Embed Size (px)
Citation preview

contact n°161/162 - June-July and August-September 19982
THE CMC STORY
In this double issue of Contact, we aredelighted to share with readers “TheCMC Story”. It analyses the work of theChristian Medical Commission in a waywhich reminds us of what has beenachieved and helps us to rethink whereChristian health and healing should beheading in the future.
Over the past 30 years, the CMC haschanged thinking on health both withinthe churches and in the internationalarena. In the early days, it stimulatedthe World Health Organization (WHO)into early discussions about primaryhealth care. Then, by becoming the firstmajor non-governmental organization(NGO) with an official relationship withWHO, it strengthened the foundationsfor a more public and communityoriented approach to internationalhealth policy. Its campaigns – to promotebreastfeeding and to limit “donations”of expired, useless and even danger-ous medicines – have producedchanges in thinking and policy both atWHO and within governments andtransnational corporations.
Most recently, the renamed CMC -Churches’ Action for Health haschanged attitudes within the churchestowards those infected with HIV or
suffering from AIDS. Forseveral years after the epi-demic began, there wasconsiderable prejudice,ignorance and often moralcondemnation in commu-nities and churches. Sincethen, many churches havebecome role models of safeand welcoming centres forthose living with AIDS.
Throughout the years,CMC has helped shapeconcepts of “health”. Manyof the NGOs and networkswhich have evolved morerecently have adopted the“wholistic”, or wholeperson, approach in whichpeace of mind, relation-ships with others, and aperson’s social, economicand cultural situation are
seen as crucial to an understanding ofthe root causes of ill-health. From itsestablishment in 1968, CMC haspromoted a “bottom up”(or people- andcommunity-determined) rather than a“top down” (government service- orhealth professional-determined) model.Today, nearly all justice-minded devel-opment groups have embraced CMC’sfundamental principle of peoples’ par-ticipation in decision making on issuesaffecting their own health and develop-ment. The practical benefits of CMC’sapproach and emphasis have beenrepeatedly documented in Contact.
CMC’s ideals and achievements arehighlighted throughout “The CMCStory”. The final chapter “At the cross-roads” poses questions for the future.Do let us know which ones you feel arethe most important. We would like youto send your comments on the sheetfound on page 53.
The “CMC Story” was written by GillianPaterson, author of “Whose Ministry?”and “Love in a Time of AIDS”, bothWCC publications. Gillian made herwriting a highly participatory process,and I would like to take this opportunityto thank Gillian and others involved indeveloping this issue.
Future of ContactThanks to the tremendous support ofreaders, and particularly to participantsat a WCC meeting in March, Contactwill continue publication. Appearingquarterly (rather than every two months),it will become the responsibility of apartnership of CMAI – the ChristianMedical Association of India; WCC;DIFÄM, the German Institute for MedicalMission in Tübingen; and MCS, theMedical Coordination Secretariat of theNetherlands. From January 1998,Darlena David, who works at CMAI, willtake over as editor, producing her firstissue from the WCC Eighth Assemblyin Harare, Zimbabwe.
Like myself, I am sure all Contact readerswill want to congratulate Darlena on hernew position, and to wish her all thevery best for a very bright future.
Diana SmithEditor
CoverA child’s drawing from WCC’sJustice, Peace and the Integrityof Creation (JPIC) Children’s ArtContest.
BelowChurch community action at theEphisus Church, Katutura,Namibia
Pet
er W
illia
ms/
WC
C
EDITORIAL
contact n°161/162 - June-July and August-September 1998 3
THE CMC STORY
gradually handing over to nationalchurches who are asking to run theirown affairs. In the Roman Catholicchurch, preparing for the SecondVatican Council, the idea of Christianityas a force for change has taken root. AtMedellin, in Colombia, the Bishops’Conference of Latin America sets outthe basis for a renewed theology whichlooks to the oppressed to set the agendafor the people of God. At the WCCAssembly in Uppsala, the Council’s
member churches promise totake a lead in development
and aid, and to give priorityto justice and the voiceof the poor.
Small beginningsIn Geneva, a littlegroup of peoplegathers, called to-gether by the WorldCouncil ofChurches. The
Christian MedicalCommission, under
its first director JamesMcGilvray, has been
charged with the respon-sibility to promote the coordi-
nation of national church-relatedmedical programmes, and to engage instudy and research into the mostappropriate ways in which the churchesmight express their concern for totalhealth care.
But that was then. Thirty years on, it isnow 1998. A new millennium is just overthe horizon. This year, CMC celebratesits thirtieth anniversary. We wish theCMC-Churches’ Action for Health, andall the thousands of people who havebeen involved in its work, a “HappyBirthday”.
THE CMC STORY1968 - 1998
by Gillian Paterson
Happy Birthday!Imagine that it is June 1968. The worldis changing. In Latin America, there is astrong liberationist force struggling totransform authoritarian and unjust struc-tures. In Asia and Africa, colonialism isin retreat. In its wake, it leaves poverty,uncertainty, and in some places civilwar. It leaves governmental, militaryand civil institutions modelled on thoseof the colonialist powers, with westernvalues and expatriate staff. But for allthat, there is optimism. A newand more democratic worldorder is possible. There isthe conviction that thedispossessed will atlast come into theirown. There is the joyof liberation in the air.There is hope.
In the industrialisedcountries of theWest, it is the boom-ing sixties. It wouldbe a happy time, butfor the underlying anxi-ety about the future. Thetides of Empire on the ebb,what will now be the relation-ship between South and North?How does one protect oneself from theideological and military threat from theeastern side of the iron curtain? Andhow to ensure that newly independentcountries in the South do not fall undercommunist influence? The world is fullof hidden dangers. By the end of 1968,Soviet tanks have rolled into Czecho-slovakia and US forces are “defendingdemocracy” in Vietnam.
The churches are changing, too. TheWestern missionary church, so closelytied in with the colonialist agenda, is
WCC memberchurches promiseto take a lead indevelopment andaid.

contact n°161/162 - June-July and August-September 19984
THE CMC STORY
INTRODUCTION
TOWARDS HARARE
where other important changes in self-understanding and internal organiza-tion of the WCC take place.
As part of the restructuring, this doubleissue will be the final edition of Contactto come exclusively from the WCC.From now on, a partnership of the WCCand three Christian health agencies willproduce Contact (see Editorial). So thisis an excellent moment for looking back,not just on past glories, but on pastrealities, and on what, over the years,has made the Christian Medical Com-mission such an exciting family of whichto be a part.
A future roleBut times of change are also momentsfor looking forward, for dreaming dreamsand seeing visions. As the millenniumapproaches, what might the role of aglobal Christian health network be? Thepromotion of the philosophy of primaryhealth care (PHC), which was part ofwhat made the CMC experience such acompelling one in the early days, hasled to disappointments. Its promotionhas not brought about the structuralchanges needed to alleviate the povertythat causes much of the world’s ill-health. Today, the effect of marketforces’ economics in a globalizing worldis increasing the gap between rich andpoor, and the emphasis in PHC is onsustainability and long-term mainte-nance, and on the experience of diggingin for a long struggle.
All the PHC issues remain important.Gender issues and the position ofwomen, disability, rational use of drugs,inequitable use of resources, scarcityof funding: these will continue to beimportant challenges for any organiza-tion concerned with community-based
Today, CMC-Churches’ Action forHealth is at a crossroads. It is part of theWorld Council of Churches (WCC), afellowship of churches from around theworld which is currently taking a radicallook at the way it should be structuringits mission. This involves rethinking theway in which its different priorities relateto each other. Health is structured atpresent within the unit that deals withevangelism, education and mission. Butthere are important connectionsbetween the health agenda and that ofthe units focusing on faith and order,justice and peace, and service andsharing. The new relationships withinWCC should make it possible for itsmember bodies to think about healthand healing from a much broader base.
Thirty years ago, there seemed nothingstrange in big, centralised, Europe-based organizations like WCC settingout to speak for everyone. But the world
has moved on since thoseearly days. Things thatworked well in the late1960s may no longer beappropriate in the late1990s. From now on, theWCC in Geneva will bestructured as acoordinating secretariatwith a minimum staff, inrecognition of the fact thatthe real action – and there-fore the most pressingneed for resources – is atthe regional, national andgrassroots level. TheEighth Assembly of theWCC, which will takeplace in Harare,Zimbabwe, in December1998, will be the place
Street children at WCC’sConference on WorldMission and Evangelism,Bahia, Brazil, November1996.
Chr
is B
lack
/WC
C
As the millenniumapproaches, what might
the role of a globalChristian health
network be?

contact n°161/162 - June-July and August-September 1998 5
INTRODUCTION
health care among poor people. Theyare the challenges which Contactreaders face every day. They are vitallyimportant, and they will always be withus.
But the early excitement of CMCstemmed from the fact that it was athink-tank for ideas. It attracted someextraordinary people, from all over theworld. Some had come from a back-ground in medical mission, seen thelimitations of the mission hospital, andfound themselves swept up in the move-ment to make primary health care hap-pen. Others were theologians, churchpeople, politicians and academics.Today, in most countries, PHC is widelydiscussed and accepted but its under-standing is far from the visionary dreamwhich fired so many with energy andenthusiasm in the early days. Thedisappointments came because manyof the basic principles of PHC (seepage 13) were not taken to heart, oftenresisted by key elements in govern-ments and medical establishments.Most crucially, PHC came to be under-stood as a fragmented series of services– immunization and family planning forexample – instead of a comprehensiveand participatory initiative leading to amajor reallocation of resources.
Which way now?The true prophet always operates fromoutside the system. What are theprophets saying today? Here, on thecusp of change, the time has come tolisten very carefully for the still smallvoices which may just be articulatingthe major themes of the future. Contactreaders will be among those voices.Where will they come from? In recentyears, CMC has taken the lead in WCC’swork on AIDS. Maybe there are voicescoming from the experience of living orworking with HIV which might help setthe agenda for the future. Or how aboutthe Health, Healing and Wholenessstudy of the 1980s? What, in our violent,battered, confused world, do we meantoday, when we talk about the healingministry? Has the moment come,perhaps, to reclaim that ministry for andwith the churches?
After each section of this issue, thereare some suggestions designed to helpyou relate the-story-so-far to your ownsituation, and also some suggestionsfor biblical work which might light upyour thinking. At the end, we have setout the themes and concerns that havebeen identified as concentration pointsfor the CMC family, with the support andspecial guidance of the WCC. Thesehave come up at recent internationalmeetings. We hope you will read themcarefully and we encourage you to writeyour comments on them, or offer othersuggestions. To do this, we haveincluded a response sheet that we inviteyou to send to our Geneva address.Readers’ responses will be used bystaff in discussions with the CMC familyfor the fine-tuning of their own work andfor ideas for themes in Contact or othereducational resources.
At the WCC Assembly in Harare, inDecember, there will be hearings and“padares” or workshops, where the del-egates will report and discuss many ofthe key issues affecting the life andwitness of the churches today. Amongthem, of course, areissues of health andhealing. All thesediscussions willhave a bearing onthe shape of thefuture work of theWCC.
As the WCCrestructures, thecontinuation of thelink with you, yourcommunities andthe people withwhom you work,through Contact,will be essential toour commoninvolvement inhealth and healing.
A beggar and her child in Berlin,Germany
Wol
f K
utna
hors
ky/W
CC
But the early excitementof CMC stemmed fromthe fact that it was athink-tank for ideas.
contact n°161/162 - June-July and August-September 19986
THE CMC STORY
CHAPTER ONE
THE QUEST FOR HEALTH
There were many people working inChristian medical situations whobelieved that there was in fact a uniqueChristian understanding of health andhealing, which should inform and colourthe way the churches handled thecurrent time of change. In 1964, WCCand the Lutheran World Federation(LWF) decided to sponsor a consulta-tion on these issues. In parallel, theyinitiated a series of surveys which woulddo two things. First they would discoverthe relevance of Christian medical workto the existing needs of people in thedeveloping world; and then they wouldlook at the relevance of this work to thechurches themselves at local andnational level.
The first consultation – taking place in1963 at DIFÄM (German Institute forMedical Mission) – came to be knownas Tübingen I. Having reached theconclusion that health care was morethan mission hospitals, it set in motiona process aimed at establishing what,in a post-colonialist world, the role of“medical mission” might be.
Tübingen I recognised that theChristian gospel was more concernedwith the sick person than with theparticular sickness and that the sickperson was part of an environmentand a community which also stood inneed of healing.James McGilvray, first Director of CMC
The report that emerged from thismeeting was called The Healing Church(WCC 1965). From the regional consul-tations that followed the first Tübingenmeeting, and from the surveys commis-sioned by WCC and LWF in 1963, camethe evidence that set the agenda for thesecond Tübingen meeting in 1967, andultimately for the Christian MedicalCommission itself.
Writing a history of the Christian Medi-cal Commission is a confusing experi-ence until you have grasped one veryimportant fact: that certain key, agenda-setting things happened before theCommission itself existed.
The young CMC was born out of a longhistory of Christian involvement in healthcare. For over a hundred years, medicalwork had provided one of the mainfocuses for Christian missionary work,the others being education and churchplanting. As a result, there were morethan 1,200 Christian hospitals in theworld relating to member churches ofWCC alone. What, if any, was thestrategy behind their work? What wasthe healing ministry basically for? Wasit a means of making converts? WereChristian health professionals just fillinggaps in locations (for example by pro-viding services in remote rural areas)and specialities (leprosy, for instance)which were unattractive to others?
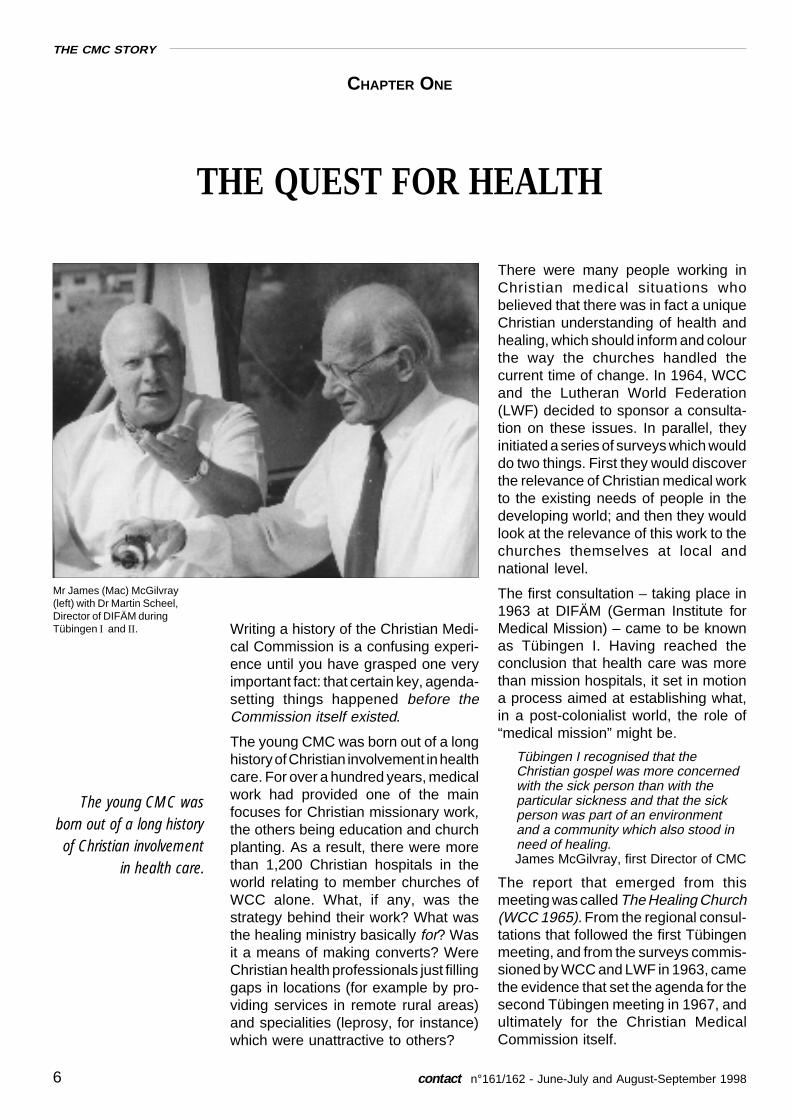
Mr James (Mac) McGilvray(left) with Dr Martin Scheel,Director of DIFÄM duringTübingen I and II.
The young CMC wasborn out of a long historyof Christian involvement
in health care.

contact n°161/162 - June-July and August-September 1998 7
The first group of country-wide surveys,that led to CMC’s formation, wererequested by the Protestant churchesof Kenya, Uganda and Nigeria. Theywere closely followed by Malawi, whereby happy chance the Roman Catholicchurch was also involved. Then cameCameroon and Indonesia, and thenIndia, and so on. The Quest for Healthand Wholeness, James McGilvray’soutstanding account of the 1960s and1970s, contains a detailed report of thefindings of these surveys. But in anutshell, what they found was thefollowing:
• The churches collectively were makinga considerable contribution to thecountries’ medical facilities (for exam-ple 43% in Tanzania, 26% in Taiwan,13% in Pakistan).
• Governments, in formulating devel-opment plans, tended to ignore thecontribution of the churches, claimingthat the lack of coordination betweenthe churches made it impossible towork with them.
• Ninety-five per cent of the churches'medical activities were focused roundcurative services in hospitals andclinics, run mainly on Western models.Little was being done to promotehealth and prevent disease.
• The cost of operating these institu-tions was increasing annually by aboutfour times the increase in per capitaincome. As a result, higher fees hadto be charged, and the servicesbecame inaccessible to the poorestpeople.
• The location of the units tended to bedetermined not by health needs butby proximity to ecclesiastical (church)headquarters, leading to duplication.
In a word, there was an urgent need, inrelation to medical provision, for col-laboration and cooperation between thechurches at national level so that scarceresources could be used more effec-tively, and negotiations with govern-ments made possible. The currentmultiplicity of bi-lateral relationshipsbetween individual churches and “their”mission agencies, “their” hospitals was
exacerbating divisions at country level.Unless there was some kind of ration-alisation of efforts, the bulk of theirprogrammes would, before long, faceclosure.
The brief for the second Tübingen con-sultation, held in 1967, was to explorethe relationship between healing andsalvation. But the 1960s had seen anexplosion of interest in medicine in thedeveloping world; there was greaterunderstanding of the significance forthe health agenda of socio-economicfactors; and participants had far moredata – more, at any rate than those whotook part in Tübingen I – to enable themto evaluate the actual role of the churchin this field. The discussions that tookplace at Tübingen II, therefore, weremuch more concerned with finding arole for the church itself to play in anexciting and fast developing story.Bishop Ian Ramsey commented thatthey seemed to have invented anentirely new, liberated process for theo-logical reflection, grappling with theproblems and issues implicit in thecontext, allowing new insights toemerge, allowing these insights to throwlight on the gospel, then bringing thisillumination to bear on the particularproblems before them.
The report, when it came, was entitledHealth - Theological and Medical Per-spectives. It consisted of just five papers,of which shortened versions areincluded in the back of James
1 - THE QUEST FOR HEALTH
There was greaterunderstanding of thesignificance for thehealth agenda of socio-economic factors.
Girls and women in CentralAmerica demonstrate for healthand work.
Sea
n S
prag
ue/P
anos
pho
tos
contact n°161/162 - June-July and August-September 19988
THE CMC STORY
McGilvray’s The Quest for Health andWholeness. They were On Death by aphysician and religious sister, SisterMary Luke; Health and the Congrega-tion by Dr R A Lambourne; The Sacra-ments in the Church by Dr David Jenkins,theologian; Implications for Medicineby Dr T F Davey, a physician; and TheMedicine of Poverty by Dr Aart H vonSoest, a physician. Between them, with-out providing real answers, thesevisionary papers set the agenda for theChristian Medical Commission, whichstarted work, a year later in May 1968.
For discussion: Isaiah 61, 1-6. It gives people greatconfidence when they believe they are doing God'swill, particularly if it is a group of people workingtogether. How would you know if the spirit of the Lordwas upon you? Does the passage give any clues?Have you ever felt like that?
Prophet and broker
CMC’s importance was determined bythe fact that it came around at the righttime and it was possible to utilise the“kairos” of that time. New independentnations and churches in the former“mission lands” made it imperative tofind new solutions for the healingmission of the churches and theCHURCH. Handling the medicalmission heritage dominated during thefirst years.
Hakan Hellberg, 1998
The first meeting of the Christian Medi-cal Commission took place, in Geneva,in September 1968. CMC had an initialfive year mandate. In effect, it was to beboth prophet and broker. It had first toidentify and communicate the vision,and then to enable it to happen. Itstasks were:
a) to help the churches in their searchfor a Christian understanding ofhealth and healing
b) to promote innovative approachesto health care
c) to encourage church-related healthcare programmes to collaborate witheach other.
The statement that came out of thatmeeting was called The Commission’sUnderstanding of its Task, and much ofit is as relevant today as it was thirtyyears ago. Here is the first paragraph:
“While we are justifiably entitled topride in reviewing the legacy ofChristian medical work, we realise thatsome of the earlier initiatives are nolonger open to us and that we mustsearch for a new relevance today. Partof what was distinctive in Christianmedical programmes was theirpioneering nature – in offering medicalcare to those who otherwise would bedestitute. However, today, govern-ments and secular services are in-creasingly offering such services, andwe must discover how our pro-grammes can be coordinated withtheirs. This is not to say that thepioneering aspect of our services isover. There are whole new dimensionsof pioneering possibilities which arestill open to us. Yet in the discovery ofthem we must always be aware thatrelevance is always relative. What isrelevant today may be quite irrelevantin the days to come, and so we mustalways be open to renewal as wesearch for the appropriate ways inwhich the church can bring healingand wholeness to man.”
Nine main priority areas were identi-fied:
• Comprehensive health care• Community organization• Cooperation with governments and
other agencies• Inter-church coordination and coop-
eration• Planning mechanisms appropriately
structured in regional and localorganizations
• Re-orientation of personnel• Need for administrative reorganiza-
tion• Data systems• Facing the problems of population
dynamics.
And so the search for programmesbegan. CMC had a tiny staff and nofunds to hand out. It was an enablingand supporting organization. When itidentified an innovative programme, itwould use the Commission’s contactsto get funding for its work, and put itsorganizers in touch with people doingsimilar work elsewhere.
It difficult for us, today, to understandwhy the desirability of its objectives wasnot more obvious at the time. In manycountries, in the 1950s, the principle of
THE CMC STORY
CMC had first to identifyand communicate the
vision, and thento enable it to happen.

contact n°161/162 - June-July and August-September 1998 9
“letting the people choose” was alreadyaccepted. In West Africa, India andelsewhere, there had been an empha-sis on the establishment of basic healthservices in terms of village clinics, healthcentres and dispensaries. But in the1960s and 1970s, the aid programmesof western governments were stillgeared to the creation of big hospitalsand medical schools. Mulago (the hos-pital and medical college of MakerereUniversity in Kampala, Uganda) was agift from Britain; in Liberia, the John FKennedy Memorial Hospital was givenby the government of the USA. Thesehospitals absorbed a large part of thehealth budgets of both countries, pre-venting the development of more localhealth services that might have helpedpoor people; and then, because therewas no effective filtering process, theybecame in effect the district hospitalsfor the capital cities, Kampala andMonrovia. All over the world, the “top-down” mind-set turned out to be hard toshift, primarily, one suspects, becauseit protected the professionals andbecause the people who made thedecisions benefited from it.
Then in the early-1970s, news startedto emerge from China of a revolution-ary new medical system which startedat the base, with health workers cho-sen by the community. It set out toensure that medical care would be avail-able to all. Contact devoted an entireissue to “China and the less developednations” in December 1972. It con-cluded that “many third world nationshave followed patterns of developmentwhich have better suited the demandsof former colonial masters rather thantheir own present needs.” The Chinesealternative, it suggested, stressed ruralrather than urban health care, preven-tive rather than curative services, andthe use of medical auxiliaries as ameans of supporting highly traineddoctors. But the new system was partlydiscounted in the West. How could a“barefoot doctor” with no medical edu-cation do a proper job? How couldquality be maintained in this situation?Western governments came readily tothe conclusion that such an approach
could function only in a system verydifferent from their own.
Those who were involved with CMC atthe time describe vividly the tremen-dous excitement of those early days,the sense of adventure, of being at theforefront of a movement that seemedset to change the world. Its aim was thereorientation of Christian medical worktowards health care that started with thecommunity, and which focused on pre-ventive activities as much as thetreatment of disease. This would bedone through the creation of structuresand practices that would enable nationaland local churches to collaborate, bothwith one another and with governments.What did this look like in practice? Thestory of Jamkhed is an example (seebox next page).
Today, this style of working is so familiarthat it is hard for young professionals toimagine the newness and excitement ofit all to those who were involved.
“I knew that health work was morethan tablets and operations. But I feltisolated in that knowledge until oneday, in the mail, I received the 1968Tübingen report. It sought to bringback the spiritual role of healing, and itmade connections between the mis-sion of the church and what goes on inhealth care. It confirmed my belief thatthe roots of suffering are in the com-munity. Those pioneering days were soexciting. We felt we were part of aworld-wide movement that would
1 - THE QUEST FOR HEALTH
The Chinese alternative,it suggested, stressedrural rather than urbanhealth care, preventiverather than curativeservices, and the use ofmedical auxiliaries as ameans of supportinghighly trained doctors.
A barefoot doctor (left) servingthe family of a rural herdsman.

contact n°161/162 - June-July and August-September 199810
THE CMC STORY
Jamkhed, Maharashtra: a new experience in Christian medical work in India
other illnesses, thus reducing the stigma attachedto the condition.
The logical next step was to have a village healthworker in every community. But young auxiliarynurse midwives did not like going and living in thevillages. Their level of achievement was thereforerelatively low, although their pay was substantial.Furthermore, there was no real need for highlyspecialised people to do this work. The factorsresponsible for ill-health in rural areas are not tech-nically complex. A high degree of trust in the healthworker is far more important than literacy or ascientific education, either of which is likely todistance the health worker from the people. As onemember of the team put it, “I can teach a chimpanzeehow to give an injection, but I need human beings togo to the villages and change attitudes towardshealth.” So the Aroles asked the village councilsthemselves to propose suitable middle-aged women,who would receive training in Jamkhed, work withfamilies and children, and liaise with the health teamon its regular visits.
There were no western-style health services in thearea when the Aroles arrived, but there was aninfrastructure of indigenous practitioners who wouldnormally have been rebuffed by allopathic practi-tioners, whom they would see as a threat to theirlivelihood. The Aroles established a rapport withthis network, treating them as colleagues and usingthem as consultants, so that eventually the indig-enous practitioners became part of the health team.
Jamkhed is a small market town, the centre of apoor rural area in central India. Mabelle andRajanikant Arole arrived there in 1969, havingagreed with community leaders to explore the pos-sibility of setting up a community-based healthprogramme in the thirty villages in the surroundingarea. Four years working in a rural hospital hadconvinced them that all they were doing was treatingthe individuals who came to the door, and doingnothing for the health of the surrounding commu-nity. Seventy per cent of the illnesses they treatedwere preventable, and large numbers of the patients“cured” were going home to the environment thatcaused the problem in the first place, and thenreturning to the hospital with the same illness. “Thisrepetitive pattern of simple preventable illnesses,”they said, “could not be changed by the hospitaleven though it was situated in the heart of the ruralarea.”
In effect, the hospital appeared to be offering asolution to health problems, then failing to fulfil thatpromise, but in the process preventing the peoplefrom working out ways of improving their own health.In Jamkhed, agreement was reached with commu-nity leaders to spend six months “testing” thecommunities’ willingness to solve its own problems.
Health – a low priorityThe Aroles had been amazed to discover, in talkingto local people, how low a priority health care wasfor them. Their greatest felt need was for food andwater, schooling for children, and adequate roadsfor taking surplus produce to market. There was adrought at the time, so they raised money to financethe digging of deep tube-wells fitted with handpumps, and villagers started poultry and dairyschemes. In the meantime they were recruiting andtraining local staff, and trying to identify and contactall indigenous practitioners and health workers inthe area. They developed mobile health teams,consisting of a doctor, nurse supervisor, socialworker, nurse midwife, driver, paramedical workerand village health worker.
These mobile teams proved to be hugely beneficialin terms of health promotion, health education,mother and child care, treatment of children withdiarrhoea, immediate response to local emergen-cies and epidemics. They identified cases of tuber-culosis and leprosy, which were treated alongside
Young, local women involved in communityhealth work.

contact n°161/162 - June-July and August-September 1998 11
change everything. Being in contactwith other people who thought thesame thing made it possible to developwhat was in effect a “hospital withoutwalls”.
Bert Supit, Director of the ChurchHospital in the Christian Evangelical
Church, Tomohon, Indonesia
For discussion: Romans 8, 31-end. St Paul makes it allsound easy. Think about times when things go wrong.How would you make sense of this passage?
Getting the act togetherDame Nita Barrow, subsequentlyGovernor General of Barbados,describes a survey of the Christianhealth centres in Malawi. Dr HastingsBanda, the President, was trying to setup a national plan for hospitals andhealth centres. Church hospitals werenot involved, in spite of the fact that theywere among the best equipped in thecountry. Why was this, she asked DrBanda. “How,” he replied, “do you talkto twenty-nine people who do not eventalk to each other over their own backfences?”
“What began as an exercise limited tothe Protestant churches quicklybecame ecumenical when the sur-veyor was asked by a Catholic bishopif he would include their institutions inthe study. With the approval of theNational Council of Churches, he didso.
..... At the conclusion of the survey,those whose institutions had beenexamined were asked to assemble tohear the results of the study and itsrecommendations, The first of thesewas that they disregard the labels ontheir doors because labels never curedanyone but tended to inhibit dialogue.It was further recommended that theyshould form an association to co-ordinate their activities and engage injoint planning amongst themselvesand, collectively, with government.”
CMC report of the Third Conferencefor Coordinators of Church-relatedHealth Work in Africa, Mombasa,
Kenya, 1975
An important part of the challenge toCMC in the 1970s was to create moreeffective national structures for Christianmedical work. Working in the Philippinesin the 1950s, James McGilvray hadexperienced the benefits of cooperationbetween the programmes of differentchurches. In India, there had been afellowship of doctors since 1905, but
the Medical Association of India did notadmit non-whites until 1950. Amongchurch-related health professionalsthere was already considerable experi-ence of productive collaboration.
As a result of the Malawian experience,a “coordinating agency for church-related health work” was established.With the encouragement of CMC, it wasfollowed by similar groups: in 1967 theChurch Hospital Association of Ghana(CHAG), in 1968 the Medical Associa-tion of Zambia, the Association ofRhodesian (now Zimbabwean) Church-related Hospitals (ZACH), the Associa-tion of Medical Missions in Botswana(AMMB), the Church Hospital Associa-tion of Nigeria (CHAN) and so on. InIndia, where the Christian MedicalAssociation of India (CMAI) and theCatholic Health Association (CHA)already existed, the two bodies cametogether to form the CoordinatingAgency for Health Planning.
Of course not all countries wanted toestablish formal links of this kind. Butthe benefits, where it did happen, wereenormous. They included the following:
• joining together to pressure govern-ments to grant import duty exemp-tions to voluntary agencies
• cheaper pharmaceutical suppliesthrough bulk buying
• provision of a platform for influencinggovernments and other NGOs, andlobbying governments on politicalissues
1 - THE QUEST FOR HEALTH
A mother weights her baby atPhebe hospital, Bong County,
northern Liberia. The hospital isa long-standing member of theChristian Health Association of
Liberia(CHAL).
Jona
s E
stro
mer
/WC
C
contact n°161/162 - June-July and August-September 199812
THE CMC STORY
• avoidance of wasteful duplication andcompetition
• working together on training and otherissues.
One great advantage of collaborationat this level was how often it broughtProtestant and Roman Catholicagencies together: something whichwas proving less easy at the interna-tional level. There had been strongCatholic involvement in the earlydebates, and in particular at the second
Tübingen consultationin 1967. Today, spon-sored by the PontificalCouncil promotingChristian Unity, there isa Roman Catholic staffmember in the missionteam of the WCC sec-retariat in Geneva. Atpresent this post is heldby a Columban sister,Elizabeth Moran, with amandate that is generalenough to allow a verywide range of involve-ment and activity.
For discussion: Genesis 11,1-9.Not being able to talk togetherover the fence of the back yardwas God’s punishment to hu-man beings for building theTower of Babel. Are there or-ganizations or people you donot communicate with? Can youwork out why? Would Jesusapprove or not?
Establishing ContactContact has always been a numberone priority programme for CMC. It isimpossible to over-emphasise theimportance it has had in promotingprimary health care and, in particular,encouraging communities to participatein building primary health care serv-ices. It has created links between peo-ple all over the world – Christian andnon-Christian – who are involved in it.
My first knowledge of CMC wasthrough the publication Contact. Theissue on rural health quoting from aChinese writer “Go to the people, learnfrom them” became an inspiration forme. It redirected my understanding ofthe practice of medicine since I tookthis as a “hermeneutic principle” in my
personal transformation.Dr Erlinda Senturias
CMC’s most valuable and influentialwork was through Contact. Every-where I have gone to represent CMCI have heard testimony to the extraor-dinary value of the publication.
Sylvia Talbot, Moderator of CMC1975-83
In the early days of CMC, primary healthcare was new and the small stepsforward needed to be shared widely.Having identified key programmes, thechallenge was how to make them inter-nationally known. And so, in November1970, Contact was born, initially as anoccasional paper with a circulation of afew hundred copies. At first it was allhand-typed and printed from metalplates. By the mid-1970s, French andSpanish translations were beingpublished, and circulation reached10,000 by 1976. It has since developedinto a popular bi-monthly magazine infour languages (English, French,Spanish and Portuguese), with a currentcirculation of about 15,000. Occasionalissues were translated into Arabic andKiswahili during the 1980s.
From the start, Contact has empha-sised the varied aspects of the commu-nity’s involvement in health. It wasdirected primarily at health workers,especially those working in churchhealth programmes, government pro-grammes, NGOs and communityorganizations. Today, it remains aunique international publication in thatit combines ethical values with practicalexamples of community action to solveproblems in health care. Each issuefocuses on a particular theme (forinstance, empowerment of women,financing health care, the rational useof drugs), with a main article supportedby local experiences from different partsof the world. Contact also has a popularcorrespondence column, and a list ofupdated resources and addresses.
Why are we not able to produceexcellent things like this one done bythat little outfit across the fields?*
Halfdan Mahler, Director General ofWorld Health Organization,
speaking to his staff
*WHO headquarters is situated very closeby the WCCEcumenical Centre.
Front cover of Contact 25,Primary Health Care and theVillage Health Worker,February 1975

contact n°161/162 - June-July and August-September 1998 13
For discussion: Luke 28, 1-8. The two Marys broughtgood news to the disciples. At the end of the chapter,Jesus tells his followers to go out and teach all nations.What would be “good news” to you? Does it matter howor by whom it is communicated? Do you have goodnews to share with others? Why was Contact sosuccessful?
The church mouse and thearchbishopOn 22 March 1974, Dr Halfdan Mahler,Director-General of the World HealthOrganization (WHO), called togethersenior staff for a joint meeting with (allfive!) senior staff of the Christian MedicalCommission. As a result of this meeting,a joint committee was set up to explorethe possibilities of collaboration andcooperation in “matters of mutualconcern”. Returning from this meeting,commenting on the bureaucraticatmosphere they had encountered atWHO, “Mac” McGilvray said to hiscolleagues, “I felt like a church mouse infront of an archbishop”.
In spite of the disparity in size, therelationship between the two organiza-tions turned out to be exceptionallyfruitful. For a long time Mahler, McGilvrayand Lesslie Newbigin (later Bishop ofMadras) met for weekly lunch, to keepup to date with what was going on theother side of the field. The joint WHO/
UNICEF paper “Alternative approachesto meeting basic health needs ofpopulations in developing countries”included some experimental workassociated with CMC. In Ken Newell’sHealth by the People, a key bookpublished by WHO in 1975, four out ofthe ten examples were CMC-affiliatedprogrammes, ensuring that CMC’sphilosophy reached a much wideraudience than the Commission’s usualconstituency. But the most significantresult of the CMC/WHO relationshipwas the formulation by WHO, in 1975,of the principles of primary health care.This marked a radical shift in WHOpriorities, with massive implications forhealth care systems everywhere.
At WHO’s 1976 Assembly, Dr Mahlercalled for the use of primary healthmethodology to make health servicesavailable to all by the year 2000, andoffered the facilities of WHO to analyzethe problems of each country, so as toenable the development of healthpolicies and targets which would helpnational governments to achieve thisgoal. This proposal was adopted, andbecame the subject of the InternationalConference on Primary Health Care
1 - THE QUEST FOR HEALTH
The Principles of Primary Health Care (WHO 1975)
services for both the communityand the individual;
(v) All health interventions should beundertaken at the most peripheralpracticable level of the healthservices by the worker most simplytrained for this activity;
(vi) Other echelons of services shouldbe designed in support of theneeds of the peripheral level,especially as this pertains to tech-nical, supply, supervisory andreferral support;
(vii)Primary health services should befully integrated with the servicesof the other sectors involved incommunity development (agricul-ture, education, public works,housing and communication).
(i) Primary health care should beshaped around the life patterns ofthe population it should serve;
(ii) A local population should beactively involved in the formula-tion of health care activities sothat health care can be broughtinto line with local needs andpriorities;
(iii) Health care offered should placea maximum reliance on availablecommunity resources, especiallythose which have hithertoremained untapped, and shouldremain within the stringent costlimitations that are often present;
(iv) Primary health care should be anintegrated approach of preven-tive, curative and promotive
Dr Halfdan Mahler, FormerDirector-General of the World
Health Organization
T F
arka
s/W
CC
“I felt like a churchmouse in front of onarchbishop.”

contact n°161/162 - June-July and August-September 199814
THE CMC STORY
held in Alma Ata in the USSR inSeptember 1978. CMC was closelyinvolved in the planning, and many ofthe presentations came from membersof the CMC family.
In this process, WHO was trying todevelop a simple and easily under-standable methodology, which couldbe replicated, and which carried a stampof approval which might make it accept-able to governments. But making PHCuniversal through government pro-grammes created its own problems.The original vision of PHC had been asa force for liberation and empowermentthrough the promotion of health care.Once it had been watered down tomethodology acceptable to govern-ments, it could no longer address keyissues such as corruption and oppres-sive systems. Governments interpretedplacing “maximum reliance on avail-able community resources” as a meansof saving costs. The controversy overwhether PHC was an alternative to hos-pitals took the debate away from themore important issue of how “otherechelons of services should be designedin support of the needs of the peripheral
level”.
Acceptance of PHCWHO’s approach wasimmediately adoptedby the government ofSudan, then, withlocal modification, byGuinea-Bissau andCape Verde. Manyother countries fol-lowed, but few gov-ernments allocatedthe necessary fundsand political will tocreate real change. Inthe Philippines, forexample, the Depart-ment of Health organ-ized a one-off, three-day programme forBarangay healthworkers who would beresponsible for thehealth of the villages.
Meanwhile, CMC and other NGOs madeevery effort to promote the originalconcept emphasising the need for com-munity involvement and the need todraw in other sections, such as agricul-tural and education. However, graduallyPHC came to be a top-down govern-ment approach rather than bottom-uppeoples’ initiative.
Warning sounds about how PHC wouldwork in practice were made early on. In1975, the Christian Medical Commis-sion invited Dr (now Professor) CharlesElliot, a priest and economist, to addressits annual meeting. He entitled his talk‘Is Primary Health Care the New Priority?Yes, but......’ It is printed in full in ContactIssue 28.
Over twenty years on, Dr Elliott’sconcerns ring many bells. He hadserious reservations about the ability ofPHC to bring health care within reach ofthe millions who were currently deniedit. He doubted whether equality ofaccess to health care resources wouldever be a realistic objective. He warnedof the dangers of PHC methodologiespredicting that they would becomeinstitutionalised in a way that preventedPHC from reaching the poorest; thathealth is not in fact stated as a highpriority by most communities; that ablepeople want to get on in life, and PHCmade no provision for upward mobilityamong newly skilled health workers;and that without fundamental changein the budgetary allocations of govern-ments, the structure of health servicesand the training of health professionals,it was unlikely that “other echelons ofthe service” would ever be designed “insupport of the needs of the base”. Whatwas more likely was that the existingtwo-tier system would be strengthened,with the minority having access to high-cost technology while the poor majoritygot primary health care.
For discussion: Daniel 1, 3-20. Why is KingNebuchadnezzar favouring these young men in thisway? He clearly believes that everything Babylonian isbetter than everything Israelite. Does this belief ringany bells in your own experience? How important is it,and for whom, to convince the king that their way isbetter?
A community health worker inYamblo village, Sudan
contact n°161/162 - June-July and August-September 1998 15
2 - A CHRISTIAN MEDICAL COMMISSION
CHAPTER TWO
A CHRISTIAN MEDICAL COMMISSION
The third issue wasthe extreme difficultyof changing people'sattitudes to healthwithout engaging withother political, socio-logical and culturalissues as well.People's feelingsabout their bodies arerooted in values,beliefs and spiritual-ity that are part of ourcultural identity.Change may meetresistance from – andalso have implica-tions for – the wholepolitical and culturalcontext in which peo-ple live. As Christians,therefore, we shouldnot be saying we wantto reform ourapproach to healthunless we are also willing to addressthe church's failure to engage with thestruggle to reform society.
I think one trouble with us Christians isthat we imagine that we are a healedcommunity because Christ is whole.We also imagine that we can healothers although remaining sick our-selves, perhaps without noticing itwhile everyone else does notice.
Archbishop Anthony Bloom,Metropolitan of Sourozhm
The group's first debate focused onpossible starting points for discussion.Where should you begin? With theproblems of the world, or with the Bible?“The Bible,” said one participant, “doesnot portray the discovery of God's willand calling through being biblical. Itdisplays such discoveries through facing
Why Christian?In the preface to the first Commissionmeeting in 1968, the then director,James McGilvray wrote: “The CMCcame into being as a focus of twoconverging interests, one functional andone theological.” The functional concernwe have dealt with in the first chapter.The theological concern was that theCommission should seek new insightsinto the interconnections betweenhealing, the Gospel and the mission ofthe churches. Eight years later, inreviewing the Commission's progress,members felt that they had done quitewell with the functional without any com-parable progress in clarifying what mightbe unique in Christian understandingsof health and healing.
As a contribution to the Commission'sstudy, a small group of participants hadstarted to meet at DIFÄM in Tübingen.Their discussions focused on threeissues. The first was the unease thatwas felt in promoting more egalitarianhealth policies for the developing world,when there was virtually no expectationthat the industrialised nations wouldfollow suit or set an example.
Second, the congregations of churchesthemselves were failing to engage withpeople in their present suffering. It wasfurther felt that the actual systems andpractices of parish life, worship andtraining did not often make suchengagement easy. For the participantsin the Tübingen group, this was aproblem. They believed profoundly thatthe way to true health and wholenesslay in the salvation offered by JesusChrist, but they saw the churches them-selves failing to communicate this mostimportant message.
Woman in a Presbyterian chapelin Chimaltenango, Guatemala,
carrying a bible on her head.
Change may meetresistance from – andalso have implicationsfor – the wholepolitical and culturalcontext in whichpeople live.
contact n°161/162 - June-July and August-September 199816
THE CMC STORY
up to problems in the contemporaryhistory and experience of society,responded to in the light of insightsderived from the tradition and life of thepeople of God.” It was agreed that thetask of this study group would be tofocus on the existing situation in medi-cine and health care and to scrutinise itin the light of a Christian understandingof human nature, and what the Biblehas to say about health and healing.Their first position paper was called“The Mission and Service of the Churchin Sickness and Health Care.”
It is difficult to overestimate the impor-tance of this dialogue. Given the generalfeeling that CMC had concentrated toosingle-mindedly on the promotion ofPHC, these discussions enabled theCommission to enter the 1980s with amuch more deliberate focus on theexploration of the theological implica-tions of health care. This explorationhas been a major thrust for theCommission ever since.
That this new focus was so generallywelcomed was due, in part, to the factthat WCC and its member churcheshad become convinced that the work ofCMC and its friends had an importancewhich extended far beyond the provisionof health services in the developingworld. The ideas they were promotingrang bells in other quarters, too. Theyhad implications for the identity of the
church itself and the history of thekingdom of God.
The last word in this section must comefrom Charles Elliott. “We have a lot incommon with WHO,” he said, “but ourultimate aims are not the same. For aChristian organization to ignore theimportance of the spiritual dimension ofhealth is for it to ignore the really crucialinput it has to make to the debate aboutthe nature of healing. Health is morethan medicine. It is to do with the wayyou live and the way you die, the qualityof life and the quality of death. Theultimate answer to disease lies in a wayof life – a life of surrender and obedi-ence that leads to wholeness.”
The interesting thing is that WHO, today,is coming to agree.
For discussion: Acts 5, 12-16. From the earliest times,belief in Christ has been associated with health andhealing. What does this mean for you? Is it possible forthe spiritual aspects of your work to become submergedby the urgency of getting the job done? Try relating theconcerns set out in paragraphs 2 and 3 of this sectionto you own experience of the church.
The Jenkins/Bryant dialogues
There is a crisis in medicine, to thepoint at which some people are sayingthat healing lies outside the medicalprofession, and that doctors are theones who oppose true health. There isa crisis for the church, with somesaying that the real church lies outsidethe church. And there is a crisis in theconsciousness of many Christiandoctors, nurses, teachers and socialworkers who believe there is truth inChrist, in Bible and Christian religion,and yet find that what seems toenlighten them in their chosen workand in their personal lives is somethingelse; hence they go through lifedivided.
R A Lambourne, 1969 (first printed inContact Issue 1)
The Christian Medical Commission wasborn out of a belief that there is some-thing peculiarly Christian about thebusiness of health and healing. Jesushealed. The beneficiaries of his ministrywere not primarily the rich or the strong,although these were by no means ex-cluded: they were the poor, the sick, thestigmatised, the disabled. Since theMiddle Ages (European history between472 and 1453), then, the establishment
Seen near Juba, Sudan.
Pet
er W
illia
ms/
WC
C
The work of CMC and itsfriends had an
importance whichextended far beyond
the provision ofhealth services in the
developing world.

contact n°161/162 - June-July and August-September 1998 17
and maintenance of institutions to carefor the sick had been a priority for theWestern church. Medical work had beena major thrust of Christian mission inAfrica, Asia and Latin America.
All over the world, though, it seemedthe churches' health work had some-how become divorced from the life ofthe congregations of Christians whogathered in churches on Sundays.Christians saw it as their task to raisemoney to support it. They did not expectto get involved with it themselves. Thatwas for the doctors, nurses and teacherswhose job it was to do it. The churchhad in effect “contracted out” its caringrole to professionals and told them toget on with it as best they could. As aresult, the local church was in danger ofbecoming a ghetto, while the front-lineof Christian encounter with the worldwas somewhere else. The consequencewas an increasingly privatised religionthat had nothing very much to do withwhat was happening in the world, whilemembers of the so-called caring pro-fessions, many of whom came to thework with strongly Christian motivation,found it impossible to bring their profes-sional concerns into the arena of theworshipping community. Further, therewas much work to be done on the
development of a theology of healing:one that took seriously the relationshipbetween the structures of health careand the kingdom of God.
Technology is to do with problemsolving but theology is to do with livingwith problems.
David Jenkins, CMC annual meeting1969
It had always been part of CMC'smandate that it should address theseissues, which formed the subject matterof the second Tübingen consultation in1967. In the early 1970s, the Commis-sion's annual meetings opened with anon-going dialogue between Dr JackBryant, Moderator of CMC, and theBritish theologian Dr David Jenkins (laterBishop of Durham) who at that time wasworking for WCC. First Jack Bryantchallenged Dr Jenkins to set out whatthe discipline of theology had to offer tophysicians having to make life and deathdecisions about priorities in health work.Once, the hospital had provided a frame-work for these. What does it mean for aphysician to be responsible for a ruralarea of – say – 100,000 people in 100villages? Our care for individuals oftenresults in the neglect of many times thatnumber. Is there such a thing as “statis-tical compassion” and what is its theo-logical equivalent? In trying to providehealth care for large numbers of peopleon limited resources, what are the theo-logical concepts that will give thedecision makers a system of human
2 - A CHRISTIAN MEDICAL COMMISSION
Dr David Jenkins at a recentCMC meeting in London. Withhim are CMC/WCC Commis-sioners, Mrs Marion Morgan,
Executive director of ChristianHealth Association of Sierra
Leone (CHASL) and Ms GwenCrawley.
Dia
na S
mith
There was much workto be done on... therelationship betweenthe structures ofhealth care and thekingdom of God.
Spiritual dimension: the smile ofa refugee girl in Namibia.
Pet
er W
illia
ms/
WC
C

contact n°161/162 - June-July and August-September 199818
THE CMC STORY
values to fit into the technologicalmethodologies? Can the churchesdevelop a social morality of health carethat might be of use to governmentsand secular institutions?
The first dialogue, then, focused onmaking moral decisions, and the chal-lenge of living with them. How do youmake moral sense of a situation inwhich you are taking decisions whichwill benefit some while possibly bringingabout the preventable death or disabil-ity of others? In asking this, we raisefurther questions. Of what value arethose lives we are deciding about? Whatis human life for? How are human valuesto be brought into the framework oftechnology? What does it actually meanto be responsible for the health of100,000 people in an area, and to havemake choices between treatment andprevention? So the second dialogue,arising from the first, was about values.
In the third dialogue, the two of themaddressed problems of health care andjustice: issues which bring one face toface with politics, power and the injus-tices inherent in human systems. Howfar down that road is it appropriate togo? And what hope is there, if the diceare so loaded? Dr Jenkins finished withthree memorable phrases. Christiansdo have resources to help them livewith integrity while acknowledging thesin of the world. We need, he said, to
Helper in a polio immunizationprogramme in Morocco. P
Abe
nsur
/WH
O
hang on to “the hopefulness of solidar-ity in sin”; “the non-utopian nature ofimpossible hopes”; and “the possibili-ties of the infinite in the finite”.
The great problems of change seem tome to be institutional problems. Butthe institutional problems are thosewhich trap human beings and to whichhuman beings respond. And unless wecan become ourselves persons whoare free for re-identification and helpothers to become such, all this talkabout re-identification and so on isquite hopeless.
David Jenkins, 1970
Commissioners who were present atthese early meetings describe theJenkins / Bryant debate as one of thehighlights of their time with CMC. TheCommission's work continually raisedquestions about morality, the role of thechurch, the relationship between healthand salvation. The 1970s had seen theurgent need to implement the morefunctional aspects of the Commission'stask. By the end of the decade, it wastime to invite the CMC family and net-works to start looking, in a more sys-tematic way, at the theological andecclesiological implications of what theyhad been doing.
For discussion: Luke 10, 38-42. This tends to be usedas a story about the role of women. But it is not justwomen who find themselves too busy to talk theology.Why is it that we tend to leave it to the theologians? Doyou think you make enough time to share with col-leagues and friends about the connections betweenyour work and your faith?
We need, saidDr Jenkins, to hang on to
“the hopefulness ofsolidarity in sin”; “the
non-utopian nature ofimpossible hopes”; and“the possibilities of the
infinite in the finite”.





























