Embed Size (px)
Citation preview

508 BRYAN ASHWORTH
gram is of no value in the diagnosis of carotid artery occlusion since it may be normal and any abnormality found is likely to be due to associated disease of the retina.
Bristol Royal Infirmary (2).
ACKNOWLEDGMENT
I am grateful to the physicians of the United Bristol Hospitals and Frenchay Hospital and the surgeons of the Bristol Eye Hospital for allowing me to investigate their patients and in particular to Dr. D. R. Coles for his help and for many discussions.
The prognosis of retinoblastoma is related to its pathologic characteristics.1"3'8"8
This study is based on all the retinoblastoma specimens received by the Department of Pathology, Institute of Ophthalmology, Columbia-Presbyterian Medical Center, New York, from 1929 until 1963. A total of 534 globes representing 266 bilateral and 196 unilateral cases were reviewed. The first 50 eyes represent the period from 1929 to 1942, while the second 50 were received from 1942 to 1946. Thus most of the specimens, 434, represent cases from 1946 to 1962. In the unilateral cases, the eye was not treated with radiation or triethylene mel-amine before enucleation. In the bilateral cases, the eye recorded is the first one enucleated and in no case had been treated.
* From the Tumor Clinic under the direction of A. B. Reese, M.D., and the Ocular Pathology Department under the direction of J. A. C. Wads-worth, M.D., and with the help of G. M. Howard, M.D., Institute of Ophthalmology, Columbia-Presbyterian Medical Center. This study was supported by United States Public Health Service grant 1-S01-FR-05395-04 and by a research grant from H. W. Brown, M.D., Division of Para-sitology, Columbia University.
R E F E R E N C E S
1. Arden, G. B., Barrada, A., and Kelsey, J. H. : New clinical test of retinal function based upon the standing potential of the eye. Brit. J. Ophth., 46 : 449,1962.
2. Arden, G. B., and Barrada A.: Analysis of the electro-oculogram of a series of Normal subjects. Brit. J. Ophth., 46 :468, 1962.
3. Denny-Brown, D. : The treatment of recurrent cerebrovascular symptoms and the question of vasospasm. Med. Clin. N. Am., 34:1457, 1951.
4. Duke-Elder, W. S., and Smith, R. J. H. : System of Ophthalmology: Vol. VII. St. Louis, Mosby, 1962, p. 439.
5. Keith, N. M., Wagener, H. P., and Barker, N. W. : Some different types of essential hypertension : Their course and prognosis. Am. J. M. Sei., 197:332, 1939.
Therefore, these eyes represent untreated specimens but, in many cases, the patients were further treated. The treatment of these cases has previously been reviewed.4*5
CLINICAL DATA
As less than one half of these 462 cases could be adequately followed, this series is based on 81 unilateral cases of retinoblastoma which were followed for two or more years after enucleation and on 123 bilateral cases followed for three or more years. The difference in the follow-up period between the unilateral and bilateral cases is based upon the data in Table 1.
In all of the unilateral cases in which the patients died, death was in the first two years. Of the 18 cases for which adequate information was available, the average interval from enucleation to death was 9.2 months, with a range of two to 17 months. The time of death in the bilateral cases was not confined to the first two years. Even by three years, only 76% of the fatal cases had occurred. These late cases are true retinoblastoma deaths and are not due to radia-
THE CLINICOPATHOLOGY OF RETINOBLASTOMA*
DAVID HENDERSON BROWN New York

CLINICOPATHOLOGY OF RETINOBLASTOMA 509
TABLE 1 CUMULATIVE FOLLOW-UP: TIME IN YEARS FROM
ENUCLEATION TO FOLLOW-UP
Years
2 3 S
10 20 25
Unilateral
Alive
59 51 34 18
Dead*
18 18 18 18
Bilateral
Alive
109 90 68 26 2 0
Deadf
27 32 34 38 41 42
* Four deaths are not recorded due to insufficient data.
t One death is not recorded.
tion-induced sarcoma or to other causes. A three-year follow-up is used for the bilateral cases, conforming to custom.3 Perhaps the difference in length of survival between the bilateral and unilateral cases represents a tendency of some of the unilateral cases to become bilateral and then result in a later death.
Of the 81 patients with unilateral retino-
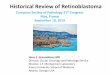
Fig. 1 (Brown). A retinoblastoma, showing true rosettes.
Fig. 2 (Brown). Pseudorosettes. Circular arrangement is evident but no limiting membranes are present.
blastoma, 22 died (27% mortality). Of the 123 bilateral patients, 42 died, (35% mortality). Twenty-three of the 53 bilateral patients treated with bilateral enucleation died (43% mortality). Of the 70 bilateral cases treated with unilateral enucleation, 19 proved fatal (27% mortality). It is evident that the bilateral cases were more serious (table 1).
PATHOLOGIC DATA
The classification of the pathologic characteristics of retinoblastoma usually divides tumors with rosettes (neuroepitheliomatous type of retinoblastoma) from those without.8 The classification used here differs in being a purely pragmatic one based on an impression of the tumor as a whole.
1. Predominantly true rosettes (figs. 1, 4 and 5). This category uses Reese's* definition of a true rosette as a group of columnar cells arranged in a ring about a central circular lumen bordered by a fine limiting membrane. A retinoblastoma was

510 DAVID HENDERSON BROWN
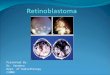
Fig. 3 (Brown). Perivascular proliferation. Note the necrotic areas between the tumor groups.
classed as showing predominantly true rosettes if 25% of the high power ( X750) microscopic fields contained true rosettes.
2. Predominantly pseudorosettes (fig. 2) . This includes tumors showing 25% of the microscopic fields with a group of columnar cells arranged in a circle around a lumen which is not bordered by a membrane and which does not contain a blood vessel. It is almost a true rosette. These cases are not common.
3. Few rosettes. Those retinoblastomas with less than 25% of the fields having rosettes but with more than a total of 10 rosettes fall in this category.
4. No rosettes. This category includes tu
mors with up to a total of 10 rosettes with less than 50% necrosis or calcification.
5. Necrosis and calcification. This represents tumors with 50% or more necrosis and calcification.
6. Perivascular proliferation (fig. 3) . Tumors with groups of 100 or more cells surrounding a medium-sized blood vessel with necrosis between separate groups are included in this category. The proliferation around the blood vessel is occasionally made up of several true rosettes.
Categories 1, 2, 3A and 3B take precedence over 6 if there is a combination of different categories (table 2) .
Table 2 shows that unilateral cases with predominantly true rosettes suffered only a 6% (1/17) mortality, while those with no rosettes had a 63% (12/19) mortality. This difference is not as clear-cut in the bilateral cases where there was a 2 1 % (11/53) fatality for those with predominantly true rosettes, while 42% (14/33) died of those with no rosettes. Patients whose eyes showed necrosis and calcification had a lower percentage of mortality than those with no rosettes in the unilateral cases. However, in bilateral cases, the percentage mortality is greater for the category of necrosis and calcification than for the category of no rosettes. These cases represent untreated eyes, the necrosis not being due to treatment.
TABLE 2 CORRELATION OF THE HISTOPATHOLOGY OF
RETINOBLASTOMA AND MORTALITY
Histopathology
Predominantly true rosettes Predominantly pseudo-rosettes Few rosettes A. True rosettes B. Pseudorosettes No rosettes Necrosis and calcification Perivascular proliferation
Percentage Mortality
Unilateral
6(1/17)
0(0/3) 0(0/11) 0 (0/10) 0 (0/1)
63 (12/19)
SO (5/10)
19 (4/21)
Bilateral
21 (11/53)
50 (2/4) 19 (5/27) 19 (5/27) 0 (0/0)
42 (14/33)
59 (20/34)
67 (6/9)

CLINICOPATHOLOGY
Herrn and Heath3 and CarbajaP both suggest that the longer retinoblastoma is present, the more undifferentiated it becomes. Following this reasoning, it is not the differentiation of the tumor (no rosettes being less differentiated than true rosettes) which is related to a fatal outcome, but the time the tumor has been in the eye. Supporting evidence for this theory is found in Table 3. The time from birth to enucleation was calculated, as precise times of diagnosis were not obtainable. Table 3 may be interpreted many ways. One interpretation is that the natural history of the tumor follows the different stages and that the tumor becomes more undifferentiated the older it is (table 3).
Retinoblastoma first forms true rosettes. These true rosettes may either decrease in quantity and fall into the category of few true rosettes, or they may change in quality and form pseudorosettes. I have listed pseudorosettes as Stage II even though the time from birth to enucleation is longer (29.2 months) than for Stage III. This is probably due to the small number of cases (6) in Stage II ; actually, Stage II appears to be often, but not invariably, a step on the way to Stage III. In Stage III, necrosis and calcification is an end-point, but both the other two groups in Stage III, few true rosettes and few pseudorosettes, may go on to Stage IV. Perivascular proliferation occurs when tumor cells outgrow their blood supply and then the only remaining viable cells are clustered around blood vessels.
TABLE 3 NATURAL HISTORY OF RETINOBLASTOMA: TIME
IN MONTHS FROM BIRTH TO ENUCLEATION IN UNTREATED CASES
Months Cases
Stage I True rosettes 12.4 160 Stage II Pseudorosettes 29.2 6 Stage III
A. Necrosis and calcification 18. S 35 B. Few true rosettes 20.2 85 C. Few pseudorosettes 24.0 2
Stage IV A. Perivascular Proliferation 28.4 42 B. No rosettes 31.1 75
OF RETINOBLASTOMA 511
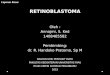
Fig. 4 (Brown). Choroidal invasion, Grade 00. The lamina vitrea has not been penetrated.
Choroidal involvement by retinoblastoma has gained increased emphasis in the literature1'8 in recent years. This classification largely follows the work of Carbajal :2
Grade 0: No involvement of choroid; tumor internal to pigment epithelium.
Grade 00 : No involvement of choroid ; tumor cells are external to pigment epithelium and are internal to Bruch's membrane (figs. 4 and 5).
Grade I : Tumor cells are confined to the choriocapillaris.
Grade II : Tumor cells have invaded the layer of larger vessels of the choriod but they do not occupy the entire choriodal thickness.
Grade III : The entire choriodal thickness is involved with tumor cells.
Grade IV: Only the suprachoroidal space is involved with tumor cells (fig. 6). If both Grade 00 and Grade IV were present, the eye was said to be Grade IV.
No attempt was made to judge the area of the choroid or the number of locations involved with tumor (table 4) .
Grade I and Grade II are very rare, as there is no natural boundary to stop the spread of tumor in these categories. Since there are only eight cases in both Grade I

512 DAVID HENDERSON BROWN
TABLE 4 CORRELATION OF THE CHOROIDAL INVOLVEMENT
OF RETINOBLASTOMA AND MORTALITY
Fig. 5 (Brown). High-power view of Figure 4. True rosettes with well-formed limiting membranes are visible. The lamina vitrea (A) limits the tumor which has undermined the pigment epithelium (B).
Fig. 6 (Brown). Retinoblastoma is only found in the suprachoroidal space. Tumor is in circle.
and Grade II, the data are not significant for these groups. It should not be inferred, because of the low apparent percentage mortality for Grades I and II, that these grades carry an actual percentage mortality less than Grade 0 and Grade 00. Although 11%-16% of unilateral patients and 20%-4 1 % of bilateral patients who showed no choroidal involvement died, Grade III proved to have a higher percentage mortality. Grade IV, tumor cells in the suprachoroidal space only, is either a late event just before enu-cleation and hence not a cause of death or it
Choroidal Percentage Mortality Involvement
Grade 0 Grade 00 Grade I Grade II Grade III Grade IV
Unilateral
16 (3/19) 11 (3/28) 0(0/0) 0(0/4)
62 (16/26) 0 (0/4)
Bilateral
41 (20/49) 20(12/61) 0 (0/1)
33 (1/3) 60 (25/42) 0 (0/5)
is an artifact caused by sectioning. Scierai involvement is important in prog
nosis. It may occur either by direct spread from the choroid or along the emissary vessels (fig. 7). Table 5 shows that scierai involvement leads, roughly, to the same percentage mortality in both the unilateral and bilateral cases (table 5).
Epibulbar involvement has always been found to be fatal.3 The present series shows that some of these cases have been successfully treated (table 6) .
Epibulbar involvement is attended by a high mortality, especially in the bilateral cases. The unilateral group is small but treatment seems to have been successful in four cases. However, in these four cases, only a few cells were evident in the epibulbar region and these may represent artifact.
Optic-nerve involvement (figs. 8, 9 and
Fig. 7 (Brown). Retinoblastoma has completely involved the choroid (Grade III) and is extending out around the emissary vessels.

C L I N I C O P A T H O L O G Y O F R E T I N O B L A S T O M A 513
Fig. 8 (Brown) . Retinoblastoma has extended to, but not beyond, the lamina cribrosa.
10) has received the greatest amount of attention in recent years and it has been fairly well documented that a higher percentage mortality results from greater involvement. The classification found in Table 6 is based on Carbajal's2 outline (table 7).
Table 7 shows that when the optic nerve is involved, the percentage mortality is
TABLE S CORRELATION OF SCLERAL INVOLVEMENT OF
RETINOBLASTOMA AND MORTALITY
Percentage Mortality
Unilateral Bilateral
Sciera involved 80 (8/10) 72 (13/18) Sciera not involved 20 (14/71) 31 (45/143)
TABLE 6 CORRELATION OF EPIBULBAR INVOLVEMENT OF
RETINOBLASTOMA AND MORTALITY
Percentage Mortality
Unilateral Bilateral
Epibulbar involvement 43 (3/7) 85 (11/13)
No Epibulbar involvement 26 (19/74) 32 (47/148)
Fr.;. 9 (Brown). Retinoblastoma has extended beyond the line of transection.
higher. The reason that the difference between optic-nerve involvement and no involvement is no more distinct is that many tumors were included in the categories of optic cup or anterior to lamina cribrosa which are shown to have no higher mortali-
Fig. 10 (Brown) . A mass of retinoblastoma cells has penetrated between the optic-nerve axis and its vaginal sheath.

514 D A V I D H E N D E R S O N B R O W N
TABLE 7 CORRELATION OF OPTIC-NERVE INVOLVEMENT
IN RETINOBLASTOMA AND MORTALITY
Percentage Mortality Optic Nerve Involvement
Unilateral Bilateral
ty than no optic-nerve involvement at all. If the categories showing tumor posterior to the lamina cribrosa are compared, a clear correlation between optic-nerve involvement and prognosis is evident.
SUMMARY
1. Eighty-one unilateral cases of retino-blastoma were followed for at least two years and 123 bilateral cases were followed for at least three years.
2. All of the fatalities in the unilateral cases occurred within two years after enu-cleation. Only 76% of the fatalities of the bilateral cases occurred in the first three years.
3. The prognosis of retinoblastoma is directly related to:
A. Differentiation. Cases with tumors with true rosettes and pseudorosettes have a better prognosis than those with no rosettes or those that are necrotic and calcified.
B. Choroidal involvement, if it occupies the whole choroidal thickness, has a 60%-62% mortality.
C. Scierai involvement has a 72%-80% mortality.
D. Epibulbar involvement leads to a 43%-85% mortality, but artifact may account for the lower percentage.
E. Optic-nerve involvement shows a higher percentage mortality the farther it has progressed.
4. Dedifferentiation of retinoblastoma from a histologie pattern of many true rosettes to no rosettes may occur in a definite time sequence as outlined.
50 Haven Avenue (10032).
REFERENCES
1. Boniuk, M. : Ocular and Adnexal Tumors. St. Louis, Mosby, 1964, p. 198.
2. Carbajal, U. M. : Observations on retinoblastoma. Am. J. Ophth., 45 :391, 1958.
3. Herrn, R. J., and Heath, P. : A study on retinoblastoma. Am. J. Ophth., 22:30, 1956.
4. Reese, A. B., and Ellworth, R. M. : Evaluation and current concepts of retinoblastoma therapy. Tr. Am. Acad. Ophth. OtolaryngoL, 67:164, 1963.
5. Reese, A. B., et al : The treatment of retinoblastoma by X-ray and triethylene melamine. Arch. Ophth., 60:897, 1958.
6. : Tumors of the Eye. New York, Hoeber, ed. 2, 1963, p. 93.
7. Tsukarhara, I. : A histopathological study on the prognosis and radiosensitivity of retinoblastoma. Arch. Ophth., 63 :1005, 1960.
8. Zimmerman, L. E. : The Registry of Ophthalmic Pathology: Past, Present, and Future. Tr. Am. Academy Ophth. OtolaryngoL, 65 :95, 1961.
I. Optic nerve not involved
II. Optic nerve involved A. Anterior to lamina
cribrosa 1. Optic cup 2. Anterior to or in
cluding lamina cribrosa
B. Posterior to lamina cribrosa 1. Nerve axis only 2. Vaginal sheath
only 3. Both nerve axis
and vaginal sheath C. Tumor cells cross line
of transection D. Tumor cells do not
cross line of transection
10(2/21) 32 (18/56)
0 (0/12)
18 (3/17)
50 (9/18)
50 (2/4)
80 (4/5)
83 (10/12)
33 (22/66) 39 (36/93)
12 (4/34)
33 (6/18)
71(15/21)
67 (2/3)
82(9/11)
80(12/15)
50 (5/10) 70 (14/20)