Embed Size (px)
Citation preview

5o6
THE ASSESSMENT OF PLATELET FUNCTIONBy A. A. SHARP, M.D., B.Sc.
Lecturer in Haematology, United Oxford Hospitals
The blood platelets have attracted the attentionof several generations of clinicians, haemato-logists, physiologists and in recent years pharma-cologists and biochemists.Those who first described these cells, as
separate elements of the blood, recognized thatthey played an integral part in the sequence ofblood coagulation and in the mechanism ofhaemostasis (Hayem, I878, I882, I883; Bizzozero,i882; Eberth and Schimmelbusch, i888). Earlyhypotheses of the mechanism of fibrin formationin shed blood included the platelets as taking partin the series of reactions (Morawitz, I905; Nolf,I908; Howell, 19Io; Bordet and Delange, 19I2).The modern era of research in blood coagula-
tion has confirmed the important part that plate-lets play in blood coagulation, and it is now knownthat platelets contain or have adsorbed on totheir surfaces several factors which influence in-directly the rate and amount of fibrin formation.These may be summarized as follows:
Platelet Factor i accelerates the conversion ofprothrombin to thrombin by thromboplastin.
Platelet Factor 2 accelerates the conversion offibrinogen to fibrin by thrombin.
Platelet Factor 3, the major component of theplatelet's contribution to intrinsic thromboplastinformation (Fig. i). This is a phospholipoid.
Platelet Factor 4 has antiheparin activity(Creveld and Paullsen, 195I, I952; Creveld, '954;Alkjaersig, Abe and Seegers, 1955; Deutch,Johnson and Seegers, I955).
Platelet Factor I has been shown to be adsorbedplasma Factor 5 (Hjort, Rapaport and Owren,1955), but the other factors have a separateidentity from plasma coagulation factors.
In addition to the above factors, the plateletscarry small amounts of adsorbed antihaemophilicglobulin, Christmas factor, prothrombin andfibrinogen (Bounameaux, 1956; Seligman, 1957).It is possible that the platelets take part in theearly stages of blood coagulation, and, havingbeen activated by a product produced by inter-reaction between Hageman factor (Ratnoff andColopy, I955) and plasma thromboplastin ante-
Fi rure 1
1C,0:ZCO-Ln OF t SSETiZC- CP -LWD COCAGUJTICICT!
Ha-eman F-ctar Tlloasoa'rcbo-cnIatin("Contact') Antecedo3nt
Viscous Ietamor'hosi& PLA.J2] 'ro--hirat:.cs Facto,
Antihae 'hiic Chriotro,c ?<r.toro&'ulin -
'al iUL'Ilt^i1tlsicChrooboto1)ao:tirrissue Thrornbop1a.o;tin
Factor tI
Stuart-'o,-erFactor
Factor VII
Protloror:bin-- Active 2rr;WoLborlctin
Throaobin Fibrino-enFilurin
cedent (Rosenthal, Dreskin and Rosenthal, I955),release their phospholipoid component to reactwith antihaemophilic globulin and Christmasfactor to form intrinsic thromboplastin (Fig. i).This hypothesis is based on experimental workdetailed by Biggs, Sharp, Margolis, Hardisty,Stewart and Davidson (1958).
If blood is allowed to clot in vitro fibrin forma-tion is preceded by the aggregation and fusion ofplatelets into amorphous masses (viscous meta-metamorphosis) (Eberth and Schimmelbusch,i888; Tait and Burke, 1926; Sharp, I958). Thismechanism is thought to be identical with thatobserved in the lumen of damaged blood vesselswhere the platelet clumps appear to constitute animportant barrier to prevent the escape of bloodthrough the damaged vessel wall (Zucker, I947,I949; Fulton, Ackers and Lutz, 1953).
Protected by copyright.
on June 3, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.407.506 on 1 Septem
ber 1959. Dow
nloaded from

SHARP: The Assessment of Platelet Function
The role of platelets in haemostasis has beenthe subject of argument (Macfarlane, I941), yetthe evidence is in favour of their playing a majorrole in this mechanism either by virtue of theirforming a mechanical block or by promotingfibrin formation at the site of injury. In recentyears the platelets have been found to contain orcarry pharmacologically active amines, namely,5-hydroxytryptamine (5HT) (Zucker, Friedmanand Rapport, 1954), adenosine triphosphate(ATP) (Born, I956), adrenaline and nor-adrenaline(Weil-Malherbe and Bone, I954). 5HT has beenidentified as the vasoconstrictor principle inclotted blood (Zucker et al., 1954; Hardisty andStacey, 1955). Antifibrinolytic activity has alsobeen detected in platelet extracts as has theenzyme acid phosphatase (Johnson and Schneider,1953; Creveld, I954; Stefanini and Murphy,I956; Zucker and Borrelli, 1959).
It is evident, therefore, that any deficiency inplatelet function must cause either inefficientcoagulation of the blood, or a breakdown of thenormal haemostatic mechanism, or both. Thusin any patient with an obscure haemorrhagicdiathesis, if no abnormality of plasma factors canbe detected, platelet function must be measured.
Clinical States Associated with AbnormalPlatelet FunctionThe commonest type of platelet abnormality is
a reduction of the absolute number of circulatingcells (thrombocytopenia). The causes of thissyndrome are multiple and will not be discussedhere. Alternatively, a variety of clinical stateshave been described where, the numbers ofplatelets being normal, there has been bleedingof purpuric type similar to that associated withthrombocytopenia. This bleeding usually occursspontaneously from mucous membranes, frominternal surfaces of the body such as the renaltract, but does not result in massive tissuehaemorrhages so characteristic of plasma factordefects. The number of different names appliedto this non-thrombocytopenic syndrome has ledto confusion (Soulier and Larrieu, I954), but it ispossible to divide this syndrome into two mainsub-groups. One consists of cases of a hereditaryhaemorrhagic state, the only constant abnormalfinding being a prolonged bleeding time (vonWillebrand's syndrome). In all other respectsplatelets appear to be normal.The other is a heterogenous group, where a
hereditary or acquired functional deficiency of theplatelets can be demonstrated. The terms' thrombopathy," thrombocytopathia ' or ' throm-boasthenia' have been applied to this group.An increase in the number of circulating plate-
lets is also associated with a similar clinical syn-
drome. The term ' thrombocythaemia ' is usedto describe this condition.
Methods for Assessing Platelet FunctionNumbers of Circulating PlateletsThe determination of the number of circulating
platelets is the first essential in assessing plateletfunction. The direct counting method of Brecherand Cronkite (1950), using i per cent. ammoniumoxalate, has been found to be reliable. Thenormal range varies with the method used, butusually is within the range 150,000-300,000cu.mm. Significant thrombocytopenia exists ifthe count is below ioo,000 cu.mm.
Indirect methods of counting have not beenfound to be so reliable as direct methods.
Platelet MorphologyThis has been studied by various methods:(I) In normal blood films stained by Roman-
owsky dyes (Bernard and Soulier, 1948;Hardisty and Wolff, 1955).
(2) By phase contast microscopy (Bessis andTabuis, I955; Bernard, Caen and Maroteau,1957).
(3) Electron microscopy (Bessis and Burstein,I948; Bloom, 1955).
By any method it is difficult to define accuratelythe variations in normal morphology and only byexamining large numbers of preparations is itpossible to establish any criteria of normal andabnormal morphology. The most easily recog-nized abnormality is a marked variation in theshape and size of the platelets with the presenceof definite giant forms which may vary from 5 to2zo. in diameter. This feature is easily deter-mined by either of the first two methods whichare also useful for determining the presence ofplatelet clumping or viscous metamorphosis inany given platelet preparation.
Variation in the minute structure of platelets isdifficult to determine by direct or phase micro-scopy and resort must be made to electronmicroscopy. Normal platelets dried on theFormvar grid for electron microscopy showpseudopod or dentrite formation by the struc-tureless hyalomere around the periphery of thecell. The absence of this phenomenon has beenregarded as evidence of abnormal platelet mor-phology (Braunsteiner, Felliger and Pakesch,1954; Ulutin, I958), and has been described incases of thrombopathia. This method also allowsdetailed study of platelet clumping and disinte-gration in viscous metamorphosis (Bloom, 1955;Marx, Stich and Ehrhart, 1956; Koppel, I958).As electron microscopy becomes more univer-
sally available for the routine study of platelet
September I959 507
Protected by copyright.
on June 3, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.407.506 on 1 Septem
ber 1959. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
morphology, so more exact criteria of normal andabnormal morphology will be established.
Megakaryocyte morphology is abnormal in cer-tain thrombocytopenic syndromes (Dameshek andMiller, I946), but no definite abnormalities havebeen described in association with other func-tional platelet deficiencies apart from hyperplasiain the marrow of patients with thrombocythaemia(Hardisty and Wolff, I955).
Bleeding TimeThe best available test of primary haemostasis
is the bleeding time. The role of platelets inhaemostasis has already been discussed brieflyand any significant deficiency of their functiondue to a reduction in numbers or due to a func-tional deficiency is usually accompanied by aprolongation of the bleeding time.The method described by Ivy (Biggs and
Macfarlane, I957) is more likely to reveal milddefects in the haemostatic mechanism than theDuke method. The normal range of the formermethod is I to 6 minutes. In males the bleedingtime is rarely prolonged beyond 4 minutes.
Capillary FragilityPlatelet dysfunction is often associated with
abnormal fragility of the capillaries. Tests thatmeasure this fragility cannot, however, be usedto measure platelet function.
Clot RetractionThe retraction of fibrin after clotting has taken
place is a function of normal intact and viableplatelets and this phenomenon is partially ortotally absent if the numbers of platelets in theclotting blood is reduced (Budtz-Olsen, 195I).Imperfect retraction in the presence of a normalnumber of platelets represents a functional defectof the-platelets and examples have been recordedby Imerslund (1947), Alexander and Landwehr(I949), Jackson, Hartman and Conley (1953).The test of clot retraction in whole blood is simpleto perform and provides consistent results innormal whole blood where the clot retracts by40-60 per cent. in i hour after fibrin formation(Biggs and Macfarlane, 1957).
Prothrombin Consumption IndexIt has already been described how platelets
may play their part in the formation of thrombo-plastin and the consequent conversion of pro-thrombin to thrombin. Thus, if the numbers ofcirculating platelets are reduced or their functionaltered in respect of Platelet Factor 3, the amountof prothombin converted to thrombin, duringcoagulation of the whole blood, will be reduced(Quick, Shaneberg and Stefanini, 1949).
TABLE IPROTHROMBIN CONSUMPTION INDEX (Biggs andMacfarlane, 1957) MODIFIED TO DEMONSTRATE
ABNORMAL PLATELET FUNCTIONTo o.s ml. platelet-poor native plasma is added o.5 ml.platelet-rich native plasma and the mixtures allowed toclot at 370C. The amount of residual prothrombin is
measured at 30 minutes and i hourPlatelet-rich
nativeplasma Normal Patient Normal Patient
Platelet-poornativeplasma Normal Normal Patient Patient
The expectedProthrom-bin con-sumptionindex whena plateletdefectexists Normal Abnormal Normal Abnormal
The test of prothrombin consumption describedby Merskey (I950) is a sensitive indicator ofplatelet function provided no plasma coagulationfactors necessary for thromboplastin formationare absent.Where whole blood shows abnormal pro-
thrombin consumption, a sensitive test of plateletfunction has been evolved in this laboratoryusing the same basis of prothrombin consumption(see acknowledgments). The relative amounts ofresidual prothrombin are estimated when mix-tures of normal and test platelet-rich and platelet-poor native plasmas are allowed to clot at 370 C.(Table I).This test has been found to be a sensitive
method of determining a reduction or a failureof release of Platelet Factor 3.
Thromboplastin Generation TestThe ability of the platelets to generate normal
amounts of thromboplastin in conjunction withother plasma factors can be estimated by theabove test (Biggs and Douglas, 1953). This hasbeen the test most widely used in the measure-ment of platelet function and it is presumed thatit does measure selectively the phospholipoidfraction or Platelet Factor 3 (Soulier and Larrieu,'954; Nicola, I954; Soulier. Larrieu and Wartelle,I955; Braunsteiner, 1955; Bernard, Caen andMaroteau, I957; Bonnin, 1957). Washed sus-pensions of platelets from the patient are com-pared with a similar suspension prepared fromnormal blood. Care must be taken to ensurethat the number of platelets in each suspensionis similar and this may be achieved by comparingthe relative opacity of the suspensions by use ofa visual photometer or a photoelectric colorimeter.
508 S-eptember I959P
rotected by copyright. on June 3, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.407.506 on 1 S
eptember 1959. D
ownloaded from

September 1959 SHAIRP: The Assessment of Platelet Function 509
...... . . . . .....
a .A....A....
T"!~:il*;?.SOM
TPi;,4
r N.l.. ..4-.........................M~
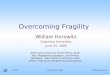
FIG. 2.-Thromboelastograph. These tracings show the effect of thrombo-cytopenia on the clotting of plasma as measured by the thromboelasto-graph. The figures to the left of the tracings indicate the numbers ofplatelets in the samples of plasma tested.
The thromboplastin generation test sometimesfails to detect mild defects of platelet functionand may be sensitized by making progressivedilutions of both suspensions and retesting.Further sensitization may be achieved by lysingthe platelets in distilled water. The failure ofthe lysed platelets to generate normal amounts ofthromboplastin suggests that they are abnormallyresistant to hypotonic solutions, and such resist-ance is thought to be characteristic of platelets inthrombopathy of a secondary type (Centingil,Ulutin and Karaca, 1958). If platelets, whichshow abnormal thromboplastin generation by con-ventional tests, show normal generation afterlysis, the condition is probably an inheritedabnormality (Ulutin and Karaca, 1956).
It has been found that the thromboplastingeneration test is a less sensitive indicator ofplatelet dysfunction than the test for prothrombinconsumption. This is possibly the result ofpartial platelet damage while preparing the washedplatelet suspension.
Platelet Activity in SerumO'Brien (I955) pointed out that serum coII-
tained platelet-like activity when added to plate-let-free plasma and that this activity was notpresent in serum derived from platelet-freeblood.
Alagille and Soulier (1957), modifying O'Brien'soriginal method, determined the ability of serumcontaining platelet-like material to correct theprothrombin consumption when platelet-freeplasma was allowed to clot. They confirmedthat this activity depended on the number ofplatelets in the blood from which the serum wasderived and in addition they found abnormalserum activity in some cases of thrombopathy.While this method may confirm platelet abnor-malities detected by other methods, it is possiblethat this platelet-like activity of serum may bedependent on a factor or factors still to be definedand that cases where a defect can be demonstratedconstitute a separate syndrome (Braunsteiner andPakesch, 1956).
Protected by copyright.
on June 3, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.407.506 on 1 Septem
ber 1959. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
ThromboelastographyThe ingenious apparatus devised by Hartert
(I95i) has been used to measure platelet activity.It records photographically the onset of fibrinformation, the speed of increasing clot rigidityand the tenacity of the formed clot. Thesefactors are all altered proportionally as thenumbers of platelets in the clotting blood arediminished (Fig. 2), and similar findings may befound in cases of thrombopathy (Introzzi andNicola, I956).Although an expensive apparatus, it can provide
a convenient method of detecting possible plateletdefects, but it does not obviate the necessity ofperforming other tests to define the culpability ofthese cells.
Platelet Viscous MetamorphosisThe ability of platelets to clump and fuse
together prior to fibrin formation has already beendescribed. This phenomenon has been shown tobe a constant feature of normal platelet sus-pensions (Sharp, 1957a, 1958), and if absent mustrepresent an abnormality of platelet function dueeither to an inherent defect of the cells or to adeficiency of certain coagulation factors (Biggset al., 1958). Abnormalities in platelet clumpingor viscous metamorphosis have been described incases where abnormal function has been suspected(Soulier et al., I955; Braunsteiner, I955; Seref-Inceman, I955, J956; Centingil et al., I958), butabnormalities of viscous metamorphosis do notnecessarily occur in every case where abnormalplatelet function can be detected by other tests(unpublished observations).
Platelet AdhesivenessThe ability bf platelets to adhere to glass
surfaces has been studied quantitatively by manyworkers, including Wright (I941), Weiner, Zelt-macher, Reich and Shapiro (1948), and Bouna-meaux (1958). The failure of the platelets toadhere to these surfaces has been thought to bea measure of platelet dysfunction (Moolten,Vroman and Vroman, I949; Seref-Inceman, I956).Bounameaux (1957) has suggested that adhesive-ness and viscous metamorphosis are in factsynonymous and it is probable that the quanti-tative measurement of adhesiveness may also bea quantitative measurement of viscous meta-morphosis. Viscous metamorphosis can, however,take place without the platelets showing anytendency to adhere to glass (personal observation).The test of adhesiveness may be a better measureof increased coagulability of the blood than ofdecreased platelet function (MacDonald andEdgill, 1957).
Platelet AminesPlatelet 5-hydroxytryptamine (5HT) and adeno-
sine trophosphate (ATP) can be measured quan-titatively as can the ability of platelets to release5-hydroxytryptamine on clotting. Further, theability of these cells to absorb sHT from thesurrounding medium can also be assessed. Thevasoconstrictor action of 5HT has already beendescribed and this amine is released from theplatelets as they clump (Zucker and Borrelli,I955). Doubt has been cast on the haemostaticactions of sHT by Haverbach, Dutcher, Share,Tomch, Terry and Brodie (I957), who showedthat when circulating platelets were deprived of5HT by the action of Reserpine no abnormalityof haemostasis could be detected. Yet in somecases of thrombocythaemia and thrombocyto-pathia abnormalities of platelet function havebeer associated with abnormally low levels ofplatelet 5HT (Bigelow, 1954; Zucker and Borrelli,I956; Hardisty and Wolff, 1955; Quiry, Caenand Bernard, 1958). Platelets contain a largeamount of ATP (Born, 1956), but the role of thisamine has not yet been defined. Two hypotheseshave been advanced: ATP may bind sHT selec-tively in the platelets as adrenaline is bound inthe adrenal glands, or alternatively it may beresponsible for the active uptake of 5HT by theplatelets. It may be that both are correct (Bornand Gillson, 1959; Born and Bricknel, 1959).Platelets once they are removed from the bodyand stored lose their amine content within 24hours (Born, 1959), and this loss of activity mayrepresent an important loss of platelet viability.This aspect of platelet physiology will be dis-cussed later.The accurate estimation of these amines in
platelet extracts necessitates the use of complextechniques which are not readily available to theroutine haematologist.
Platelet Fragility TestsThe lysis of platelets by hypotonic saline solu-
tions has been observed (Gurevitch and Nelken,I956; Morita, 1958) and increased resistance tolysis has been encountered in cases of thrombo-pathy (Ulutin and Karaca, 1956).
Micro-electrophoresisThe principles of electrophoresis of platelets
have been applied to platelet suspensions con-tained in special cells (Bigelow and Desforges,I953; Ross and Ebert, 1959). Variations in plateletmobility in such a system must depend on theirsurface charge and, as this charge probably con-trols many of their activities, application of this
S-eptember I95951IP
rotected by copyright. on June 3, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.407.506 on 1 S
eptember 1959. D
ownloaded from

SHARP: The Assessment of Platelet Function
method to the problem of detecting abnormalplatelet function is a worthwhile task.
Analysis of the platelet constituents, especiallythe protein and phospholipoid fraction, by con-ventional paper electrophoresis (Donner, Machand Brancava, 1958) may lead to more specificdetermination of fractions than can be achievedby coagulation tests.
Platelet SurvivalA crucial test of platelet viability is to deter-
mine whether they survive for their normal spanin the blood of normal persons. Normal plateletstagged with radioactive di-isopropylfluorophos-phate (DFP32) and sodium chromate (Cr5l) havebeen found to survive for 9- iI days in the cir-culation of normal individuals (Leeksma andCohen, 1956; Aas and Gardner, 1958), SO ab-normal survival of platelets in the circulatingblood of normal persons must represent diminishedplatelet viability. Whether such shortening ofsurvival is characteristic of thrombopathia has yetto be determined.
Platelet TransfusionIn any case where a platelet defect is thought
to be responsible for abnormal haemorrhage andwhere all attempts to measure this abnormalityhave failed, the therapeutic effect of the trans-fusion of normal platelets may be of value.Evidence of clinical and haemostatic improvementby such a transfusion confirms the presence ofplatelet dysfunction. The association of this testwith a survival study of the transfused plateletsmay also be of value. If normal platelets fail tosurvive normally when transfused into thepatient's circulation it does suggest that somefactor external to the platelets is destroying ordamaging them in the circulation (Sprague,Harrington, Lange and Shapleigh, 1952).
Other Platelet FactorsNo case has yet been described where Platelet
Factor 2 has been found to be deficient.Creveld and Paullsen (1952) and Soulier and
Larrieau (1954) report abnormalities in theamount of Platelet Factor 4 in association withother platelet defects.
Deficiencies of platelet antifibrinolytic activityhave been reported in patients with abnormalplatelet function (Stefanini and Murphy, I956).The accurate measurement of these latter factors
is difficult to determine and there is little evidencethat the trouble involved is worthwhile.
DiscussionAttempts to measure platelet function often
produce equivocal results. This is undoubtedly
due to the platelets being partially damagedduring collection of the blood, the preparation ofplatelet-rich plasma and the preparation of plateletsuspensions free from plasma. One major factorthat has been found to cause platelet damage isfaulty venepuncture technique and this variableis more likely to cause non-specific alterations ofthe platelets than any other (Sharp, I957b).Such non-specific damage may result in abnormalplatelets appearing to be normal (see thrombo-plastin generation test), or alternatively normalplatelets may be so damaged by collection thatthey may appear to have abnormal function.By far the best preparation for assessing platelet
function is native plasma prepared in the coldwithout anticoagulant (Sharp, 1958). With thismethod it is possible to reduce non-specific factorsto a minimum and to study viscous metamor-phosis, platelet morphology and the ability ofplatelets to promote prothrombin consumption.A study of the results of platelet function in
patients with haemorrhagic symptoms suggeststhat certain clinical groups can be recognized.The following classification has been suggested(Biggs and Macfarlane, 1957) and has much tocommend it:
I. The thrombocytopenicgroup is self-explanatory.It must be stressed that not all patients withthrombocytopenia show evidence of spontaneoushaemorrhage or abnormal haemostasis, and it isprobable that haemorrhagic symptoms developonly when thrombocytopenia and abnormal plate-let function co-exist (Bonnin, 1957).
2. The von Willebrand's syndrome. In thissyndrome a prolonged bleeding time is associatedwith normal numbers of platelets and normalplatelet function, but now unusually low levels ofantihaemophilic globulin appear to be the mostconstant defect encountered in this syndrome.Whether this latter factor, associated with acapillary defect, such as that described by Mac-farlane (1941), or with some as yet undefinedplasma factor (Nilsson, Blomback, Jorpes, Blom-back and Johansson, 1957), is responsible for thehaemostatic defect has yet to be defined. On theevidence that exists at present this syndrome doesnot justify classification with other examples ofplatelet dysfunction.
3. Thrombopathia, thrombopathy, thrombocyto-pathia. This group is associated with normalnumbers of platelets but with abnormal pro-thrombin consumption, decreased thromboplastin-forming ability, and prolonged bleeding time, allother platelet function tests being normal. Twosub-divisions of this group exist, namely, (a) thosepatients with a definite familial haemorrhagicstate, and (b) those where the platelet defect wassecondary to a disease process such as uraemia,
September 19519 5-ItP
rotected by copyright. on June 3, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.407.506 on 1 S
eptember 1959. D
ownloaded from

512 POSTGRADUATE MEDICAL JOURNAL September 1959
liver disease, scurvy and congenital heart disease(Lewis, Zucker and Ferguson, 1956; Lewis, Fer-guson, Spaugh, Fresh and Zucker, I957; Centingilet al., I958; Alagille, Heim, Guery, Passeleeq,Blondeau and Dubost, I958). Evidence of throm-bopathia is occasionally encountered in patientsrecovering from an episode of thrombocytopenia(Creveld, Liem Khe Ho and Veder, I958).
4. Thromboasthenia. Coagulation function inthis group is normal in respect of prothrombinconsumption and thromboplastin generation, butclot retraction, agglutination or viscous meta-morphosis are abnormal. In manv instances thebleeding time is also prolonged. The number ofplatelets is within normal limits.
5. Thrombocythaemia. Increased numbers ofcirculating platelets in this syndrome are fre-quently associated with abnormal thromboplastingeneration and prothrombin consumption and along bleeding time. Clot retraction is normal orgreater than normal (Hardisty and Wolff, 1955).
Other cases are encountered which do not fitinto this classification and these must be namedafter the specific platelet factor which is reducedin activity or absent.A word must be said on the difference between
normal platelet function and platelet viability.When platelet transfusions are given to improvehaemostatic function in the thrombocytopenicpatient, fresh blood, platelet-rich plasma or plateletconcentrates must be used, as any preparationmore than 24 hours old does not appear to conferany beneficial effect. Yet the platelets frompreparations several days old and which have losttheir ability to improve haemostasis, still functionnormally in respect of clot retraction, viscousmetamorphosis, prothrombin consumption andthromboplastin generation (Mustard, I956; Sharp,unpublished observations). Therefore, unless ourconcepts of the beneficial effects of transfusedplatelets are wrong, normal platelet function andnormal platelet viability are not synonymousterms. The only platelet factors that are knownto deteriorate rapidly in the first 24 hours afterremoval from the body are sHT and ATP (Born,1959), and as they may play an important rolein haemostasis, measurement of these amines maybe a useful method of assessing platelet viability.The viability of platelets may also be estimatedby measuring their metabolic activity in respectof oxygen consumption (Campbell, Small andDameshek, 1956), but it is unknown whether theability of platelets to consume oxygen and theirability to correct a defective haemostatic mechan-ism disappear at the same time.
In conclusion, the methods we have availablefor the measurement of platelet function are notentirely reliable, but in many instances they
provide information of value in the assessment ofclinical cases. Simpler and more rapid methodsare needed to establish the presence of plateletdefects in those cases of non-thrombocytopenicpi,rpura that are encountered. The modern trendof research would suggest that these new testswill be biochemical in nature rather than newtests of coagulation function.
SummaryMethods for measuring platelet function have
been described and their inadequacies discussed.The need for new and more reliable tests isstressed.
AcknowledgmentsI am indebted to Dr. M. Willoughby, Radcliffe
Infirmary, Oxford, for permission to publishdetails of this modification of the prothrombinconsumption test.
BIBLIOGRAPHYAAS, K. A., and GARDNER, F. H. (I958),J. clin. Invest., 37, 1257.ALAGILLE, D., and SOULIER, J. P. (1957), Rev. Franfaise,
2, 231.ALAGILLE, D., HEIM, R., GUERY, J., PASSELEEQ, J.,BLONDEAU, J., and DUBOST, Ch. (l958), Ibid., 3, 322.ALEXANDER, B., and LANDWEHR, G. (I949), New Engl. J7.Med., 241, 965.ALKJAERSIG, N., ABE, T., and SEEGERS, W. H. (I955)Amer. J. Physiol., x8I, 304.BERNARD, J., and SOULIER, J. P. (I948), Sem. H6p. Paris, 97,I.BERNARD, J., CAEN, J., and MAROTEAU, P. (1957), Rev.Hemat., 12, 222.BESSIS, M., and BURSTEIN, M. (1948), Ibid., 3, 48.BESSIS, M., and TABUIS, J. (i955), Ibid., 10, 753.BIGGS, R., and DOUGLAS, A. S. (I953), . clin. Path., 6, 23.BIGGS, R., MACFARLANE, R. G. (1957), 'Human BloodCoagulation and its Disorders,' Blackwell Scientific Publica-tions, Oxford.BIGGS, R., SHARP, A. A., MARGOLIS, J., HARDISTY,R. M., STEWART, J., and DAVIDSON, W. M. (I958),Brit. .7. Haemat., 4, 177.BIGELOW, F. S. (954), . Lab. clin. Med., 43, 759.BIGELOW, F. S., and DESFORGES, J. F. (0953), Amer. Y. Med.,
'4, 495.BIZZOZERO, G. (1882), Virchows Arch., 90, 26I.BLOOM, G. (I955), Z. Zellforsch., 42, 365.BONNIN, J. A. (I957), Aust. Ann. Med., 6, I96.BORDET, J., and DELANGE, J. (1912), Ann. Inst. Pasteur, 26,657.BORN, G. V. R. (1956), Biochem. Y., 62, 33.BORN, G. V. R. (I959), personal communication.BORN, G. V. R., and GILLSON, R. E. (959), . Physiol., in press.BORN, G. V. R., and BRICKNEL, J. (i9s9), Ibid., in press.BOUNAMEAUX, Y. (1956), Rev. Franfaise, 2, 52.BOUNAMEAUX, Y. (19-7), Actes 2nd Symp. Found. Baldacci,Lisbon, p. 87.BOUNAMEAUX, Y. (1958), M6m. Acad. roy. Med. Belg., 3, Is.BRAUNSTEINER, H. (I955), Wien. Z. inn. Med., 36, 421.BRAUNSTEINER, H., FELLIGER, K., and PAKESCH, F.(I954), Blood, 9, 595.BRAUNSTEINER, H., and PAKESCH, F. (I956), Ibid., ii, 965.BRECHER, C., and CRONKITE, E. P. (I95o), . appl. Physiol.,3, 365.BUDTZ-OLSEN, 0. E. (Ig5i), 'Clot Retraction,' BlackwellScientific Publications, Oxford.CAMPBELL, E. W., SMALL, W. J., and DAMESHEK, W.(I956), Y. Lab. clin. Med., 47, 835.CENTINGIL, A. I., ULUTIN, 0. N., and KARACA, M. (xg58),Brit.J_. Haemat., 4, 350.CREVELD, S. (i954), Acta haemat. (Basel), 12, 229.CREVELD, S., and PAULLSEN, M. M. P. (I95x), Lancet, it, 242.
Protected by copyright.
on June 3, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.407.506 on 1 Septem
ber 1959. Dow
nloaded from

September I 959 SHIARP: The As.essment of Platelet Function 513
CREVELD, S., and PAULLSEN, M. M. P. (1952), Ibid., i, 23.CREVELD, S., LIEM KHE HO, and VEDER, H. A. (1958),
Acta haemat. (Basel), I9, I99.DAMESHEK, W., and MILLER, E. B. (1946), Blood, I, 27.DEUTCH, E., JOHNSON, S. A., and SEEGERS, W. H. (i955),
Circulation Res., 3, II0.DONNER, V. I., MACH, O., and BRANCAVA, S. (i958), Acta
haemat. (Basel), 20, 369.EBERTH, J. C., and SCHIMMELBUSCH, C. (i888), Virchows
Arch. path. Anat., 103, 39.FULTON, G. P., ACKERS, R. P., and LUTZ, B. R. (I953),
Blood, 8, 140.GUREVITCH, J., and NELKEN, D. (1956), Ibid., 10, 924.HARDISTY, R. M., and STACEY, R. S. (I955), J. Physiol.,
130, 7II.HARDISTY, R. M., and WOLFF, H. H. (I955), Brit. J. Haemat.,
I1 390.HARTERT, H. (igsx), Z. ges. exp. Med., 117, I89.HAVERBACH, B. J., DUTCHER, T. F., SHARE, P. A., TOMCH,
E. G., TERRY, L. L., and BRODIE, B. B. (I957), New Engl.Y. Med., 256, 343.
HAYEM, G. (1878), C. R. Acad. Sci. U.R.S.S., 86, 58.HAYEM, G. (I882), Ibid., 95, I8.HAYEM, G. (1883), Ibid., 97, 458.HJORT, P., RAPAPORT, S. I., and OWREN, P. A. (I955), Blood,
I0, 1139.HOWELL, W. H. (I9I0), Amer. J. Physiol., 26, 453.IMMERSLUND, 0. (I947), Acta paediat. (Uppsala), 34, 315.INTROZZI, P., and NICOLA, P. DE (I956), Sci. med. ital., 4 656.JACKSON, D. P., HARTMAN, R. C., CONLEY, C. 1. (1953),
Bull. Yohns Hopk. Hosp., 93, 370.JOHNSON, S. G., and SCHNEIDER, C. L. (1953), Science,
117, 229.KOPPEL, U. (I958), Z. Zellforsch., 47, 401.LEEKSMA, C. H. W., and COHEN, J. A. (1956), J. clin. Invest.,
35, 964.LEWIS, J. H., FERGUSON, J. H., SPAUGH, E., FRESH,
J. W., and ZUCKER, M. B. (I957), Blood, 12, 84.LEWIS, J. H., ZUCKER, M. B., and FERGuSON, J. H. (1956),
Ibid., II, 1073.MAcDONALD, L., and EDGILL, M. (I957), Lancet, Ri, 457.MACFARLANE, R. G. (I94I), Quart. J. Med., 34, I.MARX, R., STITCH, W., and EHRHART, H. (I956), Proc. VIth
Int. Cong. Haemat., p. 560.MERSKEY, C. (I950), J. clin. Path., 3, 130.MOOLTEN, S. E., VROMAN, L., and VROMAN, G. M. S.
(I949), Amer. . clin. Path., I9, 814.MORAWITZ, P. (I905), Ergebn. Physiol., 4, 307.MORITA, H. (1958), 'Blood Platelets in Chemical Medicine,'
Tokyo.
MUSTARD, J. F. (I956), Brit. J. Haemat., 2, 17.NICOLA, P. DE (I954), Rev. Hemat., 9, 536.NILSSON, I. M., BLOMBACK, M., JORPES, E., BLOMBACTI.,
B., and JOHANSSON, S. A. (I9S7), Acta med. scand., 159, 179.NOLF, P. (I908), Arch. int. Physiol., 6, I.O'BRIEN, J. R. (i955), Brit. J. Haemat., 1, 223.QUICK, A. J., SHANEBERGE, J. N., and STEFANINI, M.
(I949), Amer. 7. med. Sci., 217, I98.QUIRY, D., CAEN, J., and BERNARD, J. (I958), Rev. Fran;aise,
3, 477.RATNOFF, 0. D., and COLOPY, J. E. (I95s), 7. clin. Invest.,
34, 602.ROSENTHAL, R. L., DRESKIN, 0. H., and ROSENTHAL, N.
(i95s), Blood, 1o, I20.ROSS, S. W., and EBERT, R. V. (x959), J. clin. Invest., 38, I55.SELIGMAN, M. (I957), C. R. Acad. Sci. U.R.S.S., 224, 2192.SEREF-INCEMAN (I955), Sang, 26, I90.SEREF-INCEMAN (x956), Forum Med., 2, 105.SHARP, A. A. (1957a), 'Actes 2nd Symposium Foundation
Baldacci,' Lisbon, p. 72.SHARP, A. A. (1957b), 'Physiological and Antigenic Properties
of Blood Platelets,' p. 76, thesis for degree of M.D., Universityof Edinburgh.
SHARP, A. A. (I958), Brit. 7. Haemat., 4, a8.SOULIER, J. P., and LARRIEU, M. J. (19S4), Rev. Hemat., 9,77.SOULIER, J. P., LARRIEU, M. J., and WARTELLE, 0. (I955),
Acta haemat. (Basel), 14, I6o.SPRAGUE, C. C., HARRINGTON, W. J., LANGE, R. D., and
SHAviLEIGH, J. B. (1952),3. Amer. med. Ass., I50, II93.STEFANINI, M., and MURPHY, I. S. (I956), 7. clin. Invest.,
35, 355-TAIT, J., and BURKE, H. E. (1926), Quart. .7. exp. Physiol.,
x6, 141.ULUTIN, 0. N. (I958), Lancet, ii, S91.ULUTIN, 0. N., and KARACA, M. (I956), Forum Med., 4,257.WEIL-MALHERBE, H., and BONE, A. D. (1954), Nature, Lond.,
174, 557-WEINER, M., ZELTMACHER, K., REICH, C., and SHAPIRO,
S. (1948), Blood, 3, 1275.WRIGHT, H. P. (I94I), . Path. Bact., 53, 255.ZUCKER, M. B. (I947), Amer. Y. Physiol., 148, 275.ZUCKER, H. D. (I949), Blood, 4,631.ZUCKER, M. B., FRIEDMAN, B. K., and RAPPORT, M. M.
(I954), Proc. Soc. e4s. Biol., N.Y., 85, 282.ZUCKER, M. B., and BORRELLI, J. (i9ss), Y. appl. Physiol.,
7, 425.ZUCKER, M. B., and BORRELLI, J. (I956), Amer. . clin. Path.,
26, 13.ZUCKER, M. B., and BORRELLI, J. (I9S9), Y. clin. Invest., 138,
148.
Bibliographv from page 5o; -7. W. Stewirt, M.B., B.S., aid P. 7. Crosland-Taylor, M.B., B.Chir.BIBLIOGRAPHY
ALFEROW, S. (1884), Arch. Physiol. Norm. Path., 3, 269.BERKSON, J., MAGATH, T. B., and HURN, M. (1940), Amer.
3'. Physiol., 128, 309.BIGGS, R., and MACMILLAN, R. L. (1948),J7. clin. Path., x,
269, 288.BRACHETT, R 3., MATTERS, C. F., and OLSON, B. F. (I953),
Amer. .7. clin. Path., 23, 73I.BRECHER, G., SCHNEIDERMAN, M., and WILLIAMS, G. Z.
(1956), Amer. J3. clin. Path., 26, 1439.BURKER, K. (ii9i), Arch. ges. Physiol. (Pflugers Archives), I42,
337.COOK, H. F. (I952), Brit. Y. applied Phys., 3, 249.COOKE YARBOROUGH, E. H., and WHYARD, R. E. (1954),
Brit. J. applied Phys., 5, Suppl. 3, S. 147.CRAMER, A. (I855), quoted from Plum. Nederlandisch Lancet,
3rd Ser., 4, 453.CROSLAND-TAYLOR, P. J. (1953), Nature (Lond.), 171, 37.CROSLAND-TAYLOR, P. J., STEWART, J. W., and HAGGIS,
G. (I958), Blood, 13, 398.DANNINGEN, K., and GRANT, E. H. (I958), Atom Praxis, 4
(Io), Oct. x958.GOWERS, W. R. (I877), Lancet, ii, 797.HAYEM, G., and NACHET, A. (i875), C.R. Acad. Sdi., Paris,
8o, I o83.
HIRSCH, F. G., and TEXTER, E. C. (I950), Blood, 5, 1017, 1036.LAGERCRANTZ, C. (I952), Acta physiol. scand., 26, Sup. 93.MACFARLANE, R. J., PAYNE, A. M. M., POOLE, J. C. F.,
TOMvLINSON, A. H., and WOOLF, H. S. (i959), Brit. J.Haemat., 5, i.
MATTERN, C. F., BRACHETT, F. S., and OLSON, B. J. (I957),Y. applied Physiol., 10, 56.
MOLDAVAN, A. (I934), Science, 8o, I88.OLIVER, G. (I896), Y. Physiol., I9, Proc. Physiol. Soc. XVI.PLUM, P. (1936), Acta med. scand., 90, 342.PONDER, E. (I935), Amer. J3. Physiol., IiI, 99.ROBERTS, F., and YOUNG, J. S. Z. (I952), The Proc. Instn.
elect. Engrs., 99, Pt. IIIA, No. 20.STEWART, G. N. (I897), J. Boston Soc. M. Sc. No. x6, x8, quoted
by Stewart.STEWART, G. N. (I899), J. Physiol., 24, 356.STUDENT (1907), Biometrika, 5, 351.VIERODT, K. (I852), Arch. Physiol. Heilk., II, 26, 327, 854.WAGNER, R. (I838), 'Nachtrage fur vergleichenden Physiologie
des Blutes', Leipzig.WELCHER, H. (I854), Vjachr. Prakt. Heilk. (Prague), 44, xI.WHITLOCK, J. H. (I947), Blood, 2, 463.WILSON, T. M. (I905), Amer. J7. Physiol., 13, 139.
Protected by copyright.
on June 3, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.407.506 on 1 Septem
ber 1959. Dow
nloaded from