Embed Size (px)
Citation preview

DENTAL TECHNIQUE
aAssociate PrPrivate practbFaculty, Dep
THE JOURNA
The combination prosthesis: A digitally designed retrievablecement- and screw-retained implant-supported prosthesis
Periklis Proussaefs, DDS, MSa and Abdulaziz AlHelal, BDS, MSb
ABSTRACTThe technique described offers a digital workflow for designing and fabricating a combinationcement- and screw-retained implant-supported prosthesis. After making the definitive impressionand definitive stone cast, the definitive combination prosthesis is digitally designed. Custom-milledtitanium abutments and cementable superstructure prosthesis are designed and milled by havingocclusal access channels of the prosthesis correspond to the occlusal access channels of the customabutments. After intraorally confirming the esthetics, occlusion, and fit, the prosthesis is cementedintraorally and removed as a screw-retained prosthesis. After excess cement is removed, thecombination prosthesis is placed intraorally, and composite resin is used to seal the occlusal accesschannels. (J Prosthet Dent 2018;119:535-9)
Screw-retained prostheseshave the advantage of beingeasily retrievable.1,2 However,the presence of occlusal accesschannels compromises theiresthetics, ceramic strength, andocclusion.3 Cement-retainedprostheses are easier to fabri-cate, offer easier delivery in theposterior area of the mouth,
and have higher potential for passive fit.1,2,4,5 Although anearlier systematic review focusing on implant and pros-thesis survival rate indicated no differences betweencement-retained and screw-retained prostheses,6 a morerecent systematic review revealed significantly more bio-logical complications with cement-retained prostheses,whereas screw-retained prostheses demonstratedincreased technical complications.7 Similar findings werepublished by Wittneben et al8 and Millen et al,9 wherescrew-retained restorations were associated with anincreased rate of technical complications. Finite elementanalysis10 and clinical11 studies have indicated similarresults when screw-retained prostheses were associatedwith an increased risk of mechanical complications.A major limitation of cement-retained implant res-torations is the difficulty in removing the excesscement.12,13 Residual cement remnants have beenassociated with peri-implantitis.14-19 To address thislimitation, some authors20-23 have introduced a newdesign of screw-retrievable and cement-retained implantsupported prostheses featuring the combined advantagesof both modes of retention. Nissan et al23 in a clinicalstudy reported that the combination of cement- and
ofessor, Advanced education Program in Implant Dentistry, Department oice, Ventura, Calif.artment of Prosthetic Dental Sciences, College of Dentistry, King Saud Un
L OF PROSTHETIC DENTISTRY
screw-retained implant prosthesis improves the survivalrates of the prosthesis and lowers the cost of mainte-nance without increasing the risk for porcelain fracture orscrew loosening.
The purpose of this article was to describe a digitalworkflow for the fabrication of a combination screw- andcement-retained prosthesis for patients with partialedentulism. The combination prosthesis may offer theadvantages of both retentive mechanisms for the defin-itive implant prosthesis.
TECHNIQUE
1. Inspect the peri-implant soft tissue for any sign ofsoft tissue pathosis. Evaluate periapical radiographsto ensure osseointegration. Evaluate implant mobilityby using either the Perio test device (PerioTest;Siemens AG)24 or resonance frequency analysis.25 Inthe clinical situation, 2 parallel threaded, root formresorbable blast medium (RBM)-surfaced dentalimplants (Hahn Tapered Implants; Glidewell Labo-ratories) were placed at the maxillary left firstpremolar and first molar area.
f Restorative Dentistry, Loma Linda University, Loma Linda, Calif; and
iversity, Riyadh, Saudi Arabia.
535

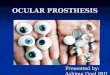
Figure 1. Definitive prosthesis design.
536 Volume 119 Issue 4
TH
2. Make complete-arch definitive impressions of thepatient’s maxillary and mandibular arches withpolyvinyl siloxane impression (PVS) material (GenieVPS; Sultan Healthcare). Make an interocclusal re-cord with PVS occlusal registration material (ExabiteII NSD; GC America Inc). Fabricate the definitivestone cast from Type IV dental stone (Glastone;Dentsply Sirona) after making the definitiveimpression with the intraoral splinting technique.26
3. Place a scanning abutment on the implant analogand scan the impressions (D700; 3Shape). Simulatethe definitive prosthesis with the provided software.Design 2 separate milled titanium abutments and acementable superstructure zirconia prosthesis(Fig. 1). Design the cementable prosthesis with anocclusal access opening so that access to the abut-ment screw can be obtained from the occlusal sur-face (Fig. 2).
4. Mill the titanium abutments from a titanium blank(Inclusive Custom Titanium Abutments Blanks;Glidewell Laboratories) and the cementable super-structure prosthesis from a zirconia blank (BrixZirMilling Blank; Glidewell Laboratories) by using amilling machine (TS150 Milling Solution; IOSTechnologies).
5. Place the milled titanium abutments intraorally. Sealthe occlusal access channels with low-viscosity PVSimpression material (Exafast NDS; GC America, Inc)(Fig. 3A).
6. Position the prosthesis over the abutments (Fig. 3B).Evaluate the interproximal contact areas; and com-plete the prosthesis fit, occlusion, esthetics, andaccessibility for oral hygiene.
7. Place cement (RelyX Luting Plus Cement; 3M ESPE)in the prosthesis and secure the prosthesis over theabutments. Apply pressure and allow sufficient timefor the cement to polymerize (Fig. 4).
8. Clean the excess cement from the occlusal accesschannels and remove the prosthesis (Fig. 5A). The
E JOURNAL OF PROSTHETIC DENTISTRY
prosthesis has now been converted into a screw-retained prosthesis. Remove the excess cementfrom the cervical area of the prosthesis (Fig. 5B).
9. Insert the definitive combination prosthesis intra-orally. Tighten the abutments according to themanufacturer’s recommendations. Confirm occlu-sion and proximal contacts. Place a cotton pellet andcomposite resin (Filtek Supreme Ultra; 3M ESPE) toseal the occlusal access channels (Fig. 6).
DISCUSSION
The primary advantage of a screw-retained design is theease of prosthesis retrievability.1,2 Prosthetic complica-tions can be better addressed when the prosthesis iseasily retrievable. However, cement-retained prostheseshave been documented to offer better esthetics,1,2 betterocclusion,1 and superior passive fit than screw-retrievableprostheses.4,5 Superior passive fit is associated withhigher reduction of stresses on the supporting implantsand strain on the prosthesis.10 Both retentive mecha-nisms are acceptable as long as the clinician can weighthe advantages and limitations of each retentive mech-anism for a specific clinical situation. The suggestedcombination screw- and cement-retained implant-sup-ported prosthesis20-23 combines the advantages of boththe cement and screw retention mechanism, offering anadditional design consideration.
Rajan and Gunaseelan22 introduced the concept offabricating a combination screw- and cement-retainedprosthesis. The concept was first applied for a singleimplant-supported crown where a metal-ceramiccrown was cemented on a cast custom abutment.22
Uludag and Celik20 and Uludag et al21 described theconcept of a combination prosthesis for multiunitimplant restorations where a fixed metal-ceramic par-tial denture was cemented on multiple cast customabutments. The significance of the described method-ology is the implementation of digital technology indesigning and fabricating such a combination pros-thesis. Currently published papers describing thefabrication of a combination prosthesis involve con-ventional cast custom abutments and conventionalmetal-ceramic crowns or multiunit prostheses made ofcast high noble metal.20,21
The described technique is not limited by the avail-ability of a definitive stone cast but can be applied to aclinical situation where an intraoral scanner is usedinstead of a definitive impression. It can also be appliedfor long span prostheses involving multiple abutments,assuming all abutments are designed with axial wallsthat would allow a path of insertion for thesuperstructure.
The described combination prosthesis offers anadvantage compared with an implant-supported zirconia
Proussaefs and AlHelal

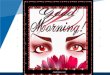
Figure 2. A, Facial view, custom-milled abutments and cementable superstructure prosthesis with occlusal access channels. B, Facial illustration ofdefinitive combination prosthesis.
Figure 3. A, Intraoral view, custom-milled titanium abutments. B, Milled superstructure zirconia prosthesis positioned on custom abutments.
Figure 4. Superstructure prosthesis cemented on abutments.
April 2018 537
fixed partial denture that involves cementation of theprosthesis on prefabricated titanium inserts. Thedescribed combination prosthesis allows the additionof porcelain on the superstructure after the prosthesisis completed. When the interproximal contacts have
Proussaefs and AlHelal
been confirmed, the clinician can then cement thesuperstructure intraorally as described. In contrast, azirconia prosthesis that has cemented prefabricatedtitanium inserts does not allow porcelain applicationafter completion because the high temperature in aporcelain oven would damage the composite resintypically used to cement the titanium inserts. There-fore, if an open contact is observed after fabricating azirconia prosthesis with cemented prefabricated tita-nium inserts, the clinician may have to remake theprosthesis.
A limitation of the described design protocol is thelimited clinical data available to support the imple-mentation of such a protocol on a routine basis. Nissanet al23 published a clinical study that included 274 com-bination prostheses that were observed over a 12-yearperiod. In that study, the abutments were cast customabutments, and the superstructures were metal-ceramicprostheses made of cast high-noble metal. The combi-nation prosthesis demonstrated an improved prostheticsurvival rate and lower cost of maintenance compared
THE JOURNAL OF PROSTHETIC DENTISTRY

Figure 5. A, Definitive combination prosthesis removed. Notice excess cement around cervical area. B, Definitive combination prosthesis aftercement removal.
Figure 6. Definitive combination prosthesis after occlusal accesschannels sealed with composite resin.
538 Volume 119 Issue 4
with a conventionally cemented prosthesis without anocclusal access channel.
Another limitation of the described technique wasthe risk of intraoral locking of the combinationprosthesis during cementation. This can occur if thesupporting implants are not parallel. If nonparallelimplants are restored with a combination prosthesis,nonengaging abutments should be used with a customabutment orientation device. In addition, the describedtechnique may not be used to restore unfavorably placedimplants.
SUMMARY
The proposed technique offers an alternative methodof fabricating a cement- and screw-retained combi-nation prosthesis by implementing digital technology.Long-term human studies are needed to validate theuse of the described technique on a routine clinicalbasis.
THE JOURNAL OF PROSTHETIC DENTISTRY
REFERENCES
1. Hebel KS, Gajjar RC. Cement-retained versus screw-retained implant res-torations: achieving optimal occlusion and esthetics in implant dentistry.J Prosthet Dent 1997;77:28-35.
2. Chee W, Felton DA, Johnson PF, Sullivan DY. Cemented versus screw-retained implant prostheses: which is better? Int J Oral Maxillofac Implants1999;14:137-41.
3. AlHelal A, Kattadiyil MT, Clark JL, AlBader B. Diagnostic classification anddesign considerations for implant-supported fixed partial dentures and screwaccess channel: The ABC/PBC and SAC Classifications. Int J Prosthodont2017;30:490-5.
4. Guichet DL, Caputo AA, Choi H, Sorensen JA. Passivity of fit and marginalopening in screw- or cement-retained implant fixed partial denture designs.Int J Oral Maxillofac Implants 2000;15:239-46.
5. Michalakis KX, Hirayama H, Garefis PD. Cement-retained versus screw-retained implant restorations: a critical review. Int J Oral Maxillofac Implants2003;18:719-28.
6. Weber HP, Sukotjo C. Does the type of implant prosthesis affect outcomes inthe partially edentulous patient? Int J Oral Maxillofac Implants2007;22(suppl):140-72.
7. Sailer I, Mühlemann S, Zwahlen M, Hämmerle CH, Schneider D.Cemented and screw-retained implant reconstructions: a systematic reviewof the survival and complication rates. Clin Oral Implants Res 2012;23:163-201.
8. Wittneben JG, Millen C, Brägger U. Clinical performance of screw- versuscement-retained fixed implant-supported reconstructions: a systematic re-view. Int J Oral Maxillofac Implants 2014;29(suppl):84-98.
9. Millen C, Brägger U, Wittneben JG. Influence of prosthesis type and reten-tion mechanism on complications with fixed implant-supported prostheses:a systematic review applying multivariate analyses. Int J Oral MaxillofacImplants 2015;30:110-24.
10. Silva GC, Cornacchia TM, de Magalhães CS, Bueno AC, Moreira AN.Biomechanical evaluation of screw- and cement-retained implant-supportedprostheses: a nonlinear finite element analysis. J Prosthet Dent 2014;112:1479-88.
11. Nissan J, Narobai D, Gross O, Ghelfan O, Chaushu G. Long-term outcomeof cemented versus screw-retained implant-supported partial restorations.Int J Oral Maxillofac Implants 2011;26:1102-7.
12. Agar JR, Cameron SM, Hughbanks JC, Parker MH. Cement removal fromrestorations luted to titanium abutments with simulated subgingival margins.J Prosthet Dent 1997;78:43-7.
13. Pauletto N, Lahiffe BJ, Walton JN. Complications associated with excesscement around crowns on osseointegrated implants: a clinical report. Int JOral Maxillofac Implants 1999;14:865-8.
14. Behr M, Spitzer A, Preis V, Weng D, Gosau M, Rosentritt M. The extent ofluting agent remnants on titanium and zirconia abutment analogs afterscaling. Int J Oral Maxillofac Implants 2014;29:1185-92.
15. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol2009;80:1388-92.
16. Shapoff CA, Lahey BJ. Crestal bone loss and the consequences of retainedexcess cement around dental implants. Compend Contin Educ Dent 2012;33:94-101.
17. Burbano M, Wilson TG Jr, Valderrama P, Blansett J, Wadhwani CP,Choudhary PK, et al. Characterization of cement particles found in
Proussaefs and AlHelal

April 2018 539
peri-implantitis-affected human biopsy specimens. Int J Oral MaxillofacImplants 2015;30:1168-73.
18. Korsch M, Obst U, Walther W. Cement-associated peri-implantitis: aretrospective clinical observational study of fixed implant-supported resto-rations using a methacrylate cement. Clin Oral Implants Res 2014;25:797-802.
19. Ramer N, Wadhwani C, Kim A, Hershman D. Histologic findings withinperi-implant soft tissue in failed implants secondary to excess cement: reportof two cases and review of literature. N Y State Dent J 2014;80:43-6.
20. Uludag B, Celik G. Fabrication of a cement- and screw-retained multiunitimplant restoration. J Oral Implantol 2006;32:248-50.
21. Uludag B, Ozturk O, Celik G, Goktug G. Fabrication of a retrievable cement-and screw-retained implant-supported zirconium fixed partial denture: a casereport. J Oral Implantol 2008;34:59-62.
22. Rajan M, Gunaseelan R. Fabrication of a cement- and screw-retained implantprosthesis. J Prosthet Dent 2004;92:578-80.
23. Nissan J, Snir D, Rosner O, Kolerman R, Chaushu L, Chaushu G. Reliabilityof retrievable cemented implant-supported prostheses. J Prosthet Dent2016;115:587-91.
24. Teerlinck J, Quirynen M, Darius P, van Steenberghe D. Periotest: an objectiveclinical diagnosis of bone apposition towards implants. Int J Oral MaxillofacImplants 1991;6:55-61.
Noteworthy Abstracts of
Implant utilization and time to prosthetic rehfibular free flap reconstruction of the maxilla
Chuka R, Abdullah W, Rieger J, Nayar S, Seikaly HInt J Prosthodont 2017;30:289-94
Purpose. Precisely designed jaw reconstruction rehabilitationoral functions. Advanced three-dimensional (3D) digital surgpotential to reduce time to reconstructive and dental treatmrehabilitation. This study investigated the use of SDS in JRR
Material and methods. A retrospective chart review was conwho completed JRR treatment with a fibular free flap (FFF)SDS technique (with-SDS) and conventional, nondigitally plosseointegrated implants. Data were collected from adult patiInstitute for Reconstructive Sciences in Medicine (iRSM). Pataining augmentation to the FFF reconstruction. The withoureconstruction followed by nonguided implant placement. Thwith guided implant placement during the reconstructive sur(ratio of implants placed to connected) and time to prosthettest was used to analyze the data.
Results. The digital SDS technique (with-SDS) group computilization of implants as well as a significantly shorter time
Conclusions. SDS allows an interdisciplinary treatment teamgreater efficiency in patient treatment time and utilization o
Reprinted with permission of Quintessence Publishing.
Proussaefs and AlHelal
25. Manzano-Moreno FJ, Herrera-Briones FJ, Bassam T, Vallecillo-Capilla MF,Reyes-Botella C. Factors affecting dental implant stability measured using theOstell Mentor device: a systematic review. Implant Dent 2015;24:565-77.
26. Papaspyridakos P, Lal K, White GS, Weber HP, Gallucci GO. Effect ofsplinted and nonsplinted impression techniques on the accuracy of fit of fixedimplant prostheses in edentulous patients: a comparative study. Int J OralMaxillofac Implants 2011;26:1267-72.
Corresponding author:Dr Periklis ProussaefsAdvanced Education Program in Implant DentistryDepartment of Restorative Dentistry3585 Telegraph Rd, Suite CVentura, CA 93003Email: [email protected]
AcknowledgmentsThe authors thank Dr Abdulrahman Taleb, BDS, for designing the combinationprosthesis sketches.
Copyright © 2017 by the Editorial Council for The Journal of Prosthetic Dentistry.
the Current Literature
abilitation in conventional and advancedand mandible
, Osswald M, Wolfaardt J
(JRR) is important to the integrity of the jaw structure andical design and simulation (SDS) techniques have theent completion, thereby promoting early functional oralprocedures.
ducted on adult head and neck tumor (HNT) participantsreconstruction. Two treatment approaches, advanced 3Danned technique (without-SDS), included the use ofents treated between January 2000 and March 2014 at therticipants were excluded if they underwent a bone-con-t-SDS group underwent a conventional, nonguided FFFe with-SDS group underwent a guided FFF reconstructiongery. The outcome measures included implant utilizationic connection after FFF reconstruction. Mann-Whitney U
leted prosthetic treatment with a significantly higherto prosthetic delivery.
to work together to create a virtual plan that leads tof dental implants.
THE JOURNAL OF PROSTHETIC DENTISTRY
![Intelligent Prosthesis - tams. · PDF fileI Electrooculography (EOG) I Electrocorticogram (EcoG) [ ] Irina Intelligent Prosthesis 4/21. ... Irina Intelligent Prosthesis 21/21](https://img.pdfslide.us/doc/110x75/5aab10c57f8b9aa9488b839d/intelligent-prosthesis-tams-electrooculography-eog-i-electrocorticogram-ecog.jpg)
![INDEX [microdentsystem.com] · INTRODUCTION REMOVABLE AND IMMEDIATE . PROSTHESIS MULTIPLE PROSTHESIS. CEMENTED PROSTHESIS. Microdent Genius conical (straight) abutment or Microdent](https://img.pdfslide.us/doc/110x75/5facd9ef77a5ed547a36b19e/index-introduction-removable-and-immediate-prosthesis-multiple-prosthesis.jpg)