the case for lung cancer screening
-
Upload
others
-
View
3
-
Download
0
Embed Size (px)
Citation preview
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus12
Evidence for lung cancer screening 1) Lung cancer specific
mortality reduction: Screening efficacy has been described in
several large trials, including a 20% relative reduction in lung
cancer specific mortality in the landmark National Lung Screening
Trial (NLST),4 and a 25% reduction (for men) in the Dutch-Belgian
Lung Cancer Screening (NELSON) trial.5 Adherence to annual
screening in these two large clinical trials exceeded 90%, directly
contributing to lung cancer mortality reductions, with 58% and 73%
of stage I lung cancers detected on annual imaging in the NLST and
NELSON trials, respectively.4,5
2) Early detection of lung cancer: Overall, 50% of all CT detected
lung cancers diagnosed in the NLST were stage I.4 Similar rates of
early lung cancer diagnoses were observed in the Nelson trial, with
59% of CT detected cancers reported as stage I.5 High rates of
stage I lung cancer diagnosis rates have also been reported outside
of clinical trial settings, community healthcare systems and
clinics have also reported stage I diagnosis rates of at least
63%.6, 7
3) Initial low uptake of lung cancer screening: As a new cancer
screening modality, initial uptake of lung cancer screening has
been low with only 2-16% of eligible individuals currently
receiving screening.8-12 While low uptake can be linked to barriers
at the patient, provider, and system level, there is a general lack
of awareness about lung cancer screening in the medical and lay
communities.13 Continued education about screening is vital, so
that one day low-dose CT screening will be as commonly known as
mammography and colonoscopy for breast and colon cancer
screenings.
4) Lung cancer screening disparities: Individuals that smoke
tobacco, and are also potentially eligible for lung cancer
screening, are likely to already face health disparities.14 This
includes racial and ethnic minorities, sexual and gender
minorities, individuals with low-socioeconomic status, and
individuals that live in rural areas of the country.14 These
populations also face increased lung cancer incidence and mortality
with longer time to diagnosis and treatment.15 Anyone that works
within a lung cancer screening program can help reduce these lung
cancer disparities by thinking how best to reach these populations
and educate them about lung cancer screening.
chapter 1 the case for lung cancer screening Objective:
Understand the need, evidence, requirements, process, risks,
benefits, cost, and outcomes of lung cancer screening to consider
the need for patient navigation within your healthcare clinic or
system.
Overview of lung cancer Lung cancer is the leading cause of cancer
death for both men and women in the United States, killing more
people than breast, colon, and prostate cancers combined1. There
are two main types of lung cancer, small cell and non-small cell2.
Small cell lung cancer accounts for ~15% of all lung cancer cases
and is typically more aggressive and faster growing2. The remaining
85% of cases are non-small cell lung cancer2. Lung cancer is
usually diagnosed at advanced stages. 5-year survival of advanced
lung cancer is less than 10%, with 5-year survival of early-stage
lung cancer exceeding 55%3. The problem is that currently only 17%
of patients are diagnosed with early stage disease3. Early
detection is critical to reducing lung cancer specific mortality.
Lung cancer screening with low dose CT is the only recommended test
that finds lung cancer at an early stage when curative treatment
options exist.
Find out more about types of lung cancers and staging of lung
cancer from the American Cancer Society!
Check your knowledge about lung cancer types and staging in the
patient navigation online training.
www.cancer.org/cancer/lung-cancer/
detection-diagnosis-staging.html
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus 13
5) Patient navigation in lung cancer screening: Patient navigation
has increased screening rates in a wide range of racial and ethnic
groups in colon, breast, and cervical cancer screenings with both
nurse navigators and lay navigators.16 Moreover, patient navigation
has successfully reduced cancer rates by eliminating barriers for
vulnerable populations17 and has recently been identified as a
method to reduce disparities in lung cancer screening.15 The United
States Preventive Services Task Force recommends several strategies
to increase screening rates for breast, colon, and cervical cancers
that can also be easily used for lung cancer screening (patient
reminders, patient education, barrier reduction, small media, and
provider reminders).18 Lung cancer screening programs can greatly
benefit from the use of patient navigation to both optimize the
screening process and improve patient outcomes with increased
screening and reduced mortality rates!
Overview of lung cancer screening requirements and process The goal
of lung cancer screening is to find and diagnose early-stage
disease before signs and symptoms occur. However, there are several
elements of lung cancer screening that are different from other
cancer screenings.
Lung cancer screening should be thought of as a process that
requires several steps not required for other types of cancer
screenings. Table 1-1 gives a broad overview of important elements
to know and consider for high-quality lung cancer screening.
Screening Steps & Process Important Elements and Considerations
Determining Candidate Eligibility
Screening of eligible individuals is extremely important to
maximize the efficacy of lung cancer screening.
• In general, private insurance companies follow guideline
recommendations from the US Preventive Services Task Force and
Medicare beneficiaries follow the guidelines established from the
Centers for Medicare and Medicaid Services. Lung cancer screening
is also covered for Medicaid beneficiaries in some states.
• Finding potentially eligible screening candidates can be
difficult because smoking history is not often accurate in the
electronic medical record.
Shared Decision-Making (SDM) Counseling visit between the screening
candidate and ordering provider to determine screening eligibility
and discuss the risks and benefits of screening.
• Required by Medicare for reimbursement purposes and strongly
recommended by the US Preventive Services Task Force.
• Must be completed prior to the low-dose CT procedure. • Must be
completed by a clinician (MD or advanced practice provider). • Must
utilize a decision aid to address risks and benefits. • Completion
of SDM visit must be recorded in the medical record. •
Historically, SDM was required to take place in-person, but
telehealth
options have recently been allowable due to the COVID-19 pandemic.
Tobacco Cessation Services
Cessation services must be offered to all individuals that
currently smoke cigarettes. Positive reinforcement of behavior for
individuals that formerly smoke cigarettes should also be
considered.
• Required by Medicare for reimbursement purposes and strongly
recommended by the US Preventive Services Task Force.
• Must be completed prior to the low-dose CT procedure. • Cessation
services may include quitline referrals, referrals to tobacco
treatment specialists, providing fact sheets and brochures, or
prescriptions for cessation aids (Chantix, Wellbutrin, nicotine
replacement, etc.).
The low-dose CT scan Individual and imaging information flows back
and forth between the ordering provider and the imaging center to
facilitate the screening process. Ensuring proper flow and
completion of this information will help the screening process run
smoothly
• Requires a written order documenting the patient’s eligibility
and confirming completion of shared decision-making and tobacco
cessation.
• Recommended CT scan is completed at a screening facility
accredited by the American College of Radiology that utilizes
appropriate radiology dose recommendations and has trained thoracic
radiologists for scan interpretation.
• The results should be read utilizing Lung-RADs (a standardized
lung nodule identification, classification and reporting system) to
report the low dose CT results and provides suggested follow-up
guidelines.
Reporting and Follow-up Data collection can be time consuming but
can lead to improved program processes and outcomes through
continuous quality improvement.
• Information about all screening participants and CT, regardless
of insurance payer, must be submitted to the American College of
Radiology Lung Cancer Screening Registry to enable providers to
meet quality reporting requirements. Transmitting information to
the registry is often completed by the imaging center.
• Next steps following the low dose CT will depend on the results
of the screening low dose CT scan. Tracking and sending follow-up
reminders will ensure timely follow-up and decrease time to
possible diagnosis or treatment.
• Screening programs should collect additional evaluation metrics
(e.g. determination of eligible candidates, characteristics of
screened patients, screening process and outcomes) to help
understand who your program is screening and track important
outcome metrics.
Use this information to talk with your healthcare organization
about implementing lung cancer screening using the ‘Lung Cancer
Screening Evidence Summary’ tool.
Table 1-1. Overview of Lung Cancer Screening Process and
Elements
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus14
Screening Steps & Process Important Elements and Considerations
Determining Candidate Eligibility
Screening of eligible individuals is extremely important to
maximize the efficacy of lung cancer screening.
• In general, private insurance companies follow guideline
recommendations from the US Preventive Services Task Force and
Medicare beneficiaries follow the guidelines established from the
Centers for Medicare and Medicaid Services. Lung cancer screening
is also covered for Medicaid beneficiaries in some states.
• Finding potentially eligible screening candidates can be
difficult because smoking history is not often accurate in the
electronic medical record.
Shared Decision-Making (SDM) Counseling visit between the screening
candidate and ordering provider to determine screening eligibility
and discuss the risks and benefits of screening.
• Required by Medicare for reimbursement purposes and strongly
recommended by the US Preventive Services Task Force.
• Must be completed prior to the low-dose CT procedure. • Must be
completed by a clinician (MD or advanced practice provider). • Must
utilize a decision aid to address risks and benefits. • Completion
of SDM visit must be recorded in the medical record. •
Historically, SDM was required to take place in-person, but
telehealth
options have recently been allowable due to the COVID-19 pandemic.
Tobacco Cessation Services
Cessation services must be offered to all individuals that
currently smoke cigarettes. Positive reinforcement of behavior for
individuals that formerly smoke cigarettes should also be
considered.
• Required by Medicare for reimbursement purposes and strongly
recommended by the US Preventive Services Task Force.
• Must be completed prior to the low-dose CT procedure. • Cessation
services may include quitline referrals, referrals to tobacco
treatment specialists, providing fact sheets and brochures, or
prescriptions for cessation aids (Chantix, Wellbutrin, nicotine
replacement, etc.).
The low-dose CT scan Individual and imaging information flows back
and forth between the ordering provider and the imaging center to
facilitate the screening process. Ensuring proper flow and
completion of this information will help the screening process run
smoothly
• Requires a written order documenting the patient’s eligibility
and confirming completion of shared decision-making and tobacco
cessation.
• Recommended CT scan is completed at a screening facility
accredited by the American College of Radiology that utilizes
appropriate radiology dose recommendations and has trained thoracic
radiologists for scan interpretation.
• The results should be read utilizing Lung-RADs (a standardized
lung nodule identification, classification and reporting system) to
report the low dose CT results and provides suggested follow-up
guidelines.
Reporting and Follow-up Data collection can be time consuming but
can lead to improved program processes and outcomes through
continuous quality improvement.
• Information about all screening participants and CT, regardless
of insurance payer, must be submitted to the American College of
Radiology Lung Cancer Screening Registry to enable providers to
meet quality reporting requirements. Transmitting information to
the registry is often completed by the imaging center.
• Next steps following the low dose CT will depend on the results
of the screening low dose CT scan. Tracking and sending follow-up
reminders will ensure timely follow-up and decrease time to
possible diagnosis or treatment.
• Screening programs should collect additional evaluation metrics
(e.g. determination of eligible candidates, characteristics of
screened patients, screening process and outcomes) to help
understand who your program is screening and track important
outcome metrics.
Other important lung cancer screening elements to remember and
consider:
Lung cancer screening is recommended on an annual basis. Adherence
to the recommended follow-up is imperative to reach the maximum
benefit of lung cancer screening at the individual and population
level.
Eligibility is based on a life-style choice that is heavily
associated with the stigma of smoking. Patient navigators should
focus on normalizing lung cancer screening as a way to maintain
optimal health for those eligible and adopting person-first
language when discussing lung cancer screening. For example,
referring to people as ‘a smoker’ is stigmatizing language, instead
say ‘someone that smokes cigarettes.’
It is important to confirm insurance coverage and eligibility prior
to scheduling a shared decision-making or CT appointment, some may
require pre-authorization.
Become familiar with the imaging centers accredited by the American
College of Radiology for lung cancer screening in your area. Know
which ones offer extended or weekend hours!
See the ‘Lung Cancer Screening Initial Outreach Tip Sheet’ tool to
learn more about person-first language and tips on how to reduce
the stigma of cigarette smoking.
Learn more about the screening process and associated navigator
duties in Chapter 2.
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus 15
Lung cancer screening eligibility Lung cancer screening is
recommended on an annual basis by the US Preventive Services Task
Force (USPSTF)19 and the Centers for Medicare and Medicaid
Services.20 These recommendations mean that screening is covered as
a preventive service by commercial insurance companies, Medicare,
and Medicaid (in some states).
Eligibility for lung cancer screening varies slightly between
USPSTF and Medicare guidelines and is based on age, smoking status,
and smoking history. The National Comprehensive Cancer Network
(NCCN) also has recommendations for screening based on smoking
history and other factors that can make an individual high risk for
developing lung cancer.21 Table 1-2 presents the differences in
eligibility for USPSTF, Medicare, and the National Comprehensive
Cancer Network. In addition to basic eligibility requirements,
there are other patient and clinical characteristics that patients
and navigators should consider about being screened:
Table 1-2 Lung Cancer Screening Eligibility Guidelines for USPSTF,
Medicare, and NCCN Category 2
*USPSTF expanded screening guidelines on March 9, 2021, lowering
eligibility to 50 years of age and tobacco exposure to 20 pack
years. Private insurance payers have until January 1, 2023 to adopt
and cover the expanded guidelines but may voluntarily do so before
that date. You may need to check with each private payer to verify
if they are currently covering the expanded guidelines.
Read more about lung cancer screening eligibility guidelines for
Medicare, USPSTF, and NCCN
• Medicare -
https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.
aspx?NCAId=274 • USPSTF -
https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung-cancer-
screening • NCCN category 2 -
https://www.nccn.org/patients/guidelines/content/PDF/lung_screening-patient.pdf
USPSTF19 Medicare20 NCCN Category 221
Age 50-80* 55-77 ≥ 50 Smoking history ≥ 20 pack years* ≥ 30 pack
years ≥20 pack years Smoking status Current or quit within
past 15 years Current or quit within past
15 years N/A
Additional criteria • No signs or symptoms of lung cancer. •
Patients with comorbidities that limit life expectancy
should be screened with caution. • Willing to be treated if cancer
is found.
• Radon or asbestos exposure • COPD/ emphysema • Personal history
of cancer • Family history of lung cancer
• Individuals showing signs of lung cancer (coughing up blood,
unexplained weight loss, cough that won’t go away) should not have
a screening CT, but rather meet with a clinician to go over
symptoms and possibly be referred for a diagnostic CT.
• Individuals with limited life expectancy due to other comorbid
conditions or those that are poor surgical candidates should be
screened with caution. Eligibility should be reviewed by a
clinician.
• Individuals that are not willing to be treated should a lung
cancer be found are unlikely to benefit from screening.
• Individuals that had a chest CT for another diagnostic reason in
the past year should wait until a full year has passed before
having a CT for lung cancer screening.
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus16
Find and determine potential eligible individuals from case studies
in the companion navigator training.
When to stop screening for lung cancer?
The US Preventive Services Task Force recommends that individuals
stop being screened when:
• They reach >80 years of age;
• They have quit smoking cigarettes >15 years ago;
• They develop a comorbid condition that limits life expectancy or
the ability to have lung surgery.
A note about risk-based screening Another method of selecting
high-risk individuals for lung cancer screening is with the use of
risk calculators that estimate an individual’s risk of developing
lung cancer over a pre- specified time period. These risk
calculators consider variables that heighten someone’s risk of
developing lung cancer, such as cigarette smoking, family history
of lung cancer, personal history of cancer, personal history of
COPD/ emphysema/ chronic bronchitis, and exposure to cancer causing
agents such as radon and asbestos. Using risk calculators to
determine lung cancer screening eligibility is not currently
covered by insurance companies but is thought to efficiently select
individuals for screening. Clinicians may also use risk
calculators, such as the PLCOm2012 model22 available at
www.shouldiscreen.com, to talk with individuals about the risks and
benefits of screening. Read more about using risk-based screening
for participant selection:
https://www.acpjournals.org/doi/abs/10.7326/M17-2701?journalCode=aim
Explore lung cancer risk calculators here:
http://lungcancerrisk.s3-website-us-east-1.amazonaws.com/
The Low Dose CT Procedure Lung cancer screening is completed using
a low-dose computed tomography (CT) scan. A CT scan is a series of
x-rays that are taken from different angles and reconstructed by a
computer to give a detailed look at bones, blood vessels, and soft
tissues, such as heart and other organs in the chest region. The
patient will be asked to lay on their back on table that will slide
the patient into the CT scanner feet first.23
The good news is that the low dose CT procedure requires no special
or additional preparation. The patient simply needs to arrive at
the right place at the right time. He/she will be asked to remove
all metal from their body such as jewelry or belts. For women, you
may want to instruct them to wear a bra without any underwire.
Depending on the facility and what the person is wearing he/she may
be asked to change into a gown.23 The entire process should only
take about 5 minutes!
The low dose CT Procedure vs Indication for Annual Lung Cancer
Screening
A low dose CT refers to the technique of the CT procedure, meaning
that the CT is performed with a low dose of radiation. Many CT
procedures, including some diagnostic CTs, are performed as
low-dose to minimize the amount of radiation a patient is
receiving.
You may encounter a screening participant that is due for a yearly
lung cancer screening as being due for an annual low dose CT.
Remember that the low dose CT is the technique used for the CT
scan, it is not meant to represent the indication or reason for the
procedure (annual lung cancer screening.)
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus 17
39.1 -52
26 -39
52.1 -65
65.1 -78
78.1 -91
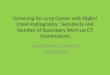
Incidence rates, 2013-2017 by state, for lung and bronchus
Average annual rate per 100,000, age adjusted to the 2000 US
standard population.
Data Sources: North American Association of Central Cancer
Registries (NAACCR), 2020
© 2021 America Cancer Society
CancerStatisticsCenter.cancer.org
Visit the American Cancer Society’s lung and bronchus cancer
webpage to find specific lung cancer incidence and death rates for
your state.
cancerstatisticscenter.cancer.org/#!/cancer-site/Lung%20and%20bronchus
Benefits and Risks of Lung Cancer Screening Benefits of lung cancer
screening include:
• Lung cancer screening is the only proven way to detect cancer at
an early stage!24
• By finding more cancers at an early stage we can decrease the
number of deaths caused by lung cancer!24
Figure 1-1 shows the incidence rates of lung and bronchus (per
100,000 population) by state.
Figure 1-1. Incidence rates of lung and bronchus cancer by
state.
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus18
Like any screening test, there are some risks associated with lung
cancer screening:
• Lung cancer screening can result in false positives or false
alarms, meaning a pulmonary nodule will be found but it will not be
known if the spot is cancerous without further testing. The
ordering provider may need to order additional tests to figure out
if the spot is cancerous24. Additional tests may include:
o More CT scans
o A PET scan
o A biopsy to take a small tissue sample of the spot.
o In some cases, surgery to remove the nodule may also be
necessary. • There is a possibility that lung cancer screening will
detect a cancer that is very slow growing and would not have caused
any problems for the patient in their lifetime. This is called
overdiagnosis, meaning that this type of cancer may lead to
unnecessary testing, treatment or surgery. The harms from
overdiagnosis can be mitigated through proper monitoring of the
suspicious area and following established radiology guidelines
(Lung-RADs).24, 25
• The patient will receive a small dose of radiation from the low
dose CT. Exposure to low levels of radiation, such as environmental
exposures, does not cause any immediate health risks but
contributes slightly to one’s overall cancer risk. The dose of
radiation a person receives from a low dose CT scan is about the
same amount receiving from the environment over one year.25
• Stress and psychological distress - As with any type of medical
screening, stress and distress can occur. Fear and anxiety can come
from the screening process itself, anticipation of results, or when
learning of a positive screen. It is essential to talk to and
educate the patient about potential screening results and listen to
their concerns before moving forward.24
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus 19
Visit Chapter 3 to read more about Medicaid coverage of lung cancer
screening and determining if your screening program should offer a
self-pay coverage option.
The cost of lung cancer screening Cost of screening for the
candidate/ patient
Lung cancer screening is a reimbursable preventive service for
patients that meet eligibility guidelines and have commercial
(private) insurance and Medicare. Medicaid also provides coverage
in some states and requires pre- authorization. Screening is a
preventive service under the Affordable Healthcare Act and patients
that meet eligibility criteria should not have associated co-pays.
You should always verify insurance coverage for screening
candidates prior to scheduling them for shared decision-making or a
low-dose CT. Your screening program may also decide to offer a
self-pay option for individuals that do not have insurance or would
like to be screened but do not meeting current eligibility
criteria.
It is also important to remember that reimbursement of screening as
a preventive service only covers the cost of the shared-decision
making and low-dose CT scan. If there is additional recommended
follow-up the cost of these procedures will be billed to insurance
coverage.
Billing for Lung Cancer Screening Services
Reimbursement is available for two aspects of lung cancer
screening: 1) Shared Decision-Making (for Medicare beneficiaries)
and 2) the low-dose CT.
To bill for lung cancer screening services the following codes must
be used (information from the American College of Radiology)
26:
• G0296 — Counseling visit to discuss need for lung cancer
screening using low-dose CT scan (service is for eligibility
determination and shared decision making)
• 71271— Computed tomography, thorax, low dose for lung cancer
screening, without contrast material(s). Prior to January 2021, the
billing code for the low dose CT was G0297. The old code should no
longer be used.
These services must also be billed with a nicotine dependence
ICD-10 diagnosis code. Medicare will deny G0296 and 71271 for
claims that do not contain these ICD-10 diagnosis codes:
• Z87.891 for individuals who formerly smoke cigarettes (personal
history of nicotine dependence).
• F17.21 for individuals who currently smoke cigarettes (nicotine
dependence).
Visit the American College of Radiology website for more
information about insurance coverage and billing for lung cancer
screening services.
www.acr.org/Clinical-Resources/Lung-Cancer-Screening-Resources/FAQ
www.acr.org/-/media/ACR/Files/RADS/ Lung-RADS/LungRADSAssessment
Categoriesv1-1.pdf
See the ‘Checklist for Billing and Coding for Shared
Decision-Making Visit’ tool for an individual level perspective of
coding requirements for shared decision-making.
Screening outcomes and follow-up Results for lung cancer screening
low dose CT scans are reported using the Lung Imaging Reporting and
Data System (Lung-RADs). Lung-RADs is a structured reporting system
that contains information on technique, comparison date,
description of findings, impression, Lung- RADS category and
specific management recommendations.
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus20
Category Description Probability of Malignancy
Recommended Follow- up
screening low dose CT
screening low dose CT
diagnosis low dose CT 4A
Suspicious
sampling 4B
>15% 4X
requires additional follow-up N/A Per clinical protocols/
guidelines
C Prior lung cancer N/A N/A
Table 1-3 Overview of Lung-RADs Categories
A note about nodule care pathways. Exact follow-up of positive
screens (those with a result of Lung-RADs 3 or 4) is a complex
decision of nodule location, clinician recommendation, and patient
preference. Scenarios presented here are examples of possible
diagnostic follow-up based on radiologist recommendations.
Overview of Lung-RADS scoring
The Lung-RADS assessment category for each lung cancer screening
examination is an alphanumeric score composed of two parts:
category (part 1) plus modifier (part 2). Part 1 classifies nodules
into categories 0–4 on the basis of morphology and size. Part 2
addresses findings other than lung nodules and uses the modifiers
X, C, and S. Results of Lung-RADs 1 or 2 are considered a negative
result and a result of Lung-RADs 3 or 4 is a positive result and
additional follow-up is recommended.
In general, a Lung-RADs result of 1 or 2 is considered a negative
screen with recommended follow-up in one year for annual screening.
A Lung-RADs result of is considered a positive screening for a lung
cancer that needs shorter-term follow-up to watch the nodule for
growth or change or to biopsy if the health care team thinks it is
necessary.
Care pathways are examples of follow-up based on pulmonary nodule
management algorithms defined by the Lung-RADs results. Exact
recommendations for individual patients will be listed on the
screening CT radiology report. Table 1.3 gives an overview of each
Lung-RADs category with description, probability or malignancy and
recommended follow-up.
When is it no longer screening?
Once a patient is diagnosed with lung cancer, further diagnostic
management is often necessary (including additional imaging such as
PET/ CT) for the purposes of lung cancer staging. These additional
diagnostic procedures are no longer elements of screening.
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus 21
Estimates of Lung-RAD results by population prevalence
The prevalence of Lung-RADs 1 and 2 result distribution may differ
between areas in the country that have endemic fungal infections,
commonly aspergillus, histoplasmosis, coccidiomycosis, and
cryptococcosis.27 Fungal infections can cause small pulmonary
nodules, resulting in a higher distribution of Lung-RAD 1 (no
nodules) results in areas without endemic fungal infections and a
higher distribution of Lung-RADs 2 (small nodules not concerning
for cancer) results in areas with endemic fungal infections. This
difference is illustrated in Figure 1-2, comparing results from the
University of Colorado, 28 where endemic fungus is not a big
concern and from Cleveland Clinic,29 and area of the United States
with endemic fungus.
Figure 1-2. Lung-RADs Prevalence by Endemic Fungal Regions
Estimated ACR Prevalence* 90% - Lung-RADs 1 and 2
5%
4%13%69%14%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
University of Colorado
Lung-RADs 1 Lung-RADs 2 Lung-RADs 3 Lung-RADs 4
*1% of the estimated American College of Radiology (ACR) prevalence
is Lung-RADs category 0 (incomplete exam).
Incidental findings and significant incidental findings
An incidental finding is an abnormality that is found and is
unrelated to the purpose of the scan. When a low dose CT is
completed and viewed by the radiologist much more than lung cancer
can be found. In a CT scan of the chest the lungs, heart, liver,
breast tissue, thyroid, pancreas, gall bladder, spleen, intestines,
and spinal column can all be seen and will be looked over by the
radiologist. Though the focus is on the lungs, all areas will be
checked and any abnormalities will be reported.
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus22
This is very common with lung cancer screening. In fact up to 50%
will have an incidental finding.29 It will be important for the
provider to go over these findings and, if necessary, make
additional referrals.
Common incidental findings include:29
o Hiatal hernia
o Liver disease
o Renal issues
Significant incidental (S) findings are incidental findings for
which further medical evaluation is recommended. The American
College of Radiology Lung Cancer Screening Registry collects
information on the following S findings:
- Aortic aneurysm
- Pulmonary fibrosis
- Other interstitial lung disease, specify type if known
Management of incidental findings
Discovery of incidental findings should be reported to the primary
care provider or referring physician so they can be evaluated as
indicated by following existing guidelines. Much like a positive
screening result, exact management and evaluation of an IF will
depend on clinician recommendation and patient preference. The
screening radiology report may offer recommendations on the
management of the incidental finding as well.
Navigation Key Points
The most common incidental findings are pulmonary related and
coronary arterial calcification, both present in up to 50% of
screened patients.
All incidental findings should be reported to the patient’s primary
or referring physician so a care plan can be established if
needed.
It is important to collect and track information on the rate and
type of each incidental finding.
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus 23
Chapter 1 references
Copyright ©2021 University of Colorado Cancer Center, University of
Colorado Anschutz Medical Campus
1) American Cancer Society, Cancer Facts and Figures 2020.
Available at: https://www.cancer.org/content/dam/cancer-
org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2020/cancer-facts-and-figures-2020.pdf.
Accessed May 2021.
2) American Cancer Society, About Lung Cancer. Available at:
https://www.cancer.org/cancer/lung-cancer/about.html. Accessed May
2021.
3) SEER cancer stat facts: lung and bronchus cancer. National
Cancer Institute website. Available at:
https://seer.cancer.gov/statfacts/html/lungb.html. Accessed May
2021.
4) Aberle DR, Adams AM, Berg CD, et al. National Lung Screening
Trial Research Team. Reduced lung-cancer mortality with low-dose
computed tomographic screening. N Engl J Med. 2011; 365 (5):
395-409.
5) Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced
Lung-Cancer Mortality with Volume CT Screening in a Randomized
Trial. N Engl J Med 2020; 382:503-513.
6) Handy JR Jr, Skokan M, Rauch E, et al. Results of Lung Cancer
Screening in the Community. Ann Fam Med. 2020 May;18(3):243-249.
doi: 10.1370/afm.2519.
7) Cattaneo SM 2nd, Meisenberg BR, Geronimo MCM, et al. Lung Cancer
Screening in the Community Setting. Ann Thorac Surg. 2018
Jun;105(6):1627-1632. doi: 10.1016/j.athoracsur.2018.01.075. Epub
2018 Mar 1.
8) Jemal A and Fedewa SA. Lung cancer screening with low-dose
computed tomography in the United States-2010 to 2015. JAMA Oncol.
2017;3(9):1278–1281.
9) Pham D, Bhandari S, Oechsli M, Pinkston CM, Kloecker GH. Lung
cancer screening rates: Data from the lung cancer screening
registry. J Clin Oncol 2018;36(15_suppl):6504-6504.9.
10) Huo J, Shen C, Volk RJ, and Shih Y-CT. Use of CT and Chest
Radiography for Lung Cancer Screening Before and After Publication
of Screening Guidelines: Intended and Unintended Uptake. JAMA Int
Med 2017;177(3):439-441.11.
11) Zahnd WE and Eberth JM. Lung Cancer Screening Utilization: A
Behavioral Risk Factor Surveillance System Analysis. Am J Prev Med
2019 Aug;57(2):250-255.
12) Yong PC, Sigel K, Rehmani S, Wisnivesky J, Kale MS. Lung Cancer
Screening Uptake in the United States. Chest
2020;157(1):236-238
13) Carter-Harris L, Gould MK. Multilevel Barriers to the
Successful Implementation of Lung Cancer Screening: Why Does It
Have to Be So Hard? Ann Am Thorac Soc. 2017 Aug;14(8):1261-1265.
doi: 10.1513/AnnalsATS.201703-204PS.
14) Centers for Disease Control and Prevention. Smoking &
Tobacco Use: Tobacco Related Disparities. Available at:
https://www.cdc.gov/tobacco/disparities/index.htm. Accessed May
2021.
15) Rivera MP, Katki HA, Tanner NT, et al. Addressing Disparities
in Lung Cancer Screening Eligibility and Healthcare Access. An
Official American Thoracic Society Statement. Am J Respir Crit Care
Med. 2020 Oct 1;202(7):e95-e112. doi:
10.1164/rccm.202008-3053ST.
16) Ali-Faisal SF, Scott LB, Colella TJF, and Medina-Jaudes N.
Patient Navigation Effectiveness on Improving Cancer Screening
Rates: A Meta-Analysis of Randomized Controlled Trials. Journal of
Oncology Navigation & Survivorship. 2017; 8(7): 316-324.
17) Shusted CS, Barta JA, Lake M, Brawer R, Ruane B, Giamboy TE,
Sundaram B, Evans NR, Myers RE, Kane GC. The Case for Patient
Navigation in Lung Cancer Screening in Vulnerable Populations: A
Systematic Review. Popul Health Manag. 2019 Aug;22(4):347-361. doi:
10.1089/pop.2018.0128.
18) The Community Guide. CPSTF Findings for Cancer Prevention and
Control. Available at:
https://www.thecommunityguide.org/content/task-force-findings-cancer-prevention-and-control.
Accessed May 2021.
19) US Preventive Services Task Force. Screening for lung cancer.
March 9, 2021. Available at:
https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/lung-cancer-screening.
Accessed May 2021.
20) Centers for Medicare & Medicaid Services. Final National
Coverage Determination on Screening for Lung Cancer with Low Dose
Computed Tomography (LDCT). 2015. Available at
https://www.cms.gov/medicare-coverage-database/details/nca-
decision-memo.aspx?NCAid=274. Accessed May 2021.
21) NCCN Guidelines for Patients. Lung Cancer Screening, 2020.
Available at:
https://www.nccn.org/patients/guidelines/content/PDF/lung_screening-patient.pdf.
Accessed May 2021.
22) Tammemägi MC, Katki HA, Hocking WC, et al. Selection Criteria
for Lung-Cancer Screening. N Engl J Med. 2013 Feb 21;368(8):728-36.
doi: 10.1056/NEJMoa1211776.
23) GO2 Foundation for Lung Cancer. Lung Cancer Screening – What to
Expect. Availabe at: https://go2foundation.org/blog/lung-
cancer-screening-expect/. Accessed March 2021.
24) American Thoracic Society. Decision Aid for Lung Cancer
Screening with Computerized Tomography (CT). Available at:
https://www.thoracic.org/patients/patient-resources/resources/decision-aid-lcs.pdf.
Accessed March 2021.
25) Agency for Healthcare Research and Quality. Lung Cancer
Screening: A Summary Guide for Primary Care Clinicians. Available
at:
https://effectivehealthcare.ahrq.gov/decision-aids/lung-cancer-screening/clinician-summary.html.
Accessed March 2021.
26) American College of Radiology. Low-Dose CT Lung Cancer
Screening FAQ. Available at: https://www.acr.org/Clinical-
Resources/Lung-Cancer-Screening-Resources/FAQ. Accessed May
2021.
27) Cleveland Clinic. Pulmonary Nodules. Available at:
https://my.clevelandclinic.org/health/diseases/14799-pulmonary-nodules
Accessed May 2021.
28) Hirsch EA, New ML, Brown SL, Barón AE, Sachs PB, Malkoski SP.
Impact of a Hybrid Lung Cancer Screening Model on Patient Outcomes
and Provider Behavior. Clin Lung Cancer. 2020 Nov;21(6):e640-e646.
doi: 10.1016/j.cllc.2020.05.018. Epub 2020 May 23.
29) Morgan L, Choi H, Reid M, Khawaja A, Mazzone PJ. Frequency of
Incidental Findings and Subsequent Evaluation in Low- Dose Computed
Tomographic Scans for Lung Cancer Screening. Ann Am Thorac Soc.
2017 Sep;14(9):1450-1456. doi:
10.1513/AnnalsATS.201612-1023OC.
11. FINAL_7LCS Barriers Assessment 5.26.2021.pdf
Patient Barriers to Lung Cancer Screening Assessment
Client Name:
Patient Navigator Name/Clinic:
How to use this tool: This tool can guide conversations with
individuals who are eligible for lung cancer screening to help the
patient navigator identify potential actions and opportunities to
reduce barriers to care and increase screening rates.
It is not intended to be used as a stand-alone or self-administered
tool but instead to guide a patient-centered visit or
discussion.
When having a guided conversation with clients:
Client should be informed about how the information will be stored
and used.
Client should be informed that they can skip any questions they
feel are sensitive or private.
Patient navigator should use active listening and empathetic
communication, utilizing this tool as a guide for gathering helpful
information.
Personal Assets and Barriers to LCS
Awareness & Attitudes as Barriers to LCS
Attitude towards Smoking as Barrier to LCS
Optional Questions