Embed Size (px)
Citation preview

Proceedings of UCLA Healthcare -VOLUME 21 (2017)-
CLINICAL VIGNETTE
The Clinical Spectrum of Crowned Dens Syndrome: An Analysis of Seven Cases
Ralph Yachoui, M.D.
Abstract
The crowned dens syndrome is an unusual manifestation of
calcium pyrophosphate dihydrate crystal deposition disease and
represents a rare cause of neck pain. We report seven cases of
crowned dens syndrome, assessing clinical and radiological
features, associated conditions, therapy, and outcome. The
acute presentation of crowned dens syndrome raised suspicion
for infectious meningitis and cranial giant cell arteritis in two
cases. Cervical cord compression was the initial presentation of
periodontoid calcium pyrophosphate deposition disease in two
other cases. A prior history or concurrent, self-limited,
peripheral arthritis was clinically or radiologically apparent.
Computed tomography scans performed better than magnetic
resonance imaging in assessing calcifications of the dens area.
We found a unique association with diffuse idiopathic squeletal
hyperostosis, Eagle’s syndrome, and Paget’s disease of bone.
Prompt initiation of therapy including isolated or combinations
of non-steroidal anti-inflammatory drugs, corticosteroids, and
colchicine yielded a dramatic response.
Introduction
Crowned dens syndrome (CDS) was first described in 1985 by
Bouvet et al1 and represents a rare cause of severe neck pain in
older adults. This radioclinical syndrome is defined by the
association of periodontoid calcifications in a crown-like
configuration and periodic attacks of febrile neck pain and
stiffness.2 This report illustrates the clinical and radiological
features of seven cases of patients with CDS.
Discussion
Crowned dens syndrome (CDS), also known as acute
pseudogout of the neck, is an unusual manifestation of calcium
pyrophosphate dihydrate crystal deposition disease (CPPD) and
is related to the microcrystalline deposition of calcium
pyrophosphate crystals in a periodontoid distribution.1 CDS
usually occurs in patients over 60 years of age and has a female
predominance.3
CDS is characterized by periodic attacks of acute, severe neck,
and shoulder girdle pain and stiffness mainly while attempting
to rotate the head from side to side.3,4 Fever, headaches, and
raised inflammatory markers are frequently present.2-4 As
illustrated in the cases we will present in this report, a prior
history or concurrent, self-limited, peripheral arthritis may be
clinically or radiologically apparent.5 CPPD deposition can be
precipitated by an underlying metabolic condition like
hyperparathyroidism. We found a unique association with
diffuse idiopathic squeletal hyperostosis, Eagle’s syndrome,
and Paget’s disease of bone.
The acute presentation of CDS frequently raises suspicion for
infectious meningitis, epidural abscess, polymyalgia
rheumatica, giant cell arteritis, and/or metastatic malignancy.5
A thorough investigation, such as we describe in cases 5 and 7,
is necessary to make the correct diagnosis of CPPD.
Cervical CPPD is common in patients with peripheral CPPD,
often remaining asymptomatic.6-8 In a retrospective study
conducted by Salaffi et al,6 in 25 of 49 patients (51%) affected
by peripheral CPPD, computed tomography (CT) scan of the
cervico-occipital junction showed periodontoid calcified
deposits. Only nine of the cervical CPPD cases had neck
symptoms.
CT scanning performs better than magnetic resonance imaging
(MRI) in assessing calcifications of the dens area and, therefore,
considered the gold standard for diagnosis.6 Plain radiograph is
notoriously insensitive in detecting periodontoid opacification.
CPPD crystal deposits in and around C1-C2 can lead to osseous
abnormalities of the odontoid process, such as subchondral
cysts, erosions, and even fractures of the odontoid.6,9
Cases 1 and 2 were particularly interesting, as cervicomedullary
compression was the initial presentation of periodontoid CPPD.
To date, few cases of cervical CPPD causing atlantoaxial
instability, spinal cord compression, and myelopathy have been
reported.10-12 Similar to our index patient, most lesions were
treated by surgical decompression via the transoral route with
good post-surgical outcomes.13
Treatment first involves non-steroidal anti-inflammatory drugs,
which are highly effective within days. Systemic
corticosteroids, C1-2 steroid injection, or colchicine have also
been used with good clinical efficacy.1,2,4,5,14

Case 1
A 64-year-old man was admitted to the intensive care unit for
respiratory failure and quadriparesis. He had a history of
thyroid cancer treated with surgical resection, currently on
thyroid replacement, newly-diagnosed primary
hyperparathyroidism, and diffuse idiopathic skeletal
hyperostosis. On examination, he could not lift all four
extremities against gravity. There was no clear sensory level.
MRI of the cervical spine revealed low signal intensity mass on
T2-weighted image posterior to the C2 vertebral body leading
to severe canal compromise and myelopathic signal changes
within the cord [Figure 1A-C]. On non-enhanced CT imaging,
the mass had amorphous mineralization compatible with CPPD
[Figure 1D].
The patient underwent C1 through 5 laminectomies with
posterior instrumented fusion. Four months after the initial
presentation, his quadriparesis completely resolved.
Case 2
An 84-year-old man was seen by neurosurgery for severe neck
pain and cord compression on imaging. He had been well until
2 years earlier, when he developed neck pain and stiffness that
was initially intermittent but became constant. His pain was
localized to the left side of the neck with radiation to the left
parietal area and left forehead. He denied numbness or
weakness in the arms or legs, swallowing or breathing
difficulties. He had a history of generalized osteoarthritis, and
prior C3-7 laminectomy. On examination, there was tenderness
on palpation of the cervical spine with limited range of motion
in all planes.
MRI scans showed a large nonenhancing soft tissue mass
involving the C1-2 articulation with a cystic component
extending into the canal on the left side, causing mild cord
compression. There was no high signal seen within the cervical
spinal cord at this level [Figure 2A-D]. A CT scan demonstrated
amorphous calcifications within the soft tissue mass and mild
erosive changes of the dens, most compatible with cervical
deposition of calcium pyrophosphate crystals [Figure 2E, F].
Bilateral hand and knee radiographs showed chondrocalcinosis
and findings typical of calcium pyrophosphate arthropathy.
Given the absence of signs and symptoms of a progressive
myelopathy, non-operative treatment with low-dose prednisone
and topical diclofenac was initiated. The neck pain and stiffness
significantly improved.
Case 3
A 71-year-old man was evaluated for a 5-year history of
episodic upper cervical pain and stiffness. He had a history of
documented crystal pseudogout affecting the wrists and knees.
Other medical problems included stage IV chronic kidney
disease, secondary hyperparathyroidism and coronary artery
disease. He had tenderness and restriction of neck movement,
especially on any attempt to rotate the head from side to side.
His erythrocyte sedimentation rate (ESR) was 90 mm/h, and C-
reactive protein was 12 mg/dL (range, 0.0-1.0 mg/dL).
Cervical MRI revealed soft tissue thickening at the C1-2 level
extending slightly within the spinal canal without compression
of the spinal cord [Figure 3A]. A subsequent CT showed a
pannus with crown-like mineralization surrounding and slightly
eroding the dens. On dual energy images, the calcification had
blue signal similar to the cortex of the skull base and cervical
spine, consistent with calcium pyrophosphate crystals [Figure
3B-D]. Skeletal radiographs revealed chondrocalcinosis at
bilateral hips, knees, wrists and pubic symphysis. Treatment
with prednisone 5 mg daily and colchicine 0.6 mg twice daily
was followed by rapid improvement in neck symptoms and
reduction in the frequency of flare-ups.
Case 4
A 54-year-old man was seen with diffuse chondrocalcinosis. He
had a history of a chronic arthropathy manifesting as mild joint
pain and stiffness of knees, wrists, metacarpophalangeal joints,
and shoulders. He reported intermittent neck pain associated
with marked stiffness. Physical examination elicited tenderness
throughout the posterior cervical spine and severe loss of neck
and shoulder movement.
Plain radiographs showed multilevel cervical spondylosis, and
1st through 3rd metacarpophalangeal predominant arthropathy
with chondrocalcinosis of knees, bilateral glenohumeral, and
acromioclavicular joints. Laboratory workup including ferritin
level, parathyroid hormone, calcium, magnesium, and alkaline
phosphatase was normal. A cervical CT revealed periodontoid
calcifications affecting the transverse ligament of the atlas in a
‘crown-like’ appearance, compatible with CPPD [Figure 4A,
B].
A trial of nonsteroidal anti-inflammatory drugs was
unsuccessful because of gastric intolerance. He was started on
short cycles of low-dose prednisone with satisfactory control of
his neck symptoms.
Case 5
A 92-year-old man presented to the emergency department with
complaints of severe headaches and neck pain for 5 days. Initial
clinical examination found cervical stiffness with Brudzinski’s
sign. Laboratory tests showed white blood cells 14 400/mm3,
ESR 71 mm/hr, and C-reactive protein 18 mg/dL. Infectious
meningitis was suspected; however, a lumbar puncture was
normal.
Skeletal radiographs revealed extensive chondocalcinosis of
shoulders, knees, and wrists. A cervical CT scan of C1/C2
allowed the diagnosis of crowned dens syndrome showing
small mineralization behind the odontoid process in addition to
subtle posterior longitudinal ligament mineralization at C2-C3
and C3-C4 [Figure 4C].
His headaches, neck pain, and stiffness dramatically improved
3 days later with low-dose prednisone and with normalization
of biological parameters in 14 days.

Case 6
An 86-year-old man was hospitalized with upper cervical
thoracic pain that had profoundly worsened over the last week.
The pain was severe, nonradicular, nonmyelopathic, and
unrelated to time of day, positioning, or activity. He had a
history of tophaceous gout, Paget’s disease of bone, generalized
osteoarthritis, and severe osteoporosis. Examination showed
greatly limited cervical extension and flexion, particularly
lateral rotation.
CT examination of the cervical spine revealed extensive
multilevel degenerative changes, ossification of the stylohyoid
ligament bilaterally, and chondrocalcinosis present at the C1-2
level compatible with CPPD [Figure 4D].
Treatment with prednisone 10 mg daily and low dose colchicine
resulted in rapid symptom improvement. The patient died 1
month later from unrelated cryoglobulinemic vasculitis.
Case 7
An 85-year-old woman developed intermittent right-sided
headache, which became daily after a couple of weeks. The
head pain was felt most intensely in the right temporal-occipital
area. There was no jaw or tongue claudication, visual
disturbances, diffuse myalgias, or constitutional symptoms. She
had a history of crystal-proven pseudogout of the ankle, C1
vertebral body ring fracture from a previous fall, osteoporosis,
and diabetes mellitus. The neurological and general
examinations were normal, except for a reduced range of
motion of the neck and slight tenderness over the right temporal
artery.
She was referred to a rheumatologist for suspicion of cranial
giant cell arteritis. Her ESR was 55 mm/h, and C-reactive
protein was normal. She received steroid therapy in anticipation
of the temporal biopsy. Giant cell arteritis was not confirmed
on histological examination of the right temporal artery.
A cervical CT showed atlantoaxial instability with widening of
the predental space, cranial settling with occipital condyles
essentially articulating with C2 lateral masses due to separate
C1 lateral masses as a consequence of the previous C1 fracture
and an extensive retrodental partially calcified soft tissue mass
leading to marked disintegration of dens and mild spinal canal
stenosis consistent with CPPD [Figure 4E-G]. The
neurosurgeon opted against surgical intervention because of
absence of neurological signs and cervical myelopathy.
The patient was prescribed colchicine 0.6 mg daily. After a
week, her headache improved. After 2 months, colchicine was
stopped as she was completely asymptomatic.
Conclusion
Clinicians should be aware of CDS as a significant cause of
acute febrile neck pain in older adults. Often asymptomatic,
CDS is likely under recognized, as many cases go undiagnosed.
The prompt initiation of therapy usually yields a dramatic
response. Long-term follow-up is necessary, as neck CPPD can
sometimes lead to cord compression with significant
neurological sequelae.
Table and Figures
Table 1.
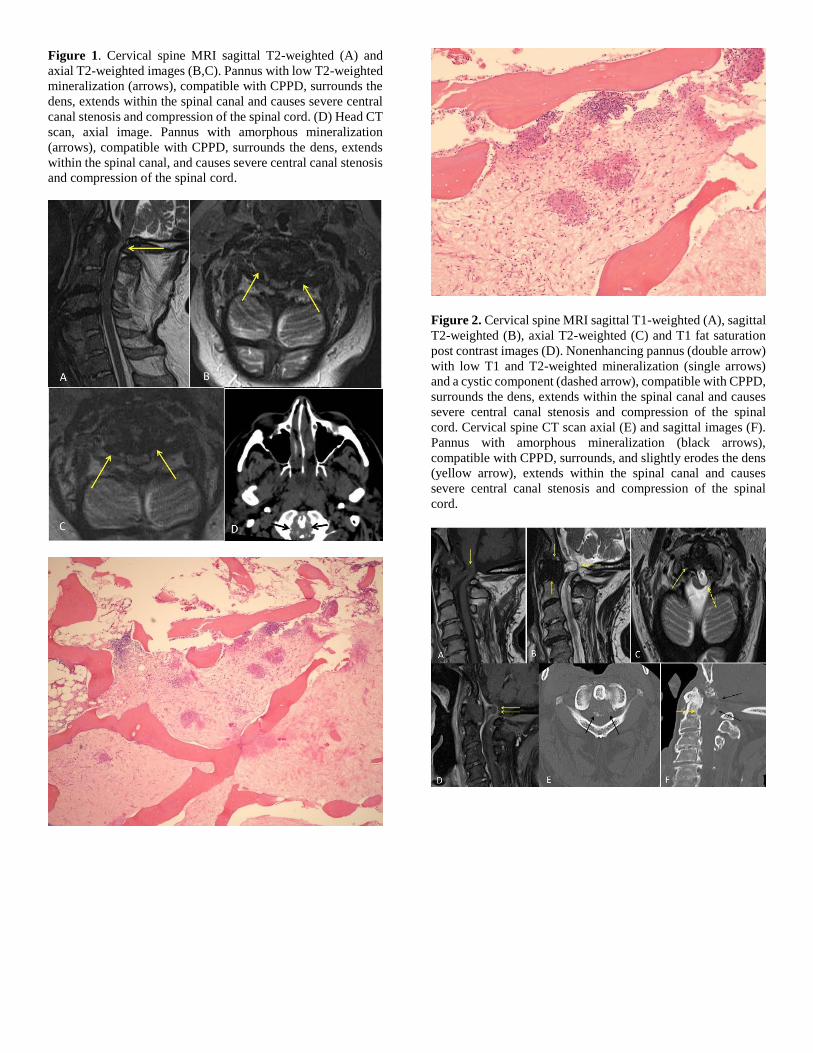
Figure 1. Cervical spine MRI sagittal T2-weighted (A) and
axial T2-weighted images (B,C). Pannus with low T2-weighted
mineralization (arrows), compatible with CPPD, surrounds the
dens, extends within the spinal canal and causes severe central
canal stenosis and compression of the spinal cord. (D) Head CT
scan, axial image. Pannus with amorphous mineralization
(arrows), compatible with CPPD, surrounds the dens, extends
within the spinal canal, and causes severe central canal stenosis
and compression of the spinal cord.
Figure 2. Cervical spine MRI sagittal T1-weighted (A), sagittal
T2-weighted (B), axial T2-weighted (C) and T1 fat saturation
post contrast images (D). Nonenhancing pannus (double arrow)
with low T1 and T2-weighted mineralization (single arrows)
and a cystic component (dashed arrow), compatible with CPPD,
surrounds the dens, extends within the spinal canal and causes
severe central canal stenosis and compression of the spinal
cord. Cervical spine CT scan axial (E) and sagittal images (F).
Pannus with amorphous mineralization (black arrows),
compatible with CPPD, surrounds, and slightly erodes the dens
(yellow arrow), extends within the spinal canal and causes
severe central canal stenosis and compression of the spinal
cord.

Figure 3. Cervical spine MRI sagittal T2-weighted image. (A)
Pannus with low T2-weighted mineralization (arrow),
compatible with CPPD, surrounds the dens and slightly extends
within the spinal canal without compression of the spinal cord.
Cervical spine CT sagittal (B), dual energy sagittal (C), and
dual energy axial images (D). Pannus with amorphous
mineralization (arrows), compatible with CPPD, surrounds and
slightly erodes the dens (dashed arrow). On the dual energy
images (B,C), the CPPD is blue due to calcium, which matches
the same blue color as the adjacent bone.
Figure 4. Cervical spine CT sagittal (A) and axial with soft
tissue algorithm images (B). Mineralization surrounding the
dens (arrows), compatible with CPPD. Cervical CT axial (C) at
the C1/C2 level showing linear calcifications of the transverse
ligament of the atlas. Cervical spine CT sagittal (D). Pannus
with amorphous mineralization (arrow), compatible with
CPPD, surrounds the dens. CT cervical spine sagittal (E) shows
extensive soft tissue thickening surrounding the dens with
erosion secondary to CPPD. The pannus formation displaces
the cervicomedullary junction posteriorly; (F) shows extensive
erosion of the dens with adjacent osseous debris and
mineralization, compatible with CPPD. Marked diastasis of the
atlantodental interval and cranial settling are due to a chronic
C1 Jefferson fracture, which are not completely visualized on
this image. CT cervical spine axial image (G) shows
mineralization and pannus surrounding an eroded dens,
compatible with CPPD.
REFERENCES
1. Bouvet JP, le Parc JM, Michalski B, Benlahrache C,
Auquier L. Acute neck pain due to calcifications
surrounding the odontoid process: the crowned dens
syndrome. Arthritis Rheum. 1985 Dec;28(12):1417-20.
PubMed PMID: 4084331.
2. Uh M, Dewar C, Spouge D, Blocka K. Crowned dens
syndrome: a rare cause of acute neck pain. Clin
Rheumatol. 2013 May;32(5):711-4. doi: 10.1007/s10067-
013-2179-5. Epub 2013 Feb 8. Review. PubMed PMID:
23392827.
3. Goto S, Umehara J, Aizawa T, Kokubun S. Crowned
Dens syndrome. J Bone Joint Surg Am. 2007
Dec;89(12):2732-6. PubMed PMID: 18056506.
4. Wu DW, Reginato AJ, Torriani M, Robinson DR,
Reginato AM. The crowned dens syndrome as a cause of
neck pain: report of two new cases and review of the
literature. Arthritis Rheum. 2005 Feb 15;53(1):133-7.
Review. PubMed PMID:15696551.
5. Aouba A, Vuillemin-Bodaghi V, Mutschler C, De
Bandt M. Crowned dens syndrome misdiagnosed as
polymyalgia rheumatica, giant cell arteritis, meningitis or
spondylitis: an analysis of eight cases. Rheumatology
(Oxford). 2004 Dec;43(12):1508-12. Epub 2004 Aug 17.
PubMed PMID: 15316123.
6. Salaffi F, Carotti M, Guglielmi G, Passarini G, Grassi
W. The crowned dens syndrome as a cause of neck pain:
clinical and computed tomography study in patients with
calcium pyrophosphate dihydrate deposition disease. Clin
Exp Rheumatol. 2008 Nov-Dec;26(6):1040-6. PubMed
PMID: 19210868.
7. Finckh A, Van Linthoudt D, Duvoisin B, Bovay P,
Gerster JC. The cervical spine in calcium pyrophosphate
dihydrate deposition disease. A prevalent case-control
study. J Rheumatol. 2004 Mar;31(3):545-9. PubMed
PMID: 14994403.

8. Constantin A, Marin F, Bon E, Fedele M, Lagarrigue
B, Bouteiller G. Calcification of the transverse ligament
of the atlas in chondrocalcinosis: computed tomography
study. Ann Rheum Dis. 1996 Feb;55(2):137-9. PubMed
PMID:8712865; PubMed Central PMCID: PMC1010109.
9. Kakitsubata Y, Boutin RD, Theodorou DJ, Kerr RM,
Steinbach LS, Chan KK, Pathria MN, Haghighi P,
Resnick D. Calcium pyrophosphate dihydrate crystal
deposition in and around the atlantoaxial joint: association
with type 2 odontoid fractures in nine patients. Radiology.
2000 Jul;216(1):213-9. PubMed PMID:10887250.
10. Zünkeler B, Schelper R, Menezes AH. Periodontoid
calcium pyrophosphate dihydrate deposition disease:
"pseudogout" mass lesions of the craniocervical junction.
J Neurosurg. 1996 Nov;85(5):803-9. PubMed PMID:
8893717.
11. Ishida T, Dorfman HD, Bullough PG. Tophaceous
pseudogout (tumoral calcium pyrophosphate dihydrate
crystal deposition disease). Hum Pathol. 1995
Jun;26(6):587-93. PubMed PMID: 7774886.
12. Ciricillo SF, Weinstein PR. Foramen magnum syndrome
from pseudogout of the atlanto-occipital ligament. Case
report. J Neurosurg. 1989 Jul;71(1):141-3. PubMed
PMID: 2738632.
13. Wells CR, Morgello S, DiCarlo E. Cervical myelopathy
due to calcium pyrophosphate dihydrate deposition
disease. J Neurol Neurosurg Psychiatry. 1991
Jul;54(7):658-9. PubMed PMID: 1895139; PubMed
Central PMCID: PMC1014449.
14. Frey ME, Dery FJ Jr, Cifu DX. C1-2 steroid injection
for crowned dens syndrome. PM R. 2009 Apr;1(4):379-
82. doi: 10.1016/j.pmrj.2009.01.014. PubMed PMID:
19627922.
Submitted May 30, 2017





























