Embed Size (px)
Citation preview

Acta Pædiatrica ISSN 0803–5253
SHORT COMMUNICATION
The clinical relevance of duodenal intraepithelial lymphocyte countsin children treated for coeliac diseaseC Grant1, L Hogberg ([email protected])2, K Falth-Magnusson3, E Grodzinsky4, T Sundqvist5, L Stenhammar2,3
1.Laboratory Medicine Ostergotland, Department of Pathology, Norrkoping Hospital, Norrkoping, Sweden2.Department of Paediatrics, Norrkoping Hospital, Norrkoping, Sweden3.Division of Paediatrics, Department of Molecular and Clinical Medicine, Linkoping University, Sweden4.Department of Research and Development in Local Health Care, County Council of Ostergotland, Linkoping, Sweden5.Division of Medical Microbiology, Department of Molecular and Clinical Medicine, Linkoping University, Linkoping, Sweden
CorrespondenceLotta Hogberg, M.D., Ph.D., Department ofPaediatrics, Norrkoping Hospital,SE-601 82 Norrkoping, Sweden.Tel: +46-11-222000 |Fax: +46-11-223735 |Email: [email protected]
Received20 August 2007; revised 1 October 2007;accepted 22 October 2007.
DOI:10.1111/j.1651-2227.2008.00874.x
Coeliac disease (CD) is characterized by a small intestinalmucosal lesion secondary to a T-cell-mediated reaction togliadin, the alcohol-soluble fraction of gluten peptide fromwheat proteins (1). The current routine for diagnosing CDrests on the demonstration of enteropathy in a small bowelmucosal biopsy. According to the Marsh concept (2), dy-namic progression of the lesion goes from initially increasedduodenal intraepithelial lymphocyte (IEL) counts to end-stage subtotal/total villus atrophy, a reversible process aftercessation of gluten exposure. The duodenal IEL counts fo-cus on the cells believed to mediate the mucosal damage ofgluten enteropathy (3). For new patients, IEL counts abovewhat are generally considered to be normal in an architec-turally normal mucosa raise an alert to the possibility of CD.But what about known and treated CD children? Do IELcounts in follow-up biopsies from CD patients respondingto treatment give additive information of clinical value? Wehave assessed the IEL counts of the follow-up biopsies ob-tained from a well-defined group of coeliac children partic-ipating in a recent multicentre, double-blind study compar-ing a conventional gluten-free diet with a diet containing oatproducts (4). In addition, we have compared the IEL countsin the follow-up biopsies with coeliac serological markers,age and sex.
Ninety-two children (median 6.0 years; range 8 months–17.2 years; 40 boys, 52 girls) with newly diagnosed CD ateight participating Swedish paediatric clinics were randomlyassigned to a conventional gluten-free diet or to a gluten-freediet containing oat products. The initial diagnosis was basedon anamnesis, clinical status, coeliac serological markersand a pretreatment duodenal biopsy. After they had been fora year on their assigned diet, their serological status and duo-denal histology were reassessed. Antigliadin, antiendomy-sium and antitissue transglutaminase antibody titres and a
control biopsy under dietary treatment were available for89 children.
The duodenal biopsies, taken either by capsule or endo-scopically, were routinely processed for microscopy. IELcounts were done by one person (CG) on haematoxylin-eosin sections from all biopsies, without knowledge of clini-cal data regarding the patient. Only stretches where the villusenterocytes with their nuclei were sectioned perpendicularlyor nearly so to the basal membrane were counted using ablood-cell counter (Celloscope) to keep track of the subto-tals. In practice, this gave an upper limit of 300 countableenterocytes per biopsy. To be counted as a lymphocyte, thenucleus had to be clearly identifiable in the plane of section.Three sets of 100 enterocytes each were counted and themean IEL count was taken to the nearest whole number. AnELISA was used for detection of IgA antigliadin antibodies(cut-off value ≥ 30 Units) (4,5). IgA and IgG antiendomy-sium antibodies were measured by indirect immunofluores-cence microscopy (cut-off values ≥ titre 1/10) (5). IgA an-titissue translutaminase antibody titre was measured usingthe commercially available ELISA kit Celikey® (PharmaciaDiagnostics AB, Freiburg, Germany) with human recombi-nant tissue transglutaminase as the antigen (cut-off value >
8 Units/mL). All sera were analysed for total serum IgA us-ing a routine nephelometric assay. Relationships betweencontinuous variables were assessed by the Students t-test. Ap-value less than 0.05 was considered significant. Dis-criminant analysis was performed using SPSS (SPSS Inc,Chicago, IL, USA; v. 14.0 for Windows). The study was ap-proved by the Human Research Ethics Committee of theFaculty of Health Sciences, Linkoping University.
All children had an architecturally restored duodenal mu-cosa. The mean IEL number was 16 (range 3–29; SD 4.8).Graphical presentation of the results gives a symmetrical
C©2008 The Author/Journal Compilation C©2008 Foundation Acta Pædiatrica/Acta Pædiatrica 2008 97, pp. 1133–1135 1133

Intraepithelial lymphocyte count in coeliac disease Grant et al.
0
2
4
6
8
10
12
14
1 4 7
10
13
16
19
22
25
28
Number of IEL
Fre
qu
en
cy
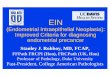
Figure 1 Number of intraepithelial lymphocytes (IEL) per 100 enterocytes insmall bowel biopsy samples from coeliac children on gluten-free diet in relationto number of patients.
0 5 10 15 20 25 30 35
Number of IEL
Em
A (
titr
e)
1/80
1/60
1/40
1/20
(a)
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
16,0
0 5 10 15 20 25 30 35
Number of IEL
TG
A (
U/m
l)
(b)
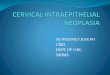
Figure 2 Number of intraepithelial lymphocytes (IEL) per 100 enterocytes in small bowel biopsy samples from coeliac children on gluten-free diet in relationto (A) S-IgA antiendomysium antibody (EmA) titres (cut-off values ≥titre 1/10) and (B) S-IgA antitissue transglutaminase antibodies (TGA) (U/mL; cut-off value≥8 U/mL).
distribution curve for the IEL counts (Fig. 1). There was nosignificant difference in IEL counts between boys and girls.Age, from less than 1 year to nearly 18, did not skew thecounts.
Antigliadin antibodies were normal in all children. Theserological data regarding antiendomysium and antitissuetransglutaminase antibodies gave no discriminatory clusters(Fig. 2A and B).
The mean IEL count, SD and range for the 89 treated chil-dren fit in well with the generally accepted ‘normal’ levelsfor children and adults (6,7). In 18 ‘normal’ adults reportedby Veress et al. (8), there was an upper limit of 20 IEL/100enterocytes for haematoxylin-eosin sections. Applying thislimit to our treated coeliac children would mean drawing anarbitrary line through a normal Gaussian distribution curve.The quick way out in routine diagnostic work would be toreport simply ‘few’, ‘moderate numbers’ or ‘numerous’ IELsor apply the rule of thumb proposed by Veress et al. (8)and look at a few villi to establish the approximate ratioof 1:5 or 1:6 IELs to enterocytes to avoid time-consuming‘accurate’ counts. For clinical research on CD and itspathogenesis, there is naturally a need to characterize sub-populations among duodenal IELs (9).
1134 C©2008 The Author/Journal Compilation C©2008 Foundation Acta Pædiatrica/Acta Pædiatrica 2008 97, pp. 1133–1135

Grant et al. Intraepithelial lymphocyte count in coeliac disease
We have looked at conventional duodenal biopsies stainedconventionally with haematoxylin-eosin. With a CD3 anti-body and looking at lymphocytic cytoplasmic ramificationsinstead of lymphocyte nuclei, the IEL-counts would presum-ably be shifted to the right but still maintain the pattern ofa few low or high counts and a cluster in the middle. Thechildren participating in our study had follow-up visits toa dietician and/or specialized nurse every third month, i.e.more frequently than usual in routine clinical practice, pos-sibly encouraging stricter dietary compliance. This may havecontributed to our good results, i.e. low counts of IEL, as in-creased numbers of IEL even in well-treated patients havebeen reported by others (6).
The IEL -counts on the follow-up biopsies from theCD children after a year on gluten-free diet fell within alimited range and gave no additional information whenmatched against the other parameters. This supports cur-rent recommendations proposed by the European and NorthAmerican paediatric gastroenterology societies (ESPGHANand NASPGHAN, respectively) for discontinuing routinefollow-up biopsies, the empirical clinical recommendationsnot based on studies of duodenal morphology (10,11). Poorclinical response or diagnostic doubts, of course, remain asindications for renewed biopsy. For new patients with sus-pected CD, both societies stipulate a full diagnostic work-upincluding the demonstration of duodenal enteropathy com-patible with CD. The original ESPGHAN criteria from 1970(12), with follow-up biopsies after a period of gluten-free dietand then after a gluten challenge, are currently to be limitedto children under 2 years of age at initial biopsy. Most non-coeliac disorders, which mimic classic gluten enteropathy,affect this age group and are not permanent in the majority ofcases. For the time being, many paediatric clinics, more thanhalf those in Sweden, for example (13), routinely rebiopsytheir CD patients while on gluten-free diet. A changeover toa one-biopsy routine in diagnosing childhood CD would freeresources for concentration on finding cases of atypical orsilent CD. Judging from preliminary results from a currentSwedish screening survey of 12-year olds, this is an unchar-tered area demanding attention (14). Moreover, a recentlypublished Swedish study provides evidence that the diagno-sis of CD in children can be based on only one pathologicsmall bowel biopsy in combination with normal S-IgA andincreased serum IgA antitissue transglutaminase antibodiesat presentation and normalization of the celiac serology, nor-mal growth and remission of clinical symptoms after 1 yearof gluten-free diet (15).
In conclusion, the symmetrical distribution pattern for theIEL counts in follow-up biopsies from 89 CD children aftera year on a gluten-free diet argues against establishing rigidnumerical limits for what is normal or abnormal. The IELcounts gave no useful clues, alone or in combination withother parameters, as to current clinical status or to future im-plications. This supports the concept that follow-up biopsyas a routine measure is not warranted, unless there is poorresponse to the dietary treatment or otherwise any diagnos-tic doubts.
ACKNOWLEDGEMENTWe wish to express our sincere gratitude to the follow-ing Swedish paediatricians, who contributed with smallbowel biopsy material and clinical data: Henry Ascher, LarsBrowaldh, Jan-Åke Hammersjo, Gunnar Jansson, Eva Lind-berg and Urban Myrdal.
References
1. Sollid LM. Coeliac disease: dissecting a complex inflammatorydisorder. Nat Rev Immunol 2002; 9: 647–55.
2. Marsh MN. Gluten, major histocompatibility complex, and thesmall intestine. A molecular and immunologic approach to thespectrum of gluten sensitivity (“celiac sprue”).Gastroenterology 1992; 102: 330–54.
3. van Heel DA, West J. Recent advances in celiac disease. Gut2006; 55: 1037–46.
4. Hogberg L, Laurin P, Falth-Magnusson K, Grant C,Grodzinsky E, Jansson G, et al. Oats to children with newlydiagnosed coeliac disease: a randomised double blind study.Gut 2004; 53: 649–54.
5. Grodzinsky E, Jansson G, Stenhammar L, Falth-Magnusson K.Anti-endomysium antibodies and anti-gliadin antibodies asserological markers for coeliac disease in childhood: a clinicalstudy to develop a practical routine. Acta Paediatr 1995; 84:294–8.
6. Kuitunen P, Kosnai I, Savilahti E. Morphometric study of thejejunal mucosa in various childhood enteropathies with specialreference to intraepithelial lymphocytes. J PediatrGastroenterol Nutr 1982; 1: 525–31.
7. Hayat M, Cairns A, Dixon MF, O’Mahony S. Quantitation ofintraepithelial lymphocytes in human duodenum: what isnormal? J Clin Pathol 2002; 55: 393–4.
8. Veress B, Franzen L, Bodin L, Borch K. Duodenalintraepithelial lymphocyte-count revisited. Scand JGastroenterol 2004; 39: 138–44.
9. Lahdeaho M-L, Kaukinen K, Collin P, Ruuska T, Partanen J,Haapala A-M, et al. Celiac disease: from inflammation toatrophy: a long-term follow-up study. J Pediatr GastroenterolNutr 2005; 41: 44–8.
10. Walker-Smith JA, Guandalini S, Schmitz J, Shmerling DH,Visakorpi JK. Revised criteria for diagnosis of celiac disease.Report of Working Group of European Society of PaediatricGastroenterology and Nutrition. Arch Dis Child 1990; 65:909–11.
11. Hill ID, Dirks MH, Liptak GS, Colletti RB, Fasano A,Guandalini S, et al. Guideline for the diagnosis and treatmentof celiac disease in children: recommendations of the NorthAmerican Society for Pediatric Gastroenterology, Hepatologyand Nutrition. J Pediatr Gastroenterol Nutr 2005; 40: 1–19.
12. Meeuwisse GW. Diagnostic criteria in coeliac disease. ActaPaediatr Scand 1970; 59: 461–3.
13. Stenhammar L, Hogberg L, Danielsson L, Ascher H, DannaeusA, Hernell O, et al. How do Swedish paediatric clinicsdiagnose coeliac disease? Results of a nationwidequestionnaire study. Acta Paediatr 2006; 95: 1495–7.
14. Myleus A, Ivarsson A, Webb L, Danielsson L, Hernell O,Hogberg L, et al. Exploring the iceberg of celiacs in Sweden – apopulation-based screening study of twelve-year-old children.Presentation at the 40th Annual Meeting of the EuropeanSociety for Paediatric Gastroenterology, Hepatology andNutrition, Barcelona, Spain, May 2007.
15. Killander A, Arnell H, Hagenas L, Finkel Y. Omitting controlbiopsy in paediatric coeliac disease: a follow-up study. ActaPaediatr 2007; 96: 1190–4.
C©2008 The Author/Journal Compilation C©2008 Foundation Acta Pædiatrica/Acta Pædiatrica 2008 97, pp. 1133–1135 1135