing an autonomous assessment is best practice
Sequence: Proceed in Head to toe assessment * genital area last- this is the only particularly invasive assessment to adolescents
Adolescent (12yo-18yo)

Provider Tip:
EMOTIONAL DEVELOPMENTAL status is more relevant than age!
Follow recommendations for the age corresponding with development
Physical Development DOES NOT equal mental/ emotional development

PHYSICAL EXAM

General Guidelines on Physical Exam: Other Helpful hints
• Have space well lit• Always approach child from front• Always ask permission; give choices
• Don’t Lie- if it’s going to hurt, find a way to downplay it without lying “little pinch”
• Have toys/ TV/ distraction• Involve Parents as much as possible
• Avoid long explanations, child appropriate “Let me feel those strong muscles”
• Approach exam prepared and organized • Limit others in room besides family members
• Maintain privacy; dignity

Your Assessment •How do these trend with age?
Heart rate- lowers with age
BP- raises with age
RR- Lowers with age
Sp02- Does not change- “norm” is always 95-100%
How do vital signs reflect compensation in Pediatrics?
Trend ___first, then trend ____ once this change occurs prognosis is OMINOUS
Vital Signs

General Impression

Your Assessment “General”
Options:
AwakeAlerttired ListlessLethargic**Ill-appearing/ well-appearing
interactive paleThinFlushed Content
What your assessing..
Facies Posture Body movement Hygiene Nutrition Behavior Development State of awareness

Nose: • Position, alignment• Turbinates- color/ swelling of mucosa?• Nares*
Throat: • Tonsils-Grade 1-4, exudate, color
Mouth:• Teeth**, gums, buccal mucosa • Pharynx • Soft/ hard palate
HEENT Head
• Shape, Symmetry, Molding, circumfererence?
• Strength (head lag), ROM, scalp, hair • Fontanelles
Eyes• Placement• Lids- observe placement, movement• Conjunctiva
Palpebral/ Bulbar• Discharge?
Ears: • Placement/ development• Note presence of any abnormal
openings, tags of skin, or sinuses. • Inspect hygiene (odor, discharge,
color).
What body system develops the same time as ears?

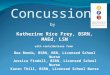
Your Assessment Inspection:• Shape, size, symmetry, • Evaluate respiratory movements for rate,
rhythm, depth, quality, and character movement
• Work of breathingAuscultation: • (Diaphragm of stethoscope- for HIGH pitched
sounds)
• Needs to be quiet!
• Where do you get most information?
• What is normal?
• What are abnormals?•Percussion:• What does it tell us? What is the
“normal”?Appreciate dullness of the left anterior chest due to heart and right lower chest due to liver. Note the hyper-resonance of the left lower anterior chest due to air filled stomach.
Respiratory Auscultation: http://www.practicalclinicalskills.com/auscultation-course-contents.aspx?courseid=201
Trach? Add:Inspection: • Tracheostomy Site- ties in place, skin
condition, secretions• Connected to source of O2/ vent
settings?
Auscultation: • Diaphragm of stethoscope
• Needs to be really quiet!
• Coarse breath sounds likely to be patient norm
• Vent: Differentiate self-initiated breaths/ vs. vent “breaths”
**This is when knowing pt baseline is critical!

Respiratory… Tracheostomy…
Inspection: • Tracheostomy Site- ties in place, skin
condition, secretions• Connected to source of O2/ vent
settings?
Auscultation: • Diaphragm of stethoscope
• Needs to be really quiet!
• Coarse breath sounds likely to be patient norm
• Vent: Differentiate self-initiated breaths/ vs. vent “breaths”
**This is when knowing pt baseline is critical!
Suction?-Pre-assessment
-Amount , consistency, color of secretions
-Post-assessment! (…Did it work?!)

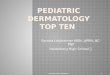
Inspection• Heaves, lifts
Palpation• Thrills
Auscultation• Where do you listen?• What position should the child
be in?
Cardiac
ValvesAortic area—Second right intercostal space close to sternumPulmonic area—Second left intercostal space close to sternumErb point—Second and third left intercostal spaces close to sternumTricuspid area—Fifth right and left intercostal spaces close to sternumMitral or apical area—Fifth intercostal space, left midclavicular line (third to fourth intercostal space and lateral to left midclavicular line [MCL] in infants)
PalenessPulsesSOB
“bluing”Tires easily
*think feedings for infants

Your Assessment Cardiac
Murmurs-Most benign murmurs are early - mid systolic.-Diastolic murmurs almost always indicate pathology.-A systolic murmur is present between S1 and S2-A diastolic murmur is present between S2 and S1-A continuous murmur is present in systole and diastole
Mitral areaMitral valve prolapse, regurgitation, and stenosis; Still’s murmur, aortic stenosisTricuspid areaTricuspid regurgitation, ventricular septal defect (VSD), Still’s murmur, hypertrophic cardiomyopathy.Pulmonary areaPulmonary regurgitation and stenosis, ASD, TAPVR, PDA, and pulmonary flow murmurs.Aortic areaAortic stenosis, benign aortic systolic murmurUsing the bell and diaphragm, you should first perform a sweep at these locations for heart sounds and then a second sweep for murmurs.S1/S2
http://www.easyauscultation.com/cases?coursecaseorder=1&courseid=223rd Heart tone (physiologic) http://www.easyauscultation.com/cases?coursecaseorder=4&courseid=22Innocent Murmur http://www.easyauscultation.com/cases?coursecaseorder=5&courseid=22

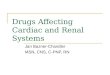
Your Assessment Abdomen/ G.I
InspectionSize, contour, shape, umbilicus
-> GT? Location? Patent?-> Ostomy site?
AuscultationWhat is normal?
Palpation• Location of internal organs
important to interpret findings
Percussion • Which anatomy produces which
sounds? • *Subjective information, Pain
What tells us most about the G.I tract and it’s functioning?

Documentation

How does this compare to the head to toe
assessment you learned in school?
What indicates more information is needed?
•Any chronically effected system
•Changes to previous assessment/ baseline
• ANY documented “abnormal”- regardless of history

1. Head to Toe
1. To be completed at the beginning of shift (1st hour)
2. Comprehensive- every system
2. On-Going Assessment/ “Progress note”
1. System specific re-assessment based on systems that are affected
(see previous slide)
2. About every 2hours- based on patient condition
3. Intervention based Assessment
1. Re-evaluation based on interventions, medications
2. Pre-assessment, intervention assessment, Post-assessment (see
suctioning example
I think of physical assessment as 3 components …

Shift head to toe assessment
On-Going Assessment/ “Progress note”
Procedural

Case Studies


References:
Allen, P., Vessey, J., & Schapiro, N. (2010). Child with a chronic condition (5th Ed.). St.Louis, MO: Mosby Elsevier.
Burns, C., Dunn, A., Brady, M., Starr, N., & Blosser, C. (2013). Pediatric Primary Care (5th). Philadelphia, PA: Mosby Elsevier
Craven, R., Hirnle, C., & Jenson, S. (2013). Fundamentals of nursing; Human health and function (7th. Ed.). Philadelphia, PA: Wolters Kluwer Health/ Lippincot WIlliams & Wilkins.