Embed Size (px)
Citation preview

The complexities of Care for
People with Dementia
Professor Ríona Mulcahy
University Hospital Waterford
-

Challenges in Dementia
Ageing population
Significant number of younger people with dementia
Access to Diagnosis
Maintaining Independence and Living well
Impact on carers,
Sense of Loss, isolation, loneliness
Behavioural and psychological changes
Polypharmacy
Acute Hospital care/ Environmental Challenges
Supports and care in the community
End of Life/Palliative care
Nursing home care
Will, Power of attorney, Advance directives

Ageing Statistics
Those over 65 increased by 14.4% between
2006 and 2011
Each year the total number of people over
the age of 65 grows by around 20,000
Increase greatest amongst the ‘oldest old’
Those aged 85+ increased by 22% between
2006 and 2011 and will have doubled by
2025 • Source: Department of Health, 2012, Future Health, p 2

Dementia in Ireland
48,000 people with dementia in Ireland
4,000 people aged less than 65 with dementia
For every one person with dementia, 3 family
members are affected
Dementia remains a neglected illness
Irish National Dementia Strategy
December 2014


Programme for Government
2011 - 2016
Improve Dementia Care
– Increase awareness “whole community approach”
– Early Diagnosis and intervention
– Enhanced community based services
Live well as long as possible
Appropriate Services and supports
Access to specialist care when required
Die with comfort and Dignity

To understand Alzheimer’s disease, it’s important to know a bit about the
brain…
The Brain’s Vital Statistics
Adult weight: about 3 pounds
Adult size: a medium cauliflower
Number of neurons: 100,000,000,000
(100 billion)
Number of synapses (the gap between
neurons): 100,000,000,000,000
(100 trillion)

Brain ageing- some facts
• Brain cells shrink, nerve fibers that transmit signals from one brain
region to another, start to degrade around age 50
• After age 60, the brain shrinks, losing around 0.5-1% of
its volume per year
• The effects are greatest in the part of the brain responsible for
remembering
• a telephone number while you're dialing
• planning, focus, and behavior choices and sometimes in the area
involved in memory.




Memory
Long term memory - Storage
Short term memory
Movement of short term memory to storage
Retrieval
Brain
– Frontal Cortex
– Occipital cortex/Parietal cortex
– Hippocampus
– Precuneus

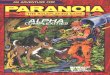
Differential diagnosis of dementia
Vascular dementias
– multi-infarct dementia
– Binswanger’s disease
DLBD
– Parkinson’s disease
– diffuse DLB
– Lewy body variant of AD
Other dementias
– frontal lobe dementia
– Creutzfeldt-Jakob disease
– corticobasal degeneration
– progressive supranuclear palsy
– potentially reversible dementias
AD
Gersing et al., 1998; Cras, 1998
17.5%
7.5%
55% 20%

Cognitive features altered in AD
• Memory (particularly short term) - PROGRESSIVE
• Language skills – word finding difficulty
• Executive function: problem solving, planning
• Visuospatial function: orientation, getting lost
• Agnosia: ability to recognize individuals and objects
Adapted from Dastoor and Mohr, 1996
Adapted from Coyle et al., 1983
Frontal cortex
Parietal cortex
Occipital cortexMedial septal
nucleus
Nucleus
basalis Hippocampus

Factors influencing the
development of AD
Dartigues and Orgogozo, 2000;
Lannfelt, 1996; Mullan, 2000;
Geerlings et al., 1999
Well-established risk factors*
– increasing age
– ApoE4 genotype
– Down’s syndrome
– previous head injury
– low educational achievement
Possibly protective
– EXERCISE
– moderate wine consumption
– ApoE2 genotype
– high educational achievement
– oestrogen
– antioxidants
Causative factors
– chromosome mutations
(including loci on
chromosomes 1, 14, 19, 21)
Risk factors
– female gender
– smoking
– vascular disease
– Hypertension
– Dyslipdaemia
*Clearly supported in literature


Reisberg, B. Geriatrics, 1986, 41 (4): 30-46.


What is Delirium?
Disturbance of consciousness
A change in cognition
Develops over a short period of time
Fluctuates during the course of the day

How common is Delirium?
Older patients admitted to hospital – 30%
Hip fracture - up to 50%
Even higher in ICU and terminal care patients
30 – 40% cases of delirium are preventable

Delirium – Latin word
Lira the ridge between two furrows of
ploughed land
De – lira out of the ridge or “off track”

Chest infection
Antibiotics
HOME
Consequences of Delirium
Increased risk of institutionalisation
Increased functional dependency
Longer length of hospital stay
Increased mortality

Reserve

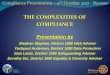
Delirium and Dementia
• Patients with dementia MUCH more likely
to develop delirium
•Patients with delirium are MUCH more
likely to develop dementia
•Delirium may indicate incipient dementia
40%
25%
25-33%
RecoveryPermanent Cognitive ImpairmentMortality
Recovery Mortality
Permanent
Cognitive
impairment
Outcome following
delirium

Environment
Acute hospital 29% of all patients in an acute hospital may have
dementia
– Irish National Audit of Dementia
• 94% hospitals - no dementia care pathway
• Mixed wards/Moving wards
• Noisy, changing staff
• Confined environment
• People with dementia admitted to hospitals have
poorer outcomes and increased mortality
• Spend significantly longer in hospital (>4 times)
• Higher risk of institutionalization

BPSD Behavioural and Psychological Symptoms of Dementia
Delusions
Hallucinations
Depression
Anxiety
Agitation
Aggression
Wandering
Sleep disturbance
↑ prevalence with
disease severity (60 –
90%)
BPSD → prognostic
significance
↑ functional impairment
↑ carer distress
↑ hospitalization or NH

Psychotic Symptoms
Delusions
“abnormal beliefs held with firm conviction in the absence of confirmatory evidence – not in keeping with social, cultural or religious norms”
Paranoid
Poisoning
Intruders
Delusional misidentification
(Capgras’ syndrome)
Hallucinations
“perceptions occurring in the absence of a stimulus”
Visual > auditory > olfactory
20 – 30% AD
70 – 80% DLB
Also in VD

Depression in Dementia
≥ 1 depressive symptom ≈ 50%
Actual depressive disorder ≈ 20%
Symptoms
agitation
irritability
slowness of speech or movement
↓ appetite or sleep disturbance
↓ interest in surroundings
↓ interest in previously enjoyed activity
Risk factors
personal or family history
social isolation
chronic and painful physical illness
bereavement

Anxiety in Dementia
Causes
insight into condition
reaction to change in
routine or environment
may not fully
understand a situation
hallucinations
delusions
↓ functional ability
↓functional ability
↓confidence
↑anxiety
↑dependency

Agitation “Inappropriate motor, verbal or vocal activity”
Common manifestations
Repetitive purposeless
movements
Restlessness
Pacing
Wandering “Must get home”
Hand-wringing
Foot tapping
Groaning
Shouting
“Sundowning”
Common causes
Boredom
Profound disorientation
Frustration
Over-stimulation
Depression
Discomfort
Pain
Medications
Delirium
Poor relationships

Pharmacological treatment
(Only one aspect of management)
Antipsychotics
Antidepressants
Cholinesterase inhibitors
NMDA antagonists
Anti-epileptics / mood stabilizers
Benzodiazepines
Carers
Training
Environment
Support

Weight loss in dementia
Commonly develop feeding problems, weight loss,
and nutritional deficiencies
Often a cause of upset for families, carers and health
care professionals
“Starving them to death”
“Can’t just stand by and do nothing”

PEG – percutaneous feeding
“What about a PEG” – percutaneous feeding
– No increase in survival
– No reduction in aspiration pneumonia
– No reduction in pressure ulcers
– Poorer quality of life
– 50% - 30 day mortality
– 90% - 1 year mortality
– BMJ 2010; 340

So what do we do?
Education
– Poor oral intake and weight loss part of the disease
process
– Upsetting for the people “looking on”, not the
patient themselves
– Allow patients to take what they want when they
can
– Adapt physiologically

Management of pain in Dementia
50% regularly experience pain
80% of nursing home patients have acute or chronic
pain.
Pain is often a contributory factor in behavioral and
psychological symptoms of dementia
Many of these individuals are unable to communicate
their thoughts and feelings which makes symptom
management complex.
Awareness and prompt management key

Young onset dementia
Other challenges
– Young family
– Still in the work force
– Role change
– Implications for other family members
“I am not suffering”
“I am struggling to be part of things – to stay
connected to who I would was”
“Live in the moment – that’s really all I can do”


https://www.youtube.com/watch?feature=player_detai
lpage&v=ZrXrZ5iiR0o#t=17

Long term care options
24 hour care required
34% of all people with dementia in nursing homes

Common Scenario (Brindle & Holmes, Stewart et al, Age Ageing 2005)
Consult to old age medicine/psychiatry
Tx of acute illness in older person completed
Residual physical/cognitive problems
Family/doctors/PHN want long-term care
– ‘Best interests’
– ‘At risk’
– ‘Can’t cope’
– Family ‘won’t take her home’
– What does the patient want?

Discussion with patient
“I want to go home”
“I would rather die than go to a nursing home”
“I will only leave my own home in a box”
“What would they (family) know about it”
“I managed until I come in here!”
“Risk – what about it!”

Standard Argument?
You are not able to care for yourself properly / not safe/
neglecting yourself.
What if……?
You will be better off in residential home where you will
receive such care

Looking for Answers? Reality?

How better off?
It’ll be nice for you to be with other confused people?
You’ll be less confused? – ‘Nursing home placement associated with accelerated short-
term cognitive decline in Alzheimer’s disease’. (Wilson, Am J Psych 2007)
You’ll be happier? – ‘Increased feelings of loneliness and marginalization;
psychiatric symptoms worsened and quality of life perceived more poorly’. (Scocco, Int J Geriatr Psych 2006)
You’ll get better medical care?
You’ll live longer? – Shorter life expectancy in Alzheimer’s disease admitted to LTC
(McKee, J Gerontol 2006)

AP – 78 Year old
Living alone
Admitted post fall and tissue injury/bruising
Cognitive impairment – MMSE 16/30 6 months earlier
Home help once per week (not always let in!)
Refused meals on wheels
Nephew in Dublin ”Shouldn’t be sent home again”
– “Your responsibility to sort it out”
PHN – limited access – concerned
Supportive neighbour
Occasional incontinence – wears pads at home

Assessment
Physio – Independent with a frame (often forgets it!)
OT – MMSE 15/30
– Slow in ADLS but mainly independent
– Falls risk ++
– Intermittently disoriented on the ward
– Occasionally incontinent
Nurses – not having to do a lot for her as refuses help
“constantly asking to go home”
Collateral – always a very private lady
House neglected
Poor heating

Discussion
Concerns and risks highlighted by all team
“I do not want to go to a nursing home”
“It’s my choice”
“Would prefer to die in my own home”
“You are holding me here against my will”
MDT
Rehab
Package of care/day centres/Alzheimer’s pack
Home
Review of notes – Hip fracture 9 months earlier –
similar concerns then

And what about the family and carers?
Face complex and challenging problems as the disease
progresses:
aggressive behavior, restlessness, wandering,
incontinence, delusions and hallucinations, reduced
mobility and feeding problems.
“out of my depth”, “isolated”, “worn out”
Education including improved training for health and
social care professionals.
Supports
Guidelines/Clear pathways of care
Access to services when required

Prognosis in Alzheimer’s disease
Progressive neurodegenerative disorder
Average life expectancy from onset of dementia – 8 to
10 years but ……
– Depends on age of onset of symptoms
– Stage of disease at time of diagnosis
– Comorbidities
– Most common cause of death is pneumonia

Management of Dementia
Multidisciplinary approach
Look for and treat reversible conditions
Assessing patients needs and wishes
Collateral from family, carers, PHN
Carer supports and services
Voluntary societies
Have specific goals when introducing new medication
Routine / Familiar environment
Access specialist opinion where required
Most physicians can add medications
Few physicians can subtract!

Focus on quality of life, rather than length of
life, in the final stages of dementia.
Dementia is a progressive life limiting condition with
increasing prevalence and complex needs
– Physical, emotional and spiritual
– Palliative care needs often poorly addressed
• Pain (under recognized and treated)
• Care planning
• Burdensome interventions
• Place of death

Key Components of Care when providing a Palliative
Approach to People with Dementia.