Embed Size (px)
Citation preview

Randi Abrahamsen, DDS PhD
23rd. November 2018
The Beauty of Healing
in Chronic Pain
11th International Congress
of Medical Hypnosis


An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.
IASP 1994
Background
Pain

Pain Experience
Tracey and Mantyh, Neuron 2007

Brain activity
Possitionemmissontomoghrafi (PET)
Functionel magnetic resonance (fMRI)
Electroencephalography (EEG)

Rainville et al 2000
PET

Pain mechanism
Tracey and Mantyh, Neuron 2007

Background Previous eksperimental studies of pain mechanism
Tracey and Mantyh, Neuron 2007
Rainville et al. 1997, 2002 Marquet et al. 1999
Faymonville et al. 2000,2003 Derbyshire et al. 2004 Schulz-Stübner 2004
Raji et al 2005

Background Previous eksperimental studies of pain mechanism
Tracey and Mantyh, Neuron 2007
Healthy subjects High hypnotic suggestibility No facial painstimulation

Effect of hypnosis on brain activity
Patients and behavioral outcome
19 TMD patients with myofascial pain
(1 man and 18 women)
Pain intensity (NRS)
Pain unpleasantness (NRS)
Hypnotic susceptibility Harvard Group Scale of Hypnotic Susceptibility (0-12)

Effect of hypnosis on brain activity
Hypnosis training
1 hour hypnosis training prior to fMRI:
1. Progressive musclerelaxation
2. Autobiographic safeplace
3. Gloveanalgesia (2 buckets with hot and cold water) combined with autobiographic memory of analgesia.
4. Transferring analgesia to test region
5. Posthypnotic cues for fMRI session
No training in hyperalgesia

3 different experimental conditions with
identical pain stimulation:
Baseline
Control
Hypnotic
hyper-
algesia
Hypnotic
analgesia
A GE Signa HDx 3T scanner (General Electric, Milwaukee, WI,
USA) gradient-Echo EPI, acceleration resolution 128 x 128
pixels, field-of-view 240 mm, slice thickness 3.5 mm, and 39
slices per volume.
Effect of hypnosis on brain activity. Material and Methods
Experimental design
Pain stimulation 30 seconds- 30 seconds off Repeated in 5 cycles
Randomised hypnotic conditons.

Pain
Control Hyperalgesia Hypnotic analgesia
NR
S
(0
- 1
0)
0
2
4
6
8
10
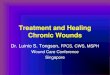
Modulation of pin-prick stimulation in control, hypnotically induced hyperalgesia, and hypnotic analgesia.
Control Hyperalgesia Hypnotic analgesia
0
2
4
6
8
10
Unpleasantness
Effect of hypnosis on brain activity. Results
Pain intensity and unpleasantness
*** **
** **
Time effects ***(P=0.001)** (P<0.01) Abrahamsen et al. Pain 2010

Control Hypnotic analgesia
Control-control.off hyponotic analgesia- hyponitic analgesia. off
Effect of hypnosis on brain activity. Results
Brain activity during hypnotic analgesia
Abrahamsen et al. Pain 2010

Control
Hypnotic analgesia
Effect of hypnosis on brain activity. Results
Brain activity during hypnotic analgesia
Abrahamsen et al. Pain 2010

Eksperimentelle studier af hypnoses
smertelindrende effekt
Tracey and Mantyh, Neuron 2007
Brainstem reflexes

Diffences in brain activity Physically induced pain Hypnotically inducered pain Imagined pain
Derbyshire 2004
N=7

Difference in brain activity between patients
with high and low pain score
Derbyshire 2004
Person with lowest painscore
Person with highest painscore
Person with highest painscore

Catastrophizing
Catastorphizing related to anticipation
interpretation of pain
Automatic circuits nucl. claudatus og
lentiformes
Tracey and Mantyh, Neuron 2007

Anxiety
Tracey and Mantyh, Neuron 2007

Acquired brain injury
Lindeløv et al. 2017

From: Improving working memory performance in brain-injured patients using hypnotic suggestion Brain. 2017;140(4):1100-1106. doi:10.1093/brain/awx001
Brain | © The Author (2017). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For
Permissions, please email: [email protected]

From: Improving working memory performance in brain-injured patients using hypnotic suggestion Brain. 2017;140(4):1100-1106. doi:10.1093/brain/awx001
Brain | © The Author (2017). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For
Permissions, please email: [email protected]

Chronic pain
19% af the European population
have pain >5 (pain scale 0-10)
Breivik et al. 2006
56%
44%
Age: 41-60 years Average 50 years
40% insufficient paincontrol sideeffects

Pain and traumatic events
Often relation between pain and mental stress /traumatic events (divorce, workloads and
-shifts, severe disease and death in close family)
Reduced activity at work and at home
Reduced participation in social life
Poor sleep
Less exercise
Large consumption of painkillers-many side effects
Increased use of health care system
Depression

How can we use this for chronic pain

Somatosensory cortex
Function of Somatosensory cortex S1,S2 : information about nociception: pain intensity, pain area, pain quality
Suggestions to alter pain:reduce area, intensity, change pain quality
Chudler & Bonia 2001 May 2007

Anterior cingulate cortex (ACC)
Part of the limbic system: affective part of the pain- the meaning of the pain
Suggestions to change the meaning of pain, amnesia
Craig 2008, Rainville 2002

Insula
Insula: superior monitoring central, risk evaluation
Suggestions on safety and comfort
Craig 2008,

Præfrontal korteks (PFL)
PFL: Pain memory, meaning of pain, activity
Suggestions to change pain memories (meaning) change of activity (age regression- progression)

The brain is amazing
The brain does what you train it to do!

Clinical studies
PIOP persistent ideophatic pain
Temporomandibular disorders

• RDC/TMD
• Coping stategies
• SCL
Inclusion
•VAS pain intensity
•Medication
•Sleep
After treatment
• VAS pain intensity
• RDC/TMD
• Coping strategies
• SCL
• Medication
• Sleep
• Hypnotic susceptibility
4 individual sessions of hypnosis (6 PIOP)
CD with hypnosis for training
1 week
Hypnosis
Control
Baseline
4 individual sessions of relaxation (6 PIOP) I CD with relaxation for training
Effect of hypnosis in PIOP and TMD patients
Experimental design

Effect of hypnosis in PIOP and TMD patients Material and methods
Primary Outcome
Average daily pain intensity
scored 3 times daily on
a Visual Analogue Scale (VAS)
(0-10)

1 Hypnosis Progressive relaxation
Guided imaginary to a safe comfortable place
Hypnotic suggestions of:
Feelings of success, calm, peace of mind, and inner strengths
Changing pain perception
Feeling of anesthesia
Stress coping
Refraiming of psychological trauma
2. Control Progressive relaxation
Guided imaginary to a safe comfortable place
Effect of hypnosis in PIOP and TMD patients Material and methods
Intervention

Effect of hypnosis in PIOP patients. Results
Daily pain intensity
Hypnosis (N=22)
Control (N=19)
Time effects ***(P >0.001)** (P<0.01) * P<0.05) Group difference # # (P<0.01) ###(P<0.001)

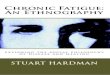
Study 2 Effect of hypnosis in TMD patients. Results
Daily pain intensity N
RS
pain
(0 -
10
)
0
2
4
6
8
10 Hypnosis (N=20)
Control (N=20)
# # #
* * *
* * * * * *
Time effects (P >0.001) # Group difference (P = 0.024)
baseline week1 week 2 week 4

-10
0
10
20
30
40
50
60
70
% r
ed
uc
tio
n in
pa
in s
co
res
hypnosis gruppe
control gruppe
Effect on hypnosis on chronic orofacial pain
% Reduction in daily score

Case
Accident on skies 17 years old male Previously attempted treatment: Painkillers even opiods Chiropractor: manipulation Physiotherapy: massage, ultrasound, Acupuncture, excercise Dentist: Splint Treatment at a pain clinic All of it is virtually without effect. Daily pain at 7-8

Treatment with hypnosis
Pain free days
Several pain free days
Average pain Worst pain

Follow up
Telefonfollow up 2 months later: Feeling Ok
no more treatment needed – uses selfhypnosis. Started to study again
1 year later: Still doing well

Acknowledgement All the patients who participated in the study Department of Clinical Oral Physiology Professor Peter Svensson, DDS, PhD, Dr.Odont. Associate Professor Lene Baad-Hansen, DDS, PhD Sara Baram, dental research student Bente Haugsted, research assistent Eduardo Castrillon, DDS, PhD Elin Norbud, Anni Stagstup, secretaries Karina Bendixen, DDS PhD student Faramarz Jadidi, medical engineer, PhD student
Psychooncology Research Unit, Aarhus University Hospital Professor Bobby Zachariae, MSc, MD Sci, Cand Psych, Dr Med,
Center of Functionally Integrative Neuroscience Associate professor Andreas Roepstorff , cand. scient., cand. phil., PhD Professor Leif Østergaard MD, MSc, PhD, DMSc Physicist Ryan Sangill MSc Research Radiographer Dora Zeidler RT, PgD in MR Sanne Lodahl PhD Martin Dietz PhD
Danish Dental Association Vi FAB (Danish Ministry of the Interior) Aarhus University Research Foundation

European Society of Hypnosis
Research project for clinicians
Patients: Consent Symptomdiary and medication MYMOP before and after Dissociative scale
Clinicians: Time registration
Interested ?? please contact Peter Naish: [email protected] Randi Abrahamsen: [email protected]

Thank you for your
attention