Embed Size (px)
Citation preview

The birth of therapy withcultured cellsHoward Green
SummaryLong ago, I set out to solve a problem, but somethinghappened along the way: I was diverted by an unexpectedobservation. Thereafter, the direction of my research wasguided at each stage by increasing familiarity with theexperimental material and what could be done with it. Theresult was the birth of therapy with cultured keratino-cytes. Subsequent developments soon led to the for-mation of the company Biosurface Technology (latertaken over by the Genzyme Corporation), which providedautologous cultures for burn victims in many parts of theworld. Further progress by others led to new therapeuticapplications of cultured keratinocytes, such as treatmentof an ocular disease and gene therapy. Unfortunately,there have developed serious regulatory problems thatare a danger to future progress. As described in thisbrief history, the initial stages of development of celltherapy for the treatment of human disease were possibleonly because there was no restraint by committeesor governmental regulations. BioEssays 30:897–903,2008. � 2008 Wiley Periodicals, Inc.
The beginnings of keratinocyte cultivation
In 1974, I had no intention of studying therapy with cultured
cells or the treatment of human burns. At that time, current
thinking was that much could be learned about embryogenesis
from the study of cultivated murine teratomas. In general, this
hope was not fulfilled, but for me, studying cultures of a serially
transplantable teratoma derived by Leroy Stevens,(1) turned
out to be a very fruitful enterprise.
In the course of these studies, whose purpose had nothing
to do with what followed, my graduate student James
Rheinwald and I noticed that when the teratoma cells were
cultivated, some of them gave rise to interesting colonies of
epithelial appearance against a background of what appeared
to be fibroblasts. We attempted to obtain the epithelial cells in a
pure state, but we were unsuccessful because the isolated
cells grew very poorly. In order to support their growth, we
added lethally irradiated cells of the fibroblast line 3T3 that
had been made in my laboratory years earlier.(2) Under these
conditions, the epithelial cells grew quite nicely (Fig. 1). The
ability of 3T3 cells to support growth of an epithelial cell type
turned out to be specific for fibroblasts;(3,4) it was not simply
the result of increasing the cell density.
What was the nature of these epithelial cells that grew out of
the teratomal cultures? When sections through colonies were
examined by electron microscopy, they showed the presence
of desmosomes, keratohyalin granules and aggregated
tonofilaments.(4) These are features of the keratinocyte, the
principal cell type of stratified squamous epithelia, such as the
epidermis.
If, by adding 3T3 cell support, we could grow very well in
culture keratinocytes derived from a murine teratoma, could
we do the same thing with human keratinocytes, which I knew
had never been grown to an appreciable extent in cell culture?
We obtained a fragment of human skin, dissociated the
cells and put them into culture with 3T3 support.(5) Rapidly
growing colonies formed from single cells (Fig. 2). Successive
improvements in the cultivation made the keratinocyte the
most proliferative of all cultured human cell types.(6–11)
Starting with the cells of a small biopsy, we could now generate
in culture a number of epidermal cells sufficient to cover the
entire body of a human.
How to apply the cells?
We then developed a method of making a graft out of a
confluent sheet of cultured keratinocytes, using the enzyme
Dispase. This neutral protease has the property of breaking
the attachments of the cells to the surface of the dish without
affecting the junctions between adjacent cells. The confluent
sheet detaches intact.(12)
The next step was obviously to determine whether a
Dispase-detached sheet of human keratinocytes could engraft
on an animal.(13) We prepared such sheets, grafted them
to wounds prepared on athymic mice and showed that
they generated a human epidermis (Fig. 3). This was evident
from the greater thickness of the epidermis seen in histo-
logical sections and proven by reaction of that epidermis with
antibody specific for a human envelope precursor,(14) later
called involucrin.(15)
Having learned that we could grow vast amounts of such
cultures and that they could engraft successfully on a mouse,
we had to ask: could such a culture prepared from the residual
skin of a human whose epidermis had been extensively
destroyed by a burn be used to regenerate that epidermis?
Department of Cell Biology, Harvard Medical School, Harvard Medical
School, 240 Longwood Ave, Boston, MA 02115.
E-mail: [email protected]
DOI 10.1002/bies.20797
Published online in Wiley InterScience (www.interscience.wiley.com).
BioEssays 30:897–903, � 2008 Wiley Periodicals, Inc. BioEssays 30.9 897
Roots

The beginnings of human therapy
The first therapy of humans with third degree burns using
autologous cultures was performed on two patients at the
Peter Bent Brigham Hospital in 1980. The decision to carry
out this therapy was made by Dr. Nicholas O’Connor, Director
of the Burn Unit and myself. Before making that decision, we
discussed the possible risks, not with any committee (there
was none), but with individual colleagues who were located in
different institutions and whose judgment we respected. What
we heard from them supported our decision to proceed.
Small skin biopsies were taken from the patient, the
epidermal cells were cultivated in my laboratory and the
Dispase-detached grafts were applied to prepared wound
surfaces. The grafts generated epidermis on both patients.
One of the patients, a 61-year old man, had sustained partial
and full-thickness burns over 40% of his body surface. The
dorso-lateral surface of his left arm was excised to fascia
and numerous cultured grafts were applied. The patches
of regenerated epidermis resulting from the application of
circular (Petri dish) cultures are easily visible against
the background of the excised surface (Fig. 4). Successive
applications of such cultures resulted in complete coverage of
the arm.(16)
The next advance in the use of autologous cultures for
therapy of burns was the demonstration that large-scale use
of the method could be life saving.(17) Five- and six-year old
brothers in Wyoming sustained flame burns over 97 and
98 percent of their body surface. Of the burned areas, 83 and
89 percent were of third degree. Dr. John Remensnyder,
Director of the Shriners Burns Institute of Boston, informed me
that the two brothers had no chance of survival with conven-
tional treatment but if I would try to save them with cultured
cells, he would accept the brothers in transfer from Wyoming.
Although I was not prepared for the scale of the necessary
cultivation, I agreed and both brothers were grafted with
cultures of autologous epidermis. The application of the
cultures to the surface of the abdomen of one of the brothers
and the complete regeneration of the skin 14 weeks later is
shown in Fig. 4. Both brothers survived the terrible suffering of
the temporary skinless state and lived for over 20 years before
they died of complications not directly related to their burns.
Soon after, the regeneration of the skin resulting from
the application of cultured grafts was thoroughly studied by
Compton et al.(18) Prior to this work, some surgeons believed
that a healthy epidermis depends on the dermis and that if
the dermis is destroyed, grafting of epidermal cells alone
cannot produce a durable epidermis.(19) The work by Compton
et al. showed conclusively that when epidermal cultures were
transplanted to a wound bed lacking dermis, the quality of the
resulting epidermis did not deteriorate over the long term.
Moreover, a fully regenerated dermis developed beneath that
epidermis.
Compton et al. studied the regeneration of the skin in
twenty-one patients of age 4 months to 18 years grafted with
autologous epidermal cultures. A fully stratified epidermis
developed very quickly after grafting, including the granular
and cornified layers. After a much longer period, rete ridges
appeared at the dermo-epidermal junction of the regenerated
skin and became progressively more normal over suc-
ceeding years. The sub-epidermal connective tissue was
remodeled to produce papillary and reticular dermis, with fine
collagen fibers in the sub-epidermal region and thicker fibers
below. After one or two years, the number and size of the
anchoring fibrils closely resembled those of normal skin. All of
the characteristic features of the dermis continued to improve
Figure 1. Clones of XB cells, an epithelial cell line derived
from a murine teratoma, growing on a layer of lethally irradiated
3T3 cells.
Figure 2. Colonies of human epidermal keratinocytes
stained with rhodamine.
Roots
898 BioEssays 30.9

with time. Five years after grafting, the dermis appeared
completely regenerated (Fig. 5).
Similar results were obtained after grafting of a five year old
burn patient with epidermal cultures prepared in the laboratory
of Dr. Yann Barrandon, located at that time in Paris.(20,21)
For this treatment, the cultured grafts were prepared on a
detachable fibrin matrix, instead of by the older Dispase
method. I believe that this has been the only important
improvement in the preparation of autologous human kerati-
nocytes for grafting. The presence of 3T3 cells is still required,
but the fibrin-supported cultures have advantages over
Dispase-detached cultures for the treatment of burns.(21)
The time required to produce graftable cultures is shortened.
Fibrin-supported cultures are easier to prepare and easier to
use by the surgeon. Moreover, a fibrin substrate has been
essential for the grafting of human limbal cells.(22) The method
was developed entirely in France and Italy; to my knowledge, it
is not being used in the United States.
Studies of the stem cells of cultured
epidermal keratinocytes
At the time the early therapy with cultured keratinocytes
was carried out, there was not yet an understanding of the
necessity for the presence of stem cells in the cultured graft. A
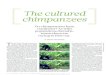
Figure 3. Human epidermis generated on an athymic mouse 108 days after application of a cultured human epidermal sheet. A: Note
thickness of generated human epidermis compared with mouse epidermis. Only the human epidermis stains with a specific antibody
to involucrin. B,C: Comparison of B with C shows that involucrin is present in only the outer, terminally differentiating layers of the
human epidermis generated from the culture. The thick stratum corneum, typical of the human but not of the mouse, is also shown in C. The
numbers and arrows in B and C indicate identical positions in cell layers stained for involucrin (B) and those revealed by
phase microscopy (C).
Figure 4. Left, regions of engraftment of Petri dish cultures of autologous epidermal cells to an excised surface of first human treated.
Center, abdomen of one of the brothers treated several years later by application of now rectangular grafts to abdominal surface excised to
muscle fascia; right, 14 weeks later, when the surface was covered with thick confluent epidermis.
Roots
BioEssays 30.9 899

method of analysis of proliferative capacity was developed a
few years later (23). Single cells were isolated from a strain
of keratinocytes and each cell was inoculated into a dish
containing supporting lethally irradiated 3T3 cells. Seven days
later, each growing colony produced by a founding cell was
isolated and trypsinized. The cells were transferred to
duplicate indicator dishes, again containing supporting 3T3
cells. Twelve days later, the cultures were fixed and stained.
From the appearance of the colonies in the indicator dishes,
we identified three clonal types of founding cells and classified
them as holoclones, meroclones or paraclones (Fig. 6). The
holoclone has the greatest proliferative capacity, giving rise to
fewer than 5% of terminal colonies. The paraclone has the
least proliferative capacity, as all the colonies abort and
terminally differentiate. The intermediate meroclone is a broad
category with considerable proliferative potential but less than
the holoclone. The evolution of clonal type is holoclone or
stem cell!meroclone! paraclone. Interest in stem cells on
the part of both scientists and lay public was destined to grow
enormously during subsequent years.
We also noted the decline in stem cell population with
age. In contrast to cultures derived from newborns, in which
28–31 percent of clones were holoclones, by age 64 the value
dropped to 3 percent and by age 78, to zero; only meroclones
and paraclones remained. It was shown later that the number
of holoclones in a cultured graft could be determined from the
number of cells possessing the DNp63 isoform a, since the
two were demonstrated to be closely correlated in humans of
different ages.(24)
Unanticipated but beneficial consequences
When scientific discovery opens up a new field of research, it is
impossible to anticipate where it may lead. I now wish to turn to
some unanticipated consequences of the discoveries that
I have just described.
We knew from early experiments on cultivating keratino-
cytes of all stratified squamous epithelia (esophageal, oral,
vaginal etc.) that corneal keratinocytes grew poorly on
subcultivation. The reason for this was elucidated in an
extremely important article from the laboratory of T.T. Sun.(25)
From an analysis of the keratins of corneal cells and the
surrounding limbal cells, as well as other data, the authors
postulated that the stem cells of the cornea were located in the
limbus, which surrounds the cornea and separates it from the
conjunctiva (Fig. 7).
Chemical burns of the eye, if they destroy the limbal stem
cells, can lead to a very nasty condition of inflammation,
pain and loss of vision. The limbus can be restored by grafts
from the healthy eye to the affected one.(26) This requires large
transfers of limbal tissue from the healthy eye. But limbal
stem cells belong to the same family as epidermal keratino-
cytes and can therefore be cultivated in the same way,
starting with a tiny biopsy. Thiswas first shown in the laboratory
of J. Rheinwald.(27)
A few years later it was demonstrated in the laboratory of
M. De Luca and G. Pellegrini, formerly in Venice and now in
Modena, that limbal cultures could be used therapeutically.
They took a 1–2 mm biopsy from the limbal region of the
healthy eye, grew the cells in culture, prepared a graft and
applied it to the suitably prepared injured eye.(28) Later, they
introduced the use of fibrin-supported limbal cultures and,
in collaboration with numerous ophthalmologists,(22) they
obtained relief of symptoms in 80% of over 100 patients. With
subsequent repair of deeper injury, vision could be totally
restored (Fig. 7).
Figure 5. The regenerated epidermis appears normal
with regularly spaced rete ridges (stars). The subepithelial
connective tissue is bilayered, with finer collagen bundles
superficially and coarser collagen bundles beneath, together
with normal vascular architecture (From Compton CC, Gill JM,
Regauer J, Gallico GG, O’Connor NE. 1989. Lab Invest 60:
600–612 with permission).
Figure 6. Colonies produced on indicator dishes by each of
the three founding clones. The holoclone gives rise predomi-
nantly to large colonies with smooth perimeters. The paraclone
gives rise to small colonies, with irregular perimeters, contain-
ing markers of terminal differentiation. The meroclone gives
rise to large and small colonies, many of which have irregular
perimeters.
Roots
900 BioEssays 30.9

Another unanticipated consequence of the work on
cultured keratinocytes was their use for gene therapy. This
discovery was another contribution of the laboratory of M. De
Luca and G. Pellegrini.(29) They studied a severe genetically
determined blistering disease of the skin—Junctional Epider-
molysis Bullosa. The patient that they studied was a double
heterozygote containing a frame shift/single point mutation in
the gene for Laminin 5-b3, which links basal epidermal cells to
the basement membrane.
They cultivated epidermal cells of the patient and trans-
duced them with a retroviral vector bearing a full-length Lam5-
b3 cDNA under control of the Moloney virus LTR. They then
removed some affected skin and replaced it with grafts of
transduced cells (all treatment with virus was ex vivo). As
shown in Fig. 8, the disease was cured.
Strangulation by regulation
Returning now to the beginning of this story, I remind you how
the decision to graft humans with cultured cells was made
in 1980 by Dr. Nicholas O’Connor and myself. By 1992, I was
unable to do any experiment on a mouse without approval by
a committee. Since that time, there has been continuous
increase in what has been called Regulation but might better
be called Strangulation. By this I mean that the ever-increasing
regulation threatens experimental work on new therapies with
cultured cells. I may summarize the situation in this way: if the
present regulatory climate in the United States had existed in
1980, I would never have pursued the development of therapy
with cultured cells.
The American regulatory authorities have classified cul-
tured epidermal grafts as xenografts (grafts derived from a
non-human species) because 3T3 (mouse) cells are used to
support the multiplication of the autologous keratinocytes. It
has been shown that, by the time the graft is prepared,
there are very few remaining 3T3 cells. More importantly,
all the 3T3 cells are lethally irradiated and could not possibly
engraft. In addition, in 1990, our 3T3 cultures were exhaus-
tively tested and shown to be free of pathogens. After the
cultured autologous epidermal cells had been made available
to patients for 10 years, the regulatory authorities decided that
they must determine that the product does not pose an
unreasonable or significant risk of illness or injury. Of course,
no consideration was given to the fact that, since the birth of
therapy with cultured epidermal cells in my laboratories
twenty seven years ago and after its extensive use in the US,
France and Italy, no example could be cited of a harmful
effect resulting from the use of these ‘‘xeno’’ grafts. Such
considerations apparently did not influence the regulatory
authorities. What if, they said, even a tiny number of irradiated
3T3 cells remain on the surface of the grafted person so that
they could support the growth of a mouse virus? All this is the
result of a fevered collective imagination.
Another consequence of this exaggerated concern over
hypothetical dangers is a tendency to move the field toward
other methods of cultivation that do not require 3T3 cells.
Actually, after many years of use of 3T3-supported cultures for
preparing grafts, a medium containing bovine products, but not
3T3 cells, was invented for cultivation of human keratinocytes.
It is a useful method for many experiments but the proliferative
capacity of the keratinocytes is not nearly as well preserved
as in 3T3-supported cells. As I have described above, in the
preparation of autologous grafts, it is essential to preserve the
stem cells to the maximum degree possible. For this reason,
the 3T3 cells cannot as yet be dispensed with. It is a disservice
Figure 7. A: From Schermer A, Galvin S, Sun TT. 1986. J Cell
Biol 103:49–62with permission;B: before treatment;C: 5 years
after graft of limbal culture and 4 years after corneal transplant
to remove stromal scarring (De Luca et al.).(24)
Roots
BioEssays 30.9 901

to the field to press for a change, where no suitable alternative
exists.
Recently, several changes have taken place in the re-
gulatory situation in various countries. At the end of 2002,
Tego Science, in Seoul, Korea received Marketing Approval for
their autologous cultured epidermal cells (Holoderm) for the
treatment of burns and nevi, and for scar revision.
On October 3, 2007, the Japanese Ministry of Healthcare,
Labor and Welfare publicly announced its regulatory approval for
cultured autologous epidermal grafts for the treatment of burns
by the Japan Tissue Engineering Company (J-TEC) in Aichi,
Japan.
On October 29, 2007, after twenty years of ‘unapproved’
use, the Genzyme Corporation in Boston, Massachusetts,
unexpectedly received FDA Marketing Approval for its cultured
autologous epidermal grafts (Epicel) for the treatment of burns.
Conclusion
I have described how the research that gave birth to therapy
with cultured cells was unplanned and was guided by the
new possibilities that developed at each stage of the work.
From the use of cultured keratinocytes for the treatment of
burns, practical applications were extended in the laboratory
of Professors De Luca and Pellegrini to the unanticipated
therapeutic use of cultured limbal cells to repair corneal
defects and the use of epidermal keratinocytes for gene
therapy of inherited blistering diseases. Many investigators
throughout the world are now attempting to use cultured cells
for other therapeutic purposes, some more realistically than
others. One group I would specially like to mention is that of
Dr. Anders Lindahl and his collaborators in Gothenburg, who
developed a therapeutic use for cultured chondrocytes.(30)
The use of such cells for therapy of cranio-facial deformities
Figure 8. A: Untreated region. Arrows indicate blisters. B: Excisions followed by application of grafts. C: 8 days after grafting. D: 60 days
after grafting. Hatched line in D corresponds to hatched line in A. (From Mavilio F, Pellegrini G, Ferrari S, Di Nunzio F, Di Iorio E, et al. 2006.
Nat Med 12:1397–1402 with permission.)
Roots
902 BioEssays 30.9

has also been successful.(31) With respect to dangers, there
can be no progress in therapy without some risk, but regulatory
committees have not dealt realistically with the problem. It
should be the primary responsibility of those scientists and
clinicians who know the subject best to evaluate that risk, in
consultation with individual colleagues whose opinions they
respect.
Acknowledgments
Based in part on a lecture to the European Academy of
Sciences in Brussels, September 12, 2007.
References1. Stevens LC. 1970. The development of transplantable teratocarcinomas
from intratesticular grafts of pre- and postimplantation mouse embryos.
Dev Biol 21:364–382.
2. Todaro G, Green H. 1963. Quantitative studies of the growth of mouse
embyro cells in culture and their development into established lines.
J Cell Biol 17:299–313.
3. Green H, Rheinwald JG, Sun TT. 1977. Properties of an epithelial cell
type in culture: the epidermal keratinocyte and its dependence on
products of the fibroblast. In: Revel JP, Henning U, Fox CF, editors. Cell
Shape and Surface Architecture. NY: Alan R. Liss, Inc. p 493–500.
4. Rheinwald JG, Green H. 1975. Formation of a keratinizing epithelium in
culture by a cloned cell line derived from a teratoma. Cell 6:317–
330.
5. Rheinwald JG, Green H. 1975. Serial cultivation of strains of human
epidermal keratinocytes: the formation of keratinizing colonies from
single cells. Cell 6:331–343.
6. Allen-Hoffmann BL, Rheinwald JG. 1984. Polycyclic aromatic hydro-
carbon mutagenesis of human epidermal keratinocytes in culture. Proc
Natl Acad Sci USA 81:7802–7806.
7. Green H. 1978. Cyclic AMP in relation to proliferation of the epidermal
cell: a new view. Cell 15:801–811.
8. Peehl DM, Ham RG. 1980. Clonal growth of human keratinocytes with
small amounts of dialyzed serum. In Vitro 16:526–540.
9. Rheinwald JG, Green H. 1977. Epidermal growth factor and the multi-
plication of cultured human epidermal keratinocytes. Nature 265:421–
424.
10. Simon M, Green H. 1985. Enzymatic cross-linking of involucrin and other
proteins by keratinocyte particulates in vitro. Cell 40:677–683.
11. Wu YJ, Parker LM, Binder NE, Beckett MA, Sinard JH, et al. 1982. The
mesothelial keratins: a new family of cytoskeletal proteins identified in
cultured mesothelial cells and nonkeratinizing epithelia. Cell 31:693–
703.
12. Green H, Kehinde O, Thomas J. 1979. Growth of cultured human
epidermal cells into multiple epithelia suitable for grafting. Proc Natl
Acad Sci USA 76:5665–5668.
13. Banks-Schlegel S, Green H. 1980. Formation of epidermis by serially
cultivated human epidermal cells transplanted as an epithelium to
athymic mice. Transplantation 29:308–313.
14. Rice RH, Green H. 1979. Presence in human epidermal cells of a
soluble protein precursor of the cross-linked envelope: activation of the
cross-linking by calcium ions. Cell 18:681–694.
15. Watt FM, Green H. 1981. Involucrin synthesis is correlated with cell size
in human epidermal cultures. J Cell Biol 90:738–742.
16. O’Connor NE, Mulliken JB, Banks-Schlegel S, Kehinde O, Green H.
1981. Grafting of burns with cultured epithelium prepared from
autologous epidermal cells. Lancet 1:75–78.
17. Gallico GG, O’Connor NE, Compton CC, Kehinde O, Green H. 1984.
Permanent coverage of large burn wounds with autologous cultured
human epithelium. N Engl J Med 311:448–451.
18. Compton CC, Gill JM, Bradford DA, Regauer S, Gallico GG, O’Connor
NE. 1989. Skin regenerated from cultured epithelial autografts on full-
thickness burn wounds from 6 days to 5 years after grafting. A light,
electron microscopic and immunohistochemical study. Lab Invest 60:
600–612.
19. Green H. 1989. Regeneration of the skin after grafting of epidermal
cultures [editorial]. Lab Invest 60:583–584.
20. Rochat A, Barrandon Y. 2006. Regeneration of Epidermis from Adult
Keratinocyte Stem Cells. In: Lanza R, Gearhart J, Hogan B, Melton D,
Pedersen R, Thomas ED, Thomson J, West M, editors. Essentials of Stem
Cell Biology. Boston: Elsevier Academic Press. p 439–447.
21. Ronfard V, Rives JM, Neveux Y, Carsin H, Barrandon Y. 2000. Long-term
regeneration of human epidermis on third degree burns transplant-
ed with autologous cultured epithelium grown on a fibrin matrix.
Transplantation 70:1588–1598.
22. Rama P, Bonini S, Lambiase A, Golisano O, Paterna P, et al. 2001.
Autologous fibrin-cultured limbal stem cells permanently restore the
corneal surface of patients with total limbal stem cell deficiency.
Transplantation 72:1478–1485.
23. Barrandon Y, Green H. 1987. Three clonal types of keratinocyte with
different capacities for multiplication. Proc Natl Acad Sci USA 84:2302–
2306.
24. De Luca M, Pellegrini G, Green H. 2006. Regeneration of squamous
epithelia from stem cells of cultured grafts. Regen Med 1:45–57.
25. Schermer A, Galvin S, Sun TT. 1986. Differentiation-related expression of
a major 64K corneal keratin in vivo and in culture suggests limbal
location of corneal epithelial stem cells. J Cell Biol 103:49–62.
26. Kenyon KR, Tseng SC. 1989. Limbal autograft transplantation for ocular
surface disorders. Ophthalmology 96:709–722; discussion 722–723.
27. Lindberg K, Brown ME, Chaves HV, Kenyon KR, Rheinwald JG. 1993. In
vitro propagation of human ocular surface epithelial cells for trans-
plantation. Invest Ophthalmol Vis Sci 34:2672–2679.
28. Pellegrini G, Traverso CE, Franzi AT, Zingirian M, Cancedda R, De Luca
M. 1997. Long-term restoration of damaged corneal surfaces with
autologous cultivated corneal epithelium. Lancet 349:990–993.
29. Mavilio F, Pellegrini G, Ferrari S, Di Nunzio F, Di Iorio E, et al. 2006.
Correction of junctional epidermolysis bullosa by transplantation of
genetically modified epidermal stem cells. Nat Med 12:1397–1402.
30. Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L.
1994. Treatment of deep cartilage defects in the knee with autologous
chondrocyte transplantation. N Engl J Med 331:889–895.
31. Yanaga H, Yanaga K, Imai K, Koga M, Soejima C, Ohmori K. 2006.
Clinical application of cultured autologous human auricular chondro-
cytes with autologous serum for craniofacial or nasal augmentation and
repair. Plast Reconstr Surg 117:2019–2030; discussion 2031–2032.
Roots
BioEssays 30.9 903