Embed Size (px)
Citation preview

Breast Cancer Research and Treatment, 2, 363-374 (1982) 0167-6806/82/020363-12 $0.20 © 1982, Martinus Nijhoff Publishers, The Hague, Printed in the Netherlands
Scandinavian Breast Cancer Symposium
The biology and physiology of 'Nolvadex'* (tamoxifen) in the treatment of breast cancer
John Patterson a, M.B., Barry Furr b, Ph.D., Alan Wakeling b, Ph.D., and Linda Battersby c, M.A. Clinical Research, b Bioscience 1, C Medical, Departments of Imperial Chemical Industries PLC, Mereside,
Alderley Park, MacclesJield SKIO 4TG, Cheshire, UK
Keywords: antioestrogen, breast, cancer, receptor, review, tamoxifen
Summary
After more than a quarter of a million patient years experience with tamoxifen in the clinic, it is perhaps appropriate to re-examine the working hypothesis for the activity of this drug. This hypothesis states that tamoxifen is an anti-oestrogen which exerts its anti-tumour activity by competing for and binding to cytoplasmic oestrogen receptor protein in the tumour.
The evidence that tamoxifen is an anti-oestrogen in animals and man is seen to vary from species to species and between target organs within a species. The balance of the evidence supports the conclusion that this drug acts as an oestrogen antagonist in man.
If the activity of this drug were confined to an effect mediated by the oestrogen receptor (ER), there should be a clear correlation between the anti-tumour effect of tamoxifen and the presence of ER. The clinical and pre-clinical data are reviewed. Whilst the majority of the evidence points to an effect in advanced breast cancer mediated through the ER, there are data that show the correlation is not absolute. The data are examined and the evidence for non-receptor mediated anti-tumour activity is reviewed.
We conclude that whilst the majority of the activity of tamoxifen is that of an anti-oestrogen mediated through the ER, compelling evidence exists that this may not be its only anti-tumour activity at normal clinical doses. These findings might explain tamoxifen's activity in some ER negative tumours.
Introduction
The advent of non-steroidal endocrine therapy for breast cancer coincided with the discovery of a specific oestrogen receptor protein (ER) in the cytoplasm of some breast tumour cells. This re- ceptor protein was shown to bind both the naturally occurring oestrogens and the synthetic triphenyl-
ethylene compounds, of which tamoxifen is the most widely used example. It was found that tamoxifen could antagonise oestrogen-induced cellular proliferation and it and its congeners were termed anti-oestrogens. A working hypothesis was developed which postulated (1) that tamoxifen (and all 'anti-oestrogens') exhibited their anti-tumour activity through the ER and might therefore be
* 'Nolvadex' is a trade mark, the property of Imperial ChemicaI Industries PLC.
Addressjbr reprints: J.S. Patterson, ClinicaI Research Dept., Imperial Chemical Industries PLC, Mereside, Alderley Park, Macclesfield SK10 4TG, Cheshire, UK.
364
expected to be inactive in its absence. Tamoxifen has been available and widely used in
the medical management of breast cancer for a number of years. A considerable amount of in vivo, in vitro, and ex vivo data has accumulated, and the hypothesis will be examined in the light of the currently available evidence.
The activity of tamoxifen in three distinct areas may be considered when examining this hypothesis. These considerations are: (1) the evidence that tamoxifen is an oestrogen antagonist in animals and man; (2) the evidence that this drug may exert its anti-tumour effect indirectly through an alteration in the hormonal milieu; (3) the correlation between turnout oestrogen receptor status and clinical re- sponse to tamoxifen therapy.
Is tamoxifen an oestrogen antagonist?
None of the currently available anti-oestrogens is a pure antagonist devoid of oestrogenic properties (2). Tamoxifen is no exception to this general rule.
Studies of the drug in vitro avoid the problems of metabolism in the whole animal (3). Lippman (4, 6) showed tamoxifen to be anti-oestrogenic in MCF-7 cell lines at low concentrations. This effect was completely reversed with a lower concentration of oestradiol. The ZR 75-1 cell line, grown in serum- free conditions (6, 7), confirmed the MCF-7 find- ings, and both cell lines showed that, in the absence of oestradiol, tamoxifen was able to inhibit growth below control levels and cause cell death. Thus tamoxifen appeared to be having an effect on the oestrogen sensitive cells that could not be explained simply by competitive inhibition of oestradiol. At the concentrations and conditions used, Lippman found no evidence of anti-tumour activity on cell lines which did not contain the receptor protein, and concluded that the effect was mediated through the ER.
There is no evidence that tamoxifen acts as an agonist in MCF-7 cells when growth is the end- point, However, Horwitz (8) has studied the ago- nist effects of tamoxifen in MCF-7 cells on pro- gesterone receptor synthesis, a marker of oestrogen action. There was clear evidence of agonism at low
concentrations which had disappeared by I#M, when tamoxifen suppressed progesterone receptor synthesis and cell growth and was thus behaving as a complete oestrogen antagonist.
Rochefort (3), using a different parameter, the 46K secretory protein, could only show pure antag- onist activity for tamoxifen, given in a 102-104 molar excess over oestradiol. Thus, even in one cell system, in vitro, the agonist/antagonist ratio of tamoxifen is dependent on the conditions and the parameters measured.
The animal pharmacology has been compre- hensively reviewed elsewhere (1, 9, 10) and the activity ranges from full agonism to pure antag- onism. The rat uterus is a good example of the difficulties in this area. Anti-oestrogens appear to be partial agonists in this organ (11). However, the increase in organ weight is not paralleled by a rise in DNA content (10), and hypertrophy is seen in contrast to the hyperplasia induced by oestradiol (12). The response is qualitatively and quanti- tatively different from that induced by oestradiol in spite of the induction of progesterone receptor that has been shown by Jordan (10) to occur without DNA induction.
Thus, the interaction of tamoxifen with ER containing tissues can give rise to a spectrum of activity that is complex and qualitatively and quan- titatively different from that produced by oes- tradiol. The relevance of these systems as predictors of tamoxifen's activity in humans must be open to question.
The human data show a predominance of anti- oestrogenic effects and have also been recently reviewed (9). The effects on the vagina typify the morphological changes that are seen. Preme- nopausal women with fully oestrogenised vaginae show anti-oestrogenic effects (13). In postme- nopausal women, Ferrazzi (14) reported a partial agonist effect in the majority of a group of postme- nopausal women while Estevez (15) saw mainly anti-oestrogenic or no effects. Bonte (16) reported oestrogenic effects on the vagina but anti-oestro- genic effects on the endometrium in the same patients.
Further data illustrating the overall effect of an anti-oestrogen in man are derived from the side
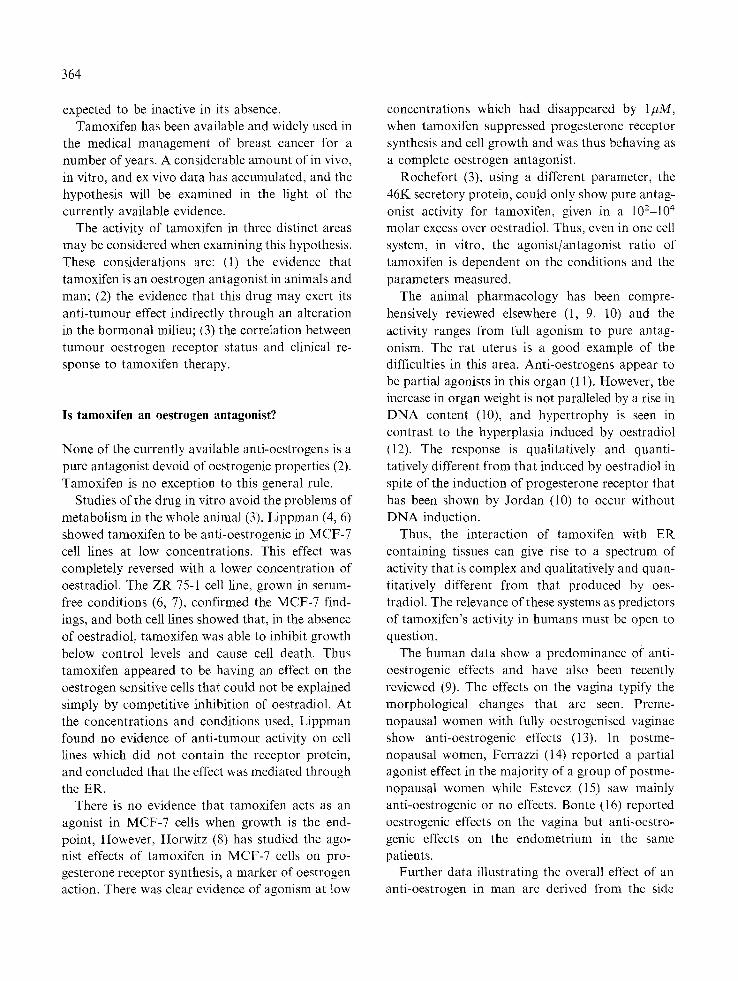
effect profile. Side effects of oestrogen have been well studied and documented (17). The most com- mon side effects of tamoxifen are shown in Table 1. Less than 3~ of patients in a large series (18) could not tolerate therapy, and the side effect profile is a clear manifestation of the anti-oestrogenic effects of the drug with the classical oestrogenic problems seen in few of the patients (22 with mild fluid retention compared with 194 cases of hot flushes).
Thus, the human and animal data suggest that tamoxifen is, on balance, an anti-oestrogen. Its anti-tumour properties may be either directly or indirectly mediated.
Does an oestrogen antagonist influence tumour growth indirectly through the endocrine milieu?
A number of authors have investigated the effects of tamoxifen on circulating hormones. These data (9), in summary, show that anti-oestrogens cause changes in circulating steroid and peptide hor- mones. These changes may account for part of the anti-tumour activity, but it seems unlikely that they represent the major effect on breast cancer cells as they can show markedly differing trends in pre- and postmenopausal women and males whilst a con- sistent anti-tumour effect is seen. It is possible that more subtle changes in the environment of the tumour cell may account for the indirect activity, but no clear evidence of this is currently available.
Table 1. Most common side effects of tamoxifen and their relation to withdrawal of therapy. Data from 2232 patients.
No. % % Withdrawal
Nausea/vomiting 207 (9.3) Hot flushes 194 (8.7 Thrombocytopenia 61 (2.7 Tumour flare 50 (2.2 Leukopenia 29 (1.3 Fatigue 28 (1.2 Hypercalcaemia 27 ( 1.2 Depression 25 (1.1 Rash 24 (1.1 Fluid retention 22 (1.0 Vaginal bleeding 22 (i.0 Vaginal discharge 18 (0.
(1.1) (o) (o.1) (0.4) (o) (o) (0.2) (o) (o) (o) (o) (o)
365
Is there a direct anti-tumour effect mediated through the ER?
Many papers have been published which provide detailed biochemical mechanisms for the blockade of cytoplasmic ER and subsequent interference with nuclear events by tamoxifen (1, 19, 20). Much has now been published on the correlation of therapeutic response to endocrine therapy with the presence of ER. We have reviewed the available published data on tamoxifen.
Forty studies are available for analysis (21 60). it is a striking feature that many of the investigators report on small numbers of patients and that the number available for analysis is miniscule in com- parison to the total patient population exposed to tamoxifen. This could reflect a number of things, including the inaccessibility of tumour in many patients with advanced cancer, the lack of a wide- spread ER assay service, or failure of those labora- tories who undertake assay services to report re- trospective correlations with therapeutic results. In the 40 studies analysed here in Tables 2 and 3, the value of the cut-off point was defined by the individual laboratory and varied between 1 fmol and 20 fmol per mg of cytosol protein. Eight of the publications (26, 27, 33, 46, 51, 55, 57, 58) define a borderline zone. These data are not displayed separately as they involve a small number of tu- mours.
The criteria for response in these data were those or similar to those published by the UICC (61) in 36/40 (90~) of the publications, and care has been taken to avoid duplicating any patient whose data were published on more than one occasion. These data show that the complete and partial response rate in ER positive tumours was 47~, which is significantly better than the 33% seen in an un- selected patient population (18). The 10% of re- ceptor negative patients showing a complete or partial response cannot be ignored; this finding raises some questions as to the clinical utility of the ER assay.
These doubts are strengthened when the patients who entered the no change category are also as- sessed. The data in Table 3 show that the addition of this group whose disease failed to progress

366
Table 2. Advanced breast cancer. Response to 'Nolvadex' with respect to tumour oestrogen receptor (ER) status.
Investigator Definition ER positive ER negative of ER positive
( C R + P R ) / ( C R + P R + ( C R + P R ) / ( C R + P R + Total NC)/Total Total NC)/Total
Lerner (2 l) > 1 fmol/mg protein 9/13 11 / 13 0/4 1/4 Morgan (22) > 10 11/25 0/6 Manni (23) > 3 31/49 3 l/49 0/6 0/6 Brule (24) NS 5/19 13/19 1/7 4/7 Rose (25) >20 10/21 - 2/19 - Kiang (26) > 10 6/10 - 0/10 Roberts (27) > 10 6/24 2/8 Cheix (28) NS 16/38 23/38 4/17 7/17 Barnes (29) > 5 10/18 12/18 4/29 6/29 Heuson (30) > 10 2/6 0/1 Westerberg (3.1) >0.03 fmol//~g DNA 12/18 1/17 Leclerq (32) NS 2/2 - 0/1 - O 'Connor (33) > 10 fmol/mg protein 12/23 - 0/6 - Plotkin (34) NS - 10/I 7 1/8 Saez (35) NS 13/34 1/14 - Legha (36) NS 3/4 4/4 1/2 1/2 Wada (37) NS 8/13 - 1/15 - Wiggans (38) NS 8/29 13/29 0/3 0/3 Bloom (39) > 7 fmol/mg protein 11/20 - 0/5 - Arnold (40) NS 8/24 14/24 0/12 3/12 Koenders (41) NS 10/20 0/9 - Bishop (42) NS 11/18 7/25 Stewart (43) NS 7/18 - 0/5 Rainer (44) > 15 9/12 - 1/4 - Allegra (45) > 10 11/19 0/7 - De Lena (46) NS 3/20 10/20 1/3 1/3 Tominaga (47) NS 2/4 3/4 0/3 I/3 Nomura (48) > 2 4/9 - 0/6 Holdaway (49) > 5 14/20 2/19 - Margreiter (50) NS 6/25 17/25 0/22 5/22 Morimoto (51) > 15 6/7 1/8 - Van Maillot (52) > 15 18/27 - 0/9 Rubens (53) > 5 4/20 1/10 - Fabian (54) NS 1/6 4/6 0/5 0/5 Nagai (55) NS 4/7 4/7 2/7 4/7 Beex (56) >5 7/13 0/7 - Hanshin (57) NS 7/20 15/20 4/13 7/13 Pritchard (58) NS 5/12 6/12 0/8 1/8 Wada (59) NS 4/4 0/6 - Kobayashi (60) NS - 0/4 0/4
NS = not stated CR = complete remission PR = partial regression NC = no change (stabilisation)
- = data not available

Table 3. Response to 'Nolvadex' in advanced breast cancer with respect to ER status.
ER positive ER negative
Responders/Total Responders/Total (%) (%)
CR+PR 316/671 (47) 36/362 (10) CR+PR+NC 190/305 (62) 42/153 (27)
increases the predictivity of a positive receptor assay to 62~ but shows that 1 in 4 patients who are assessed to be ER negative will get some benefit from anti-oestrogen therapy. Whilst there are a number of reasons why a receptor-rich tumour may not respond to an anti-oestrogen, it is of greater interest to focus on the response in the receptor- poor group, as many clinicians use this finding as a clinical contra-indication to endocrine therapy with an anti-oestrogen.
Reasons why tamoxifen may be effective in patients with oestrogen receptor negative tumours
Reliability of oestrogen receptor (ER) assays
If it is assumed that only ER positive tumours will respond to tamoxifen, and that approximately 50% of ER positive patients respond, then the 10~ good response rate in ER negative patients implies that at least 20% of ER positive tumours are incorrectly classified as ER negative. It is crucial to have some estimate of assay reliability to indicate whether method failure could account for such a high level of error. A wide variety of methods have been used for ER assay (62), but the most commonly applied is the dextran-coated charcoal method (63). Despite attempts to establish standard procedures (64) and the recent introduction of quality control pro- cedures (65 67), serious limitations remain (68). In addition, a wide variation in ER content has been observed in histologically comparable portions of the same tumour (62); a range as large as 0-300 fmol/mg protein has been reported (68).
Collection, transport and storage of tumour specimens can also have a very profound effect on
367
apparent ER content. For example, it has been reported (69) that transport in liquid nitrogen, compared to solid CO2, increases the proportion of ER positive assays (69~ vs 56~) with a correspond- ing decrease in ER negative assays. A recent report (70) shows that, in 38 tumours analysed after immediate freezing in liquid nitrogen or after being left at room temperature for 1 hour before freezing, 5 of 25 tumours analysed as ER positive after immediate freezing were analysed as ER negative when freezing was delayed. It is clear that practical and technical limitations profoundly affect the validity of present ER assays. These difficulties are of sufficient magnitude to account for at least some of the apparent discrepancies in correlation be- tween ER status and clinical response.
Nearly all ER data so far reported refer to cytosol receptor status (ERc). Stimulation of tu- mour growth by oestrogens requires binding of the hormone to ERc, receptor activation, and translo- cation to the nucleus (ERn) to promote gene transcription. Deficiencies in one or more of this complex sequence of events may occur in breast tumours, and account for at least some of response failures in ERe positive patients. Measurement of progesterone receptors in addition to ERe has been suggested to improve clinical correlation and this has met with some success (71).
Measurement of ER, may also improve clinical correlation (72) and has revealed that a small proportion (9%) of postmenopausal women are ER~ negative but ERn positive. It is possible that these women might derive benefit from tamoxifen therapy by direct binding of the anti-oestrogen to the nuclear receptors. These patients have a prog- nosis better than that of ER~ negative/ERn neg- ative patients (73). Receptor status of primary breast cancer has important prognostic impli- cations; ER~ positive patients generally experience a longer disease-free interval (74, 75). It has been recently shown, however, that if both ERe and ERn are measured there is only a 63% concordance between receptor status in primary and secondary disease (72). To base treatment decisions in ad- vanced breast cancer solely on ER status of primary disease is questionable for all of the reasons given above.

368
Effects o f tamoxifen on human mammary tumours in culture
It has already been shown that tamoxifen will inhibit the growth of hormone-responsive human breast cancer cell lines such as MCF-7 (4) and ZR- 75 (76), both of which are ER positive. More recent data show that the effect of tamoxifen at 2 #M on cell growth can be completely reversed by oestradiol but at 6/~M no reversal is seen (77). This is good evidence that not all of the growth inhibitory effects of tamoxifen in vitro are mediated through the oestrogen receptor. Indeed it is not yet known whether cell death, as against inhibition of growth, is mediated by the oestrogen receptor. It is known that tamoxifen at 6 or 10 #M does prevent pro- gression of cells from Go/G1 into the S phase (78) and it is assumed that this changes the balance between cell growth and cell death so that cell death predominates. Of interest too is the finding that tamoxifen causes death of uterine gland cells in vivo in rats and that this effect is not reversed by oestrogen (79).
There is now evidence that tamoxifen will inhibit growth of ER negative breast cancer cells in culture (78). The EDso is around 6/~M and complete cell death is seen at 10 /~M concentrations. These investigations have shown that these concentrations of tamoxifen produce similar effects on the MCF-7 cell line. Similar results have been obtained using mouse A31 C2 fibroblasts which do not contain the oestrogen receptor. The increased [3H]-thymidine labelling index seen in response to high serum oestrogen concentrations is markedly inhibited by tamoxifen at 10 6M (L. Martin, University of Queensland, personal communication). Not all ER negative breast cancer cells respond to tamoxifen, however, since it has been shown that growth of G- 11, MDA-231, and HT-39 cells is not inhibited, although concentrations above 1/~M were not used (4).
Further evidence that tumours without oestrogen receptors will respond to tamoxifen both in vitro and in vivo is provided by very recent work (80). Mammary tumour explants were exposed to tam- oxifen in vitro and the results were correlated with the clinical response to therapy with tamoxifen and
the ER status in the same tumours. There was a good correlation between responses to tamoxifen in vitro and in vivo since of 11 tumours responding in vitro, 9 showed objective clinical response; of 10 unresponsive tumours in vitro 7 were unresponsive in vivo. The investigators found that 2 tumours which were ER negative did respond to tamoxifen in vitro and also showed an objective clinical response.
Effects on the androgen receptor
Unpublished work from our laboratory has shown that tamoxifen has a low affinity for the androgen receptor. Although the affinity is two orders of magnitude less than that of the natural ligand, 5c~- dihydrotestosterone, the relative binding affinity is not dissimilar to that oftamoxifen for the oestrogen receptor. Since androgen receptors are present in human breast tumour cells and androgen can stimulate growth (81), tamoxifen may exert in- hibitory effects on oestrogen receptor negative tu- mours through an androgen receptor system.
Eff'ects through the 'anti-oestrogen binding site'
An 'anti-oestrogen binding site', which binds tam- oxifen and 4-hydroxytamoxifen but is distinct from the oestrogen receptor, has been found in a number of tissues including human breast carcinoma cells (82) and cytosols prepared from human breast tumours (83). The term "anti-oestrogen binding site' is probably erroneous since it also binds the oestro- genic cis-isomer of tamoxifen, ICI 47699 (82).
Although the exact role for this binding site has yet to be determined there are two new pieces of evidence which suggest that it may be important in the regulation of tumour growth. Firstly, Jozan et al. (84) have isolated two clones of MCF-7 cells; the growth of one is inhibited by tamoxifen and that of the other is unaffected. Both clones have compara- ble oestrogen receptor concentrations but the tamo- xifen-resistant clone has significantly fewer anti- oestrogen binding sites. Of similar interest is the finding that ICI 145680, which has identical affinity to tamoxifen for the oestrogen receptor of MCF-7 cells (R.L. Sutherland, personal communication), is
at least as potent as tamoxifen in rat anti-iltero- trophic tests (ICI, unpublished results) but has no affinity for the 'anti-oestrogen binding site' and is also markedly inferior to tamoxifen in inhibiting growth of MCF-7 cells (R. L. Sutherland, personal communication).
These data suggest that tamoxifen, by binding to the 'anti-oestrogen binding site', may effect tumour growth even in tumours which do not contain oestrogen receptors.
Effects of hormonal steroids on cell growth not mediated by the oestrogen receptor
The effects of oestradiol (0.1 mg, i.m., daily) and progesterone (1 mg, i.m., daily) on [3H]-thymidine incorporation by explants of human breast tumours ex vivo have been studied (85). Biopsies were performed in 10 patients with multiple skin and soft tissue metastases before and at various times after treatment. These 'physiological' levels of steroid hormones caused an increase in [3HJ-thymidine labelling in tumours from 7 patients, three of which were ER negative; two of the latter tumours were also progesterone receptor negative. This finding is unlikely to be due to variations between biopsy specimens because biopsy specimens taken at 3, 6, and 9 days of treatment showed consistent values, and in simultaneous multiple biopsies from two patients the labelling varied by only 3 and 5% respectively.
This small study demonstrates that steroid hor- mones can exert effects on the regulation of growth of mammary tumours by a mechanism not involv- ing the oestrogen receptor. Although it is not known whether this is a direct effect on the tumour or an indirect stimulus mediated by another growth factor, it is conceivable that tamoxifen could in- terfere with this action.
Acute effects of tamoxijen
It has recently been shown that tamoxifen has acute effects on the responsiveness of rat myometrial strips in vitro to stimulation by oxytocin and prostaglandin F2~ (86). Tissue prepared from rats pretreated with oestradiol was stimulated with
369
oxytocin and tissue from animals given proges- terone was stimulated with prostaglandin F2~. Tamoxifen produced a dose-related inhibition of contraction over the range 10 7 to 10- 6M within 10 minutes of addition to the organ bath. Maximal effects were seen after 1-2 hours and the effect was reversible within 1-2 hours in drug-free medium. Since the effect could not be reversed by oestradiol (10-6M), and since the oestrogenic cis-isomer of tamoxifen, ICI 47699, behaves similarly to tam- oxifen, it is unlikely to be mediated by the classical oestrogen receptor.
This activity is probably due to a membrane effect of tamoxifen leading to perturbation of the membrane receptors for oxytocin and prosta- glandin F2~. Certainly membrane effects of tam- oxifen do occur" since Perris (personal communi- cation) has shown that tamoxifen, at concen- trations of 10 100 ng/ml, will block both calcium and magnesium-induced mitogenesis of thymic lymphocytes. Moreover tamoxifen will block the action of calcium and magnesium-dependent mi- togens in this system. Interestingly, oestradiol at similar concentrations will also block calcium-in- duced mitogenesis, and this may offer a partial explanation for the anti-tumour activity of pharma- cological doses of oestrogens.
There is evidence that hormones other than oestrogens influence the growth of breast tumours. Insulin (87, 88), pituitary hormones, and probably growth hormone (23, 89), stimulate growth through membrane receptors on the tumour cell. It is possible, therefore, that by exerting an effect on the cell membrane, tamoxifen may influence the ability of breast tumours to respond to these peptide hormone mitogens.
Effects on prostaglandin synthetase
There is evidence that tamoxifen, at comparable concentrations to aspirin, is an inhibitor of the prostaglandin synthetase complex in human mam- mary tumours (90). There is considerable con- troversy concerning the role of prostaglandins in the regulation of tumour growth, and evidence that they can both stimulate and inhibit tumour growth can be cited (91). Prostaglandins produced by some

370
tumours can cause bone erosion which would
facil i tate g rowth o f b o n y metastases; this effect can
be prevented in vi t ro by add i t ion o f p ros t ag land in
synthetase inh ib i to rs (92-95). There is cons iderable
evidence tha t inh ib i tors o f p ros t ag l and in p roduc-
t ion will l imit g rowth of t u m o u r cells and reduce
metas tas is (96 103).
M o r e o v e r there is evidence tha t p ros t ag l and in E
p roduc t ion by t umour s has an immunosuppress ive
effect and tha t inhib i tors o f p ros t ag land in synthesis
res tore the i m m u n e response and thereby re tard
t u m o r g rowth (104).
Thus, by act ing as an inh ib i tor of p ros t ag land in
synthetase, t amoxi fen has the poten t ia l to l imit
t u m o u r g rowth whether or not the t u m o u r pos-
sesses oes t rogen receptors .
Blood and tissue concentrations o f tamoxifen
It is c lear ly i m p o r t a n t to es tabl ish whether the
effects descr ibed above occur over the range of
concen t ra t ions found in b lood and tissues after
admin i s t r a t ion of t amoxi fen at clinical doses. Table
4 shows tha t mean s teady state concen t ra t ions o f
t amoxi fen in b l o o d f rom pat ien ts range f rom 141 to
300 ng/ml depend ing on the dose given.
Mean concen t ra t ions of t amoxi fen in breas t tu-
m o u r homogena t e s were 25.1 ng /mg pro te in (108).
Assuming a 10% pro te in conten t in the t u m o u r this
is equivalent to 6.7/~M. A n equal or greater a m o u n t
of the m a j o r N-desme thy l t amoxi fen metabol i te ,
also an an t i -oes t rogen , is l ikely to be present.
I t is clear, therefore, tha t t amoxi fen given at
2 0 4 0 mg dai ly, is present in b lood and tissues at
concen t ra t ions which are capab le of elicit ing the
effects descr ibed above.
Conclusions
The initial hypothes i s was tha t t amoxi fen and other
t r iphenyle thylenes were ant i -oes t rogenic com-
pounds which exhibi ted their an t i - t umour effect
t h rough the cy top lasmic ER. The ma jo r i ty o f the evidence would suppor t the hypothes is but there are
da t a to show tha t an t i -oes t rogenic effects are not
the only ac t ions of this drug. There is clinical
Table 4. Blood concentrations of tamoxifen in patients (the values given are the mean steady state values).
Dose Blood concentration ng/ml Reference
10 mg/m 2 260 105 20 mg b.i.d. 285 4- I5
(range 153-494) 106 10 mg b.i.d. 141 4- 20 107 20 mg b.i.d. 300 4- 162 108
(range 27a-520)
aThis patient probably showed poor compliance since the next lowest value was 146 ng/ml.
evidence tha t it can have an an t i - t umour act ion in a
p r o p o r t i o n of pa t ien ts who do not have ER in their
breas t t u m o u r and da t a are d isp layed tha t help to
account for this discrepancy. A t the concen t ra t ions
o f t amoxi fen c o m m o n l y found dur ing an t i - t umour
the rapy with this d rug it is not surpr is ing that some
ER negative t umour s are seen to show a clinical
response.
References
1. Furr BJA, Patterson JS, Richardson DN, Slater SR, Wakeling AE: Tamoxifen. In ME Goldberg (ed). Pharma- cological and Biochemical Properties of Drug Substances, Vol 2. Am Pharmaceutical Assoc, Washington, 1979, pp 355400.
2. Martin L: The biology of anti-oestrogens. Biochem Soc Trans 7: 551-556, 1979.
3. Rochefort M, Borgna JL, Coezy E, Vignon, Westley B: Mechanisms of action of tamoxifen and metabolites in MCF 7 human breast cancer cells. In RL Sutherland and VC Jordan (eds). Non-steroidal Antioestrogens - Molec- ular Pharmacology and Antitumour Activity. Academic Press, Sydney, 1981, pp 355 363.
4. Lippman ME, Bolan G, Huff K: Effects of estrogens and antioestrogens on hormone-responsive human breast can- cer in long-term tissue culture. Cancer Res 36: 45954601, 1976.
5. Lippman ME, Monaco ME, Bolan G: Effects of estrone, estradiol and estriol on hormone-responsive human breast cancer in long-term tissue culture. Cancer Res 37: 1901 1907, 1977.
6. Engel LW, Young NA, Tralka TS, Lippman ME, O'Brien S J, Joyce M J: Establishment and characterisation of three new continuous cell lines derived from human breast carcinomas. Cancer Res 38:3352 3364, 1978.
7. Lippman ME, Aitken SC, Allegra JC: Regulation of
growth and DNA synthesis by oestrogens and anti- oestrogens in human breast cancer cell lines. In: RL Sutherland and VC Jordan (eds). Non-steroidal Anti- oestrogens Molecular Pharmacology and Antitumour Activity. Academic Press, Sydney, 1981, pp 365 395.
8. Horwitz KB, Koseki Y, McGuire WL: Estrogen control of progesterone receptor in human breast cancer: role of estradiol and antiestrogen. Endocrinology 103: 1742 1751, 1978.
9. Patterson JS: Clinical aspects and development of anti- oestrogen therapy: a review of the endocrine effects of tamoxifen in animals and man. J Endocr 89: 67P-75P, 1981.
10. Jordan VC: The pharmacology of tamoxifen with special reference to the control of hormone-dependent cancer. In
MK Agarwal (ed). Antihormones. Elsevier/North Hol- land Biomedical Press, 1979, pp 235-252.
11. Harper MJK, Walpole AL: A new derivative of tri- phenylethylene: effect of implantation and mode of action in rats. J Reprod Fertil 13:101 119, 1967.
12. Clark ER, Dix CJ, Jordan VC, Prestwich G, Sexton S: A comparison at the cellular and subcellular levels, of the effects of tamoxifen and oestradiol benzoate on the immature rat uterus. Br J PharmacoI 62: 442P, 1978.
13. Tajima C, Tamaki Y, Takamizawa H: Trials of tamoxifen for the induction of ovulation. Acta Obstet Gynaecol Japan 29: 57-69, 1977.
14. Ferrazzi E, Cartel G, Mattarozzo R, Fiorentio M: Oes- trogen-like effect of tamoxifen on vaginal epithelium: Br Med J (6072) 1351, 1977.
15. Estevez RA, Breier S, Kotliar ML, Alvarez CA, Machado CG: Como otros antestrogenicos, el tamoxifen tiene propiedades anovulatorias y produce efectos antitu- morales en animales de laboratorio y humanos. In Proc 12th Int Cong Cancer, Buenos Aires, UICC Proc 12th Int Cong Cancer, Buenos Aires, 5-11 October, 1978.
16. Bonte J, Ide P, Billiet G, Synants P: Tamoxifen as a possible chemotherapeutic agent in endometrial adenocar- cinoma. Gynecol Oncol 11:140 161. 1981.
17. Stoll BA: In Hormonal Management of Breast Cancer. Pitman Medical Publishing Co Ltd, London, 1969, 54-67.
18. Patterson JS, Battersby LA: Tamoxifen: clinical pharma- cology, safety and clinical development. In Clinical Appli- cations in Oncology. Published as a special report by Custom Communications. Postgraduate Medicine, Mc- Graw-Hill Publications Co, October 1981.
19. Katzenellenbogen BS: Basic mechanisms of antioestrogen action. In WL McGuire (ed). Hormone Receptors and Breast Cancer. Raven Press, New York, 1981, pp 135-157.
20. Nicholson RI, Daniel P, Gaskell SJ, Syne JS, Davies P, Griffiths K: The biochemistry of tumour therapy of breast cancer. In MK Agarwal (ed). Antihormones. Elsevier/ North Holland, 1979, pp 253-267.
21. Lerner HJ, Band PB, Israel L, Leung S: Phase 11 study of tamoxifen: report of 74 patients with Stage IV breast cancer. Cancer Treat Rep 60:1431 1435, 1976.
371
22. Morgan LR, Schein PS, Woolley PV, Hoth D, Macdonald J, Lippman M, Posey LE, Beazley RW: Therapeutic use of tamoxifen in advanced breast cancer: correlation with biochemical parameters. Cancer Treat Rep 60:I437 1443, 1976.
23. Manni A, Trujillo JE, James SM, Brodkey J, Pearson OH: Antihormone treatment of Stage IV breast cancer. Cancer 43: 444-450, 1979.
24. Brule G: Co-operative clinical study of 178 patients treated with 'Nolvadex'. Proc Syrup Hormonal Control of Breast Cancer, Manchester, 1978, pp 35-39.
25. Rose C, Thorpe SM, Lober J, Daenfeldt JL, Palshof T, Mouridsen HT: Therapeutic effect of tamoxifen related to estrogen receptor level. In B Henningsen et al. (eds). Recent Results in Cancer Research. Springer-Verlag, Berlin, Heidelberg, New York, 1980, pp 134-141.
26. Kiang DT, Kennedy BJ: Tamoxifen (antiestrogen) thera- py in advanced breast cancer. Ann Int Med 87:687 690, 1977.
27. Roberts MM, Rubens RD, King RJB, Hawkins RA, Millis RR, Hayward JL, Forrest APM: Oestrogen re- ceptors and their response to endocrine therapy in advan- ced breast cancer. Br J Cancer 38: 431-436, 1978.
28. Cheix F, Pommatau E, Clavel M, Mayer M, Saez S: Cancer ~volue du sein: Correlations entre la presence de r~cepteurs d'estradiol et la r~ponse/~ un antiestrog~ne, le tamoxif~ne. Nouvelle Presse M~dicale 7: 3633-3635, 1978.
29. Barnes DM, Skinner LG, Ribeiro GG: Triple hormone- receptor assay: A more accurate predictive tool for the treatment of advanced breast cancer. Br J Cancer 40: 86~865, 1979.
30. Heuson JC, Longeval E, Mattheiem WH, Deboel MC, Sylvester RJ, Leclercq G: Significance of quantitative assessment of estrogen receptors for endocrine therapy in advanced breast cancer. Cancer 39:1971 1978, 1977.
31. Westerberg H, Nordenskjold B, Wrange O, Gustafsson J- A, Humla S, Theve NO, Silfversward C, Granberg P-O: Effect of antiestrogen therapy on human mammary car- cinomas with different estrogen receptor contents. Europ J Cancer 14: 619-622, 1978.
32. Leclercq G, Heuson JC, Deboel MC, Legros N, Longeval E, Mattheiem WH: Estrogen and progesterone receptors in human breast cancer. In W L McGuire (ed). Prog- esterone Receptors in Normal and Neoplastic Tissues. Raven Press, New York, 1977, pp 141-153.
33. O'Connor T, Rosenbaum C, Cardellicchio D, Cohen JL, Stolbach L: Estrogen receptor (ER) predicts tamoxifen response in advanced breast cancer. Proc 69th Meeting Am Assoc Cancer Res, C272: 374, 1978.
34. Plotkin D, Lechner JJ, Jung WE, Rosen PJ: Tamoxifen flare in advanced breast cancer. JAMA 240: 2644~646, 1978.
35. Saez S, Brunat M, Cheix F, Colon J, Mayer M: Estradiol and progesterone receptors in human breast tumors: prognostic significance in patients treated by ablative endocrine surgery. Reviews on Endocrine-Related Cancer, Suppl Apr 78: 37-50, 1978.

372
36. Legha SS, Buzdar AU, Hortobagyi GN, Wiseman C, Benjamin RS, Blumenschein GR: Tamoxifen use in treat- ment of metastatic breast cancer refractory to corn- bination chemotherapy. JAMA 242:49 52, 1979.
37. Wada T, Koyama H, Takahashi Y, Nishizawa I, Iwanaga T, Aoki Y, Terasawa T: Tamoxifen therapy in locally advanced primary and recurrent breast cancer. J Jap Soc Cancer Ther 14: 819-824, 1979.
38. Wiggans RG, Woolley PV, Smythe T, Hoth D, Mac- donald JS, Green L, Schein PS: Phase II trial of tamoxifen in advanced breast cancer. Cancer Chemother Pharmacol 3: 4548, 1979.
39. Bloom ND, Tobin EH, Schreibman BA, Degenshein CA: The role of progesterone receptors in the management of advanced breast cancer. Cancer 45: 2992-2997, 1980.
40. Arnold D, Hacker S, Markham M, Marucci C: Combined analysis of cytosol and chromatin associated estrogen receptor in prediction of response to tamoxifen. Proc AACR and ASCO 20: 348, 1979.
41. Koenders AJM, Beex LVM, Geurts-Moespot J, Benraad T J: Steroid hormone receptors in mammary carcinoma: the effect of tamoxifen. Breast Cancer Esp + Clin Aspects 616: 63-66, 1980.
42. Bishop HM, Nicholson R, Blamey RW, Eston CW: Oestrogen receptor in locally advanced breast cancers. Br Assn Surg Oncol and Br Assn Cancer Res, Joint Mtg, July 1979, p 41.
43. Stewart HJ: Edinburgh study on 'Nolvadex' (tamoxifen) against oestrogens. Reviews on Endocrine-Related Can- cer, Suppl 3, pp 51 55, 1979.
44. Rainer H, Morz R, Moser K, Bettelheim P, Bieglmayer C, Chaput B, Kolb R, Jakesz R, Micksche M, Reiner G, Spona J: Treatment of metastatic breast cancer with tarnoxifen. Proc l lth Int Congr Chemother, Boston, 674-675, 1980.
45. Allegra JC, Lippman ME: Estrogen receptor determi- nation predicts response to tamoxifen therapy. In B
Henningsen, F Linder, and C Steichele (eds). Endocrine Treatment of Breast Cancer. Springer Verlag, 1980, pp 16-19.
46. De Lena M, Brambilla C, Jirillo A: Tamoxifen efficacy in advanced breast cancer previously treated with endocrine and cytotoxic therapy. Tumori 66: 339-348, 1980.
47. Tominaga K, Kitamura M, Kaneko H, Hayashi K, Takahashi I, Ito K, Saito T: Effect of tamoxifen on advanced breast cancer. BasicPharmacol Ther 7:259 263, 1979.
48. Nomura Y, Yamagata J, Takenaka K, Tashiro H: Anti- estrogen (tamoxifen) therapy in advanced breast cancer with special reference to relation to estrogen receptor. Jap J Cancer Clinics 28: 340-343, 1980.
49. Holdaway IM: Oestrogen receptors and the response of metastatic breast cancer to aminoglutethimide or tam- oxifen. Aust NZ J Surg 51: 345-347, 1981.
50. Margreiter R: Die antioestrogene Substanz Tamoxifen in der Behandlung des fortgeschrittenen Mammacarcinoms.
Langenbecks Archiv f~r Chirurgie, Springer-Verlag,
249~62, 1980. 51. Morimoto T, Sonoo H, Kakuta E, Fujiwara H, Kitamura
M, Nishiyama F, Inoue M, Inoue K: Tamoxifen therapy in advanced and recurrent breast cancer. Cancer Chem- other 8: 111-118, 1981.
52. yon Maillot K, Gentsch HH, Gunselmann W: Steroid receptors and response to endocrine treatment and chemo- therapy of advanced breast cancer. J Cancer Res Clin Oncol 98: 301-313, 1980.
53. Rubens RD, Stewart JF, King RJB, Minton M J, Sparrow GEA, Knight RK: Primary endocrine therapy + predni- solone in advanced breast cancer. Proc AACR and ASCO Abs C404: 436, 1981.
54. Fabian C, Sternson L, E1-Serafi M, Cain L, Hearne E: Clinical pharmacology of tamoxifen in patients with breast cancer. Cancer 48:876 882, 1981.
55. Nagai R, Kumaoka S: Clinical evaluation of tamoxifen in advanced breast cancer (primary and recurrent). Clin Eval 8:321 352, 1980.
56. Beex L, Pieters G, Smals A, Koenders A, Benraad T, Klappenborg P: Tamoxifen versus ethinyl estradiol in the treatment of postmenopausal women with advanced breast cancer. Cancer Treat Rep 65:179 185, 1981.
57. Hanshin Breast Cancer Research Assn: Clinical eval- uation of tamoxifen in advanced and recurrent breast cancer. Clin Endocr 28: 73-84, 1980.
58. Pritchard KI, Thomson DB, Myers RE, Sutherland DJA, Mobbs BG, Meakin JW: Tamoxifen: a Phase II trial in premenopausal women with metastatic carcinoma of the breast. Reviews on Endocrine-Related Cancer, Suppi 9, 399408, 1981.
59. Wada T, Koyama H, Terasawa T: Effect of tamoxifen in premenopausal Japanese women with advanced breast cancer. Cancer Treat Rep 65: 728-729, 198l.
60. Kobayashi S, Kataoka M, Saito K, Tobioka N, Sakuma S, Nagai R: Therapeutic effect of an antiestrogen agent (tamoxifen) on advanced breast cancer. Basic Pharmacol Ther 7: 67-71, 1979.
61. Hayward JL, Carbone PP, Heuson J-C, Kumaoka S, Segaloff A, Rubens RD: Assessment of response to therapy in advanced breast cancer. Eur J Cancer 13: 89~4, 1977.
62. Hawkins RA, Roberts MM, Forrest APM: Oestrogen receptors and breast cancer: current status. Br J Surg 67: 153 169, I980.
63. McGuire WL, De La Garza M, Chamness GC: Eval- uation of estrogen receptor assays in human breast cancer tissue. Cancer Res 37: 637-639, 1977.
64. EORTC Breast Cancer Co-operative Group: Standards for the assessment of estrogen receptors in human breast cancer. Eur J Cancer 9: 379-381, 1973.
65. King RJB, Barnes DN, Hawkins RA, Leake RE, May- nard PV, Roberts MM: Measurement of oestradiol re- ceptors by five institutions on common tissue samples. Br J Cancer 38: 428430, 1978.

66. EORTC Breast Cancer Co-operative Group: Revision of the standards for the assessment of hormone receptors in human breast cancer. Eur J Cancer 16: 1513-1515, 1980.
67. Fumero S, Bernito GP, Pelizzola D, Grilli S, Buttazzi C, Di Fronzo G, Ronchi E, Bozzetti C, MoriP, Concolino G, Marocchi A, Della Cuna GR, Zibera C, Cerrutti G, Ros A, Piffanelli A: Results of the Italian Interlaboratory Quality Control Program for estradiol receptor assay. Tumori 67: 301-306, 1981.
68. Poulsen HS: Oestrogen receptor assay - limitations of the method. Eur J Cancer 17:495 501, 1981.
69. Muschenheim F, Furst JL, Bates HA: Increased incidence of positive tests for estrogen binding in mammary car- cinoma specimens transported in liquid nitrogen. Am J Clin Pathol 70: 780-782, 1978.
70. Bishop HM, Poole T, Blamey RW, Nicholson RI, Grif- fiths K: The importance of rapid freezing of breast tumours for the accurate determination of cytoplasmic oestradiol receptor (ER) status in primary breast cancer. Clinical Oncol 8: 86, 1982.
71. McGuire WL, Horwitz KB, Zava DT, Garola RE, Cham- ness GC: Hormones in breast cancer: Update 1978. Metabolism 27:487 501, 1978.
72. Leake RE, Laing L, Calman KC, Macbeth FR, Crawford D, Smith DC: Oestrogen-receptor status and endocrine therapy of breast cancer: Response rates and status stability. Br J Cancer 43:59 66, 1981.
73. Leake RE, Laing L, McArdle C, Smith DC: Soluble nuclear oestrogen receptor status in human breast cancer in relation to prognosis. Br J Cancer 43:67 71, i981.
74. Knight WA, Livingston RB, Gregory E J, McGuire WL: Estrogen receptor as an independent prognostic factor for early recurrence in breast cancer. Cancer Res 37: 46694671, 1977.
75. Block GE, Ellis RS, DeSombre E, Jensen E: Correlation of estrophilin content of primary mammary cancer to eventual endocrine treatment. Ann Surg 188:372 376, 1978.
76. Allegra JC, Lippman ME: The effects of 17~-estradiol and tamoxifen on the ZR-75-1 human breast cancer cell line in defined medium. Eur J Cancer 16:1007 1015, 1980.
77. Sutherland RL, Whybourne AM, Taylor IW: Cell cycle effects of tamoxifen on MCF 7 human mammary car- cinoma cells in culture. Reviews on Endocrine-Related Cancer, Suppl 9, 169-176, 1981.
78. Green MD, Whybourne AM, Taylor IW, Sutherland RL: Effects of antioestrogens on the growth and cell cycle kinetics of cultured human mammary carcinoma cells. In
RL Sutherland and VC Jordan (eds). Non-steroidal Anti- oestrogens. Academic Press, Sydney, 1981, pp 397412.
79. Martin L: Estrogens, antiestrogens and the regulation of ceil proliferation in the female reproductive tract in vivo. In JA McLachlan (ed). Estrogens in the Environment. Elsevier North Holland, 1980, pp 103 131.
80. Holt S, Croton R, Prichard J, Leinster S, George W,
373
Nicholson R, Griffiths K: An in vitro assay of tamoxifen sensitivity in advanced breast cancer. Surg Res Soc Ab- stract, 1982 (in press).
81. Lippman M, Bolan G, Huff K: The effects of androgens and antiandrogens on hormone-responsive human breast cancer in long-term tissue culture. Cancer Res 36: 45974618, 1976.
82. Murphy LC, Sutherland RL: A high affinity intracellular binding site for non-steroidal oestrogen antagonists. Re- views on Endocrine-Related Cancer, Suppl 9, 177-184, 1981.
83. Murphy LC, Foo MS, Green M, Milthorpe BK, Why- bourne AM, Krozowsky ZS, Sutherland RL: Binding of non-steroidal antioestrogens to saturable binding sites distinct from the oestrogen receptor in normal and neo- plastic tissues. In RL Sutherland and VC Jordan (eds). Non-steroidal Antioestrogens. Academic Press, Sydney, 1981, pp 317 337.
84. Jozan S, Elalamy H, Bayard F: Etude du m6canisme d'action d'un antioestrogene du groupe triphenylethylene sur la croissance de la ligne cellulaire de cancer du sein humain MCF-7 en culture. Acad Sci, Serie III, 292: 767 770, 1981.
85. Dao TL, Sinha DK, Nemoto T, Patel J: Effect of estrogen and progesterone on cellular replication of human breast tumors. Cancer Res 42:359 362, 1982.
86. Lipton A, Martin L: Inhibition of rat myometrium by tamoxifen. Proc Australian Physiol and Parmacol Soc 13: 52P, 1982.
87. Osborne CK, Bolan G, Monaco ME, Lippman ME: Hormone responsive human breast cancer in long-term tissue culture: Effect of insulin. Proc Natl Acad Sci USA 73: 45364540, 1976.
88. Shafie S, Brooks SC: Effect of prolactin on growth and the estrogen receptor level of human breast cancer cells (MCF-7). Cancer Res 37: 792-799, 1977.
89. Manni A, Trujillo JE, Marshall JS, Brodkey J, Pearson OH: Antihormone treatment of Stage IV breast cancer. Cancer 43: 444~450, 1979.
90. Ritchie G: The direct inhibition of prostaglandin syn- thetase of human breast cancer turnout tissue by 'Nol- vadex'. Reviews on Endocrine-Related Cancer, Supp Oct 78, 35-39, 1978.
91. Furr BJA: Future prospects in the treatment of hormone- responsive cancer. Clinics in Oncology i: 289 307, 1982.
92. Dowsett M, Easty GC, Powles TJ, Easty DM, Neville AM: Human breast tumour-induced osteolysis and prostaglandins. Prostaglandins 11: 447460, 1976.
93. Powles TJ, Dowsett M, Easty GC, Easty DM, Neville AM: Breast cancer osteolysis, bone metastases and anti- osteolytic effects of aspirin. Lancet i: 608-610, 1976.
94. Bennett A, Charlier EM, McDonald AM, Simpson JS, Stamford IF, Zebro T: Prostaglandins and breast cancer. Lancet ii: 624-626, 1977.
95. Greaves M, Atkins D, Ibbotson K, Martin TJ: Breast
374
tumours, bone resorption and prostaglandins. Clin Sci Mol Med 54: 20P, 1978.
96. Gasic GJ, Gasic TB, Galanti N, Johnson T, Murphy S: Platelet-tumor cell interactions in mice. The role of plate- lets in the spread of malignant disease. Int J Cancer 11: 704-718.
97. Tashjian AH, Voelkel EF, Goldhaber P, Levine L: Suc- cessful treatment of hypercalcemia by indomethacin in mice bearing a prostaglandin-producing fibrosarcoma. Prostaglandins 3: 515-524.
98. Humes JL, Cupo JJ, Strausser HR: Effects of indo- methacin on moloney sarcoma virus-induced tumors. Prostaglandins 6: 463473, 1974.
99. Strausser HR, Humes JL: Prostaglandin synthesis in- hibition: Effect on bone changes and sarcoma tumor induction in Balb/c mice. Int J Cancer 15: 724~730, 1975.
100. Hial V, Horakova Z, Shaft RE, Beaven MA: Alteration of tumor growth by aspirin and indomethacin: Studies with two transplantable tumors in mouse. Eur J Pharmacol 37: 367-376, 1976.
101. Bennett A, Houghton J, Leaper D J, Stamford IF: Tumour growth and response to treatment: beneficial effect of the prostaglandin synthesis inhibitor flurbiprofen. Br J Phar- macol 63: 356P-357P, 1978.
102. Bennett A, Houghton J, Leaper DJ, Stamford IF: Cancer growth, response to treatment and survival time in mice:
Beneficial effect of the prostaglandin synthesis inhibitor Flurbiprofen. Prostaglandins 17: 179-191, 1979.
103. Leaper DJ, French BT, Bennett A: Breast cancer and prostaglandins: a new approach to treatment. Br J Surg 66:683 686, 1979.
104. Plescia OJ, Smith AH, Grinw, ich K: Subversion of im- mune system by tumor cells and role of prostaglandins. Proc Natl Acad Sci USA 72: 1848-1851, 1975.
105. Fabian C, Sternson L, Barnett M: Clinical pharmacology of tamoxifen in patients with breast cancer: Comparison of traditional and loading dose schedules. Cancer Treat Rep 64: 765-773, 1980.
106. Patterson JS, Settatree RS, Adam HK, Kemp JV: Serum concentrations of tamoxifen and maj or metabolites during long-term nolvadex therapy, correlated with clinical re- sponse. In HT Mouridsen and T Palshof (eds). Breast Cancer Experimental and Clinical Aspects . Pergamon Press, Oxford, 1980, pp 89-92.
107. Wilkinson P, Ribeiro G, Adam H, Patterson J: Clinical pharmacology of tamoxifen and N-desmethyltamoxifen in patients with advanced breast cancer. Cancer Chemother Pharmacol 5: 109-111, 1980.
108. Daniel P, Gaskell SJ, Bishop H, Campbell C, Nicholson RI: Determination of tamoxifen and biologically active metabolites in human breast tumours and plasma. Eur J Cancer 17:1183 1189, 1981.