Embed Size (px)
Citation preview

THE ‘ANAEROBIC ’ THRESHOLD: PHYSIOLOGY AND IDENTIFICATION
Susan A. Ward DPhil
Human Bio-Energetics Research Centre
Crickhowell, Powys, United Kingdom

The term “Anaerobic Threshold”
seems to polarize investigators into
those who believe it to be a milestone
in advancing the understanding of
exercise bioenergetics ....
and those who believe it to be a millstone.
bfe
Whipp BJ. Unpublished Susan A. Ward
Anaesthesia, 2011, 66, pages 111–123 doi:10.1111/j.1365-2044.2010.06604.x....................................................................................................................................................................................................................
REVIEW ARTICLE
Controversies in the physiological basis of the ‘anaerobicthreshold’ and their implications for clinicalcardiopulmonary exercise testing
J. G. Hopker,1 S. A. Jobson2 and J. J. Pandit3
1 Lecturer, 2 Research Fellow, Centre for Sports Studies, University of Kent, Chatham Maritime, Chatham, Kent, UK3 Consultant Anaesthetist, Nuffield Department of Anaesthetics, Senior Lecturer, Nuffield Department of ClinicalNeurosciences and Fellow of St John’s College, Oxford, UK
B. J. Whipp and S. A. Ward
Human Bio-Energetics Research Centre, Crickhowell, Powys, U.K.
The physiological basis of the 'anaerobic threshold' and implications for clinical cardiopulmonary exercise testing
LETTER TO THE EDITOR
Anaesthesia 2011 66 pages 1048-1049 http://www.respond2articles.com/ANA/forums/thread/876.aspx
bfe

“ANAEROBIC”:
a) Yes (O2 not used in the lactate formation)
b) No (PCr decreases at all work rates)
c) Maybe (Are there regions in the contracting
muscles where the PO2 is “critical”? -
no definitive resolution at present)
THE “ANAEROBIC” THRESHOLD
(lactate; lactic acidosis; ventilatory; gas exchange; …)
bfe
Whipp BJ. Unpublished Susan A. Ward
bfe
Whipp BJ. Unpublished Susan A. Ward
The “Lactate Threshold” (estimated from pulmonary gas
exchange indices) is currently used for:
Assessing the normalcy, or otherwise, of an individual’s
integrative systemic function;
Optimising race pace strategy in athletes;
Optimising the intensity of training and rehabilitative
work rates;
Judging an individual’s appropriateness to undergo major
thoracic or abdominal surgery;
Triaging a patient post-operatively to “the ward” or to an
intensive care facility; and
As an index of life expectancy in patients with heart
disease.

Contributors to buffering
But do not yield CO 2
pH = pK 1 + log [HCO 3-] = pK 2 + log [NaPO 4
-] = pK 3 + log [Pr -] = pK 4 + log [org]
[H2CO3] [H2PO4-] [HPr] [ H org]
bfe
Modified from Handbook for Fellows . Div. Resp. Med., Harbor General Hospital. 1967
THE METABOLIC ACIDOSIS OF EXERCISE
* * **
∝
* *
bfe
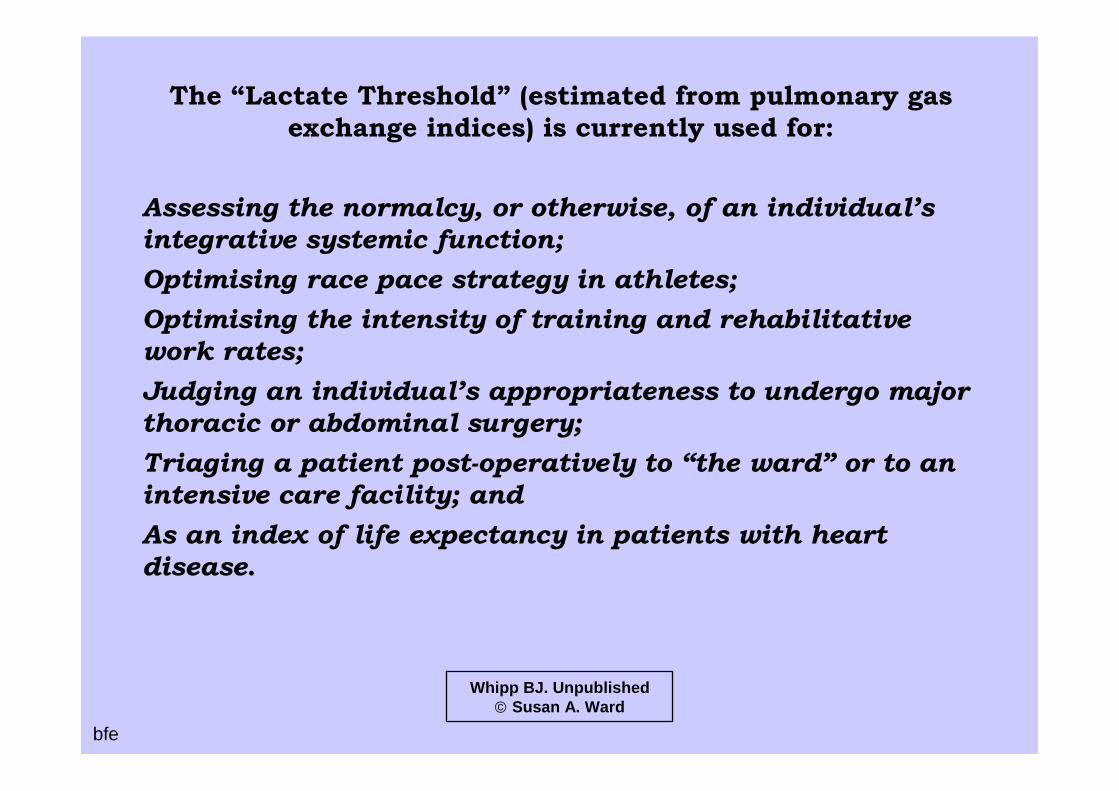
LACTATE THRESHOLD ESTIMATION
Whipp BJ. Unpublished Susan A. Ward
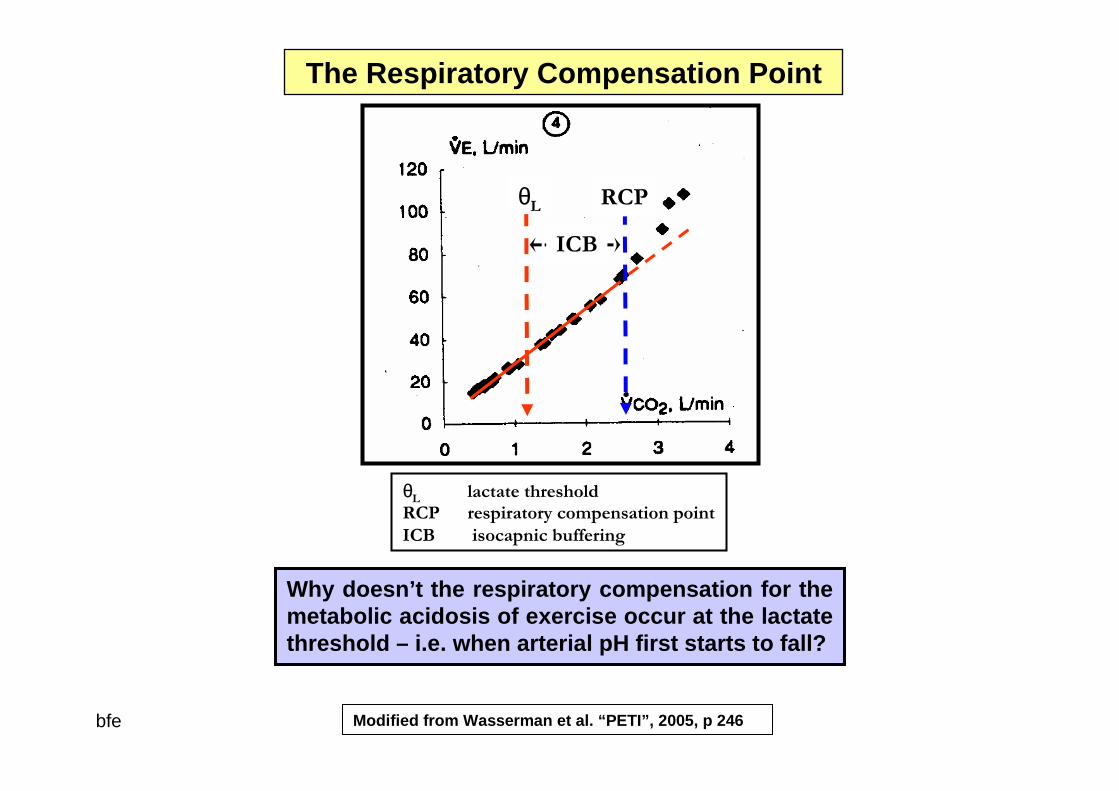
θL
bfe
θL lactate threshold
RCP respiratory compensation point
ICB isocapnic buffering
Why doesn’t the respiratory compensation for the metabolic acidosis of exercise occur at the lactate threshold – i.e. when arterial pH first starts to fa ll?
The Respiratory Compensation Point
ICB
RCP
Modified from Wasserman et al. “PETI”, 2005, p 246
bfe
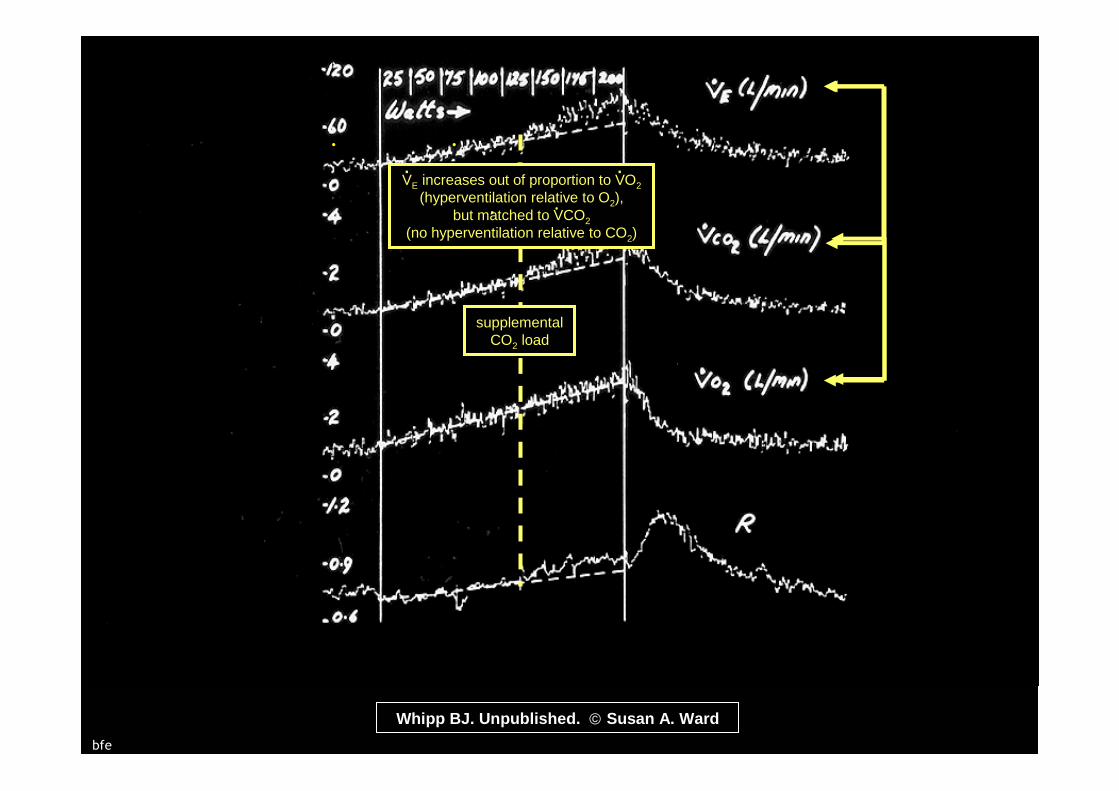
supplementalCO2 load
.
.
.
Whipp BJ. Unpublished. Susan A. Ward
VE increases out of proportion to VO2
(hyperventilation relative to O2),but matched to VCO2
(no hyperventilation relative to CO2)
. .
. .

1: supplementalCO2 load
2: hyperventilationrelative to O 2
Henson et al. Eur J Appl Physiol 59:21-28, 1989.bfe
Region of Interest

Sources of “Excess” CO2 Output
during Ramp Exercise
1) Accelerated aerobic substrate catabolism
2) Pulmonary hyperventilation, with a fall in alveolar (end-tidal) and arterial PCO2?
3) Bicarbonate buffering:
(NaHCO3 in blood and KHCO3 in muscle)
bfe
Whipp BJ. Unpublished Susan A. Ward
TONACDONOHOTONACDONOHO
ThresholdOf
NonAerobic
CarbonDioxide
OutputNot
OfHyperventilatory
Origin
bfe
Whipp BJ. Unpublished Susan A. Ward

θ̂L
1: supplementalCO2 load
2: hyperventilationrelative to O 2but not CO2
bfe Whipp BJ & Ward SA. Unpublished

bfe
Sue et al. Chest 94:931-938, 1988
S=1
θLˆ
Whipp BJ. Unpublished Susan A. Ward
Some Some ““Be Be CarefulsCarefuls””!!
bfe
Whipp BJ. Unpublished Susan A. Ward

bfe
Whipp BJ. Unpublished Susan A. Ward
V-slope graph scaling

Work Rate (Watts)
VO2
(ml/min)VCO2
(ml/min)R ΔVCO2/
ΔVO2
“0” 500 400 0.8
50 1000 950 0.95
Δ = 50 Δ = 500 Δ = 550 S1 = 1.1
VCO2 - VO2 Relationship: S1 > 1.0?. .
. . .
.
bfe
Whipp BJ. Unpublished Susan A. Ward
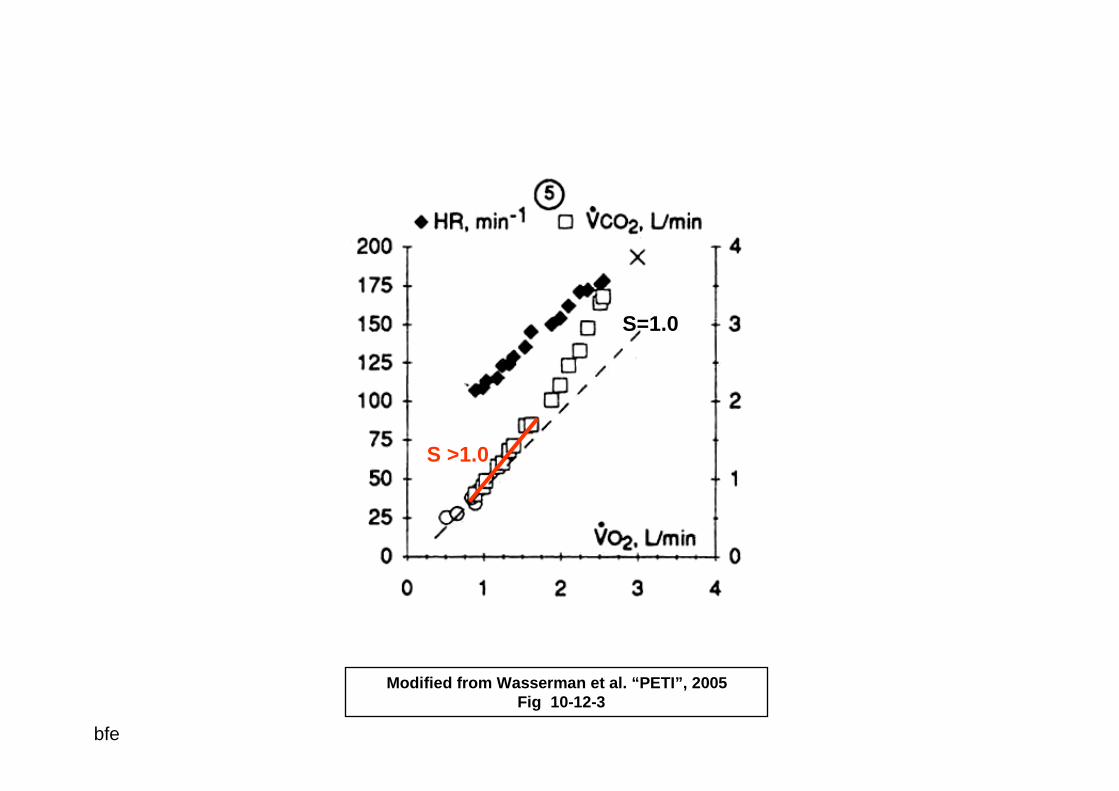
S=1.0
S >1.0
Modified from Wasserman et al. “PETI”, 2005Fig 10-12-3
bfe
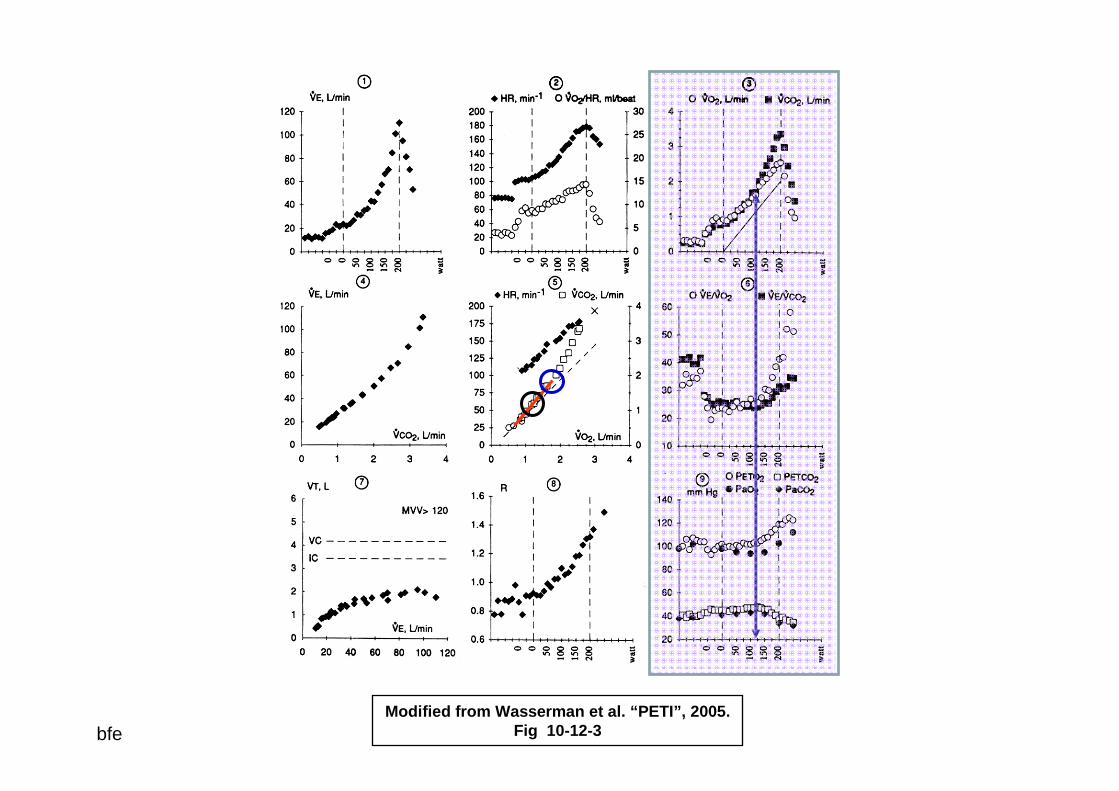
Modified from Wasserman et al. “PETI”, 2005. Fig 10-12-3 bfe
But:
VCO2 can begin to increase faster than VO2 :
not just because it begins to be “produced” faster,
but also because its rate of “storage” begins to
slow or stop!!
2OV&
2COV&
. .
bfe
Whipp BJ. Unpublished Susan A. Ward
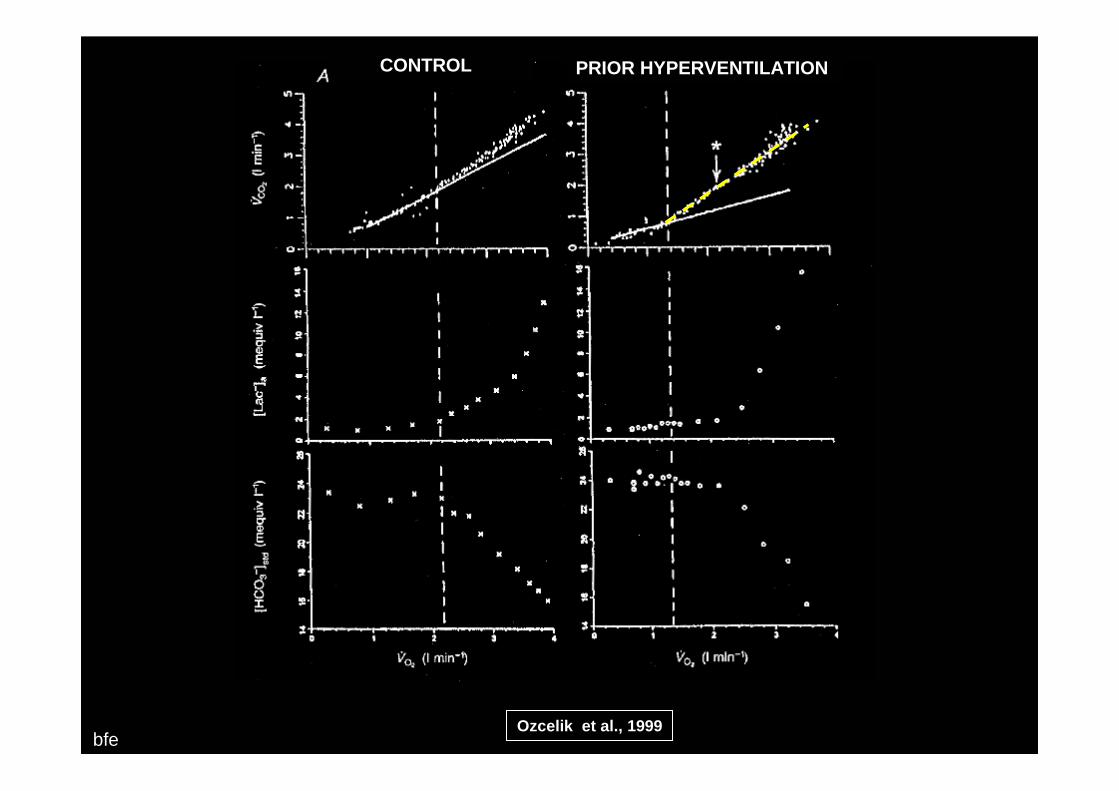
bfeOzcelik et al., 1999
CONTROL PRIOR HYPERVENTILATION

THRESHOLD DISCRIMINATION:
What to do – and why!
What not to do – and why!
bfe
Whipp BJ. Unpublished Susan A. Ward

Brian J. Whipp PhD, DSc.
The Anaerobic Threshold:
Physiology and Identification The Science and the Art
bfe
Whipp BJ. Unpublished Susan A. Ward