Embed Size (px)
Citation preview

The Assessment Of Sequential Antibiotics Therapy In University Malaya Medical Centre (UMMC)
Che Zuraini SulaimanPharmacist
UMMC
INTRODUCTION
Sequential Antibiotics Therapy the conversion of intravenous to oral antibiotic treatment using
the same medication (Lelekis, et al. 2001) Pre-set criteria to direct sequential antibiotic therapy vs
physician-directed conversion
Advantages Cheaper treatment costs (Lelekis, et al. 2001) Shortens LOS (Lelekis et al., 2001, Hunter et al., 1995, van der Eerden et
al., 2004) Reduce IV catheter-related complications ((Lelekis, et al. 2001, van
der Eerden et al., 2004, Vogel, F, 1995) Convenient to patients and hospital personnel (Vogel, F, 1995)
AIM & OBJECTIVES
AIM To assess the need to establish a sequential
antibiotic therapy program in UMMC
OBJECTIVES 1. To identify the current practice of IV-to-
oral conversions in UMMC2. To calculate the potential cost-savings of sequential antibiotic therapy
METHODOLOGY
STUDY DESIGN
prospective observational study
DURATION OF STUDYDec 2006 - Feb 2007
STUDY POPULATIONall patients admitted to UMMC receiving targeted antibiotics and fulfilling the inclusion criteria
CALCULATED SAMPLE SIZE302 (confidence level 95%, confidence interval 5%, estimated prevalence 0.50)

Targeted Antibiotics Ampicillin AzithromycinBenzypenicillin ClindamycinCloxacillin CotrimoxazoleAmoxicilin/clavulanic acid CiprofloxacinAmpicillin/sulbactam Cefuroxime

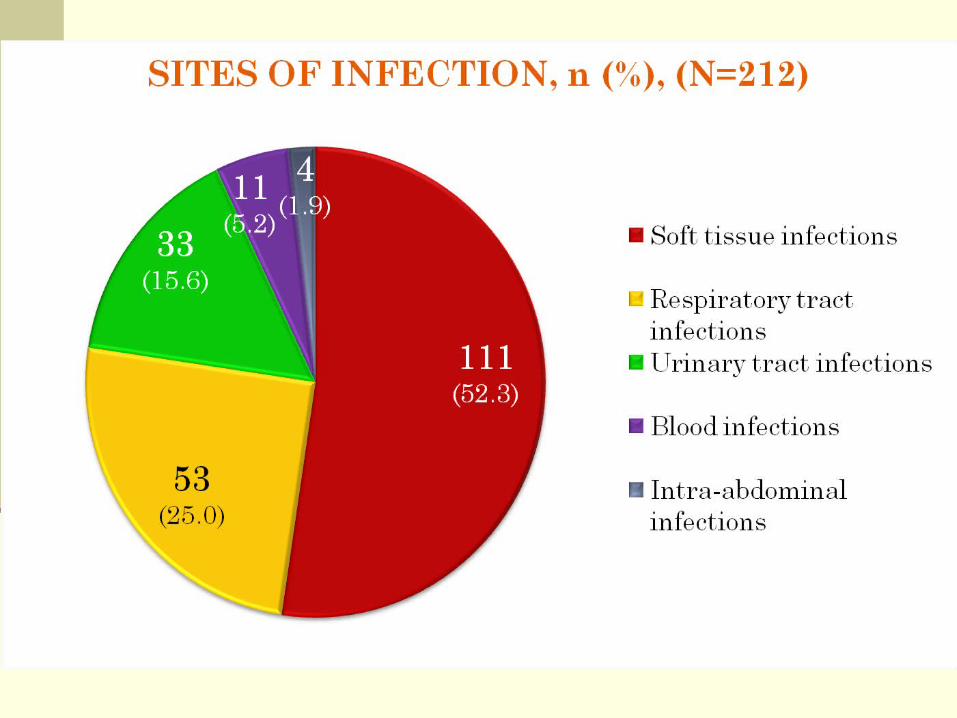
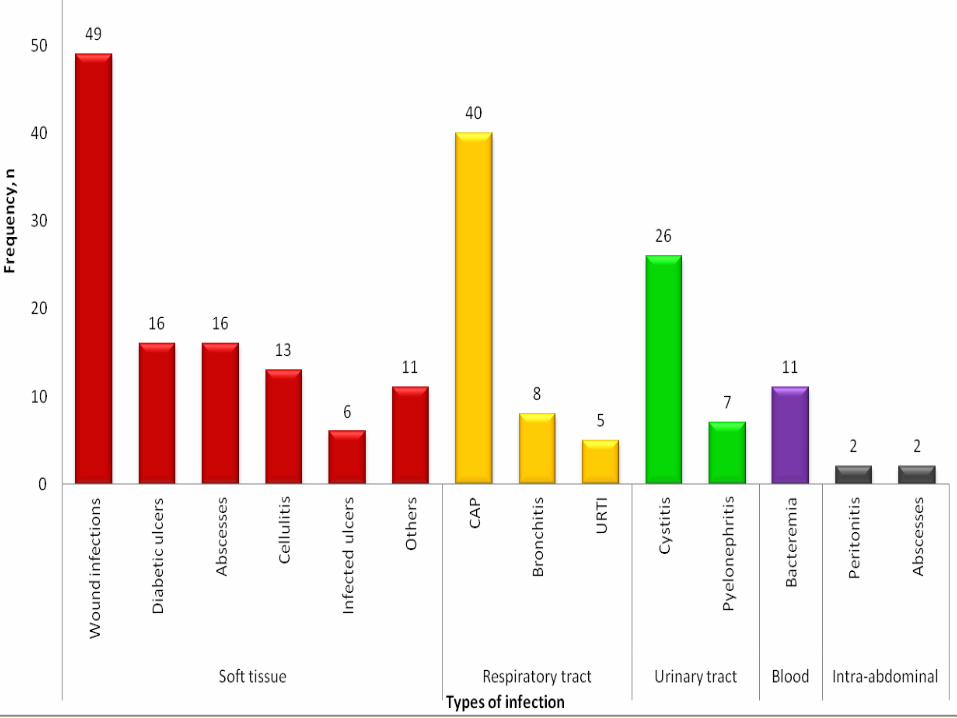
Inclusions-soft tissue infection-RTI-UTI-blood infection-intra-abdominal infection
ExclusionsMalignancyNeutropenia or immuno- compromisedConcomitant infections requiring IV antibacterials for sustained periodsPregnant or moribundConcomitant disease states that contraindicate the use of oral medications

CRITERIA FOR IV TO ORAL CONVERSION(based on Dundee Infectious Disease Unit Criteria for Intravenous-Oral Switch & Duke University Medical Centre Criteria for Switching to Oral Antimicrobial Therapy)
-Signs and/or symptoms of infection are improved or have resolved according to physician’s assessments
-Patient is afebrile (Temperature ≤37.9°C) or has had consistent improvement in fever over a 24-hour period
-White blood cells are normalizing (if repeated measurements are available)
-GI absorption of drugs is normal (absence of vomiting or abnormal GI anatomy)
-The patient is able to receive enteral therapy (orally or through gastric feeding tubes) as evidenced by concomitant enteral medications or nutrition
-No evidence of continuing sepsis with two or more of the following: temperature >38˚C, pulse >90 beats/min, respiratory rate >20 breaths/min or white cell count <4 or >12x109/L

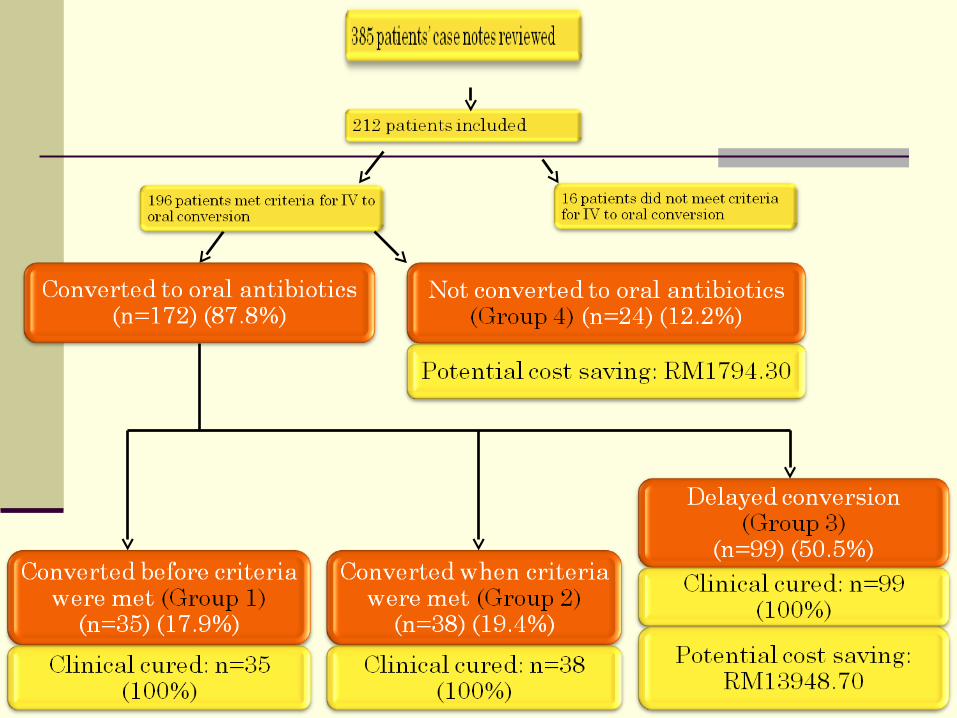
1)Percentage receiving sequential antibiotic therapy
2)Outcome of sequential antibiotic therapy
3)Potential cost savings of sequential antibiotic therapy
potential cost saving of sequential
antibiotic therapy
=
antibiotic acquisition cost for IV antibiotic
_
antibiotic acquisition cost
for oral antibiotic
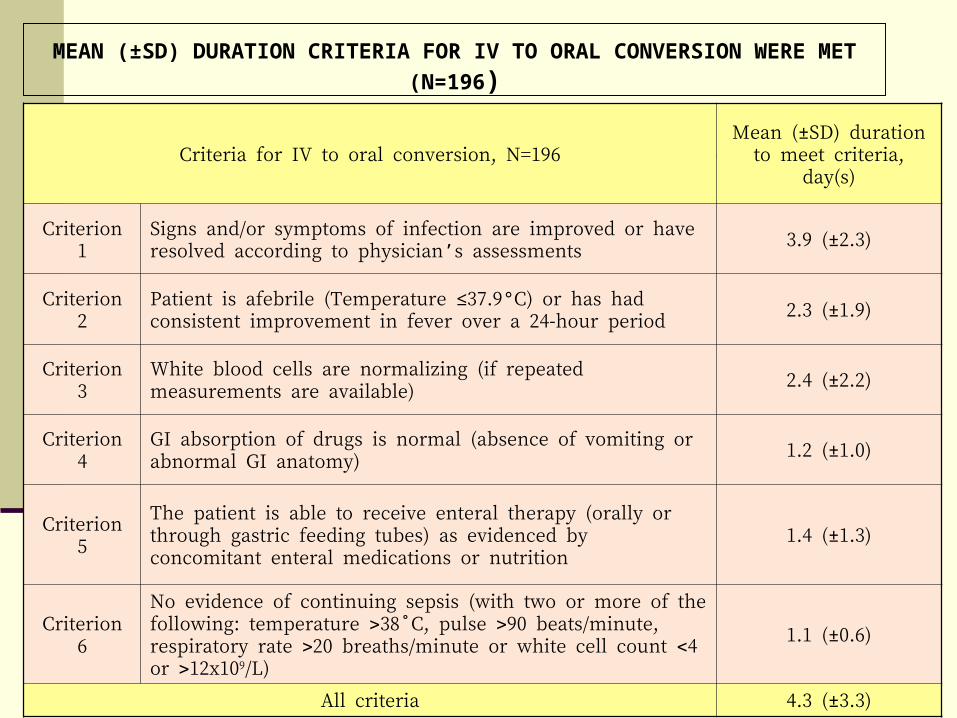
MEAN (±SD) DURATION CRITERIA FOR IV TO ORAL CONVERSION WERE MET
(N=196)
Criteria for IV to oral conversion, N=196Mean (±SD) duration to
meet criteria, day(s)
Criterion 1Signs and/or symptoms of infection are improved or have resolved according to physician’s assessments
3.9 (±2.3)
Criterion 2Patient is afebrile (Temperature ≤37.9°C) or has had consistent improvement in fever over a 24-hour period
2.3 (±1.9)
Criterion 3White blood cells are normalizing (if repeated measurements are available)
2.4 (±2.2)
Criterion 4GI absorption of drugs is normal (absence of vomiting or abnormal GI anatomy)
1.2 (±1.0)
Criterion 5The patient is able to receive enteral therapy (orally or through gastric feeding tubes) as evidenced by concomitant enteral medications or nutrition
1.4 (±1.3)
Criterion 6No evidence of continuing sepsis (with two or more of the following: temperature 38˚C, pulse 90 beats/minute, respiratory rate 20 breaths/minute or white cell count 4 or 12x109/L)
1.1 (±0.6)
All criteria 4.3 (±3.3)

IV TO ORAL CONVERSION OF ANTIBIOTICS ACCORDING TO SITES OF INFECTION (N=196)

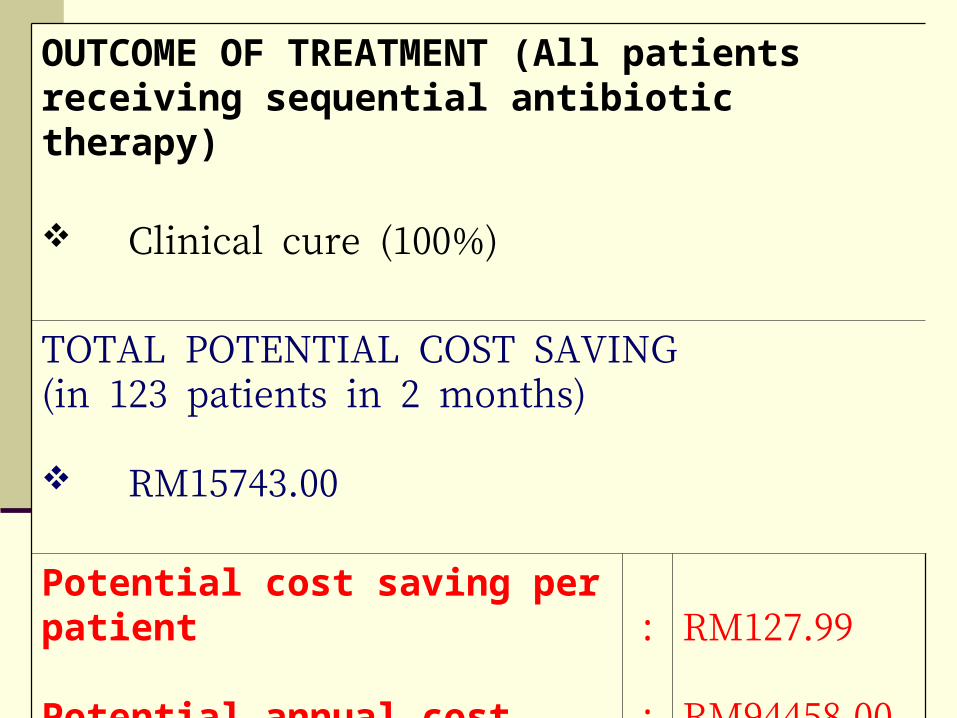
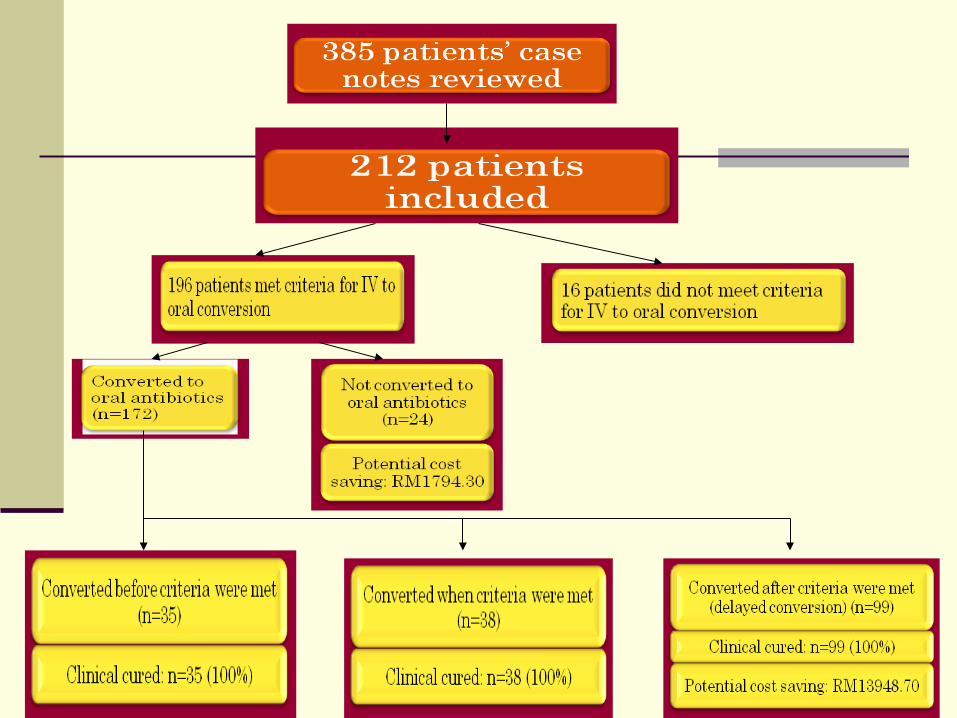
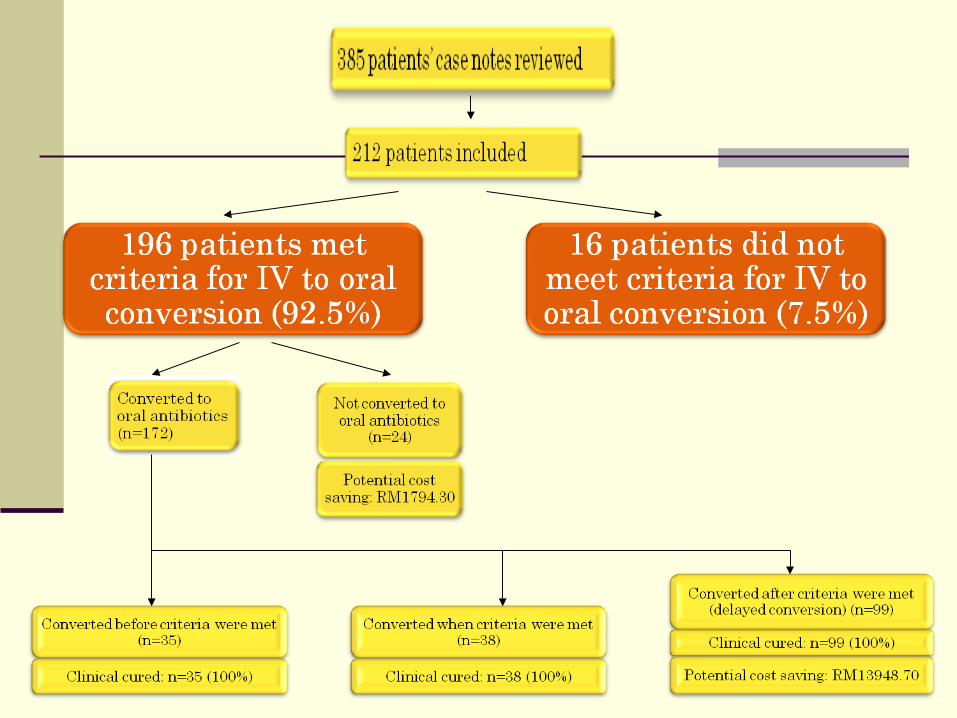
OUTCOME OF TREATMENT (All patients receiving sequential antibiotic therapy)
Clinical cure (100%)
TOTAL POTENTIAL COST SAVING(in 123 patients in 2 months)
RM15743.00
Potential cost saving per patient
Potential annual cost savings
:
:
RM127.99
RM94458.00
STUDY LIMITATIONSexclusion of patients receiving
targeted antibiotics that were kept as ward stock
inability to perform a detailed cost analysis
sequential antibiotic therapy is commonly practised in UMMC
the conversions from IV to oral antibiotics are often delayed
total potential cost savings was estimated to be approximately RM100,000 annually
RECOMMENDATIONS
Establishment of a safe and cost-effective policy of sequential antibiotic therapy in UMMC
Development of a set of criteria for IV to oral conversion with the help of ID team
Implementation of sequential antibiotic therapy program through team approach

Acknowledgement
Ms Ho See Wan1, Ms Reena Rajasuriar1, Prof Dr Adeeba A Kamarulzaman2
1 Department of Pharmacy, University Malaya 2 Infectious Disease Unit, University Malaya Medical Centre
1. Lelekis, M & Gould, IM 2001, ‘Sequential antibiotic therapy for cost containment in the hospital setting: why not?’, Journal of Hospital Infection, vol. 48, no. 4, pp. 249-257. Retrieved July 25, 2006, from Science Direct database.
2. Shah, PM 2000, ‘Sequential or switch treatment - which criteria should be fulfilled?’, International Journal of Antimicrobial Agents, vol. 16, no. 301, pp. 301-302. Retrieved July 25, 2006, from Science Direct database.
3. Hunter, KA & Dormaier, GK 1995, ‘Pharmacist-managed intravenous to oral step-down program’, Clinical Therapeutics, vol. 17, no. 3, pp. 534-540. Retrieved July 16 2006, from Science Direct database.
4. van der Eerden, MM, de Graaff, CS, Vlaspolder, C, Bronsveld, V, Jansen, HM & Boersma, WG 2004, ‘Evaluation of an algorithm for switching from IV to PO therapy in clinical practice in patients with community-acquired pneumonia’, Clinical Therapies, vol. 26, no.2,pp. 294-303.
5. Vogel, F 1995, ‘Sequential therapy in the hospital management of lower respiratory infections’, The American Journal of Medicine, vol. 99, no. supplement 6B, pp. 14S-19S.
6. Barlow, GD & Nathwani, D 2000, ‘Sequential antibiotic therapy’, Current Opinion in Infectious Diseases, vol. 13, no. 6, pp. 599-607.
Thank You
Formula
number of days of delayed conversion=number of days with IV antibiotic−day all criteria of conversion were met
acquisition cost for IV antibiotic=number of days of delayed conversionxbasic units of IV antibiotic given per dayxbasic unit acquisition price of IV antibiotic
acquisition cost for oral antibiotic=number of days of delayed conversionxbasic units of oral antibiotic given per dayxbasic unit acquisition price of oral antibiotic
the potential cost saving of antibiotic acquisition cost=antibiotic acquisition cost for IV antibiotic−antibiotic acquisition cost for oral antibiotic