Embed Size (px)
Citation preview

THE CLINICAL BIOCHEMISTRYOF KIDNEY FUNCTIONS
2019 Dr Boldizsár CZÉH

The kidneys are vital organs
Functional unit: Nephron


Perfusion rate / day
Protein amount / day
Blood ~ 1500 L 100-130 kgPrimary filtrate
~ 180 L 9 – 18 g
Urine (endproduct)
~ 1 L < 300 mg
Filtration and reabsorption

RENAL FUNCTIONSElectrolyte & Fluid BalancesAcid-Base BalancesElimination of Metabolic WastesBlood Pressure RegulationEndocrine functions: Vitamin D Synthesis, EPO, RAA systemRed Blood Cell ProductionProstaglandins Synthesis

Why do we test renal functions?
To identify renal dysfunction.
To diagnose renal disease.
To monitor disease progression.
To monitor response to treatment.
To assess changes in function that may impact
therapeutic efficacy (e.g. Digoxin, chemotherapy).

Urinalysis
Liquid ‘biopsy’ of the urinary tract.
Painless, non-invasive, inexpensive.
Yields much information quickly.

The 3 stages of urine analysis
FRESH SAMPLE!!

Urine samples

Gross appearance Amount– 800 – 1800 mL / die – Polyuria > 2.5 L / die– Oliguria < 400 mL / die, Anuria 100 ml / die– Pollakisuria: frequent, but small amount, becasue of tumor or
infection Color – Normally yellowish– Food, drugs– Blood, myoglobin
Transparency– Infection, blood, bacteria, fungi
Odortypical urine smellsweet: sugarammoniac

Biochemical Tests of Renal FunctionpHGlucoseProteinMicroalbuminuriaRBCHaemoglobinWBCNitritBilirubinUrobilinogenKeton bodiesSpecific gravityOsmolality

Microscopic analysis should follow when the biochemical tests are positive.
Analyze spontaneous-urinesample within 4 h after sampling.
Look for and count the cellular and inorganic (crystal) elements in the sediment.
Urine sediment: microscopic examination from freshly passed urine

Functional tests

Glomerular Function = GFR

Measurement of Glomerular Filtration Rate: determination of clearance
GFR is essential to renal functionMost frequently performed test of renal function.Measurement is based on concept of clearance: “clearance is a pharmacokinetic measurement of the volume of plasma from which a substance is completely removed per unit time; the usual units are ml / min”

Measurement of Glomerular Filtration Rate: determination of clearance
Clearance = (U x V) / P where U = is the urinary concentration of a given substance V = is the volume of urine produced (mL/min)P = is the plasma concentration of the given substance
Unit = volume / time (mL/min)
If clearance = GFR then: – freely filtered by glomerulus– glomerulus = sole route of excretion from the body – (no tubular secretion or reabsorption) – Non-toxic and easily measurable

1-2 % / day of muscle creatineconverted to creatinine.Amount produced relates to muscle mass.Freely filtered at the glomerulus.Some tubular excretion.
Creatinine Clearance

Creatinine ClearanceTimed urine collection for creatinine measurement (usually 24h)Blood sample taken within the period of collection.
Problems: Practical problems of accurate urine collection and volume measurement.Within subject variability = 11% Interference in creatinine measurement
In vitro interference:acetoacetate, ascorbic acid, fructose, pyruvate, cephalosporins, creatine, proline, chronic lidocaine administration, bilirubin. In vivo inhibition of creatinine secretion occurs with cimetidine or trimethoprim.

Estimated GFR (eGFR) Plasma Creatinine Concentration
Difficulties: Concentration depends on balance between input and output.Production determined by muscle mass which is related to age, sex and weight.High between subject variability.Concentration inversely related to GFR.– Small changes in creatinine within and around the
reference limits = large changes in GFR.Reference limits can be misleading.

Estimated GFR (eGFR) Plasma Creatinine Concentration: ProblemsPlasma creatinine can increase following protein loads.– Goulash effect: 80% rise in creatinine after 300g of
cooked beef.– Less variability in early morning creatinine
Strenuous exercise may increase creatinine by 14%Muscle mass more difficult to predict in oedematouspatients and late pregnancyPatients with muscle wastingPatients with liver diseaseDrugs inhibiting tubular secretion can raise creatinine concentration.

CreatinineInput
NormalMuscleMass
NormalKidneys
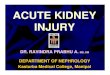
Effect of Muscle Mass on Serum Creatinine
Kidney output
Creatinine Plasma Level

Kidney output
CreatinineInput
NormalMuscleMass
NormalKidneys
DiseasedKidneys
NormalMuscleMass
Effect of Muscle Mass on Serum Creatinine
CreatininePlasmaLevel

CreatinineInput
NormalMuscleMass
NormalKidneys
DiseasedKidneys
NormalMuscleMass
NormalKidneys
IncreasedMuscleMass
Effect of Muscle Mass on Serum Creatinine
Kidney output
CreatininePlasmaLevel

CreatininePlasmaLevel
CreatinineInput
NormalMuscleMass
NormalKidneys
DiseasedKidneys
NormalMuscleMass
DiseasedKidneys
NormalKidneys
IncreasedMuscleMass Reduced
MuscleMass
Effect of Muscle Mass on Serum Creatinine
Kidney output

Estimated GFR (eGFR) Plasma Creatinine Concentration: Problems

Cystatin-C
Cysteine proteinase inhibitor C (MW13 000)Small size = freely filtered at glomerulusConstant production rate by all nucleated cellsNo known extra-renal excretion routesNot influenced by muscle mass, diet or sex
Estimation of GFR for/in:– Early detection of kidney
disease– Acute and chronic renal
disease– Renal transplantation and
haemodialysis– Diseases associated with
kidneys, e.g. diabetes mellitus, hypertension
– Patients receiving nephrotoxic drugs
– Liver failure– Paediatrics and elderly

Guidelines for the estimation of GFR in the clinical practice
GFR(ml / min / 1.73m3)
Parameter Clinical indication
60 – 90 Cystatin C Elderly people > 60 yChildren > 1 y , < 18 y
20 – 60 MDRD FormulaCockroft-Gaul FormulaSchwartz FormulaCystatin C
CKD-EPIMDRD FormulaCockroft-Gaul Formula
AdultsAdultsChildrenBMI > 30 kg / m2
Nephrotic syndrome Acute Renal Failure on the basis of a Chronic Renal FailureAdultsAdultsAdults
< 20 (Creatinine-Clearance +Urea-Clearance) / 2

Tubular Functions

Tests of Tubular FunctionsProximal Tubular Functions– Phosphate reabsorption– Aminoaciduria– Glycosuria– Fractional HCO3
-
excretion.Distal Tubular Functions– Acidification – Concentration
Normal urine concentrating capacity if urine osmolality > 600 mosmol/kg

Renal faliureAcute renal faliure
– Sudden development within hours or days
– GFR drops rapidly
– In most cases it is REVERSIBLE
Chronic renal faliure
– Develops over months or years
– It is IRREVERSIBLE

Acute Renal Failure (ARF)Sudden loss of kidney function over a period of hours or days– Characterized by:
A rapid ↓ GFR Retention of metabolic waste
– A progressive ↑ BUN and ↑ Creatinine (Azotemia)
– Associated with:Classic finding of Oliguria (UO < 400ml/day)Fluid, electrolyte and acid-base imbalances
– Usually reversible with prompt treatment

Classification of ARF: according to the location of the insult
– Prerenal↓ Blood flow to kidneysOccurs in about 50-70% of all ARF cases
– Intrarenalactual damage to kidneysOccurs in about 20-30% of all ARF cases
– Postrenalobstruction of urinary excretionOccurs in about 1-10% of all ARF cases

Pre-Renal ARFRenal blood flow is decreased before reaching the kidney.– ↓ Renal Perfusion = ↓ GFR leading to Oliguria– Most common type of ARF– Common Causes:
Hypotension (severe and abrupt)HypovolemiaLow Cardiac Output States
– Treatment to correct cause, if not corrected it may cause intrarenal failure i.e. acute tubular necrosis (ATN)

Intrarenal ARF: a condition that leads to actual damage of the renal tissue (parenchyma) resulting
in malfunction of nephrons.
Acute Tubular Necrosis (ATN)Damage to the renal tubules caused by ischemia or toxinsCharacterized by varying degrees of cellular damage or death.– Ischemic: trauma to kidneys,
massive hemorrhage or post-surgery
– Nephrotoxic: I.V. contrast dyes, heavy metals or antibiotics (aminoglyclosides)

Pre-renal versus renal ARF
TEST RESULT
Pre-renal Renal
Urea & Creatinine Urea Both
Protein in the urine - +
Creatininein serum

Pre-renal versus renal ARF
TEST RESULTPre-renal Renal
Urine Na+ (mmol / L) < 20 > 40
Urine / PlasmaOsmolality > 1.5 : 1 < 1.1 : 1
Urine urea cc / Plasma urea cc > 10 < 5

Postrenal ARF: conditions that block urine flow distal to kidneys
– Caused by an obstruction below the kidneys in the urinary tract
Calculi (stones)Tumors or massesBlood clotsBenign prostate hypertrophy (BPH)
– ↓ Urine Output common; Oliguria or anuria (UO < 50 ml/day)
Causes urine to back up into the kidneys; eventually increases pressures leading to a ↓ GFR

Chronic Renal Failure

Chronic Renal FailureA progressive and irreversible loss of renal function over a period of months to years
– The kidneys can loose up to 80% of all nephrons withrelatively few overt changes in functioning of the body
– Nephrons are destroyed and replaced with scar tissue; remaining nephrons become hypertrophied and do not function as well.
– Resulting in systemic disease involving all of the body’s organs (Uremic syndrome of CRF)

Etiology of Chronic Renal FailureDiabetes Mellitus (35%)Hypertension (25%)Chronic glomerulonephritis (10%)
Vascular disordersInfectionsNephrotoxic medicationsToxic agent exposureSickle cell anemiaSystemic lupus erythematosusPyelonephritisObstructions of the urinary tractPolycystic kidney disease

Three Stages of CRFStage 1– Reduced renal reserve
Characterized by a 40-75% loss of nephron functionUsually asymptomatic; normal BUN & Creatinine
Stage 2– Renal Insufficiency
Characterized by a 75-90% loss of nephron function↑BUN and ↑Creatinine
– Kidneys loose ability to concentrate urine; client may report polyuria or/and nocturia; Anemia develops
Stage 3– End-stage renal
disease (ESRD)Final StageCharacterized by a >90% loss of nephron functionCharacterized by ↑BUN ↑Creatinine and electrolyte imbalancesUremic symptomsRequires Life-long Dialysis

Nephrotic syndrome

Pathophysiology of nephrotic syndrome
Increased glomerularcapillary permeability
Heavy proteinuria
Hypoalbuminemia Loss of antithrombin-3Hypogammaglobulinemia
Susceptibility to infection Edema Compensatory
Increase in lipoprotein synthesis
Hyperlipemia Hypercoagulability

Systemic biochemical manifestations, complications
Anemia– Inadequate erythropoietin production– Decreased life span of RBC– Nutritional deficits
S/SX: fatigue, shortness of breath and even angina
Renal Osteodystrophy– A syndrome of skeletal changes
found in CRF from alterations in calcium & phosphate metabolism and elevated PTH levels:
↑ PTH reabsorbs calcium & phosphorous from bone stores in an attempt to increase serum calcium levels. Long term effects: bone deformity and weakness
– Increased triglyceride levels
Occurs in 30-70% in CFR– Increased blood sugars
Usually moderate; alterations cellular use of glucose
– Increased tendency to bleed
Altered platelet function and coagulation factors
– Increased risk of InfectionImpaired leukocyte function and immune responses
– Reproductive Dysfunction Infertility and decreased libido

Biochemical manifestations: electrolyte imbalances
– HyperkalemiaKidney’s can’t excrete 80-90% of body’s potassium like normal Irritability, restlessness, weakness, diarrhea and abdominal pain/cramping
– HyperphosphatemiaPrimarily excreted by kidneys; ↓UO = decreased excretion
– HypocalcemiaThe active form of Vitamin D is required for Ca2+ to be absorbed; only functioning kidneys can activate Vitamin D
– HypermagnesemiaUsually normal or slightly elevated
– HyponatremiaSodium levels maybe decreased due to hemodilution from fluid overload.

Thank you!