Embed Size (px)
Citation preview
The Aging Prostate: Presentation, Diagnosis &
Management
Professor Riyadh F. Talic, MDProfessor of Urology & Andrology
College of Medicine, King Khalid University Hospital
And Consultant Urologist & Andrologist at Specialized Medical Center, SMC
Etiology of BPH
• Increasing Age
• Testosterone
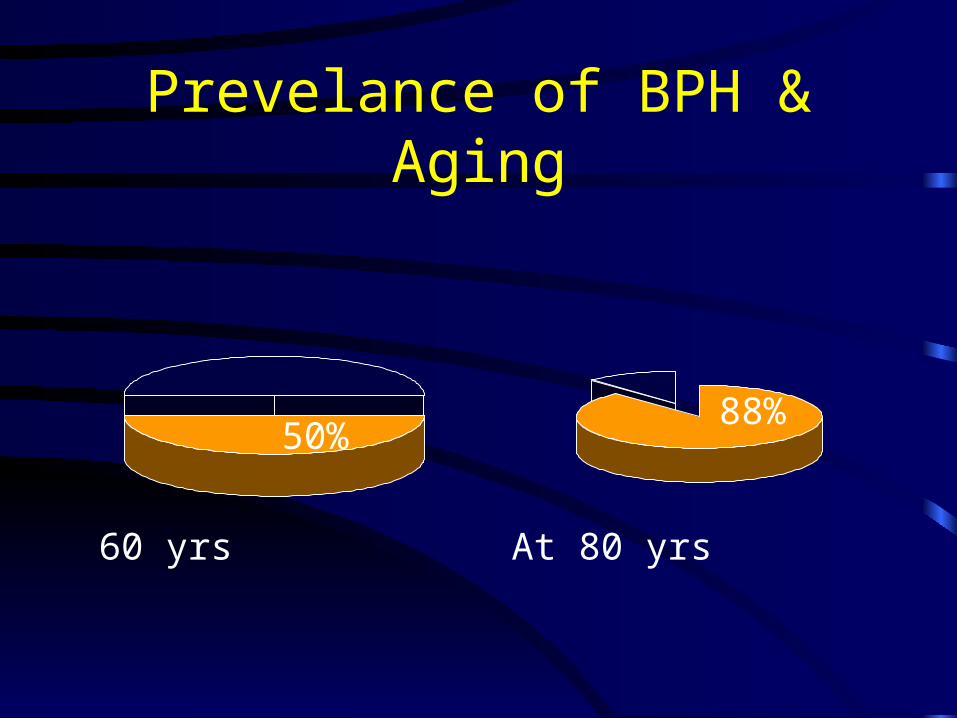
Prevelance of BPH & Aging
60 yrs
50%
At 80 yrs
88%

Aging Prostate Terminology
• Benign Prostatic Hypertrophy (BPH)
• Benign Prostatic Obstruction (BPO)
• Lower Urinary tract symptoms (LUTS)
Benign Prostatic Hypertrophy
LUTS
BPH
Bladder dysfunction
Urinary Obstruction
Prostatic LUTS• Storage LUTS
(i.e. irritative LUTS) :– Frequency
– Nocturia
– Urgency
– Urge incontinence
• Voiding LUTS (i.e. obstructive LUTS):
– Hesitancy
– Weak stream
– Intermittency
– Sense of incomplete emptying
Causes for Storage LUTS (Irritative LUTS)
• Urinary Outflow Obstruction
• Locally irritating pathology
• Neuro-vesical dysfunction
Cystitis
Tumors
Stones
Adverse effects of BPH
• Erodes Quality of Life
• Complications:– Urinary retention
– Recurrent hematuria
– Bladder stones
– Compromised renal function

BPH effects on Quality of Life
• Limits fluids before travel 58%• Limits fluids before bed time 63%• Cannot drive for more than 2 hours 51%• Not getting enough sleep at night 51%• Avoids places without toilets 62%• Limits playing outdoor sports 33%
Tsang et al: Prostate 1993

Evaluation of patients with BPH
• Digital rectal examination (size not relevant)
• Urinalysis (pyuria, microhematuria)
• Urine Cytology (in patients & irritative LUTS)
• Prostate Specific Antigen (PSA)
• Urine Flowmetry
• U/S KUB & post void residue estimation
Management Options for patients with BPH
• Medical therapy• Instrumental (minimally invasive)
therapy
• Surgical therapy

Medical Therapies for BPH is the first line of
management of patients with symptomatic BPH
Medical Therapies for BPH
• 5 α reductase inhibitors: – Finasteride (Proscar).
• Alpha- blockers:– Trazosin (Itrin).– Doxazosin (Cardura).– Alfuzosin (Xatral).– Tamsulosin (Flomax, Omnic).

Finasteride (Proscar).• 5 α reductase inhibitors offer medical
prostatectomy.• Need 6/52 for patients to realize benefits.• Valuable in large prostate > 50 gms.• Adverse effects:
– Erectile dysfunction.– Retrograde ejaculation.– Teratogenic effects on Fetus ?– Alters PSA levels.
Alpha- blockers• Alpha- blockers act on α-receptors in
the BN & Prostatic capsule.• Rapid onset of action (within 2/52).
• Enhances sexual function ??• Adverse effects:
– Postural Hypotension.– Retrograde ejaculation.
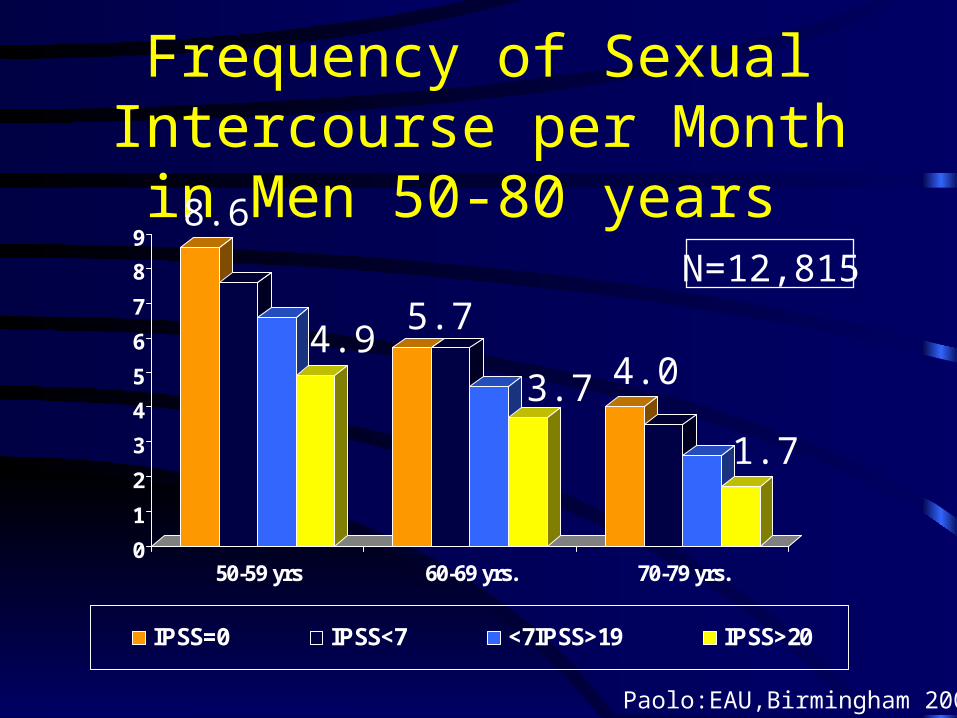
Frequency of Sexual Intercourse per Month in Men 50-80 years
0
1
2
3
4
5
6
7
8
9
50-59 yrs 60-69 yrs. 70-79 yrs.
IPSS=0 IPSS<7 <7IPSS>19 IPSS>20
8.6
4.95.7
3.7 4.0
1.7
N=12,815
Paolo:EAU,Birmingham 2002
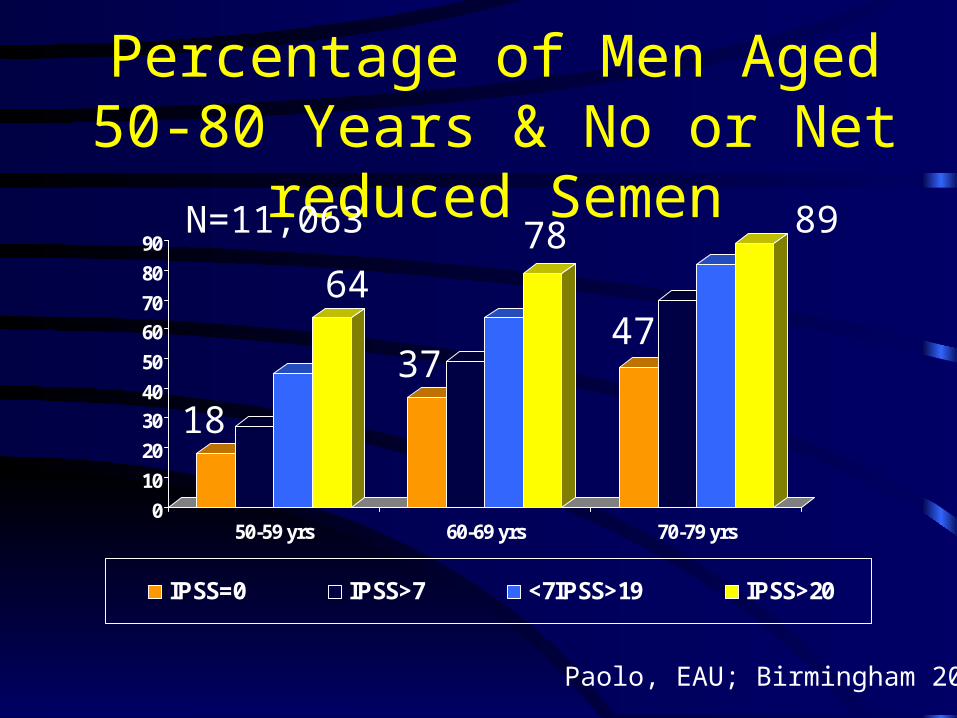
Percentage of Men Aged 50-80 Years & No or Net reduced Semen
0
10
20
30
40
50
60
70
80
90
50-59 yrs 60-69 yrs 70-79 yrs
IPSS=0 IPSS>7 <7IPSS>19 IPSS>20
6478 89
18
3747
N=11,063
Paolo, EAU; Birmingham 2002

Effect of Alfuzosin on the number of erections induced by Apomorphine
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Apomorphine Apomorhine + Alfuzosin
Num
ber of E
rections
McKenna: EAU, Birmingham, 2002
Which Alpha- blocker ?
• Efficacy (Uro-selectivity ?)
• Dosing– Single dose / Day
– No need for titration
• Minimal side effects– Postural hypotension
– No retrograde ejaculation
• Cost of the treatment
Minimally Invasive Therapies for BPO
• TUIP (Incision)
• Prostate balloon dilatation
• Urethral (prostatic) stents
• Hyperthermia
• Cryosurgery
• TUNA
• Laser devices
Surgical Therapy for BPO• Based on removal & debulking of
the obstructing prostatic adenoma, indicated in:– Failed medical treatment– Complications:
• Urinary retention.• Renal back pressure changes.• Hematuria.• Large vesical stones.
Surgical Therapy of BPO
• Open prostatectomy
• Transurethral prostatectomy– TURP (Resection)– TUVP (Vaporization)
– TUVRP (Vaporization-Resection)

Transurethral resection of the Prostate (TURP) using a standard wire loop and electrosurgical unit is still
regarded as the “Gold Standard” in the treatment
of men with BPO
Morbidity associated with TURP • Bleeding• TUR syndrome (Low serum sodium)
• Infection
• Urinary incontinence• Erectile dysfunction.
Transurethral Vaporization Resection Prostatectomy (TUVRP)
• Thick Loop (Resection)• Augmented Electocutting energy (Electrovaporization)• TUVRP = TURP + TUVP• Technique of operation!

TUVRP• TUVRP improves safety of
transurethral prostatectomy and has the potential to reduce the
main 2 morbidities that are associated with standard TURP namely; bleeding and electrolyte
disturbances.

TUVRP• The shorter post operative
catheterization time that is noted following TUVRP is clinically
significant considering the demand for lower morbidity profiles and
hospitalization time by the patients and health care providers
Conclusions
Symptomatic BPH affects men over 40 years of age and
erodes their quality of life

Conclusions
• Pre treatment evaluation of patients is necessary to rule out other
pathology that needs a different therapeutic approach
Conclusions• Alpha- blockers should be the first
line of treatment in every patient that is presenting with BPH with the aim of restoring quality of life
and Sexual function
Conclusions
• The Alpha-blocker of choice should be efficacious, once
daily dose (with no titration), No sexual adverse effects and
cost effective
Conclusions
• Patients that fail medical treatment or develop complications related to
BPH should be referred to the Urologist for further work-up and
interventional managment







![g y : Open ond e l Andrology Andrology-Open Access · morphogenesis of the urogenital organs, which takes place primarily in the postnatal period after birth [1,2]. The potential](https://img.pdfslide.us/doc/110x75/603f2626fdc77331c164f118/g-y-open-ond-e-l-andrology-andrology-open-access-morphogenesis-of-the-urogenital.jpg)






















