Embed Size (px)
Citation preview

The Annals of Human Genetics has an archive of material originally published in print format
by the Annals of Eugenics (1925-1954). This material is available in specialised libraries and
archives. We believe there is a clear academic interest in making this historical material more
widely available to a scholarly audience online.
These articles have been made available online, by the Annals of Human Genetics, UCL and
Blackwell Publishing Ltd strictly for historical and academic reasons. The work of
eugenicists was often pervaded by prejudice against racial, ethnic and disabled groups.
Publication of this material online is for scholarly research purposes is not an endorsement or
promotion of the views expressed in any of these articles or eugenics in general. All articles
are published in full, except where necessary to protect individual privacy.
We welcome your comments about this archive and its online publication.

NO. Mean
23.23 f.26 25.16 rt.84 21.30 f.67 20.60 1.76
European 6 (669) ? (113)
Japanese 3 (74) ? (48)
Standard Deviation
9.98 1.18 13.27 1.60 8-53 1-47 7.82 **54

270 AGE O F ONSET I N HEREDITARY OPTIC ATROPHY Now these values suggest that whatever factors operate to determine the age of onset in the
males of the Japanese race, they operate at the same age for Japanese females, and in both cases at an age earlier than for European races; the numbers for the Japanese are small, but so far as they carry any weight they do perhaps fall into line with the view that eastern races develop earlier than western, and it would appear to be legitimate to combine the statistics from the two sexes as homogeneous material. When, however, we regard the different values for males and females of European races, something further requires explanation in the increased variability of the female. The frequency distributions corresponding to the four series are as follows:
Age of Onset
0-3 4-7 8-1 1
12-15 16-19
24-27 28-31 32-35 36-39 40-43 4 4 4 7 48-51 52-55 56-59 1 60-63
20-23
64-67
Europeans Japanese
8 P I d 9 15 6 19 3 26 12 50 16
119 5 194 10 94 15 70 10 28 10 10 8 13 10 7 3
14 4 3 5 1 1 1
- - -
I - - - I ; 2
20 14 11 10
3 1 8
4 I f 6 1 1 1 1
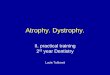
- I - The graph* given on p. 271, based on these values, illustrating the frequency percentage of cases
in which the onset occurred within each age group for males and females of the two series, suggests that the factors determining the onset differ markedly in the male and female of European races and supports the view that the combined male and female data for the Japanese race provide homogeneous material.
We know that a temporary condition closely resembling hereditary optic atrophy in its symptoms may be induced as a result of toxic influences, and there is some evidence in support of the view that a toxic influence, or indeed any disturbance of normal health, has power to precipitate the onset in the presence of the tendency to the hereditary form of the disease; it is therefore possible that the first peak shown by the female curve for Europeans is contributed to by the physiological disturbances associated with menstruation, the second peak between the ages of 20 and 43 years being influenced by the toxic effects of pregnancy. On this hypothesis we need to ask why the Japanese female curve shows no similar distribution but on the contrary follows very closely to the male curve for the race.
To call attention to one other fact shown by this graph-the climacteric appears to have no significance with regard to the onset of the disease, and yet the contrary is very commonly stated. Perhaps if a woman is liable to the disease at all she is bound to suffer from periods of lowered resistance or low vitality which would give the tendency an opportunity to manifest itself before the time of the menopause, but whatever the explanation may be I think that we may insist that the onset of hereditary optic atrophy must no$ be added to the list of ills liable to befall woman at this period of her life.
* The graph is given in this form instead of as a histogram in order to show the differences between the four series in one diagram.

J U L I A BELL 27 1
A more complete discussion of these curves will be given in the forthcoming memoir, the only reason for including them here being to justify my action in combining data given by males and females of the Japanese material and keeping the values for European males and females separate from each other and from those of the Japanese in any attempt to measure the intensity of inheritance for one factor of the disease.
HEREDTTARY OPTTC ATROPHY- AGE OF ONSET OF THE DISEASE.
0
Males of European Populafion N = 669 - - - Females 1 ) N = i t3
Mates o f Japanese ~7 N = 14 . . . . . . . . . . . . . Females 19 17 N = 48
11
- ----
The information concerning Japanese cases is taken from a paper by Kawakami*, who published an extensive pedigree himself and further collected a number of family histories of the disease published by other Japanese authors. The paper is of great interest and Kawakami himself calls attention to the differences he observed in the distribution of the age of onset of the disease for the two races, but no detailed description of the cases is given, and in the absence of this it is not
* Kawakami, R. : ‘‘ Beitrage zur Vererbung der familiaren Sehnervenatrophie,” Archiv f. Ophthalmologie, Bd. CXVI, S. 568-95. Berlin, 1926.

272 AGE O F ONSET I N H E R E D I T A R Y OPTIC ATROPHY possible to throw any light on the source of the differences. It is a great misfortune that so little of the Japanese literature concerned with hereditary eye disease is accessible to western readers. It is not easy to see why a disease which is relatively sex-limited in one group of peoples should have such a vastly differing sex-incidence in another, and much additional material with far more detailed histories of Japanese cases will be necessary before the factors operating to produce this state of things can be made clear; in the meantime the two series must be considered separately.
On the Influence of the Disease in the Mother upon the Age of Onset in the Offspring. It is only possible to point to tendencies with regard to this influence, for the relative rarity of the affection in the European female and thus in the mother, and the scantiness of the Japanese material, render any exact measurement impracticable. Thus we have records of only 63 affected males of the European series whose age of onset is given who are known to have had an affected mother, whereas 565 such males were known to have had an unaffected mother; in the former group the onset occurred before the age of 16 years in 23 or in 36.5 % of cases; in the latter group with unaffected mothers the onset occurred before the age of 16 years in only 15.0 % of cases. Manifest disease in the mother, then, appears to hasten the onset of the condition in her sons; the source of this relationship is obscure and I can only state the observed facts but can offer no explanation. I hesitate to give corresponding percentages for the affected females as the numbers are so small, but with the warning that too much significance should not be attached to them, the values are as follow. Of 31 affected females of the European series who had affected mothers, the onset of the disease occurred before the age of 16 in 13 or in 42.0 yo of cases; of 70 females whose mothers were unaffected 32.9 % showed the disease before the age of 16 years. Thus the condition of the mother would appear to have less effect on the hastening of the onset in her daughters than in her sons; but evidently the two cases are not parallel for a far higher percentage of affected females have an affected mother than is the case with affected males. This is a fact of some im- portance to be borne in mind when we consider what are the conditions predisposing to the affection in the female. The Japanese series provides too small numbers to enable any estimation to be made of the influence of affected parentage on the age of onset, but so far as one can judge the figures tend to lead to conclusions similar to those drawn from the European series; in this series also affected females have an affected mother in a markedly higher percentage of cases than have the affected males.
On the Age of Onset as a Factor in the Consideration of the Prognosis of the Disease. The histories of my collection do not in many cases give any history from which one can judge whether improve- ment has occurred or not, and in almost all cases the information is vague and indefinite; in practice however no ophthalmologist feels particularly hopeful regarding the outlook for the patient who comes to him suffering from hereditary optic atrophy. My records include 211 cases in males which appear to have shown no improvement over a period of years, and 86 cases in which improvement however has been noted, that is to say 29.0 yo of these males showed some measure of improvement, 12 of the 86 improved cases showed complete recovery, 15 showed marked improvement and 59 improved to some less extent. The common story for the patient who does not mend is that of a rapid onset with progression of symptoms during a short and limited period when the maximum disability is reached, and the condition henceforth remains stationary. The percentage of 29.0 almost certainly indicates too high a rate of improve- ment from the fact that there is probably a tendency to note improvement when it occurs and to make no comment when the condition is found to be unchanged; it however constitutes a maximum value and it may be set against a minimum value of 10 yo based on the supposition

J U L I A BELL 273
that only 86 of my whole series of 837 males showed improvement; the true value undoubtedly lies somewhere between these two and perhaps nearer to the upper limit than to the lower.
On examining the statistics giving the age at which onset had occurred in the improved and not improved classes of males it is found that in 75 males in whom improvement is noted the age of onset had been earlier than 16 years in 26.7 yo of cases, whereas in the 200 cases which showed no improvement the age of onset had been earlier than 16 years in only 9.5 yo of cases; thus an early onset would appear to denote a relatively favourable outlook. The figures regarding improve- ment in females are too small to be of any value, but such as they are we find 15 cases improved or recovered and 37 cases in which no improvement occurred, but, by an interesting coincidence, the maximum and minimum recovery or improvement rates work out at 29 yo and 10 yo re- spectively, that is to the same values practically as those given above for males.
The Inheritance of Age of Onset in Hereditary Optic Atrophy. This disease is evidently to a very prominent degree transmitted through the female; it would appear from many pedigrees to be entirely confined to the female line, the transmitting agent herself being commonly unaffected. Hence, the father very rarely transmitting the disease and the mother in a large proportion of cases carrying the disease in a latent form only, it is not possible to form tables giving the age of onset in parent and offspring. It is possible however to obtain a measure of the hereditary intensity of the factor under consideration by correlating the values known for pairs of brothers of the European series and for pairs of siblings of Japanese pedigrees in which male and female data may be regarded as statistically homogeneous. My histories also enable me to measure the resemblance between the ages at which uncles and nephews and pairs of male first cousins of affected stocks tend to become affected, and thus provide correlation coefficients which may be compared with those known to hold for other hereditary conditions.
The following table includes the values obtained, demonstrating that a single feature of a
Mean Age of Onset
Pairs of Siblings (Japanese) 19.64 f .33 Pairs of Brothers (European) 22.41 5-23
24.71 5.27 18.50 f.51 gg:p and} (European) 22-87 h.67 25-95 f.31 g;leFd] (European) 22.95 k.28
-~
Pairs of Male First Cousins (European)
Age of Onset in
Standard Deviation
6-72 f .23 9.64 f.16 7.97 f.19 9.27 f.36
12-33 f.48 9-06 f-22 8.17 f.20
Pairs of Siblings (Japanese) Pairs of Brothers (European) Brother and Sister (European) Nephew and Maternal Uncle (European) Pairs of Male First Cousins (European)
I No. I
Correlation Coefficient
+.5073 j1.0356 +.5104 k.0175 f.6233 f.0335 +.2090 f.0325 +.1159 f.0337
Striking features of these results are (a) the rather unexpectedly high value of the correlation between brother and sister; ( b ) the relatively low mean age of onset in the case of brothers who
35 EUGENICS 111, I11 & IV
274 AGE O F ONSET I N HEREDITARY OPTIC ATROPHY have affected sisters’(the mean for all males 6eing 23.23 years) ; (c) the difference in the mean age of onset in the case of uncle and nephew.
Now, with regard to (a) and ( b ) it is possible that the two facts referred to have a common explanation in some enforcement of the factor determining the manifestation of the disease in the female and thus in the males of the same sibship; any intensified liability to the disease in siblings would presumably raise the correlation of its characteristic features between them, and would almost surely tend to hasten the age of onset in the male relatively to that of the male without this enforcement. I have endeavoured to obtain some further confirmation of these suggestions from other correlation coefficients, between pairs of sisters and between male and female first cousins, and though the numbers are so small that we cannot insist upon the signi- ficance of the values obtained, they are in accord with the suggestions offered, although they must await full confirmation when adequate material has accumulated*.
The hastening of the age of onset in the nephew relatively to that of the uncle may be too readily put forward as an example of ante-dating in the next generation, but this is by no means justified from a consideration of the facts. We need to remember that the nephew and his generation tend to be the patients who are under observation when the case is reported, and members of this generation have frequently not yet reached the age at which a late onset may occur; moreover exact knowledge of the age of onset in members of the previous generation who became affected early in life is liable to be forgotten; both these facts would tend to lead to such difference as is shown by my statistics, which thus may well be accounted for by a selection in the collection of the material and may have no inherent significance. True ante-dating can only be demonstrated on completed pedigrees t.
With regard to the Japanese material, the value of the correlation of -51 between the ages of onset of the disease for siblings regardless of sex would appear to indicate that for this race the liability to disease in females may become manifest without the re-enforcement necessary in the case of European females; this possibility is supported also by the marked difference in the sex incidence for the eastern and western races.
It had been my impression, formed during the collection of many histories of hereditary disease, that the predominant features of the disease tended to be stationary within the same stock, and that, for example, all affected members of the same stock would tend to present symptoms at the same period of life; just as from pedigrees of retinitis pigmentosa it has been shown that if one member of a stock affected by this disease be deaf, all other affected members of the stock also become deaf, to give one illustration only. But such is evidently not universally the case, and we now see that a single clinical feature of a disease may be inherited, not in its entirety, but with the same intensity which has been shown to hold for a great variety of characters, physical and mental in man, i.e. we see that regression holds.
Let us then remember never to allow ourselves to be influenced by impressions until the phenomena have been subjected to measurement.
* The provisional values obtained for the correlation coefficient are as follows: Pairs of sisters, N = 58, r = -7208 5 a0425; male first cousin and female first cousin, N = 52, r = -5322 f -0671.
t Ante-dating may or may not occur in a variety of diseases. My point is not that it never occurs but that too many investigators have applied quite inadequate statistical methods to demonstrate its occurrence. See Biornetrika, Vol. x, p. 358 et seq.

J U L I A B E L L 275
24-27
-
1 3
16 38 26 5
10 1 1
- - -
109
Table I. Hereditary Optic Atrophy. Age of Onset in Pairs of Siblings (Japanese).
28-31 ~~
- 2 -
1 6
10 13 5
48 5 3 4
3 - 3 -
- - -
~~
95
16-19
- 1 7
11 60 33 16 10 6 4 1 2 - - - -
20-23 -~
- 4 3 6
33 104 38 13 16 1 3 3 4
2 1
-
- - 1 1 1 6 5 6 1 4 4 4 1
34
- - - 1
2 7 2 1 2 1 1
-
- _ _ _ ~
17
Age of Onset
8-1 1 12-15 16-19
24-27 28-31 32-35 36-39 4 0 4 3 4 4 4 7 48-51
20-23
Totals
Table 11. Age of Onset in Pairs of Brothers (Europeans), -
rotals __
6 23 19 52
151 231 109 95 41 20 19 16 18 4 7 1
0-3 4-7 8-1 1 12-15
2 4 5
12 11 6 3 6 1 1
1
__
-
- - - -
32-35 $6-39 $ 0 4 3 L447 $8-5 1 52-55 Age of Onset
- - - 1 4 1 1 3 1 2 3 1 1 1 1 -
0-3 4-7 8-1 1
12-15 16-19 20-23 24-27 28-31 32-35 36-39 4 0 4 3 4 4 4 7 48-51 52-55 56-59 60-63
6 ~
23 -
19 - 52 - 151 1 231 41 -
16 18 812 20 I 19 7 1 1 Totals
Table 111. Hereditary Optic Atrophy. Age of Onset in Brother and Xister (Europeans). Age of Brother
20-23 I 24-27 4 0 4 3 Age of Onset Totals 16-19
- - 1 6 2 6 1 9 4
1 - - -
30
4 4 4 7
9 10 17 19 8
15 19 19 11 10 7 6 2
0-3 4-7 8-1 1
12-15 16-19 20-23 24-27 28-31 32-35 36-39 4 0 4 3 4 4 4 7 48-51
Totals 12 I 11 I 16 12 2 152
35-2

276
Age of Onset
0-3 4-7 8-11
12-15 16-19 20-23 24-27 28-3 1 32-35 36-39 4043 4447 48-51 52-55 56-59
Totals
AGE OF ONSET I N H E R E D I T A R Y OPTIC ATROPHY
0-3
- - - - - 1 - - - 1 - - - - -
2
Table IV. Age of Onset in Pairs of First Cousins (European males).
24-27
-
20 20 11
- - 1
71
- 16-19 ~
-_ 2 1 7
20 14 9 2 9 - - 1 2 - -
~
67
28-31 -- - _
1
3 2 9 2
14 11 4
7 3
1
1
- -
- - -
- - - - ~-
39
8-1 1 12-15 !O-23 32-35 36-39 L0-43 (8-51 52-55 56-59 Totals
1 1 1 6
14 48 20 14 8 5 3 1 1
1 -
2 5 2
19 67
124 71 39 35 6 6 3
10
1 -
1 1
5 2 - 19 124 - 35 -
6 6 3 10 390
Table V. Hereditary Optic Atrophy. Age of Onset in Uncle and Nephew (Europeans). Age of Nephew
Age of Onset 0-3 8-1 1 12-15 16-19
- - 1 3 9
34 12 7 3 1 2 4 5
2 1
84
-
-
20-23 24-27 28-31 52-35 36-39 L0-43 L8-51 52-55 Totals
2 9
17 36
153 59 63 14 2
10 9
12
6 1
393
-
- 2 3 9
65 19 15 6 1 2 1 - - - - - 123
- 1
2 16 16 8 2
1 1 1
-
-
- - -
~
48
4-7 8-1 1
12-15 16-19 20-23 24-27 28-3 1 32-35 36-39 40-43 44-47 48-51 52-55 56-59 60-63
Totals


![Cerebellar Atrophy in Cortical Myoclonic Tremor and Not in ... · presence of head tremor and disease onset represent different ETsubtypes [4, 5], subgroup analyses were performed](https://img.pdfslide.us/doc/110x75/5d66c02588c99356168b4884/cerebellar-atrophy-in-cortical-myoclonic-tremor-and-not-in-presence-of-head.jpg)











![Spinraza® and Zolgensma® for Spinal Muscular Atrophy: … · Infantile-onset (Type I) SMA • 1 sham-controlled, randomized controlled trial (RCT) [ENDEAR] • Later-onset (Type](https://img.pdfslide.us/doc/110x75/5d286dcf88c993c82d8d448d/spinraza-and-zolgensma-for-spinal-muscular-atrophy-infantile-onset-type.jpg)