Embed Size (px)
Citation preview

The Commissioning and Delivery System for children and young people’s mental health
Lisa Williams, Consultant and member of the BOND Consortium

• What we mean by the commissioning and delivery system• Earlier intervention mental health services• How do the VCSOs fit in to this, and to the pilot?• What is happening to the market?• What we heard from Tees Valley

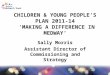
Tier 4: Inpatient Care
Infrequent competition amongst larger MH provider trusts
Some variety of providers More frequent tendering + increasing competition (usually LAs, NHS)
Numerous providers + commissioners Large + small organisations More VCS Less clinical governance Smaller contracts Frequent tendering
Tier 3: Clinical/ medical care (diagnosis/ medication)
Tier 3/2 interface: Primary MH services LAC, YOS, other targeted CAMHS
Tier 2/1 interface: ‘Generic’ School + community based e.g. counselling + IAG services Related services e.g. drop-in, youth support, family support
Limited contestability Increasing levels of competiti
on

Access
Service ‘tiers’ 1 4

Mental health expertise
Service ‘tiers’ 1 4

Mental health expertise
Service ‘tiers’ 1 4
Access
?

Mental health expertise
Service ‘tiers’ 1 4
Access GP
LA School

Mental health expertise
Service ‘tiers’ 1 4
Access
School Counselling
Activity
based
Mediation
Young Carers
D.V.
Drop in
Mental Health Services

Feedback from Tees Valley pilot participants
In groups:
What is your role?Does this model match your local
experience?What are the key issues for you?

Quality
• All have safeguarding in place
• Several generic quality schemes e.g. IIP, PQASSO
• Others – NICE, MATRIX, CORC
• Commissioners tend not to specify quality measures & can change with each tender
• Accreditation to professional bodies – varies depending on service e.g. BACP
• All identified a level of CYP involvement in service quality development

• Range from 0% to 100%
• Majority experience reductions (up to 1/3)
• Around half total income via local public service contracts
• Majority of this NHS and LA
• Rest is trusts, foundations, grants etc
• Very small % from schools for some

• Mainly competitive tendering and grants
• Schools – tend to favour spot purchasing and fees for direct services
• Some consortia bidding (relatively successful)
• All interested in bidding for more contracts

• Funding • Competition vs partnership• Statutory service domination of partnerships• Commissioners concerns about quality from VCS
(focus on clinical services)• Capacity to compete –process excludes smaller
organisations or less ‘networked’ VCSOs• New requirements e.g. PBR, outcome measures• Business planning on shifting sand– personnel,
policy, environment• Lack of leadership and strategic direction

• How can we strengthen our position in the market place and compete more effectively?
• Should we specialise more, or be more holistic and focus on access?
• What are the best ‘vehicles’ for delivery e.g. social enterprise, community interest companies, mutuals, consortiums etc?
• Why don’t commissioners value what we do as much as more medical/clinical services?
• How can we access schools when there are so many with such varied levels of interest?

• Ensure services are ‘safe’ and high quality?• Fully understand the market, let alone develop it?• Use commissioning to develop services for the most
difficult to reach groups? • Ensure timely access to appropriate MH expertise in
the right part of the system?• Know what is the best value for money?• Influence other commissioners so that they don’t
make cuts which then impact on services I commission?

• How do we identify students with a mental health problem?
• How can we get help quickly?• Why can’t we refer to CAMHS? And why can’t we have
information back from CAMHS about pupils?• How do we know what works and what’s the difference
between services?• What impact will emotional and mental health support
have on pupils’ attainment?• What services should be offered to schools, what should
we have ‘in house’, and who should pay?