Embed Size (px)
Citation preview

KirstenTornøe
TheChallengeofConsolation:
Aqualitativestudyofnurses’experienceswithpracticingand
teachingspiritualandexistentialcareforthedying
PhDThesis
MFNorwegianSchoolofTheology
Oslo2017

“Itisinthefearfulmomentsofdesolationwherethereisnomeaningleftthatabravestatementofconsolationpenetratesthedarknessandcreatesnewmeaning.Thishappensontheborderwherenothingispossibleanymore.”(Kierkegaard,citedinNorberg,BergstenandLundman,2001p.545)
I
Contents1.Acknowledgments....................................................................................................................III2.Abstract.........................................................................................................................................V3.Listoforiginalpapers............................................................................................................VII4.Introduction..................................................................................................................................14.1Background..........................................................................................................................................14.1.1Conceptualclarifications............................................................................................................................4
4.2Spiritualandexistentialcare:Thestudy’stheoreticalposition........................................54.3Whyresearchlivedexperience?.................................................................................................10
5.Theaimofthestudy................................................................................................................115.1Thespecificaims..............................................................................................................................115.2Theresearchquestions.................................................................................................................11
6.MethodologicalFrameworkPhenomenologicalHermeneutics..............................126.1EdmundHusserl...............................................................................................................................136.2MartinHeidegger.............................................................................................................................156.3Hans-GeorgGadamer.....................................................................................................................176.4PaulRicoeur......................................................................................................................................206.4.1Textunderstoodashumanaction.......................................................................................................216.4.2Distanciationandappropriation..........................................................................................................216.4.3Explanationandunderstanding...........................................................................................................226.4.4Guessingandvalidation...........................................................................................................................22
7.Themethods..............................................................................................................................247.1Datacollection:Narrativeinterviews.......................................................................................247.1.1Thenarrativefocusgroupinterview..................................................................................................26
7.2Dataanalysis:Interpretingtheinterviewtexts.....................................................................267.2.1Thenaïvereading.......................................................................................................................................277.2.2Thestructuralanalysis.............................................................................................................................277.2.3Comprehensiveunderstanding(Interpretedwhole)..................................................................28
7.3Methodologicalconsiderations...................................................................................................297.3.1Thetrustworthinessofthedatacollection......................................................................................307.3.2Thetrustworthinessofthedataanalysis.........................................................................................327.3.3Rationaleforconductingaphenomenologicalhermeneuticaldataanalysis...................347.3.4Mypreunderstanding................................................................................................................................367.3.5Studylimitations.........................................................................................................................................37
8.Thestudy....................................................................................................................................398.1Thesetting..........................................................................................................................................408.2Recruitmentstrategy......................................................................................................................418.3Thesample.........................................................................................................................................418.4Conductingtheinterviews............................................................................................................428.5Ethicalconsiderations....................................................................................................................43
9.MainresultsinPapersI-III...................................................................................................459.1PaperI.................................................................................................................................................459.2PaperII................................................................................................................................................469.3PaperIII..............................................................................................................................................47
10.Discussion................................................................................................................................4810.1Conveyingconsolation.................................................................................................................48
II
10.1.1Thehermeneuticsofconsolation......................................................................................................5010.1.2Therelationaldimensioninthenurses’consolationnarratives.........................................5210.1.3ConveyingconsolationinrelationtoSpiritual/ExistentialandPsychosocialcare....5510.1.4ConsolationthroughExistentialmeaningmaking.....................................................................5710.1.5ThePowerofConsolingpresence.....................................................................................................6010.1.6Consolationunderstoodasamoralresponsibility....................................................................61
10.2Vulnerabilityandhelplessness................................................................................................6810.2.1Vulnerabilityandembodiedengagement.....................................................................................7010.2.2Compassionfatigue.................................................................................................................................7210.2.3Compassionsatisfaction........................................................................................................................75
10.3CompassionandCourage...........................................................................................................7610.3.1Compassion.................................................................................................................................................7610.3.2Courage.........................................................................................................................................................78
10.4Cancourageandcompassionbetaught?..............................................................................8010.4.1Cancompassionbetaught?..................................................................................................................8110.4.2Cancouragebetaught?..........................................................................................................................84
10.5Pedagogicalimplications............................................................................................................8810.5.1Recommendations...................................................................................................................................91
11.Concludingremarks.............................................................................................................94References......................................................................................................................................95PaperI-III......................................................................................................................................107Appendix.......................................................................................................................................108
III
1.AcknowledgmentsLøgstrup(1997)notesthatwhileeverypersonisanindependentandresponsible
individual,healsopointsoutthatweareinescapablydependentuponeachother,and
thatwebelongtoaworldinwhichweholdsomethingofoneanother’slifeinourhands.
Accordingly,althoughaPhDthesisisanindependentpieceofresearch,itwouldnot
havebeenpossiblewithoutthecontributions,supportandencouragementfrommany
others,forwhichIamextremelygrateful.
Firstly,Iwishtoexpressmygratitudetothenurseswhoparticipatedinthestudy.
Thankyoufortrustingmeandforsharingyourspiritualandexistentialcarestories
whichreverberatewithcourage,compassionandconsolation.
Secondly,IwishtothankmysupervisorsProfessorLarsJohanDanbolt,Professor
VenkeSørlieandProfessorKariKvigne.
IamespeciallygratefultoVenkeSørlieandLarsJohanDanboltwhohelpedmepursue
mydreamofwritingthisPhDthesis.LarsJohanDanbolthasbeenmymainsupervisor.
ThankyouforsharingyourinvaluableinsightsinthefieldofPsychologyofReligionand
forhelpingmetoobtainfundingfromTheInnlandethospitaltrust.Youreffervescent
spiritandoptimisticfaithinmyprojecthasbeencontagious,upliftingandinspiring,
throughouttheentireresearchprocess.
Manythankstomyco-supervisorandcolleagueatLovisenbergDiaconalUniversity
CollegeVenkeSørlie.Venkehasaccompaniedandsupportedmeallthewayfrommy
firsttentativeresearchproposalstillthecompletionofthisthesis.Thankyouforyour
invaluableadviceandguidanceonstudydesign,phenomenologicalhermeneuticaldata
analysis,relationalethicsandforshowingme“theropes”onarticlepublishing.
Manythankstomyco-supervisorKariKvigne,whojoinedthesupervisionteamwhen
weanalyzedthedatafromthefirststudy.Thankyouforyourcontributionstointerpret
theresultsandforcriticalreviewofthemanuscripts.Thankyouforinitiatingthecourse
inphenomenologicalhermeneuticalanalysisatHedmarkUniversityCollege,andfor
givingmetheopportunitytoparticipate.Thankyoualsoforyourwarmhospitality.
IV
SpecialthankstoProfessorValerieDeMariniswhocriticallyexaminedandevaluatedmy
thesisatthefinalPhDseminarinOctober2015.
Ihavebeenfortunatetoparticipateinmonthlymeetingswiththepsychologyofreligion
PhDgroupatMFSchoolofTheology,ledbyProfessorLarsJohanDanbolt.Thisgroup
hasbeenanimportantandinspiringmeetingplace.Thankyoutomyresearchfellows
Torgeir,Liv,SigridHelene,Tor,Hege,Anneandtherestofthegroup.
Iamgratefultomyemployer,LovisenbergDiaconalUniversityCollegeandtothe
InnlandetHospitalTrustforfinancialsupport,whichgavemetheopportunitytopursue
myresearchinafulltimepositionforthreeyears.
AwarmthankyoutomycolleaguesatLovisenbergDiaconalUniversityCollegewho
haveencouragedandcheeredmeonthroughthewritingprocess,andtoourexcellent
libraryandcomputerstaff.
Spendinggruelinglonghourswriting,makesonesusceptibletotheperilsofrepetitive
stressinjuries.IamthereforegratefultomyAlexanderteacherNigelHornbyandthe
Alexandertechnique(Cranz,2000;Hollinghurstetal.,2008)whichhasenabledmeto
improvemyposturalalignmentandtoreleasemusculartensionwhilstworkingatthe
computer.
Lastbutnotleast,Iamthankfulforthesupport,loveandencouragementfrommy
familyandfriends,especiallyRigmor,BørreandAnneBerit,whohadfaithinmyPhD
questthroughoutthemanyyearsof“knockingondoors”,huntingforresearchgrants
andwritingresearchproposalsuntilmywindowofopportunityfinallyflungopen!
(ThankyouLarsandVenke!)
IamespeciallygratefultomymotherJudithTornøe,forproofreadingallthreearticles
andtheentirethesis.
Oslo,December2016
V
2.Abstract
Background:Inwesterncountriesanincreasingproportionofolderpatientswith
incurablecancerorotherchronicconditionswillrequirepalliativecare.Respondingto
thefiscalpressureintheNorwegianhealthcaresystemtheNorwegiangovernment
implementedamajorhealthcarereformin2012.This“CoordinationReform”downsized
specializedhealthcareunitsinthesecondaryhealthcaresectorandtransferredmore
palliativecareresponsibilitiestonursinghomesandhomecarenursingintheprimary
healthcaresector,whichoftenlackadequatenursingexpertise.Asaconsequence,less
qualifiedcareworkersaswellasregisterednursesincreasinglyhavetoprovide
palliativecare,whichincludestheimpeccableassessmentandtreatmentofphysical,
psychosocial,spiritualandexistentialpain.However,researchshowsthatspiritualand
existentialcareforthedyingisfrequentlyoverlookedinmostcaresettingsandthat
nursesandothercareworkersoftenfeelanxiousanduncertainaboutproviding
spiritualandexistentialcarefordyingpatients.Thisindicatesthatthereisawidespread
needforspiritualandexistentialcarecompetencyinpalliativecare.Thereisagapinthe
literatureabouthownursesmayalleviatedyingpatients’spiritualandexistential
sufferingintheireverydaypractice.Thereisalsoagapintheliteratureabouthowto
trainnursingstafftoprovidespiritualandexistentialcareforthedying.
Aim:TheoverallaimofthisPhDthesisistoilluminatethemeaningofregisterednurses’
experienceswithpracticingandteachingspiritualandexistentialcareforthedyingin
differentNorwegianhealthcarecontexts.TheaimsinstudiesI,IIandIIIwere:
I: Todescribethemeaningofhospicenurses’livedexperiencewithalleviatingdyingpatients’spiritualandexistentialsuffering
II: Todescriberegisterednurses’experienceswithspiritualandexistentialcarefordyingpatientsinageneralhospital
III: ToilluminateapioneeringNorwegianmobilehospicenurseteachingteam’sexperiencewithteachingandtrainingcareworkersinspiritualandexistentialcareforthedyinginnursinghomesandhomecaresettings
Methodsanddesign:Thisisaqualitativestudy.StudyIwasbasedoneightindividual
narrativeinterviewswithhospicenurses.StudyIIwasbasedonsixindividualnarrative

VI
interviewswithregisterednursesinamedical-oncologicalwardinageneralhospital.
StudyIIIwasbasedonanarrativefocusgroupinterviewwiththethreehospicenurses
inthemobileteachingteam.Aphenomenologicalhermeneuticalmethodwasusedto
analyzetheinterviewtexts.
Mainresults:Spiritualandexistentialcarewasaboutconsolingthedyingby
unburdeningthemandfacilitatingapeacefuldeath.Thenursesconveyedconsolationby
helpingtheirpatientstosettlepracticalissues,reconcilethemselveswiththeirloved
onesandtofindpeacewithGod,andbysimplybeingpresentwiththeirpatientsto
sharethesuffering.Conveyingconsolationprovedtobeadeeplyrelationalpractice,
whichdemandedcourageandcompassionbecauseitexposedthenursestotheirown
vulnerability,mortalityandhelplessness.Practicaltrainingprogramsproviding
experientiallearningopportunitiesthroughsituatedbedsideteachingmaybeefficient
todevelopcareworkers’courageandcompetencytoprovidespiritualandexistential
careforthedying.However,theresultssuggestthatsuchprogramsshouldalso
introducenursingstafftoreligiousperspectivesonsufferingandreligiousreasoning,
becausetheresultsshowthatthenursesexpresseduncertaintyaboutaddressing
patients’religiousneedsduetoalackofformalknowledge.
Conclusions:Whennothingelsecanbedone,bearingwitnessandsharingthepatients’
sufferingmaybeconsolingactsinthemselves.Nursesandcareworkersinend-of-life
careconfrontintractablesuffering.Hence,theycannotalwaysexpecttobesuccessfulin
theireffortstoalleviateit.Therefore,thestudyresults,whichindicatethatconsolation
maybeconveyedandsustainedthroughpresenceandrelatedness,areextremely
important.Alessqualifiedworkforceincreasinglydominatesnursinghomesand
homecarenursingatatimeofincreasingprevalenceofcomplexhealthconcerns.Mobile
expertnurseteachingteamsinspiritualandexistentialcare,(andothernursingfields)
maybeaneffectivemeanstoredressthewideninggapbetweenworkforcequalityand
thedemandforhighqualitycareintheprimaryhealthsector.
Keywords:consolation,spiritualandexistentialcare,palliativecare,healthcarereform,
phenomenologicalhermeneuticalmethod,narrativeinterviews,primaryandsecondary
healthcaresector

VII
3.ListoforiginalpapersThethesisisbasedonthefollowingpapers,whichwillbereferredtointhetextbytheir
romannumerals:
I.Tornøe,K.A.,Danbolt,L.J.,Kvigne,K.,&Sørlie,V.(2014).Thepowerofconsoling
presence-hospicenurses'livedexperiencewithspiritualandexistentialcareforthedying.BMCNursing,13(1),25.
II.Tornøe,K.A.,Danbolt,L.J.,Kvigne,K.,&Sørlie,V.(2015).Thechallengeof
consolation:nurses’experienceswithspiritualandexistentialcareforthedying-aphenomenologicalhermeneuticalstudy.BMCNursing,14(1),62.
III.Tornøe,K.,Danbolt,L.J.,Kvigne,K.,&Sørlie,V.(2015).Amobilehospicenurse
teachingteam’sexperience:trainingcareworkersinspiritualandexistentialcareforthedying-aqualitativestudy.BMCPalliativeCare,14(1),43.
1
4.IntroductionTheoverallaimofthisPhDthesisistoilluminatethemeaningofregistered
nurses’experienceswithpracticingandteachingspiritualandexistentialcarefor
thedyingindifferentNorwegianhealthcarecontexts.
4.1BackgroundInwesterncountriesanincreasingproportionofpatientsareolderpeoplelivingwith
incurablecancerorotherchronicconditionsthatwillrequirepalliativecareforshorter
orlongerperiodsoftime(Haug,Danbolt,Kvigne,&Demarinis,2014,p.68;Norwegian
DirectorateofHealth,2015;Seale,1999).TheevidenceondeathanddyinginWestern
EuropeandtheUSAsuggeststhatamajorityofpeopledieinhospitals(Costello,2006).
Inlinewiththistrend,Norwegianpalliativecarehasundergonequitedramaticchanges
duringthelastthirty-fiveyears.Movingfromitsidealisticandsocialhospiceorigins,
Norwegianpalliativecarehasbeenintegratedinthepublichealthcaresystemwhichis
wellorganizedwithintwomainsectors:theprimaryhealthandlong-termcaresector
(nursinghomesandhomecarenursing),andthesecondaryhealthcaresector,involving
hospitalandspecialistservices(Romoren,Torjesen,&Landmark,2011).Specialist
palliativecareservices,includinghospices,areorganizedwithinthelevelofsecondary
healthcareinsomatichospitals(Bollig,Rosland,&Husby,2013;Haugetal.,2014;
NorwegianDirectorateofHealth,2015;Strømskag,2012).
However,theNorwegianhealthcaresystemisstrainingunderfiscalpressure,following
theinternationaltrendofcuttinghealthcarecostsanddownsizingspecializedhospital
unitsinsecondaryhealthcare(EuclidNetwork,2012;NorwegianMinistryofHealthand
CareServices,2012;WorldHealthOrganization,2002).Respondingtotheeconomic
challengesinthehealthcaresystem,theNorwegiangovernmentimplementedamajor
healthcarereformin2012:“TheCoordinationreform”(NorwegianMinistryofHealth
andCareServices,2012).Theaimwastoalleviatepressureonthesecondaryhealth
caresectorbyupgradingtheprimaryhealthcaresectorandbytransferringmore
palliativecareresponsibilitiestonursinghomesandhomecarenursing(Bolligetal.,
2013;NorwegianMinistryofHealthandCareServices,2012).Henceforth,nursing

2
homesandhomecaresettingsarebecomingthehospicesofthefuture(Abbey,Froggatt,
Parker,&Abbey,2006).Asaconsequence,lessqualifiedcareworkers(suchas
unregulatednursingassistants)aswellasregisterednurseswillincreasinglyhaveto
providepalliativecareinnursinghomesandhomecarenursing(Annear,Lea,&
Robinson,2014;Colombo,Llena-Nozal,Mercier,&Tjadens,2011;Leclercetal.,2014).
InNorwaynearly50%ofthedyingareresidentsinnursinghomes,withunderpowered
budgetsandoftenlackingadequateexpertise(Bolligetal.,2013).
TheWorldHealthOrganization(WorldHealthOrganization,2002)maintainsthat
palliativecareincludestheimpeccableassessmentandtreatmentofphysical,
psychosocialandspiritualpain.Agrowingbodyofinternationalpalliativecareresearch
indicatesthatspiritualandexistentialcareisanintegralcomponentofholistic,
compassionatecareforthedying(Bachner,O'Rourke,&Carmel,2011;Nolan,2011;
Steinhauseretal.,2000).Oneofthekeygoalsofpalliativecareistoalleviatedying
patients’suffering(Delgado-Guayetal.,2011).EricCassel(1991a)statesthatalthough
sufferingoftenisrelatedtoacutepainorotherbodilysymptoms,itextendsbeyondthe
physical.“Mostgenerally,sufferingcanbedefinedasthestateofseveredistress
associatedwitheventsthatthreatentheintactnessofperson”(Cassell,1991a,p.33).
Dyingpatientsliterallyexperienceathreattotheir“intactnessofperson”,andassuch
arepronetoexperiencesuffering.Existentialandspiritualsufferingareamongthemost
debilitatingconditionsindyingpatients.Henceforth,thereisagreatneedforpalliative
spiritualandexistentialcarecompetencyintheprimaryaswellasthesecondarylevels
oftheNorwegianhealthcaresector(Boston,Bruce,&Schreiber,2011).
Yet,researchrevealsthatspiritualandexistentialcareisfrequentlyoverlookedin
palliativecare.Thereisagrowingawarenessthatmostcaresettingsfailtoprovide
optimalspiritualcaretothosewithseriousillnessandthoseattheendoflife(Puchalski
etal.,2009).Patientswithadvancedillnessesreportthattheirmedicalcaregivers
infrequentlyprovidespiritualcare(Balbonietal.,2013;Sæteren,Lindström,&Nåden,
2011).AccordingtoUdo(2014)severalstudiesrevealthatmanypatientsare
dissatisfiedwiththeemotionalandexistentialsupporttheyaregiven,eveniftheyare
satisfiedwiththeirmedicalandphysicalcare.ThisissupportedbyGroenvold,Pedersen,
Jensen,Faber,andJohnsen(2006)whofoundthatasignificantnumberofdyingpatients

3
longforadequatespiritualorexistentialcareandcounseling.Inspiteofthis,seriouslyill
patientsoftenrefrainfromdiscussingtheirspiritualandexistentialthoughtswith
nursesbecausetheydonotfeelthatnursesacknowledgethisneed(Udo,2014).
Researchshowsthatregisterednursesandcareworkersoftenfeelinadequately
preparedtoprovidespiritualandexistentialcareforthedying,andthatthismakes
themanxiousanduncertain(Christensen,2008;McSherry&Jamieson,2013;Noble&
Jones,2010;Pesut,Fowler,Taylor,Reimer-Kirkham,&Sawatzky,2008;Udo,2014).
Severalstudiesindicatethatalackofskillsinpsychosocialandspiritualcaremayresult
inhighlevelsofmoraldistress,griefandburnout(Back,Bauer-Wu,Rushton,&Halifax,
2009;Bosma,Apland,&Kazanjian,2010;Noble&Jones,2010;Rushtonetal.,2009;
Vivat,2008).Studiesalsoindicatethatthereisawidespreadneedfortraininginall
aspectsofspiritualandexistentialcareforthedying(Balbonietal.,2013;Holloway,
Adamson,McSherry,&Swinton,2011).Accordingtotheliterature,nurses’andcare
workers’discomfortrelatedtoprovidingspiritualandexistentialcareforthedyingmay
leadtounmetspiritualandexistentialneedspossiblyleadingtoincreasedpatient
suffering(Backetal.,2009;Bosmaetal.,2010;Noble&Jones,2010;Rushtonetal.,
2009;Vivat,2008).
Thereisagapintheresearchliteratureabouthowpatients’existentialwellbeingmay
bebestsupportedbynursesandotherhealthcareprovidersineverydaypractice
(Henoch&Danielson,2009).In2014Pesutetal.conductedascopingreviewto
summarizetheavailableevidenceconcerningpalliativecareeducationfornursesand
othernursingcareproviders(Pesutetal.,2014).Noneofthereferencesintheirreview
explicitlymentionedtrainingcareworkersinspiritualandexistentialcareforthedying.
Thissuggeststhatthereisagapintheliteratureconcerningthisissue.Thisthesis,which
isanempiricalstudyofregisterednurses’experienceswithpracticingandteaching
spiritualandexistentialcareforthedying,willhopefullycontributetobridgethese
importantgaps.
NursingresearchinspiritualcarehasuntilrecentlybeendominatedbyAnglo-American
studies.Althoughthisresearchyieldsvaluableinsights,itcannotbedirectlyappliedto
Scandinaviancontexts,duetothedifferencesinspiritualandreligiousclimatesinthese
societies(Lundmark,2006).OnthegroundsofdifferentsurveysSørensen(2012)notes
4
thatreligionisamorepervasiveanddiversephenomenonintheUSA,thaninthe
Scandinaviancountrieswherelargenumbersofthepopulationbelongtothe
protestant/Lutheranmajoritychurches.(Sørensen,2012),InNorwayapproximately73
%ofthepopulationbelongtotheChurchofNorway(StatistiskSentralbyrå(Central
BureauofStatisticsinNorway),2015).However,inspiteofthelargechurch
membership,Scandinaviansocietiesarequitesecularizedandreligiousandspiritual
thoughtsandpracticesarelargelyregardedasprivatematters.However,thisdoesnot
meanthatthemajorityhasturnedawayorishostiletoreligion(DeMarinis,2008;la
Cour,2008;laCour&Hvidt,2010).Althoughtheinterestintraditionalreligionis
declining,Norwayisgraduallybecomingamoremulticulturalandreligiouslydiverse
society(Ulland&DeMarinis,2014),andagrowingnumberofScandinaviansconsider
themselvestobe“spiritualbutnotreligious”.Dismissingdogmatictruths,their
religiosityandreligiousparticipationismainlyrootedinemotionsandhuman
experience,asameanstosearchforandexpress“authenticself-hood”(Botvar&
Schmidt,2010;DeMarinis,2008).Thisformforspiritualityor“worldviewconstruction”
isrelatedto“existentialmeaningmaking”,whichmayormaynotincludeatranscendent
dimension(DeMarinis,2008;Schnell,2009,2010;Schnell&Keenan,2011).
Despitethe“privatizedattitudes”towardsreligionandspiritualityintheScandinavian
countries,recentyearshaveyieldedagrowingnumberofScandinaviannursingstudies
inspiritualandexistentialcare(Ilkjær,2012;Sæterenetal.,2011;Torskenæs&Kalfoss,
2013;Torskenæs,Kalfoss,&Sæteren,2015;Ødbehr,2015)whichdrawontheemerging
bodyofresearchwithinthefieldofpsychologyofreligion,spiritualityandhealth(Haug,
2015;Koenig,King,&Carson,2012;Masters&Hooker,2013;Sørensen,2012;Sørensen,
Lien,Landheim,&Danbolt,2015).ThisPhD.thesisistobeviewedasaNorwegian
contributiontotheemergingfieldofScandinaviannursingresearchinspiritualand
existentialcare.
4.1.1ConceptualclarificationsSpiritualityisaninternationaltermwhichisusedbynurseacademics(Narayanasamy,
2014;Paley,2008;Pesut,2008b;Swinton&Pattison,2010)aswellasbyacademicsin
otherfieldssuchaspracticaltheology(Bueckert&Schipani,2006;Swinton&Mowat,
5
2006)andinpsychologyofreligion(Koenigetal.,2012;Paloutzian&Park,2013).
However,NorthernEuropeanandScandinaviancontextstendtobemorefamiliarwith
termssuchasviewoflife,worldview,religion,meaning-making,existentialityand
existentialquestions(Stifoss-Hanssen,1999;Stifoss-Hanssen&Kallenberg,1998;Ulland
&DeMarinis,2014).(SeeforexampleKarlsson,Friberg,WallengrenandÖhlén’s(2014)
andStrang,Henoch,Danielson,BrowallandMelin-Johansson’s(2014)Swedishstudies
aboutdyingpatients’existentialissues.)Accordingly,“itisnottobeassumedthat
Norwegiansusethetermspiritualityinclinicalpractice”(Ulland&DeMarinis,2014,p.
4).Takingthisintoaccount,thenursesinthisstudywereaskedtonarrateabouttheir
experienceswithpracticingandteachingspiritualandexistentialcareinorderto
captureasmuchin-depthdataaspossible.InlightofUllandandDeMarinis(2014)itis
interestingtonotethatthenursesdidnotdiscernbetweenspiritualandexistentialcare
duringtheinterviews.Consideringthenurses’useoftheterms,andthefactthatthese
termsoftenareusedsynonymouslyinthenursingliterature,(Bostonetal.,2011;
Boston&Mount,2006;Henoch&Danielson,2009)theterm“spiritualandexistential
care”willbeusedthroughoutthisthesis.However,itisimportanttonotethattheuseof
thesetermsvaryintheliterature,whichiscited.Forthesakeofacademicrigourthe
researchers’useofthetermswillbequoted.(SwintonandPattison(2010)forinstance
useonlytheterms“spirituality”,and“spiritualcare”.)
4.2Spiritualandexistentialcare:Thestudy’stheoreticalposition
Spiritualityisahighlydebatedconceptduetothemanyvariationswhichemergefrom
thenursingliterature(Paley,2008;Pesut,2008a).Severalresearcherspointoutthat
sincethereseemstobenosingleagreeddefinitioninthenursingliterature,theterm”
spiritualcare”isopentointerpretation(Kalish,2012;Noble&Jones,2010;Pesutetal.,
2008;Reimer-Kirkham,2009;Swinton&Pattison,2010).Itisthereforeimportantto
clarifythisstudy’stheoreticalstandpoint.
Mypreunderstandingofspiritualandexistentialcareisshapedbyseveralyearsof
experienceasaregisterednurse,caringfordyingpatientsincancerwardsandnursing
homes,mybackgroundasanordaineddeaconintheNorwegianLutheranChurch,a

6
master’sdegreeintheology,(withathesisonspiritualandexistentialend-of-lifecare
basedonnarrativetheology)andmybookaboutspiritualandexistentialcareforthe
dying,basedonmymaster’sthesis(Tornøe,1996).Asanurseeducatorandresearcher,
IfindthatSwintonandPattison’s(2010)pragmaticandfunctionalunderstandingof
spiritualityinnursingcareresonateswithmyownviewpointswhichhaveevolved
throughmyownspiritualandexistentialcareexperiencesinend-of-lifecareandmy
educationalbackground.Ihavethereforechosentogroundthisstudyintheir
understandingofspiritualitybecauseitfitsthestudy’saimwhichistoilluminatethe
meaningofregisterednurses’experienceswithpracticingandteachingspiritualand
existentialcare,ratherthanclarifyingtheontologicalandconceptualquestionsabout
howtodefinespiritualandexistentialcareintheresearchliterature(Reimer-Kirkham,
2009).Thiswillbeelaboratedinthefollowing:
WhilePaley(2008)arguesthatthewiderangeofspiritualitydefinitionsrendersthe
conceptmeaninglessandinsignificant,SwintonandPattison(2010)claimthatthe
concept’sstrengthlaysinitsvagueness,andthatitcannotbedismissedjustbecauseit
doesnotfitwithastrictempiricistviewofreality.Whilehardpositivistsmayarguethat
conceptsinlanguagewhichdonotcorrespondwitheventsorthingsinthematerial
worldshouldnotbeattendedto,SwintonandPattison(2010)statethatnotallconcepts
aresimplyreferentialandtheystillaccordvaluewithinthesocialworld.Drawingon
Wittgenstein,they(2010)pointoutthatwordsareperformativeandexpressiveaswell
asreferential.Accordingly,wordsarenotessentialistintheirmeaning.Ratherthan
deliberatingoverthelexicographicalmeaningsofspirituality,theyadvocatethatitis
moreusefultodevelop“athin,vagueandfunctionalunderstandingofwhatthisword
anditscognatesmightdointheworldofhealthcare”.(Swinton&Pattison,2010,p.227)
Henceforth,theymakeitclearthatdefiningspiritualityforhealthcarepurposesisnot
thesameasclaiminganydirectontologicalstatus(Swinton&Pattison,2010).
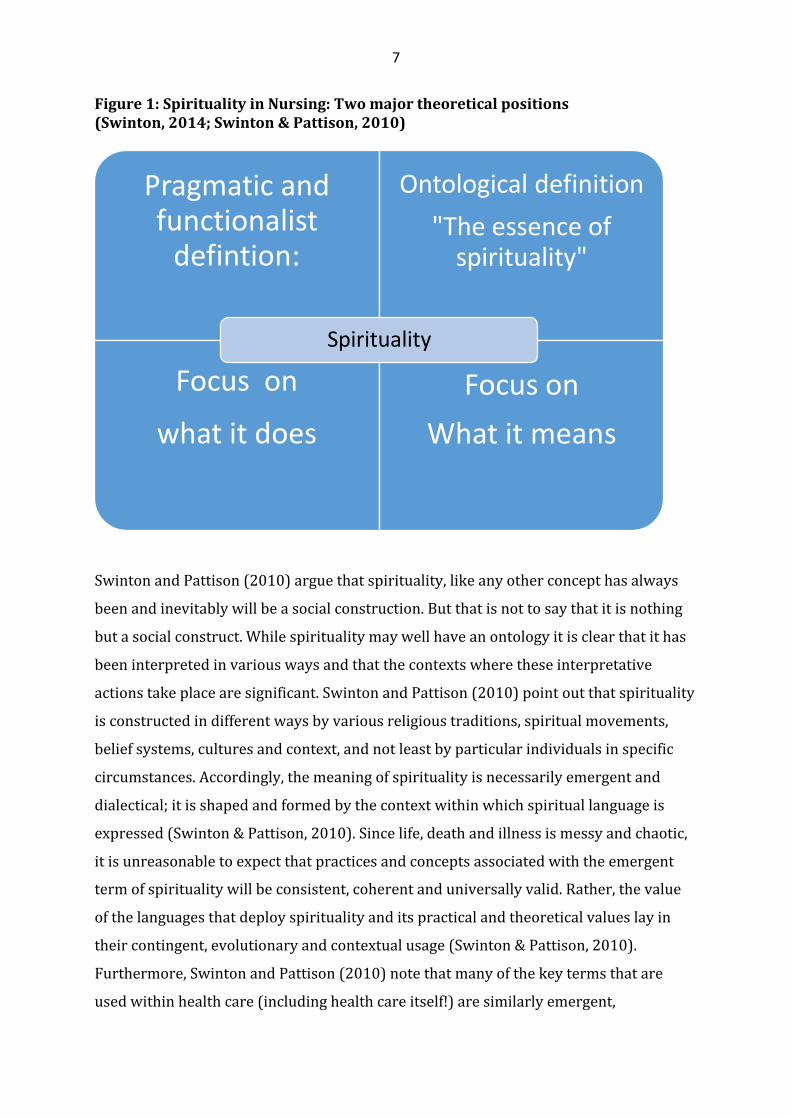
AccordingtoSwinton(2014),anydefinitionofspiritualityinhealthcareisapragmatic,
ratherthananontologicdescription,whichmeansthatthefocusisonwhattheconcept
“does”(intermsofitseffectonhealthcarepractice),ratherthanwhatit“is”(intermsof
essentialdefinitions).Thisisillustratedinfigure1.
7
Figure1:SpiritualityinNursing:Twomajortheoreticalpositions(Swinton,2014;Swinton&Pattison,2010)
SwintonandPattison(2010)arguethatspirituality,likeanyotherconcepthasalways
beenandinevitablywillbeasocialconstruction.Butthatisnottosaythatitisnothing
butasocialconstruct.Whilespiritualitymaywellhaveanontologyitisclearthatithas
beeninterpretedinvariouswaysandthatthecontextswheretheseinterpretative
actionstakeplacearesignificant.SwintonandPattison(2010)pointoutthatspirituality
isconstructedindifferentwaysbyvariousreligioustraditions,spiritualmovements,
beliefsystems,culturesandcontext,andnotleastbyparticularindividualsinspecific
circumstances.Accordingly,themeaningofspiritualityisnecessarilyemergentand
dialectical;itisshapedandformedbythecontextwithinwhichspirituallanguageis
expressed(Swinton&Pattison,2010).Sincelife,deathandillnessismessyandchaotic,
itisunreasonabletoexpectthatpracticesandconceptsassociatedwiththeemergent
termofspiritualitywillbeconsistent,coherentanduniversallyvalid.Rather,thevalue
ofthelanguagesthatdeployspiritualityanditspracticalandtheoreticalvalueslayin
theircontingent,evolutionaryandcontextualusage(Swinton&Pattison,2010).
Furthermore,SwintonandPattison(2010)notethatmanyofthekeytermsthatare
usedwithinhealthcare(includinghealthcareitself!)aresimilarlyemergent,
Pragmaticandfunctionalistdefintion:
Ontologicaldefinition"Theessenceofspirituality"
Focuson
whatitdoesFocuson
Whatitmeans
Spirituality

8
constructedandchanging.Theterms“community”,“care”,“love”and“friendship”for
instance,areequallyvague,contestedandmulti-orpolyvalent,asspiritualitybut
nonethelessimportantandnecessary.Thus,thereisnoinherentreasonwhyalackof
clarityshoulddenotealackofsignificance.Rather,multipledefinitionsmaybe
indicativeofthenecessityandtheflexibilityofthetermtomeetparticularneedsthat
wouldotherwisegounmet(Swinton&Pattison,2010).AsSwinton(2014,p.163)points
out:“Spiritualityisunabashedlyafluidanddeeplypragmaticconceptthatshiftsand
changesaccordingtothecontextwithwhichitisconstructedandtheneedsitis
attemptingtomeet.”
AccordingtoSwintonandPattison(2010),inawesternsecularizedhealthcaresystem
anemphasisonspiritualityattemptstocapturesomethingofthephenomenologyof
illness(thelivedexperienceofbeingill)whichhasbeenunderplayedbyhighly
medicalizedmodesofhealthcarestrategyanddelivery.Spiritualityinahighly
secularizedhealthcarecontextseekstorecapturethosedimensionsofthehuman
personthatwereonceexpressedinreligiouslanguageandthatarenotcaptured
effectivelybybiomedicaldiscourse,suchas“theimportanceofmeaning,purpose,hope,
love,Godandrelatedness”(Swinton&Pattison,2010,p.232).SwintonandPattison
(2010)pointoutthatsuchissuesoftencometovitalprominenceduringtheexperience
ofbeingill.Accordingtothem(2010),spiritualcarecannotbeunderstoodasasingle
task,orevenadiscreteseriesoftasks.Rather,itdenotesthemultifarious,disparateand
pluriformskillsandperspectivesthatnursesandcareworkersneedtolearninorderto
caterwellforcertainaspectsoftheexperienceofillnessasitislivedoutwithin
particularhealthcarecontexts.
SwintonandPattison(2010)notethatthetermspiritualityandthediscoursethat
surroundsit,canatitsbest,functionasasensitizingconceptthatdrawsourattentionto
suchissuesasmeaning,purpose,relationality,hope,value,love,Godandtranscendence,
areas,whichwellmaybeoverlookedinhealthcare,withoutthissensitizingfunction.
Accordingtothem(2010),spiritualityisnotperceivableasasinglething,butratherasa
responsetoavarietyofhumanquests,whichoftenareactivatedintimesofillnessand
duress.Thus,ifoneaspectoffunctionalspiritualityisthehumansearchformeaning,
thencarerswillneedtodevelopapproachesandmethodswhichenablethemtodeal

9
withtheexistentialquestsofpeopleintimesofillness.Ifspiritualitydenotesaquestfor
hope,thedesireforrelationshipsortheconstructionofpurpose,variousapproaches
andtechniqueswillberequiredtoenablenursestocarewellforthisaspectofpeople’s
livedexperienceofillness.IfspiritualityisasearchforGodandthetranscendent,then
facilitatingthatquestrequiresaparticularsetofskillsandknowledgeofreligious
traditions,theology,religiouspracticesoratleastanabilitytorecognizetheneedandto
refertoappropriatepersons(Swinton&Pattison,2010).
Forthepurposeofthisstudy,SwintonandPattison’s(2010,p.229)threemost
importantpointsare:
1. Intimesofillness,whatmightlooselybecalledspiritual,meaning,identityand
purposeissuesmaycometothefore,evenwhenreligionandspiritualityformally
definedhavenotpreviouslybeenofsignificanceforthepatient.“Itisinsuch
situationsinthe‘everydayness’oftheirlivesthatpeoplearemostlikelytothink
about‘spiritual’issuesortohave‘spiritualneeds’howeverinchoateorill-
articulated”.(Swinton&Pattison,2010,p.229)
2. Itseemstobethecasethatordinarypeople,patients,carersandprofessional
healthcareworkersseemtofindthelanguageofspiritualitytobefunctional,helpful
andmeaningfulespeciallyduringtimesofillnessandduress(WHO,1998),despite
thelackofcleardefinitionsofwhatspiritualitymightmeaninreferentialterms.
Thereisevidencetosuggestthatthevoices,habitsandperceptionsofordinary
peopleshouldbecloselyattendedtoinanyaspectofhealthcare,andespecially
whenitappearstorelatecloselytoissuesofpurpose,identityandtheself,asthe
languageofspiritualityoftendoes.
3. Ifillpeopleandtheircarersareusingtheconceptofspirituality-“andusingitwith
earnestnessandseriousintent,primafacie,theirviewsshouldbetakenseriouslyby
academicsandhealthcareproviders”.(Swinton&Pattison,2010,p.229)(However,
asnotedinsection4.1.1,itisimportanttobeawarethatinNorthernEuropeanand
Scandinaviancontexts,patientsandnursestendtobemorefamiliarwithtermssuch
10
asviewoflife,worldview,religion,meaning-making,existentialityandexistential
questions.)
InlinewithSwintonandPattison(2010),theobjectiveofthisstudyisnottoquestion
thevalidityofthenurses’languageordefinitionsofspiritualitybuttolistentothemin
ordertoexplorethemeaningoftheirlivedexperienceswithpracticingandteaching
spiritualandexistentialcare.
4.3Whyresearchlivedexperience?Overmanyyearsthescientificmethodhasbecomethemostimportantmeansof
generatingevidenceabouttheworldandhumansociety,andconsiderableefforthas
beendevotedtoimplementevidencebasedpracticeinnursing(EBP)(Avis&
Freshwater,2006).However,Benner(2000a),drawingonMerlau-Ponty(1962)points
outthatscientificlanguagewhichomitsourembodiedexperienceofillness,recovery
andhealthalsoleavesoutperceptualcapacitiesthatenablereasoningandactingas
moralagentsinparticularlifeworlds.SolvollandLindseth(2015)notethat
phenomenologicallyspeaking,weunderstand”experiences”asaseriesofsignificant
eventsthatconstitutetheworldandabodilyself.Thebodyandawarenessfindtheir
placesinthisflowratherthanprecedingit.AccordingtoSolvollandLindseth(2015)
practitioners’professionalknowledgecanbe“observed”throughtheirnarrativesabout
theirexperiences.Whileeachnarrativeisunique,inthesensethatitisbasedonthe
practitioner’spersonalexperience,onepractitioner’sexperiencemayberepresentative
ofotherpractitionerswhoworkinthesamefieldofcare.Accordingly,gleaning
knowledgefromoneexamplemaybeaformofanalogicalreasoning,whichcanbe
transferableandthuscontributetosignificantlearningforotherpractitioners.
Therefore,exploringnurses’livedexperiencewithpracticingandteachingspiritualand
existentialcaremaybeausefulmeanstouncoveressentialembodied,tacitandpractical
knowledge,whichmaybetransferableandusefulforothersinend-oflifecare(Aadland,
1997).
11
5.Theaimofthestudy
TheoverallaimofthisPhDthesisistoilluminatethemeaningofregisterednurses’
experienceswithpracticingandteachingspiritualandexistentialcarefordyingpatients
indifferentNorwegianhealthcarecontexts.
5.1Thespecificaims
PaperI:Todescribethemeaningofhospicenurses’livedexperiencewithalleviating
dyingpatientsspiritualandexistentialsuffering
PaperII:Todescriberegisterednurses’experienceswithspiritualandexistentialcare
fordyingpatientsinageneralhospital
PaperIII:ToilluminateapioneeringNorwegianmobilehospicenurseteachingteam’s
experiencewithteachingandtrainingcareworkersinspiritualandexistentialcarefor
thedyinginnursinghomesandhomecaresettings
5.2Theresearchquestions
PaperI:Whatarethehospicenurses’experienceswithalleviatingdyingpatients’
spiritualandexistentialsuffering?
PaperII:Whataretheregisterednurses’experienceswithalleviatingdyingpatients’
spiritualandexistentialsuffering?
PaperIII:Whatarethemobilehospicenurseteachingteam’sexperienceswithteaching
andtrainingcareworkersinhomecareandnursinghomesinspiritualandexistential
careforthedying?
12
6.MethodologicalFrameworkPhenomenologicalHermeneutics
Whilemethodologyhastodowiththeoverallapproachtoaparticularresearchfield,
implyingafamilyofmethodsthatshareparticularphilosophicalandepistemological
assumptions,methodsarespecifictechniquesthatareusedfordatacollectionand
analysis.Henceforth,thechoiceoftechniques(-ormethods)usedinastudy,mustbe
consistentwithitsmethodologicalframework(Swinton&Mowat,2006).Thestudy’s
methodologicalframeworkwillnowbepresented.
Theoverallaimofthisstudyistoilluminatethemeaningofnurses’experienceswith
practicingandteachingspiritualandexistentialcarefordyingpatientsindifferent
Norwegianhealthcarecontexts.Thisdeterminedthechoicetoanchorthestudyinthe
traditionofphenomenologicalhermeneutics(Gadamer,2004;Heidegger,1962;Ricoeur,
1976,1981,1984,1992,2008)withspecialemphasisonRicoeur’s(1976)interpretation
theory.FollowingRicoeur’s(1976)lineofthought,oneperson’sexperiencecannot
directlybecomeanother’s:
Aneventbelongingtoonestreamofconsciousnesscannotbetransferredassuchintoanotherstreamofconsciousness.Yet,nevertheless,somethingpassesfrommetoyou.Thissomethingisnottheexperienceasexperienced,butitsmeaning.Hereisthemiracle.Theexperienceasexperiencedaslived,remainsprivatebutitssense,itsmeaningbecomespublic.(Ricoeur,1976,pp.15-16)
DrawingonRicoeur,theoverallaimofthisstudyistointerpretand“makepublic”the
meaningofthenurses’spiritualandexistentialcareexperiences.
Phenomenologicalhermeneutics,beingtheprocessofinterpretinganddescribing
humanexperiencetounderstandthemeaningofthatexperienceiswellpositionedasa
suitablemethodologyforhumanscienceresearch.Itisnotaresearchmethodassuch,
butratherbothatheoreticalperspectiveandmethodologythatliesbehindthemethods
employedinaparticularstudy(Tan,Wilson,&Olver,2009;VanManen,2014).
Increasinglyphenomenologicalhermeneuticsisthephilosophicalunderpinningof
choiceinqualitativehealthcareresearchandisfrequentlyusedinnursingresearch
13
(Lindseth&Norberg,2004;Sørlie,2001;Tanetal.,2009;Torjuul,2009;Ødbehr,Kvigne,
Hauge,&Danbolt,2014).
Thetraditionofphenomenologicalhermeneuticswillnowbeoutlined,drawingonthe
worksofHusserl,Heidegger,GadamerandRicoeur.Thiswillbefollowedbyan
explanationofhowRicoeur’s(1976)phenomenologicalhermeneuticalinterpretation
theoryinformedandguidedthechoiceofmethodsthatwereusedinthestudy.
6.1EdmundHusserlEdmundHusserl(1859-1938)isgenerallyregardedastheintellectualfounderof
phenomenologicalphilosophy(VanManen,1990,2014).AccordingtoPorterand
Robinson(2011)Husserl’sphilosophicalresearchisnothermeneutics.Itisnoteven
hermeneuticallyinclinedinitsmethodologybecauseheavoidstakingan“interpretive”
stanceinmanyrespects,focusinginsteadonthings(phenomena)andourconsciousness
orexperienceofthem.Nonetheless,Husserl’sphenomenologyisofinvaluable
significanceforhermeneuticsindirectly,andforthedevelopmentof“phenomenological
hermeneutics”directly.Hisinfluenceisparticularlypronouncedinthehermeneutical
developmentsofMartinHeidegger(1889-1976),Hans-GeorgGadamer(1900-2002)
andPaulRicoeur(1913-2005),allofwhomhavetakenupandexpandedtheirownform
ofphenomenology(Porter&Robinson,2011).Henceforth,thisoutlineof
phenomenologicalhermeneuticalthoughtwillbeginwithabriefdescriptionof
Husserlianphenomenology.
ForHusserlphenomenologyisadisciplinethatendeavorstodescribehowtheworldis
constitutedandexperiencedthroughconsciousacts(VanManen,1990).Husserl’s
phrase“ZudenSachen”(backtothethings)hasbecomeawatchwordin
phenomenology(VanManen,2014,p.92).Generally,“tothethings”seemtomean“to
theissuesthatmatter”.Husserldefinesphenomenologyasadescriptivephilosophyof
theessencesofpureexperiences.Heaimstocaptureexperiencesinitsprimordialorigin
withoutinterpreting,explainingortheorizing.ForHusserl,theessenceswhich
phenomenologyconcernsitselfwithare“Erlebniswesen”,essencesoflivedexperiences.
Onlyknowledgethatisderivedfromimmediateexperientialevidencecanbeaccepted

14
(VanManen,2014,p.89).Inhislastandposthumouslypublishedtext“Thecrisisof
EuropeanSciencesandTranscendentalPhenomenology”(Husserl,1970),citedinVan
Manen(1990,p.182),Husserldevelopedtheideaofthelifeworldanddescribeditas
“alreadythere”,“pregiven”,theworldasexperiencedinthe“naturalprimordialattitude”
thatof“originalnaturallife”(Husserl,1970,pp.103-186)citedinVanManen(1990,p.
182).Husserlreservedthenotionofthe“naturalattitude”tothe“taken-for-
grantedness”ofeverydaythinkingandacting(VanManen,2014).This“naturalattitude”
manifestsitselfinournaturalinclinationtobelievethattheworldexistsoutthere,
independentofourpersonalexistence.Husserlianphenomenologydoesnotdenythe
externalexistenceoftheworld.Butitemphasizestheimportanceofbeingabletoshift
from“anaturaltoaphenomenologicalattitude”inordertoperceivethingsastheygive
themselvesinlivedthroughexperience–notasexternallyrealoreternallyexistent,but
asanopennessthatinvitesustoseethemasifforthefirsttime(VanManen,2014).
Inordertoshiftfromanaturaltoaphenomenologicalattitude,Husserlproposestwo
mainmethods(Porter&Robinson,2011,p.54).Husserl’sfirstmethod,theepoché
reductionistheattempttodescribephenomenaasimmediatelyapparentinexperience.
Thisreductioninvolvesbracketingorsuspendingone’ssubjectiveorprivatefeelings,
preferences,inclinations,orexpectationsthatwouldpreventonefromcomingtoterms
withaphenomenonorexperienceasitislivedthrough(Porter&Robinson,2011,pp.
54-55).Inaddition,onealsoneedstostripawaythetheoriesorscientificconceptions
andthematizationsthatoverlaythephenomenononewishestostudy,andwhich
preventsonefromseeingthephenomenoninanon-abstractingmanner(VanManen,
1990,p.185).
Husserl’ssecondmethodiscalledtheeideticreduction(Porter&Robinson,2011).Inthe
eideticreductiononeneedstoseepastorthroughtheparticularityoflivedexperience
towardstheuniversalessenceoreidosthatliesontheothersideoftheconcretenessof
livedmeaning(VanManen,1990,p.185).Thebracketingprocedureisoftenreferredto
asthetranscendentalreduction.Itiswhatmakestheeideticreductionpossible.
However,theepochéreductionisnotmeanttoreducesomethingtoitsbasicormost
fundamentalprinciplesbuttoallowaccesstothephenomenonintheleastprejudicedor
corruptedway(Porter&Robinson,2011,pp.54-55).

15
6.2MartinHeidegger
Husserlhadhopedforacontinuationofhisphilosophythroughhisformerassistantand
successor,MartinHeidegger(Porter&Robinson,2011).However,Heideggermadea
decisivebreakwithHusserl’stranscendentalphenomenologythroughhisfirstmajor
work“BeingandTime”(Heidegger,1962).ThekeypointsinHeidegger’s
phenomenologywillnowbeoutlined,basedonPorterandRobinson‘s(2011)work.In
contrasttoHusserl,Heideggerisnotinterestedinthestructuresofconsciousness,
essencesorevenknowledgeperse,butinaninvestigationintothemeaningofbeing,
(“Dasein”).Heideggerclaimsthatphenomenologycannotmerelyinvestigatepure
consciousnessbutmusttakeintoaccountthetotalityofthehumansituation,duetothe
factthatweare,eachandeveryoneofus,already“being-intheworld”.
WithHeideggerphenomenologybecomesaradicallyinterpretiveenterprise.Heclaims
thathumanexistencehasahermeneuticalstructurewhichunderliesallour
interpretationsincludingthoseoftheonticornaturalsciences;thatis,bothscientific
andculturalknowledgemustbederivedfromthestructureofbeing(Porter&Robinson,
2011).Accordingly,thereisnoneutralorunbiasedstartingplacefromwhichonemay
begintounderstand.Wearethrownintoaworldinwhichlanguage,cultureand
institutionsoflifealreadyaregiven.Sonomatterwhereorwhenwefindourselves,we
willalwaysbeconditionedbyourownhistoricalsituatedness.Henceforth,Heidegger
arguesthatwecannotpossiblybrackettheworldinordertounderstandourselvesand
thatjudgmentaboutactuallyexistentthingscannotbesuspended.Heideggerstatesthat
themeaningofthingsisknowninthecontextofourrelationshipstothemwithinthe
world.Hearguesthatweunderstandlifefromoutoflifeitself.Understandingbegins
withoursituatednessasbeing-in-theworld.Throughhermeneuticswearemaking
understandingexplicitanddisclosingthenatureofbeing,-orDaseintoourselves.
However,Heideggerpointsoutthatunderstandingmayneverbeself-evidentasifit
werecorrespondingtofactsintheworld,forDaseinhasnosingleobjectorfacttofirst
comprehend.Insteadunderstandingisinherentlycircularorhermeneutical(Porter&
Robinson,2011).

16
Heidegger’shermeneuticalcircleisbestcharacterizedintermsofpreunderstandingand
temporality(Porter&Robinson,2011).Structuresofunderstandinginvolveafore-
structurethatconstantlyprojectsuponthatwhichisalreadyunderstoodandevident.It
isananticipatorystructureorpreliminaryawarenessofmeaning.Ashistoricalbeings,
wehaveanticipationsandexpectationsofthefutureanditspossibilitiesaswellas
conditionedunderstandingfrompreviousunderstanding.Hence,allexistenceis
interpretiveandallmeaningtakesplacewithinacontextofinterpretationmediatedby
cultureandlanguage.Whatremainsininterpretationistoworkout“thethings
themselves”insteadofallowingourpre-understandingtobeguidedbymistaken
assumptionsandillusions(Porter&Robinson,2011,p.68).Evensothisworkingoutis
notatechniqueormethodmeanttoachieveunderstanding.Rather,itismeantasa
descriptionofhowunderstandingemergesasweconstantlyrespondtoourfore-
projectionandprejudgments.Understandinghappenspriortoourreflectionbecausewe
arealreadyparticipating,andthereforeunderstanding,fromaspecificorientationand
awarenessaboutoursituationandcontext(Porter&Robinson,2011).
Accordingly,forHeidegger,Daseinisanevent,anoccurrencewhereinunderstandingis
“tobe”intheworldwhichisalwaystobeunderstoodinterpretively.Heidegger’s
existentialandphenomenologicalanalysisredefineswhatitmeanstounderstand
(Porter&Robinson,2011).WhatisneededHeideggerproposes,isanexistential
analysisthatinquiresintothemeaningof“tobe”thatispresenttous,yetremainstobe
drawnout.Thismeaningwillonlybedisclosedwhenwestopattemptingtograsp
essences,factsandabstractionsandbegintolivelifewithouttryingtomanipulateit.
Knowledgeinthescientificsensemayonlybesupplementaltoourdistinctwayof
existence.Heidegger’sanalysisrestsuponadistinctionbetweentheontologicalandthe
ontic.Theonticoronticalisthefactualworldunderstoodbythesciences,suchas
chemistryandbiology.WhileDaseinhasonticqualities,asananimalinthefactual
world,“Dasein”(he,shewe)isalsounique,forDaseinaloneisconcernedwiththe
questionofbeingandwhatitmeans,“tobe”.Noneoftheotheranimalsinhabitingthe
earthareconcernedwiththemeaningofbeing.ForHeideggerthequestionofbeing
representsourdecisiontoletthequestionbeaquestionforus.Itisaturnoradecision,
aneventofrecognizingawedgebetweenbeingandbeing–anontic-ontological
difference.Wearethebeingswhoaskthequestionsofwhoweare.Wealoneareableto
17
interrogatethenatureofwhatitmeanstobe.Heidegger’sontologicalphenomenology
canbecharacterizedasahermeneuticsoflifeorwhathecalls“hermeneuticsof
facticity”.Hermeneuticsinthissenseisaninterpretationoftheconditionsand
circumstancesthatdetermineorlimitone’spossibilitiesofbeing-in-the-world(Porter&
Robinson,2011).
6.3Hans-GeorgGadamerHans-GeorgGadamerisoneoftheforemostrepresentativesofhermeneutical
phenomenology(VanManen,2014).AsaformerstudentofHeidegger,Hans-Georg
Gadamershareshisnotionthatallunderstandingishermeneuticandthatthe
hermeneuticfunctionisactuallyourbasicmodeofbeing-in-theworld(Porter&
Robinson,2011).Thetaskofhermeneutics,accordingtoHans-GeorgGadamer,isto
clarifytheconditionsinwhichunderstandingandinterpretationtakeplace(Gadamer,
2004).
ThehistoricalstrandsofFriedrichSchleiermacher(1768-1834)andWilhelmDilthey’s
(1833-1911)pioneeringhermeneutics,thephenomenologicaldescriptionofEdmund
Husserl(1859–1938)andtheontologicalanalysisofMartinHeidegger(1889-1976)all
cometogetherinGadamer’sseminalwork“WahrheitundMethode:Gründzügeeiner
philosophischenHermeneutik”(1960)translatedtotheEnglishversionas“Truthand
Method”in1975(Porter&Robinson,2011).
InthismagnumopusGadamer(2004)explicatesinaphenomenologicalmanner,the
hermeneuticmethodasithadbeenoriginallydevelopedbyFriedrichSchleiermacher
andsubsequentlybyWilhelmDiltheyandHeideggerhimself(VanManen,2014).
Schleiermacherappliedhermeneuticstotheinterpretationoftexts,andemphasizedthe
importanceofconsideringthehistoricaltemporalityandrationalityofthetext.For
Schleiermacher,hermeneuticsdealswithreconstructingthepast(VanManen,2014).
WhileGadamer(2004)agreedaboutthenecessityofapproachingtextswithopenness
andsensitivitytotheirhistoricaltraditionsandinterpretivehorizons,healsoargued
thatitwasimpossibletoplaceoneselfintheoriginalreconstructedhistoricalcontext.

18
IncontrasttoSchleiermacher’ssearchfortheauthorialintentofatext,Gadamerargues
thatancienttextsmustbeinterpretedinthecontextofone’sownsocialhistorical
existence(vanManen2014).AccordingtoGadamer(2004)thereexists:
aninsuperabledifferencebetweentheinterpreterandtheauthorthatiscreatedbyhistoricaldistance…..Therealmeaningofatext,asitspeakstotheinterpreter,doesnotdependonthecontingenciesoftheauthorandhisoriginalaudience.Itcertainlyisnotidenticalwiththem,foritisalwaysco-determinedalsobythehistoricalsituationoftheinterpreter,andhencebythetotalityoftheobjectivecourseofhistory.(Gadamer,2004,p.296)
ForGadamer(2004),hermeneuticunderstandingisachievedthroughacircular
interpretationprocess,whereonemovesbackandforthbetweenthetextasawhole
anditsindividualparts.Assuch,construingthemeaningofthewholeinvolvesmaking
senseofthepartsandgraspingthemeaningofthepartsisdependentonhavingsome
senseofthewhole:“Thusthemovementofunderstandingisconstantlyfromthewhole
tothepartandbacktothewhole.Ourtaskistoexpandtheunityoftheunderstood
meaningcentrifugally”.(Gadamer,2004,p.291)
Gadameremphasizesthatthehermeneuticcircleisnota“methodologicalcircle”,rather
itdescribesanelementoftheontologicalstructureofunderstanding(Gadamer,2004,p.
294).ThebasicmodelofunderstandingthatGadamerfinallyarrivesatin1960in“Truth
andMethod”(Gadamer,2004),isconversationanddialogue(Malpas,2015).
ConversationalwaystakesplaceinlanguageandsimilarlyGadamerviews
understandingasalwayslinguisticallymediated.ForGadamer,understandingisa
matterofnegotiationbetweenoneselfandone’spartnerinahermeneuticaldialogue.
Henceforth,theprocessofunderstandingcanbeseenasamatterofcomingtoan
“agreement”aboutthematterathand.ForGadamer(2004),interpretationand
understandingalwaysoccurfromwithinaparticular“horizon”thatisdeterminedby
ourhistoricallydeterminedsituatedness.Accordingly,comingtoanagreement,means
establishingacommonframeworkor“horizon”.Gadamerthustakesunderstandingto
beaprocessthatinvolvesa“fusionofbothparty’shorizons”or“horizontverschmelzung”
(Malpas,2015).
19
Inasmuchasunderstandingistakentoinvolvea“fusionof“horizons”italsoinvolvesthe
formationofanewcontextofmeaningthatenablesintegrationofwhatisotherwise
unfamiliar,strangeoranomalous.Inthisrespectallunderstandinginvolvesaprocessof
mediationanddialoguebetweenwhatisfamiliarandwhatisalien,inwhichneither
remainsunaffected(Malpas,2015).Gadamer(2004)pointsoutthatinthedialogueof
understandingourprejudicescometothefore.Heclaimsthatourprejudicesplaya
crucialroleinopeningupwhatistobeunderstood,inasmuchastheythemselves
becomeevidentinthatprocess.Asourprejudicestherebybecomeapparenttous,they
canalsobecomethefocusofquestioningintheirownreturn:
Theessenceofthequestionistoopenuppossibilitiesandkeepthemopen….Infact,ourownprejudiceisproperlybroughtintoplaybybeingputatrisk.Onlybybeinggivenfullplayisitabletoexperiencetheother’sclaimtotruthandmakeitpossibleforhimtohavefullplayhimself.(Gadamer,2004,pp.298-299)
Notsurprisingly,oneofGadamer’s(2004)mostcontroversialmovesishisdefenseof
theimportanceofprejudiceininterpretation.ForGadamer,understandingrequires
presuppositionsandassumptionsthatenableunderstandingaswellas
misunderstanding(Porter&Robinson,2011).Gadamer(2004)maintainsthatwe
alwaysbringourfiniteandhistoricallyconditionedawarenesswithuswhenwe
encountersomething.Thismeansthatwemustallowourtraditionsandlongheld
assumptionstobechallengedandtested.Theremaybenonewexperienceand
understandingotherwise.Authenticexperienceshakesusawakeandopensoureyesto
thenewandunexpected,thatwhichliesbeyondourpersonalhorizon.Gadamer(2004)
pointsoutthatwithineveryunderstanding,truthispartiallyrelativetotheinterpreter’s
ownhorizonthoughneverentirelyconsumedbyit.Justlikeourlivingrelationshipto
thetruthofatext,ourwholeexperienceoflifereflectsthesameuniversalhermeneutical
dynamics.Gadamer’s(2004)descriptionofhermeneuticsintermsofwhatitmeansto
understandisnotonlyamatterofhowweknowclassicalandphilosophicaltexts,works
ofartandthelike.Rather,Gadamerianhermeneuticsisawayofdisclosingwhatit
meanstohaveanexperienceofunderstandinguniversally(Porter&Robinson,2011).
20
6.4PaulRicoeurPaulRicoeurmorethananyother,cementedtheconnectionandmutualaffinity
betweenhermeneuticsandphenomenology(Ricoeur,1981,2008;Tanetal.,2009).
Inhislandmarkessay“Phenomenologyandhermeneutics”,Ricoeur(1981)confrontsthe
questionofwhatremainsofEdwardHusserl’sphenomenologicalprograminthewake
ofHeideggerandGadamer’sdevastatingcritiqueofphenomenology.Inlinewiththe
hermeneuticsofHeideggerandGadamer,Ricoeurdiscussesourembeddednessinthe
worldoflanguageandsocialrelationshipsandtheinescapablehistoricityofall
understanding(Finlay,2012;Ricoeur,1981).Ricoeurconvincinglydemonstratesthat
whatsuccumbstothehermeneuticalcritiqueisnotphenomenologyassuch,butrather
phenomenologyinitsmostidealisticHusserlianform(Ricoeur,1981).
WhileHusserlarguedthatphenomenologyconsistsofdescribingwhatappearsin
consciousness,Ricoeur(1981,p.137)showsthataccordingtoHusserl’sownaccounts,
whateverappearsinconsciousnessisalreadytheworkoftheconstitutingego.Andin
thisconstitutionprocess,theinterpretiveisalreadyatwork(VanManen,2014).
Ricoeur(1981)pointsoutthatbeyondthesimpleoppositionbetweenphenomenology
andhermeneuticsthereexistsamutualbelongingbetweenthem.Ontheonehand,
hermeneuticsiserectedonthebasisofphenomenology,andthuspreservessomething
ofthephilosophyfromwhichitdiffers.Ontheotherhand,phenomenologycannot
constituteitselfwithoutahermeneuticalpresupposition:
…beyondthecritiqueofHusserlianidealism,phenomenologyremainstheunsurpassablepresuppositionofhermeneutics;andontheotherhand,thatphenomenologycannotcarryoutitsprogrammeofconstitutionwithoutconstitutingitselfintheinterpretationoftheexperienceoftheego.(Ricoeur,1981,p.114)
ThisbringsustothemaintenetsofRicoeur’s(1976)phenomenologicalhermeneutical
interpretationtheory,whichhaveinformedandguidedthisthesis.ForRicoeur(1976),
interpretationisthehingebetweenlanguageandlivedexperience(Geanellos,2000).In
hisfamousinterpretationtheory,Ricoeurattemptedtograftthehermeneuticalproblem
ofinterpretationtocontemporaryinsightsinphenomenology(Ricoeur,1999).
21
6.4.1Textunderstoodashumanaction
AlthoughRicoeur(1976)originallyformulatedhisinterpretationtheorywithrespectto
texts,healsopointsoutthathumanactioncanbeunderstoodasdiscourseand
interpretedastext,whenithasbeenobjectifiedandfixatedthroughwriting.
Accordingly,hisinterpretationtheorycanbeextendedintothesphereofthesocial
sciences(Ricoeur,1981).Inlightofthis,Ricoeur’s(1976)interpretationtheoryis
applicabletointerpretnurses’narrativesabouttheirexperienceswithspiritualand
existentialcare.Thiswillbeelaboratedoninthemethodssection.
6.4.2Distanciationandappropriation
Writingrendersthetextautonomouswithrespecttotheauthor’sintention.When
spokendiscourseiswrittendown,(i.e.liketheresearchinterviewsinthisstudy),the
fixateddiscourseanditsmeaningbecomesdistancedfromthespeechevent.Through
thisdistanciation,thetextbecomes“decontextualized”fromthespeecheventandits
socialandhistoricalconditions,thusopeningitselfuptoanunlimitedseriesofreadings
(Ricoeur,1976,1981,2008).Distanciationcreatesaneedtorecontextualizeand
appropriatethetext,-tofamiliarizeourselveswiththetextandmakeitourown
(Ricoeur,1976).Ricoeur(1976,p.43)pointsoutthat:
readingisthepharmakonthe“remedy”bywhichthemeaningofthetextis“rescued”fromtheestrangementofdistanciationandputinanewproximity,aproximitywhichsuppressesandpreservestheculturaldistanceandincludestheothernesswithintheowness.
Accordingly,thereexistsadialecticrelationshipbetweendistanciationand
appropriationintheinterpretationprocess:“Tomakeone’sownwhatwaspreviously
foreignremainstheultimateaimofallhermeneutics…Thisgoalisachievedinsofaras
interpretationactualizesthemeaningofthetextforthepresentreader”.(Ricoeur,1976,
pp.91-92)

22
Methodologicallydistanciationandappropriationallowresearcherstomovebeyondthe
notionthatonlytheresearchparticipants’understandingismeaningfulandorcorrect.It
alsoallowstheinterpreterstointerpretthesametextfaithfully,yetsomewhat
differentlybecauseitisacknowledgedthattextshavemanymeanings(Geanellos,2000).
6.4.3Explanationandunderstanding
Interpretingatextinvolvesmovingbeyondunderstandingwhatthetextsays(itssense)
tounderstandingwhatittalksabout(itsreference)(Ricoeur,1976,p.88).Assuch,the
text’ssenseanditsreferenceembodiesthetwostagesofRicoeur’sinterpretation
theory:(i)explanation,-orwhatthetextsaysand(ii)understanding,orwhatthetext
talksabout(Geanellos,2000).Whileexplanationisdirectedtowardanalysisofthe
internalrelationsofthetext(theparts)understandingisdirectedtowardgraspingthe
meaningsthetextdiscloses(thewholeinrelationtotheparts)Inthisway,interpretive
understandinggoesforwardinacontinualmovementbetweenthepartsandthewhole
allowingunderstandingtobeenlargedanddeepened(Geanellos,2000).“Ultimatelythe
correlationbetweenexplanationandunderstanding,betweenunderstandingand
explanationis‘thehermeneuticcircle’.”(Ricoeur,2008,p.163)Hence,thesenseofatext
isnotbehindthetext,butinfrontofit.Itisnotsomethinghidden,butsomething
disclosed:
Whathastobeunderstoodisnottheinitialsituationofdiscourse,butwhatpointstoapossibleworld.Thetextspeaksofapossibleworldandofapossiblewayoforientatingoneselfwithinit.Thedimensionsofthisworldareproperlyopenedupanddisclosedbythetext.(Ricoeur,1976,pp.87-88)
6.4.4Guessingandvalidation
Allinterpretiveactivityinvolvesadialecticbetweenguessingandvalidating(Ricoeur,
2008).Wemakeaneducatedguessaboutthemeaningofapartandcheckitagainstthe
wholeandviceversa.Inthesameway,webeginbyguessingaboutthemeaningofthe
wholeasdeterminingtherelativeimportanceofseveralparts.Throughoutthisprocess
ofguessandvalidationwecancometoanendwhenwesaythisishowweunderstand
things.Butthereisnodefiniteoutcome(Dauenhauer&Pellauer,2014,p.154).
23
Itisalwayspossibletorelatesentences,oractionstooneanotherinmorethanone
way:“Thisplurivocityistypicalofthetextconsideredasawhole,opentoseveral
readingsandtoseveralconstructions”(Ricoeur,2008,p.154).Althoughatextmayhave
severalinterpretations,someinterpretationsaremoreprobablethanothers.Itis
thereforenecessarytovalidateourguesses.Validatingguessesisclosertoalogicof
probability,thantoalogicofempiricalverification.Wevalidateaninterpretationby
vindicatingitagainstcompetinginterpretations.Thus,validationisnotverification
(Ricoeur,2008).Rather,itisan“argumentativedisciplinecomparabletothejudicial
proceduresoflegalinterpretation.Itisalogicofuncertaintyandofqualitative
probability.”(Ricoeur,2008,p.155)Guessandvalidationarecircularlyrelatedas
subjectiveandobjectiveapproachestothetext.Althoughthereisalwaysmorethanone
interpretation,allinterpretationsarenotequal.Onemustthereforetrytofindthemost
probableinterpretation.Ricoeurpointsoutthat:
Thetextisalimitedfieldofpossibleconstructions.Thelogicofvalidationallowsustomovebetweenthetwolimitsofdogmatismandskepticism.Itisalwayspossibletoargueagainstaninterpretation,toconfrontinterpretations,toarbitratebetweenthemandtoseekforanagreement,evenifthisagreementremainsbeyondourreach.(Ricoeur,2008,p.155)
Asmentionedinthebeginningofthischapter,theresearcher’schoiceofmethodsto
carryoutastudymustbeconsistentwiththestudy’smethodologicalframework
(Swinton&Mowat,2006).Thelinkbetweenthisstudy’sphilosophicalunderpinnings
andthemethodsusedinthestudy(VanManen,2014)willthereforebeexplicatedinthe
followingchapter.
24
7.ThemethodsDatawerecollectedthroughnarrativeinterviews(Mishler,1986)anda
phenomenologicalhermeneuticalinterpretationmethod(Lindseth&Norberg,2004)
waschosentoanalyzethedata.
7.1Datacollection:NarrativeinterviewsOpen-endednarrativeinterviews(Mishler,1986)wereusedtocollectthedatainall
threestudies.ThenarrativeinterviewsinpaperIandIIwereconductedasindividual
interviews,whilethenarrativeinterviewinpaperIIIwasconductedasafocusgroup
meetingwiththemobilehospicenurseteachingteam.
Ricoeur’s(2008)theoryofnarrativesstatesthatlifehasaprenarrativequalityandthat
actioncanbelookeduponasapotentialnarrative(Vandervelde,2008).Ricoeurnotes
that:
Lifeislived;historyisrecounted….Inremainingboundtotimeandtochange,historyremainstiedtoaction.….Ultimatelyhistorycannotmakeacompletebreakwithnarrativebecauseitcannotbreakwithaction,whichitselfimpliesagents,aimsandcircumstances,interactionsandresultsbothintendedandunintended.(Ricoeur,2008,p.5)
Ricoeurmaintainsthatactionandlifearestructuredororganizedintheirbeingby
narrative-likefeatures,sothattellingthestoryisnotanafter-thefactreorganizationof
whattookplace,butthemakingexplicitofwhatwasalreadyimplicitinactionandin
life.Accordingly,understandingtakestheformofnarrativesandispermeatedbya
culturalworldthatisitselfmadeofnarratives.Aninchoatenarrativestructureliesatthe
heartofpeople,thingsandevents.Narrativesarethusnotmeredescriptionsof
somethingthatwouldbeotherwiseavailableindependentlyofdescription,butare
ontologicallayers,partandparcelofthepastofactionsandexperiences(Ricoeur,2008;
Vandervelde,2008,p.141).
DrawingonRicoeur’sargumentabouttheinterconnectionbetweennarrativeand
humanexperience(Ivic,2009)itseemedreasonabletobelievethatthenarrative
25
interview(Mishler,1986)wouldbeasuitablemethodtogainaccesstotheparticipants’
experienceswithpracticingandteachingspiritualandexistentialcareforthedying.
Thiswasbasedonthepresuppositionthattheinterviewees’perspectiveswouldbebest
revealedinnarrativeswheretheyusetheirspontaneouslanguagetotalkabouttheir
experiences(Mishler,1986;VanManen,1990).AccordingtoMishler(1986,p.68)
“thereisawiderecognitionofthespecialimportanceofnarrativeasamodethrough
whichindividualsexpresstheirunderstandingofeventsandexperiences”.Mishler
(1986)pointsoutthat:“wearemorelikelytofindstoriesreportedinstudies“using
relativelyunstructuredinterviewswhererespondentsareinvitedtospeakintheirown
voices,allowedtocontroltheintroductionandflowoftopics,andencouragedtoextend
theirresponses”.(Mishler,1986,p.69)Thenarrativeinterviewswereconducted,using
oneopen-endedquestion.Clarifyingfollow-upquestionswereusedwhennecessary.
AsdiscussedinChapter4.2,spiritualcareisahighlydebatedconceptduetothemany
variationswhichemergefromthenursingliterature.Theauthorschosenottopresent
anyofthesevariationsduringtheinterviews.Theyalsoavoideddefiningpalliativeand
terminalcare,sincethesetermsareincommonandsometimeinterchangeableuse
(Clark&Seymour,1999)andthemomentwhenapatienttransitionsfrom“palliative”to
“terminal”careisdebatedintheliterature(Clark&Seymour,1999;Harlos,2010).
Accordingly,theauthorschoseanopenapproachtoensurethatthenursesfeltthey
couldnarratefreelyabouttheirexperienceswithspiritualandexistentialcareforthe
dying.Theauthorspresumedthatthiswouldgivethemthebestchancetocollectas
manyrichnarrativesaspossible.
ThehospicenursesinpaperI,andthenursesinpaperIIwereaskedthequestion:“What
areyourexperienceswithprovidingspiritualandexistentialcaretodyingpatients?”
InpaperIIIthemobilespiritualandexistentialcareteachingteamwasaskedthe
question:“Whatareyourexperienceswithteachingandsupervisingcareworkersin
existentialandspiritualcareforthedying?”

26
7.1.1Thenarrativefocusgroupinterview
Thenarrativeinterviewinthelastpartofthestudy(paperIII)wasconductedasafocus
groupmeetingbecausetheauthorswantedtocollectnarrativesaboutthegroup’s
experienceasauniquepioneermobilespiritualandexistentialcareteachingteam.
BelzileandÖberg(2012)pointoutthatfocusgroupsareusefultostudytheperceptions,
feelings,meaningsorwaysofthinkingthatareheldbyagroupwhoshareinaparticular
intersubjectivereality.Thefocusgroupisanefficientwaytoobtaindatafrom
participantswhoworktogetherdaily:“…colleaguescanrelatetoeachother’scomments
toincidentsintheirdailysharedlives.Theymayevenchallengeeachotheron
contradictionsbetweenwhattheyprofesstobelieveandhowtheyactuallybehave”.
(Kitzinger,1995,p.300)
7.2Dataanalysis:Interpretingtheinterviewtexts
DrawingontheworksofHeidegger,GadamerandRicoeur,LindsethandNorberg(2004)
underlinethatessentialmeaningissomethingthathumansarefamiliarwithinthe
practicesoflifeandthatthisfamiliarityisexpressedthroughactions,narrativesand
reflections.However,inordertostudytheessentialmeaningofresearchparticipants
livedexperience,theirnarrativesmustbewrittendownandinterpreted.Itisimportant
tonotethatwhenLindsethandNorberg(2004)usethetermessentialmeaning,their
methoddoesnotinvolvea“pure”Husserlian”phenomenologicalsearchformeaning
thatisuncontaminatedbyinterpretation.Nordoesitinvolvea“pure”hermeneutical
textinterpretation,sincetheaimoftheinterpretationistotranscendthemeaningofthe
textinordertorevealessentialtraitsofourlifeworld:“Thusweseethat
phenomenologymustbephenomenologicalhermeneutics.Essentialmeaningmustbe
studiedandrevealedintheinterpretationoftext”(Lindseth&Norberg,2004,p.147).
InLindsethandNorberg’s(2004)interpretationmethod,eachinterviewislookedupon
asatext.Theinterpretationmethodimpliesadialecticmovementbetweenthetextasa
wholeandpartsofthetext.Themethodconsistsofthreepracticalstepsinvolving:
1.Naïvereading,2.Structuralanalysis,3.Comprehensiveunderstanding.

27
7.2.1Thenaïvereading
Theaimofthenaivereadingistograspanoverallimpressionofthetextandtogain
accesstotheparticipants’livedexperience.Duringthenaïvereading,theresearcher
muststrivetoavoidmakingjudgmentsaboutthefactualinthenarratives.Rather,the
researchermustkeepanopenmind,allowingherselftobetouchedandmovedbythe
narratives.Todothis,theresearchermustshiftfroma“natural”toa“phenomenological
attitude”orinotherwords,accomplish“epoché”or“bracketing”(Lindseth&Norberg,
2004,p.147).ItisimportanttonotethatwhenLindsethandNorberg(2004)usethe
Husserlianconceptsof“essentialmeaning”,“epoché”and“bracketing”theydonotmean
thatresearchersshouldgiveuptheirpreunderstandingsinordertoarriveatapureun-
interpretedanduncontaminatedessentialmeaning.Thisisneitherpossiblenor
desirable.Researchersshouldinsteadstrivetobrackettheireagernesstoclassifythe
participants’storiesintocategories,explanationsandmodelsinordertoletthe
participantsleaveanimpressiononthem(Lindseth&Norberg,2004).Byencountering
theparticipantswithopennessandreceptivity,aspaceofattentionopensup.Whenthe
participant’s“expressioncanmakeanimpression,somethingfundamentalhappens...A
spaceofattentionopensup,inwhichwhathasbeensaidcanshowitselfwithgreater
clarity”(Lindseth,2015,p.51).
Strivingtokeepanopenmind,theauthorsrereadtheinterviewtextsseveraltimes.The
processofrereadingdrovetheanalysistowardsaphenomenologicalworld,which
allowedtheauthorstobetouchedbythenarratives.Thenaïveunderstandingofthetext
revealedthedirectionforthestructuralanalyses(Lindseth&Norberg,2004;Ricoeur,
1976,1981,1984).Theresultsfromthenaïvereadingswerediscussedbetweenthe
authors.Thenaïvereadingguidedthestructuralanalysis,whichwasthesecondstepin
theinterpretationprocess.
7.2.2Thestructuralanalysis
Thestructuralanalysisincludesvariousexaminationsofthepartsofthetextinorderto
understandandexplainwhatitsaysandhowitissaid.Thestructuralanalysiscanbe
viewedasastagebetweenanaïveandacomprehensiveinterpretation,orbetweena
28
surfaceandadeepinterpretation.Theobjectiveofthestructuralanalysiswastoexplain
whatthetextwassaying(Lindseth&Norberg,2004;Torjuul,2009).Theauthorsreread
thetranscriptsseveraltimestolookformeaningfulpartsandpatternsthatcouldbe
dividedintonarrativemeaningunits.Ameaningunitcouldconsistofonesentence,
partsofasentenceorawholeparagraphwithrelatedmeaning.Themeaningunitswere
thencondensed,comparedandreflectedupontoidentifythespiritualandexistential
carethemesandsubthemesthatpenetratedthewholeorpartsofthetext.Athememay
beregardedasathreadofmeaningthatpermeatesthetextsasawholeorpartsofit
(Lindseth&Norberg,2004;Torjuul,2009).Themeaningunits,themesandsubthemes
werediscussedandreflecteduponbytheauthors.Theprocessofreading,identifying
anddiscussingthethemesandsubthemeswererepeateduntiltheauthorsreachedan
interpretativeagreement,weretheyfeltthatthethemescorrespondedtotheirtext
interpretations.LindsethandNorberg(2004),theobjectiveofthestructuralanalysisis
toexplainwhatthetextissaying.Hence,thestructuralanalysiscanbeviewedasthe
methodicor“objective”partoftheinterpretationprocess,sincethemeaningunitsare
decontextualizedfromtheindividualaccountsandthetextasawhole(inotherwords:
thepartsandmeaningunitsareconsideredindependentlyfromtheircontextinthe
interviewtexts(Lindseth&Norberg,2004)).Torecontextualizethetext,themeaning
unitsweregroupedtogethertocreatetentativethemesaccordingtotheauthors’naïve
reading.Theauthorsvalidatedthestructuralanalysis,bycheckingtheirinterpretations,
rereadingthetextandcomparingthethemesandmeaningunitswiththeirnaïve
understandingofthetextasawhole.
7.2.3Comprehensiveunderstanding(Interpretedwhole)
Inthethirdandlaststepoftheinterpretationprocess,acomprehensiveunderstanding
wasdeveloped.Thecomprehensiveinterpretationisdevelopedthroughamergingof
theresearchers’pre-understanding,naïvereading,thestructuralanalysis,previous
researchandrelevanttheory(Lindseth&Norberg,2004;Sørlie,2001;Ødbehretal.,
2014).Todevelopacomprehensiveunderstanding,theresearchersmustreflectonthe
themesinrelationtotheresearchquestionandthecontextofthestudy(Lindseth&
Norberg,2004).Theaimofthisstepistogainadeeperunderstandingoftheinterviews
asawhole,-inRicoeur’stermstorecontextualizethetext(Ricoeur,1976).Methodically,
29
interpretationallowsactualizationsofthemeaningsofthetext.ForRicoeur(1976)this
occursthrough“appropriatingthetext”;i.e.tomakeone’sownwhatwaspreviously
foreigninthetext(Ricoeur,1976,pp.91-92).Whentheworldofthetextis
appropriated,thehorizonoftheresearcherisexpanded.Thisopensupthepossibilityof
seeingthingsdifferentlyandorientingoneselfdifferentlyintheworld.Itisthislink
betweenunderstanding,experienceandself-understandingthatgroundsRicoeur’s
theoryinexistence(Geanellos,2000;Ricoeur,1976;Torjuul,2009).Whilethe
structuralanalysisischaracterizedasthemethodicorobjectivepoleofthis
interpretationmethod,LindsethandNorberg(2004)statethatthedevelopmentofa
comprehensiveunderstandingcanbelookeduponasthemethod’snonmethodicpoleof
understandingandtheypointoutthatimaginationisimportantbecauseitisnotpossible
tofollowstrictmethodologicalrulesintheprocessofrecontextualizingthetext.
Accordingly,LindsethandNorbergemphasizethattheirphenomenological
hermeneuticalinterpretationmethodliesbetweenartandscience:“Weuseourartistic
talentstoformulatethenaïveunderstanding,ourscientifictalentstoperformthe
structuralanalysisandourcriticaltalentstoarriveatacomprehensiveunderstanding”
(Lindseth&Norberg,2004,p.152).
Todevelopacomprehensiveunderstanding,thethemesfromthestructuralanalysisin
paperI,II,IIIandthemainresultsinthethesisarediscussedinlightofrelevant
theoreticalperspectivessuchasNorberg,BergstenandLundman’s(2001)modelof
consolation.Thecomprehensiveunderstandingineachindividualstudyispresentedin
thediscussionsectionineachpaper,whilethecomprehensiveunderstandingofthe
mainresultsfromtheentirestudyispresentedinchapter10inthisthesis.
7.3Methodologicalconsiderations
Whatconstitutesqualityinqualitativeresearchandthemeanstodetermineorenhance
ithasbeenasubjectofdebateandcontroversyinrecentyears(Cho&Trent,2006;
Golafshani,2003;Morse,Barrett,Mayan,Olson,&Spiers,2008;Onwuegbuzie&Leech,
2007;Torjuul,2009).Themattersofdisputehaveprimarilyevolvedaroundissues
concerningreliabilityandvalidity.However,tothisdatenoneofthedefinitionsofthese
30
conceptsrepresentahegemonyinqualitativeresearch(Cho&Trent,2006;Golafshani,
2003;Morseetal.,2008;Onwuegbuzie&Leech,2007;Torjuul,2009).Thearrayof
criteriaandterminologyusedmakethisdiscourseproblematicandrathercomplicated.
Moreover,thereexistsnosinglesetofphilosophicalandmethodological
presuppositionsthatcanunderpinaqualitativeparadigm.Inaddition,thereexistsno
uncontestedcollectionofmethodsandstandardsforreportingandevaluating
qualitativeresearchintheliterature(Cho&Trent,2006;Golafshani,2003;Kvale&
Brinkmann,2008;Morseetal.,2008;Onwuegbuzie&Leech,2007;Torjuul,2009).
Nevertheless,qualitativeresearchersagreethatastudy’scredibilityortrustworthiness
hastobewarrantedbyconformingtosomegenerallyacceptedscientificstandards.
Suchstandardsincludemethodologicalcongruence,auditability,orrigourin
documentingandexplainingtheresearchprocess,ethicalrigourandthecredibilityor
fittingnessofthedatainterpretation(Cho&Trent,2006;Golafshani,2003;Morseetal.,
2008;Onwuegbuzie&Leech,2007;Torjuul,2009).
DrawingonLincolnandGuba(1985),Seale(1999)statesthatestablishing
trustworthinessofaresearchreportliesattheheartofissuesconventionallydiscussed
asvalidityandreliability.AccordingtoKvaleandBrinkman(2008)reliabilitypertains
totheconsistencyandtrustworthinessofresearchfindings,whilevaliditypertainsto
thedegreethatamethodinvestigateswhatitisintendedtoinvestigate.Validation
consistsofaconsistentqualitycontrolthroughouteverystageofknowledgeproduction,
ratherthananinspectionattheendoftheproductionline(Kvale&Brinkmann,2008).
FollowingKvaleandBrinkman(2008),anattempttoestablishmethodological
congruencehasalreadybeenconductedinthedescriptionofthestudy’smethodological
frameworkandmethods.Inordertostrengthenthecredibilityofthestudy,therestof
thischapterwilldiscussmethodologicaltrustworthinessrelatedtodatacollection,data
analysis,studylimitationsandthefirstauthor’spreunderstanding.
7.3.1Thetrustworthinessofthedatacollection
Thenarrativeinterviewmethodwasusedtocollectasmanyrichnarrativesaspossible
inordertoachievethestudy’soverallaim,ofilluminatingthenurses’livedexperience.

31
Theauthors’ambitionwastocaptureasmanyfeaturesanddimensionsofthenurses’
experiencesaspossibleinordertoensureauthenticityandtoavoidsuperficialdata
(Lindseth&Norberg,2004;Torjuul,2009).However,asAppleton(1995)andMishler
(1986)emphasize,thequalityofthedatageneratedthroughnarrativeinterviewsis
largelydependentontheskillsandexpertiseoftheinterviewer.
Inordertopromotetrustworthiness,theauthorsstrovetocreateapermissiveandnon-
judgingclimate,encouragingthenursestousetheirownwordsandtonarrateasopenly
andhonestlyaspossibleabouttheirexperiencesduringtheinterviews(Appleton,1995;
Mishler,1986).Nodefinitionsofspiritualandexistentialcarewereintroduced,inorder
toallowthenursestotalkfreelyaboutwhattheyconsideredasspiritualandexistential
care.Carewastakentoavoidinterruptingthenurses’narrativeflowandreflectionin
ordertogivethemenoughtimeandspacetofollowtheirownthoughtsandworkout
theirownstories.Thisrequiredtheabilitytobepatientandenduremomentsofsilence.
Theauthorsfolloweduponthethemesthatthenursesfocusedonduringtheinterview
inordertoobtainthemeaningoftheirnarratives(Gadamer,2004).Thiswasdoneby
tyingquestionsandcommentstothenarrativesandrepeatingthenurses’words
wheneverpossible(Riessman,1993).Occasionallytheauthorswoulduseprobing
questions,suchas“Whathappenedthen?”or“Couldyoupleasetellmemoreabout…?”
toencouragethenurses’narrativeflow.However,itwasnecessarytobesensitiveto
theirresponsesandreactionsinordertoavoidprobingtoomuch(attheriskofinvading
thenurses)andprobingtoolittle(attheriskofmissingoutonimportantstories).In
ordertoincreasetrustworthiness,theauthorsalsostrovetoclarifyunclearquestions
andunclearanswersinordertoreducepotentialmisunderstandingswiththenurses.
Inspiteoftheseprecautions,onecanneveravoidthatsomeresearchparticipantsmight
notbewillingto,ordaretotellstories,whileothersmaynotremember,orfindit
difficulttoexpresstheirthoughtsandfeelings.Thischallengestheresearchertopay
attentiontocuesthatcouldsuggestthatthenursesmighthavemoretosay(Lindseth&
Norberg,2004;Torjuul,2009).
Theactoftellingastorymusttakeplaceaftertheactualeventtookplace:“Lifeislived
historyisrecounted”(Ricoeur,2008,p.5).Assuch,participants’narrativesarestories
32
aboutpastexperiences.Hence,narrativesarenotstoriesconcerningfactualtruths;
rather,theyareasynthesisbetweenaperson’sexperiencedeventsandincidents.
Accordingly,arecountedstoryisalwaysmorethantheactualsumofthesingleevents
(Benzein,1999;Polkinghorne,1988;Ricoeur,2008;Sørlie,2001).Oneoftheproblems
withretrospectiveinterviewsisthatparticipantsmayreconstructthepastwitha
frameworkthattheyhavelearnedlater.Ontheotherhand,narrativeinterviewsgive
participantstheopportunitytospeakaboutwhatisimportantforthemfromtheir
memory(Sørlie,2001).Assuch,thenarrativeinterviewmethodisanimportantwayto
obtaininformationaboutparticipants’experiences.
Nevertheless,theresearchinterviewisalsoasituationwhereparticipantsenacttheir
identitiesthroughtalking,wantingtopresentthemselvesasexperienced,moraland
knowledgeable.Theymaythereforebetemptedtowithholdexperiencesthatmight
proveotherwise(Gullestad,1996;Jordens&Little,2004;Ricoeur,1992;Torjuul,2009).
However,thestudyresultsdidnotgivethisimpression.Inseveraltouchingnarratives,
thenursestoldabouttheiruncertainty;ambiguityandvulnerabilityrelatedto
alleviatingdyingpatients’spiritualandexistentialsuffering.Astheauthorsdidnot
knowthenursespersonally,thismayhavehelpedthemtoexpressthemselvesfreely.
7.3.2Thetrustworthinessofthedataanalysis
Thetrustworthinessofthedataanalysiscanbejudgediftheresearcherisopenabout
howthestepsintheanalysiswerecarriedout(Benzein,1999).Inallthreepapers,care
wastakentodescribethestepsinthephenomenologicalhermeneuticalanalysisto
allowthereadertofollowtheprocessfromthenaïvereading(step1)throughthe
structuralanalysis(step2)towardsthecomprehensiveunderstanding(step3)
(Lindseth&Norberg,2004).
Sincetheaimofthephenomenologicalhermeneuticalanalysisistoobtainthemeaning
thatisopenedupinfrontoftheinterviewtext,-nottosearchfortheparticipants’
meaningsorauthorialintent(Lindseth&Norberg,2004;Ricoeur,1976),the
researchers’interpretationscannotbereturnedtotheparticipantsforvalidationin
ordertoincreasethetrustworthinessoftheinterpretation(Riessman,1993;
33
Sandelowski,1993).Instead,validationisaccomplishedthroughthestructuralanalysis,
wheretheresultsfromthestructuralanalysisarecomparedwiththeinitial
interpretationsstemmingfromthenaïvereadingsinstep1.Thestructuralanalysisis
theobjectivepartoftheinterpretation(Lindseth&Norberg,2004;Ricoeur,1976,pp.
82-88).
Itisimportanttonotethataninterpretiveconstructionreliesoncluescontainedwithin
thetextthatpointtotheirmeaning.Thesecluespermitaninterpretationbecausethe
clueseithermakesenseorinhibitaninterpretationbecausetheydonotfit(Ricoeur,
1976).Ricoeur(1976,2008)emphasizesthatatexthasmultipleinterpretations,and
thatallinterpretationsarenotequal.Becausetherearemultiplepossiblemeanings
withinatext,theinterpretersmustmakechoicesaboutcompetinginterpretationsand
thedifferentpossibilitiesofnamingandframingthem(Torjuul,2009).Following
Ricoeur,researchersneedtoappreciatethatnosingleinterpretationcaneverexhaust
themeaningofatext.Everyinterpretationisthereforeanapproximation.Accordingly,it
istheresearchers’tasktoarguefortheirinterpretation(Benzein,1999;Geanellos,
2000).
Inordertoarriveatthemostplausibleofcompetinginterpretations,alloftheauthors
readtheinterviews,followedthepathsintheanalysisanddiscussedpossible
interpretationsuntilaconsensuswasreached.Thiskindofresearchercooperationis
calledanalysttriangulation(Benzein,1999;Patton,1990).Analysttriangulationis
aimedatreducingthepotentialbias,whichmayoccurwhenasingleresearchercollects
andinterpretsthedata.Analysttriangulationprovidesameansofmoredirectly
assessingthereliabilityandvalidityoftheresults(Benzein,1999).Theauthors’
cooperationandcriticaldiscussionsgavethemawiderframeofreference(horizon)to
interpretthetexts,sinceitenabledthemtoquestioneachother’sinterpretations.
LindsethandNorberg(2004)emphasizethattheresearchermustcheckwhetherthe
resultsfromthestructuralanalysisvalidateorinvalidatetheinitialnaïveunderstanding.
Ifthestructuralanalysisinvalidatesthenaïveunderstanding,thewholetextmustbe
rereadtodevelopanewnaïveunderstanding.Thenewnaïvereadingmustthenbe
checkedbyanewstructuralanalysis.Theresearchermustrepeattheprocessuntils/he
34
experiencesthatthenaïveunderstandingisvalidatedbythestructuralanalysis
(Lindseth&Norberg,2004).Theauthorscheckedthethemesfromthestructural
analysisinrelationtotheirnaïvereadings,whichwerefoundtobeconsistentwiththeir
initialnaïveunderstanding.Thisstrengthenedthetrustworthinessoftheir
interpretations.ThethemesarepresentedintheResultssectioninthethreepapers.
Somenurseresearchersclaimthatusingaphenomenologicalhermeneuticalmethodto
analyzefocusgroupinterviewsisacontroversialchoice.Criticsstatethat
phenomenology’semphasisonindividual,livedexperienceisinconsistentwithgroup
approaches(Webb,2003;Webb&Kevern,2001).Thiscontroversyhasbeenthoroughly
discussedinpaperIwheretheauthorsarguethatthefocusgroupapproachdoesnot
excludeindividualperspectivesandthatsubjectingfocusgroupinterviewsto
phenomenologicalhermeneuticalanalysisisconsistentwithRicoeur’s(1976)
interpretationtheorybecausetheaimofthephenomenologicalhermeneuticalanalysis
istointerpretthemeaningoftheinterviewtext,ratherthantheexperienceofindividual
participants(Lindseth&Norberg,2004;Ricoeur,1976).Thefirstauthor,whoconducted
theinterview,madesurethatalloftheteammemberswereheardandencouragedthe
lessvociferoustotalkabouttheirexperiencesinordertocapturethewholegroup’s
experienceasateachingteam.
7.3.3Rationaleforconductingaphenomenologicalhermeneuticaldataanalysis
Differentepistemologicalperspectivesandpluralismhavecreatedanarrayof
qualitativeapproaches,suchasgroundedtheory,variousformsforphenomenology,
ethnography,actionresearchandqualitativecontentanalysis.Thereisaconsiderable
overlapamongavailableapproachesintermsofmethods,proceduresandtechniques.It
canthereforebechallengingforresearcherstodeterminewhichapproachismost
suitabletoanswertheirresearchquestions(Vaismoradi,Turunen,&Bondas,2013).
Inthisstudywechosetoapplyaphenomenologicalhermeneuticalmethod(Lindseth&
Norberg,2004)toanalyzetheinterviewtexts.Itcouldalsohavebeenpossibletouse
qualitativecontentanalysis(Graneheim&Lundman,2004).Initially,thismethod
focusedonanalyzingthemanifestcontent,-whattheinterviewtextsays,itsvisible,
obviouscomponents(Graneheim&Lundman,2004,p.106).-orinRicoeur’sterms“its
35
sense”(Ricoeur,1976,pp.19-23).However,overtime,qualitativecontentanalysishas
expandedtoincludeinterpretationsofwhatthetexttalksabout,-itslatentcontent
(Graneheim&Lundman,2004,p.106),-orinRicoeur’sterms“thetext’sreference”
(Ricoeur,1976,pp.19-23).Assuch,phenomenologicalhermeneuticalanalysis(Lindseth
&Norberg,2004)andqualitativecontentanalysis(Graneheim&Lundman,2004)seem
toshareacommonaimofanalyzingnarrativematerialsbybreakingthemintorelatively
smallunitsofcontentandsubmittingthemtodescriptiveandinterpretativetreatment.
However,accordingtoSandelowskiandBarroso’s(2003)typologyofqualitative
studies,qualitativecontentanalysisemploysalowerlevelofinterpretationthan
phenomenologicalhermeneuticalapproaches.Theauthorsthereforejudgedthatit
wouldbemoresuitabletoapplyaphenomenologicalhermeneuticalmethodtoanalyze
theinterviewtextsbecausethestudy’soverallaimto“illuminatethemeaningof
registerednurses’experienceswithpracticingandteachingspiritualandexistentialcare
forthedying”demandedamethodwhichemploysahighlevelofinterpretive
complexity.AsvanManen(2014,p.226)notes:”Thephenomenologicalstudyoflivedor
existentialmeaningsattemptstodescribeandinterpretthesemeaningstoacertain
degreeofdepthandrichness.”
UsingLindsethandNorberg’s(2004)phenomenologicalhermeneuticalmethodto
interpretthenarrativeinterviewsprovedtobeagoodchoiceforthisstudy,becauseit
enabledtheauthorstointerpretthenurses’livedexperience.Theinterpretations
providedafruitfuldeparturepointtodevelopacomprehensiveunderstandingaboutthe
meaningofthenurses’experienceswithpracticingandteachingspiritualandexistential
careforthedying.
However,asmentionedearlier,phenomenologicalhermeneuticalresearchersmust
“bracket”theirjudgmentsaboutthefactualinnarrativeinterviewtextsinorderto
disclosethetexts’essentialmeaning.Itisimportanttonotethatbracketingone’s
judgmentisnotthesameasbracketingone’spreunderstanding(Lindseth&Norberg,
2004).DrawingonRicoeur(1976),LindsethandNorberg(2004)pointoutthatevery
humanbeinghasanimplicitpreunderstandingoflifewhichtheycannotfreethemselves
fromandthatresearcherscanonlyunderstandandinterprettheirinformants’
narrativesinrelationtotheirownpreunderstandings.Accordingly,tostrengthena
36
phenomenologicalhermeneuticalstudy’strustworthiness,researchersmustreflect
criticallyanddocumenthowtheirpreunderstandingshaveinfluencedtheresearch
processandthedatainterpretation.Thiswillbepresentedinthefollowing:
7.3.4Mypreunderstanding
AsmentionedinChapter4.2,whenIbeganmyresearch,Ihadapreunderstandingof
spiritualandexistentialcare,whichhadevolvedthroughmyownnursingexperiencein
palliativecareandmytheoreticalframeofreferenceinnursingandnarrativetheology.
Inretrospect,Iseethatthisbackgroundhashaditsadvantagesaswellasdisadvantages.
Ontheonehand,beinganursewithpalliativespiritualandexistentialcareexperience
gavemeanassetasaresearcher,becauseitenabledmetoestablishtrustandrapport
withthenurses.Comingfromthesamebackground,helpedmetocommunicatewith
them.Iexperiencedthatthenursesopenedupandtalkedquitefranklywithmeabout
theirchallengesandstrugglesbecauseIwas“oneofthem”.(Iinformedthembriefly
aboutmybackgroundwhenIpresentedmyselfatthebeginningofeachinterview.)
However,beingviewedas“oneofthem”,alsohaditschallenges.Whenthenursestold
memovingstories,Ioftenfeltthattheyappealedtomeforrecognition,whentheyheld
mygazeandsaidthingslike:“…-youknowwhatImean…!!?”Thiswasespecially
challengingduringmyfirstinterviews,becauseIwasnewtotheroleastheresearcher.I
quicklydiscoveredthatIwastemptedtorespondspontaneouslytotheirappealsasa
fellownurse,andIexperiencedthatIhadtomakeaconsciousefforttoinhibitmy
reactionsinordertomaintainmyroleasaresearcher.Resistingthetemptationto
confirmthatI“absolutelyunderstoodthem”asafellownurse,Imadeanefforttosettle
backandencouragethenursestotellmemoreabouttheirexperiences.Aimingtobe
faithfultoLindsethandNorberg’s(2004)method,Istrovetobracketmythoughtsand
feelingsasmuchaspossible,inordertorefrainfromjudgingorcomparingthenurses’
storieswithmyownnursingbackground(duringtheinterviewsandthroughoutthe
interpretationprocess).Iexperiencedthatthiswasabsolutelynecessaryinorderto
listenactivelyandfocusonthemeaningofthenurses’experiences.Thiscouldbe
especiallychallengingwhentheirstoriesevokedsomeofmyownmemoriesaboutdying
patientswhohadtouchedmedeeply(Tornøe,1996).
37
Duringmyfirstinterpretationattempts,IdiscoveredthatItendedtooverlaythe
interpretationswithmyownnursingexperienceandtheoreticalpreunderstandings.
However,asIgainedproficiencyintheinterpretationmethod,Iwasgraduallyabletolet
goofmynaturalattitude(already“knowing”inlightofmypreunderstanding)to
cultivateamoreopenphenomenologicalattitude(Lindseth,2015;Lindseth&Norberg,
2004).Iexperiencedthatthedialecticalprocessofcomparingmystructuralanalyses
withmyinitialnaïvereadingsexpandedmyinterpretativehorizon.Ibelievethis
reducedtheimpactofmypreunderstandingsandhelpedmetoexploreandinterpretthe
essentialmeaningsintheinterviewtranscripts.
7.3.5Studylimitations
Asthisisaqualitativestudy,itisnotreasonabletodiscusstheconceptsofvalidity,
reliabilityandgeneralizabilityintheirtraditionalsenses.Thenumberofinformantsin
qualitativeresearchprojectsisnotsufficienttoallowforgeneralizedconclusions.
However,theydoinsurestrengthandrepresentativityinrelationtotransferability,as
theypermitanin-depthinsightintothephenomenaunderstudy.Qualitativeprojects
canthereforebestatedtoshowahighcontentvalidity.Thismeansthatthereisahigh
degreeofdetailinthedata(Dehlholm-Lambertsen&Maunsbach,1997).Threetofive
informantsaresufficienttoachieveahighcontentvalidity(Kvale&Brinkmann,2008;
Mishler,1986).Ourdecisionaboutthesamplesizewasguidedbytheneedtoensurea
varietyofin-depthexperiences.Sincequalitativestudiesarenotdesignedtobe
representativeintermsofstatisticalgenerability,theymaygainlittlefromexpanding
samplesizeexceptamorecumbersomedataset,allowingforlessdepthandrichnessto
beextractedfromthematerial(Carlsen&Glenton,2011;Pope,Ziebland,&Mays,2000).
Eventhoughtheresultsinthisstudycannotbegeneralized,theresultsaredeemedas
credibleortrustworthyifpeoplewithsimilarexperiencescanrecognizetheresultsof
thestudy(Benzein,1999;Sandelowski,1993;Sørlie,2001).Inconclusionhowever,one
canargueforandagainsttheinterpretationofthisparticularphenomenological
hermeneuticalstudy,astheresultsthatarepresentedareonlyoneofseveralpossible
interpretations:

38
Aninterpretationmustnotonlybeprobable,butmoreprobablethananotherinterpretation…Itisalwayspossibletoarguefororagainstaninterpretation,toconfrontinterpretations,toarbitratebetweenthemandtoseekagreement,evenifthisagreementremainsbeyondourimmediatereach.(Ricoeur,1976,p.79)
Althoughthehospicenursesinthefirstpapermentionedthattheysometimeshad
Muslimpatientsandthattheyweresensitivetothesepatients’spiritualandexistential
needs,theyhadlimitedexperiencewithspiritualandexistentialcareforpatientsfrom
differentethnicbackgroundsand/orreligioustraditions(paperI).ThestudyinpaperII
wasconductedinasmallruralNorwegiantownwherethemajorityofthepopulation
consistedofethnicNorwegians.NoneoftheparticipantsinpaperIIandIIImentioned
thattheyhadprovidedspiritualandexistentialcaretopatientsfromotherethnic
groupsorreligiousfaiths.TheparticipantsinallthreepaperswereethnicNorwegians.
Duetothestudy’sgeographicalandculturalcontextthestudyislimitedtothe
participants’experienceswithprovidingspiritualandexistentialcaretoethnic
Norwegianpatients.AlthoughNorwayisbecominganincreasinglypluralisticand
multiculturalsociety(Botvar&Schmidt,2010;Aadnanes,2008),approximately73%of
thepopulationhaveanaffiliationtotheChurchofNorway(StatistiskSentralbyrå
(CentralBureauofStatisticsinNorway),2015).Henceforth,theresultsfromthisstudy
arestillrelevantinspiteoftheselimitations.
39
8.Thestudy
AccordingtoHalcomb,Gholizadeh,DiGiacomo,Phillips,andDavidson(2007),itis
importanttoselectpotentialparticipantsthatareabletoprovideinsightintoand
informationabouttheresearchtopicandthattheyareabletoarticulatetheir
perspectiveonrelevantissues.
PaperIandpaperIIexplorehospicenurses’andregisterednurses’spiritualand
existentialcareexperienceswithinthespecializedlevelsofcare,whilepaperIIIexplores
amobilehospicenurseteachingteam’sexperienceswithteachingandsupervisingcare
workersinspiritualandexistentialcarewithintheprimarylevelsofcare.These
healthcarecontextswerechosentocaptureabroadestpossiblerangeofnursing
experiencesrelatedtopracticingandteachingspiritualandexistentialcareforthe
dying.
Forthefirstpartofthestudy(paperI),eightexperiencedhospicenursesfroma
leadingNorwegianhospiceinamajorcitywererecruited.Sincehospicenurseswork
withdyingpatients,itseemedreasonablethatthesenurseswouldbeabletoprovide
richnarrativesabouttheirexperienceswithspiritualandexistentialcareforthedying.
Forthesecondpartofthestudy(paperII)sixregisterednursesfromamedicaland
oncologicalwardinageneralhospitalwererecruited.Incontrasttohospicenurses,
hospitalnursesmustmaintaincurativeresponsibilitiesforpatientswhileatthesame
timecaringforthedyingaspartoftheirdailywork(Costello,2006).Inthisward,eight
bedswereespeciallydesignatedforpatientswithadvancedstagesofcancer.The
authorsassumedthatthesenurseswouldhaveexperiencedthetensionbetween
managingcurativeresponsibilitiesandprovidingspiritualandexistentialcareforthe
dying.
Forthethirdpartofthestudy(paperIII)threehospicenursesinamobilespiritual
andexistentialcareteachingteamwererecruited.Thefourthauthorwasfamiliarwith
themobileteachingteamfrompreviousresearchprojectsatthehospiceandknewthat
theywereableandwillingtoparticipateinresearch.AsNorway’sfirstandonlymobile
spiritualandexistentialcareteachingteam,thesehospicenursespossessedaunique

40
experiencewithtrainingcareworkersinspiritualandexistentialcareforthedyingin
nursinghomesandhomecare.
Anoverviewofthestudy,participantsandpaperscomprisingthisthesisisshownin
table1.
Table1:Overviewofthestudy,participantsandpapersTheStudy Participants Data
collectionInterpretationMethod
Papers Focus
TheHospice Eighthospicenurses
Individualnarrativeinterviews
Phenomenologicalhermeneutical
PaperI Experienceswithpracticingspiritualandexistentialcareforthedying
Medicalandoncologicalwardinageneralhospital
Sixregisterednurses
Individualnarrativeinterviews
Phenomenologicalhermeneutical
PaperII Experienceswithpracticingspiritualandexistentialcareforthedying
Themobilehospicenurseteachingteam
Threehospicenurses
Narrativefocusgroupinterview
Phenomenologicalhermeneutical
PaperIII
Experienceswithtrainingcareworkersinspiritualandexistentialcareforthedying
8.1ThesettingThefirstandthirdpartsofthestudy(paperIandpaperIII)wereconductedwith
hospicenurseswhowereemployedinthesameleadinghospiceinamajorNorwegian
city.Thehospicewasanintegratedunitinasomatichospital.Thehospicenursesin
paperIperformedbedsidenursinginthehospice,whilethehospicenursesinpaperIII,
workedoutsidethehospice,ambulatingbetweenthecity’snursinghomesandhome
caresettingstoteachandtraincareworkersinspiritualandexistentialcare.Thesecond
partofthestudy(paperII)wasconductedwithregisterednurseswhoworkedina
medicalandoncologicalwardinageneralhospital.Thehospitalwassituatedinarural
Norwegiantown.
41
8.2RecruitmentstrategyApurposivesamplingstrategy(Devers&Frankel,2000;Patton,2002)wasappliedto
recruitkeyinformantsfromthechosenhealthcarecontextsinordertofulfilltheoverall
aimofthethesis.Theinclusioncriteriawerethatthenurseswereinterestedinpalliative
careandthattheyhadawidevarietyofexperienceswithspiritualandexistentialcare
fordyingpatients.Inaddition,thenursesinthethirdpartofthestudyalsoneededtobe
experiencedteachersandsupervisorsinspiritualandexistentialcareforthedying.
Forthefirstandthirdpartofthestudy(paperI,andpaperIII),theauthorscontacted
thehospiceleaderandobtainedherpermissiontocarryouttheresearch.Sheassistedin
recruitingparticipantsbyinformingthehospicenursesaboutthestudyandforwarded
theauthors’informationsheetandformalwrittenrequesttoparticipateinthestudy.
Thefirsteighthospicenursesthatsignedupforthestudywereinterviewed.Torecruit
participantsforthelastpartofthestudy(paperIII),thehospiceleaderaskedthethree
hospicenursesinthemobilespiritualandexistentialcareteachingteamiftheywanted
toparticipateinthestudyandsheforwardedtheauthors’informationsheetandformal
writtenrequesttoparticipateinthestudy.Torecruitnursesforthesecondpartofthe
study(paperII),theauthorscontactedtheheadnurseinthemedicalandoncological
hospitalwardandobtainedherpermissiontocarryouttheresearch.Sheassistedin
recruitingparticipantsbytellingthenursesaboutthestudyandsheforwardedthe
authors’writteninformationandformalrequesttoparticipateinthestudy.Thefirstsix
nursesthatsignedupforthestudywereinterviewed.
8.3ThesampleTheeightparticipantsinpaperIwereexperiencedhospicenursesbetweentheages
offorty-oneandsixty-oneyears,witheighttothirty-fiveyearsofnursingexperience.
Everyoneheldnursingdegreesespeciallyrelevantforpalliativecare,suchaspalliative
careandoncologynursing.
ThesixparticipantsinpaperIIwereexperiencedregisterednursesbetweentheages
ofthirty-sevenandsixty-oneyearswithninetotwentyyearsofnursingexperience.
Fourofthemhaddegreesinoncologynursingandpalliativecare.
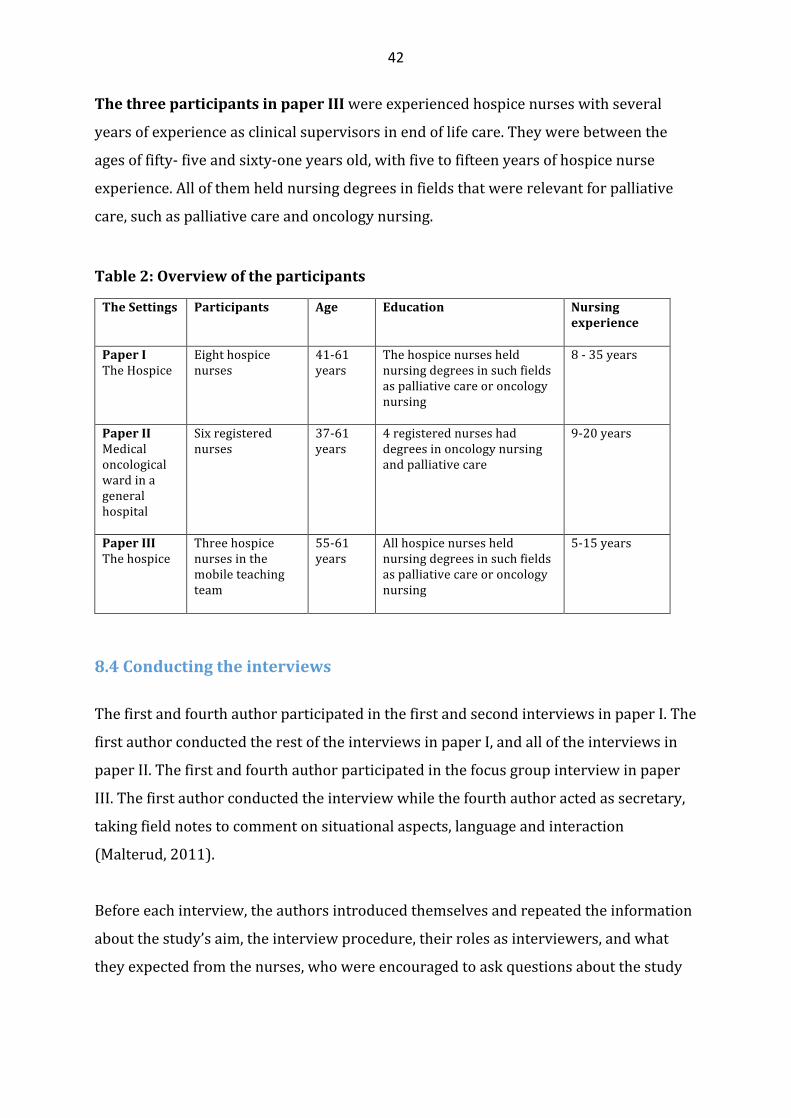
42
ThethreeparticipantsinpaperIIIwereexperiencedhospicenurseswithseveral
yearsofexperienceasclinicalsupervisorsinendoflifecare.Theywerebetweenthe
agesoffifty-fiveandsixty-oneyearsold,withfivetofifteenyearsofhospicenurse
experience.Allofthemheldnursingdegreesinfieldsthatwererelevantforpalliative
care,suchaspalliativecareandoncologynursing.
Table2:Overviewoftheparticipants
TheSettings
Participants Age Education Nursingexperience
PaperITheHospice
Eighthospicenurses
41-61years
Thehospicenursesheldnursingdegreesinsuchfieldsaspalliativecareoroncologynursing
8-35years
PaperIIMedicaloncologicalwardinageneralhospital
Sixregisterednurses
37-61years
4registerednurseshaddegreesinoncologynursingandpalliativecare
9-20years
PaperIIIThehospice
Threehospicenursesinthemobileteachingteam
55-61years
Allhospicenursesheldnursingdegreesinsuchfieldsaspalliativecareoroncologynursing
5-15years
8.4Conductingtheinterviews
ThefirstandfourthauthorparticipatedinthefirstandsecondinterviewsinpaperI.The
firstauthorconductedtherestoftheinterviewsinpaperI,andalloftheinterviewsin
paperII.Thefirstandfourthauthorparticipatedinthefocusgroupinterviewinpaper
III.Thefirstauthorconductedtheinterviewwhilethefourthauthoractedassecretary,
takingfieldnotestocommentonsituationalaspects,languageandinteraction
(Malterud,2011).
Beforeeachinterview,theauthorsintroducedthemselvesandrepeatedtheinformation
aboutthestudy’saim,theinterviewprocedure,theirrolesasinterviewers,andwhat
theyexpectedfromthenurses,whowereencouragedtoaskquestionsaboutthestudy
43
andtheinterviewprocedure.Personalinformationabouteachnursewasobtainedand
writtendown,andthenursesgavetheirwrittenconsent.
TheinterviewswiththehospicenursesinpaperIandpaperIIItookplacein2012and
wereheldinthehospicemeetingroom.Theinterviewswithregisterednursesinpaper
IItookplacein2014andwereheldinameetingroomoutsidethenurses’medical-
oncologicalward.TheindividualinterviewsinpaperIandpaperIIlastedapproximately
onehour.ThefocusgroupinterviewinpaperIIIlasted80minutes.Alloftheinterviews
tookplaceduringthenurses’workinghours.Theinterviewswererecordedand
transcribedverbatimbythefirstauthor.
8.5EthicalconsiderationsThestudywasconductedaccordingtotheHelsinkideclaration(WorldMedical
Association,2001).ApprovalwasobtainedfromtheNorwegianCenterforResearch,
(Norsksamfunnsvitenskapeligdatatjeneste),projectnumber29973.Theethical
considerationsthroughouttheresearchprocesswasinformedbytheHelsinki
declaration(WorldMedicalAssociation,2001)andtheNorwegianCenterforResearch
Data’spolicyandguidelines(NSD,2016).
Theauthorsdistributedaformalwrittenrequestandashortinformationsheetabout
thestudytothenurses.Theinformationsheetdescribedthestudy’saimand
backgroundandexplainedthattheinterviewswouldberecordedandtranscribed
verbatim.Measurestoensureconfidentialityandanonymitywerealsodescribed.The
informationsheetalsostatedthatthenurseswerefreetowithdrawtheirconsentatany
giventime,duringoraftertheinterview.Theinformationwasrepeatedbeforeeach
interviewstarted.Measurestoensureconfidentialityandanonymityrelatedto
publicationwererepeatedandemphasized.Allofthenursesgavetheirwritten,
informedconsenttoparticipateinthestudy.
TheHelsinkideclaration’sethicalguidelinesforhealthcareresearch(WorldMedical
Association,2001)emphasizetheresearcher’sdutytoprotecttheparticipants’life,
health,privacy,dignityandrespect.Italsostressestheimportanceofsafeguarding
44
vulnerableanddisadvantagedindividualsfromthepotentialrisksofthestudyandthe
discomfortitmayentail.Thenursesinthisstudydidnotbelongtoavulnerableor
underprivilegedgroupinsociety,norcantheybesaidtoneedspecialprotectionfrom
theresearcher.However,patientsandtheirlovedonesplayedanimportantroleinthe
nurses’narrativesandwereatriskofbeingexposed.Thisdidnotcauseanyethical
problemsbecausethenursesmadeanefforttopreservepatients’,familymembers’and
colleagues’confidentialityandanonymitywhentheytalkedabouttheirspiritualand
existentialcareexperiences.Thenursesdidnotdiscloseanynamesintheinterviews
andtheyoccasionallyomitteddetailsfromtheirstoriestosafeguardanonymityand
confidentiality.
InScandinaviancountries,spirituality,religionandexistentialissuesareconsideredto
beprivateandsensitivefieldsofenquiry(Botvar&Schmidt,2010;DeMarinis,2008;la
Cour,2008;Aadnanes,2008).Itwasthereforeimportanttobesensitivetothisduring
theinterviewsbecauseoftheasymmetryofpowerintheinterviewee–interviewer
relationship(Mishler,1986).Choosingthenarrativeinterviewmethodwasawayto
rebalancethepowerstructurebetweentheresearcherandthenurses,becausewhena
researcherencouragesintervieweestonarrateabouttheirexperiences,s/heisalso
encouragingthemtofindandspeakintheirownvoice(Mishler,1986).
45
9.MainresultsinPapersI-III
9.1PaperIThenursesdescribedtheirpatients’sufferingasakindof“totalpain”,whichincluded
emotional,spiritualandexistentialdistressandphysicalpain.Theytoldthatthismadeit
difficulttosortoutspiritualandexistentialsuffering.Alleviatingphysicalsymptoms
wasimportant,sinceuncheckedphysicalpainwoulddrainthepatients’energytofocus
onspiritualand/orexistentialconcerns.Thenursessaidthattheyneededagoodsense
oftiming,situationalunderstandingandtheabilityto“senseandtuneinon”patients’
verbalandnon-verbalcuesduringnursingcare,inordertopickupeachpatient’s
existentialand/orspiritualdistressandtorespondadequatelytotheirneeds.
Accordingtothenurses“beingthere”fortheirpatientsliedattheheartoftheirspiritual
andexistentialcarepractice.“Beingthere”wasaboutconveyingconsolationthrough
silentpresencing,companionship,deepexistentialandreligiousconversations,andby
supportingpatients’expressionsoffaithandrituals.Thenursesexpressedthatbuilding
trustingrelationships,easingsuffering,andhelpingpatientsandtheirfamiliestofind
peace,acceptanceofdeathandreconciliation,wasdeeplymeaningfulandrewarding.
Thenursessawthatpatientswhowereunabletoexpresstheirthoughtsandfeelings
aboutdeathcouldbecomestuckinstatesofanxietyanddenial.Itwasthenurses’
impressionthatpatientswhovoicedtheirdistressdiedmorepeacefullythanthosewho
“bottledeverythingup,andtheydescribedanethicaldilemmabetweentheirwishto
helppatientsfindpeaceby“nudgingthemtoopenup”andacceptingthatsomeofthem
wouldnotorcouldnotsharetheirsuffering(p.3).Thenurseswereconcernedaboutthe
riskofviolatingtheirpatients’autonomyandintegrity,andtheystressedthattheywere
boundbytheirprofessionalethicstorespecttheirpatients’choices.Thenurses
expressedthatitwasdeeplypainfulwhentheywereunabletoreachintotheirpatients.
Bearingwitnesstodyingpatients’sufferingandpain,inspiteoftheirconsolationefforts
wasemotionallychallengingbecauseitmadethenursesfeelhelplessandvulnerable.
Theythereforeplacedgreatimportanceondebriefingandsupportfromtheircolleagues
inordertoenduretheemotionaldemandsofbeingwiththedying.
46
9.2PaperII
Thenursesexperiencedthatdyingpatients’spiritualandexistentialsufferingemerged
assubtleandelusiveentanglementsofphysical,emotional,relational,spiritualand
existentialpain.Thenursestoldthatspiritualandexistentialsuffering(whichdidnot
alwaysincludereligiousaspects)couldemergespontaneously,forexampleduring
physicalcare.Theabilitytozoominonfleetingmoments,whenpatientswantedand
neededtotalkwasthereforeviewedasanessentialskill.
Thenursesstrovetoconveyconsolationbyunburdeningtheirpatientstofacilitatea
peacefulandharmoniousdeath.Theytoldthatthiscouldinvolvehelpingpatientsto
resolvepracticalworries,(i.e.completingahomerenovation),aswellashelpingthemto
makepeacewiththeirpast,theirlovedonesandwithGod(p.6).Thenursesfelttheyhad
beenabletoconveyconsolationwhentheysawthattheireffortshadhelpedpatientsto
experienceagood,peacefulandharmoniousdeath.Witnessingthepeacefulpassingofa
patientwasdescribedasaspecialmomentthatfilledthemwithreverenceandawe.This
wasexperiencedasveryrewardingandfulfilling.Thenursesweredeeplymovedand
amazedwhenpatientssharedtheirtrustandopenness:“SometimesI’mreally
astonishedthattheychoosetosharetheirtroublesandworrieswithme!Eventhough
I’mtheirnurse,I’mstillastranger!”(p.7)
Thenursesexpressedthattheyhadanimportantfunctionas“emotionalcontainers”
whentheylistenedandencourageddyingpatientstoventtheirfeelings.“Itdoesn’tdo
anyharmifpeoplestarttocry.Iusuallytellmypatientsthattheydon’thavetofeel
ashamedoftheirtears.Tearsareonlymeltingice!”(p.8).However,thenursesalso
statedthatbearingwitnesstopatients’spiritualandexistentialdistresscouldbe
challengingbecauseitexposedthemtotheirownfeelingsoffinitudeandvulnerability.
Bearingwitnesstounconsolablepatientsprovedtobethenurses’greatestemotional
challenge.Beingunabletohelppatientstowardsapeacefuldeathcouldmakethemfeel
professionallyinadequateandhelplessandtheyfeltthattheyhadnotdoneagood
enoughjob.However,thenursesalsoemphasizedthat,whatpatientsneededmost,were
nurseswhoshowedthattheywerewillingtostandbytheirpatients,andwouldnot
abandonthemintheirtimeofneed.
47
9.3PaperIIIAccordingtothemobilehospicenurseteachingteam,careworkersfrequently
expressedthattheywerereluctanttoaddressdyingpatients’existentialandspiritual
suffering.Theteamexperiencedthatcareworkerscouldbequiteafraidoftalkingwith
patientsabouttheirexistentialandspiritualconcerns.Theteamexpressedthatmanyof
themwereafraidofsilenceand“justbeingwith”thepatient“intheroomofdeath”(p.4-
5).Theteamthereforestressedtheimportanceofhelpingthecareworkersdevelop
theircourageandcompetencytoprovidespiritualandexistentialcare.Theteam
believedthatthecareworkers’fearanduncertaintystemmedfrompersonalinsecurity
aswellasinsufficientcommunicationandlisteningskills.Theythereforeplacedgreat
emphasisontherelationalaspectofspiritualandexistentialcarewhentheytaughtthe
careworkersto“workfromtheheart”.
Theteamtaughtcareworkerstoidentifypatients’spiritualandexistentialsuffering,
initiateexistentialandspiritualconversationsandtoconveyconsolationthroughsilent
presencingandactivelistening.Theteamtransferredtheirpersonalspiritualand
existentialcareknowledgebyparticipatingactivelyinpatientcaretogetherwiththe
careworkers,andbyprovidingsupervisionandfeedbackrelatedtothesesituations.
Thiswascalled“bedsideteaching”,whichcouldtakeplaceduringmanydifferentkinds
ofpatientencounters,suchasgivingphysicalcare,doingnursingprocedures,orjust
takingpartinconversationswithpatients.Theteamemphasizedthatcriticalreflection
wasanimportantpartofbedside“learningbydoing”.Theteamthereforeplacedgreat
weightonconductingreflectivedialogueswiththecareworkersabouttheirchallenges
andexperiencesbeforeandafterthepatientencounter(p.5).
Drawingoncareworkerfeedbackandtheirownobservations,theteamconsideredthat
situated“bed-sideteaching”hadproventobeanimportanttooltodevelopcare
workers’courageandcompetencytoprovidespiritualandexistentialcareforthedying.
Theteamobservedthatcareworkersbecamemoreinvolvedandwillingtoexpose
themselvestotheirpatients’spiritualandexistentialsuffering.Theteamthoughtthis
indicatedthatthecareworkershadbecomemorecourageous:“Iseethattheydareto
involvethemselvesmoreinthesesituations,exposingtheirvulnerability.Iseethatthey
havebecomebraver.”(p.6)

48
10.DiscussionInthisstudythenursesnarratedabouttheirlivedexperiencewithpracticingand
teachingspiritualandexistentialcarefordyingpatientsinthreedifferentNorwegian
healthcarecontexts.
Threethemesemergedthroughthecomprehensiveunderstanding,(discussion)ofthe
resultsinpaperI-III:Conveyingconsolation,Vulnerabilityandhelplessness,Compassion
andcourage.Todevelopthislaststepintheanalysis,thepaperswerereadasawhole,
takingintoaccounttheauthor’spreunderstanding,previousresearchandrelevant
theory.AlthoughconsolationdidnotemergeasanexplicitthemeinpaperIII,themobile
hospiceteachingteam’ssituatedbedsideteaching(p.3)provedtobeconsistentwiththe
consolationtheme,whichemergedinpaperI(p.3-5)andpaperII(p.7-8).
10.1ConveyingconsolationConveyingconsolationprovedtobeanoverarchingthemeinthestudy.Accordingto
Klass(2014),“solace”isunderstoodasasenseofsoothingwhichcaninvolvepleasure,
enjoymentordelightinthemidstofsorrow,hopelessnessanddespair,hencetobe
consoledistobecomforted.Theetymologyofthewordcomfort,carriesthesenseof
intersubjectivitybecauseitisderivedfromtheLatinfortis,whichmeansstrongor
powerfulandtheprefixcom,whichmeanswith(Klass,2014).Accordingly,toconsoleor
comfortanothermeanstostrengthenortofindstrengthtogether(Klass,2014,p.7).
Theresultsshowthatthenursesconveyedconsolationthroughactivepresencingand
relationshipmaintainingactivities,whichcouldinvolvegentlehandorfootmassages,
usingacaringtouchandlisteningandcommunicatingemphaticallywiththeirpatients
duringphysicalcare,orbyjustbeingwiththeminsharedsilence.Thenursesstroveto
createatrustingrelationalhaven,wherethedyingcouldfeelsafeenoughtoopen
themselvesandexpresstheirspiritualandexistentialdistress(paperIp.3-5andpaper
IIp.6-7).
49
ThenursesinpaperIandIIandthemobilehospicenurseteachingteaminpaperIII
emphasizedtheimportanceofseizing“thefleetingmoments”whenpatientsneededand
wantedtotalkabouttheirsuffering.Thenursesstressedthatthisdemandeda“fine
tunedantenna”(paperIIp.5),andthat“Ifyoudothingsproperlyandshowthatyou
care,existentialorspiritualdistresseventuallysurfacesifit’sthere”(paperIp.5).
Strivingto“getitright”thenursestried“totuneinon”theindividualpatient,paying
attentiontotheirenergylevelsandemotionalstates,neitherforcingnoravoiding
spiritualandexistentialconversations(paperIp.3).Themobilehospicenurseteaching
teaminpaperIIIplacedgreatemphasisonshowingthecareworkershowtousenatural
opportunitiesduringphysicalcaretoassessspiritualandexistentialneedsandto
integrateappropriateinterventions.Accordingtotheteachingteam,teachingthecare
workerstoaskpatientsthesimplequestion:“Howareyou?”couldbeenoughto“open
thedoortomeaningfulandsafedialogueswithpatientsabouttheirthoughtsand
feelings”(paperIIIp.5).Theteachingteamtaughtthecareworkerstolistenattentively
andtopayattentiontotheirpatients’facialexpressionsandbodylanguage.(paperIIIp.
5)
Theseresultssuggestthatconsolationcannotbeplanned,prescribedorimposedon
patientsthroughproceduralrulesand/orguidelines.Rather,conveyingconsolation
seemstobeadeeplypersonalandspontaneousactivity,whichdependsonthenurses’
andcareworkers’abilitytoapplytheirrelationalcompetence,creativityand
compassionateperceptivenessinordertotuneintotheparticularpatient’s
circumstances.ThisissupportedbyseveralSwedishconsolationstudies,(Norbergetal.,
2001;Roxberg,Eriksson,Rehnsfeldt,&Fridlund,2008;Söderberg,Gilje,&Norberg,
1999;Talseth,Gilje,&Norberg,2003),whichindicatethatconsolationcanonlybe
conveyedthroughcommunionanddialogueintrustingnurse-patientrelationships.
Whenthesufferingpatientbecomesopenandexpressessuffering,andwhenthenurse
mediatingconsolationbecomesopenandlistensinanemphaticandnon-judgmental
manner,theyareincommunionanddialogue.Duringthesemoments,thenurseandthe
patientmayexperiencemutualconsolation.Thesufferingpatientdrawsconsolation
fromthenurse’spresenceandthenursedrawsconsolationfromobservingthatthe
patient’sdistressedandanguishedstatemovestowardspeaceandtranquility(Norberg
etal.,2001).
50
10.1.1Thehermeneuticsofconsolation
AccordingtoNorbergetal.(2001,p.551),“theimportantprerequisiteforcommunionis
asharedaffectivestate,ratherthanasharedcognitiveinterpretationofthesituation.”
However,drawingontheworksofGadamer(2004)andRicoeur(1976,2008)itcanbe
arguedthatsharingthepatient’ssufferingalsorequiresaninterpretationaldialogue
aboutthemeaningofthepatient’ssuffering.Henceforth,conveyingconsolationthrough
communionanddialoguecanalsobeviewedasahermeneuticalactivity.Thiswillbe
explicatedinthefollowing.
InNorbergetal.’s(2001)consolationmodel,communionanddialogueislinkedtotwo
domains,-thepatient’sexperienceofhisorhersufferingandthenurse’sexperienceof
thepatient’ssuffering.Henceforth,sharingtheirexperienceofthepatient’ssuffering
requiresmorethanjustsharinganaffectivestate,becausethepatient’sexperience
cannotdirectlybecomethenurse’sexperience,andviceversa:
….whatisexperiencedbyonepersoncannotbetransferredwholeassuchandsuchexperiencetosomeoneelse.Myexperiencecannotdirectlybecomeyourexperience.Aneventbelongingtoonestreamofconsciousnesscannotbetransferredassuchintoanotherstreamofconsciousness.(Ricoeur,1976,p.16)
However,Ricoeur(1976)maintainsthatsomethingistransferredfromonesphereof
lifetoanother.“Thatsomething”isnottheexperienceasexperienced,butitsmeaning.
Henceforth,experienceaslived,remainsprivate,butitssense,itsmeaningbecomes
public(Ricoeur,1976).InRicoeur’swords:“….communicationinthiswayisthe
overcomingoftheradicalnon-communicabilityofthelivedexperienceaslived”
(Ricoeur,1976,p.16).Henceforth,thenursecanonlyinterpretthemeaningofthe
patient’ssufferingthroughcommunionanddialogue,inwhichsheexperiencesthe
patientassufferingornot(Kahn&Steeves,1986).AsGadamer(2004,p.292)points
out:“Thetaskofhermeneuticsistoclarifythemiracleofunderstanding,whichisnota
mysteriouscommunionofsouls,butsharingacommonmeaning”.Henceforth,drawing
onGadamer(2004)andRicoeur(1976,2008)conveyingconsolationthrough
51
communionanddialogue(Norbergetal.,2001)canbeunderstoodasakindofclinical
hermeneutics(Kahn&Steeves,1986).Humanactionsarelikeatextwhichawaitsfresh
interpretationsthatdecidetheirmeaning(Ricoeur,2008).Thus,allsignificantevents
anddeedsofhumanactionareopentoakindofpracticalinterpretation,whichisopen
toanybodywhocanread(Ricoeur,2008,p.151).FollowingRicoeur’s(1976,2008)
phenomenologicalhermeneuticallineofthought,theinterpretationofthepatient’s
sufferingdependsonthedialogicinteractionofthreeelements:thetext,thereaderand
thecontext:Thepatient’sexperienceofsufferingcanbeunderstoodasthetextwhich
thereader–nursemustinterpret,andviceversa(Kahn&Steeves,1986).Asthenurse
“reads”thepatient,thestory,andthebody,soalsothepatientalwaysengagesina
reversehermeneuticswherethepatient“reads”andinterpretsthenurse,andjudgeshis
orherinterestandcareforthepatientasauniqueperson(Schei,2006).
Cultural,spiritualandexistentialmeaningsthatthenurseandthepatientshareordo
notshareaboutsufferinginducingeventswillalsoinfluencehowtheyinterpretthe
meaningofthepatient’ssuffering.Inaddition,contextualfactorswithintheparticular
healthcaresetting,suchasphysical,psychologicalandsocioculturalenvironmental
features,alsoimpactonhowthenurseandthepatient“readandinterpret”themeaning
ofthepatient’ssuffering(DeMarinis,Ulland,&Karlsen,2011;Kahn&Steeves,1986;
Ulland&DeMarinis,2014).
Theresultsrevealthatthenurses’ownlifeexperiencesandpersonalbeliefsinfluenced
howtheyfeltaboutprovidingconsolation,especiallyrelatedtothepatients’religious
issues.Althoughthenursesacknowledgedthattheyhadaprofessionalobligationto
supportthepatients’sourcesoffaith,meaningandhope,regardlessoftheirownbeliefs,
someofthemhadmixedfeelingsaboutthisbecausetheywerenot:
veryreligiousor“veryChristian”astheyputit:“Actually,IfeelabituncomfortablewhenpatientstellmethattheyplacetheirlifeinGod’shands.Ithinkit’sprobablybecauseI’mnotabeliever.I’mveryskepticaltowardstheBibleandtheChristianfaith”.(paperIp.4)
Ingeneral,thenursesviewedreligionasaveryprivateandpersonalmatter,which
madethemwaryofimposingthemselvesontheirpatients(paperIIp.5-6).Somealso
saidthattheypreferredtoreferpatientstothehospiceorhospitalchaplainforreligious
52
supportbecausetheyfeltuncertainandinsecureaboutaddressingpatients’religious
concerns(paperIp.4,paperIIp.5,paperIIIp.4-5).TwoofthenursesinpaperIhad
pursuedtheologicalstudiespriortonursing.Theircolleaguesregardedthemasvaluable
resourcesbecausetheywereabletohelppatientswiththeirspiritualandexistential
distressbycombiningtheirpersonalfaithwiththeologicalknowledgeandpastoral
counselingskills.(paperIp.4)However,inspiteoftheirambivalence,thestudyshows
thatthenursesthoughtitwasimportanttoalleviatingtheirdyingpatients’spiritualand
existentialsufferingandtheystrovetoconsolethemasbesttheycouldwithintheir
limitedtimeandresources.(paperIIp.6)
10.1.2Therelationaldimensioninthenurses’consolationnarratives
Schei(2006)pointsoutthatatherapeuticalliancebetweentheclinicianandthepatient
emergesthroughreciprocalinterpretationandprojectionwheregestures,facial
expressions,intonation,pausesandeyemovementstypicallyconveymoreinformation
thanmerewords.Assuch,meaningistransmittedonseverallevelssimultaneously;
compassionandunderstandingmaybeexpressedthroughthelookinthenurse’seyes
orthetimbreofvoice,orthespeedoftalkingwhilefactualbusinessiscarriedoutinthe
explicitverballane.Bothparticipantsinadialoguemonitorthemselves,andtheother,
includingtheother’sapparentinterpretationsofone’sownutterances,incomplex
recursiveinterplay.Thus,thedialoguecontinuallyproducesnewmeanings,basedon
whathasalreadyhappenedintheconversationandinthenurse-patientrelationship.
Importantlessonsmaybegleanedfromtheseconsiderations(Schei,2006).Tothe
extentthatpatientswithorwithoutseriousdisease,alsosuffer,i.e.experiencemental
imbalance,isolation,grief,fearandotherfeelingscommonlyassociatedwithillness,pain
andexistentialloss,theresearchliteraturesuggeststhatbecomingapartofa
therapeuticalliancemayinitselfbeconducivetohealingandadaptation(Eells,1999;
Schei,2006).Moreover,Schei(2006)assertsthatthismaybeespeciallytrue–and
valuablewhenmedicaltechnologyhaslittletoofferinthewayoffurtherdiagnosticor
therapeuticprocedures.Henceforth,receivingconsolationthroughcommunionand
dialoguewiththenurse(Norbergetal.,2001)maybeoftherapeuticvalueforthedying.
Thiswillbediscussedinlightofthreeofthestudy’sconsolationnarratives.
53
1. Breakingtheboil
Inthefirstnarrative,adyingyoungcancerpatient“justwantedtofloatawayinadrug
daze.”(paperIp.4)Thenursedescribedthepatients’spiritualandexistentialpainas“a
largefesteringboil.“I’mnotsurehowwemanagedtopunctureitbecausewehadtrieda
lotofthings.”Oneday,thedoctorspontaneouslyaskedthepatientifshewasbitter
becauseshewasdyingsoyoung.Thedoctor’soutburstseemedtosnapthepatientoutof
herdrugdazebecausesheretortedthatshewasnotbittersinceherillnesshad“helped
hertogrowandmatureinwaysshecouldn’timagineevenifshehadlivedtoaripeold
age”.Accordingtothenurse,thisconversationbrokeopentheboilofsuffering,which
seemedtocreateaturningpointinthepatient’slife,becausesherosefromher
deathbed,reconnectedwithhersisterandmother,andwenthometoherflatonelast
timetosetheraffairsinorder.(paperIp.4)Andthenursethoughttoherself:“Yes!
Exactlythatquestionshiftedsomethingbecausenowwehadagirltakingbackherlife!”
2. Disappearingintoablackhole
Inthesecondnarrative(paperIIp.6),thenursetoldaboutawomanwhowasdyingof
lungcancer.Sensingheranxiety,thenurseaskedwhatshethoughtaboutdeath.The
patientfearedthatshewouldjust“disappearintoabigblackhole”whenshedied.“Isn’t
thereanythingmoreafterwards?”sheaskedthenurse.Thenursewasabletorelievethe
patient’sanxietybysharingherpersonalbeliefthatshewouldbereunitedwithher
lovedoneswhenshepassedaway.Accordingtothenurse,thepatientseemedtodraw
consolationfromthehopeofreunitingwithherdeceasedfather:“Perhapshe’sstanding
therewaitingforme!”sheexclaimed.Althoughthepatientseemedcalmer,shewasstill
worriedaboutnotbeingabletofinishrenovatingherfamily’shome.Toeaseher
worries,thenursecontactedthesocialworkerwhoorganizedherfamilyandfriendsto
completethejob.
3. ApunishmentfromGod
Thethirdandlastnarrative,whichwillbementionedhere,isanarrativeaboutadying
elderlywomanwhorefusedtoreceivemorphinebecauseshebelievedthatGodwas
punishingherthroughherpain.Inthiscasethenursehadtodealwiththepatient’s
religiousissuesbeforeshewaspermittedtorelievethepatient’sphysicalpain.
54
Desperatelysearchingforawaytoreachintothepatientitsuddenlydawnedonthe
nursethatshecoulduseprayer“toturnthesituationaround”assheputit.(paperIIp.
6)Sothenurseaskedthepatientifshewantedtosay“TheLord’sPrayer”withher.
Accordingtothenurse,sharingtheprayerhelpedhertoconnectwiththepatient,which
openedupanaturalopportunitytotalkwithheraboutherpictureofapunishingand
vengefulGod.Althoughthenurseclaimedthatshewasnot“veryreligious”sheshared
herbelieveinatrustingandlovingGod:“TheGodIbelieveinlovesusandwantstohelp
us!AndnowIcanhelpyoutotakeyourpainaway,-atleastsomeofit!–Ifyou’llletme!”
(paperIIp.7)Thenursethoughtthatthepatientseemedtodrawconsolationfromthe
prayerandtheconversation,becausesheacceptedtoreceivemorphineregularlyafter
that,andaccordingtothenurse,thepatientdiedpainfreeandatpeacewithGod.
Inthesenarrativesthepatients’spiritualandexistentialsufferingseemedtoevolve
aroundtheirdisconnectedrelationshipswithself,familymembersandwithGod.The
nursesthereforestrovetohelpthepatientstoreconnectandrestoretheirrelationships
by:
Ø Challengingthepatienttofacehersuffering,insteadofescapinginadrugdaze,
whichstimulatedthepatienttotakechargeofherlife,settleheraffairsand
reconnectwithhersisterandmother(narrative1)
Ø Helpingthepatienttoovercomeherexistentialfearandlonelinessrelatedto
dying,byconveyingahopeofreconnectingwithherlovedonesinthe“here
after”(narrative2)
Ø Helpingthepatienttomaintainherfamilytiesandresponsibilitiesrelatedto
completingtherenovationofherfamilyhome(narrative2)
Ø HelpingthepatienttoconnectwithGodandtoshiftherperceptionofGodfrom
vengefulandpunishingtocaringandloving(narrative3)
InthefollowingtheseresultswillbereflectedoninlightofSulmasy’s(2002)relational
perspectiveonsuffering.AccordingtoSulmasy(2002),illnessdisturbsrelationships
bothinsideandoutsidethebody.Inspiteofthis,contemporaryscientifichealinghas
untilrecentlybeenlimitedtorestoringthephysiologicalhomeostaticrelationships
withinthepatient’sbody,(suchasrestoringadiabetespatient’sbloodsugarbalancein
relationtootherbiochemicalprocesses).Illnesshowever,disturbsmorethanthe

55
relationshipsinsidethehumanorganism.Itcontributestosufferingbecauseitdisrupts
familiesandworkplaces.Itshatterspreexistingpatternsofcoping,anditraises
questionsaboutone’srelationshipwiththetranscendent(Sulmasy,2002).Accordingly,
illnessdisturbstherelationshipbetweentheindividualpatientandhisorher
environment,includingthefamilialandsocialnexusofrelationships,whichsurround
thepatientanditdisturbstherelationshipbetweenthepatientandthetranscendent
(Sulmasy,2002).ThisissupportedbyCassel’s(1991b)work,whichshowsthat
sufferinggeneratesexistentialloneliness,becauseitalienatesthesuffererfromhisor
herrelationshipswithothers,fromtheworldandfromhisorhertranscendentsourceof
meaning.AccordingtoSulmasy(2002)healingimpliesthatgenuineholistichealthcare
attendstoallofthedisturbedrelationshipsoftheillpersonasawhole,restoringthose
thatcanberestored,evenifthepersonisnotcompletelyrestoredtoperfectwholeness.
Thismeansthatattheendoflifewherethepatient’shealthnolongercanberestored,
healingisstillpossible(Sulmasy,2002).FollowingSulmasy(2002)theconsolation
narrativescanbeunderstoodashealingsincetheyinvolverestoringthepatients’
significantrelationshipstoself,othersandthetranscendent.Theresultssuggestthat
appropriateconsolationrequiresattentiontotherestorationofalltheintrapersonaland
extrapersonalrelationshipsthatcanstillbeaddressedevenattheendoflife(Sulmasy,
2002).
10.1.3ConveyingconsolationinrelationtoSpiritual/ExistentialandPsychosocialcare
Giventhenurses’strongfocusonhelpingtheirpatientstorestoredisconnected
relationshipsitcanbediscussedwhethertheconsolationnarrativesprimarilyare
concernedwithpsychosocialcare.Withinthepalliativecarecontext,psychosocialcare
hasbeendefinedasconcernwiththepsychologicalandemotionalwellbeingofthe
patientandtheirfamily/carers,includingissuesofself-esteem,insightintoand
adaptationtoillnessanditsconsequences,communication,socialfunctioningand
relationships(Tan,Wilson,Olver,&Barton,2011).Thereexistsathindividebetween
spiritual/existentialandpsychosocialcareinthepalliativecareliterature,becausethe
importanceofrelationshipsisemphasizedinbothdomains(Sinclair&Chochinov,2012;
Tanetal.,2011).Itisthereforeunderstandablethatpsychosocialandspiritual/
existentialissuestendedtooverlapinthenurses’consolationnarratives:“Shestill

56
worriedaboutherfamilybecauseshewasgoingtodiefromherkids,sointhiscase
unburdeningherwiththepracticalstuffwasanimportantpartofspiritualcare”
(narrative2,paperIIp.6).Thisissupportedbyotherstudies,whichsuggestthatin
clinicalpracticethespiritualdomaincoalesceswithotherdomainsandmaythereforebe
addressedthroughbothpsychologicalandspiritualmodalities(Sinclair&Chochinov,
2012,p.73).Itisthereforeinterestingtonotethattherelationaldimensioninthe
consolationnarrativesalsoresonatewithseveraldefinitionsthatexpressspiritualityin
relationalandtranscendentalterms.Puchalskietal.(2009)forinstance,define
spiritualityas:“theaspectofhumanitythatreferstothewayindividualsseekand
expressmeaningandpurposeandthewaytheyexperiencetheirconnectednesstothe
moment,toself,toothers,tonatureandtothesignificantorsacred”(Puchalskietal.,
2009,p.887).
ThisisinlinewithPargament(2013),whopointsoutthattherelationaldimensionof
spiritualitybecomesespeciallyapparentduringsacredmomentswhichare
characterizedbyadeepsenseofinterconnectednessandcaring.He(2013)maintains
thatsacredmomentsareextraordinarymomentswhennursescanseeintowhotheir
patientsareandtheycanseeintowhothenursesare.Duringthesemoments,thenurse
andthepatienttouchandaretouchedbyeachother.Assuch,sacredmomentsare
momentsofprofoundinterconnectedness(Pargament,2013).Thiscorrespondsto
Norbergetal.’s(2001)pointofview.Accordingtothem,consolationgivesafeelingof
meaning,homecomingandcontactwiththesacreddimension(transcendence).When
thenurseparticipatesinthepatient’spain,communionemerges.Norbergetal.(2001)
maintainthatcommunionisadeepconnectionthattouchesthesacreddimensionwhich
isakintoaconnectionwithsuchphenomenaasbeauty,joyandgoodness.Following
Pargament(2013)andNorbergetal.(2001),thenurses’consolationnarrativescanbe
understoodasdescriptionsofsuchsacredmoments.Itisimportanttonotethat
Pargament(2013)usestheterm“sacred”inapsychologicalratherthanatheological
sense.Accordingtohim(2013)“sacred”referstohumanperceptionsofqualitiesoften
associatedwiththedivineorhigherpowers.Healsopointsoutthattheseperceptions
donotreferonewayortheothertotheontologicalrealityofthesacred,higherpowers
orGod.Rather,theyreflectonhumancharacterandhumanrelationships(Pargament,
2013).Fromthisperspective,itcanbearguedthatnursesmayexperiencesacred
57
momentsintheirworkwhethertheyconsiderthemselvestobereligiousornot.
Henceforthitseemsreasonabletointerpretthenurses’consolationnarrativesas
“sacredmoments”inPargament’spsychologicalsenseoftheterm,althoughsomeofthe
nursesexpressedthattheydidnotexperiencethemselvesasvery“religiousor
Christian”(paperIp.4,paperIIp.6).
Rumbold(2003,p.S12),drawingonLartey(1997),describesspiritualityasthewebof
relationshipsthatgivecoherencetoourlivesandthatreligionmayormaynotbeapart
ofsuchaweb.Rumbold(2003)pointsoutthatoftenpeopleonlybecomeawareof
strandsinthewebwhentheyarestretchedorbroken,whichmayhappenduringlife-
changingeventslikeadiagnosisofseriousillnessinoneselforlovedones.Accordingto
Lartey(1997)citedinRumbold(2003),thiswebofrelationshipsinvolvesrelationships
withplacesandthings,withourselves,withsignificantothers,withgroupsor
communitiesandwithtranscendence.Theserelationshipsformauniquepatternfor
eachofus,andeachofusneedsthatpatterntobelargelyintactinordertofeelwhole.
ThisisconsistentwithSulmasy’s(2002)relationalunderstandingofhealing.Lartey
(1997),citedinRumbold(2003).maintainsthat:“Ourwebofkeyrelationshipsdefines
whoweare,andwhenthoserelationshipsaredisrupted,wefeelvulnerable.”Klass
(1999)citedinRumbold(2003)maintainsthatagoodwaytothinkaboutspirituallifeis
tolookforthosemomentswhenwefeelmostdeeplyconnectedtoourworld.Whenwe
feelleastisolatedinsideourusualegoboundaries,wefeelapartofsomethinglarger
thanourselves,andtherestoftheworldmakessense(Klass,1999).
10.1.4ConsolationthroughExistentialmeaningmaking
DrawingonFrankl(1969),Park(2013)pointsoutthatmeaningiswidelyregardedas
centraltohumanexperience.Iffundamentalrelationsorconditionsinlifearebroken,
sourcesofmeaningareusedtorestorethebalancebetweentheindividual’s
expectationsoflifeandtherealityasitisexperiencedhereandnow.Suchreappraisal
andusageofsourcesofmeaningareessentialwhenoneisconfrontedwithdemanding
lifesituations(Sørensenetal.,2015).Norbergetal.(2001)pointoutthatpeoplewho
suffer,experiencealossofmeaningandintegritybecause“everythingfallsapart”.
InspiredbytheexistentialphilosopherSørenKierkegaard,they(2001)statethatitis“in

58
thefearfulmomentsofdesolationwherethereisnomeaningleftthatabravestatement
ofconsolationpenetratesthedarknessandcreatesnewmeaning.Thishappensonthe
borderwherenothingispossibleanymore”(Norbergetal.,2001,p.545).Henceforth,
assistingpatientsintheirexistentialmeaningmaking,whichaccordingtoSchnell’s
(2009),researchmayormaynotinvolveatranscendentdimension,isalsoanimportant
partofconveyingconsolation.
Schnell(2009)definesmeaningfulnessasafundamentalsenseofmeaning,basedonan
appraisalofone’slifeascoherent,significant,directedandbelonging,andshe(2009)
categorizessourcesofmeaninginthefollowinggroups:Self-transcendence,which
concernsone’scommitmenttoobjectivesbeyondone’simmediateneeds.Verticalself-
transcendence,whichconsistsofreligionandspirituality,thatisorientatedtowardsan
immaterialcosmicpower.Horizontalself-transcendence,whichislinkedtotaking
responsibilityfor(worldly)affairsbeyondone’simmediateconcerns.Self-actualization
referstoemploying,challengingandfosteringone’scapacities.Orderislinkedtoholding
ontovalues,practicality,decencyandthetriedandtested.ThelastofSchnell’s(2009)
sourcesofmeaningiscategorizedaswellbeingandrelatedness,whichinvolves
cultivatingandenjoyinglife’spleasuresinprivacyandcompany.
Schnell’s(2009)researchonexistentialmeaningmakingtakesasecularEuropean
contextintoaccount(laCour,2008;laCour&Hvidt,2010),whichmakesitespecially
relevantforthestudy’sNorwegianhealthcarecontext,whereamajorityofthe
populationeitherdefinethemselvesas“secular”or“spiritualbutnotreligious”(Botvar&
Schmidt,2010;Aadnanes,2008).Inthefollowing,Schnell’s(2009)sourcesofmeaning
willthereforebeappliedtointerprettheconsolationnarratives.
Inthefirstnarrative(paperIp.4),thepatientwishedtowithdrawfromherexistential
sufferinginadazeofMorphineandStesolid.Inherconversationwiththepatient,the
doctoraskedthepatientifshewasbitterbecauseshewasgoingtodiesoyoung.By
confrontingthepatientwithhervulnerability,thedoctorliterally“heldupamirror”
whichchallengedthepatienttoreflectonthemeaningofhersuffering.Accordingtothe
nurse,thepatientlookedthedoctorsquarelyintheeyeandexclaimedthatshewasnot
bitterbecauseheryearsofillnesshadcontributedtogrowthandmaturitybeyondher
59
age(paperIp.4).Thenursebelievedthatthisconversationgeneratedashiftinthe
patient’swayofdealingwithhersituationbecauseshewenthometosetheraffairsin
orderandshereconnectedwithhermotherandsister.Thissuggeststhatthedoctor
stimulatedthepatient’sprocessofexistentialmeaningmakingrelatedtohorizontal
formsofself-transcendence:self-actualization,order,wellbeingandrelatedness
(Schnell,2009).
Inthesecondnarrative(paperIIp.6),thepatient’sneedformeaningseemedtobe
relatedtoorder(wishingtocompletethefamilyhomerenovationbeforeshedied)and
horizontalself-transcendence,sincefixingupthefamilyhomealsoinvolvedthepatient’s
needformeaningbytakingresponsibilityfor(worldly)affairsbeyondherimmediate
concern(Schnell,2009).Thepatient’sneedformeaningwasalsorelatedtowellbeing
andrelatedness(Schnell,2009),becauseshewasafraidthatshewouldceasetoexist
afterdeath,andthatthiswouldcutherofffromherlovedones.Accordingtothenurse,
thepatientseemedtodrawconsolationfromthepossibilityofreunitingwithherloved
onesinthehereafter.
Inthelastnarrative(paperIIp.6-7),thepatient’sneedformeaningwaslinkedto
verticalself-transcendence,wellbeingandrelatedness(Schnell,2009).Thepatient
sufferedfromphysicalandspiritualpain,becauseshethoughtshehadtoendureher
painasGod’spunishmentforhersins.Byprayingwiththepatientandtalkingwithher
aboutwhyshethoughtGodwaspunishingher,thenursewasabletohelpthepatientto
findpeacewithGod.Thisallowedthepatienttoacceptmorphinefromthenurse,which
alleviatedherphysicalsuffering.
TosummarizetheresultsofthisinterpretationinSchnell’s(2009)terms:Conveying
consolationwasaboutassistingpatientsintheirexistentialmeaningmakingrelatedto
thehorizontalrelationaldimension:-helpingpatientstorepairandmaintaintheir
relationshipswithfamilymembers(narrative1and2).Italsoinvolvedassisting
patientsintheirexistentialmeaningmakingrelatedtotheverticalrelationaldimension:
-helpingthepatienttofindpeacewithGod(narrative3).

60
ThisisinlinewithReed’s(1992)understandingofspirituality.Accordingtoher(1992),
spiritualityspecificallyreferstothepropensitytomakemeaningthroughasenseof
relatednesstodimensionsthattranscendtheselfinsuchawaythatempowersanddoes
notdevaluetheindividual.Reed(1992)pointsoutthatthisrelatednessmaybe
experiencedintra-personally(asaconnectednesswithoneself),interpersonally(inthe
contextofothersandthenaturalenvironment),andtrans-personally(referringtoa
senseofrelatednesstotheunseen,Godorpowergreaterthantheselfandordinary
sourceswhichimpliesanexpansionofboundaries,inward,outwardandupward:
“Spiritualitythenismanifestedthroughthesevariouspatternsofconnectedness,in
whichonestepsbeyondthestructuresofeverydayexistencetoendowtheordinary
withextra-ordinarymeaning”.(Reed,1992,p.350)
Thenurses’consolationeffortswhichevolvedaroundenablingtheirpatientstoregain
andmaintaintheirrelatednesstoself,significantothersandtoGodcorrespondwith
Schnell’s(2009)conceptofexistentialmeaningmakingandReed’s(1992)
transcendentalandrelationalunderstandingofspirituality.
10.1.5ThePowerofConsolingpresence
Althoughthenursesexperiencedthattheymanagedtoconsoletheirpatientswhenthey
wereabletohelpthemfindmeaningintheirsuffering,theresultsalsoshowthatthis
wasnotalwayspossible.Thenursesexpressedthat:“Thereissuchathingaspointless
suffering!”andthattheysometimesjusthadtoacceptthat:“Thingsdon’talwayshavea
deepermeaning”(paperIIp.8).Inthesesituations,thenursesfeltthatconveying
consolationby“justbeingthere”tosharethepatient’ssufferingwasmoreimportant
thantryingtoresolvetheirspiritualandexistentialissues.Thenursesexperiencedthat
embracingthesilencetogetherwiththeirpatientscouldhaveapowerfulconsoling
effect,andtheyexpressedthatthisdemandedamentalshiftfromfocusingon“doing
somethingforthepatient”to“beingwiththepatient”(paperIp.3,paperIIp.8,paperIII
p.5).Thenursesexperiencedthattheyhadanimportantfunctionas“emotional
containers”whentheyjuststoodbytheirpatients,listeningandencouragingthemto
venttheirthoughtsandfeelingswhichcouldinvolvetears,griefandsorrowaswellas
angerandfrustration:“Itdoesn’tdoanyharmifpeoplestarttocry.Iusuallytellmy
61
patientsthattheydon’thavetofeelashamedoftheirtears.Tearsareonlymeltingice.”
(paperIIp.8)Thenursesalsopointedoutthatsomepatientscouldbetootiredtotalk
needingthenurse’sconsolingpresence.Eventuallytherewouldcomeapointintime
whenitwastoolateforwords,andinsomecaseswordslostallmeaningduetothe
brevityofthesituation:“Whentheyaresosickthattheyarevomitingtheirownfecal
matter,theonlythingyoucandoistobethere,holdingthem,comfortingthemand
warmingthem”.(paperIp.3)
Accordingtothenurses,whatpatientsneededmost,werenurseswhowerewillingto
endureandstandbytheirpatients,containingthepatients’emotionsandshowingthem
thattheywouldnotbeabandonedintheirtimeofneed(paperIp.3,paperIIp.8)“-just
beingtheresharingthepainandlettingthemtalk,ifthat’swhattheyneed,sometimes
that’sallyoucando”(paperIp.3).ThisissupportedbyRushtonet.al.(2009,p.407),
whodefinepresenceasthecapacityto“befullytherewithaqualityofattentionand
authenticitythatinformsrelationshipsandactions”.Accordingtothem(2009),modern
medicine’semphasison“curing,fixinganddoing”(whichmaynolongerbeappropriate
whenpeoplearedying)mustbebalancedwiththequalityofbeingpresentwiththose
whoaresuffering,andtheypointoutthatbeingpresentwiththedyingandbearing
witnesstotheirsufferingarehealingactsinthemselvesandareoften“enough”
(Rushtonetal.,2009).
10.1.6Consolationunderstoodasamoralresponsibility
AccordingtoNortvedt(1998),“toencounterapatient’spainandunderstandingthat
painassufferingistobestruckbytheother’sagonyasamoralreality”(Nortvedt,1998,
p.387).Hence,Nortvedt(1998)maintainsthatnurseshaveamoralresponsibilitytobe
answerableforthepatients’condition,pain,sufferingandvulnerability.Following
Nortvedt(1998),itcanbearguedthatnurseshavearesponsibilitytoconvey
consolationasameanstoeasetheirpatients’spiritualandexistentialsuffering.
ThiswillbeexplicatedinlightoftheNorwegiannursingphilosopherKariMartinsen’s
philosophyofcare(Martinsen,1993,2000,2006)andtheDanishphilosopherand
theologianK.E.Løgstrup’srelationalethics(Lindseth,1992,pp.102-103),withspecial
62
referenceto“TheEthicalDemand”(Løgstrup,1956,1997)1.Thesethinkerswere
chosen,becausetheirrelationalperspectivesareconsistentwiththenurses’emphasis
ontherelationaldimensionofconsolation.Martinsen(1993,2000,2006)anchorsher
philosophyofcareinLøgstrup’sideasabout“theethicaldemand”(Løgstrup,1997)and
thesovereignexpressionsoflife(Løgstrup,2007)2.Astheseideasaredecisiveto
understandMartinsen’sphilosophyofcare(Delmar,2012)theywillbeoutlinedbriefly
beforeweproceedtoMartinsen’sthoughtsoncare.
“TheEthicalDemand”InTheEthicalDemand,Løgstrup(1997)maintainsthathumanbeingsarealways
alreadyentangledorintertwinedwith,andinthelifeofothers,andthatthisisabasic
ontologicalfactofhumanexistence,whichispriortoourconstitutionasindividuals.For
Løgstrup(1997),toexistashumanbeingsistoexistwithothers.Althoughwemaytend
toviewanotherperson’sworldasseparatefromourown,Løgstruppointsoutthatthis
isnotso.Onthecontrary:“Weareeachother’sworldandeachother’sdestiny”
(Løgstrup,1997,p.16)andLøgstrupisveryclearabouttheconsequencesofthismutual
entanglement.Forhim,theethicaldemandisimplied“bytheveryfactthataperson
belongstotheworldinwhichtheotherpersonholdssomethingofthatperson’slifein
hisorherhands,itisthereforeademandtotakecareofthatperson’slife”(Løgstrup,
1997,p.22).Theethicaldemandissilentinthatitisunspoken,unarticulatedand
merelyimplicit.Moreover,itisnotidenticalwithanydemandthattheotherpersonlays
onyou.Rather,itdemandsthatyou,tothebestofyourknowledge,dowhatwillbenefit
theotherperson.Inaddition,theethicaldemandisradical,unconditionalandabsolute,
whichmeansthatyoumustactexclusivelyandunselfishlyforthesakeoftheother,
regardlessofwhotheotherpersonisoryourrelationshiptothatperson(Løgstrup,
1997,pp.44-46).
1TheEthicalDemand(DenEtiskefordring),(Løgstrup,1956))wastranslatedfromtheoriginalDanishin1997.2Løgstrupelaboratedonhisconceptionof“thesovereignexpressionsoflife”inOpgørmedKierkegaard(Løgstrup,1968)andseverallaterethicalworks(vanKootenNiekerk,2007).MajorexcerptsfromtheseLøgstruptextsweretranslatedfromDanishinBeyondtheEthicalDemand(Løgstrup,2007).
63
Løgstrup(2007)maintainsthatweareboundtotheworldthroughsuchsovereign
expressionsoflifeastrust,opennessofspeech,hopeandmercy.Theseexpressionsbelong
totheverybasicsoflifeandtheyaregivenbylifeitself.Theyarerelationallylivedand
experiencedandtheyappearspontaneouslythroughourengagementswithone
another.Theymakeclaimsonusthroughourembeddednessintheworld,which
accordingtoLøgstrup(2007),subjectsustotheradicaldemandtocareforothers.As
waysoftakingcareofothers,thesovereignexpressionsoflifefulfilltheethicaldemand,
-beforethedemandhasevenmadeitselffelt.However,theethicaldemanddoesnot
makeitselffeltuntilthesovereignexpressionsoflifefail.Løgstrup(2007)statesthatthe
aspectofdutyandmoralitysetsinwhenwearetemptedtopassbyapersonwhoisin
needofourhelp.Whenthedrivetoperformanactofmercystemsfromourmoral
deliberations,ouractisreducedfromaspontaneouslifeexpressiontodutyforduty’s
sake.AsLøgstrup(2007,p.76)pointsout:“DutyenterswhenIamtryingtowriggleout
ofthesituation”.Assoonasopennessofspeech,hopeandmercyareinstrumentalized
theirspontaneityisbroken,whichdestroysthemandturnsthemintotheiropposite.If
mercyforinstance,ismadetoserveoneselforathirdparty,itisnolongermercybut
unmercifulness.Accordingly,thesovereignexpressionsoflifedefybeingmadeameans
toothergoalsthantheirown,whichistheimmediateservicetoone’sneighbor
(Løgstrup,2007).However,Løgstrupdoesnotprovidespecificrulesandguidelines
abouthowtoact.Rather,heassertsthatitisuptoeachindividualtousehisorher
insight,understandingandimaginationtofigureoutwhatthedemandrequires
(Løgstrup,1997,p.22).
DrawingonTheEthicalDemand(Løgstrup,1997),KariMartinsen’scaringphilosophy
(Martinsen,1993,2000,2006)takesonarelationalperspective(Delmar,2012).Using
Løgstrup’sterms(Løgstrup,1997,2007),Martinsen(1993,2000,2006)maintainsthat
thepatientunderstoodas“theother”,makesaphysicalimpressiononthenursethrough
hisorhersenses,whichgeneratesan“appealtolookaftertheother’slife”(Martinsen,
1993,p.19).AccordingtoMartinsen(1993,2000,2006),theappealtocareforthe
patientispoweredbytheethicaldemand(Løgstrup,1997),whichchallengesustoactin
thebestinterestof“theother”and“totakecareofthelifewhichtrusthasplacedinour
hands”(Løgstrup,1997,p.18).Beingmovedandtouchedbytheethicalappealfromthe
patientcompelsthenursetocareforhimorher.Accordingly,somethingaboutthe
64
patientmustappealtothenursetocreateanawarenessofthepatients’plight
(Martinsen,2000,2006).FollowingLøgstrup(Løgstrup,1997,2007)andMartinsen’s
(2000,2006)lineofthought,thenurses’spontaneousandcompassionatereactionsto
theirpatients’sufferingsuggestsanimplicitacceptanceoftheirmoralresponsibilityto
beanswerabletotheethicaldemand.AsMartinsen(2006,p.89)pointsout:“Perceiving
theotherisalreadybeinginanethicalrelationshiptohim.”
“TheMasteryofSeeing”
However,Martinsen(2000,p.17)alsonotesthatpeopleresponddifferentlytothe
sufferingofothers,andthathowtheyrespond,dependsentirelyontheirability“tosee”.
Accordingly,torespondtothepatients’ethicalappeal,Martinsen(2000,2006)asserts
thatnursesmustengagein“amasteryofseeing”.DrawingonLøgstrup’s(1971)
interpretationoftheparableabouttheGoodSamaritan,inTheNewTestament,Luke10:
25-37(Biblegateway,2011),Martinsen(2000,2006)reflectsonwhatitmeans,“tosee”.
IntheparableJesustellsaboutthereactionsofapriest,aLeviteandaSamaritanwhen
theydiscoveredahalfdeadwaylaidman.WhenthepriestandtheLevitesawthevictim,
theparablestatesthattheypassedhimbyontheothersideoftheroad,leavingthe
victimtohisowndevices:“ButaSamaritan,ashetraveled,camewherethemanwas;
andwhenhesawhim,hetookpityonhim”(Luke10:33,Biblegateway,2011).
Martinsen(2000,2006)emphasizesthatitwasthesightofthebatteredandbleeding
manthatgeneratedtheSamaritan’spityforhim.Comingovertothehalfdeadmanthe
Samaritandidnotstandthereanalyzingthesituation.Rather,thesightofthevictim’s
bodilypain,strucktheSamaritanwithagutwrenchingforce,whichpropelledhiminto
action.AsMartinsenpointsout:“TheopenandreceptiveeyesoftheSamaritanwere
struckbytheotherandthesituationhewasin,andwithpityandgreatpainhecoulddo
nothingbutnurseanddressthevictim’swounds”(Martinsen,2006,p.84).Martinsen
(2000,2006)emphasizesthattheSamaritan“sawwithhiswholebody”throughhis
sensesandwastouched.Accordingtoher,theSamaritan“sawwithhis“heart’seye”,
becausehisattentionwasdrawntothesufferingvictiminsteadofhisownpainful
feelingsandself-pity,whichwereinducedbythesightofthebatteredman(Martinsen,
2000,2006).Asthesituationbecamecleartohimheexperiencedanimmediate
65
identificationwiththewoundedman,-that“theother”likehimselfwasafellowhuman
being,whileatthesametime,“theother”wasalsodifferentfromhim,asavictimin
needofhelp.Martinsen(2000,2006)assertsthatliketheSamaritan,nursesmustalso
seethroughtheir“heart’seye”inordertoperceivetheethicalappealfromthepatient.
Thenursemustidentifywiththepatientasafellowhumanbeing,whileatthesametime
beingawareoftheirdifferentness,becausethepatientisinneedofthenurse’shelp.
Thusly,drawingonLøgstrup(1971,1997),Martinsen(2000,2006)assertsthat“Seeing
withtheheart’seye”impliesthattheprofessionalnursemustdaretobeahumanbeing
whoisopentohisorheremotions,whileatthesametimeholdingthembacktoallow
thepatienttoemergeinordertofindoutwhatserveshimbest.Martinsen(2000,2006)
maintainsthatdecidingontherightandbestcarerequiresa“friendlyinteraction”
betweenthenurses’spontaneous,sensory-basedandpre-reflectiveimpressionofthe
patient(wearetouchedandmovedbeforeweunderstand)andherreflective
understandingofthepatient’sillness,(whichisbasedonherprofessionaljudgment).
Whilethenurseisspontaneouslymovedtocareforthepatientbyherimmediate
impression,herreflectiveprofessionaljudgmentenableshertoactinthebestinterestof
thepatient.
Theresultsrevealthatitcouldbechallengingtogetagriponwhatreallytroubledthe
patient.Thenursesexperiencedthatthepatients’spiritualandexistentialsufferingwas
frequentlyembeddedandentangledinawebofpsychosocialandphysicalpain,which
madeitdifficulttosortout(paperIp.5,paperIIp.5,paperIIIp.5).Theytherefore
neededtousetheirclinicaljudgmenttoreflectontheirimmediateemotional
impressionstodecideontherightcourseofactiontoalleviatetheirpatients’suffering.
Thisisillustratedinthefollowingquotes:
Irememberonemanwhowasterriblyrestlessandanxious.Hecouldn’tsleep.NomatterhowIaskedhimhejustsaidthathehurtallover.Butitmusthavebeenmorethanthephysicalpainbecausehewasreceivingstronganalgesicsthroughtwodifferentpumps.Ioftenwonderifwecouldhavedonemoreforhim.Igottheimpressionofaverysadandlonelyman.(paperIp.5)

66
TherewasthisyoungwomanwithCancerofthepancreas.ShewasconstantlycravingMorphineandStesolid.Itseemedlikeshewishedtofloatawayfromallherexistentialpain,butitwasstillthere,underneaththedrugdaze.(paperIp.4)
Inthenurses’experience,such“neverending”requestsforextrapainmedicationor
tranquilizersusuallysuggestedsomekindofunderlyingdistresswhichneededfurther
lookingintoandtheyhadthereforedevelopedakeeneyetopickupimplicitclues,and
toexercisetheirclinicaljudgmenttofindthesourcesforthepatient’ssufferingandto
decideontheappropriateinterventions.
The“EthicalDemand”andthe“seductivepull”ofhelping
Asmentionedearlier,Løgstrup(1997)maintains,theethicaldemandand“thesovereign
expressionsoflifedefybeingmadeameanstoothergoalsthantheirown,whichisthe
immediateservicetoone’sneighbor.Thisimpliesthatanyothermotivationaldriveto
conveyconsolationwhetherovertorcovertcorruptsthesovereignexpressionsoflifein
thenurse-patientrelationship.However,itisimportanttonotethatthefamiliarityand
trustwhichdevelopsbetweenanurseandapatient,coupledwiththeseductivepullof
helping,thecomplexityofthepatient’streatmentneeds,andapotentiallackof
understandingofthepatient’sboundariescanthreatentheintegrityofthenurse’s
relationshipwithherpatients.Thismayultimatelyleadtoaviolationofpatient
autonomy(Peternelj-Taylor&Yonge,2003).Paradoxically,beingdeeplymovedand
touchedbyapatient’ssufferingmayputnursesatriskofoversteppingtheir
professionalboundaries(Peternelj-Taylor&Yonge,2003).Martinsen(2000,2006)
takesthisintoconsiderationinhercrucialdistinctionbetween“emotionality”and
“seeingemotions”.AccordingtoMartinsen(2000,2006)whenanurseisstrickenand
stuckin“emotionality”thenursecirclesaroundherownneedsandemotions,“and
limitstheothertobeingdrawnintoherownhorizon”,whereasintheperceptive,
“seeingemotions”thenursecentersherattentiononthepatient’sexperienceof
sufferingbecausethepatientisperceivedas“theother”whichconcernsandappealsto
thenurse(Martinsen,2006,pp.74-75).Inlightof“theethicaldemand”(Løgstrup,
1997),thisimpliesthatthepatientmustbemetwhereheorsheisspirituallyand
existentiallysituatedatthemoment.
67
Itisthereforeimportanttokeepinmindthatthereexistsapowerdifferentialbetween
thenurseandthepatient,whichcannotbeoverlooked.Byitsverynaturethe
therapeuticnurse-patientrelationshipisasymmetrical.Thepatientbyvirtueofneeding
helpisautomaticallyplacedinapositionofvulnerability;whilethenurseontheother
handassumesapositionofpowerthroughtheroleofthehelper(Martinsen,2000,
2006;Peternelj-Taylor&Yonge,2003).Peternejl-TaylorandYonge(2003)pointout
thatnursesembracemanyrolesintheirpersonalandprofessionallives,andare
involvedin“thedanceofrelationships”.Ifnursesforgetwhich“dancetheyaredancing”
orwhichroletheyareassuming,theirownneedscanbecomemostimportanttothe
relationship.Henceforth,thereisaneedforcautionandethicalawareness,inorderto
avoidintrusivenessandviolationofpatientautonomy(Peternelj-Taylor&Yonge,2003).
Thisisechoedintheresultsofthestudy,whichshowthatthenursesreflectedontheir
ethicalchallengesrelatedtoencouragingpatientstosharetheirsuffering.Whilethe
nursesexperiencedthatpatientswhowereabletoexpresstheirfeelingsoftendied
morepeacefullythanthosewho“bottledeverythingup,”(paperIp.3,paperIIp.7),they
alsostressedthattheyhadtoputasidetheirownviewsandpersonalneedstoreachin
topatientswhowereunwillingorunabletosharetheirsuffering.Thenurses
emphasizedthattheywereprofessionallyandethicallyobligedtorespectthepatients’
choice.“Whoarewetojudgewhatisbestforthem”,theyreflected(paperIp.3)andthey
pointedoutthattherearenoeasyanswersbecauseeverypatientisdifferent(paperIp.
4).Itwasthereforecrucialtosensetheturningpoints,whenpatientsbecamereadyto
sharetheirsufferingandreceiveconsolation.Accordingtothenursesthisdemandeda
goodsenseoftiming,situationalunderstandingandtheabilityto“tuneinon”patients’
verbalandnonverbalcueswhilstperformingnursingcare(paperIp.5,paperIIp.5,
paperIIIp.7).
ThisresonateswithLøgstrup’s(1997,p.15)emphasisontuningintolistento“thenote,
whichisstruck”.AccordingtoLøgstrup(1997)thisisessentialineveryconversation,
becausewedeliverourselvesoverintothehandofanotherinthespeechrelationship,
whichdemandsbasictrust:“Thatallspeechtakesplaceinsuchfundamentaltrustis
evidentinthefactthatthemostcasualcommenttakesonafalsenoteifonebelievesthat
68
itisnotacceptedinthesensethatisintended”.(Løgstrup,1997,p.15)Thusly,ifanurse
ignoresordoesnothearthenoteinwhatthepatientsays,thenthatnurseisatriskof
violatingherpatient’sintegrity,whichinturnwillviolatethepatients’basictrustinher.
InspiredbyLøgstrup(1997),Martinsen(2006,p.60)assertsthat“thetone”3pointstoa
commonworldandprovidesacontextofinterpretationforwhatisgoingoninthe
situation,andsheemphasizesthatthenurseandthepatienttogethermustfind“the
tone”inthesituationwhichenablesbothparties,-nurseandpatient–eachintheir
ownway,todaretocomeforth.
10.2VulnerabilityandhelplessnessWhenthenurseswereaskedtonarrateabouttheirexperienceswithspiritualand
existentialcare,theirconsolationnarrativesevolvedaroundtheireffortstohelptheir
patientstofindpeaceandharmonyduringthefinalstagesofdying(paperIandII).The
resultsshowthatthenursesfelttheyhadbeensuccessfulwhentheywereableto
unburdensomeofthepatients’mostpressingsourcesofanxietyanddistress(paperII
p.12).Thisisillustratedinthethreeconsolationnarratives,insection10.1.2,which
showthatthenursesmanagedtohelptheirpatientstorestoretheirintra,interand
transpersonalrelationships,-theirrelationshipwith,self,lovedonesandwithGod(Reed,
1992).Regainingtheserelationshipsenabledthepatientstotranscendtheisolating
spiritualandexistentiallonelinessofdying.Assuch,theseconsolationnarrativescanbe
characterizedas“successful”consolationnarratives.
However,thenursesalsonarratedabout“unsuccessful”consolationexperiences,which
couldmakethemfeelprofessionallyinadequateandhelpless.Althoughthenurses
acknowledgedthatsufferinganddyingarefactsoflife,whichcannotbecompletely
alleviated,theyfounditdifficulttoacceptthattheycouldnotalleviatetheirdying
patientsdistress(paperIp.6,paperII7-8).Thisishighlightedinthefollowingquote:
Ayoungcancerpatientanxiouslybattleddeathtillthebitterend.Allofusthoughtitwasterriblethewayhedied!Wereallytried,butnobodycouldhelphimfindpeace,becausehesimplyrefusedtodie!Wesatthereholdinghishand,listeningtohim.Buthewascompletelyinconsolable!Itwasvery,very
3(orinLøgstrup’s(1997)terms“thenote”)
69
challengingandfrustratingeventhoughweknowthatweprobablydidallwecould!(paperIIp.7)
Bearingwitnesstopatientswhocontinuedtoradiateanguish,protestanddespairin
spiteofthenurses’consolationeffortswasexperiencedasemotionallychallengingand
draining.The“unconsolablepatients”werelookeduponasproblematic,formingthe
focusofpeersupportanddebriefing(paperIp.6-7,paperIIp.7-8).Inaddition,the
nursesfounditchallengingtobearwitnesstothedyingpatients’sufferingbecauseit
exposedthemtotheirownlatentfearsofmortalityandvulnerability(paperIp.6,paper
IIp.8).Asonenursepointedout:”Youhavetocometotermswithyourownthoughts
andfeelingsaboutyourownvulnerabilitytoendureworkinghereovertime.It’sa
demandingjob!Notallnursesarecutouttocareforthedying”(paperIIp.8).
InpaperIIIthemobilehospicenurseteachingteamstatedthatthecareworkers’main
obstacletoengageinspiritualandexistentialcarewastheirfearanduncertaintyof
facingdyingpatients’suffering(paperIIIp.4-6).Itseemsreasonabletoassumethat
likethenursesinpaperIandII,thecareworkers’reluctancetobewiththedying
stemmedfromtheirfearofrelatingtotheirownmortalityandvulnerability.
Whilevulnerabilityandsufferingareontologicalconditionsoflife,whichare
experiencedbyallhumans(Heidegger,1962;Turner&Dumas,2013),workingonthe
edgebetweenlifeanddeathposesdailypsychosocialchallengeswhichforcenursesand
careworkerstobecomeacutelyawareofthefragilityoflife(Najjar,Davis,Beck-Coon,&
Doebbeling,2009).Researchshowsthattheemotionalstressorsrelatedtocaringfor
patientswhoaresufferingand/ordying,placenursesandcareworkersinaunique
positionofvulnerability(Gjengedaletal.,2013).Recentresearchindicatesthat
emotionsarefeltinthebody(Back,Rushton,Kaszniak,&Halifax,2015).Thisresonates
withtheresultsinthisstudy,whichshowthatthenurses’spontaneousimpressionsof
theirpatients’sufferingcouldbesostrongthattheydescribeditintermsofphysical
sensationsintheirownbodies:
Wefeelthefearanddesperationthemomentweentertheroomeventhoughitisn’tours.IhaveenteredroomsIjusthavetogetoutof.Theatmosphereissoloadedwithsorrow.It’slikeaphysicalsensation.Thegriefjusthitsyoulikeawall!Howdoyoudealwiththat?(paperIp.5)

70
Icanbecomeveryoverwhelmedwhenpatientssharetheirinnermostthoughtsandfeelingsaboutlifeanddeath!Italmostknocksmeoutsometimes!(paperIIp.7)Theiremotionalanguishcanbesostrong.It’softenworsethanthephysicalpain!It’sliketheirheartsarebeingtornout!Howdoyourelievethatkindofpain?(paperIp.3)Youbecomequitefondofthepatients!Sometimestheyjustleapintoyourheart!(paperIp.6)
AccordingtoBenner&Wrubel(1989),citedinRaingruber&Kent(2003),bodily
responsesarestrongerwhenoneisdeeplyinvolvedwithandconcernedabouta
situation.Furthermore,Benner(2000a)pointsoutthattheempiricalresearchof
cognitivescientistsandneurobiologists(Damasio,1999;Lakoff&Johnson,1999;Rosch,
1981)revealsthatemotionsandembodiedfeelings,sensori-motorperceptionsand
skillsshaperationalthoughtandknowingandthatthesocial,sentient,sensori-motor
bodyplaysakeyroleinthoughtandaction.Hence,whenanursefeelsthatherpatientis
sufferingsomuchthat“itseemslikehisheartisbeingtornout”(paperIp.3)”andshe
becomessofondofthepatientthathe“leapsrightintoherheart”(paperIp.6)itseems
reasonablethatthepatients’painwillresonateinthenurse’s“ownheart”.Thiswas
especiallythecasewhenthenursescaredforpatientswhoremindedthemof
themselves:“Oneofmypatientshadalittlebaby.ThatwasreallytoughbecauseIama
mothermyself!”(paperIIp.7).
10.2.1Vulnerabilityandembodiedengagement
AfterabriefreturntoKariMartinsen’scaringphilosophy(Martinsen,2000,2006),
thenurses’physicalreactionstotheirpatients’sufferingwillbediscussedinlightof
Merleau-Ponty’s(1962)conceptofembodiedengagement.Asmentionedinsection
10.1.6,Martinsen(2000,2006)pointsoutthatinordertorespondtotheethicalappeal
fromthepatientthenursemustdareto“seewithherheart’seye”.Thisimpliesthatthe
nurseiswillingtotakeinthepatient’ssufferingthroughheropenandreceptiveeyes
andthatthiscompelshertoalleviatethepatients’suffering.Martinsen(2000,2006)
pointsoutthatfortheSamaritan,thebodilypainofthewaylaidmanstruckhimclose,
withoutdistance:“TheSamaritansawwithhisheart’seye,withhiswholebodywhich
71
waspainfullyopenandreceptive,turnedtowardstheother,attentivelytryingto
understandwiththoughtandwillaswell,whatisatstake”(Martinsen,2006,p.86).
AccordingtoMartinsen(2006,p.89):
Theopennessofperceptioncanbeterrifying.IntheeyesoftheSamaritanthepainoftheotherstruckintohisbody.Hestoodreceptiveandopenbutdidnotknowwhathewaslookingfor.Heonlyfeltit,thatthepainoftheotherconcernedhim.
BoththeSamaritan’sandthenurses’physicalreactionswhichstemmedfrom“seeingthe
sufferer”throughtheir“heart’seye”(Martinsen,2006)canbeunderstoodinlightof
Merleau-Ponty’s(1962)conceptofembodiedengagement.
Merleau-Ponty(1962),citedinRay(2006),conceptualizedthebodyascatching,
comprehendingandspontaneouslyrespondingtothecommunicationsofanother
person,whichhedefinedasembodiedengagement.AccordingtoMerleau-Ponty(1962),
citedinRay(2006),embodimentreflectshowweliveinandexperiencetheworld
throughourbodies,especiallythroughperception,emotion,language,movementin
space,timeandsexuality.Merleau-Ponty(1962),citedinRay(2006),maintainsthat
existencecanonlybeknowninandthroughthebodybecausethephenomenalbodyis
theonlymeansofbeingintheworld.Inthenursingcontextillness,pain,anddisability
areessentiallyconstitutedasembodiedexperiences(McDonald&McIntyre,2001).
Hence,tobeengagedwiththepatient,thenursemustbeengagedwiththepatient’s
existential,subjectiveandembodiedbeing:“Itisthepatient’sbodyasbothobjectand
subjectthatcallsoutforourministerings”(Hess,2003,p.145).
DrawingonLøgstrup(1997),Merleau-Ponty,Dreyfus,andDreyfus(1964)and
Martinsen(1997),Benner(2000a),maintainsthatgoodnursingpracticereliesonthe
humanbackdropofembodimentandourembodiedcapacitiestoexperience“the
spontaneoussovereignexpressionsoflife”(Løgstrup,1997),whichincludetrust,mercy,
opennessofspeech,andourcommonhumanconditionoffinitude,dependencyand
interdependence.InlightofLøgstrup(1997),she(2000a)alsopointsoutthatitisthe
immediateexperienceofembodiment,whichenablesthenursetorespond
spontaneouslywithmercy,withnoadditionalthoughtorcalculation.Nevertheless,
72
bearingwitnesstosufferingcanbeagonizing.AccordingtoMalone(2000),witnessing,-
orinMartinsen’s(2000,2006)termsseeingwith“theheart’seye”isqualitatively
distinctfrommerelooking;witnessingengagesthenurseasabeareroftruththatthe
sufferingpersoncannottell.Malone(2000)maintainsthatthisaspectofnursing
practiceislargelyunacknowledged,andthatthevulnerabilityitrequiresnursesto
experienceisrarelyaddressed.Twonotionsofvulnerabilitydominateinthenursing
literatureaccordingtoMalone(2000).One,whichmightbecalledapublichealthmodel
ofvulnerability,equatesvulnerabilitytothesusceptibilitytoparticularharmfulagents,
conditionsorcircumstances.Assuch,vulnerabilityissomethingtobeavoidedor
resisted.Theotherviewregardsvulnerabilityasthecommonconditionofallsentient
beings.Accordingtothisperspective,vulnerabilityisaconstantconditionofhuman
experience,acommonalitythatwesharebyvirtueofourembodiedexistenceandour
finitude.Assuchvulnerabilitygivesaccesstounderstandingaspectsofthepatients’
experiencesandisregardedpositively(Malone,2000).
Acknowledgingtheirownaswellastheirpatients’vulnerability,sharpensthenurses’
sensitivity,whichenablesthemtoopenthemselvestotheirpatient’ssituation(Norberg,
2001;Sarvimäki&Stenbock-Hult,2014).Asembodiedandvulnerablebeings,nurses
canexperiencetheirpatients’worldandengageintheillpersons’embodiedexperience
(Hess,2003).Thisenablesnursestounderstandmorethanwhatisbeingsaidand
observed,becausetheirimpressionofthepatients’conditionmanifestsitselfas
embodiedsensationsandphysicalresponsesbeforethenursescanunderstandthese
impressionsintellectually(Martinsen,2000,2006;Raingruber&Kent,2003).
10.2.2Compassionfatigue
Researchshowsthatbeingdeeplyengagedinpatients’sufferingoverprolongedperiods
oftimeexposeshealthcareproviderstovariousformsforoccupationalstress.(Backet
al.,2009;Hardiman&Simmonds,2013;Sabo,2008,2011a,2011b;Sandgren,Thulesius,
Fridlund,&Petersson,2006;Smartetal.,2014).Theconceptsofcompassionfatigue,
vicarioustraumatization,secondarytraumaticstressandburnouthavebeencompared
andusedinterchangeablywithintheliterature.Althoughtheseconcepts,have

73
significantsimilaritiestheyalsohavesignificantdifferences(Najjaretal.,2009;Smartet
al.,2014).
Forthepurposeofthisstudyitwillsufficetodiscusstheresultsinlightoftheconceptof
compassionfatiguewhichhasreceivedconsiderableattentionasapotentialformfor
occupationalstressduringrecentyears(Sabo,2011a).Compassionfatiguehasbeen
describedas“thenaturalconsequentbehaviorsandemotionsresultingfromknowing
aboutatraumatizingeventexperiencedbyasignificantother–theresultfromhelping
orwantingtohelpatraumatizedorsufferingperson”(Figley,1995,p.7),citedinSabo
(2011a).
AccordingtoSabo(2011a),severalstudiessuggestthatcompassionfatigueisconnected
tothetherapeuticrelationshipbetweenhealthcareprovidersandpatients,inthatthe
traumaticorsufferingexperienceofthepatienttriggersaresponseonmultiplelevelsin
thehealthcareprovider.Inparticular,anindividual’scapacityforempathyandabilityto
engage,orenterintoatherapeuticrelationshipisconsideredtobecentralto
compassionfatigue.Providingassistancetoindividualsexperiencingpain,sufferingor
trauma,theprofessionalmayexperienceadverseeffectssimilartotheirclients.
CoetzeeandKlopper(2010)claimthatcompassionfatigueisthefinalresultofa
progressiveandcumulativeprocess,whichiscausedbyprolonged,continuous,and
intensecontactwithpatients,theuseoftheselfandexposuretostress.Thephysical
effectsofcompassionfatigueincludeweariness,lossofstrength,reducedoutput,
diminishedperformance,lossofenduranceandincreasedphysicalcomplaint.The
emotionaleffectsincludelessenedenthusiasm,desensitization,diminishedability,
irritabilityandbeingemotionallyoverwhelmed.Thesocialeffectsincludeaninabilityto
aidandshareinthesufferingofpatients.Compassionfatigueissaidtooccurwhen
healthcareproviderscloselyidentifywiththeirpatientsandpersonallyabsorbthe
patients’traumaorpain.Itresultsfromgivinghighlevelsofenergyandcompassion
overaprolongedperiodoftime,particularlywhennursesdonotexperiencethepositive
outcomesofseeingpatientsgetbetter(Najjaretal.,2009).Inlightoftheafore-cited
literature,itseemsreasonablethatthenurseswereatriskofdevelopingcompassion
fatiguebecauseoftheirdeeprelationshipswithpatients,andtheiremotionaland
embodiedreactionstotheirpatients’suffering.
74
However,Sabo’s(2011a)studyoftheHSCTnurses’psychosocialhealth,foundthat
compassionatepresencingandinvolvementinthenurse-patientrelationshipmay
actuallyprovideapotentialbufferingagainsttheadverseeffectsofcaringforthe
seriouslyillanddying,whereasdistancingordisengagementthroughemotionalsurvival
strategiessuchasemotionalshielding,emotionalprocessingandemotionalpostponing
(Sandgrenetal.,2006)mayincreasetheriskofexperiencingcompassionfatigueand
othertypesofoccupationalstress.
AccordingtoSabo(2011a),thereexistsasignificantdifferencebetween“compassionate
presencing”and“emotionalsurvivalstrategies”.Wherecompassionatepresencereflects
thenotionof:“beingwith”,-alivingoutofthecaringnatureofnursingthrough
connectionsandrelationships,emotionalsurvivalgenerallyattendstostrategiesor
methodstoaddressaproblem,“inessenceto“avoidbeingwith”(Sabo,2011a,p.109).
Sabo(2011a)maintainsthatcompassionatepresenceconveysapositivetone,where
connectionorrelationshipscarrybenefits,whileemotionalsurvival(Sandgrenetal.,
2006),suggeststhatcaringmayleadtonegativeeffects,whichnursesmaypostponeby
employingvariousavoidancestrategies.However,Sabo(2011a)doesnotclaimthatthe
potentialriskforpsychological/emotionalpainasaresultofcaringrelationshipsis
non-existentifoneis“compassionatelypresent”rathershepointsoutthatcaringshould
beperceivedasadouble-edgedswordandthatthepotentialforadversepsychosocial
effectssuchascompassionfatiguemaybereducedifnursesareabletobe
compassionatelypresent.AccordingtoSabo’s(2011a)study,theHSCTnursesneededto
remainvigilantaboutwhosepainandsufferingwasbeingshared.Afailuretoestablish
clearboundariesbetweenthepersonalandprofessionalcouldplacethenurseatriskfor
adverseeffects.Sabo’s(2011a)resultsareconsistentwiththeresultsinthisthesis,
whichshowthatthenursesstrovetostrikeabalancebetweendisengagingandover-
engagingintheirpatients’suffering.Thisaspecthasbeenthoroughlydiscussedinpaper
IIp.10.
Sabo(2011a)pointsoutthat“compassionatepresence”isawayofbeingand
connecting,whichrequiresthenursetobeauthentic/genuine,openandavailableto
shareintheethical-moralmomentsoftheirpatientsandfamilies.Compassionate
presenceisareflectionofholisticnursingpracticeembracingthephysical,
75
psychological,emotionalandspiritualdomains.Thisbearscloseresemblancetothe
nurses’emphasisonsharingtheirpatients’sufferingthroughconsolingpresenceand
relationshipmaintainingactivities(paperIp.3-5andpaperIIp.6-7).
10.2.3Compassionsatisfaction
CoetzeeandKlopper’s(2010)distinctionbetween“compassionfatigue”and“compassion
satisfaction”supportsSabo’s(2011a)study.CoetzeeandKlopper(2010)pointoutthat
althoughnursesareexposedtotheexactsameriskfactorsofcontact,useoftheselfand
stress,somenursescontinuetoflourishinthesecircumstances.AccordingtoCoetzee
andKlopper(2010)nurseswhoexperiencecompassionsatisfactionareabletoconnect
withtheirpatientsregardlessofthecircumstances,whichleadstomeaningfuland
purposefulinteractionsbetweennursesandtheirpatients,whilstnurseswho
experiencecompassionfatigue,graduallydistanceandisolatethemselvesfromtheir
patients,whichresultsinthefactthatneitherthenurses’northepatient’sneedsare
fulfilled.
Sabo(2011a)andCoetzeeandKlopper‘s(2010)studiessuggestthatbeingdeeply
involvedinthenurse-patientrelationshipmayprovidemoreprotectionagainst
compassionfatiguethanusingemotionalsurvivalstrategies(Sandgrenetal.,2006)to
avoidthepainfulimpactofwitnessingdyingpatients’suffering.Whiletheprocessof
compassionfatigueiscumulativeandprogressive,movingfromdiscomforttostressand
finallytofatigue,theprocessofcompassionsatisfactionisrestorativeandcircular,
presentingasymbioticrelationshipbetweenthepatientandthenurse,aseachfinds
fulfillmentintheother(Coetzee&Klopper,2010).ItisinterestingtonotethatCoetzee
andKlopper’s(2010)definitionofcompassionsatisfactionresonateswithNorberget
al.’s(2001)claimthatnursesandpatientsmayexperiencemutualconsolationthrough
communionanddialog.
Whiletheresultsinthisstudyshowthatbearingwitnessto“unconsolable”patients’
sufferingcouldbeemotionallydrainingandchallenging(paperIIp.7),theyalsoreveal
thatthenursesfeltthatconveyingconsolationcouldbedeeplymeaningfuland
rewarding(paperIp.6,paperIIp.7).Bearingwitnesstoapatient’speacefulpassing

76
filledthemwithreverenceandawe:“Theroomwasveryquietandthepatientdied
calmlyandpeacefully.Itwasaveryspecialmoment”(paperIIp.7),andthenurses
expressedthattheyfelt“honoredandtouched”whenthepatientssharedtheirtrustand
chosetoconfideinthem(paperIIp.7).
InlightofSabo’s(2011a)andCoetzeeandKlopper’s(2010)studies,itisinterestingto
notethatnoneofthenursesmentionedthattheyhadconsideredchangingtheirlineof
workortakingaleaveofabsence,althoughtheycouldfeelemotionallydrainedand
helplesswhentheywereunabletoconsoletheirpatients.Takingthisintoconsideration
andthefactthatthenurses’workingexperienceinend-of-life-carerangedfromfiveto
thirty-fiveyears,itseemsreasonabletoassumethatthenursesexperiencedsufficient
compassionsatisfactionthroughtheirrelationshipswiththedyingthatitcounter-
balancedpossibleadverseeffectsofcompassionfatigue.Theseresults,togetherwiththe
aforementionedstudiesunderscorethevalueoftherelationaldimensioninconsolation
work(paperIp.3-5andpaperIIp.6-7).
10.3CompassionandCourage
10.3.1Compassion
AccordingtoRushtonetal.,(2013)compassionoptimallyinvolvesaqualityofpresence
thatconveysstabilityandresiliencewithabalancedconcernandheartfeltconnection,
butisnotdepletingoroverwhelmingtoeitherperson.Lazarus(1991)pointsoutthat
compassionimpliesfeelingpersonaldistressatthesufferingofanotherandwantingto
ameliorateit:“Thecorerelationalthemeforcompassion,therefore,isbeingmovedby
another’ssufferingandwantingtohelp”(Lazarus,1991,p.289).Thisresonateswiththe
results,whichshowthatthenursesweredeeplymovedandtouchedbytheirpatients
andyearnedtoconsolethem(paperIp.6,paperIIp.7).However,theresultsalso
indicatethatthenursesinpaperIandII,aswellasthecareworkersinpaperIII,could
beambivalentandreluctanttoaddresstheirpatients’spiritualandexistentialanguish
becauseitconfrontedthemwiththeirownvulnerabilityandlatentfearsofsufferingand
death(paperIp.7,paperIIp.8,paperIIIp.4-5).
77
ThesereactionsareunderstandableaccordingtoSasserandPuchalski(2010,p.3).They
(2010)pointoutthatcaringfordyingpatientsoverthecourseoftheirillnesstrajectory
exposeshealthcareproviderstogut-wrenchingstoriesofhumantragedy,whichovera
periodoftimemayevokeacertainamountof“accompaniphobia”thatmayleadto
avoidancestrategies(Sandgrenetal.,2006).AccordingtoSasserandPuchalski(2010)
thetendencytoavoidaddressingpatients’sufferingmaystemfromapossible
resonancewithunhealedwoundsdeepwithinthehealthcareproviders’ownsoulsthat
needsfurtherworkontheirpart.Thissuggeststhatnursesandcareworkersmust
possesscourageaswellascompassioninordertosuspendtheirpersonalreluctance
andanxietynomatterhowdisquietingthismightbeinordertoaccompanythedying
wheretheywanttogo,whentheywanttogothere,andwhetherthenursesandcare
workerswanttoornot(Sasser&Puchalski,2010).Takingthisintoconsideration,itis
interestingtonotethatthewordcompassionisderivedfromtheLatin“pati”and“cum”
whichliterallymeans,“tosufferwith”(Nouwen,McNeill,&Morrison,2008).Nouwen
et.al.(2008)pointoutthat:
Compassionasksustogowhereithurts,toenterintoplacesofpain,toshareinbrokenness,fear,confusionandanguish.Compassionchallengesustocryoutwiththoseinmisery,tomournwiththosewhoarelonely,toweepwiththoseintears.Compassionrequiresustobeweakwiththeweak,vulnerablewiththevulnerable,andpowerlesswiththepowerless.Compassionmeansfullimmersionintheconditionofbeinghuman.Whenwelookatcompassioninthisway,itbecomesclearthatsomethingmoreisinvolvedthanageneralkindnessortenderheartedness.(Nouwenetal.,2008,pp.3-4)
Nouwenetal.’s(2008)descriptionof“thechallengeofcompassion”resonatesdeeply
withthenurses’andcareworkers’challengesrelatedtoconveyingconsolation.While
Nouwenetal.(2008,p.4)statethat“Compassionmeansfullimmersioninthecondition
ofbeinghuman”,Norbergetal.(2001,p.549)maintainthatconsolationinvolvesbeing
willingto“sinkintosomebodyelse’shellandstaythere”.Beingincommunionwith
patientsinordertosharetheirsuffering(Norbergetal.,2001),-orinNouwenetal.’s
(2008)words:“goingwhereithurts”,demandsopenness,presenceandavailability,
whichcreatestrust.Whentherelationshipistrusting,thereisroomtouncoverthe
wound(thecauseofthesuffering),whichcalmsthesufferingpatientwhodarestolook
athisorherwounds,whilethenursewhomediatesconsolationby“walkingalongside”
showsthepatientthathisorherweakness,griefandexpressionsofpainareaccepted.
78
Intheshortperspective“uncoveringthewound”mayincreasethepainbecausethe
woundbecomesobvious,exposing“allthatisraggedandbroken”(Norbergetal.,2001,
p.548).
Uncertainty
Theresultsshowthatthenursesandcareworkersoftenfeltuncertainabouttheright
andbestthingtosayordotoalleviatetheirpatients’spiritualandexistentialsuffering.
Althoughinthefirstconsolationnarrative(“Breakingtheboil”paperIp.4)thenurse
thoughtthatsomepatientscould“needalittlepush”tohelpthemtranscenda
depressivespiralofexistentiallonelinessandalienation,thenursesexpressedthat
strikingtherightbalancebetweenmildpersuasionandacceptingthepatients’choices
to“bottleuptheirsuffering”couldbedifficult.Choosingtherightapproachwasfraught
withuncertainty,especiallyrelatedtoethicaldilemmasconcerningthepatients’
vulnerability,autonomyandtheasymmetricalpowerstructureinthenurse-patient
relationship.Thenursesexpressedthattheycouldneverbecertainaboutmakingthe
rightchoiceduetounpredictablechangesinthepatients’condition,andtheycouldalso
beuncertainabouthowtheirpatientsmightreacttowardstheirattemptstoconsole
them.Asthenursespointedout:“Eachpatientisdifferentandtherearenoeasy
answers.”(paperIp.4)
10.3.2Courage
Theseresultsindicatethattoconveyconsolationnursesandcareworkersmustbe
willingtoexposethemselvestotheirownaswellastheirpatients’vulnerability,to
accompanytheirpatientsintotheexperienceofuncertainty,andtogiveupcontroland
self-determination.Thisdemandscouragebecauseawindowisopenedtotheunknown
(Thorup,Rundqvist,Roberts,&Delmar,2012).Jordan(2003)definescourageas“the
capacitytoactmeaningfullyandwithintegrityinthefaceofacknowledgedvulnerability
“(Jordan,2003,p.2).AccordingtoJordan(2003),courageandvulnerabilityare
inextricablelinkedtogetherandtherecanbenorealcouragewherevulnerabilityand
feararedenied.Drawingonafeministperspective,Jordan(2003)pointsoutthatthe
traditionalmaleEurocentricmythofthecourageous,loneindividualwhodefies
79
vulnerabilityandfearobscuresthefactthatweallneedencouragementandconnection
throughoutourentirelives,andthathavingthecouragetomovebeyondcertaintyand
invulnerabilityenablesustoentertheworldoflearning,curiosityandlove.From
Jordan’s(2003)pointofview,courageisbuiltthroughvulnerabilityandconnectivity,
whereone’sopennesstobeingaffectedisessentialforconnection.Withoutopenness
peoplerelateinauthentically,adoptingrolesandcomingfromdistancedandprotected
places,whereaswhenwehavethecouragetobevulnerable,wearecapableofbeing
“moved”byourinternalaffectiveexperienceaswellasbeingaffectedbyotherpeople
(Jordan,2003),whichenablesustoexperiencecompassionforthesufferingofothers
(Lazarus,1991).Jordan’s(2003)understandingofcourageresonateswithLøgstrup’s
viewsontheinterdependentnatureofhumanexistenceandtheethicaldemand“totake
careofthelifewhichtrusthasplacedinourhands”(Løgstrup,1997,p.18),as
mentionedinsection10.1.6.AccordingtoDelmar(2004),citedinThorupetal.(2012),
enteringintoseriouspatientrelationshipsdemandscourage,becauseitrequiresa
willingnessfromthenursetoruntheriskofrejection.InlinewithNouwenetal.(2008)
andNorbergetal.(2001),Thorupetal.(2012)pointoutthattheoreticalandempirical
studiesshowthatthenurses’couragelaysinhisorherwillingnesstowalkalongsidethe
patientsontheirjourneytoovercometheirsuffering,nomatterwheretheroadleads.
Thisjourneyishighlyunpredictableandseemstorequirethewillingnessandabilityto
bearwitnesstothepatients’vulnerabilityandsuffering(Thorupetal.,2012).
Thorupetal.’sresearch(2012)revealsthatcouragebecomesevidentinsituations
wherenursesarecapableofcopinginanindeterminatesituation,ofstandingout“inthe
open”ofengagingwithandlisteningtovulnerableandsufferingpatients,insituations
thatexposethemtotheriskofrejection.Couragemanifestsitselfastheabilityand
willingnesstohelppatientstofacetheirownvulnerabilityandsuffering,tobearwitness
topatients’vulnerabilityandsufferingandtohavetheself-confidencetoargueforand
provideforprofessionalcare(Thorupetal.,2012).Thorupetal.’s(2012)work
resonateswiththisstudy,whichshowsthatthenursesandcareworkersneeded
couragetoovercometheirfearandemotionalambivalencetoconsolethedying,because
thisexposedthemtotheirownfearsofmortality,vulnerabilityandprofessional
helplessness.Aspreviouslymentionedcouragewasespeciallyneededinorderto
endurebeingwiththe“unconsolable”patients.(paperIIp.7)
80
AccordingtoThorupetal.(2012),courageisaprerequisiteinnerqualityandafirststep
towardstheexistentialcaringencounter.Thissupportsthestudyresults,whichshow
thathavingthecouragetoovercometheirfearsandreluctancetobewiththedyingwas
aprerequisiteforthenurses’willingnesstoengageincompassionateandconsoling
relationshipswiththeirpatients.Thorupetal.(2012)pointoutthatonthisexistential
level,infacingtheunpredictable,couragecontributestothenurturanceofpersonaland
professionaldevelopment.InlightofThorupetal.’s(2012)study,itisinterestingto
notethatthenursesinpaperIIexperiencedthattheiroldercolleaguesseemedtobe
morewillingtoengagethemselvesinthepatients’spiritualandexistentialsuffering
thantheyoungernurses,andtheyassumedthiswasbecausetheoldernurses’personal
andprofessionallifeexperienceshadmadethemmorematureandrobusttobearthe
weightofthepatients’distressthantheiryoungercolleagues(paperIIp.12).
(Seesection10.4.1,table1)
10.4Cancourageandcompassionbetaught?Thisstudyindicatesthatconsolingthesufferinganddyingisadeeplyrelationaland
compassionateactivity,whichrestsonnurses’andcareworkers’couragetoovercome
theirfearandreluctancetoaddresstheirdyingpatients’spiritualandexistential
distress.Thisraisesimportantpedagogicalquestionsabouthowtoteachandtrain
nursesandcareworkerstoconveyconsolation:
- Cancompassionandcouragebetaught?
- Whatarethepedagogicalimplicationsforteachingandtrainingnursesandcare
workerstoconveyconsolation?
Theseissueswillbediscussedinthefollowing:
81
10.4.1Cancompassionbetaught?Halifax(2012)pointsoutthatthefactorswhichfostercompassionarenotwell
understood.Accordingtoher(2012),whethercompassionisaninherentpersonal
quality,orifitcanbetaughtandlearnedisacentralquestionintheemergingfieldof
compassionresearch(Halifax,2012,2014;Sinclairetal.,2016;StanfordUniversity
SchoolofMedicine,2008).Theanswertothisquestionisimportantbecauseithas
pedagogicalimplicationsforteachingandtrainingcurrentandfuturenursesandcare
workerstoconveyconsolation.
Whiletheconventionaldescriptionofcompassionisbasedontwomaincomponents
fromtheaffectivedomain:theaffectivefeelingofcaringforthesuffererandthe
motivationtorelievesuffering(Lazarus,1991),Halifax(2012,2014)drawingonrecent
neuroscienceresearch,describescompassionasacontingentandemergentprocess,
whicharisesoutoftheinteractionbetweenanumberofinterdependentnon-
compassionelements,whichbelongtothecognitiveandbehavioraldomainsaswellas
theaffectivedomains.AccordingtoHalifax(2012,2014),thesenon-compassion
elements,(whichincludeattentionandaffect(theaffectivedomain),intentionand
insight(thecognitivedomain)andembodimentandengagement(thebehavioral
domain)),interactwitheachotherinacomplexandadaptivesystem.Asaconsequence,
onecannotdirectlytrainincompassionperse,accordingtoHalifax(2012,2014).
However,Halifax(2012,2014)pointsoutthatonecanindirectlysetthefieldforthe
emergenceofcompassionbytrainingtheindividualinsituationsandprocesseswhich
arerelatedtothenon-compassionelementsintheaffective,cognitiveandbehavioral
domains.Theconsolationprocesswhichemergedthroughthestudy,bearsclose
resemblancetothecontingentandemergentprocessbetweentheaffective,cognitive
andbehavioralnon-compassionelementswhicharedescribedinHalifax’s(2012)model
ofenactivecompassion.Assuch,conveyingconsolingcanbeunderstoodasaformfor
enactivecompassion(Halifax,2012).Thisisillustratedinfigure1:

82
Figure1: Conveying consolation through “enactive compassion” based on Halifax (2012)
AccordingtoHalifax’sresearch(2012,2014),itispossibletoindirectlyprimenurses’
andcareworkers’capacityforcompassionbydesigningteachingandtrainingschemes,
aimedatdevelopingnursingcompetencies,whichpertaintothetrainablenon-
compassionelements.Thefollowingtableprovidesasummaryoftheconsolation
challengesandcompetencies,whichwereidentifiedinthethreepapersandtheir
relationshiptoHalifax’s(2012,2014)“non-compassionelements”.
BehavioraldomainConsolingactions:
Respondingappropriatelytopatient'sverbalandnonverbalcues
Consolingthroughpresence,sharedsilenceandphysicaltouch
Consolingthroughspiritual,existentialandreligiousconversations
Alternatingskillfullybetweentalkinglisteningandbeingsilent
Cognitivdomain:Clinicaljudgementand
reflection-assesspatients'needstodecideonthebestcourseofactionandevaluate
outcomes
Affectivedomain:Sensningpatients'suffering
Embodiedreactionstopatients'suffering
Emotionalambivalencetoengageinpatients'sufferingMusteringcouragetobeopen
tothepatients'suffering
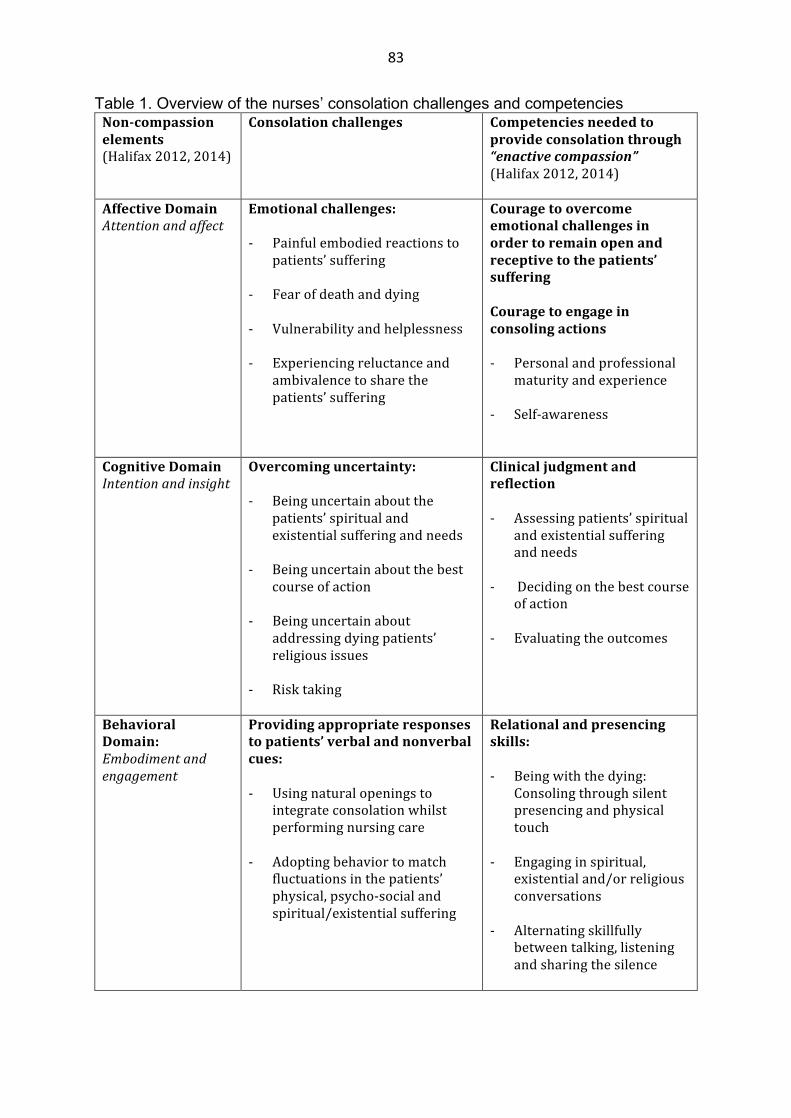
83
Table 1. Overview of the nurses’ consolation challenges and competencies Non-compassionelements(Halifax2012,2014)
Consolationchallenges Competenciesneededtoprovideconsolationthrough“enactivecompassion”(Halifax2012,2014)
AffectiveDomainAttentionandaffect
Emotionalchallenges:- Painfulembodiedreactionsto
patients’suffering
- Fearofdeathanddying- Vulnerabilityandhelplessness- Experiencingreluctanceand
ambivalencetosharethepatients’suffering
Couragetoovercomeemotionalchallengesinordertoremainopenandreceptivetothepatients’sufferingCouragetoengageinconsolingactions
- Personalandprofessional
maturityandexperience
- Self-awareness
CognitiveDomainIntentionandinsight
Overcominguncertainty:- Beinguncertainaboutthe
patients’spiritualandexistentialsufferingandneeds
- Beinguncertainaboutthebestcourseofaction
- Beinguncertainabout
addressingdyingpatients’religiousissues
- Risktaking
Clinicaljudgmentandreflection- Assessingpatients’spiritual
andexistentialsufferingandneeds
- Decidingonthebestcourseofaction
- Evaluatingtheoutcomes
BehavioralDomain:Embodimentandengagement
Providingappropriateresponsestopatients’verbalandnonverbalcues:
- Usingnaturalopeningsto
integrateconsolationwhilstperformingnursingcare
- Adoptingbehaviortomatchfluctuationsinthepatients’physical,psycho-socialandspiritual/existentialsuffering
Relationalandpresencingskills:- Beingwiththedying:
Consolingthroughsilentpresencingandphysicaltouch
- Engaginginspiritual,existentialand/orreligiousconversations
- Alternatingskillfullybetweentalking,listeningandsharingthesilence

84
10.4.2Cancouragebetaught?
Asmentionedinsection10.3.2Jordan(2003)describescourageastheabilitytobe
movedandaffectedbyothersandtoembraceandacceptvulnerabilityanduncertainty.
Thisposesanimportantpedagogicalquestion:Isitpossibletoteachandtrainnurses
andcareworkerstoovercometheirfearsandreluctancetowalkwiththedyingtoshare
theirsuffering(Norbergetal.,2001)?
WhileThorupetal.(2012)foundthatcourageisaprerequisiteinnerquality,which
contributestothenurturanceofpersonalandprofessionaldevelopment;theyalsopoint
outthatcourageisnotonlyanisolatedandinherentquality,becauseaspectsofvolition
arealsoinvolvedinnurses’courageousactions.Takingthisintoconsideration,itseems
reasonablethatthevolitionalaspectsofcouragemaybedeveloped.Thissuggeststhatit
ispossibletotrainone’sabilitytoactcourageously.Inthefollowingthiswillbe
discussedinlightofGoud’s(2005)studyconcerningthenatureanddevelopmentof
courage.Drawingonseveralpsychologicalschoolsandtheorists,whichemphasizethat
allorganicandhumanlifehasaninnatedrivetowardsgrowthandself-actualization
(Horney,1950;Jung&VonFranz,1968;Maslow,1968,1972;Maslow,Frager,Fadiman,
McReynolds,&Cox,1970;Rogers,1961,1980).Goud(2005,p.102)definescourageas
the“energizingcatalystforchoosinggrowthoversafetyneeds”.AccordingtoGould
(2005)agapiscreatedwhenevergrowthforcesencounterpowerfulsafetyforces
(fears)andthisgapmustbeleapedinorderforgrowthtoproceed.Gould(2005)points
outthatcourageallowsonetoeffectivelyactunderconditionsofdanger,fear,andrisk.
Withoutcourage,theindividualorgroupremainsstuckinexistingpatternsor
immobilizedinfear.
Inordertopresentaconceptualmodelofcourageandtodescribeguidelinesfor
developingcourageGoud(2005)examinedavarietyofdisciplinesfortheirviewson
courage.Thedisciplinesspannedfrommilitaryhistoryandresearch,variousschoolsof
psychology,literatureandphilosophy.Gould(2005)performedacontentanalysisofthe
divergentsourcesofliterature,whichyieldedthreeprimarydimensionsofcourage,
whichincluded:fear,appropriateactionandahigherpurpose.Gould(2005)foundthat
whiletherearewidevariationsamongstudentsofcourageastothekindsoffears,
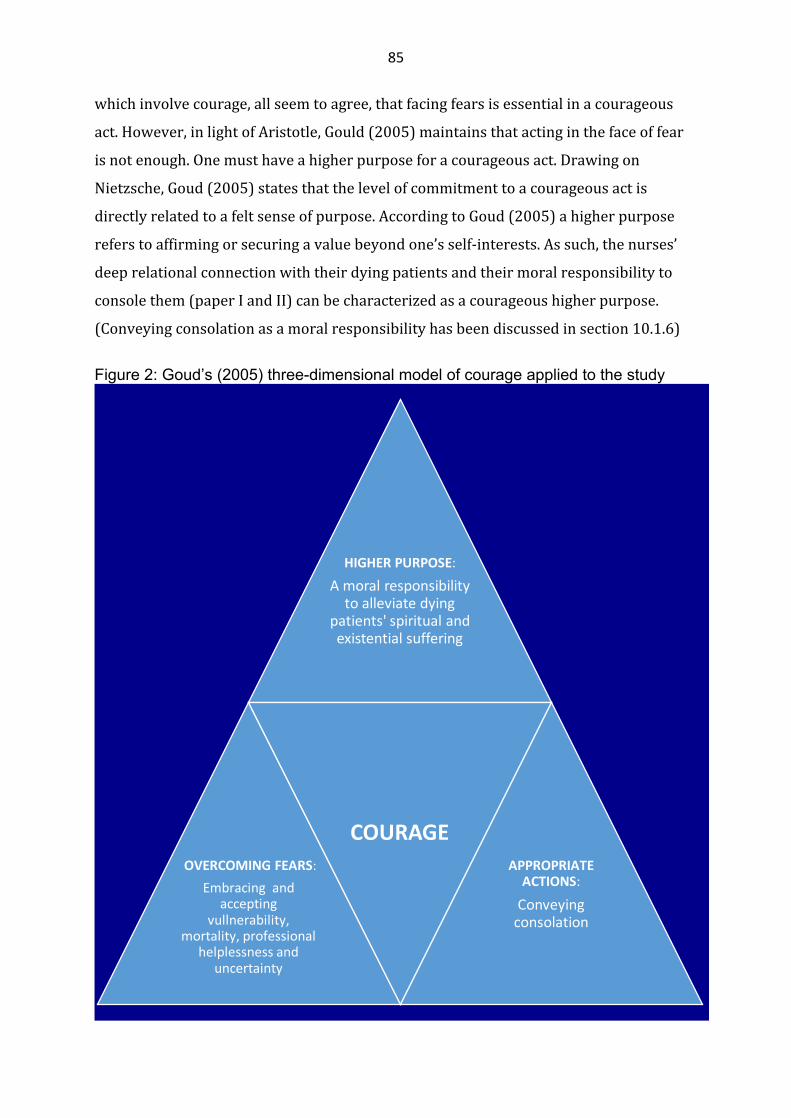
85
whichinvolvecourage,allseemtoagree,thatfacingfearsisessentialinacourageous
act.However,inlightofAristotle,Gould(2005)maintainsthatactinginthefaceoffear
isnotenough.Onemusthaveahigherpurposeforacourageousact.Drawingon
Nietzsche,Goud(2005)statesthatthelevelofcommitmenttoacourageousactis
directlyrelatedtoafeltsenseofpurpose.AccordingtoGoud(2005)ahigherpurpose
referstoaffirmingorsecuringavaluebeyondone’sself-interests.Assuch,thenurses’
deeprelationalconnectionwiththeirdyingpatientsandtheirmoralresponsibilityto
consolethem(paperIandII)canbecharacterizedasacourageoushigherpurpose.
(Conveyingconsolationasamoralresponsibilityhasbeendiscussedinsection10.1.6)
Figure 2: Goud’s (2005) three-dimensional model of courage applied to the study
HIGHERPURPOSE:Amoralresponsibilitytoalleviatedying
patients'spiritualandexistentialsuffering
OVERCOMINGFEARS:Embracingand
acceptingvullnerability,
mortality,professionalhelplessnessand
uncertainty
COURAGEAPPROPRIATEACTIONS:Conveyingconsolation

86
Asmentionedearlier,althoughstudies(Halifax,2012,2014;Thorupetal.,2012)
indicatethat,compassionandcourageseemtobeinherentpersonalqualities,these
studiesalsoindicatethatitmaybepossibletocultivatethesequalitiesthroughtraining.
Goud’s(2005)studywhich,drawsonRachman’sresearch(1978)supportsthese
results.AccordingtoRachman(1978),citedinGoud(2005),trainingindangerousjobs
suchasfirefighting,emphasizesgradualandgraduatedpracticeofthedangeroustasks.
Rachman(1978)concludedthat:“Courageousbehaviorisdeterminedpredominantlyby
thecombinationofcompetenceandconfidence,andbothofthesequalitiesare
strengthenedbyrepeatedandsuccessfulpractice.”(Rachman,1978,p.248),citedin
Goud(2005,p.111).Assuch,practicingforcourageisaprocessofmoral,psychological,
andphysical“toughening”accordingtoGoud(2005).Henceforth,“doingtherightthing”
inthefaceoffeardemandsagoodamountofconfidence,fortitudeanddiscipline.
Accordingly,developingtheabilitytotoleraterisksanduncertainty,meansaccepting
fearandanxietyaspartofthisprocess,ratherthansomethingtobeavoided(Goud,
2005).
DrawingonRachman(1978),Gould(2005)statesthatdevelopingconfidenceandself-
efficacy,observingrolemodelsandbolsteringasenseofpurposearepotentforcesfor
developingcourageandcounteractingfears.Developingconfidenceinone’scapabilities
isaprimaryforceincounteringfears,risksandthesafetyimpulse,whereself-efficacy,
whichisaspecificformofself-confidence,isofspecialimport.Self-efficacyisan
estimateofone’scapabilitiestohandlespecificchallengesandtasks.AccordingtoGoud
(2005)self-efficacyisanimportantdeterminantofhowmucheffortpeoplewillexert
andhowlongtheywillpersevereinthefaceofsignificantchallenges.Inlightof
Rachman’s(1978)summaryofstudiesaboutfearandcourage,Goud(2005)
recommendsrisktakingandcomfortzoneexpansionasameansforcourage
development.Theideaistoengagethelearneringradualrisktakingactivities,which
arejustbeyondtheindividual’scomfortzone(inthesamewayaparentcoaxesatoddler
totakeafewsteps).Attemptingtaskstoofarbeyondone’scapabilitiesusuallyresultsin
overwhelmingfailureandfears.Thefearfulpersonwillthen,quitereasonablyretreatto
safetyandbeextremelyhesitanttoriskanynewbehaviors.
87
Inadditiontofacilitatingcouragebuildingopportunitiesthroughactivities,which
involvegradualriskexposure,Goud(2005)recommendsobservationallearningor
modelingasanotherpowerfulmodalitytodevelopcourage.DrawingonBandura
(1986),Goud(2005)statesthatwatchingsomeonesimilartooneselfsucceedinatask
tendstoincreaseone’sconfidenceinperformingthesametasks(whilethereversalso
holdstrue).AccordingtoGoud(2005),beingexposedtodirectmodelsthat
demonstratecourageousbehaviorsincreasesthelikelihoodthatitwillencouragethe
samebehaviorsintheobserver.Goud’s(2005)researchsupportstheresultsinpaperIII
whichshowthatsituated,relationalandexperientialteachingapproachesintheclinical
contextseemtobeanefficientmeanstoteachandtraincareworkerstoprovide
spiritualandexistentialcareforthedying.Thiswillbeexplicatedinthefollowing:
ThemobilehospicenurseteachingteaminpaperIIIfrequentlyexperiencedthatthe
careworkersfeltfearfulandreluctantaboutaddressingtheirdyingpatients’spiritual
andexistentialsuffering.Theteachingteambelievedthatthecareworkers’fearof
exposingthemselvestotheirpatients’spiritualandexistentialsufferingstemmedfrom
personalinsecurityaswellasinsufficientcommunicationandlisteningskills(paperIII
p.5).Tostrengthenthecareworkers’courageandcompetency,themobileteaching
teamtransferredtheirpersonalspiritualandexistentialcareknowledgethrough
situatedbedsideteaching,whichinvolvedparticipatingactivelyinpatientcaretogether
withthecareworkers.Actingasrolemodelsandbyprovidingindividualsupervision
andfeedbackbefore,duringandafterpatientcare,theteamgraduallyencouragedthe
careworkerstoconductthespiritualandexistentialcareconversations,whichthey
wereafraidofinitiating.
Inthebeginning,theteammemberswouldactasrolemodels,(Goud,2005):“Sometimes
theyneedtohearthekindofquestionsIaskandseehowIrelatetothepatient.”(paper
IIIp.5)Theteachingteamgraduallyencouragedthecareworkerstostepoutoftheir
comfortzone(Goud,2005)toconductthepatientconversationsindependentlywhile
theteammemberwouldstayinthebackgroundtoprovidesupport.Astheteaching
teamobservedthatthecareworkersbecamemorecourageousandcompetent,they
graduallywithdrewtheirsupport,transferringtheresponsibilitytothecareworkers:
88
“Manyjustneedalittlepushandencouragementtotalkwiththepatientsalone,using
measaconversationpartnertohelpthemreflectonhowtheyhandledthesituation.”
(paperIIIp.5)Accordingtothemobilehospicenurseteachingteam,supervising,
supportingandencouragingthecareworkersthroughtheirchallengesoveraperiodof
timehadmadethemmorecourageoustobewiththedyingandtotalkwiththemabout
theirspiritualandexistentialsuffering.Drawingoncareworkerfeedbackandtheirown
observations,theteachingteamconsideredthatsituatedbedsideteachinghadprovento
beanimportanttool:”WhenIhaveaccompaniedthesamecareworkertothesame
patientsseveraltimesI’venoticedthattheyhavegraduallybecomebraverbecausethey
actuallydaretoasktheirpatientssomeofthedifficultquestions.”(paperIIIp.6)……”I
seethattheydaretoinvolvethemselvesmoreinthesesituations,exposingtheir
vulnerability.Iseethattheyhavebecomebraver.”(paperIIIp.6)
10.5Pedagogicalimplications
Asmentionedinsection10.4.1and10.4.2,studiesindicatethatitispossibletoprime
nurses’andcareworkers’courageandcompassiontoconveyconsolationthrough
training(Goud,2005;Halifax,2012,2014;Thorupetal.,2012)andthatthismight
increasetheirendurancetobewiththedying.(Seesection10.2.3)
Inthefollowing,thepedagogicalchallengesrelatedtoteachingandtrainingnursesand
careworkerstoconveyconsolationwillbediscussedinlightofeducationalnursing
research,whichdrawsontheAristotelianconceptofphronesis(Benner,1984,2000a,
2000b;Benner,Sutphen,Leonard,&Day,2010;Rowe&Broadie,2002)andsituated
learningtheory(Brown,Collins,&Duguid,1989;Gieselman,Stark,&Farruggia,2000;
Lave&Wenger,1991).
AccordingtoÖhlen(2001),Aristotleviewshumanactionasapracticalskillwhich
involvesthefollowingthreeknowledgeforms:episteme,(theoreticalorformal
knowledge),techne(hands-onskills)andphronesis(thepersonalabilitytotakeactionin
awiseandprudentmanner).Öhlen(2001)pointsoutthatallthreeknowledgeformsare
eachother’sprerequisites.Assuch,noneofthemaresufficientalone.Theabilitytoact
prudentlyandwiselytoalleviatesuffering(phronesis)presumestheoreticalknowledge
89
(episteme)aboutsufferingandalleviatingsufferingaswellashands-onnursingskills
(techne)toalleviatethatsufferingandviceversa(Öhlen,2001)
Thestudyrevealedthatconsolingthedyingwasacomplex,multidimensionaland
deeplypersonalandrelationalnursingchallengewhichdemandingclinicaljudgment
andreflectivepractice.Thisisillustratedinthethreepaperswhichshowthatthenurses
(paperIandII)andthehospicenurseteachingteam(paperIII)strovetointegrateand
mergedtheirtheoreticalandpracticalknowledgeintoaholisticefforttoconsoleand
easethespiritualandexistentialsufferingofthedying.(ThisisillustratedinFigure1
andTable1insection10.4.1.)
TheresultsshowthatboththenursesinpaperIandIIandthehospicenurseteaching
teaminpaperIII,demonstratedaformforspiritualandexistentialcare,whichis
consistentwithSwintonandPattison’s(2010)pragmaticandfunctionalapproachto
spiritualityandspiritualcare,whichhasbeendescribedinchapter4.2.Accordingto
SwintonandPattison(2010)inordertoprovidefunctionalandpragmaticspiritualand
existentialcare,nursesandcareworkersmusthavethecompetencytoidentifyand
respondeffectivelytotheparticularspiritualandexistentialqueststhattheyencounter,
withinwhateversituationtheyfindthemselvesin.SwintonandPattison(2010,p.235)
notethat:
whatiscalledforintermsofnurseeducationisthereforeflexibilityandconsciousnessraising.Thiswillmeanteachingnursesthesignificanceofspiritualityinwaysthatareflexibleandcontextuallyworkableandraisesthenurses’consciousnesstodimensionsoftheircaringpracticesthatareoftenhiddenorforgotten.
Hence,torisetothechallengeofconsolation,nursesandcareworkersareinneedof
phroneticknowledge(Öhlen,2001).Thiswillbeexplicatedinthefollowing:
DrawingonAristotle,Benner(2000a)pointsoutthatlearningtobeagoodpractitioner
requiresdevelopingthemoralimaginationandskillsofbeingagoodpractitioner.
AccordingtoBenner(2000a),Aristotlelabeledthekindofknowingwhichrequires
moralagency,discernmentandrelationshipasphronesis,incontrasttotechne,which
involvesknowledgeaboutmakingthingsorproducingoutcomesandshe(2000a)

90
emphasizesthatnursing,asapracticerequiresbothtechneandphronesisasdescribed
byAristotle.Benner(2000a)emphasizesthatwhiletechne,ortheactivityofproducing
outcomes,isgovernedbyameans-endrationality,phronesisbycontrast,islodgedina
practicewhichcannotrelystrictlyonameans-endrationalitybecauseone’sactsare
governedbyconcernfordoinggoodinparticularcircumstances,wherebeingin
relationshipanddiscerningparticularhumanactionsareatstakeandguideaction.
Benner(2004)emphasizesthatmeansandendsareinextricablyrelatedincaringforthe
ill.
AccordingtoBenner(2000a,2004)thenurseandthepatientbendandrespondtoeach
othersothathorizonsandtheworldareopenedandreconstitutedsothatnew
possibilitiesemerge.Healingandrecoveryofone’sembodiedrelationshiptotheworld
ismysterious.Itislivedratherthanmasteredandrequiresrelationship,opennessand
trust.(Benner’sviewpoints(2000a,2004)resonatewiththerelationalandhealing
dimensionsofconsolation,whichhavebeendiscussedinsections10.1.2and10.1.3.)
Hence,techniquealonecannotaddresstheinterpersonalandrelationalresponsibilities,
discernment,situatedpossibilitiesandchallengesthatnursesandcareworkers
encounterintheireffortstoconsolethevulnerablesufferinganddying.
Benner(2000a)notesthatthephroneticknowledgewhichexperiencednursespossess
canonlybetransferredtothelessexperiencedthroughsituatedexperientiallearningin
communitiesofpractitionerswhoforthesakeofgoodpracticecontinuetoliveoutand
improvepractice.Oneofthefeaturesoflearninginapracticecontextisthatexpertsare
abletoguidenovicesthroughthecomplexitiesofpractice(Benner,1984).Benner
(1984)emphasizesthatmuchclinicalknowhowissituationalandtacitandcanonlybe
demonstratedastheparticularsituationarises.Thevarietyandexceptionsinactual
clinicalpracticeeludetextbookdescriptionsbutgraduallyyieldtotheexperienced
nurse’sfundofpastsimilaranddissimilarsituations.Itisthisdemonstrationthatisso
essentialtothenovice(Benneretal.,2010).Benner(1984,2000a)andBenneretal.’s
(2010)viewpointsaresupportedbysituatedlearningtheorists,whomaintainthat
knowledgeisembeddedwithinthecontextinwhichitisusedandcannotbeseparated
fromtheactivity,contextandcultureofthatsituation(Gieselmanetal.,2000).
AccordingtoLaveandWenger(1991)situatedlearningiscentralforbecoming

91
proficientandtheystatethatlearninginpracticeisamatterofacculturation,ofjoininga
communityofpractice,ratherthantheapplicationofdecontextualizedskillsand
principles.
AccordingtoConeandGiske’s(2013)study,nursingstudentsneedtoseehowspiritual
carecanbepromotedinthefastpacedhospital-environmentaswellasotherclinical
settings,andtheypointoutthatmakingspiritualcareassessmentsandinterventions
morevisibleandexplicitinclinicalstudieswillpromotestudents’maturationandthus
improvetheirprofessionalgrowth.ConeandGiske(2013)foundthatthereisagreat
needfornursingstudentstoseenurseswhorole-modelassessment,spiritualcare
givinganddocumentation,andthey(2013)pointoutthatnursescanplayakeyrolein
providingsupportforstudentstostayindifficultorchallengingsituations.By
promotinganopenatmospherefornursingstudentsitiseasierforthemtoovercome
theirvulnerabilityandtosafeguardethicalissues.ConeandGiske(2013)pointoutthat
althoughtheimportanceofrolemodelingiswidelyreportedintheliteratureitisoften
missinginpractice.Thischallengesnurseeducatorstocollaboratewithnursestohelp
thembemoreexplicitinsharinghowtheyprovidespiritualcare.Ifnurseeducatorsare
notdirectlyinvolvedinclinicalsupervisionofstudentsitiscriticallyimportantforthem
toassistnursesandnursepreceptorstomodelspiritualcareassessmentand
interventionsandtodemonstratehowitisdiscussedanddocumentedasapartof
nursingresponsibilities(Cone&Giske,2013).ConeandGiske(2013)emphasizethat
thisisespeciallyimportantinaNorwegiancontextwerespiritualityandreligionare
regardedasveryprivateandpersonalareas(Botvar&Schmidt,2010;Stifoss-Hanssen,
1999;Stifoss-Hanssen&Kallenberg,1998;Ulland&DeMarinis,2014).
10.5.1Recommendations
Theresultsfromthisstudysuggeststhatnursingleaders(inspecialistcareaswellasin
homecareandnursinghomes)andnurseeducatorsshouldcollaboratetocreate
teachingandtrainingschemesbasedonsituatedexperientialandrelationalteaching
formats,inordertoenablecurrentandfuturenursesandcareworkerstoprovide
competentandcompassionatespiritualandexistentialcareforthedying.Thisis
supportedbysituatedlearningtheory(Brownetal.,1989;Gieselmanetal.,2000;Lave&

92
Wenger,1991),andeducationalnursingresearch(Benner,1984,2000a,2000b,2004;
Benneretal.,2010;Cone&Giske,2013),whichunderpintheimportanceofdeveloping
phroneticspiritualandexistentialcarecompetencybylearningfromexperienced
nursesincommunitiesofclinicalpractice(Lave&Wenger,1991).
Nevertheless,althoughthestudyshowsthatthenurses’maturityaswellastheir
personalbeliefsandprofessionalexperiencewereimportant(asillustratedinthe
consolationnarrativesinsection10.1.2),thestudyalsoshowsthatsometimesthiswas
notenough.Withtheexceptionofthetwonurseswhohadstudiedtheologypriorto
takingupnursingcareers,thenursessaidtheyhadmixedfeelingsabouttheirabilityto
provideexistentialandspiritualcarebecausetheyfeltinsecureanduncertainabout
providingreligiousconsolation(paperIp.4).Accordingtothenurses,theirdiscomfort
anduncertaintystemmedfromtheirownpersonalattitudestowardsreligion(paperI
p.4)astheydidnotconsiderthemselvestobereligiousor“veryChristian”asoneof
themputit(paperIIp.5.)andtheyalsoexpressedthattheydidnothaveenoughformal
knowledgeaboutreligion.(Seesection10.1.1)
Thissuggeststhatspiritualandexistentialcareneedstobe“moved”fromtheprivate
commitmentoftheindividualnurseandcareworkertoapublicunderstanding(Ødbehr,
2015).Practicaltrainingprogramsinspiritualandexistentialcareshould,(inaddition
toprovidingexperientiallearningopportunitiesthroughsituatedbedsideteaching),
introducenursesandcareworkerstothenatureandlexiconoflivedreligion,religious
perspectivesonsufferingandreligiousreasoning(Pesut,2016;Swinton&Pattison,
2010).Practicaltrainingprogramscouldalsoincludeinterdisciplinaryandcross
professionalcollaborationbetweennursingstaffandchaplains.(Ødbehr,2015).This
mightenhancenurses’andcareworkers’couragetorisetothechallengeofconsolation
insituationswherethecomplexitiesofspiritualityandreligioncomeintoplay:AsPesut
pointsout:“Thedegreetowhichpatientscontinuetobringreligiousperspectivesto
careisthedegreetowhichnursingneedstoconsiderthoseperspectives.”(Pesut,2016,
p.7)
93
Baldacchino(2011)constructedastudyunitinspiritualcareforqualifiednursesnamed
“SpiritualCopinginIllnessandcare”.Thestudyunitconsistedof4ECTSandemployeda
varietyofdidacticmethods,whichincludedlectures,patientcasestudies,smallgroup
discussionsandsharingclinicalexperiences,self-reflectiveexercisesonpersonal
spiritualityandnursingpractice.AccordingtoBaldacchino(2011),theevaluation
reportedthatthestudyunithadbeenbeneficialasthelearnershadtimetothink
criticallyabouttheirownspiritualityandtheircurrentclinicalpractice.Theevaluation
suggestedthatthenurses’increasedknowledgeaboutconceptsofspirituality,spiritual
distress,spiritualwellbeing,spiritualcopingandspiritualcareappearedtohelpthemto
seethepossibilityofmeetingpatients’needsthroughtheimplementationofholistic
careandtobecomearesourceofknowledgefortheircolleagues.However,Baldacchino
(2011)alsopointedoutthatinalong-termperspective,mentorshipisneededinorder
toenablenursestoputtheoryintopracticeandtosustaintheminpracticingwhatthey
havelearned.
Alessqualifiedworkforceincreasinglydominatesnursinghomesandhomecarenursing
atatimeofincreasingprevalenceofcomplexheathconcerns(Annearetal.,2014;
Colomboetal.,2011;Leclercetal.,2014;NorwegianMinistryofHealthandCare
Services,2012).Mobileexpertnurseteachingteamsinspiritualandexistentialcare,
(andotherrelevantfieldsofnursing,suchashospice,dementiaandgeriatriccare)may
beapedagogicallyeffectiveandpracticalmeanstoredressthewideninggapbetween
workforcequalityandthedemandforhighqualitycareinprimaryhealthcare(Annear
etal.,2014).However,whilethelevelofindividualnursingcompetencyisimportant,
onemustalsokeepinmindthatthequalityofthecarewhichisdeliveredalsorestson
institutionalvariables,suchasthegeneralworkplaceculture,philosophy,leadership
andorganizationofcare,includingtimeandstaffresources(Caseyetal.,2011).

94
11.Concludingremarks
Thestudyshowsthatconsolationisadeeplyrelationalpractice,andthatenteringinto
relationshipswiththesufferinganddyingdemandscourageandcompassion.Being
willingtoembraceandacceptone’sownaswellasthepatients’vulnerability,mortality
andhelplessnessrequirespersonalmaturityandenduranceaswellasclinical
competencyandprofessionaljudgment(phronesis).Thestudysuggeststhatnursesand
careworkersmayeasesomeofthedyingpatient’sexistentialandspiritualloneliness
throughthepowerofconsolingpresence.Whennothingelsecanbedone,bearing
witnessandsharingthepatients’sufferingmaybeconsolingactsinthemselves.Nurses
andcareworkersinend-of-lifecareconfrontintractablesuffering.Hence,theycannot
alwaysexpecttobesuccessfulintheireffortstoalleviatethespiritualandexistential
sufferingofthedying.Therefore,thestudyresults,whichindicatethatconsolationcan
beconveyedandsustainedthroughpresenceandrelatedness,areextremelyimportant.
Furtherempiricalresearch(qualitativeaswellasquantitative)isneededtouncover
hownursesprovidespiritualandexistentialcarefordyingpatientsineverydaypractice
andtodevisepractical,experientialandrelationaltoolsandcurriculatoteachandtrain
currentandfuturenursingstaff(nursesandcareworkers)toprovidecompetentand
compassionatespiritualandexistentialcareforthedying.Suchresearchisanimportant
andvaluableknowledgesupplementtotheoreticalstudiesinthisfield.
95
ReferencesAbbey,J.,Froggatt,K.A.,Parker,D.,&Abbey,B.(2006).Palliativecareinlong-termcare:
asysteminchange.InternationalJournalofOlderPeopleNursing,1(1),56-63.doi:10.1111/j.1748-3743.2006.00010.x
Annear,M.,Lea,E.,&Robinson,A.(2014).Arecareworkersappropriatementorsfornursingstudentsinresidentialagedcare?BMCNursing,13(1),44.
Appleton,J.V.(1995).Analysingqualitativeinterviewdata:addressingissuesofvalidityandreliability.JournalofAdvancedNursing,22(5),993-997.
Avis,M.,&Freshwater,D.(2006).Evidenceforpractice,epistemology,andcriticalreflection.NursingPhilosophy,7(4),216-224.
Bachner,Y.,O'Rourke,N.,&Carmel,S.(2011).FearofDeath,MortalityCommunication,andPsychologicalDistressAmongSecularandReligiouslyObservantFamilyCaregiversofTerminalCancerPatients.DeathStudies,35(2),163-187.doi:10.1080/07481187.2010.535390
Back,A.L.,Bauer-Wu,S.M.,Rushton,C.H.,&Halifax,J.(2009).Compassionatesilenceinthepatient-clinicianencounter:acontemplativeapproach.JournalofPalliativeMedicine,12(12),1113-1117.doi:10.1089/jpm.2009.0175
Back,A.L.,Rushton,C.H.,Kaszniak,A.W.,&Halifax,J.S.(2015).“WhyAreWeDoingThis?”:ClinicianHelplessnessintheFaceofSuffering.JournalofPalliativeMedicine,18(1),26-30.
Balboni,M.J.,Sullivan,A.,Amobi,A.,Phelps,A.C.,Gorman,D.P.,Zollfrank,A.,...Balboni,T.A.(2013).Whyisspiritualcareinfrequentattheendoflife?Spiritualcareperceptionsamongpatients,nurses,andphysiciansandtheroleoftraining.JournalofClinicalOncology,31(4),461-467.doi:10.1200/jco.2012.44.6443
Baldacchino,D.R.(2011).Teachingonspiritualcare:Theperceivedimpactonqualifiednurses.NurseEducationinPractice,11(1),47-53.
Bandura,A.(1986).Socialfoundationsofthoughtandaction:Asocialcognitivetheory:Prentice-Hall,Inc.
Belzile,J.A.,&Öberg,G.(2012).Wheretobegin?Grapplingwithhowtouseparticipantinteractioninfocusgroupdesign.QualitativeResearch,12(4),459-472.
Benner,P.(1984).Fromnovicetoexpert:excellenceandpowerinclinicalnursingpractice.MenloPark,Calif.:Addison-Wesley.
Benner,P.(2000a).Therolesofembodiment,emotionandlifeworldforrationalityandagencyinnursingpractice.NursingPhilosophy,1(1),5-1915p.
Benner,P.(2000b).Thewisdomofourpractice.AJNTheAmericanJournalofNursing,100(10),99-105.
Benner,P.(2004).UsingtheDreyfusmodelofskillacquisitiontodescribeandinterpretskillacquisitionandclinicaljudgmentinnursingpracticeandeducation.Bulletinofscience,technology&society,24(3),188-199.
Benner,P.,Sutphen,M.,Leonard,V.,&Day,L.(2010).Educatingnurses:acallforradicaltransformation.SanFrancisco,Calif.:Jossey-Bass.
Benner,P.,&Wrubel,J.(1989).Theprimacyofcaring:Stressandcopinginhealthandillness:Addison-Wesley/AddisonWesleyLongman.
Benzein,E.(1999).Tracesofhope.(PhD.thesis),UmeåUniversity,MedicalDissertations,UmeåUniversity(NewSeriesNo.636–ISSN0346-6612)
Biblegateway.(2011).TheNewTestament,NewInternationalVersion.Retrievedfromhttps://www.biblegateway.com/passage/?search=Luke+10%3A25-37
96
Bollig,G.,Rosland,J.H.,&Husby,B.(2013).AchievementandchallengesofpalliativecareinNorway.EuropeanJournalofPalliativeCare,20,256-259.
Bosma,H.,Apland,L.,&Kazanjian,A.(2010).Culturalconceptualizationsofhospicepalliativecare:moresimilaritiesthandifferences.PalliativeMedicine,24(5),510-522.doi:10.1177/0269216309351380
Boston,P.,Bruce,A.,&Schreiber,R.(2011).Existentialsufferinginthepalliativecaresetting:anintegratedliteraturereview.JournalofPainandSymptomManagement,41(3),604-618.
Boston,P.,&Mount,B.M.(2006).Thecaregiver'sperspectiveonexistentialandspiritualdistressinpalliativecare.JournalofPainandSymptomManagement,32(1),13-26.
Botvar,P.K.,&Schmidt,U.(Eds.).(2010).ReligionidagensNorge:mellomsekulariseringogsakralisering(ReligionincontemporaryNorway.Betweensecularizationandsacralization).Oslo:Universitetsforlaget
Brown,J.S.,Collins,A.,&Duguid,P.(1989).Situatedcognitionandthecultureoflearning.Educationalresearcher,18(1),32-42.
Bueckert,L.D.,&Schipani,D.S.(Eds.).(2006).SpiritualcaregivinginthehospitalWindowstochaplaincyministry.Kitchener,Ontario:PandoraPress.
Carlsen,B.,&Glenton,C.(2011).WhataboutN?Amethodologicalstudyofsample-sizereportinginfocusgroupstudies.BMCMedicalResearchMethodology,11(1),26.
Casey,D.,Murphy,K.,NiLeime,A.,Larkin,P.,Payne,S.,Froggatt,K.A.,&O’Shea,E.(2011).Dyingwell:factorsthatinfluencetheprovisionofgoodend-of-lifecareforolderpeopleinacuteandlong-staycaresettingsinIreland.JournalofClinicalNursing,20(13-14),1824-1833.
Cassell,E.J.(1991a).Thenatureofsufferingandthegoalsofmedicine:OxfordUniversityPress.
Cassell,E.J.(1991b).Recognizingsuffering.HastingsCenterReport,21(3),24-24.Cho,J.,&Trent,A.(2006).Validityinqualitativeresearchrevisited.QualitativeResearch,
6(3),319-340.Christensen,K.H.(2008).SpiritualcareperspectivesofDanishregisterednurses.
JournalofHolisticNursing,26(1),7-14.Clark,D.,&Seymour,J.(1999).Reflectionsonpalliativecare.BuckinghamPhiladelphia:
OpenUniversityPress.Coetzee,S.K.,&Klopper,H.C.(2010).Compassionfatiguewithinnursingpractice:A
conceptanalysis.Nursing&HealthSciences,12(2),235-243.Colombo,F.,Llena-Nozal,A.,Mercier,J.,&Tjadens,F.(2011).HelpWanted?:Providing
andPayingforLong-TermCare:OECDPublishing.Cone,P.H.,&Giske,T.(2013).Teachingspiritualcare–agroundedtheorystudyamong
undergraduatenursingeducators.JournalofClinicalNursing,22(13-14),1951-1960.
Costello,J.(2006).Dyingwell:nurses’experiencesof‘goodandbad’deathsinhospital.JournalofAdvancedNursing,54(5),594-601.
Cranz,G.(2000).TheAlexanderTechniqueintheworldofdesign:postureandthecommonchair.JournalofBodyworkandMovementTherapies,4(2),90-98.doi:http://dx.doi.org/10.1054/jbmt.1999.0162
Damasio,A.(1999).TheFeelingofWhatHappens,BodyandEmotionintheMakingofConsciousness.NewYork:Harcourt&BraceCo.
97
Dauenhauer,B.,&Pellauer,D.(2014).PaulRicoeur.TheStanfordEncyclopediaofPhilosophy.Summer2014.Retrievedfromhttp://plato.stanford.edu/archives/sum2014/entries/ricoeur/
Dehlholm-Lambertsen,B.,&Maunsbach,M.(1997).Qualitativemethodsinempiricalhealthresearch.III.Theindividualin-depthinterview.NordiskMedicin,112(3),94-98.
Delgado-Guay,M.O.,Hui,D.,Parsons,H.A.,Govan,K.,DelaCruz,M.,Thorney,S.,&Bruera,E.(2011).Spirituality,religiosity,andspiritualpaininadvancedcancerpatients.JournalofPainandSymptomManagement,41(6),986-994.
Delmar,C.(2004).DevelopmentofEthicalExpertise:AQuestionofCourage.InternationalJournalforHumanCaring,8(3).
Delmar,C.(2012).Theexcessesofcare:amatterofunderstandingtheasymmetryofpower.NursingPhilosophy,13(4),236-243.
DeMarinis,V.(2008).TheimpactofpostmodernizationonexistentialhealthinSweden:psychologyofreligion'sfunctioninexistentialpublichealthanalysis.ArchiveforthePsychologyofReligion/ArchivfürReligionspychologie,30(1),57-74.
DeMarinis,V.,Ulland,D.,&Karlsen,K.E.(2011).Philosophy’sroleforguidingtheoryandpracticeinclinicalcontextsgroundedinaculturalpsychiatryfocus:AcasestudyillustrationfromsouthernNorway.WorldCulturalPsychiatryResearchReview,6(1),47-56.
Devers,K.J.,&Frankel,R.M.(2000).PRACTICALADVICE,Studydesigninqualitativeresearch—2:Samplinganddatacollectionstrategies.Educationforhealth,13(2),263-271.
Eells,T.D.(1999).WhatDoWeKnowAboutMasterTherapists?TheJournalofPsychotherapyPracticeandResearch,8(4),314-317.
EuclidNetwork.(2012).RoundtableoninnovationandvalueinpalliativecareinEurope(Report).Retrievedfromhttp://www.euclidnetwork.eu/projects/current-projects/social-experimentation/roundtable-on-innovation-and-value-in-palliative-care-in-europe.html
Figley,C.R.(1995).Compassionfatigue:Copingwithsecondarytraumaticstressdisorderinthosewhotreatthetraumatized:Routledge.
Finlay,L.(2012).DebatingphenomenologicalmethodsHermeneuticphenomenologyineducation(pp.17-37):Springer.
Frankl,V.(1969).Thewilltomeaning:Principlesandapplicationoflogotherapy.World,NewYork.
Gadamer,H.-G.(2004).TruthandMethod(Second,RevisedEditioned.).LondonNewYork:Continuum.
Geanellos,R.(2000).ExploringRicoeur’shermeneutictheoryofinterpretationasamethodofanalysingresearchtexts.NursingInquiry,7(2),112-119.
Gieselman,J.A.,Stark,N.,&Farruggia,M.J.(2000).Implicationsofthesituatedlearningmodelforteachingandlearningnursingresearch.TheJournalofContinuingEducationinNursing,31(6),263-268.
Gjengedal,E.,Ekra,E.M.,Hol,H.,Kjelsvik,M.,Lykkeslet,E.,Michaelsen,R.,...Wogn-Henriksen,K.(2013).Vulnerabilityinhealthcare–reflectionsonencountersineverydaypractice.NursingPhilosophy,14(2),127-138.doi:10.1111/j.1466-769X.2012.00558.x
Golafshani,N.(2003).Understandingreliabilityandvalidityinqualitativeresearch.Thequalitativereport,8(4),597-606.
98
Goud,N.H.(2005).Courage:Itsnatureanddevelopment.TheJournalofHumanisticCounseling,EducationandDevelopment,44(1),102-116.
Graneheim,U.H.,&Lundman,B.(2004).Qualitativecontentanalysisinnursingresearch:concepts,proceduresandmeasurestoachievetrustworthiness.NurseEducationToday,24(2),105-112.
Groenvold,M.,Pedersen,C.,Jensen,C.,Faber,M.,&Johnsen,A.(2006).Kræftpatientensverden-enundersøgelseafhvaddanskekræftpatienterharbrugfor-resultater,vurderingerogforslag(Thecancerpatients'world-astudyofwhatDanishcancerpatientsneed).Retrievedfromhttp://forskningsbasen.deff.dk/Share.external?sp=Sdfb3a4b0-70eb-11dc-bee9-02004c4f4f50&sp=Sku
Gullestad,M.(1996).EverydayLifePhilosophers.Norway:Universitetsforlaget.Halcomb,E.J.,Gholizadeh,L.,DiGiacomo,M.,Phillips,J.,&Davidson,P.M.(2007).
Literaturereview:considerationsinundertakingfocusgroupresearchwithculturallyandlinguisticallydiversegroups.JournalofClinicalNursing,16(6),1000-1011.doi:10.1111/j.1365-2702.2006.01760.x
Halifax,J.(2012).Aheuristicmodelofenactivecompassion.CurrOpinSupportPalliatCare,6(2),228-235.
Halifax,J.(2014).GRACEfornurses:Cultivatingcompassioninnurse/patientinteractions.JournalofNursingEducationandPractice,4(1),121.
Hardiman,P.,&Simmonds,J.G.(2013).Spiritualwell-being,burnoutandtraumaincounsellorsandpsychotherapists.MentalHealth,Religion&Culture,16(10),1044-1055.
Harlos,M.(2010).Theterminalphase.InN.A.Christakis,Cherny,N.I(Ed.),Oxfordtextbookofpalliativemedicine.(Fourtheditioned.,pp.1549-1559).Oxford:OxfordUniversityPress.
Haug,S.H.K.(2015).”Theillnessexperiencesofolderpeoplewithincurablecancerinspecializedpalliativehealthcarecontexts.Aqualitativestudyinclinicalpsychologyofreligionoftheinteractionsbetweendailylivingandexistentialmeaning–making.”.(PhD,MFSchoolofTheology,OsloPhD),MFSchoolofTheology,Oslo,Oslo.
Haug,S.H.K.,Danbolt,L.J.,Kvigne,K.,&Demarinis,V.(2014).Howolderpeoplewithincurablecancerexperiencedailyliving:AqualitativestudyfromNorway.PalliativeandSupportiveCare,1-12.
Heidegger,M.(1962).Beingandtime(JohnMacquarrieandEdwardRobinson,Trans.).Oxford:BasilBlackwell.
Henoch,I.,&Danielson,E.(2009).Existentialconcernsamongpatientswithcancerandinterventionstomeetthem:anintegrativeliteraturereview.Psycho-Oncology,18(3),225-236.
Hess,J.D.(2003).Gadow'srelationalnarrative:anelaboration.NursingPhilosophy,4(2),137-148112p.
Hollinghurst,S.,Sharp,D.,Ballard,K.,Barnett,J.,Beattie,A.,Evans,M.,...Little,P.(2008).RandomisedcontrolledtrialofAlexandertechniquelessons,exercise,andmassage(ATEAM)forchronicandrecurrentbackpain:economicevaluation.BMJ,337.doi:10.1136/bmj.a2656
Holloway,M.,Adamson,S.,McSherry,W.,&Swinton,J.(2011).Spiritualcareattheendoflife:Asystematicreviewoftheliterature.DepartmentofHealth,London.
Horney,K.(1950).TheCollectedWorksofKarenHorney:Selfanalysis.Neurosisandhumangrowth(Vol.2):WWNorton.
99
Husserl,E.(1970).ThecrisisofEuropeansciencesandtranscendentalphenomenology:Anintroductiontophenomenologicalphilosophy(D.Carr,Trans.):Evanston,IL:NorthwesternUniversityPress.
Ilkjær,I.(2012).Ånde-nød:Enundersøgelseafeksistentielleogåndeligefænomenersbetydningforalvorligtsygepatientermedkronisklungelidelse.(Difficultiesinbreathing.Aninvestigationofsignificanceofexistentialandspiritualphenomenaforseriouslyillpatientswithchronicobstructivepulmonarydisease.).(Phd,DetTeologiskeFakultet,UniversitetetiKøbenhavn(UniversityofCopenhagen).).Retrievedfromhttp://curis.ku.dk/ws/files/63613346/Ingeborg_Ilkjaer_Aande_noed_til_CURIS.pdf
Ivic,S.(2009).Ricoeur’snarrativetheoryappliedtoscience.PhilosophicalPapersandReviews,1(3),044-051.
Jordan,J.V.(2003).Valuingvulnerability:Newdefinitionsofcourage.WorkinProgress,paperNo102,1-13.
Jordens,C.F.,&Little,M.(2004).‘Inthisscenario,Idothis,forthesereasons’:narrative,genreandethicalreasoningintheclinic.SocialScienceandMedicine,58(9),1635-1645.
Jung,C.G.,&VonFranz,M.-L.(1968).Manandhissymbols:Laurel.Kahn,D.L.,&Steeves,R.H.(1986).Theexperienceofsuffering:conceptualclarification
andtheoreticaldefinition.JournalofAdvancedNursing,11(6),623-631.Kalish,N.(2012).Evidence-basedspiritualcare:aliteraturereview.CurrOpinSupport
PalliatCare,6(2),242-246.doi:10.1097/SPC.0b013e328353811cKarlsson,M.,Friberg,F.,Wallengren,C.,&Öhlén,J.(2014).Meaningsofexistential
uncertaintyandcertaintyforpeoplediagnosedwithcancerandreceivingpalliativetreatment:alife-worldphenomenologicalstudy.BMCPalliativeCare,13(1),28.
Kitzinger,J.(1995).Qualitativeresearch.Introducingfocusgroups.BMJ,311(7000),299-302.
Klass,D.(1999).Thespirituallivesofbereavedparents:PsychologyPress.Klass,D.(2014).Grief,Consolation,andReligions:AConceptualFramework.OMEGA-
JournalofDeathandDying,69(1),1-18.doi:10.2190/OM.69.1.aKoenig,H.,King,D.,&Carson,V.B.(2012).Handbookofreligionandhealth:Oxford
universitypress.Kvale,S.,&Brinkmann,S.(2008).Interviews:Learningthecraftofqualitativeresearch
interviewing:SagePublications,Incorporated.laCour,P.(2008).Existentialandreligiousissueswhenadmittedtohospitalinasecular
society:Patternsofchange.MentalHealth,Religion&Culture,11(8),769-782.laCour,P.,&Hvidt,N.C.(2010).Researchonmeaning-makingandhealthinsecular
society:Secular,spiritualandreligiousexistentialorientations.SocialScienceandMedicine,71(7),1292-1299.
Lakoff,G.,&Johnson,M.(1999).Philosophyintheflesh:Theembodiedmindanditschallengetowesternthought:Basicbooks.
Lartey,E.Y.(1997).Inlivingcolour:aninterculturalapproachtopastoralcareandcounselling:Cassell.
Lave,J.,&Wenger,E.(1991).Situatedlearning:legitimateperipheralparticipation.Cambridge:CambridgeUniversityPress.
Lazarus,R.S.(1991).Emotionandadaptation.NewYork:OxfordUniversityPress.
100
Leclerc,B.S.,Lessard,S.,Bechennec,C.,LeGal,E.,Benoit,S.,&Bellerose,L.(2014).Attitudestowarddeath,dying,end-of-lifepalliativecare,andinterdisciplinarypracticeinlongtermcareworkers.JournaloftheAmericanMedicalDirectorsAssociation,15(3),207-213.doi:10.1016/j.jamda.2013.11.017
Lincoln,Y.S.,&Guba,E.G.(1985).Naturalisticinquiry.BeverlyHills,Calif.:Sage.Lindseth,A.(1992).Theroleofcaringinnursingethics.InG.Udén(Ed.),Quality
developmentinnursingcare.Frompracticetoscience(1ed.,pp.97-106).LinköpingUniversity,LinköpingSweden:LinköpingCollaborationCentreLCC.
Lindseth,A.(2015).BeingIllasanInevitableLifeTopicPossibilitesofPhilosophicalPracticeinHealthCareandPsychotherapy.InM.N.Weiss(Ed.),TheSocraticHandbook(Vol.Band9,pp.440).Wien,Österreich:LITVerlag.
Lindseth,A.,&Norberg,A.(2004).Aphenomenologicalhermeneuticalmethodforresearchinglivedexperience.ScandinavianJournalofCaringSciences,18(2),145-153.
Lundmark,M.(2006).AttitudestospiritualcareamongnursingstaffinaSwedishoncologyclinic.JournalofClinicalNursing,15(7),863-874.doi:10.1111/j.1365-2702.2006.01189.x
Løgstrup,K.E.(1956).DenEtiskeFordring(TheEthicalDemand)København:Gyldendal.Løgstrup,K.E.(1968).OpgørmedKierkegaard.København:Gyldendal.Løgstrup,K.E.(1971).Etiskebegreberogproblemer(Ethicalconceptsandproblems)
København:GyldendalskeBoghandel,NordiskforlagAS.Løgstrup,K.E.(1997).TheEthicalDemand(T.I.Jensen,Puckering,G.,Watkins,E.,
Trans.).NotreDame,Ill:UniversityofNotreDamePress.Løgstrup,K.E.(2007).BeyondtheEthicalDemand,withintroductionbyKeesvanKooten
Niekerk(SusanDewandHeidiFlegal,Trans.):UniversityofNotreDamePress,NotreDame,Indiana.
Malone,R.E.(2000).Dimensionsofvulnerabilityinemergencynurses'narratives.Advancesinnursingscience,23(1),1-11.
Malpas,J.(2015).Hans-GeorgGadamer.TheStanfordEncyclopediaofPhilosophyRetrievedfrom<http://plato.stanford.edu/archives/sum2015/entries/gadamer/>
Malterud,K.(2011).Kvalitativemetoderimedisinskforskning:eninnføring(Anintroductiontoqualitativemethodsinmedicalresearch).Oslo:Universitetsforl.
Martinsen,K.(1993).FraMarxtilLøgstrup.Ometikkogsanselighetisykepleien(FromMarxtoLøgstrup.Aboutethicsandsensitivityinnursing).TANOAS,Otta.
Martinsen,K.(1997).FromMarxtoLogstrup(Translationinprogress)(2ndedn.ed.).Oslo,Norway:Tano.
Martinsen,K.(2000).Øyetogkallet(TheEyeandtheCalling):Fagboklaget.Martinsen,K.(2006).Careandvulnerability:Akribe.Maslow,A.H.(1968).Towardapsychologyofbeing.NewYork:HarperandRow.Maslow,A.H.(1972).Thefartherreachesofhumannature:MauriceBassett.Maslow,A.H.,Frager,R.,Fadiman,J.,McReynolds,C.,&Cox,R.(1970).Motivationand
personality(Vol.2):Harper&RowNewYork.Masters,K.,&Hooker,S.(2013).Religion,spirituality,andhealth.InR.F.Paloutzian,&
Park.C.L(Ed.),Handbookofthepsychologyofreligionandspirituality(pp.519-539).NewYork,London:TheGuilfordPress.
McDonald,C.,&McIntyre,M.(2001).Reinstatingthemarginalizedbodyinnursingscience:epistemologicalprivilegeandthelivedlife.NursingPhilosophy,2(3),234-239.
101
McSherry,W.,&Jamieson,S.(2013).Thequalitativefindingsfromanonlinesurveyinvestigatingnurses'perceptionsofspiritualityandspiritualcare.JournalofClinicalNursing,22(21-22),3170-3182.doi:10.1111/jocn.12411
Merleau-Ponty,M.(1962).PhenomenologyofPerception[PhénoménologiedelaPerception](C.Smith,Trans.):Routledge&KeganPaul.
Merleau-Ponty,M.,Dreyfus,H.L.,&Dreyfus,P.A.(1964).Senseandnon-sense.Evanston,Ill.:NorthwesternUniversityPress.
Mishler,E.G.(1986).Researchinterviewing:contextandnarrative.Cambridge,Mass.:HarvardUniversityPress.
Morse,J.M.,Barrett,M.,Mayan,M.,Olson,K.,&Spiers,J.(2008).Verificationstrategiesforestablishingreliabilityandvalidityinqualitativeresearch.Internationaljournalofqualitativemethods,1(2),13-22.
Najjar,N.,Davis,L.W.,Beck-Coon,K.,&Doebbeling,C.C.(2009).Compassionfatigueareviewoftheresearchtodateandrelevancetocancer-careproviders.JournalofHealthPsychology,14(2),267-277.
Narayanasamy,A.(2014).TheChallengesofTeachingandLearningSpiritualityinNursing.JournalofNursingCare,3(189),2167-1168.1000189.
Noble,A.,&Jones,C.(2010).Gettingitright:oncologynurses'understandingofspirituality.InternationalJournalofPalliativeNursing,16(11),565-569.
Nolan,S.,Saltmarsh,P.,Leget,C.(2011).Spiritualcareinpalliativecare:workingtowardsanEAPCTaskForce.EJPC,18,86-89.
Norberg,A.(2001).ConsolingCareforPeoplewithAlzheimer'sDiseaseorAnotherDementiaintheAdvancedStage.Alzheimer'sCareToday,2(2),46-52.
Norberg,A.,Bergsten,M.,&Lundman,B.(2001).Amodelofconsolation.NursingEthics,8(6),544-553.
Nortvedt,P.(1998).Sensitivejudgement:aninquiryintothefoundationsofnursingethics.NursingEthics,5(5),385-386.
NorwegianDirectorateofHealth.(2015).Nasjonalthandlingsprogrammedretningslinjerforpalliasjonikreftomsorgen(Nationalactionprogramwithguidelinesforpalliativecancercare)Retrievedfromhttps://helsedirektoratet.no/retningslinjer/nasjonalt-handlingsprogram-med-retningslinjer-for-palliasjon-i-kreftomsorgen
NorwegianMinistryofHealthandCareServices.(2012).ReportNo10(2012-2013)totheStorting(Parliament).Goodquality-safeservicesQualityandpatientsafetyinhealthandcareservices.Oslo:FullversioninNorwegian:Stortingsmeldingnr.10(2012-2013)Godkvalitet-tryggetjenesterKvalitetogpasientsikkerhetihelseogomsorgstjenestenOslo:Helseogomsorgsdepartementet2012.Retrievedfromhttp://www.regjeringen.no/pages/38154897/PDFS/STM201220130010000DDDPDFS.pdf
Nouwen,H.,McNeill,D.,&Morrison,D.(2008).Compassion:areflectionontheChristianlife.London:Darton,LongmanandTodd.
NSD.(2016).DataProtectionOfficialforResearch.Retrievedfromhttp://www.nsd.uib.no/nsd/english/pvo.html
Onwuegbuzie,A.J.,&Leech,N.L.(2007).Validityandqualitativeresearch:Anoxymoron?Quality&Quantity,41(2),233-249.
Paley,J.(2008).Spiritualityandnursing:areductionistapproach.NursingPhilosophy,9(1),3-18.
Paloutzian,R.F.,&Park,C.L.(Eds.).(2013).Handbookofthepsychologyofreligionandspirituality.NewYorkLondon:GuilfordPress.
102
Pargament,K.I.(2013).ConversationswithEeyore:Spiritualityandthegenerationofhopeamongmentalhealthproviders.BulletinoftheMenningerClinic,77(4),395-412.
Park,C.L.(2013).RelgionandMeaning.InR.F.Paloutzian&C.L.Park(Eds.),Handbookofthepsychologyofreligionandspirituality:TheGuildfordPressNewYork.
Patton,M.Q.(1990).Qualitativeevaluationandresearchmethods:SAGEPublications,inc.
Patton,M.Q.(2002).Qualitativeresearch&evaluationmethods.ThousandOaks,Calif.:SagePublications.
Pesut,B.(2008a).Areplyto‘Spiritualityandnursing:areductionistapproach’byJohnPaley.NursingPhilosophy,9(2),131-137.
Pesut,B.(2008b).Spiritualityandspiritualcareinnursingfundamentalstextbooks.JournalofNursingEducation,47(4),167-173.
Pesut,B.(2016).Therebedragons:effectsofunexploredreligiononnurses’competenceinspiritualcare.NursingInquiry.
Pesut,B.,Fowler,M.,Taylor,E.J.,Reimer-Kirkham,S.,&Sawatzky,R.(2008).Conceptualisingspiritualityandreligionforhealthcare.JournalofClinicalNursing,17(21),2803-2810.doi:10.1111/j.1365-2702.2008.02344.x
Pesut,B.,Sawatzky,R.,Stajduhar,K.I.,McLeod,B.,Erbacker,L.,&Chan,E.K.(2014).Educatingnursesforpalliativecare:Ascopingreview.JournalofHospiceandPalliativeNursing,16(1),47-54.
Peternelj-Taylor,C.A.,&Yonge,O.(2003).ExploringBoundariesintheNurse-ClientRelationship:ProfessionalRolesandResponsibilities.PerspectivesinPsychiatricCare,39(2),55-66.
Polkinghorne,D.E.(1988).Narrativeknowingandthehumansciences:SunyPress.Pope,C.,Ziebland,S.,&Mays,N.(2000).Qualitativeresearchinhealthcare:analysing
qualitativedata.BMJ:BritishMedicalJournal,320(7227),114.Porter,S.E.,&Robinson,J.C.(2011).Hermeneutics:Anintroductiontointerpretive
theory:Wm.B.EerdmansPublishing.Puchalski,C.M.,Ferrell,B.,Virani,R.,Otis-Green,S.,Baird,P.,Bull,J.,...Sulmasy,D.
(2009).Improvingthequalityofspiritualcareasadimensionofpalliativecare:thereportoftheConsensusConference.JournalofPalliativeMedicine,12(10),885-904.doi:10.1089/jpm.2009.0142
Rachman,S.J.(1978).Fearandcourage:SanFrancisco:Freeman.Raingruber,B.,&Kent,M.(2003).Attendingtoembodiedresponses:Awaytoidentify
practice-basedandhumanmeaningsassociatedwithsecondarytrauma.QualitativeHealthResearch,13(4),449-468.
Ray,S.L.(2006).Embodimentandembodiedengagement:Centralconcernsforthenursingcareofcontemporarypeacekeeperssufferingfrompsychologicaltrauma.PerspectivesinPsychiatricCare,42(2),106-113.
Reed,P.G.(1992).Anemergingparadigmfortheinvestigationofspiritualityinnursing.ResearchinNursingandHealth,15(5),349-357.
Reimer-Kirkham,S.(2009).Livedreligion:implicationsfornursingethics.NursingEthics,16(4),406-417.doi:10.1177/0969733009104605
Ricoeur,P.(1976).Interpretationtheory:discourseandthesurplusofmeaning.FortWorth,Tex.:TexasChristianUniversityPress.
Ricoeur,P.(1981).Hermeneuticsandthehumansciences:Essaysonlanguage,actionandinterpretation(J.B.Thompson,Trans.J.B.ThompsonEd.):Cambridgeuniversitypress.
103
Ricoeur,P.(1984).Timeandnarrative.Chicago:UniversityofChicagoPress.Ricoeur,P.(1992).Oneselfasanother(Frenchoriginal1990,EditionsduSeuil).(English
translationbyKBlamey):UniversityofChicagoPress,ChicagoandLondon.Ricoeur,P.(1999).Eksistensoghermeneutikk(ExistenceandHermeneutics)(H.H.Ystad
Ed.):Aschehoug.Ricoeur,P.(2008).Fromtexttoaction:essaysinhermeneutics,II(K.Blamey&J.B.
Thompson,Trans.).London:Continuum.Riessman,C.K.(1993).Narrativeanalysis.NewburyPark,Calif.:Sage.Rogers,C.R.(1961).Onbecomingaperson:Atherapist'sviewofpsychology.Boston:
HoughtonMifflin.Rogers,C.R.(1980).Awayofbeing.Boston:HoughtonMifflin.Romoren,T.I.,Torjesen,D.O.,&Landmark,B.(2011).Promotingcoordinationin
Norwegianhealthcare.IntJIntegrCare,11(Spec10thAnniversaryEd),e127.Rosch,E.(1981).Prototypeclassificationandlogicalclassification:Thetwosystems.In
E.Schnolnick(Ed.),NewtrendsinCognitiveRepresentation:ChallengestoPiaget’stheory(pp.73-96):Hillsdale,NJ:Erbaum.
Rowe,C.,&Broadie,S.(2002).Nicomacheanethics:OxfordUniversityPress.Roxberg,Å.,Eriksson,K.,Rehnsfeldt,A.,&Fridlund,B.(2008).Themeaningof
consolationasexperiencedbynursesinahome-caresetting.JournalofClinicalNursing,17(8),1079-1087.
Rumbold,B.D.(2003).Caringforthespirit:lessonsfromworkingwiththedying.MedicalJournalofAustralia,179(6),S11.
Rushton,C.H.,Kaszniak,A.W.,&Halifax,J.(2013).Aframeworkforunderstandingmoraldistressamongpalliativecareclinicians.JournalofPalliativeMedicine,16(9),1074-1079.
Rushton,C.H.,Sellers,D.E.,Heller,K.S.,Spring,B.,Dossey,B.M.,&Halifax,J.(2009).Impactofacontemplativeend-of-lifetrainingprogram:Beingwithdying.PalliativeandSupportiveCare,7(04),405-414.
Sabo,B.M.(2008).Adversepsychosocialconsequences:Compassionfatigue,burnoutandvicarioustraumatization:Arenurseswhoprovidepalliativeandhematologicalcancercarevulnerable?IndianJournalofPalliativeCare,14(1),23.
Sabo,B.M.(2011a).Compassionatepresence:Themeaningofhematopoieticstemcelltransplantnursing.EuropeanJournalofOncologyNursing,15(2),103-111.doi:http://dx.doi.org/10.1016/j.ejon.2010.06.006
Sabo,B.M.(2011b)."ReflectingontheConceptofCompassionFatigue"TheOnlineJournalofIssuesinNursing,Vol.16(No.1).RetrievedfromTheOnlineJournalofIssuesinNursingwebsite:http://www.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Vol-16-2011/No1-Jan-2011/Concept-of-Compassion-Fatigue.html
Sandelowski,M.(1993).Rigororrigormortis:theproblemofrigorinqualitativeresearchrevisited.Advancesinnursingscience,16(2),1-8.
Sandelowski,M.,&Barroso,J.(2003).Classifyingthefindingsinqualitativestudies.QualitativeHealthResearch,13(7),905-923.
Sandgren,A.,Thulesius,H.,Fridlund,B.,&Petersson,K.(2006).Strivingforemotionalsurvivalinpalliativecancernursing.QualitativeHealthResearch,16(1),79-96.
Sarvimäki,A.,&Stenbock-Hult,B.(2014).Themeaningofvulnerabilitytoolderpersons.NursingEthics,0969733014564908.
104
Sasser,C.G.,&Puchalski,C.M.(2010).Thehumanisticclinician:traversingthescienceandartofhealthcare.JournalofPainandSymptomManagement,39(5),936-940.
Schei,E.(2006).Doctoringasleadership:thepowertoheal.PerspectivesinBiologyandMedicine,49(3),393-406.
Schnell,T.(2009).TheSourcesofMeaningandMeaninginLifeQuestionnaire(SoMe):Relationstodemographicsandwell-being.TheJournalofPositivePsychology,4(6),483-499.
Schnell,T.(2010).Existentialindifference:Anotherqualityofmeaninginlife.JournalofHumanisticPsychology,50(3),351-373.
Schnell,T.,&Keenan,W.J.(2011).Meaning-makinginanatheistworld.ArchiveforthePsychologyofReligion,33(1),55-78.
Seale,C.(1999).Qualityinqualitativeresearch.Qualitativeinquiry,5(4),465-478.Sinclair,S.,&Chochinov,H.M.(2012).Communicatingwithpatientsaboutexistential
andspiritualissues:SACR-Dwork.ProgressinPalliativeCare,20(2),72-78.Sinclair,S.,Torres,M.-B.,Raffin-Bouchal,S.,Hack,T.F.,McClement,S.,Hagen,N.A.,&
Chochinov,H.M.(2016).Compassiontraininginhealthcare:whatarepatients’perspectivesontraininghealthcareproviders?BMCMedicalEducation,16(1),1-10.doi:10.1186/s12909-016-0695-0
Smart,D.,English,A.,James,J.,Wilson,M.,Daratha,K.B.,Childers,B.,&Magera,C.(2014).Compassionfatigueandsatisfaction:Across-sectionalsurveyamongUShealthcareworkers.Nursing&HealthSciences,16(1),3-10.
Solvoll,B.-A.,&Lindseth,A.(2015).Theissueofbeingtouched.Medicine,HealthCareandPhilosophy,1-8.
StanfordUniversitySchoolofMedicine.(2008).Thecenterforcompassionandaltruismresearchandeducation.Retrievedfromhttp://ccare.stanford.edu/about/mission-vision/
StatistiskSentralbyrå(CentralBureauofStatisticsinNorway).(2015).Dennorskekirke(TheNorwegianChurch,2015).Retrievedfromhttps://www.ssb.no/kultur-og-fritid/statistikker/kirke_kostra/aar/2016-05-04
Steinhauser,K.E.,Christakis,N.A.,Clipp,E.C.,McNeilly,M.,McIntyre,L.,&Tulsky,J.A.(2000).Factorsconsideredimportantattheendoflifebypatients,family,physicians,andothercareproviders.JAMA,284(19),2476-2482.
Stifoss-Hanssen,H.(1999).Religionandspirituality:WhataEuropeanearhears.TheInternationalJournalforthePsychologyofReligion,9(1),25-33.
Stifoss-Hanssen,H.,&Kallenberg,K.(1998).Livssynoghelse.Teoretiskeogkliniskeperspektiver(ViewofLifeandHealth.Theoreticalandclinicalperspectives.Oslo:AdNotamGyldendal.
Strang,S.,Henoch,I.,Danielson,E.,Browall,M.,&Melin-Johansson,C.(2014).Communicationaboutexistentialissueswithpatientsclosetodeath—nurses'reflectionsoncontent,processandmeaning.Psycho-Oncology,23(5),562-568.
Strømskag,K.(2012).Ognåskaljegdø:HospicebevegelsenogpalliasjonenshistorieiNorge(AndnowIshalldie:ThehistoryofthehospicemovementandpalliativecareinNorway).Oslo,Norway:PaxforlagA/S.
Sulmasy,D.P.(2002).Abiopsychosocial-spiritualmodelforthecareofpatientsattheendoflife.Thegerontologist,42(suppl3),24-33.
Swinton,J.(2014).Spirituality-in-Healthcare:JustBecauseitMayBe‘MadeUp’DoesNotMeanThatitisNotRealandDoesNotMatter(Keynote5).JournalfortheStudyofSpirituality,4(2),162-173.
Swinton,J.,&Mowat,H.(2006).Practicaltheologyandqualitativeresearch:SCM.
105
Swinton,J.,&Pattison,S.(2010).Movingbeyondclarity:towardsathin,vague,andusefulunderstandingofspiritualityinnursingcare.NursingPhilosophy,11(4),226-237.
Sæteren,B.,Lindström,U.Å.,&Nåden,D.(2011).Latchingontolife:livingintheareaoftensionbetweenthepossibilityoflifeandthenecessityofdeath.JournalofClinicalNursing,20(5-6),811-818.
Söderberg,A.,Gilje,F.,&Norberg,A.(1999).Transformingdesolationintoconsolation:themeaningofbeinginsituationsofethicaldifficultyinintensivecare.NursingEthics,6(5),357-373.
Sørensen,T.(2012).EpidemiologicalStudiesofReligiosBehaviorsandHealthintheNord-TrøndelagHealthStudy(HUNT-3),Norway.(PhD,MFSchoolofTheologyPhD),MFSchoolofTheology,Oslo,Oslo.
Sørensen,T.,Lien,L.,Landheim,A.,&Danbolt,L.J.(2015).Meaning-Making,ReligiousnessandSpiritualityinReligiouslyFoundedSubstanceMisuseServices—AQualitativeStudyofStaffandPatients’Experiences.Religions,6(1),92-106.
Sørlie,V.(2001).Beinginethicallydifficultcaresituations:narrativeinterviewswithregisterednursesandphysicianswithininternalmedicine,oncologyandpaediatrics.(PhD,UmeåUniversity),DepartmentofNursing,UmeåUniversity,Umeå
Talseth,A.-G.,Gilje,F.,&Norberg,A.(2003).Strugglingtobecomereadyforconsolation:experiencesofsuicidalpatients.NursingEthics,10(6),614-623.
Tan,H.M.,Wilson,A.,&Olver,I.(2009).Ricoeur’stheoryofinterpretation:Aninstrumentfordatainterpretationinhermeneuticphenomenology.Internationaljournalofqualitativemethods,8(4),1-15.
Tan,H.M.,Wilson,A.,Olver,I.,&Barton,C.(2011).Theexperienceofpalliativepatientsandtheirfamiliesofafamilymeetingutilisedasaninstrumentforspiritualandpsychosocialcare:Aqualitativestudy.(Researcharticle)(Report).BMCPalliativeCare,10,7.
Thorup,C.B.,Rundqvist,E.,Roberts,C.,&Delmar,C.(2012).Careasamatterofcourage:vulnerability,sufferingandethicalformationinnursingcare.ScandinavianJournalofCaringSciences,26(3),427-435.
Torjuul,K.(2009).Livingwithethicaldilemmas:theethicalreasoningofsurgeonsandnursesinsurgicalunits.(PhD,UniversityofTromsøPhd),UIT(UniversityofTromsø),Tromsø,Norway.Retrievedfromhttp://munin.uit.no/bitstream/handle/10037/2468/thesis.pdf?sequence=3&isAllowed=y
Tornøe,K.A.(1996).Kanvitrøstehjertene?Hvordanmøtealvorligsykeogdøendepasientersåndeligebehov?(Canweconsolethehearts?Howtomeetcriticallyillanddyingpatients'spiritualneeds).Oslo:TanoAschehough.
Torskenæs,K.B.,&Kalfoss,M.H.(2013).TranslationandFocusGroupTestingoftheWHOQOLSpirituality,Religiousness,andPersonalBeliefsModuleinNorway.JournalofHolisticNursing,31(1),25-34.
Torskenæs,K.B.,Kalfoss,M.H.,&Sæteren,B.(2015).Meaninggiventospirituality,religiousnessandpersonalbeliefs:exploredbyasampleofaNorwegianpopulation.JournalofClinicalNursing.
Turner,B.S.,&Dumas,A.(2013).Vulnerability,diversityandscarcity:onuniversalrights.Medicine,HealthCare,andPhilosophy,16(4),663-670.doi:http://dx.doi.org/10.1007/s11019-013-9500-6
106
Udo,C.(2014).Theconceptandrelevanceofexistentialissuesinnursing.EuropeanJournalofOncologyNursing,18(4),347-354.doi:10.1016/j.ejon.2014.04.002
Ulland,D.,&DeMarinis,V.(2014).UnderstandingandworkingwithexistentialinformationinaNorwegianadolescentpsychiatrycontext:aneedandachallenge.MentalHealth,Religion&Culture,17(6),582-593.
Vaismoradi,M.,Turunen,H.,&Bondas,T.(2013).Contentanalysisandthematicanalysis:Implicationsforconductingaqualitativedescriptivestudy.Nursing&HealthSciences,15(3),398-405.
vanKootenNiekerk,K.Introduction.InK.E.Løgstrup(2007),BeyondTheEthicalDemand.UniversityofNotreDamePress:NotreDame,Indiana.
VanManen,M.(1990).Researchinglivedexperience:Humanscienceforanactionsensitivepedagogy:SunyPress.
VanManen,M.(2014).Phenomenologyofpractice:Meaning-givingmethodsinphenomenologicalresearchandwriting(Vol.13):LeftCoastPress.
Vandervelde,P.(2008).Thechallengeofthe‘suchasitwas’:Ricoeur’stheoryofnarratives.InD.Kaplan(Ed.),ReadingRicoeur(pp.141-162):SUNYPress.
Vivat,B.(2008).Measuresofspiritualissuesforpalliativecarepatients:aliteraturereview.PalliativeMedicine,22(7),859-868.doi:10.1177/0269216308095990
Webb,C.(2003).Editor'snote:Introductiontoguidelinesonreportingqualitativeresearch.JournalofAdvancedNursing,42(6),544-545.doi:10.1046/j.1365-2648.2003.02716.x
Webb,C.,&Kevern,J.(2001).Focusgroupsasaresearchmethod:acritiqueofsomeaspectsoftheiruseinnursingresearch.JournalofAdvancedNursing,33(6),798-805.
WHO.(1998).WHOQOLandspirituality,religiousnessandpersonalbeliefs(SRPB).WorldHealthOrganization.(2002).InnovativecareforchronicconditionsBuildingblocks
foractionGlobalReport.Retrievedfromhttp://www.who.int/chp/knowledge/publications/icccglobalreport.pdf
WorldMedicalAssociation.(2001).WorldMedicalAssociationDeclarationofHelsinki.Ethicalprinciplesformedicalresearchinvolvinghumansubjects.BulletinoftheWorldHealthOrganization,79(4),373.
Ødbehr,L.S.(2015).Spiritualcareindementianursing-Aqualitative,exploratorystudy.(PhD,FacultyofMedicine,DepartmentofNursingScience),UniversityofOslo,Oslo.
Ødbehr,L.S.,Kvigne,K.,Hauge,S.,&Danbolt,L.J.(2014).Nurses'andcareworkers'experiencesofspiritualneedsinresidentswithdementiainnursinghomes:aqualitativestudy.BMCNursing,13(1),12.
Öhlen,J.(2001).Practicalwisdom:competenciesrequiredinalleviatingsufferinginpalliativecare.JournalofPalliativeCare,18(4),293-299.
Aadland,E.(1997).Ogegserpådeg…Vitenskapsteoriogmetodeihelse-ogsosialfag(AndIlookatyou...PhilosophyofScienceandmethodsforHealthandSocialstudies)(Vol.2):TanoAschehoug.
Aadnanes,P.M.(2008).Gudforkvarmann:Kyrkjaogdennyereligiøsiteten(Godforeveryone:TheChurchandthenewreligiosity).Oslo:Universitetsforlaget.

107
PaperI-III

108
Appendix