Embed Size (px)
Citation preview
129
130
131 MATERNAL TEMPERATURE DURING NORMAL AND ABNORMALLABOR FRITS SCHOUTEN1, HANS WOLF1, BERT SMIT2, DICK BEKE-DAM3, RIEN DE VOS4, 1Academisch Medisch Centrum Amsterdam,Obstetrics, Amsterdam, Netherlands 2Academisch Medisch Centrum Am-sterdam, Neonatology, Amsterdam, Netherlands 3Onze Lieve VrouweGasthuis Amsterdam, Obstetrics, Amsterdam, Netherlands 4AcademischMedisch Centrum Amsterdam, Epidemiology, Amsterdam, Netherlands
OBJECTIVE: To define temperature values in normal and abnormal labor.STUDY DESIGN: Rectal temperature was measured every 2-3 hours in all
women (n = 3075) with gestational age $36 weeks admitted to the labor wardfrom the start of active labor until 2 hours after delivery in 2 hospitals inAmsterdam (one university, one general) from June 2000 to January 2002.Normal labor (NL, n = 637) was defined as gestational age $37 weeks,spontaneous onset of labor, ruptured membranes < 18 hours before birth,normal progress of labor without the need for augmentation or epidural, andspontaneous vaginal delivery of an infant in good condition (5-minute Apgarscore $8), who did not need further medical observation or treatment.Intrauterine infection (IUI, n = 90) was defined by a temperature $38.58C ora temperature $38.08C with 2 of the following signs: fetal tachycardia $160,maternal tachycardia$100,meconium-stained or offensive liquor, or leukocytes$16.10E9/L. Womenwith IUI were treated with amoxicillin and gentamycin IV.Mean temperature, standard deviation, and range were calculated for 3-hourtime blocks. Temperature was compared for each time block between womenwith NL, IUI and the remaining women, defined as abnormal labor (AL,n = 2348).
RESULTS: Average temperature did not change throughout labor and wascomparable in NL and AL groups (37.18C, 95% interval 36.4-37.8). Afterepidural analgesia, >5 internal examinations, and PROM >18 hrs, averagetemperature was respectively 0.38C, 0.18C, and 0.18C higher than in remaininggroup during the last 3 hours before delivery. In IUI temperature was higherfrom 9 hours before delivery.
CONCLUSION: Temperature during labor was not different between
December 2003Am J Obstet Gynecol
S100 SMFM Abstracts
THE ASSOCIATION BETWEEN CLINICAL FINDINGS AND MICRO-BIOLOGIC PROFILES AMONG BV-POSITIVE PREGNANT WOMENLEONARDO PEREIRA1, JENNIFER CULHANE1, KELLY MCCOLLUM1,1Thomas Jefferson University, Department of Obstetrics and Gynecology,Philadelphia, PA
OBJECTIVE: To determine if the clinical findings among BV-positivepregnant women with two microbiologic profiles differ.
STUDY DESIGN: Women were enrolled at their first prenatal care visit(meanGA 14 ± SE: 13.7 ± 0.1 weeks) at public clinics in Philadelphia. Bacterialvaginosis (BV) status was assessed according to Nugent’s criteria. BV+ (Nugentscore 7-10) study participants were then classified into one of 6 mutuallyexclusive microbiologic groups. In addition, practitioners assessed clinical signsof BV (presence of clue cells on wet mount, amine odor after addition ofpotassium hydroxide [KOH], and documented patient complaints of vaginaldischarge). We compared the clinical presentation among BV+ women with andwithoutMobiluncus sp. (M+ vsM�). Data were analyzed using the chi-square test.Stratification was used to assess potential confounders (age, age at sexual debut,race, number of lifetime sexual partners, douching, smoking). Type I error wasset at 0.05 (two-sided).
RESULTS: A total of 1756 (46.6%) of the 3765 study participants were BV+.After controlling for assessed risk factors, the M+ group was significantly morelikely to have clue cells identified on wet mount (64% vs 48%; v(df)
2 = 20.1(1);P < 0.0001) and to have a positive amine odor after addition of KOH (57% vs.46%; v(df)
2 = 9.3(1); P = 0.002). There was no difference in physician diagnosisof vaginal discharge (65% vs 62%; v(df)
2 = 0.86(1); P = 0.35) or patientcomplaints of discharge (20% vs 24%; v(df)
2 = 2.9(1); P = 0.09).CONCLUSION: BV+ pregnant women with any Mobiluncus sp. are more
likely to have clue cells on wet mount and a positive amine odor after KOHpreparation compared to those withoutMobiluncus sp. However, the presence ofMobiluncus sp. is not associated with an increase in patient complaints ofdischarge or physician diagnosis of a vaginal discharge.
TIME COURSE OF PRO-INFLAMMATORY (PRO) AND ANTI-IN-FLAMMATORY (ANTI) MATERNAL CYTOKINE RESPONSE FOLLOW-ING SYSTEMIC LIPOPOLYSACCHARIDE (LPS) ADMINISTRATION DAVEGAYLE1, RON BELOOSESKY1, MINA DESAI1, FATANEH AMIDI1, SONIANUNEZ1, MICHAEL ROSS1, 1Harbor–UCLA Medical Center, Department ofObstetrics and Gynecology, Torrance, CA
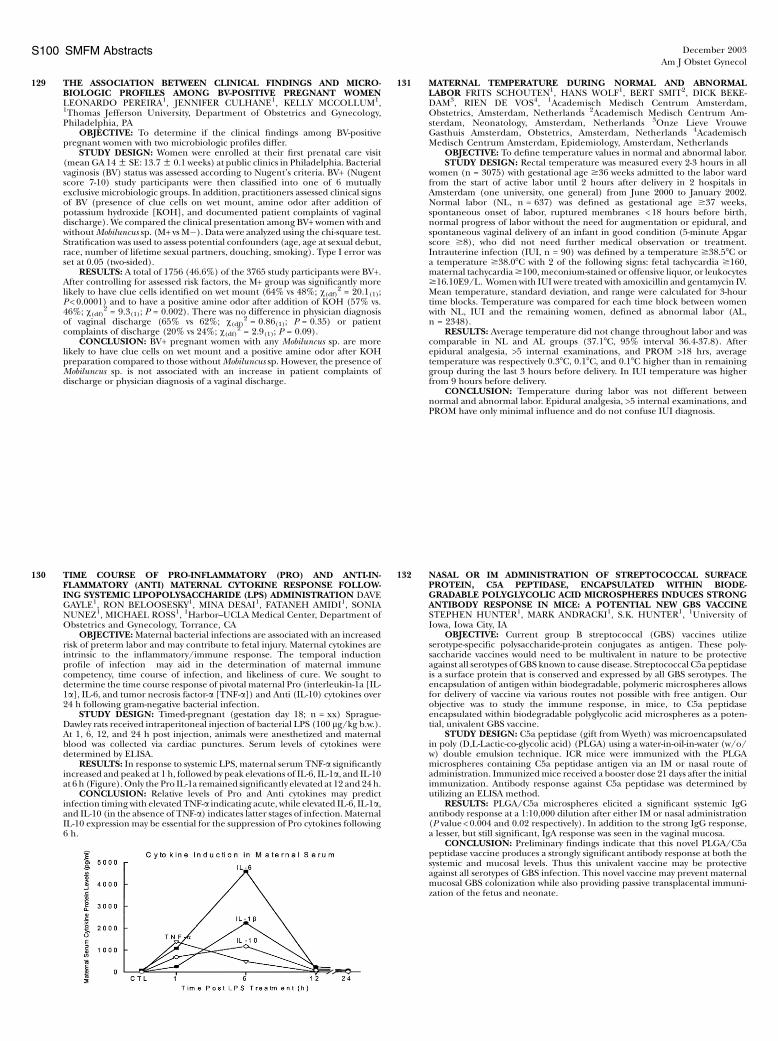
OBJECTIVE: Maternal bacterial infections are associated with an increasedrisk of preterm labor and may contribute to fetal injury. Maternal cytokines areintrinsic to the inflammatory/immune response. The temporal inductionprofile of infection may aid in the determination of maternal immunecompetency, time course of infection, and likeliness of cure. We sought todetermine the time course response of pivotal maternal Pro (interleukin-1a [IL-1a], IL-6, and tumor necrosis factor-a [TNF-a]) and Anti (IL-10) cytokines over24 h following gram-negative bacterial infection.
STUDY DESIGN: Timed-pregnant (gestation day 18; n = xx) Sprague-Dawley rats received intraperitoneal injection of bacterial LPS (100 lg/kg b.w.).At 1, 6, 12, and 24 h post injection, animals were anesthetized and maternalblood was collected via cardiac punctures. Serum levels of cytokines weredetermined by ELISA.
RESULTS: In response to systemic LPS, maternal serum TNF-a significantlyincreased and peaked at 1 h, followed by peak elevations of IL-6, IL-1a, and IL-10at 6 h (Figure). Only the Pro IL-1a remained significantly elevated at 12 and 24 h.
CONCLUSION: Relative levels of Pro and Anti cytokines may predictinfection timing with elevated TNF-a indicating acute, while elevated IL-6, IL-1a,and IL-10 (in the absence of TNF-a) indicates latter stages of infection. MaternalIL-10 expression may be essential for the suppression of Pro cytokines following6 h.
normal and abnormal labor. Epidural analgesia, >5 internal examinations, andPROM have only minimal influence and do not confuse IUI diagnosis.
132 NASAL OR IM ADMINISTRATION OF STREPTOCOCCAL SURFACEPROTEIN, C5A PEPTIDASE, ENCAPSULATED WITHIN BIODE-GRADABLE POLYGLYCOLIC ACID MICROSPHERES INDUCES STRONGANTIBODY RESPONSE IN MICE: A POTENTIAL NEW GBS VACCINESTEPHEN HUNTER1, MARK ANDRACKI1, S.K. HUNTER1, 1University ofIowa, Iowa City, IA
OBJECTIVE: Current group B streptococcal (GBS) vaccines utilizeserotype-specific polysaccharide-protein conjugates as antigen. These poly-saccharide vaccines would need to be multivalent in nature to be protectiveagainst all serotypes of GBS known to cause disease. Streptococcal C5a peptidaseis a surface protein that is conserved and expressed by all GBS serotypes. Theencapsulation of antigen within biodegradable, polymeric microspheres allowsfor delivery of vaccine via various routes not possible with free antigen. Ourobjective was to study the immune response, in mice, to C5a peptidaseencapsulated within biodegradable polyglycolic acid microspheres as a poten-tial, univalent GBS vaccine.
STUDY DESIGN: C5a peptidase (gift from Wyeth) was microencapsulatedin poly (D,L-Lactic-co-glycolic acid) (PLGA) using a water-in-oil-in-water (w/o/w) double emulsion technique. ICR mice were immunized with the PLGAmicrospheres containing C5a peptidase antigen via an IM or nasal route ofadministration. Immunizedmice received a booster dose 21 days after the initialimmunization. Antibody response against C5a peptidase was determined byutilizing an ELISA method.
RESULTS: PLGA/C5a microspheres elicited a significant systemic IgGantibody response at a 1:10,000 dilution after either IM or nasal administration(P value < 0.004 and 0.02 respectively). In addition to the strong IgG response,a lesser, but still significant, IgA response was seen in the vaginal mucosa.
CONCLUSION: Preliminary findings indicate that this novel PLGA/C5apeptidase vaccine produces a strongly significant antibody response at both thesystemic and mucosal levels. Thus this univalent vaccine may be protectiveagainst all serotypes of GBS infection. This novel vaccine may prevent maternalmucosal GBS colonization while also providing passive transplacental immuni-zation of the fetus and neonate.