Embed Size (px)
Citation preview

The Changing Landscape for Management of
Thromboembolic Risk in Atrial Fibrillation
April 10, 2013Chris Lane

I don’t actually have any disclosures

Outline
1. Developments in Afib TE and bleeding Risk Scores
2. Research around NOACs (Novel Oral Anticoagulates) for Non Valvular Atrial Fibrillation
3. NOAC Limitations and Specific Situations 4. Left Atrial Occlusion Devices5. CCS Guideline Afib Update

THROMBOEMOBLIC / STROKE RISK PREDICTION

CHADS2
Revised CHADS2 classify patients into:
Low (CHADS2= 0)Intermediate (CHADS2= 1)High risk (CHADS2 >=2)

CHADS2 Limitations
• CHADS2 = 0 still has 1.9%/year risk• Many pts fall into Int CHADS2 category• Known risk factors (female gender and
other vascular disease) not accounted for in CHADS2
• Known that risk increases as a continuous variable with age, but only 1 cut off value used in CHADS2.

CHA2DS2- VASc

CHA2DS2- VASc

CHA2DS2- VASc

CHA2DS2- VASc

Piccini et al. Circulation Jan 15, 2013
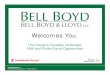
R2 CHADS2
R2CHADS2 = CHADS2 + 2 points for CrCl < 60ml/min

Piccini et al. Circulation Jan 15, 2013
R2 CHADS2

Piccini et al. Circulation Jan 15, 2013
R2 CHADS2

BLEEDING RISK PREDICTIONS

HAS-BLED – March 2010

HAS-BLED
Goal of the study: Develop a practical risk score to estimate the 1 year risk of major bleeding (intracranial, hospitalization, Hb dec > 2g/L, and/or transfusions) in a contemporary, real world cohort of patients with AF.


Definitions
HTN = uncontrolled or sBP > 160mmHg
Abnormal kidney function = chronic dialysis, renal transplantation, Cr >= 200
Abnormal liver function = chronic hepatic disease (ie cirrhosis) or biochemical evidence of hepatic derangement (bili > 2x ULN and LFTs > 3x ULN)

Definitions
Stroke = previous history, particularly lacunar
Bleeding historyLabile INR = TTR <60%Elderly = >65 yearsDrugs = antiplts, NSAIDSAlcohol Excess = > 8 / week


Effect on Management
33 pts with CHADS2 >= 1 had bleeding events – 4 (12%) of these had HAS-BLED
scores that outweighed the stroke risk21 pts with CHADS2 >= 1 discharged without anticoag who had a stroke, only 1 had HAS-BLED score that outweighed the stroke risk

Effect on Management
Therefore, if used CHADS2 and HAS-BLED together, in this population, would have withheld OAC in 4/33 (12%) pts who suffered major bleed and initiated OAC in 20/21 (95%) at high stroke risk who were discharged without OAC and suffered a stroke.

Effect on Management
For pts with CHADS2 = 1,The HAS-BLED score must exceed 2 for the
potential harm caused by OAC to outweigh the benefit

Noval Oral Anticoagulates - NOACs

Noval Oral Anticoagulates - NOACs
3 Currently available for Non-Valvular AF in Canada:• Dabigatran / Pradax RE-LY• Rivaroxaban / Xeralta ROCKET AF• Apixaban / Eliquis ARISTOTLE

RivaroxabanApixaban
Dabigatran

Pharmacology

Trial Methodology

RE-LY - Dabigatran

RE-LY - Dabigatran

RELY-ABLE• During 2.3 years of additional treatment after RE-LY® (total mean follow-up 4.3 years), rates of stroke and major bleeding remain low on dabigatran and are consistent with those seen during RE-LY®
Stroke / Embolism

Rocket AF -Rivaroxaban

ROCKET AF
Similar Results On Treatment and Intention to Treat

ROCKET AF

ROCKET AF

ARISTOTLE -Apixaban

Trial Comparisons


Valves

RE-ALIGN
• Dabigatran at 150, 220 or 300mg BID vs Warfarin postMechanical MV or AV Replacement• 2 Arms – start at time of OR and > 3 months post OR• Projected for 400 pts but stopped early due to harm

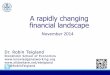
Reversal

ICH = intracranial haemorrhage; OAC = oral anticoagulant; PCC = prothrombin complex concentrate1. van Ryn J et al. Blood (ASH Annual Meeting Abstracts) 2009;114;Abs 1065; 2. Warkentin TE et al. Blood 2012;119:2172–4; 3. Zhou W et al. Stroke 2011;42:3594–9; 4. van Ryn J et al. Blood (ASH Annual Meeting Abstracts) 2011;118:Abs 2316; 5. van Ryn J et al. Pathophysiol Haemost Thromb 2010;37:A94–P486; 6. Eerenberg ES et al. Circulation 2011;124:1573–9; 7. Perzborn A et al. J Thromb Haemost 2009;7(suppl 2):Abs PP-MO-183; 8. Gruber A et al. Haematologica 2009;94(suppl 2):181 Abs 0449; 9. Godier A et al. Anesthesiology 2012;116:94–102. 10. Wang X et al. Clin Pharmacol Ther 2012;91(suppl 1):Abs PI-90; 11. Martin A-C et al. ACC 2012; 24-27 March, Chicago, IL, USA: Abs 904-8; 12. Fukuda T et al. Thromb Haemost 2012;107:253–9
42
Dabigatran Rivaroxaban Apixaban Edoxaban
Oral activated charcoal
Adsorbs and neutralizes, in vitro data1
Adsorbs and neutralizes
Adsorbs and neutralizes,
in vivo data10No data
HaemodialysisHuman volunteers,
case report2Not possible Not possible No data
Fresh frozen plasma Mouse ICH3 model No data No data No data
Activated FVIIa Mouse3, rat4 modelBaboon8, rabbit trauma9 models
Rabbit trauma11
modelRat12 model
3-factor PCC No data No data No data No data
4-factor PCCMouse3, rat4, rabbit
trauma5 model, human volunteers6
Rat7, baboon8, rabbit trauma9,
human volunteers6
Rabbit trauma11
modelRat12 model
• Boehringer-Ingelheim (Canada) Ltd cannot recommend the use of any product outside the Canadian approved Product Monograph
• The content of this slide may contain information not reviewed by Health Canada
Studies of Reversal of NOACs

Reversal
• Relationship between anticoagulation and prediction of cessation of bleeding is not well understood• Experimental data suggest that PCCs and rFVIIa may be effective though there are no clinical data• Limitations of the studies are many:
• Animal data may not be reflective of the clinical situation• Lower dosing of anticoagulants in healthy volunteers does not induce bleeding and may not reflect an emergency situation• Lack of clinical data due to rarity of events, bleeding heterogeneity and lack of predictability in emergency clinical situations

Reversal
Siegal et al. European Heart Journa On-line Dec 7, 2012

Procedures

Patient’s Risk
Spyropoulos et al. Blood 2012 120:2954-2962

Procedure Risk
Spyropoulos et al. Blood 2012 120:2954-2962

Spyropoulos et al. Blood 2012 120:2954-2962
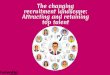
Bridging

When to Stop NOACs
Spyropoulos et al. Blood 2012 120:2954-2962
Low Risk Procedure High Risk Procedure
Normal Renal Function 2 days 3 days
Reduced Renal Function
3 days 4-5 days

Procedures

Procedures

Limitations I Discuss with All Patients
New Agents compared to WarfarinNo Reversal AgentKidney Function needs to be WatchedCostImportant not to miss doses

But they get:
No need for INR monitoring
Decreased risk of cerebral hemorrhage

Just Can’t Use Anticoagulates

Left Atrial Occlusion Devices

Protect AF - Watchman

Prevail Study - Watchman

Prevail Study - WatchmanAcute Events - 2.2% of death, ischemic stroke,
emoblism, procedural complications at 7 daysVascular Complications including perforation
18 Months:- ischemic stroke or embolism: 2.53% in the
device arm versus 2.01% in the control arm, which met the prespecified criterion for non-inferiority
- Composite of stroke, systemic embolism, and cardiovascular/unexplained death at 18 months: 6.4% both groups

CCS Recommendations

CCS Recommendations

CCS Recommendations
•For patients > 75 years, Dabigatran should likely be given at 110mg BID rather than 150mg BID

CAD

Renal Dysfunction
• GFR to be determined annually. • Warfarin is preferred agent for GFR < 30• On HD – avoid OAC and ASA

Questions / Comments