Embed Size (px)
Citation preview

CHR VOICE the monthly CHR UPDATE
The Center for Human Reproduction
Clinical Care • Research • Education
NOVEMBER 2015
The main event in the field of reproductive endocrinology and infertility in the month of October is always the Annual Meeting of the American Society for Reproductive Medicine (ASRM), which this year took place in Baltimore, Maryland. As in recent years, CHR had quite a significant presence, with a good number of accepted abstracts and with CHR’s Senior Scientist and Director of Clinical ART, David H. Barad, MD, MS, formally invited as a participant in a debate on the usefulness of androgen supplementation in female infertility. His opponent was Nanette F. Santoro, MD, Professor and E. Stewart Taylor Chair of the Department of Obstetrics and Gynecology at the University of Colorado, who previously had been his successor as Division Head in Reproductive Endocrinology at Albert Einstein College of Medicine in New York City. Before a packed auditorium, Dr. Barad represented the pro and Dr. Santoro the con positions.
News from the Annual ASRM Meeting
Implantation, Still the Big Black Box in IVFIt is generally assumed that most IVF cycles fail because of embryo quality. Most research in IVF is, therefore, concentrated on improving embryo quality and selecting the best embryos for transfer. Common wisdom holds that only ca. 15% of IVF cycle failures are caused by implantation failure. The truth, however, is that we never know why an IVF cycle fails and nobody really knows how many cycles fail because of an embryo problem, and how many because the implantation process does not work correctly.
What we know about implantation is very limited. Mostly from animal models and artificial implantation models, it has become clear that the implanting embryo starts a “conversation” with the endometrium and, likely, the maternal immune system, while swimming in the endometrial cavity fluid for ca. 48 hours prior to implantation. This “conversation” is conducted via biological substances produced by both the embryo and the maternal host. The goal of the “conversation” is two-fold: First, to find a good implantation site (ca. 95% of implantation sites are in the fundal area of the uterus, which represents only a small portion of the endometrial surface) and, second, to reprogram the maternal immune system from immunological rejection to immunological tolerance. The second step is biologically very important because the implanting embryo is really “foreign” to the maternal immune system, as 50% of it is genetically paternal.
If a woman were to receive an organ transplant from her partner, she, likely, would violently reject it without appropriate anti-rejection treatments. Even with treatments, chances of acceptance of the graft would be poor if the organ donor was genetically not very similar. Yet, in a normal pregnancy, a woman “accepts” the implanting graft (i.e., embryo) without any signs of an immunological rejection taking place. Somehow, her immune system gets “reprogrammed” by this conversation between the implanting embryo and her immune system.
Malfunction of toleranceWe now understand that this “reprogramming” of the maternal immune system sometimes malfunctions. This frequently happens in women with hyperactive immune systems; for example, in presence of autoimmunity or if women are “hyper allergenic” (i.e., allergic to many different stimulants). In such women,
Continue reading ASRM NewsFurther evidence for inadequacy of PGS .....2Peculiar disappearance of closed-system embryo culture .....4
Also in this issue:International PGS study consortium & registry .....3New patent on egg donor screening .....3Updating abnormal embryo transfer policy .....3CHR in the media .....4In Focus: Images from the lab .....4CHR participates in Service to Veterans Program .....7
1
Continue reading on page 5

of the “new” PGS now offered by many IVF centers.
That human embryos have the ability to “self-correct” had become apparent by the time the earlier PGS was formally declared useless by most professional organizations in the field. What proponents of blastocyst stage embryo biopsy, however, overlooked was the fact that the mechanism that allows embryos to “self-correct” segregates abnormal cell lines away from the so-called inner cell mass (from which the embryo arises) into the trophectoderm (which becomes the placenta). It is the trophectoderm, as we repeatedly noted in these pages before, from which embryo biopsies are now taken with the “new” PGS, and this trophectoderm can be expected to be highly mosaic (see figure below).
And this is what Dr. Grifo and his co-workers now confirmed in an excellent presentation at ASRM.
Their and others’ observation of a high degree of mosaicism in trophectoderm basically confirms PGS as a “crapshoot,” with results depending on where a biopsy is taken from. If the biopsy is derived from a chromosomally normal part of the trophectoderm, the embryo will be designated as normal; if the biopsy comes from a chromosomally abnormal area of the segregated abnormal cell lines, the embryo will be declared abnormal, while the inner cell mass, from
Further evidence for the inadequacy of PGSAn oral presentation by CHR’s Medical Director and Chief Scientist, Norbert Gleicher, MD, also received great attention. Dr. Gleicher reported the delivery of 3 normal babies after the transfer of embryos, which after preimplantation genetic screening (PGS) in some of the leading national PGS laboratories, had been reported to be aneuploid (chromosomally abnormal), yet still resulted in normal births.
Such embryos are usually discarded. However, as readers of the VOICE will be aware, CHR has questioned the clinical utility of PGS for years. A year ago (10/27/14), CHR published a formal OPINION, in which we for the first time laid out the rationale for transferring such allegedly abnormal embryos. Two other New York IVF centers, Fertility Specialist In New York (Andrea Vidali, MD) and Braverman IVF & Reproductive Immunology (Jeffrey Braverman, MD) joined us in this practice, and contributed successful births to this report.
Dr. Gleicher’s lecture was described as one of the, if not the, most important presentations of the conference by many participants at this year’s ASRM meeting since it called into question the whole concept of PGS, which is rapidly expanding all around the world. Further evidence for the clinical inadequacy of PGS, paradoxically, came from one of the most fervent groups of supporters of PGS, our colleagues at New York’s Fertility Center of NYU Langone Medical Center, headed by James A. Grifo, MD, who reported an unexpectedly high rate of mosaicism in trophectoderm biopsies of embryos at blastocyst stage.
An embryo is mosaic if it contains more than one cell line, usually a mixture of chromosomally normal and abnormal cell lines. That human embryos frequently are mosaic has been known for many years. Indeed, mosaicism was by many considered a principal reason why the original introduction of PGS over 10 years ago failed after it was proven ineffective in improving IVF outcomes. At that time, proponents argued that the effects of mosaicism would play a much diminished role if embryo biopsy was moved from the original cleavage stage (day-3 after fertilization) to the blastocyst stage (days 5/6 after fertilization) since by that stage embryos would have had the chance to “self-correct.” Blastocyst stage embryo biopsy, therefor, has become a mainstay
The drawing demonstrates a day-5/6 blastocyst stage embryo with inner cell mass and trophoblast delineated. The area of trophoblast showing the 3 circles as potential areas of biopsy, represents the so-called trophectoderm. Because abnormal cell lines at early embryo stages are often segregated into the trophectoderm, biopsies from that region of the embryo often do not reflect the chromosomal status of the inner cell mass, from which the embryo arises, causing a so-called false-positive biopsy. Such embryos are usually discarded by IVF centers, not being aware that they would give rise to normal pregnancies.
Blastocyst-stage embryo
2
News from ASRM: Continued from Page 1
Continue reading on Page 4
Read about the failures of PGS: http://kaywa.me/Ny49f
Read the original OPINION: http://kaywa.me/1Apl1

3
Three Announcements around PGSAddendum to CHR OPINION #007, On the possibility of selectively transferring embryos, by preimplantation genetic diagnosis (PGD/PGS) determined to be chromosomally abnormal
We hereby expand from monosomies to trisomies the OPINION, originally expressed on October 27, 2014, that it is reasonable to offer embryo transfer to patients with appropriate informed consent who have no or too few euploid embryos for transfer after PGD/PGS.
This expansion of indication is based on a number of factors:
1. The recent recognition by CHR investigators that, likely, ca. 50% of blastocyst-stage embryos are mosaic (other investigators recently suggested a ca. 30% rate; Grifo et al., ASRM 2015);
2. This high rate of mosaicism does not permit reliable diagnosis of ploidy by trophectoderm biopsy even with most advanced diagnostic platforms;
3. The establishment of so far 3 known chromosomally normal pregnancies after transfer of aneuploid embryos at 3 different IVF centers (Gleicher et al, ASRM 2015);
4. Studies performed at CHR and one other center (Esfandiari et al., ESHRE 2014), which demonstrated very poor correlation between results reported from 2 reputable PGD/PGS laboratories;
5. Studies reported at another IVF center, which reported poor correlation between biopsies of trophectoderm and inner cell mass (Orvieto et al, Personal communication, reported at ASRM 2015);
6. Studies performed at CHR, which demonstrated very high outcome discrepancy between multiple biopsies of the same embryos.
CHR, therefore, concludes that the high prevalence of mosaicism in blastocyst-stage embryos renders PGS/PGD ineffective. Moreover, especially in women with few embryos, false positive embryo diagnoses will adversely affect pregnancy chances, unless such embryos are transferred.
International PGS Consortium Study GroupWe are pleased to announce the formation of the International PGS Consortium Study Group, which is open for membership to physicians and scientists interested in contributing to the better understanding of PGS in association with IVF. Membership is free. The purpose of the organization is the instant sharing of new information and collaborative research efforts. For further details, please contact the Secretariat at [email protected]. The only condition for membership is participation in below listed registry.
International PGS Registry for Transfer of Allegedly Aneuploid Embryos in IVFWe are pleased to announce the establishment of the International Registry for Transfer of Allegedly Aneuploid Embryos in IVF. Membership is open to all IVF programs worldwide, and is free. The only condition of membership is that every embryo transfer involving embryos, previously after PGS reported as aneuploid, will be registered within 1 week after transfer, and every pregnancy outcome will be reported. For further details, please contact the Secretariat at [email protected]. Membership in the International PGS Consortium Study Group is not a prerequisite for membership in the registry.
New Patent Involves Using FMR1 Gene to Screen Egg Donors
In October, CHR was awarded another patent by the U.S. Patent and Trademark Office (USPTO).
The patent describes an improved method of selecting egg donors with normal ovarian reserve who can be expected to produce a good number of eggs in an egg donation cycle. CHR’s research over the last 5-6 years have focused on the role of the FMR1 gene—particularly the genotypes and sub-genotypes defined by the number of CGG repeat counts on the gene —in the regulation of ovarian reserve over the long term. Based on this research published in various medical journals, CHR was able to refine egg donor recruitment and ensure optimum pregnancy chances for the recipients of donated eggs.
CHRReceives New
Patent
Read the original OPINION: http://kaywa.me/1Apl1

The peculiar disappearance of closed embryo culture systems with time-lapse imagingOne of the bigger surprises of the ASRM meeting was the relative absence of significant new studies of closed embryology culture systems with time lapse photography. The Annual Meeting of the European Society for Reproductive Medicine and Embryology (ESHRE) in June of this year also produced no new information. It is becoming increasingly clear that the original enthusiasm for these systems is waning.
We noted in these pages last month that studies CHR performed on one of these systems not only did not demonstrate outcome advantages, as previously claimed by some colleagues and manufacturers, but, actually, demonstrated somewhat poorer outcomes. Once again, CHR’s careful approach to the introduction of new “fashions of the moment” in the IVF field, therefore, appears validated.
Otherwise, the ASRM meeting was rather disappointing; few new ideas of substance were presented. The one pleasant surprise was the host city of Baltimore, which presented itself to visitors as a modern and quickly developing city, very different from the image the media presented in the last year of Baltimore.
4
which the embryos really arises, may be chromosomally completely normal. In such a case a false-positive diagnosis would be reached, and perfectly normal embryos would be discarded.
It, therefore, is reasonable to assume that thousands of perfectly healthy embryos are currently discarded daily at IVF centers all around the world because of false-positive diagnoses.
On page 3, we are publishing an Addendum to CHR’s above cited OPINION on the utilization of allegedly aneuploid embryos in IVF. This Addendum is partially based on these new data reported by colleagues at the
ASRM meeting, but to an even larger extent, they are based on new data CHR researchers and collaborators from other centers have developed in recent months.
While we currently are not yet at liberty to reveal details (a manuscript is in preparation for submission), these new data, with a high degree of certainty, demonstrate that PGS, even in its most recent incarnation, is clinically not helpful. In women with few embryos, the procedure will, indeed, actually significantly reduce pregnancy and live birth chances. Stay tuned for much more to come in the very near future!
News from ASRM: Continued from Page 2
Does tracking your monthly cycles on smartphone apps improve your chance of pregnancy? That was the question a Wired article tried to answer, after one of the companies selling fertility tracking apps claimed that it does at the ASRM meeting. Quoting Dr. Kushnir, this well-balanced article concluded that while these apps hold great potential for gathering fertility data from normal populations, their claim of improved fertility is likely due to selection bias.
Dr. Gleicher gave an extensive interview for a Glamour article, on the importance of early screening for premature ovarian aging (POA), a condition that affects 10% of all women. If women know that they are at risk for developing POA, they can make plans to avoid future struggles with infertility. The article coincided with the full launch of What’s My Fertility, an online POA screening program developed by CHR physicians.
... these data demonstrate that PGS is not clinically helpful
“Read more about embryoscope: http://kaywa.me/HEte1
Glamour article: http://kaywa.me/D9mNx
Wired article: http://kaywa.me/oUX2z
CHR in the Media In FocusThis feature presents microscopic images from CHR’s laboratories, edited by our Director of the Division of Laboratories and Senior Scientist, David F. Albertini, PhD.This month we feature an image of a human blastocyst. This confocal micrograph shows in green the boundaries between cells that will comprise both the placenta and the fetus. The DNA for each cell is shown in white. The majority of the cells at this stage of development carry two sets of chromosomes, one inherited from mom and one from dad, and are referred to as euploid. But mistakes happen as the cells divide and their chromosomes separate. If the chromosomes do not partition equally into the two daughter cells, a condition known as aneuploidy arises with one cell having one too many chromosomes and the other having one too few. Preimplantation genetic diagnosis (PGD) is used to test embryos for aneuploidy but both the accuracy of this test and the meaning of the results are being questioned by researchers at the CHR.

prospectively randomized studies in this area, for a variety of reasons, are almost impossible to conduct, none of them can, as of this moment, be considered well supported by a high enough level of evidence.
Implantation as an inflammatory processFrom the preceding it will be obvious that implantation is an immunological process. It also is an inflammatory process. Indeed, most key processes in human reproduction are inflammatory processes, starting with ovulation over implantation and, finally, even the onset of labor.
Reproductive immunology has been one of the main research interests at CHR for decades. Indeed, Norbert Gleicher, MD, CHR’s Medical Director and Chief Scientist, was one of the first clinical reproductive immunologists in the world, one of the original founders of the American Society for Reproductive Immunology in 1980 and the first Editor-in-Chief of the American Journal of Reproductive Immunology. Inflammation in recent years has been an increasingly important research subject at CHR as we attempt to find markers of poor tolerance in peripheral blood of affected women.
After many years of investigations, researchers at CHR have been able to identify some promising inflammatory markers, which appear strongly associated with female reproductive success and/or failure. In a number of manuscripts currently awaiting publication, they demonstrated that the well known inflammatory marker C-reactive protein (CRP) is strongly negatively associated with live birth after IVF, while the inflammatory marker interleukin 6 (IL-6) is strongly associated with miscarriages. Practically, this means that women who have elevated CRP have decreased live birth chances after IVF and those with elevated IL-6 demonstrate increased risk of miscarriages. Interestingly, these associations are linear, i.e., the higher the values of CRP and IL-6, the higher their associated risks and, to our surprise, they proved much stronger than associations with autoimmune markers, which have been known for decades.
All research at CHR is in principle translational. CHR researchers attempt to direct their investigations toward specific clinical problems. The research of inflammatory markers is a good example: It suggests that traditional treatments in women with implantation failure and/or
their immune system still, at least partially, sees the implanting embryos as “foreign,” and attacks it like it would a foreign organ transplant. This is called an allogeneic immune response, directed against the “foreign” alloantigens of the graft, in this case those of the biological father. The consequence can be difficulties of implantation (i.e., implantation failure) and/or early miscarriages.
Indeed, we often cannot differentiate between implantation failure and very early miscarriages because even the most sensitive pregnancy tests we currently have at our disposition become positive only approximately one week after implantation. It, therefore, is very likely that in many IVF cycles, considered to have failed, embryos did indeed implant but were “rejected” by the maternal immune system before a positive pregnancy test could be obtained.
Such a rejection is also known to occur later: For example, only since IVF was developed, do we
know that so-called chemical pregnancies are very frequent. These are very early pregnancies, which already result in a positive pregnancy test since the hormone human chorionic gonadotropin (hCG), produced by the implanting
embryo, can be detected in the mother’s circulation. It, of course, can be found in the mother’s blood only if the embryo, almost like a cancer, dug itself deep into her endometrium (i.e., implanted) and made contact with her vasculature. Alloimmune responses can, however, also occur much later in pregnancy, and then they can be the cause of clinical miscarriages, also called immunological miscarriages because they are caused by failure of normal development of immunological tolerance in the mother.
Apparent failure to conceive, chemical pregnancies and immunological pregnancy losses, therefore, can represent one spectrum of reproductive failure, characterized by the failure of the maternal immune system to establish normal immunological tolerance.
Though we now (believe to) understand the existence of this problem, we currently do not have reliable tests to diagnose this condition. Moreover, even if we are reasonably certain that this problem exists, we do not have well established treatments to combat it. At CHR, we prescribe various immune-suppressive treatments in such situations, but because
Black Box of Implantation: Continued from Page 1
Continued reading on Page 65
... we do not have reliable tests to diagnose these reproductive failures
“
... implantation is both an immunological and inflammatory process
“

excessively activated immune systems may in many cases have been ineffective because they primarily had been directed at autoimmune processes. CHR’s recent research, however, now suggests that in some patients treatments have to be directed at inflammatory rather than autoimmune pathways. Consequently, in such patient, treatment may have to be modified in that (auto)immune-suppressive treatments either have to be replaced by anti-inflammatory treatments or, even more likely, anti-inflammatory agents may have to be added to (auto)immune-suppressive treatments because autoimmune and inflammatory pathways often overlap and/or run in parallel.
Building on CHR’s recent research, CHR’s physicians have already started to integrate anti-inflammatory treatments in patients with obvious evidence of excessive inflammation, and are carefully studying their effects. Associations do not always reflect causations, but where such associations make physiological sense, they often do.
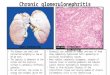
Chronic endometritis, an inflammatory disease?One aspect of CHR’s expanded investigation of the importance of inflammation in implantation failure has been the investigation of chronic endometritis. That this condition exists has been known for decades. Recently a number of studies associated the presence of this condition with implantation failure.
CHR investigators, led by Vitaly A. Kushnir, MD, Associate Scientist and Director of CHR’s Fertility Preservation Program, indeed, discovered that in a select group of women with implantation failure (i.e., multiple IVF cycle failures unexplained by other causes), almost half suffered from chronic endometritis
when endometrial biopsies were performed (a manuscript reporting this and related findings is close to submission).
The typical histological picture of chronic endometritis is characterized by infiltrates of so-called plasma cells. Those are white blood cells (WBCs), which produce antibodies. They are not the typical WBCs that can be found in bacterial infections but usually are typical for autoimmune infiltrates in sterile inflammations of endocrine organs. Indeed, in every endocrine organ of the human body, from pituitary, over adrenals, pancreas, thyroid and ovary, such sterile autoimmune inflammations have been described, except for in the endometrium. Yet, for decades, ever since this condition was originally described, chronic endometritis has been treated with antibiotics as a bacterial infection.
Some cases of chronic endometritis, indeed, have an infectious etiology, and treatment with antibiotics will cure the condition. Many others, however, as the recent CHR study again demonstrated, do not respond to antibiotics. CHR investigators, therefore, under the assumption of an inflammatory rather than direct autoimmune process, have started to treat affected patients with anti-inflammatory medications, and are investigating the effects of such treatments.
We, therefore, encourage patients with repeated implantation failure, or colleagues who have been unsuccessful in treating such patients, to contact us. We will gladly share our protocols and/or help in the treatment of such patients.
Implantation as a defense mechanism against implantation of abnormal embryosIn recent publications, some investigators have proposed an intriguing new theory that connects the concepts that embryo quality and/or implantation failure can be causes of implantation failure. In very well executed experiments, these investigators appear to demonstrate that the human endometrium has the ability to “judge” which embryo is “normal.” If confirmed, this model would suggest an explanation why most chromosomally abnormal embryos do not succeed to implant, at least for the long-term.
In addition, this hypothesis would explain why it is so
Chronic endometritis with the characteristic plasma cells (Image by Nephron. Licensed under CC BY-SA 3.0 via Wikimedia Commons)
Chronic endometritis
6
... chronic endometritis has traditionally been treated with antibiotics as a bacterial infection
“
Continued reading on Page 7
Black Box of Implantation: Continued from Page 5

difficult to differentiate between different causes of implantation failure. It would also close the circle with the above described recent recognition by investigators at CHR and elsewhere that many more embryos are mosaic than has previously been assumed. And it would, finally, explain why it takes so many eggs and embryos in IVF to establish a normal pregnancy that leads to live birth.
7
-The CHRFighting for every egg and embryo!
CHR Participates in “Service to Veterans” Program
Black Box of Implantation: Continued from Page 6
There is a strange asymmetry between active-duty military personnel and veterans when it comes to accessing fertility treatments. The Veteran’s Administration (VA) is prohibited under federal law from providing IVF. This means that vets whose service related injuries damaged their reproductive systems cannot access IVF, even though active duty military personnel can.
As legislative efforts to make IVF available to veterans have been faltering, the Society for Assisted Reproductive Technologies (SART) and ASRM have set up a “Service to Veterans” program, in which participating IVF centers offer deep discounts to veterans whose service-related injuries necessitate IVF. CHR is proud to be one of the inaugural participants in this program.
In essence, we will be extending the same discount that we have been offering to active-duty military personnel to veterans for quite some time now. If you are interested in taking advantage of this program, please inform our receptionists, who will guide you through the process.
Staying Connected
Visit CHR on Facebook:https://www.facebook.com/thechr
Follow CHR:http://twitter.com/infertilityNY
Check out our video resources:https://www.youtube.com/user/CenterForHumanReprod
International Congress on Cardiac Problems in Pregnancy (CPP 2016)The 4th Internatioanaternal Congress on Cardiac Problems in Pregnancy, scehduled for 2/27/216-3/1/2016 in Las Vegas, Nevada, focuses on maternal and fetal pregnancy-associated cardiovascular conditions. As in the previuos years, Dr. Gleicher will be one of the presenting experts at the congress. For more information about participation, go to their website at www.CPPCongress.com.
Announcement
Whether new informational material on treatments or news coverage on fertility breakthroughs, the best way to stay up to date on CHR’s activities is via our social media channels. Follow us, and never miss any important news about fertility research and treatment!