Embed Size (px)
Citation preview

Wheelchair and Seating Assessment
Process Jessica Presperin Pedersen OTD, MBA, ATP/SMS, FAOTA
Hello from Chicago

The Team
• Who is typically involved?
•Client•Therapist •Physical Therapist•Occupational
Therapist•Equipment Supplier
• Other potential team members
• Family/Caregiver• Orthotist• Nurse• Physician• Speech Therapist• Rehabilitation Engineer• School/Private Therapist• Teacher/Employer

Role of the Therapist
• Perform the subjective and hands-on evaluation
• Discuss equipment options with the supplier• Provide information on client
needs • Support
• Function
• Determine best choice
• To educate the client and involve them in the decision-making process
• Take part in fitting equipment with supplier• To ensure
• proper positioning
• support
• Train/Educate regarding • Use of equipment
• Care of equipment

Wheelchair and Seating Goals
•Maximize independence with mobility and function

Provide a Means to Get From Point A to Point B

Wheelchair and Seating Goals
•Management of Skin Integrity•Weight Shifts •Independent •Dependent

Wheelchair and Seating Goals
•ADLs•Increase stability to maximize function•Decrease the influence of abnormal tone

Wheelchair and Seating Goals
•Do not superimpose positioning intervention over function

Wheelchair and Seating Goals
•Enhance Physiologic Function•Cardiopulmonary•Vascular•Lymphatic•Swallowing•Digestion

Wheelchair and Seating Goals
•Maintain Skeletal Alignment •Slow Structural Range
of Motion Loss

Wheelchair and Seating Goals
• Increase Endurance to Promote Increased Energy for Functional Tasks

Wheelchair and Seating Goals
•Improve Condition for Visual and Perceptual Capabilities

Wheelchair and Seating Goals
•Enhance Safety

Wheelchair and Seating Goals
• Provide Equipment• That is aesthetically acceptable
• Enhances self-esteem

Wheelchair and Seating Goals
•Provide a piece of equipment that has the potential to change

Wheelchair and Seating Goals
• Provide equipment that is manageable• Environment
• Home
• Community
• Work
• Transportation
• Lifestyle

Pertinent Information
•Age•Goals•Client•Willingness to use
equipment•Caregiver/family
•Support system

Pertinent Information
•Environment(s)•Home•Secondary

Pertinent Subjective Information
•Transportation•Occupation

Pertinent Subjective Information
•Leisure interests

Pertinent Subjective Information
• Funding source• Primary• Secondary
• Current mobility base
• Current seating components

Medical Information
• Diagnosis(es)• Date of illness/injury
• Past medical hx/co-morbidities
• Surgeries (hx/future)
• Medications
• Pain
• Tonal Influence

Medical Information
• Skin integrity
• Respiratory status
• Vision/perception• Head tilt
• Hearing
• Cognition
• Sensory status
• Motor planning
• Sensory processing

ADLs
•Eating
•Dressing
•Hygiene
•Bathing
•Toileting
•Other

Describe Present Mobility BaseWhat are they using now?
• Type: Stroller, Dependent, Tilt, Manual, Power
• Manufacturer, Model, Serial #, Age
• Size, Color
• Condition of Base
• Supplier who delivered base

The Mat Assessment
How is the transfer performed?
▪Independent Transfer▪Transfer board▪Shearing?
▪Dependent▪What equipment is used?▪How many people are involved in the transfer?▪Hoes does the transfer occur?

The Mat Assessment in supine
• Assess Pelvic Mobility• Neutral in terms of TILT
• Level in terms of OBLIQUITY
• Flat in term of ROTATION
• Thigh to Trunk Angle

The Mat assessmentIn Supine
The Gravity Eliminated Position
▪Where it the head in relation to the mat surface
▪Where is the head in relation to the pelvis.
▪Pain/discomfort with repositioning

The Mat AssessmentIn supine
▪ Work of Breath and Breathing Patterns
▪ Ribcage Mobility▪ Tone ▪ Motor Control/Movement
Patterns▪ Note how tone changes in
response to movement, function, behavior, or psychological state.

The mat assessmentin Supine
Tone and Motor Control
▪Primitive Reflexes▪ ATNR
▪ STNR
▪ TLR
▪ MORO
▪Antigravity movements
▪Asymmetrical movement

Hip mobility
Assessing Hip Mobility ▪Flexion separate from pelvic movement▪Abduction/adduction▪ Internal/external rotation▪Leg Length Discrepancy▪Windblown Hips
***keeping knees flexed to keep the hamstring muscle loose.

The Hamstring

The tight hamstring
Possible Solutions
• Increase the seat to back angle
•Adjust footplates
•Angle the cushion

The Mat assessment: The Pelvis
Our base of support and stability

REducbile vs Non-reducible
•Reducible- can bring the body or extremity to a neutral position.
•Non-reducible•An asymmetrical
posture that cannot be corrected or realigned into a symmetrical position•No movement
available in any direction of plane. • Ex. A fused hip

Pelvic tilt
Pelvic Tilt
▪Neutral
▪Posterior
▪Anterior

Posterior Pelvic Tilt: concerns
Concerns:
▪ Pressure on sacrum
▪ Kyphotic posturing
▪ Decreased thoracic expansion for breathing
▪ Shoulder girdle moved forward-not aligned with pelvis
▪ Sliding may occur
▪ Increased cervical extension

Anterior pelvic tilt
Anterior Tilt
▪Leads to lordosis
▪Center of Gravity is moved forward
and balance is compromised- may use
UE for support
▪Pressure on pubis symphysis

Pelvic OBLIQUITY:concerns
Concerns with Pelvic Tilt▪ Pressure on ischial tuberosity▪Concavity at ribcage▪May lead to Scoliosis▪May lead to lateral
leaning/instability▪Can affect physiological
function

Pelvic rotation:concerns
Concerns with Pelvic Rotation
▪ Scoliosis
▪ Peak Pressure Points throughout posterior of ribcage
▪ Physiological Function
▪Rule out subluxation/dislocation

Sitting Balance
Postural Control
•Hands Free
•Hands-Dependent Sitter
•Prop Sitter
Fear of Falling- hands dependent

Sitting Balance
Hand Simulation of postural Support
• Provides information for external supports
• Provides information regarding spine and ribcage mobility

Skin integrity
Sensation
• WFL
• Impaired• Hypo-sensitive• Hypersensitive
• Defensive
• Level of Sensation

Skin Integrity
•Can they reposition themselves for comfort?
•Do they perform optimal pressure reliefs?
•Do they have any skin breakdown presently?
•Do they have a history of skin breakdown?
•Have they had any falp surgeries?
•Age

Risk factors
• Individual risk factors: •bony prominences,• Immobility/prolonged sitting• impaired nutrition or hydration, • aging skin,• compromised circulatory system,• Tendency towards moisture/sweat

Linear Measurements
• Include dimensions of the body
• Take anatomical measurements in the seated position on a firm surface with feet supported
•Use calipers, yardstick, or metal tape measure.
•Consider orthotics
•Use a firm surface


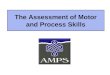
Determining the Size of a wheelchair
A. Hip width—provides information as to the width of the seat of the wheelchair
B. Buttocks Thigh / Upper Leg Length measurement – provides information as to the depth of the seat of wheelchair
C. Lower Leg Length- provides measurements for foot support placement
D. Shoulder width
E. Shoulder Height- provides measurement for back support
C
A BE
D

Hip Width
•Effective Hip Width for deviations

External knee width
•Can help specify the width of the cushion support/or the wheelchair frame

Buttock Thigh Depth(Upper leg Length)

Lower Leg Length
•Consider AFOs
•Consider type of shoes
• Effective lower leg length for windswept lower legs

Shoulder Width

Back Height (to shoulder and scapula)
•Things to Consider •TLSO•Reducible posture
(2016), Courtesy Jessica
Presperin Pedersen

Angular Measurements
• Describes a person’s body posture and orientation
●Geometry of seating
○ Thigh to trunk➔ Seat to back support angle○ Thigh to lower leg➔ Seat to legrest angle
○ Lower leg to foot angle ➔ Legrest to footplate angle

Posterior Pelvic Tilt and kyphosis
• Assess flexibility of the spine
• Determine optimal thigh to trunk

Seating Components and Equipment Trial
•Seat Cushions
•Back Cushions
•Secondary Components

Recommendations
• This is the final list of what’s the client, family/caregiver, and team agree upon
• A quote from the supplier is provided to the therapist
• Therapist documents equipment letter of medical necessity (ELMN)
• Physician signature on ELMN

Home Visit
The supplier may have to make a home or school visit to make sure the equipment can be used inside the house/school or there is access into the home.

Implement regular follow-up
Fitting
• The Therapist and supplier meet with the individual to get final measurements, make a mold, or do a specific activity required of a product before the final fit.
Final Delivery
• Wheelchair and seating equipment are delivered
• Optimal fit is determined
• Safety concerns are discussed
• Equipment care and maintenance demonstrated
• Satisfaction is the goal

Wheelchairs and Seating Interventions
Jessica Presperin Pedersen OTD, OTR/L, ATP/SMS, FAOTA

Wheelchair mobility base
• Dependent--does not allow user to self propel
• Manual base--allows independent propulsion through mechanical means
• Power base--allows independent propulsion through using a motor and controls to activate the chair

Dependent bases
• Strollers
• Tilt in space--change position in space while maintaining seat-back angle
• Recline--can open seat to back angle
• Transport chairs

Dependent base: medical stroller style

Dependent base; TNS mid-pivot
• Folding frame w/c, ordered to accommodate environment
• Body mass shifts with position of upper part of frame
• Frame of base, increased
• Mfg;

Dependent base; TNS rotation in space
• Smaller overall length
• Mfg; Sunrise, Invacare, Kimobility

Dependent base; TNS front pivot
• Front seat to floor height remains the same, application for foot propellers
• Adjustable rear seat to floor height, lower for pelvic positioning, return to neutral for ease of transfer or functional activity

Wheelchair categories
• HCPCS- code assigned by MC
• K codes established 1993, provide a minimum characteristics
• Wheelchair manufacturers apply for code, compliance with RESNA testing standards and product registration with FDA

Manual wheelchairs - standard• K0001 std. frame
• Greater 36 lbs.
• 19” or > STF height
• Weight capacity 250 lb
• 16-18” wide x 16” deep
• Non removable armrest
• K0002 hemi frame
• Greater 36 lbs.
• 18.5” STF height
• Weight capacity 250 lb
• Fixed height armrest, removable
• Medline, Invacare, E&J, Drive

Manual wheelchairs- lightweight• K0003 lightweight
• Weight 34-36 lbs.
• Weight capacity 250 lb.
• Fix/adjust height armrest
• STF height 17.5-19.5”
• K0004 HS lightweight
• Weight < 34 lbs.
• Weight capacity 250 lb.
• Lifetime warranty on frame
• Adjustable height armrests
• 16- 20” wide x 16-20” seat depth
• Super hemi height STF, 15”

Manual wheelchairs Ultralight, K0005
• Less than 30 lbs..
• Lifetime warranty on frame
• Adjustable rear axle
• Rigid or folding
• Transit tie down
• Ability to order custom fit for optimal efficiency with w/c propulsion
• Full time, long term user
• Mfg: TiLite, Sunrise, Kimobility, Colours, Motion Composites, Per4max

Intervention: Setup of Frame
Relationship between the shoulder and rear wheel
forward position:
▪ more body weight on rear wheels, ↓ RR
▪ “Long, smooth stroke”
▪ ↓ stroke frequency
▪ increases push efficiency,
▪ Boninger et al. 2001

Pediatric manual wheelchair
Seat width < 15”
Consideration:
• Self propulsion a goal
• Ordering to accommodate growth
• Transport on school bus
• Positioning needs for best alignment, stability to allow functional reach w/c propulsion and task

Bariatric wheelchair
• K0006—patient weighs more than 250#
• K0007—patient weighs > than 300#
• Manufacturers: 21st century Scientific, wheelchairs of Kansas, Quantum, Sunrise

Wheelchair components

POWER ASSIST TECHNOLOGY-
SMART DRIVE- Max mobility, weighs 12.5#
➢steering by applying resistance to handrim
EMOTION, Twion-ALBERS, weighs 22# /wheel
➢push stroke is enhanced by power motors, can adjust for left /right

Power conversion; E-fix, Albers
• Joystick and motor add on to manual w/c
• Rule out power wheelchair because of environmental barriers
• Challenges with funding

POV- scooter
• 3 or 4 wheel models
• Compact/travel, full size, heavy duty
• Mfgs, Pride, Merits, Drive Medical, Golden Technology, Pacesaver
• Go-Go is priced within reimbursement allowable
Photo Courtesy Pride Mobility Corporation. Used with Permission 2019

POV- scooter; Medicare guidelines• Cannot propel optimally
configured manual wheelchair to perform MRADLs in home
• Able to safely transfer, operate, and maintain postural stability while operating
• Significantly improve ability to participate in MRADLs in home
• Willing to use
• Meets weight capacity
• Go-Go is priced within reimbursement allowable
Photo Courtesy Pride Mobility Corporation. Used with Permission 2019

Group 1/Group 2 consumer power
• Unable to safely transfer, operate, and maintain postural stability in POV
• Home does not provide adequate access for operating POV
• Able to safely operate, or has caregiver willing to operate (who cannot push manual chair)
• Improves ability to participate in MRADLs in home
Photo Courtesy Pride Mobility Corporation. Used with Permission 2019

Group 2 power wheelchair- consumer power
• Jazzy
• Merits Vision
• Rule out less costly mobility option (cane, manual w/c, scooter)
• Needed for in home mobility and participation MRADLS
• Not dx driven, typical patient’s that qualify: OA, RA, COPD, amputations
• Can order with single power, ie tilt
• Group 2 w/ single power requires ATP certified rehab supplier per MC regulations

Group 3 power wheelchair- complex rehab
• Rule out less costly mobility option (cane, manual w/c, scooter)
• Home assessment by ATP/rehab equipment provider
• Specialty evaluation by OT/PT/DR
• Mobility limitation is due to neurological condition, myopathy or congenital skeletal deformity AND 1 of the following
• Specialty control
• Requires tilt or recline
• Uses ventilator

Group 2 vs. Group 3 Complex Rehab PWCs Specifications
Performance Characteristics Group 2 PWCs (consumer) Group 3 Complex Rehab PWCs
Standard Integrated or Remote Proportional Joystick
Yes Yes
Accommodates Seating and Positioning items
Yes Yes
Length < or = to 48" < or = to 48"
Width < or = to 34" < or = to 34"
Minimum Top End Speed 3 mph 4.5 mph
Minimum Range 7 miles 12 miles
Minimum Obstacle Climb 40 mm 60mm
Dynamic Stability Incline 6o 7.5o
Capable of Upgrade to Expandable Controller
No Yes
Capable of Upgrade to Alternative Control Devices
No Yes
Drive Wheel Suspension to Reduce Vibration
No Yes

Pediatric power
• Correlation between self initiated mobility and development (Anderson et al, ‘13, Bornstein et al, ’13
• PM and development; cog, language, social skills (Jones et al, ‘12, Lynch, et al ‘09)
• Furumasu- PM training
• RESNA PM for pediatric user 2017

Power wheelchairs: Center-Wheeled Drive
• Smaller turning radius, turn on spot
• Traction- typical design w/ 6 wheels contact ground
• User COG over drive wheels, most comparable to walking
• Caster realignment at start up; practice needed

Power wheelchairs: Front-Wheeled Drive
• Excellent traction for obstacle climbing, outdoor use
• Turns – forward pivot point
• Smaller turning radius
• Fishtails at higher speeds
• Drive uphill COG displace to rear casters w/ loss traction
• COG forward of user
• Applications- active outdoor user

Power wheelchairs: Rear-wheeled Drive
• Stable over uneven terrain
• Track straight with better drive performance at top speed and with non proportional control
• Longer footprint and Less maneuverable for indoor use
• Application- VM deficits, prior use
Photo Courtesy Invacare Corporation. Used with Permission 2019

Power seat functions; clinical application for pressure reduction
Pressure points seated in w/c

Power tilt and recline; clinical applications
• Tilt• Pressure relief
• Rest break
• Repositioning hips
• 25-65 deg of tilt
• Recline• Self catheterization
• Management BP, hip ROM
• ADLs
• Tilt/recline combo-most pressure relief RESNA

RESNA position paper on tilt, recline and ELR
• Tilt, when used alone, must be greater than about 25° to achieve pressure relief and/or tissue perfusion at the IT
• Recline, when used alone, can increase shear but may provide reduction in pressure at the IT at angles greater than 90-100°
• The greatest reductions in pressure are seen when tilt and recline are used together
• Lateral weight shifting may sufficiently offload the IT on one side, but also simultaneously increase pressure on the other.

Standing frame
• https://youtu.be/v_py9JQ9Mys • Benefits of passive standing
• Standing feature on wheelchair base (vs independent standing frame) may result in increased standing frequency

Seat elevation
• Assist with transitions and transfers
• Access to shelves, cabinets for independence with ADLS
• Visual orientation
• Vocational application
• RESNA position paper on seat elevation 2019- functional benefits, further research needed

Control options• Access sites: hand,
head or face, mouth (sip & puff), foot, combo of body parts
• Different types & shapes of knobs, switches

External Support Surfaces

Primary Support Surfaces
•Seat cushions
•Backs

Secondary Support Surfaces
• Lateral and Medial Supports• Pelvis• Thigh• Trunk
• Headrests
• Arm Support
• Foot Support

Uniform Terminology for Seating
Describe body part and where support is in relation to it:
• Posterior
• Anterior
• Lateral
• Medial
• Superior

Uniform Terminology for Seating
Describe Surface Area Support
• Planar
• Generic Contour
• Custom Molded

Generic Contoured Seating
•Generic shapes and curves
•Usually Off the Shelve
•May Vary in Sizes
•Not Specific to Individual Shape

Figures Courtesy of Jean Anne ZollarsUsed with permission

Generically Contoured Back

Aggressive Contour
Figures Courtesy of Jean Anne ZollarsUsed with permission

Molded or Custom Contour
Formed specifically to the individual’s body

Molded Simulation Process

Seating Intervention Ideas• Where to start?
• What does the individual want to do in the wheelchair?
• What intervention will allow him/her to do it?
• Where is intervention needed? What type of intervention is needed? When is it needed? How will it interface with the wheelchair?

Parameters for Intervention
• What Body Part?
• Posterior—Lateral—Anterior—Superior
• Planar– Contour– Molded
• Fixed—Flexible
• Length of Force?

Classification of Cushion or Contact Materials
• Foam
• Fluid
• Air
• Honeycomb
• Combination
• Powered

Considerations for Materials in Products
Distribute Pressure
Provide Desired Surface Area SupportAccommodate to Body Shapes
Maintenance
Weight
Durability

Intervention ideas
• Start with pelvic support/ cushion
• Consider buttocks, thighs, legs and feet
• Back
• Shoulders, arms, hands
• Head

Seat cushion intervention

Intervention at knee
• Medial thigh
• Lateral thigh
• Tight hamstrings

Intervention at feet

Considerations for BacksAdjustability
Seat depth
Position in space/Angles
Surface area Support- ShapeAccommodation
Ability to change shape
Durability
Function
Maintenance

Lateral trunk control

3 Points of Control

Anterior trunk control

Chest Support Shoulder StrapsSafe Intervention

Upper Extremity Support

Head Supports

Questions?

Wheeled Mobility and Seating Evaluation
PATIENT INFORMATION Name DOB Sex Date Time
Address Medical Record # D/C Date
Physician
The following supplier/ATP was present and participated in this evaluation and recommendation.
____________________________
Supplier Company
Phone
Therapist seating CRT experience and credentials
Phone
Therapist
Spouse/Parent/Caregiver Name
Phone
1º Insurance/Payor
Policy # 2º Insurance/Payor
Policy # Reason for Referral Current w/c no longer meets needs Current w/c beyond repair
Non-ambulatory Ambulation not independent, safe or timely Patient Goals
Caregiver Goals
Specific Mobility Limitations that May Affect Care See FMA in Medical Record
MEDICAL HISTORY Diagnosis ICD10
Code 1o Dx Onset
ICD10 Code
Diagnosis
ICD10 Code
Diagnosis ICD10 Code
Diagnosis
Progressive Disease
Relevant Past and/or Future Surgeries Bone Skin Muscle Joint ________________________
Height Weight Explain recent changes or trends in weight
Pertinent Medical History
Autonomic System
Intact Impaired Hx of Autonomic Dysreflexia Hx of Thermoregulatory Dysfunction
Comments Cardiac Status
RestingHR/Pulse Resting BP _____________
Functional Limitations
Intact Impaired Severely Impaired Pace Maker Cardiac Precautions Hx of MI Hx of A-fib Hx of Tachycardia / Bradycardia Hx of Orthostatic Hypotension Syncope _____________________________
Comments
Respiratory Status
Resting Resp. Rate ______ Resting O2 Sat. _________
Functional Limitations
Intact Impaired SOB O2 PRN L / Min. O2 Dep L / Min. Ventilator Dep Hx of Chronic Congestion _____________________________________________________________________________
Comments
Medications that may affect mobility/positioning See medication list in Medical Record
Prosthetics, Orthotics and/or Splints Used
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)1/15

CURRENT MOBILITY ASSISTIVE EQUIPMENT (MAE) / SEATING Current Mobility Device None Cane Walker Stroller Manual w/c Manual w/ tilt Manual w/ recline
Scooter Power w/c Power w/ tilt Power w/ recline Power w/ tilt & recline w/ seat elevator w/ stand
Model
Color Age of Mobility Base
Manufacturer
Serial # Additional Components
Seat Height Seat Width Seat Depth Condition of Current Mobility Device Problems with Current Mobility Device
Current Seating System
Age of Seating Components COMPONENT MANUFACTURER / CONDITION / PROBLEMS Seat Base Mounting Hardware Cushion Pelvic Support Lateral Thigh/Knee Support Medial Knee Support Foot Support Foot Strap / Heel Loop Back Mounting Hardware Lateral Trunk Supports Chest / Shoulder Support Head Support Mounting Hardware UE Support Mounting Hardware Other Other When Relevant Overall W/C Length Overall W/C Width Overall W/C Height
This section was completed by Physician/Clinician evaluating patient
This section was completed by supplier ATP present at the evaluation
This section was completed by supplier ATP on a separate document
Is the current mobility device meeting the patient’s physical, functional, environmental and medical needs?
Yes No Comments
HOME ENVIRONMENT Setting: Rural Urban Suburban Paved Roads Sidewalks Rough Terrain Other
House Condo/Town Home Apartment Asst Living LTCF Other Own Rent Lives Alone / No Caregivers Lives Alone / Caregiver Asst Lives with Caregiver(s) Hours Home Alone
Comments Ability to safely reach (in sitting) Dresser Drawers Closet Rod Medicine Cabinet BR Faucet/Shower
Freezer/Refrigerator Oven/Stove Microwave Kitchen Sink Cupboards/Drawers/Shelves Light Switches Thermostat Phone Fire Alarm Door Eye Hole/Viewer Elevator Buttons
Comments Home is Accessible to Wheelchair Yes No Storage of Wheelchair In Home Other Stairs Yes Thresholds Yes No Height Surfaces
No Ramp Yes No Degree of Incline Carpet (Describe) ___________ Tile Wood Stone/Brick Other
Non-accessible areas in home
Modifications planned Comments This section completed by Physician/Clinician Supplier ATP Supplier ATP on a separate document (check all that apply)
Type of control
Uses powered adj. height seat to do above reaching
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)2/15

COMMUNITY ENVIRONMENT Employment/Volunteer
N/A Specific requirements pertaining to mobility School
N/A Specific requirements pertaining to mobility Other Community Mobility Medical Appointments Religious Civic Duties Other _________________________
IADLs N/A Specific requirements pertaining to mobility
This section completed by Physician/Clinician Supplier ATP Supplier ATP on a separate document (check all that apply)
TRANSPORTATION Car Van SUV/Truck Public Transportation School Bus Van Service Ambulance Other _________________
Vehicle Adaptations None Ramp Lift Hand controls Other ______________________________________________ Tie Downs Type ____________________ Lock-down System Type ____________________
Method of Riding Rides in w/c Rides in vehicle seat/car seat Self drives from w/c Self drives in driver’s seat Other
Storage Where is w/c stored during transport? N/A Front seat Back seat Trunk/Bed/Cargo area Vehicle lift Other __________________________________________________ Size of area needed for transport (WxDxL)
If necessary, client or caregiver can load/unload equipment into vehicle Yes No
Vehicle Dimensions Door Height _______________ Inside Height _______________ Door Width _______________ Ramp WxL _______________ Weight Capacity _______________ Other This section completed by Physician/Clinician Supplier ATP Supplier ATP on a separate document (check all that apply)
CURRENT MRADL Status (Getting to the location where the ADL is performed with present MAE) Indep
without MAE
Indep with
current MAE
Assist with
current MAE
Unable/ Dep with current MAE
N/A Comments / Equipment
Dressing Eating Grooming/Hygiene
Toileting Bathing IADLS Bowel Mgmt Continent Incontinent Accidents Protective Undergarments Colostomy Bowel Program Comments Bladder Mgmt Continent Incontinent Accidents Protective Undergarments Urinal / Bed Pan / Commode
Intermittent Catheterization Indwelling Catheter External/Condom Catheter Supra-Pubic Catheter Comments
DESCRIBE WHAT HAS CHANGED TO REQUIRE NEW AND/OR DIFFERENT MOBILITY ASSISTIVE EQUIPMENT
PHYSICAL / FUNCTIONAL EVALUATION
VERBAL COMMUNICATION 1° Language 2° Language Communication provided by: Patient Family/Caregiver Translator AAC Other __________________________
WFL Receptive WFL Expressive Understandable Difficult to Understand Non-communicative Non-Verbal Communicator – Method Augmentative Communication Device Manufacturer/Model _______________________________________________________ AAC Mount Needed Type ________________________________________________________________________________
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)3/15

PROCESSING SKILLS Visual Processing Intact Impaired Compensated Comments Motor Planning and Execution Intact Impaired Compensated Comments
Safety awareness of self and others Intact Impaired Compensated Comments
Attention to environment Behavioral Status Additional comments regarding processing skills and ability to safely use wheelchair
PAIN, SENSATION and SKIN INTEGRITY Sensation
Intact Impaired Absent Hyposensate Hypersensate
Location(s) of impairment/absence
Comments
Yes No Pressure Relief Able to perform effective pressure relief/reperfusion at seated surface Method: Stand up (independently, without risk of falling)
Lean side to side (without risk of falling) W/C push up (4+ times / hour for 15+ sec.) Yes No Pressure relief method(s) performed consistently throughout the day
If no, why not? Uses seat functions to perform pressure relief Yes NoPressure Map Results N/A on File
Skin Integrity Current Skin Integrity
Intact Red Area Open Area Location(s) _________________________ Size(es) ___________________________
Scar Tissue At Risk -Prolonged Sitting
Hx of Pressure Injury Yes No Location(s) _________________________ When _____________________________ Limited Sitting Tolerance Yes No Hours per Day
Hx of Skin/Flap Surgery Yes No Location(s) _______________________ When ___________________________ Comments
Risk Factors for Skin Braden Score, if administered _____ (Braden Scale is used for individuals who are bedridden-not for seated persons) Bony prominences Immobility Incontinence Impaired nutritional or hydration status Aging skin Compromised circulatory status Tendency towards moisture build up (profound perspiration, skin folds) Other
Complaint of Pain Severity (No pain) 0 1 2 3 4 5 6 7 8 9 10 (Worst) Location(s)
How does pain affect mobility, sitting and/or ADLs?
STRENGTH / RANGE OF MOTION Gross Overall Strength Gross Range of Motion
Upper Extremity Lower Extremity Shoulder Normal 5 / 5 - Normal 5 / 5 - Elbow Good 4 / 5 + - Good 4 / 5 + - Wrist Fair 3 / 5 + - Fair 3 / 5 + - Hand Poor 2 / 5 + - Poor 2 / 5 + - Hip Trace 1/ 5 + - Trace 1/ 5 + - Knee No Movement No Movement Ankle
Manual Muscle Test on file/limitations noted on pgs 6/7 Goniometric Measurements on file/limitations noted on pgs 6/7 Comments
BALANCE Static Sitting Dynamic Sitting Static Standing Dynamic Standing
Independent Independent Independent Independent Min assist Min assist Min assist Min assist Mod assist Mod assist Mod assist Mod assist Max assist Max assist Max assist Max assist
Uses UE Uses UE Uses UE Uses UE Unable / Dependent Unable / Dependent Unable / Dependent Unable / Dependent
Comments
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)4/15

NEURO-MOTOR WNL Spasticity / Hypertonicity Flaccidity / Hypotonicity Fluctuating Tone Ataxia Athetoid Movements Dystonia
Primitive Reflexes Tremors Muscle Spasms / Clonus Paralysis
MODIFIED ASHWORTH SCORE (0, 1, 1+, 2, 3, 4) Muscle(s) Tested On file noted on pgs 6/7 Score
Comments
MEASUREMENTS in SITTING
Left Right A Buttock/thigh depth J Top of head
B Lower leg length K Shoulder width C Foot length L Chest width D Ischial depth M Hip width E Seat to elbow height N External knee width F PSIS height O Internal knee width G Inferior scapular height P External ankle/foot (at widest point) H Axilla height
I Shoulder height (top) + Overall width (asymmetrical width
for windswept legs, scoliotic posture or other postural asymmetry
+ Overall depth (leg length discrepancy, accommodate adipose tissue or other posture
This section completed by Physician/Clinician Supplier ATP Supplier ATP on a separate document (check all that apply)
Orientation of Seat to Back and Seat to Thigh Supports Accommodate Left Right Both sides Left Right Both sides Comments Pelvis to thigh angle Greater than 90° Less than 90° Thigh to trunk angle Greater than 90° Less than 90° Thigh to calf angle Greater than 90° Less than 90°
Comments
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)5/15

POSTURE in SITTING COMMENTS
Anterior / Posterior Obliquity (viewed from behind) Rotation - Pelvis Tonal Influence Pelvis:
Normal Paralysis Flaccid Low tone High tone Spasticity Dystonia Pelvic thrust Other:
PELVI S
Neutral Posterior Anterior WFL L low R low (Obliquity) (Obliquity)
WFL Right Left Anterior Anterior
Non-Reducible (Fixed) Partly Reducible Reducible (Flexible)
Self External Force Tendency away from neutral
Non-Reducible (Fixed) Partly Reducible Reducible (Flexible)
Self External Force Tendency away from neutral
Non-Reducible (Fixed) Partly Reducible Reducible (Flexible)
Self External Force Tendency away from neutral
Comments
TRUNK Anterior / Posterior Left / Right -Scoliosis Rotation – Shoulders and Upper Trunk
Tonal Influence Trunk:
Normal Paralysis Flaccid Low tone High tone Spasticity Dystonia Pelvic thrust Other
WFL ↑ Thoracic ↓ Thoracic Kyphosis Kyphosis
WFL Convex Convex Left Right
Neutral Left-anterior Right-anterior
☐ ☐↓ Lumbar ↑ Lumbar
Lordosis Lordosis
C-curve S-curveMultiple Apex curve(s)
Non-Reducible (Fixed) Partly Reducible Reducible (Flexible)
Self External Force Tendency away from neutral
Non-Reducible (Fixed) Partly Reducible Reducible (Flexible)
Self External Force Tendency away from neutral
Non-Reducible (Fixed) Partly Reducible Reducible (Flexible)
Self External Force Tendency away from neutral
Position Windswept Tone/Movements LE
Normal Paralysis High tone Flaccid Spasticity Low tone Dystonia
Rocks/extends at hip Kicks into knee extension Pushes legs downward into footrests Spasms/tremors with or after movement
HI PS Neutral ABduct ADduct Neutral Right Left
Non-Reducible (Fixed) Partly Reducible Reducible (Flexible) Tendency away from neutral Dislocated Subluxed
Non-Reducible (Fixed) Partly Reducible Reducible (Flexible)
Self External Force Tendency away from neutral
KNEES FEET/ANKLES EDEMA SCALE
1+ (barely detectible)2+ (slight indentation,
15 sec. to rebound) 3+ (deeper indentation,
30 sec. to rebound) 4+ (> 30 sec. to rebound)
KNEES WFL L R WFL L R
& Limitations L R Limitations L R Dorsi-Flexed L R
FEET Non-Reducible (Fixed) L R Non-Reducible
(Fixed) L R Plantar Flexed L R
Partly Reducible L R Partly Reducible L R Inversion L R Reducible (Flexible) L R Reducible
(Flexible) L R Eversion L R
Tendency away from neutral L R Tendency away
from neutral L R
Edema + L + R Edema + L (fig. 8 in.) / + R (fig. 8 in.) Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)
6/15

Functional Good Head Control Describe Tone/Movement of Head and Neck HEAD Flexed Extended Adequate Head Control
& NECK
Rotated L Rotated R Limited Head Control Lat Flexed L Lat Flexed R Absent Head Control
Cervical Hyperextension Non-Reducible Partially Reducible Reducible (Fixed) (Flexible) Tendency away from neutral Self External force
ARMS SHOULDERS ELBOWS / FOREARMS Functional Reach (in.)
Tonal Influence Upper Extremities UEs:
Paralysis Flaccid Low tone High tone Spasticity Dystonia Other
Specific Strength/ROM Issues:
Functional L R Functional L R Elevated L R Flexed L R Right Left Depressed L R Extended L R Sitting Protracted L R Pronated L R Elevated Retracted L R Supinated L R Standing Subluxed L R L R Rotated L R L R Non-Reducible (Fixed) L R Non-Reducible (Fixed) L R Good UE mvmt/control Partially Reducible L R Partially Reducible L R Functional UE mvmt/control Reducible (Flexible) L R Reducible (Flexible) L R Limited UE mvmt/control Tendency away from neutral L R Tendency away from
neutral L R Absent UE mvmt/control
WRISTS WRISTS HANDS / FINGERS HANDS Functional L R Functional L R Handedness L R
Flexed L R Flexed L R Extended L R Extended L R Grip strength L # Deviated (describe) L R Deviated (describe) L R Grip strength R # Non-Reducible (Fixed) L R Non-Reducible (Fixed) L R Partially Reducible L R Partially Reducible L R Edema L + Reducible (Flexible) L R Reducible (Flexible) L R Edema R + Tendency away from neutral L R Tendency away from
neutral L R
MOBILITY EVALUATION
TRANSFERS and AMBULATION Transfers Ambulation
Independent Indep. ______ft. w/ device w/o device Standby Asst/Supervision w/ device w/o device Standby/Contact Assist
Check all that apply
Smooth/Level Surfaces Contact Guard w/ device w/o device Min Assist Carpet Min Physical Asst w/ device w/o device Mod Asst Uneven Terrain Mod Physical Asst w/ device w/o device Max Asst Curbs, Stairs Max Physical Asst w/ device w/o device Dependent Ramps/Inclines Distance ft.
Other Dependent / Unable to Ambulate Transfer Method
Comments Stand Pivot Sit/Squat Pivot Sliding Board Lift / Sling Required Recommend transfer training
Timed Up and Go Test sec. [60-69 yo. = 8.1sec (7.1-9.0), 70-79 yo. = 9.2 sec (8.2-10.2), 70-99 yo. = 11.3 sec (10.0-12.7)] Fall History: # of falls in the past 6 mo. _____ # of “near” falls in the past 6 mo. __________
EXPLAIN WHY PATIENT IS NON-AMBULATORY or NOT A FUNCTIONAL AMBULATOR Cardiac System Comments Circulatory System Musculoskeletal Sys Neuromuscular Sys Pulmonary System
Ambulation fluctuates due to
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)7/15

WHEELCHAIR SKILLS (Shown by Trial)Indep Assist Dependent
Unable N/A*
Manual W/C Propulsion Device trialed
*MWC ruled out due to
Safe Timely Distance __________ft. Able to propel the MWC forward Able to propel the MWC in reverse Able to propel the MWC turning right / turning left Recommend MWC w/c skills training Recommend dependent MWC (stroller / tilt in space)
Method Arm Left ☐ Right ☐ BothFoot Left ☐ Right ☐ Both
Power Assist Propulsion Skills Device trialed
Indep Assist Dependent Unable
N/A*
Operate Scooter (POV) Device trialed
*POV ruled out due toInability to safely transfer indep.Inability to sit in and use POVInability to operate the tillerHome does not support its useOther
Safe Timely Distance __________ft. Able to operate the POV forward Able to operate the POV in reverse Able to operate the POV turning right / turning left Able to transfer to / from POV independently Able to sit on and operate POV independently Recommend POV skills training
Comments
FEATURES REQUIRED FOR SAFE USE OF POV
Indep Assist Dependent Unable
N/A*
Operate PWC Device trialed
*PWC ruled out due toLower lever equipment meetspatient’s current mobility needsOther
Safe Timely Distance __________ft. Able to operate the PWC forward Able to operate the PWC in reverse Able to operate the PWC turning right / turning left Recommend PWC w/c skills training
Comments
EQUIPMENT TRIALS AND RESULTS
SUMMARY: The least costly alternative for safe, functional and independent mobility was found to be: Crutch/Cane Walker Manual w/c Dependent care mobility device (stroller/tilt-in-space) Manual w/c with power assist Scooter Standard Power w/c Complex Rehab power w/c
Goals for Wheelchair Mobility and Seating System Maximize independence with mobility in the home with mobility related ADLs (MRADLs) Maximize independence with mobility at school, work and/or in the community Dependent mobility for safe transport Provide independent pressure relief Provide tilt to facilitate pressure relief, postural control, and physiological functioning Provide recline to facilitate pressure relief, postural control, physiological functioning, ADL care Optimize pressure re-distribution Provide support needed to facilitate function or safety Provide corrective forces to assist with maintaining or improving posture Accommodate client’s posture- Current seated postures and positions are not reducible or will not tolerate corrective forces Client to be independent with relieving pressure in the wheelchair Enhance physiological function such as breathing, swallowing, digestion and/or bowel/bladder elimination Manage tone/spasticity Manage painPrevent medical complications and injuryEnhance ability to live in the community rather than as institution OtherOther
Comments
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)8/15

EQUIPMENT RECOMMENDATIONS and JUSTIFICATION MOBILITY BASE JUSTIFICATION
Manufacturer ____________________ Model __________________________ Color ___________________________ Seat Width __________ Seat Depth ___________ Seat to Floor Height __________
Can be grown to __________ Length of need ___________
provide transport from point A to B promote independent mobility not a safe, functional ambulator walker or cane inadequate non-ambulatory/cannot walk enhance ability to live in the community rather than an institutionother
width/depth necessary to accommodate anatomical measurement(s) equipment is a lifetime medical need decrease caregiver burdenprevent medical complicationsmanage painmaximize independence and self-determination
Standard Manual Wheelchair Base Travel Base Dependent Base
non-functional ambulator able to self-propel in residence unable to self-propel in residence
non-ambulatory/cannot walk
Lightweight Manual Wheelchair self-propulsion medical condition/weight of w/c affect ability to self-propel standard MWC marginal propulsion skills/can and does self-propel wheelchair fits throughout house
willing and motivated to use seat to floor height required to foot propel
High-strength Lightweight MWC
Hemi-height
self-propulsion medical condition/weight of w/c affect ability to self-propel standard MWC full-time daily use lower seat to floor height required to propel with foot/feet short stature
requires features not available on a lightweight manual w/c requires a specific seat width, depth, or height willing and motivated to use required to load w/c into vehicle
Ultra-lightweight MWC Axle Position Adjustment Required Vertical
UE biomechanics (100°-120° degree elbow flexion)
seat slope (dump) for propulsion, balance or pelvic stability
Horizontal stroke length reduce weight on casters
Rotational lateral stability
full time manual w/c user requiring individualized fitting and adjustments for multiple features that cannot be provided on a standard, lightweight or high-strength lightweight w/c improved UE access to wheels reduce UE overuse injury full time w/c user for ADLs increase ability to perform high-level wheelchair skills amputee placement
improved postural stability by changing angle change axle position with increased proficiency of use allow seat to back angle changes adjust center of gravity increase stability in wheelchair increase growth adjustability due to axle changes decrease footprint of w/c for increased maneuverability
Heavy-duty Manual Wheelchair Extra Heavy-duty MWC
accommodate user weight broken frame on previous chair extreme tone excess movement
Stroller Base infant/child unable to propel MWC independent mobility is not a goal currently unable to safely operate a PMD
non-functional ambulator non-functional UE
Power Assist cannot functionally operate a manual wheelchair shoulder pain during manual w/c propulsion less expensive option to POV/PWC repetitive strain injury in shoulder girdle requires conservation of energy to participate in MRADLs
unable to propel up ramps or curbs using a manual wheelchair unwilling to use power wheelchair has been using ultralight wheelchair base for more than a year home or transportation does not accommodate a power wheelchair
Scooter/POV non-ambulatory non-functional ambulator cannot functionally propel MWC
has adequate trunk stability can safely operate & is willing to can safely transfer home environment supports use
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)9/15

MOBILITY BASE JUSTIFICATION Power Wheelchair
Group 1 PWC Group 2 PWC Group 3 PWC required for suspension to
minimize pain manage tone/spasticity mitigate reflex activity maintain balance/upright sitting maintain posture/position/head control maintain contact with drive control
Group 4 PWC Group 5 PWC for pediatric use
non-ambulatory non-functional ambulator cannot functionally propel MWC cannot functionally and/or safely operate scooter/POV home environment does not support the use of a POV home environment supports use of power wheelchair can safely operate & is willing to can safely transfer/be transferred
requires speed adjustability requires torque adjustability requires sensitivity adjustability requires acceleration adjustability requires braking adjustability requires expandable electronics requires alternative drive control
required to negotiate an incline of ° required to negotiate obstacles/ threshold of in. required to traverse distances/terrain
SEAT FUNCTIONS/POSITION CHANGES JUSTIFICATION Tilt Base or Tilt Feature Added Forward Rearward Lateral
Powered tilt on power chair Powered tilt on manual chair
Manual tilt on manual base Manual tilt on power base
change position against gravitational force on head/trunk change position for pressure redistribution/cannot weight shift improve chewing, swallowing and/or digestion minimize risk of aspiration decrease respiratory distress facilitate visual orientation decrease pain blood pressure management
increase sitting tolerance facilitate safe transfers manage tone/spasticity rest periods/inability to transfer out of chair for rest assist/maintain postural alignment facilitate postural control maintain vital organ capacity manage autonomic dysreflexia manage orthostatic hypotension
Recline Semi (>15° but < 80°) Full ( > 80°)
Power recline on power base Power recline on manual base
Manual recline on manual base Manual recline on power base
accommodate femur to back angle full pressure redistribution/cannot weight shift head/neck positioning/support maintain muscle length/joint ROM manage tone/spasticity blood pressure management decrease respiratory distress manage bowel/bladder/catheter care, intermittent catheterization, undergarment, change facilitate safe transfers participation in ADL care
recumbent rest periods and sleeping in wheelchair repositioning increase sitting tolerance facilitate postural control use in conjunction with elevating leg rests to raise LE above heart to manage edema improve circulation decrease pain use in conjunction with tilt for optimal pressure redistribution as tilt alone does not accomplish effective pressure relief/ reperfusion
Power Anterior Tilt Power Adj. Seat Height Power Standing Feature
increase independence in transfers minimize risk of fall/injury in transfers increase independence in ADLs increase functional reach minimize over shoulder reach and risk for overuse injury decrease hyper lordotic neck position minimize eliciting STNR decrease pain improve bathroom function and safety
facilitate level eye position while communicating drive at elevated height for improved line of sight and safety increased weight bearing decrease joint contractures improve digestion and elimination provide pressure distribution away from scapula, sacrum, coccyx, and ischial tuberosities support educational/vocational goals
Power Leg Elevation Center mount foot platform Center mount foot platform w/ articulation
Elevating legrests Elevating legrests w/ articulation
manage LE edema improve circulation maintain LE muscle length/joint ROM position LEs at 90° when upright, not available with standard power ELRs indep. operation of ELRs needed, not available with center mount elevate LEs during tilt, recline or tilt and recline
maintain feet on footplate increase ground clearance over thresholds, curbs or uneven terrain center mount tucks into chair to decrease turning radius in the home-
not available with ELRs physically unable to operate manual elevating leg rests
ADDITIONAL INFORMATION ON POWER SEATING FUNCTIONS
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)10/15

PWC ELECTRONICS JUSTIFICATION Control/input device
Proportional Standard joystick Expandable joystick Specialty joystick (i.e., mini, compact) Head control Chin control Other extremity control _______________________________ Specialty joystick handle
Non-proportional Electrical switches Mechanical switches Head array Sip and puff
Combination Head array sip and puff
Other ____________________________
Body Part(s) _________________________ Left Right
provides access for controlling pwc required as part of an expandable system unable to generate sufficient force to
operate a standard joystick limited movement/strength to operate
a standard joystick required to operate the pwc with the
head, chin or other body part unable to use a std joystick handle
lacks motor control to operate proportional drive control unable to understand prop. controls lacks UE function for prop. controls needed to operate control using air
pressure through straw, tube, or wand
progressive disease/changing condition
expandable controller/ wire harness
required for proper set-up of electronics with multiple power seat functions (> 3 actuators)
harness is required with an expandable controller to provide necessary connectors for operation
Through drive control operation of power seat functions
required to operate one power seat function with an alternative drive control device required to operate two or more
power seat functions with an alternative drive control device
uses a joystick and is unable to operate a switch throughout the
full range of tilt or recline uses a joystick and is unable to
operate a switch throughout the full range of two or more power seat functions
Display box necessary for alternate controls allows user to see mode/ drive profile Tracking technology to minimize the need for excessive
movements to drive the chair over thresholds and on uneven surfaces required for use with non-proportional drive control to minimize the need for excessive drive commands for safety when using a latched driving system
lack of strength to make constant corrections to safely progress in a straight line forward lack of endurance to make constant corrections to safely progress in a straight line forward lack of coordination to make constant corrections to safely progress in a straight line forward
Mount for switches Mount for joystick
swing away for safe transfers attaches joystick, switches to w/c provides for consistent access
Attendant controlled joystick and mount
allow caregiver to control wheelchair In case of medical emergency or chair malfunction user requires assistance for safety in unfamiliar environments user is no longer able to operate drive
control device throughout the day
compliance with transportation regulations allow age/developmentally
appropriate assistance when driving
Batteries / charger required to power base charge battery for wheelchair Ventilator battery required to power ventilator Lights safe operation within the home once
dwelling lights are turned off increase visibility at night or during
inclement weather increased safety crossing street
Other
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)11/15

MOBILITY BASE COMPONENTS JUSTIFICATION Angle adjustable back Depth adjustable back Height adjustable back
postural control control of tone/spasticity accommodate range of motion
UE functional control accommodate seating system accommodate growth
Dynamic Back absorb forces exerted by user to improve durability of equipment absorb forces exerted by the user to prevent loss of position in seating sys
provide movement to decrease agitation provide sensory input enhance voluntary movement accommodate abnormal involuntary movement
Armrests
fixed adj. height removable
swing away flip back reclining full length desk length tubular
waterfall arm pad _________________
accommodate seat-elbow meas. provide support with elbow at 90° postural control / trunk support assist with pressure relief allow UEs to move w/ reclining back
change height/angle for ADLs remove for transfers access to table
Foot Platform/ Footrests/ Leg Rests one-piece footplate/foot platform standard tapered V-style center mount
footrests 60° 70° 80° 90° adjustable knee angle dynamic heavy duty fixed removable swing-away
manual elevating articulating
provide LE support enable safe transfers accommodate knee ROM limitation(s) maintain muscle length/joint ROM provide change in position for legs maintain feet on footplate independent LE positioning R /L manage tone/spasticity improve circulation use in conjunction with tilt, recline or tilt and recline to decrease edema
provide sensory input accommodate involuntary movement provide movement to decrease agitation absorb forces by user to increase durability of equipment absorb forces by user to prevent loss of position in seating system absorb movement without resistance to control tone
Foot Support
flip up fixed/rigid
adjustable angle R L multi-adjustable angle R L
dynamic contracture support
provide foot support accommodate ankle ROM provide foot support with proper pressure distribution allow foot to go under w/c base facilitate safe transfers
accommodate/facilitate movement absorb forces by user to prevent loss of position in seating system absorb forces by user to increase durability of equipment prevent foot/feet from falling off foot support
Propulsion wheel Size
Spokes mag spokes
increase access to wheel allow seating system to fit on base accommodate seat to floor height decrease overall weight of w/c
increase propulsion ability maintenance free larger wheel improves ability to negotiate thresholds/uneven terrain decrease wt. for loading into vehicle
Propulsion tires pneumatic semi-pneumatic flat free inserts solid
decrease maintenance prevent frequent flats user unable to maintain air in tires decrease rolling resistance
increase shock absorbency decrease pain decrease spasms
Wheel rims / Hand rims metal plastic coated ergonomic
Projections oblique vertical
increase self-propulsion with hand weakness/decreased grasp provide ability to propel wheelchair
reduce/mitigate carpal tunnel syndrome
Alternative propulsion methods
one armed drive R L lever activated gear reduction
enable propulsion of manual wheelchair with one arm functional use of only one UE
decrease shoulder pain increase energy efficiency for self-
propulsion
Quick release axle allows wheels to be removed to decrease size for storage
decrease weight for lifting
Amputee adapter unable to counterbalance in w/c due to loss of LE
increase rearward stability
Spoke protector protect hand/fingers from injury Wheel locks push pull scissor hub foot
Extension R L
stabilize wheel for transfers lock wheels to prevent rolling independent in applying wheel locks due to decreased reach or strength
allows complete wheel clearance in unlocked position to prevent injury during propulsion
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)12/15

MOBILITY BASE COMPONENTS JUSTIFICATIONCasters Size ____________
fixed caster housing adj caster housing shock absorbing casters
Caster tires pneumatic semi-pneumatic flat free inserts solid poly soft roll
maneuverability stability of wheelchair accommodate seat to floor height durability maintenance free/prevent flats angle adjustment for postural control decrease rolling resistance keep user weight evenly distributed for decreased energy expenditure
increase shock absorbency decrease pain decrease spasms increase leverage for improved obstacle and transition management decrease fatigue from road shock decrease weight for more effective propulsion
Shock absorbers/ suspension decrease vibration decrease pain
decrease spasticity increase sitting tolerance
Specific seat height Front _______________________________ Back _______________________________
foot propulsion transfers postural stability
accommodation of lower leg length
Anti-tipping device(s) minimize risk for rearward displacement or tipping
minimize risk for forward displacement or tipping
Side guards prevent skin tears/abrasions prevent body parts from becoming caught in wheel causing injury
provide hip and pelvic stabilization prevent clothing from getting caught in wheel causing injury
Transportation tie-down option crash tested brackets for safety Rear cane/ Push handles standard angle adjustable extended dynamic
caregiver access caregiver assist
allows “hooking” to maintain balance, perform pressure relief and participate in ADLs
Canopy protect user from the elements regulate sensory input
user has light sensitivity
Crutch/Cane holder IV hanger Cylinder holder Vent tray
stabilize ventilator/accessory on wheelchair
user is dependent on device
SEATING / POSITIONING COMPONENTS COMPONENT Mfg/model/size JUSTIFICATION
Seat cushion accommodate impaired sensation decubitus ulcers present history of decubitus ulcers increase pressure distribution
stabilize pelvis prevent pelvic extension accommodate obliquity/rotation accommodate multiple deformity promote hip/femur alignment
Seat cushion – Custom Molded
custom seat cushion required “off the shelf” will not accommodate deformity
Additional seat components Seat wedge accommodate ROM limitations aggressive seat shape to decrease
sliding down in the seat Cover replacement protect back or seat cushion Seat board Seat platform Back board
support cushion to prevent hammocking of upholstery
attach cushion/back to base accommodate seat to floor height
Back support provide posterior trunk support provide posterior/lateral trunk support accommodate deformity accommodate or decrease tone facilitate tone
provide lumbar/sacral support support trunk in midline pressure relief over spinous processes
Back cushion – Custom Molded
custom back cushion required “off the shelf” will not accommodate deformity
Additional back components Mounting hardware seat back removeable fixed swing away dynamic
attach seat platform/cushion attach back platform/cushion
sensory input accommodate/facilitate movement
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)13/15

COMPONENT Mfg/model/size JUSTIFICATION Pelvic positioner Single pull belt Dual pull belt Specialized belt SubASIS bar _________________
stabilize pelvis in neutral rotation neutralize destructive postural tendency counteract rotation counteract obliquity maintain contact with w/c cushion
pad for protection over boney Prominence(s) special pull angle to control tilt, rotation and/or obliquity
Lateral pelvic support
R L
pelvis in neutral accommodate pelvic deformity
accommodate tone
Lateral pelvic support hardware removeable fixed swing away dynamic
remove/swing-away for safe transfers accommodate/facilitate movement
Lateral thigh/ knee support
R L
position thighs in alignment accommodate windswept deformity
decrease LE abduction
Lateral thigh/knee support hardware removeable fixed swing away dynamic
remove/swing-away for safe transfers accommodate/facilitate movement
Medial thigh/ knee support
decrease adduction accommodate ROM limitations
accommodate windswept deformity
Medial thigh/ knee support hardware removeable fixed swing away/flip down dynamic
remove/swing-away for safe transfers accommodate/facilitate movement
Foot support Foot box Shoe holder(s)
R L
position foot accommodate deformity
provide stability decrease tone control position
Ankle strap Toe strap Heel loops Calf Strap
support foot on foot rest decrease extraneous movement position/ support foot
provide input to heel protect foot increase stability inhibit abnormal tone patterns
Lateral thoracic Supports
R L
decrease lateral trunk leaning accommodate asymmetry contour for increased contact
safety control of tone/spasticity
Anterior chest strap, vest, or shoulder retractors
decrease forward movement of shoulder accommodate of TLSO decrease forward movement of trunk accommodate/facilitate movement
added abdominal support alignment assistance with shoulder control decrease shoulder elevation increase trunk stability
Headrest support during tilt and/or recline provide posterior head support provide posterior neck support provide lateral head support provide anterior head support placement of switches
accommodate ROM limitations improve respiration improve chewing/swallowing accommodate tone/spasticity improve visual orientation
Neck support decrease neck rotation decrease forward neck flexion
Headrest hardware removeable fixed swing away/flip back multi-axis adjustable dynamic
mount headrest to back/base mount headrest swing away lateral head/facial supports mount anterior head support mount switches swing away, flip back or remove for safe transfers
accommodate ROM limitations sensory input accommodate involuntary movement help absorb forces by user to increase durability of equipment enhance functional movement
Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)14/15

COMPONENT Mfg/model/size JUSTIFICATION Upper extremity support Arm trough R L Hand support ½ tray R L Full tray swivel mount joystick cutout elbow block R L wrist straps R L
decrease UE edema reduce shoulder subluxation decrease gravitational pull on shoulder joint control tone/spasticity support midline trunk positioning provide support for UE function maintain hand in natural position
help prevent UE from falling off support during tilt and/or recline help prevent UE from striking objects in the environment, prevent injury allow proper placement of tray without interference with controller access to AAC/ Computer/ EADL or another AT device
Essential needs bag or pouch
Required to hold, and provide access to medically necessary
medicine special food orthotics
diapers/undergarments catheter and hygiene supplies ostomy and hygiene supplies clothing for changes/weather
Other
Other
Other
ADDITIONAL INFORMATION
Follow-up / Plan of Care
Patient Name Printed
Patient/Caregiver* Signature Date * Caregiver Relationship to Patient
I, the above signed patient, certify that I am willing and able to use the recommended equipment.
Therapist Name Printed Lic. #
Therapist’s Signature Date
Supplier’s Name Printed ATP #
Supplier’s Signature Date Therapist email and contact for reviewer This is to certify that I, the above signed therapist, have the following affiliations
DME Supplier Mfg. of Recommended Eq. Patient’s LTC Facility None
I concur with the above findings and recommendations of the therapist and supplier Physician’s Name Printed and preferred contact
Physician specialty
Physician’s Signature Date Wheelchair and Seating Evaluation: Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018)
15/15

Resources
• Amy Systems
• Invacare, Motion Concepts
• Quantum Rehab, Pride
• Sunrise Medical, Quickie
• Permobil, TiLite
• Colours
• 21st Century
• Motion Composites, Canada
• Ki Mobility
• Convaid
• Stealth