Embed Size (px)
Citation preview

The AF ReportAtrial Fibrillation: Preventing A Stroke Crisis
An expert report on how we can prevent AF from causing a deadly UK stroke crisis
www.afa.org.ukwww.afa.org.uk www.anticoagulationeurope.org
www.preventaf-strokecrisis.org
A report for patients and those who care for them
A report for healthcare professionals
A report for policy makers and purchasers
www.anticoagulationeurope.org020 8289 6875


The AF Report 3
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Table of contents
Report summary 4
Call to action 5
Chapter 1 - What is AF?? 8
Chapter 2 - What is a stroke?? 12
Chapter 3 - Why does AF matter?? 17
Chapter 4 - Cost of AF to individuals and society?? 19
Chapter 5 - Who is at risk of AF?? 22
Chapter 6 - Treating AF and preventing stroke 26
Chapter 7 - The importance of guidelines 31
Chapter 8 - Current challenges 36
Chapter 9 - New treatments in development 41
References 45

The AF Report4
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Report summary
We are in the midst of a silent epidemic. Failure to act now will result in a crisis that we cannot afford.
The epidemic results from atrial fi brillation (AF), a heart rhythm disorder that causes strokes. Strokes, in turn, cause death and disability. Stroke is the brain’s equivalent of a heart attack and it affl icts one person every fi ve minutes in the UK1 and it is also a leading cause of adult disability.2,3
To prevent the tragic consequences of this epidemic it is essential that we target the prevention of stroke among the rapidly growing number of people who have AF.
Atrial fi brillation, the most common heart rhythm dis-order, is less well known than stroke but it affects an estimated 1.5 million people in the UK. Aside from many other symptoms and consequences, people with AF become fi ve times more likely to suffer a stroke.68 AF prevents blood fl owing properly through the heart. This disruption allows clots to form. The most common and damaging type of stroke results from clots that have travelled to the brain where they cause a blockage in a blood vessel. Twenty percent of all strokes of this type of stroke result directly from AF. 4
Moreover, AF-related strokes are more severe and cause greater disability than strokes in patients without AF.4,5 Half of all AF patients will fail to survive more than 12 months following a stroke.4 For many sufferers, surviving a stroke can be worse than dying; as disability and fear of death become constant companions. AF and stroke not only devastate patients’ lives,6
but also the lives of their families and carers.7
Despite the availability of free and simple checks, au-thoritative estimates suggest around half of AF patients remain undetected. This is frequently because patients are unaware that the symptoms they experience are a sign of anything serious.8,10 Tragically, for many people a stroke is the fi rst sign of underlying AF.
There remains an extremely low level of patient aware-ness of AF and stroke.9 Education is needed on the signs and symptoms of AF, on how AF is related to stroke, as well as on the risks they present both to life and health.
The current epidemic is predicted to worsen as the number of people with AF is expected to more than
double by 2050.11,12 AF affects a greater proportion of older people than younger. Unless we take action, our ageing population will increase both the number of peo-ple with AF and the number of strokes that result from AF.13 This increase will also be amplifi ed as we become better at preventing deaths from other conditions, such as heart attacks, which themselves increase the risk of AF developing.14
Properly used, existing treatments are effective and could prevent AF-related strokes, saving thousands of lives and millions from the National Health Service (NHS) budget.68 For example, when anticlotting therapy is used appropriately it is highly effective; lowering stroke risk by about two-thirds in AF patients.73
Yet, despite the existence of effective guidelines, vital anticlotting treatments are both underused and misused in clinical practice.15,16 This is largely due to perceived drawbacks16,5 associated with the most commonly used anticoagulant drug, warfarin.17,18 The impacts of warfa-rin on blood clotting need to be monitored not only to ensure that the drug is working, but also to ensure that the risk of excessive bleeding doesn’t become unaccepta-bly high. The need for monitoring and the risk of bleed-ing appear to have a disproportionate impact on the use of effective anticlotting therapy that would otherwise save thousands of lives.
There is evidence that the above perceived drawbacks frequently overshadow current guidelines. This results in many doctors sticking with out-of-date treatment advice19,20,125,21 despite compelling evidence that follow-ing current guidelines dramatically reduces death and disability.
Today, many thousands of preventable strokes occur every year leading both to thousands of early deaths and a devastating burden on individuals, families and society. This burden takes many forms including disability, healthcare costs, social care as well as loss of working hours and tax revenues.
There is therefore an urgent need for coordinated action within the NHS to achieve earlier diagnosis and better management to reduce the risk of stroke in patients with AF. To address this need, six actions called for by the AFA and ACE are explained in the next section.

The AF Report 5
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Call to action
AntiCoagulation Europe (ACE), the Atrial Fibrillation Association (AFA), and all those who endorse the recommendations in this report, call for an urgent focus on AF within the National Health Service (NHS), and call specifi cally for six actions that will improve and extend the lives of UK AF patients. If implemented, these actions will prevent thousands of fatal and debilitating cases of stroke; saving hundreds of thousands from stretched healthcare budgets.
Budgetary pressures within the NHS are ever-present and inevitable. Moreover, fi nancial pressure demands sound reasoning and compelling arguments before policy change or new services. Given the weight of the evidence collated in this report, it is clear that the oppor-tunity exists to make considerable long-term cost savings by implementing policies that today will result in the im-proved detection, diagnosis and management of patients with atrial fi brillation to prevent stroke.
Six actions
To achieve these goals, the six actions called for by the AFA and ACE are:
• Targeted screening: The introduction of a targeted national screening programme drawing on routine manual pulse checks and ECG readings
• Guideline adherence: The development and adoption of policies that increase GP motivation to follow international guidelines
• Public awareness, patient empowerment: The use of existing materials to fuel a national public and patient education campaign to improve detection and patient empowerment
• Equity of treatment: The imposition of equal access to AF treatments and services for all patients using the NHS regardless of location
• GP education: An AF education campaign for GPs to illustrate the importance of symptomatic control, appropriate referral and the value of patient empowerment
• AF research: Government support for research into the causes, prevention and treatment of AF
Targeted screening
We call for the introduction of a targeted national screening programme drawing on routine manual pulse checks and ECG readings
The prevalence of AF in our society continues to grow, but measures to detect and diagnose these patients remain insuffi cient. Consequently, there are many hun-dreds of thousands of patients with AF who are currently unaware, untreated and at substantially elevated risk of suffering a stroke. Moreover, the early diagnosis of AF is associated with an increased range of treatment options, some of which have been demonstrated to eliminate AF permanently.
A simple route to improving early detection and management of AF patients is through the introduction of an effective national AF screening programme. In chapter fi ve of this report, the potential advantages of routine screening methods are clearly outlined. For these to be effective, a nationwide policy change is required, one which requires:
• The audit of all patients in general practice to determine and fl ag those at AF and stroke risk
• Manual pulse checks for all risk-fl agged patients when visiting their local GP surgery
• Immediate access to an ECG for all fl agged patients for whom AF is suspected
• Ready access to 24 and 48-hour heart monitoring to secure a diagnosis of intermittent AF

The AF Report6
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Guideline adherence
We call for the development and adoption of policies that increase GP motivation to follow international guidelines
Evidence discussed in chapter seven of this report illus-trates that the following of guidelines is associated with improved patient treatment and a reduction in stroke. Confusingly in the UK, physicians have to draw upon two sets of confl icting guidance: the 2006 guidance from the National Institute for Health and Clinical Excellence (NICE) which all doctors in England and Wales are expected to follow; and the 2010 guidelines from the European Society of Cardiology (ESC) which represent the most current expert consensus on the affective management of patients with AF.
The existing NICE guideline for AF (CG36) is currently under review. The AFA and ACE have formally voiced their support for this review and look forward to engaging in consultation with NICE to ensure a revision that will result in harmony with European guidelines and the effective treatment of as many AF patients as possible. Specifi cally we call for accelerated review of the NICE clinical guideline on AF and for:
• NICE adoption of the treatment recommendations in the ESC 2010 guidelines
• NICE adoption of patient risk calculations using CHADS2 and CHA2DS2VASc as described in the ESC 2010 guidelines
• NICE recommendation of a national opportunistic screening programme based upon the fl agging of suitable patients, routine manual pulse checks and immediate access to ECG checks
• NICE recommendation for early referral to an appropriate specialist when many patients might be suitable for ablation and anti-arrhythmic therapy
• Replacement of the traditional but arbitrary classifi cation of AF (based upon the duration of AF episodes) for treatment decisions
We call for changes to the GP payment system to increase patient treatment in accordance with international guide-lines.
General practitioners are also currently poorly motivated by payments through the Quality Outcomes Framework (QOF) to manage AF patients in accordance with
guidelines. QOF seeks to reward doctors for the achievement of certain targets. The current system pays extra to doctors if they treat AF patients only with aspirin, despite considerable evidence that a signifi cant additional reduction in risk of stroke is possible with anti-coagulation treatment. Importantly, these data also show that the advantages of warfarin over aspirin come without a signifi cant increase in the risk of bleeding. At the time of preparation of this report, a revision to QOF has been proposed. We strongly support the rapid adoption of these revisions:
• Reward for a high proportion of AF patients for whom a formal stroke risk has been calculated
• Reward for a high proportion of AF patients receiving anticoagulation therapy
Public awareness, patient empowerment
We call for the use of existing materials to fuel a national public and patient education campaign to improve detection and patient empowerment
The importance of public and patient awareness and knowledge cannot be over-stressed. Almost anyone can perform a simple pulse check if they want to check for the possibility that they have AF. We have also reviewed evidence in chapter eight that greater treatment success is achieved in patients who have suffi cient knowledge of their condition to contribute to treatment decisions and targets.
Yet, today, not only are there many thousands of patients unaware that they currently have AF, many of those who have been diagnosed are unaware of what is wrong with their heart or why they are taking medication.
ACE and the AFA have developed a wealth of patient information, much of which could provide source material for a national public and patient awareness and education campaign. We call for Department of Health engagement in and support of these campaigns to:
• Increase patient awareness of AF, its signs and how they can check for AF and their risk of stroke with simple checks and tests
• Increase routine supply of educational material at the point of diagnosis, and from then on, so that patients can gain suffi cient knowledge to engage in treatment decisions

The AF Report 7
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Equity of treatment
We call for the equal access to AF treatments and services for all patients using the NHS regardless of location
The simple presence of confl icting clinical guidelines leads inevitably to the unequal treatment of AF patients within the NHS. This is by no means the only cause of inequity for AF patients; many are reviewed in chapter eight of this report. By having the NHS, a single body responsible for almost all UK healthcare, we have an unparalleled opportunity to ensure that effi cient and effective treatments and services are provided to all UK citizens regardless of local circumstances. Constant vigilance is required to identify and eliminate inequities for patients in the NHS but several targets for attention can easily be identifi ed. We call for government policy and medical practice that ensures:
• Equity of guideline adherence among doctors
• Equity of access to services such as anticoagulation clinics
• The defi nition and implementation of minimum standards to eliminate or improve services and treatments that fall short of what patients deserve
• Equity of treatment decisions based on clinical status not arbitrary defi nitions or timing
• Equity of access to anticoagulation treatment regardless of location of the patient or the availability of local anticoagulation services
• Equity of access to ideal referral opportunities regardless of the location of the patient or the availability of local heart rhythm specialists
GP education
We call for an AF education campaign for GPs to illustrate the importance of symptomatic control, appropriate referral and the value of patient empowerment
In chapters seven and eight of this report, we document many instances where doctors over-look symptoms, under-use treatments and where they fail to interpret correctly the amount of risk that a patient is willing to accept for a given benefi t.
Patients suffering from the symptoms of AF can benefi t signifi cantly from early diagnosis and referral for treatments that can have a signifi cant positive impact. It is important
that GPs develop an understanding of how signifi cant these symptoms are for the patient, and how effectively they can be helped once diagnosed and referred for specialist treatment.
We have also reviewed extensively, in chapter seven of this report, the discrepancies between the theoretical benefi ts of anticoagulation treatment and the actual benefi t achieved in routine clinical practice. Much of this difference can be accounted for by deviation from guide-lines founded on a misunderstanding among physicians of how their patients view the risks and benefi ts of treat-ment.
The above challenges can be met with educational efforts and tools that:
• Improve GP understanding of the impact that AF symptoms have on quality of life
• Improve GP understanding of the benefi ts of patient education and engagement in decisions
• Help GPs improve patient understanding of the risks and benefi ts of treatment
• Improve GP understanding of the potential benefi ts of early referral
AF research
We call for government support for research into the causes, prevention and treatment of AF
Many of the challenges faced by healthcare policy makers and doctors today arise from inadequate access to the necessary data to make effective decisions. This report and the document upon which it is based aim to help increase access to vital information. However, some data simply doesn’t yet exist, highlighting an urgent need for continued research into AF so that services and policies can be developed with a fi rm confi dence of success and cost effectiveness for the NHS. To this end, we call for government support for:
• An assessment of the burden and severity of disease for all patients with AF, based on patient experience and the impact on their quality of life
• Research to identify patients at risk of AF and AF- related stroke, and the likely impact of existing and new therapeutic approaches to the management of AF
• Multi-national registries and monitoring studies to evaluate the effect of interventions to manage AF and prevent AF-related stroke.

The AF Report8
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Key points• AF is the most common sustained heart rhythm disorder
• Having AF doubles the risk of death, regardless of age
• In symptomatic patients, AF is frequently associated with a highly signifi cant reduction in quality of life
• In all AF patients, the risk of suffering a stroke is increased nearly 500%
• AF can be detected with a simple pulse check but approximately half of all patients remain undiagnosed
• AF, and AF related illness, costs the NHS over £2.2 billion each year
• AF affects nearly 2% of the population, a number that is rising fast
• Between 100,000 and 200,000 people in the UK develop AF every 12 months
Atrial fi brillation (AF) is a common heart rhythm disorder associated with deadly and debilitating consequences including heart failure, stroke, poor mental health, re-duced quality of life and death.71
AF is also the most prevalent sustained heart rhythm disorder.193 Today, approaching a million Britons are diagnosed with AF,61 yet experts suggest that between one third and a half of all AF patients have not yet been detected. Today, everyone aged 40 or over has a life time risk of developing AF of at least one in four.24 For context, this compares with one in eight for breast cancer in women of the same age.25
Among many damaging and debilitating consequences, AF increases an individual’s risk of suffering a stroke by fi ve times.68 This effect alone results in considerable disability and death,193,4 not to mention avoidable mil-lions in healthcare expenditure61 that the National Health Service (NHS) cannot afford.
Chapter 1 - What is AF?
What is AF?
Atrial: pertaining to the atria (pleural of atrium) the top two chambers of the heart
Fibrillation: the rapid, irregular and unsynchronised contraction of muscle fi bres
AF is a heart rhythm disorder (a cardiac arrhythmia) of the atria. The normal beat of the heart (called sinus rhythm) is managed by a sophisticated electrical control system. This system matches heart rate with physiologi-cal demands and ensures that the four chambers of the heart contract and relax in time with one another to maintain a steady and effi cient rhythm to pump blood.
The heart’s natural pacemaker is a cluster of special cells in the atria called the sinus node. The sinus node controls the rate at which the atria contract and relax. In AF, chaotic electrical activity develops in the walls of the atria, over-riding the sinus node. The normal, steady rhythm of the atria is disrupted and they instead begin to fi brillate; quivering with a shallow but very fast rhythm as their muscular walls fail to contract with regularity and coordination.
An irregular pulse
This atrial fi brillation disrupts the electrical signals that trigger the contraction of the heart’s main pumping chambers, the ventricles. Consequently, the ventricles beat faster and their rhythm becomes irregular as the electrical conduction system is over-run by the fast and chaotic impulses from the fi brillating atria. This altered ventricular beating can be detected as an irregular pulse, a valuable yet simple test for AF.
A progressive condition
Initially for most patients, AF is an electrical problem in the heart that can be addressed by therapies which treat the rate and rhythm of the heartbeat, or which can immediately return the heart to normal sinus rhythm – a procedure called cardioversion.

The AF Report 9
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Signs, symptoms and consequences of AF
There are many negative consequences of AF frequently leading sufferers into a life of confusion and despair.28 AF is associated with a signifi cant increase in risk of stroke, heart failure and death.71 It has also been found that approximately one third of AF patients suffer per-sistent anxiety or depression. From the same research, depression was also noted to have considerable nega-tive impact on future quality of life.29 Other symptoms include palpitations, shortness of breath, light-headed-ness, fainting, fatigue and chest pain.33 For emergency admissions to hospital, AF most often presents as diffi -culty with breathing, chest pain and palpitations.64
A simple and easily identifi able sign of AF is an irregu-lar pulse. For this reason, many AF experts and patient advocacy groups are calling for pulse checks to become a free, swift and routine part of every GP visit.
However, AF is frequently intermittent and many peo-ple with AF have no or non-specifi c symptoms.8 These combine to make detection and diagnosis diffi cult; often, AF is not apparent until a person goes to see their doctor with a serious complication such as stroke, a blood clot in the leg or heart failure.64
Over time, AF which is untreated, or which fails to respond to treatment, begins to change the anatomy of the heart muscle, interfering further with the electrical conduction necessary for a normal heart beat. Eventual-ly, all treatments to correct the electrical system become ineffective, leading to therapy that aims only to prevent the consequences of AF.
Deadly consequences
Atrial fi brillation disrupts the effi cient pumping of blood through the heart and around the body. The disturbance in fl ow can allow clots to form where the blood moves too slowly. The blood stream can then carry these clots to vessels in the brain causing deadly blockages that result in stroke.
Massive NHS burden
AF is a signifi cant and growing drain on the NHS. During the past 20 years there has been a 60% increase in the number of patients being admitted to hospitals as a result of AF.26 In 2008, there were an estimated 850,000 GP visits because of AF in the UK.61 When including AF as a causative secondary diagnosis, the total cost of AF to the NHS has been calculated to be nearly £2.2 billion a year.61 Some authoritative estimates predict a three-fold increase in AF over the next 50 years.12,27
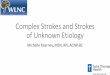
Heart failure AFCoronary artery disease
High blood pressure
50
40
30
20
10
0
Without this conditionWith this condition
Inci
denc
e of
stro
ke
Risk factors for stroke
Increases stroke risk by 340%
Increases stroke risk by 240%
Increases stroke risk by 430%
Increases stroke risk by 480%
AF increases the risk of stroke by nearly fi ve times, more than any other cardiovascular risk factor

The AF Report10
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Yet, even patients who do experience symptoms of AF
are not always diagnosed immediately. In a recent international survey, there was an average delay of 2.6 years between the onset of symptoms and the diagnosis of AF.30 In another piece of research, among patients with documented chronic AF, it was found that more than a third were not aware of their diagnosis and up to half were unaware of why they were being treat-ed.31 This indicates that many patients with AF are not being detected or managed effectively and that many are at risk of serious long-term consequences such as stroke.
Efforts have already begun to increase the rates of diagnosis and effective management of AF. For exam-ple, the National Institute for Health and Clinical Excel-lence (NICE) recommends that doctors make assess-ments for the presence of AF in all people presenting with breathlessness, palpitations, fainting/dizziness, chest discomfort, stroke or mini-stroke (TIA).32
How does AF lead to stroke?
AF results in a fi vefold increase in the risk of stroke, making it the most powerful independent risk factor for stroke.68 Moreover, strokes in patients with AF tend to be more severe than in non-AF patients.72 The above chart illustrates the impact that AF has on the likelihood of suffering a stroke compared to other stroke risk factors such as high blood pressure, heart disease and heart failure.
The risk of stroke increases because AF is associated with the formation of clots inside the heart. During AF, blood can slow as fi brillation prevents the normal high-pressure fl ow of blood through the heart and out to the arteries. When blood is allowed to travel slowly the natural formation of clots can begin. This is usually a safety mechanism to help prevent excessive bleeding at sites of injury.
In stark contrast, clots forming within the heart and arteries can be deadly. As clots travel downsteam into increasingly smaller arteries, even small clots can cause blockages that prevent oxygen and nutrients reaching the tissues. If such a blockage occurs in the brain, the damage done by the lack of blood fl ow results in a stroke. AF is estimated to be responsible for approximately 15%-20% of all strokes. 63,4
Who gets AF?
It is diffi cult to overstate just how big a problem AF presents. To provide some perspective, one authoritative
and recent study from the Mayo clinic in the US concluded that, for anyone aged 40 or above, the life-time risk of AF exceeds 25%;24 meaning that one in four adults can expect to develop AF. This compares to the lifetime risk of breast cancer in women of the same age, which is one in eight.25 However, because of improved detection methods, each new study of the prevalence of AF reports an increase for the same point in time. For example, the Mayo clinic study above was published in 2004 when AF was thought to affect less than 1% of the population they were studying.34
We now know that around 2% of the population in 2004 had AF. It is predicted that by 2050, over 4% of the population will have it.12 Consequently, it is very likely that, for those aged 40 today, the lifetime risk of devel-oping AF in fact higher than one in four .
Given the number of people who have or will develop AF, it is not easy to defi ne a typical AF patient. Men and women of all ages can be affected. In general terms, the likelihood of developing AF increases with age.193
However, some people appear to be at a higher genetic risk. This predisposition to AF is most often seen in young patients.191,199 In addition, some studies suggest that the incidence of AF is higher than normal in athletes and others who engage in frequent, vigorous exercise regardless of age.35,36 For all these reasons, AF is not just a condition of the elderly.
What causes AF?
The most common underlying causes of AF are high blood pressure, thyroid disease and, to a lesser extent, coronary artery disease and diabetes.195,178 Dietary, lifestyle and other factors that contribute to the risk of AF include emotional and physical stress and excessive caffeine, alcohol or illicit drug intake.64
The main causes of AF are different than they were 20 years ago. At that time, rheumatic disease commonly resulted in the hardening and narrowing of the heart’s mitral valve (mitral stenosis) and was an important cause of AF. The incidence of rheumatic disease in European patients has diminished consider-ably in recent decades due mainly to improved living conditions. Today, AF as a result of mitral stenosis is relatively rare. The term ‘non-valvular AF’ is used to describe cases where rhythm disturbance is not associated with these problems.8 This report is concerned only with non-valvular AF, which is that most frequently encountered in the UK.

The AF Report 11
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875How many people suffer from AF?
As we have seen, AF is responsible for many hundreds of thousands of GP visits61 despite estimates that nearly be-tween one third and a half of those affected are yet to be diagnosed. Over 800,000 patients in the UK are known to have AF.61 As symptoms are not always specifi c, and because there is no routine screening for early detection, experts estimate that the total number with AF in the UK might exceed 1.5 million.
The numbers of people affected by a condition are gen-erally measured in two ways. Prevalence is the propor-tion of a population affected at any given time; usually as a percentage. The other measure is incidence, which measures just the newly affected patients in the popula-tion over a given time span, usually 12 months.
Growing and under-detected prevalence of AF
As seen in the example above from the Mayo clinic in the US, the proportion of the UK population with diagnosed AF is also growing. Today we believe the prevalence of AF in the UK to be near 2% and increasing.27 Between 1994 and 2006, the UK prevalence of AF rose from 0.78% to 1.42%.27 This increase appears to refl ect increasing life expectancy as well as the impact of medi-cal science that enables more people to survive condi-tions such as heart attacks that can add to the likelihood
of developing AF. 66 There is also the very real likelihood that an improved focus on AF, and improved methods of detection, will uncover greater numbers still.
Independent of this increase in prevalence of AF over time in our society, the number of people with AF has been shown to double with each advancing decade of age, from 0.5% at age 50-59 years to almost 9% at age 80-89 years.193 Not surprisingly, the incidence of AF also increases with age, contributing to the growing prevalence.193
As all these factors combine, it has been predicted that the total number of people affected by AF is likely to triple by 2050.12,27
Incidence of AF in the UK
The most recently published data on the number of people in the UK who develop AF is from 2002. This research reported that the incidence of AF in the UK was 1.7 per 1,000 patient years.37 With today’s population this would mean that 105,000 people develop AF every year. If, however, the number of people developing AF has been increasing each year since 2002, similar to the increase observed above, then it could be that approaching 200,000 people in the UK are now developing AF every 12 months.37,12
Milli
ons
of a
dults
with
AF
7.0
6.0
5.0
4.0
1.0
2.0
3.0
0
Year20201990 1995 2000 2005 2010 2015 2025 2030 2035 2040 2045 2050
The number affected by AF is predicted to double by 205011

The AF Report12
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
What causes a stroke?
The vast majority, around 85%, of strokes are caused by a blockage in one of the blood vessels that supplies the brain.56 The remaining 15% are usually the result of a bleed. Strokes caused by blockages are called ischaemic (ISS-KEEM-IC). Ischaemic is a medical term denoting a lack of oxygen. The most common cause of ischaemic strokes is a blockage caused by a blood clot. Most ischaemic strokes are the result of an embo-lism, which is a clot, or other material, that travelled to the brain in the bloodstream from somewhere else. For example, a blockage caused by a clot that formed in the heart is a cardioembolic ischaemic stroke. Strokes caused by bleeds are called haemorrhagic (HEM-UH-RA-JIC).
What’s a mini-stroke or TIA?
If the blood supply to the brain is only briefl y interrupted a mini-stroke might result. Also known as a transient ischaemic attack or TIA. The symptoms of a TIA are very similar to those of a stroke but last fewer than 24 hours. It is vital that medical attention is sought regardless of the temporary effects; individuals who have had a TIA are at high risk of suffering a stroke. Studies have shown that in the 90 days following a TIA, the risk of stroke exceeds 10%.39
How many people does stroke affect?
Worldwide, stroke is the most common cardio-vascular disorder after heart disease, accounting for 5.7 million deaths annually, nearly one in ten of all deaths.43 In the UK, 150,000 people are struck by stroke each year,1 and 53,000 people are killed.40 This makes stroke the third biggest killer in the UK after heart attacks and cancer.41
Stroke accounts for 9% of all deaths among UK men and 13% among UK women.42
For many, surviving a stroke is a fate worse than death; stroke is the leading cause of adult disability. Over 300,000 people in the UK are living with permanent disabilities as a result of suffering a stroke.3
Chapter 2 - What is stroke?
Key points• Stroke accounts for 10% of all deaths
• Stroke affects 150,000 people in the UK, killing 53,000 each year
• Stroke-related costs in the UK NHS amount to £2.8 billion
• Surviving a stroke is frequently reported to be ‘worse than death’
• Stroke is a leading cause of adult disability
• The consequences of stroke are dramatic and can negatively impact many people beyond the stroke victim
The brain requires a constant supply of blood for it to receive essential oxygen and nutrients. A stroke happens when the blood supply to any part of the brain is cut off and brain tissue is damaged.
The impact of a stroke is both instant and unpredictable. The nature and the severity of the effects depend on the amount of damage caused and the part of the brain that has been affected. Frequently people become paralysed, numb or incapable of normal speech. Vision can be impaired, as can both thoughts and feelings.
Stroke accounts for 10% of all deaths,43,56 and is also a leading cause of adult disability.3,38 The sudden nature of stroke means that sufferers, families and carers have no opportunity to prepare for what is usually a tremendous blow to their lives.
Beyond the personal impact of death and disability, stroke costs us all through the massive burden it places on National Health Service (NHS) budgets and the impact it has on the wider economy. It is estimated that the direct cost of stroke to the NHS is £2.8 billion, and that stroke patients occupy up to a quarter of all hospital beds.3
Effective methods to prevent stroke in people at high risk are both widely available and inexpensive. The potential exists to save thousands of lives and millions from health-care budgets.

The AF Report 13
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875The total number of people living through the conse-
quences of stroke in Europe has been estimated to be 9.6 million.43 A World Health Organization (WHO) study reported that the annual number of new cases in Europe to be two million in 2004.43 This was compara-ble to the estimated annual incidence of cancer cases at 2.9 million for the same year.44
For countries within the EU, a study based on data from WHO estimated the number of strokes to be 1.1 mil-lion in 2000.69 Furthermore, it has been predicted that stroke incidence will increase to 1.5 million per year by 2025, largely owing to the increasing proportion of elderly individuals.69
The below charts illustrate authoritative estimates of stroke incidence throughout Europe. It is immediately apparent from the fi rst chart that some countries face a greater challenge than others and that, Europe-wide, men are generally affected more than women. It is also clear that the UK has a long way to go if we are to reduce the rate of stokes to levels currently observed in France and Switzerland. Unless we act now to prevent
avoidable strokes in AF patients, this task will become immeasurably more diffi cult.
This second chart shows the same data by age. While it is clear that stroke is most commonly an affl iction of the elderly, there are many countries within which a dispro-portionate number of those affected by stroke are aged 55-74.
Who suffers from stroke
While predominantly affecting the elderly, approximately 25% of strokes occur in people aged below 65 years.22 In the UK, it has been estimated that 20,000 strokes occur in those who are 45 and younger every year.
Several risk factors other than age contribute signifi cantly to stroke risk. Principal among them are atrial fi brilla-tion, heart failure, heart disease and high blood pres-sure. Atrial fi brillation has the most powerful impact, elevating risk over a non-AF patient by fi ve times. AF is directly responsible for 20% of strokes. High blood
Comparing stroke rates in Europe.69
0 5000 10000 15000 20000 25000
SwitzerlandFranceSpain
SlovakiaBelgium
NetherlandsIceland
DenmarkSweden
UKAustriaIreland
GermanyNorwayFinlandPolandCyprus
MaltaItaly
LuxembourgLithuaniaSloveniaHungaryEstonia
CzechRepublicGreece
PortugalLatvia
Women
Men
Total stroke
Estimated numbers of strokes as a proportion of population

The AF Report14
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
pressure on its own elevates the risk less than each of the other three main risk factors, but because so many people have high blood pressure, it represents the single biggest cause of stroke in the UK.
Lifestyle factors also play an important role. Smoking has been shown to double a person’s risk of suffering a stroke. Poor diet, lack of exercise and excessive alcohol intake have also been shown to increase stroke risk.
Some ethnic differences may also exist, refl ecting differ-ences in the predisposition to some of the risk factors associated with stroke. For example, there is a high prevalence of high blood pressure and, as a conse-quence, stroke, among afro-caribbean populations. In the UK, the death rate from stroke has also been found to be higher among individuals of south asian origin than among the caucasian population.45
What are the consequences of stroke?
As well as accounting for nearly 10% of all deaths,43 56
stroke is a major cause of long-term disability. World-wide, fi ve million stroke sufferers are left permanently disabled every year.56 In the UK, over 300,000 stroke survivors are living with permanent disabilities which leave them dependent upon others. Stroke can affect nearly all human functions, making it diffi cult for many patients to get out of bed, walk short distances or per-form the basic activities of daily living. As well as impair-ing speech and physical functioning,56 stroke can also adversely affect mental health.46
Strokes are sudden and they frequently affect people who were unaware they were at risk. Consequently, they and their families are often poorly prepared to deal with the stroke and the damage it brings to their lives.46 Long-term disability can dramatically affect the quality of life of both patient and relatives.
The risk of stroke generally increases with age.69
0 5000 10000 15000 20000 25000
SwitzerlandFranceSpain
SlovakiaBelgium
NetherlandsIceland
DenmarkSweden
UKAustriaIreland
GermanyNorwayFinlandPolandCyprus
MaltaItaly
LuxembourgLithuaniaSloveniaHungaryEstonia
CzezhRepublicGreece
PortugalLatvia
75+
55-74
25-54
Total stroke
Estimated numbers of strokes as a proportion of population

The AF Report 15
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Not only does the patient and his or her family frequently
have to shoulder the burden of an unexpected long-term disability, those living with the aftermath of a stroke are often in constant fear of death or another stroke.
The consequences of stroke are far from limited to the elderly. A long-term study assessing outcomes in young adults (aged 15–45) after a stroke found that within six years only 49% were still alive, not disabled, had not suf-fered from a recurrent event or had not undergone major vascular surgery. The majority of the survivors also re-ported emotional, social or physical effects that reduced their quality of life.47
What are the costs of stroke?
Not only are strokes tragic, fatal and debilitating, they are extremely expensive. It has been estimated that a single stroke costs the NHS between £9,500 and £14,000. The factors that cause a stroke have been found to have a bearing on the severity of a stroke. For example, people with AF tend to have more severe strokes which are consequently more expensive.48,62
Strokes cost more than their direct burden on healthcare budgets. The wider economy suffers from the loss of productivity associated with disability and death. The long-term care required for stroke survivors is usually informal and often overlooked. Yet this also comes with a tremendous cost to society. Then there is the human cost, which is incalculable.
Our NHS hospitals are also burdened with providing the physical space required to treat stroke patients. Stroke survivors occupy around 20% of all acute hospital beds and one quarter of all of long-term beds.3
The direct cost of stroke to the NHS has been estimated to be £2.8 billion every year. This huge sum, however, does not represent even half of the total costs. The indirect costs to the wider economy are £1.8 billion and the costs of informal post-stroke care amount to an esti-mated £2.4 billion.3
If just the avoidable strokes arising because of AF were prevented, the NHS would save nearly £60 million in direct stroke costs alone. In the chart below, the cost of stroke to the UK can clearly be seen. Both the total of stroke costs and the cost per head of population are among the highest spent of any country in Europe.
The cost of stroke for the whole of the EU was calculated to be over €38 billion in 2006. This fi gure included healthcare costs (about 49% of the total), productivity loss due to disability and death (23% of the total) and informal care costs (29% of the total).57 These fi gures demonstrate the tremendous fi nancial burden to society posed by stroke in Europe.
It is clear that stroke is a costly health problem in the UK and beyond. Stroke accounts for a massive burden on patients, their carers, families, friends and society. This burden falls disproportionately on the elderly, who are most at risk. Early diagnosis and effective management of atrial fi brillation would help to reduce the burden of stroke in the UK. Furthermore, the prevention of stroke with existing, cost-effective therapies in patients at high risk has the potential to reduce this huge economic bur-den signifi cantly.50
For example, in patients with AF, who are known to have a high risk of stroke, the cost of treating a stroke has been calculated to be almost four times greater than the cost of prevention with ten years’ anticlotting therapy.97

The AF Report16
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Stroke is a massive expense for the NHS and the taxpayer.57
Total Healthcare cost in millions of Euros Cost per person in Euros
0 1000
MaltaCyprus
LuxembourgEstonia
LatviaSlovenia
LithuaniaBulgariaSlovakiaHungary
IrelandRomania
Czech RepublicDenmarkBelgiumPortugalAustriaFinlandPoland
SwedenGreece
SpainNetherlands
FranceItalyUK
Germany
MaltaCyprus
LuxembourgEstonia
LatviaSlovenia
LithuaniaBulgariaSlovakiaHungary
IrelandRomania
Czech RepublicDenmarkBelgiumPortugal
AustriaFinlandPoland
SwedenGreece
SpainNetherlands
FranceItalyUK
Germany
2000 3000 50004000 0
(a () b)
20 40 60 80
Total healthcare cost Cost per person

The AF Report 17
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Chapter 3 - Why does AF matter?
Key points• Strokes in people with AF are more severe and have worse outcomes than strokes in people without AF
• AF almost doubles the death rate from stroke
• AF strokes are cardioembolic which leads the increased risk of more brain damage
• AF increases disability from stroke
• AF increases the risk of a stroke happening again
The burden of stroke for patients with AF is worse than just an increase in stroke risk. The strokes suffered by people with AF are also more severe,72 they are more frequently fatal4,55 and they are more likely to lead to disability,4,5,178,72 increased healthcare costs106 and extended hospital care than strokes in patients without AF.72 Moreover, AF-related strokes are more likely to happen again, adding not just to the risk of future strokes, but also to the potential for increased patient anxiety and a further reduction in quality of life.
Why does AF lead to more severe strokes?
The increased severity of strokes in patients with AF is thought to be related to the large size of the clots that ultimately block blood vessels in the brain. Almost all AF-related strokes are cardioembolic; which means that the clot forms in the chambers of the heart from where it travels downstream in the blood to the vessels of the brain. Clots will naturally grow rapidly in size as part of the body’s safety mechanism to prevent bleeding. The further a clot travels, the greater opportunity it has to in-crease in size. Once in the brain, a larger clot can block larger vessels. The bigger the vessel that is blocked, the greater the amount of brain tissue that is likely to be affected. And so it follows that the greater the amount of brain that has its blood supply cut off, the greater the chance of a severe stroke, death and disability.
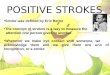
AF causes half of all dangerous embolic strokes.52
AF nearly doubles the death rate from stroke
Many aspects of strokes are more severe among AF pa-tients but one of the most dramatic is mortality; the likeli-hood that a stroke will kill. AF-related strokes kill nearly twice as frequently as non-AF strokes. In a Danish clini-cal study, stroke patients with AF were 70% more likely to be killed than those without AF.72 A larger subsequent study of Italian stroke patients found that the increase in death rate among AF patients after 12 months was even higher; almost double the rate of those without AF.4 An Austrian stroke registry also demonstrated a near dou-bling of death rate from stroke in the presence, com-pared to the absence, of AF (25% versus 14%).55
AFVentricular thrombusRheumatic heart diseaseAcute myocardial infarctionReplacement valvesOther causes
50%
10%
10%
10%
5%
15%

The AF Report18
www.afa.org.uk
www.anticoagulationeurope.org020 8289 687512 months after a stroke nearly twice as many AF
patients will have died compared to non-AF patients55
So powerful is this effect, AF has been found to be to be an independent predictor of death even after adjusting for age, sex and vascular risk factors.
A trend towards an increase in the overall early death rate in patients with AF over the last 20 years has also been reported,51 which may refl ect the increasing age of the population. With both AF prevalence11 and AF death rate increasing, there is an urgent need to improve the management of AF, in particular to prevent the most common fatal consequences, such as stroke.
For a more thorough review of the long-term conse-quences and costs of AF-related strokes, please see chapter four.
Patients with AF are therefore a vital target population for reducing the overall burden of stroke on society.
Annual death rate (%)Year With AF Without AF1 50 272 14 83 14 64 10 65 11 66 4 37 5 48 4 3

The AF Report 19
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Chapter 4 - Cost of AF to individuals and society?
Key points• AF-related stroke impairs stroke survivors’ quality of life more than non-AF-related stroke
• Permanent disability and other consequences of AF- related stroke place a heavy burden on carers, family members and health and social services
• Healthcare costs associated with stroke are higher for patients with AF than for patients without AF
Signifi cant impact on quality of life
Survivors of strokes have described their subsequent life as a fate worse than death. This description is not only dramatic and intuitively apparent, it is also supported in the scientifi c literature. For purposes of research, the impact of a stroke can be evaluated on a scale of zero to ten where 10/10 represents perfect health and 0/10 represents death.53
In a study that used these scores to evaluate the impact of stroke on the quality of life for patients with AF, 83% of patients rated their quality of life after a severe stroke as equal to, or worse than, death.54
Other scores have been developed to assess specifi c aspects of quality of life; such as neurological function. A comparison of AF and non-AF strokes is presented in table 4 across several of these aspects. As above, the scores in the table consistently show that AF-related stroke has a more negative impact on quality of life than non-AF-related stroke.72
AF also increases the risk of medical complications fol-lowing stroke. Compared with those without AF, patients with AF suffer more frequently from pneumonia, pulmo-nary oedema (accumulation of fl uid in the lungs) and bleeding in the brain after stroke.55
Heavy burden on carers, families and society
This sustained impact of strokes has a devastating impact not only on the individual and their carers but also on the wider family, particularly children.
Increased disability and poor health
More than one-third of patients who experience a stroke return to their home with some level of permanent disability.56 They then rely on informal care, typically from family members, to help with their normal daily activities and to arrange the required additional assistance from healthcare services.
The disabling consequences of stroke are worse for those patients who survive an AF-related stroke, than for those without AF. The presence of AF increases the risk of remaining disabled after a stroke by almost 50%.5
This disability takes many forms. When compared with non-AF patients, the presence of AF at the time of stroke has been found to:
• Increase signifi cantly the loss of ability to perform normal daily activities,• Decrease the level of consciousness,• Increase the partial paralysis of the arm, hand and/or leg• Increase the diffi culty in swallowing
This was found to be the case both immediately after the stroke and after rehabilitation.72
Psychological impact on patients, family and carers
In addition to providing day-today practical care, the family also has to manage the emotional, mental and behavioural changes in the patient. These changes can be among the most diffi cult for family members to han-dle. They include mood swings, personality changes, irritability, anxiety, memory loss and depression.56,58
Faced with such transformations, and the corresponding effort required to provide vital care, members of the family can experience a loss of independence, identity and social life. They also suffer extreme tiredness and depression. These carers also report fears regarding the safety of the patient and distress at not having time to attend to all of the patient’s needs.56,58

The AF Report20
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875High long-term demand on health and
social services
The rehabilitation and long-term care of stroke survivors also place a signifi cant demand on formal health and social services, often involving community nursing, social care, physiotherapy as well as speech and occupational therapy.56,59 Research indicates that AF increases the requirement and costs for the provision of this formal care compared to non-AF stroke patients.72
Increased hospitalisation, cost and recurrence with AF-related stroke
AF has been found to be associated with a 20% increase in the length of hospital stay and a 40% decrease in the likelihood of patients returning home compared to the absence of AF in surviving stroke patients.72
As described in Chapter three, almost all AF-related strokes are cardioembolic; where the clot forms in the chambers of the heart from where it travels downstream in the blood to the vessels of the brain. Compelling research has shown that those who suffer cardioembolic strokes have a poorer clinical condition on admission to hospital, experience a longer stay and endure a worse recovery following discharge than those with non-car-dioembolic stroke.106 The same study also found that costs were higher. The average cost per patient of initial hospital care for cardioembolic stroke was €4,890 per patient, compared with €3,550 for non-cardioembolic stroke, representing an increase of almost 40%.106
In addition to being more severe, cardioembolic strokes are associated with a higher risk of recurrence than other types of stroke.60 The increased severity and risk of recurrence of strokes in patients with AF compared with other strokes suggests that these patients will experience a greater impairment in quality of life than patients without AF.
Case study: a carer’s perspective
“For the past nine months my sister and I have been acting as full- time carers to our mother, who is bedrid-den following a stroke. She is unable to do anything for herself and needs 24-hour care in her own home, where she feels comfortable and safe. We have had to leave our husbands and our own homes to give mother our full support.
Full-time carers can lose their sense of identity and independence as their social life is curtailed. I am also concerned for my husband’s welfare.”
Case study: a child’s perspective
“The fi rst time I saw Daddy again, he was sitting in a wheelchair tied on with a sheet so that he would not fall. His mouth was drooping and he was making funny noises which we could not understand. I was scared of him, I didn’t want to see him any more. I was ashamed of him... he does not remember much about it. He doesn’t look like Daddy any more.”
High economic cost
As explored in chapter two, strokes are extremely expen-sive, each one costing the NHS between £9,500 and £14,000. AF stokes are more severe72 and consequently can be expected to account for a greater proportion of the more expensive strokes. This impact of AF becomes of considerable importance when considering that the cost of stroke to the UK economy has been estimated to be £2.4 billion,61 and the cost of stroke to Europe is likely to be over €38 billion.57
AF-related strokes cost more
In a clinical study that investigated the cost of different severities of stroke, it was found that the average cost of a severe stroke was more than three times higher than the average cost for a mild stroke.48
There is also direct evidence for the increased cost of stroke in patients with AF. In one study, the average direct costs of stroke per patient were found to be over a third higher in patients with AF than in patients without AF.62
The effect of AF on stroke-related inpatient costs was also recently analysed. The inpatient costs over just a three-month period were on average 8% higher for each patient with AF compared to patients without AF.196 As AF is estimated to be responsible for approximately between 15-20% of all strokes,63 the increased cost of AF-related strokes compared with other strokes represents a signifi cant economic burden.
Direct costs of AF to NHS are huge
All the above studies were focused on the economic burden of AF associated only with the elevated risk and severity of strokes. A study from the Offi ce of Health Economics published in 2009 deliberately set out to

The AF Report 21
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875evaluate the direct costs to the NHS of all AF. The study
investigated the costs of AF alone, as well as the costs of secondary problems such as AF-related stroke and AF-related heart failure.
For 2008, it was calculated that AF accounted for 5.7 million days in hospital beds and a total direct cost to the NHS of £2.2 billion.61 AF patient days spent in hospital beds cost the NHS over £1.8 billion. Non-bed in-patient costs were £124 million and outpatient costs completed the total at £205 million.
Together with loss of time in employment and contribu-tion to the community of the patient, and most probably also to those providing informal care, this amounts to a signifi cant burden on society and on thousands of individuals.
Strong rationale for stroke prevention in patients with atrial fi brillation
In conclusion, patients with AF have a higher risk of stroke and suffer from more severe strokes than patients without AF. Thus, AF-related stroke imposes an even greater burden on individuals, carers, families, society and healthcare resources than stroke in patients without AF, providing a strong rationale for effective manage-ment of AF and prevention of stroke in this high-risk population.

The AF Report22
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Chapter 5 - Who is at risk of AF?
Key points• For many people AF is silent, with no symptoms to prompt either concern or medical consultation
• AF is often not detected until the development of a serious complication such as stroke or heart failure
• Routine opportunistic pulse checks represent an effective and cost-effective method of improving the detection of AF in patients at risk of stroke
• Many methods are used by doctors to determine stroke risk for an individual patient, and hence the ideal treatment to prevent stroke
• Patients in the UK may currently be receiving inconsistent advice and therapy, due to a lack of consensus on AF risk stratifi cation
Atrial fi brillation is often present with-out symptoms
AF patients, because of their elevated risk both of having a stroke and having a severe stroke, represent an ideal focus for stroke prevention. However, we have also dis-cussed in earlier chapters that a substantial proportion of AF patients are currently undiagnosed or inappropriately treated. This chapter reviews detection, diagnosis and decisions on who and how to treat for the prevention of stroke.
Although AF may be recognized by symptoms such as palpitations or dizziness it is commonly asymptomatic, when the patient is unaware of anything that might indicate that they have AF. This is commonly called silent AF. Consequently, many people have undetected AF, and might have had it for some time.8 Studies using heart monitors that record heart rhythms 24 hours a day have shown that it is common for a patient to have periods of both symptomatic and asymptomatic AF.8 It is often the case that a diagnosis of AF is only made following a serious complication such as stroke or heart failure.64
Detection and diagnosis of atrial fi brillation
Effective AF detection and diagnosis strategies are essen-tial before treatment and the prevention of deadly and debilitating strokes become possible. Steps to improve the detection of AF have already been made; guidelines from the National Institute of Health and clinical Excel-lence (NICE) recommend that an ECG is required for all patients with an irregular pulse whether symptomatic or not.64 ECG stands for electrocardiogram and is the method doctors use to capture the electrical signature of heart rhythm problems. However, for this recommenda-tion to be effective, patients fi rst need to have their pulse checked for irregularity. Modern electric pulse meters have all but taken over this job from doctors and nurses. Unfortunately, extremely few modern electrical pulse check machines are capable of detecting an irregular rhythm. Consequently, one of the most valuable detec-tion methods for AF has largely been eradicated from the NHS by the advance of technology.
Many patients have other risk factors for stroke, such as high blood pressure, diabetes and heart disease. For these conditions they will already be receiving frequent check ups. The introduction of opportunistic screening by making routine manual pulse checks during these check ups would appear to be a prudent, simple and low cost method to increase the detection of AF and prevent strokes.
Opportunistic pulse checks are a low cost option
A UK study, involving almost 15,000 patients, compared opportunistic screening for AF, as described above, with another, systematic, method. Compared to routine clini-cal care, opportunistic screening identifi ed approximately 50% more cases of AF. Systematic screening identifi ed approximately 70% more case than routine clinical care, but was associated with a high cost per patient, nearly fi ve times the cost of the opportunistic approach.139 The opportunistic screening was associated with a cost of only £363 per patient. However, only a tiny fraction of this was for the inclusion of a manual pulse check at routine appointments. The majority of the cost was ac-

The AF Report 23
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875counted for by the subsequent ECG and interpretation;139
steps already required by the NICE Guidelines upon detection of an irregular pulse.
The study highlighted the important role of a simple, routine pulse check, in helping to improve detection of AF. The policy implications arising from the results of this study are that an opportunistic approach using pulse- taking followed by ECG is probably the most cost-effec-tive option for any screening programme implemented through primary care.139
Despite these results, today there is no policy, formal tar-get or recommendation from the Department of Health that recommends or mandates the routine manual pulse checks for any group of patients at GP surgeries.
The role of ambulatory monitoring
Episodes of AF can be both short and infrequent which adds to the diffi culty of detection and diagnosis. For some patients, for example those who have reported instances of their own pulse being irregular, there is potential value in the use of heart rhythm monitors that record the pulse constantly for up to several days at a time. A patient would need to wear the device for between 12 and 72 hours but the constant monitoring would greatly increase the likelihood of a positive diag-nosis. When prolonged monitoring is used in ischaemic stroke patients, AF is detected in one in 20 cases, provid-ing powerful evidence for the routine adoption of such monitoring in these stroke patients.
Making treatment decisions based upon risk of stroke
Once an AF patient is identifi ed, it becomes necessary to make a treatment decision that best addresses the needs of the patients; lowering risk of stroke as much as pos-sible while not adding further unnecessary risks to the patient’s health. The treatment options to prevent stroke will be covered in more detail in the following chapter but in short; patients at low risk of stroke are often can-didates for treatment with the antiplatelet drug aspirin.116
For patients at moderate and high risk of stroke, aspirin has been shown to offer only modest effi cacy despite having a similar risk for major bleeding as warfarin,65,104
that is therefore recommended for these patients. To determine who receives which of these two drugs, much attention has been given to this risk factors for stroke in AF patients.
Factors reported to increase further the risk of stroke in patients with AF include:8,66
• Being female• Being elderly• Having previously had a stroke or TIA (mini stroke)• Having high blood pressure• Having heart failure or valvular heart disease• Having diabetes• Having vascular disease
Furthermore, the factors contribute in different ways and by different amounts to the risks of an AF patient having a stroke.
For example, a history of stroke or TIA is the strongest independent predictor of stroke in patients with AF, in-creasing the risk of another stroke approximately three-fold.8 Increasing age also has a marked effect on the risk of stroke: among patients with AF, the incidence of stroke is approximately sevenfold higher in patients in their 80s compared with those in their 40s.67 High blood pressure increases the risk of stroke approximately threefold in patients with AF.68 Vascular disease also independently increases the risk of stroke and death in AF patients.81, 194,197
Specifi cally, the development of coronary artery disease in AF patients has been found to be predictive of the formation of stroke-causing clots.203
Although stroke and AF are both more prevalent in men than in women,69,70,71 the literature shows that death rate from stroke is increased fourfold in women with AF com-pared with twofold in men with AF.105 However, it should be noted that not all studies have demonstrated such a signifi cant difference between the genders.105,72
Given that every patient is different, it is necessary for doctors to work out individual AF patient risk of stroke from all the above factors. This is called risk stratifi cation. Many approaches to evaluating individual stroke risk in AF patients have been developed. Using these, doctors can quickly assess the patient’s risk and make the neces-sary treatment decisions.
Approaches to risk stratifi cation
Several different methods are used by UK doctors when seeking to determine the risk of stroke among AF pa-tients. These all provide risk scores based upon the pres-ence of risk factors including those reviewed above.73,74
Risk calculation schemes vary by the risk factors they incorporate and in their methods of scoring and risk evaluation. Schemes in current are, usually known by their acronyms, include: AFI, SPAF, ACCP, Framingham,

The AF Report24
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875An authoritative comparison of CHADS2 and 11 other
schemes concluded that there were substantial, clinically-relevant differences between them. Most were found to have only a modest ability to predict stroke and that the proportion of patients assigned to low, moderate and high risk categories varied widely between the schemes.
For example, while CHADS2 has been found to be a more accurate predictor of stroke, in patients not on anti-coagulation treatment, than the older AFI117 and SPAF118
schemes (from which it was derived), it does not take account of several common stroke risk factors. Conse-quently, CHADS2 categorises many patients as at moder-ate risk despite evidence that many of them would derive benefi t from taking an anticoagulant instead of aspirin.116
The development and validation of CHA2DS2VASc
Because of these limitations, a further development was made called CHA2DS2VASc, to complement the CHADS2scheme. CHA2DS2VASc extends CHADS2 by consider-ing additional common risk factors and focusing on a continuum of risk as opposed to arbitrary levels of low, moderate and high risk. The risk factors and scores for CHA2DS2VASc are listed below.
CHA2CHA2CHA DS2VASc and how it’s calculated
C Congestive heart failure 1 pointH Hypertension (high blood pressure) 1 pointA2 Age greater than 74 years 2 pointD Diabetes 1 pointS2 Stroke or TIA 2 pointV Vascular disease 1 pointA Age 65-74 1 pointSc Sex (i.e. female) 1 point
CHA2DS2VASc was validated in an analysis from the Euro Heart Survey79 and in several other studies.75 76 77
The most recently published international consensus guidelines, from the European Society of Cardiology, have adopted the CHA2DS2VASc scheme and endorses use of the scheme to categorise the stroke risk among patients with a CHADS2 score lower than two, to ensure the most appropriate treatment decision is made.116
Subsequent to the publication of the ESC guidelines, CHA2DS2VASc has received further support from new data illustrating that the scheme performs better than CHADS2 in predicting patients at high risk of stroke.
CHADS2 and CHA2DS2VASc. Furthering potential for the adoption of different methods among doctors, NICE developed its own new scheme instead of adopting an existing option.
NHS Improvement GRASP-AF tool
NHS Improvement has sought to assist GPs with the adoption of risk stratifi cation among AF patients through the introduction of the GRASP-AF tool. GRASP-AF is made available free to all GPs, allowing them to analyse patient records swiftly and easily for those at risk of stroke because of AF. The tool automatically calculates CHA2DS2VASc and CHADS2 scores for all patients, iden-tifying all those in need of anticoagulation. The GRASP-AF tool automates multiple steps for GPs, it:
• Identifi es AF patients• Searches for risk factors• Calculates CHA2DS2VASc and CHADS2 scores• Searches for current medication status• Searches for reasons for not treating with an anticoagulant• Alerts GPs to those patients at risk of stroke but not receiving anticoagulation medication
Considerable advances could be made in the identifi -cation and appropriate treatment of AF patients if GPs made routine use of this free and powerful tool. More information on GRASP-AF can be found in the next chap-ter and at www.improvement.nhs.uk.
The role and limitations of CHADS2
CHADS2 is a simple algorithm that is an evolution of the AFI and SPAF risk schemes. It is based on clinical trial results and works on a simple points system:
CHADS2 and how it’s calculated
C Congestive heart failure: 1 pointH Hypertension (high blood pressure): 1 pointA Age greater than 75 years: 1 pointD Diabetes: 1 pointS2 Stroke or TIA: 2 point
From these risk factors, the acronym CHADS is derived. The ‘2’ is then added denoting that Stroke and TIA at-tract double the risk score of the other factors. The points for a particular patient are then added up allowing doc-tors to assign the patient to low, moderate or high risk and prescribe the appropriate treatment.

The AF Report 25
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875The new data also showed that patients categorised as
low risk by CHA2DS2VASc were indeed at truly low risk for stroke, unlike similarly categorised patient under other schemes.81
Having different schemes, while confusing, becomes inevitable as scientifi c understanding increases and evidence builds for one method versus another. For example, at least until the next revision of the NICE guidelines on the management of AF, many British doc-tors will be in the challenging position of having different risk assessment and treatment advice being endorsed by different authorities. As a result, patients in the UK may receive inconsistent advice and therapy, depending on local preferences.
Calculating the risk of treatment-related bleeding
Despite increasing pressure from advanced stroke risk calculation schemes and recommendations of new guidelines, many physicians hesitate to use an antico-agulant because of perceived risks of the patient suffer-ing from dangerous excessive bleeding. This perception is frequently unjustifi ed. To address this concern with bleeding risk, the authors of the ESC consensus guide-lines included an additional risk calculation scheme for bleeding among AF patients.
Using data on risk factors for major bleeding from the Euro Heart Survey as well as from a systematic review of the literature, a simple bleeding risk scheme, HAS-BLED, was derived for patients with AF:80
HAS-BLED and how it is calculated
H Hypertension 1 pointA Abnormal renal/liver function 1 point eachS Stroke 1 pointB Bleeding history/predisposition 1 pointL Labile INR (unstable warfarin impact) 1 pointE Elderly (eg, >65 years) 1 pointD Drugs/alcohol 1 point for certain drugs plus 1 for alcohol excess – max 2
HAS-BLED aims to provide a simple way to evaluate risk of bleeding in AF patients so that effective treatment decisions can be made. HAS-BLED has also been devel-oped to encourage doctors to consider reducing the risk of bleeding by focusing on correctable risks such as high blood pressure and poor warfarin control. The HAS-
BLED score has been validated in large independent groups of AF patients80,200,201 and has also been recom-mended in recent Canadian treatment guidelines,198
The new ESC guidelines state that it would seem reason-able to use the HAS-BLED score to assess bleeding risk in AF patients on the basis that a score of three or greater indicates ‘high risk’.116 In the light of growing evidence, the more recent Canadian guidelines recommend that bleeding risk is assessed using the HAS-BLED score.198

The AF Report26
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Chapter 6 - Treating AF and preventing stroke
Key points• Direct treatment of AF is frequently necessary to control distressing and intrusive symptoms; some heart rhythm treatments also reduce the risk of stroke
• It is recommended that patients receiving antiarrhythmic treatment for AF also receive therapy to reduce the risk of blood clots
• Warfarin is safe, effective and cost effective for the prevention of stroke in the majority of AF patients
• Warfarin is used less in the UK than recommended in authoritative guidelines; this under use results from practical obstacles and, frequently unfounded, safety concerns
• High blood pressure and diabetes, which commonly affect patients with AF, also require management to reduce the risk of stroke
Aims of AF management
The immediate aim of AF clinical management concen-trates on the relief of symptoms and the assessment of AF-associated long term risk.116 The greater proportion of this document is focused on the serious complications of AF, specifi cally stroke. For many patients, however, ad-dressing the symptoms of AF represents a much greater concern than preventing long-term complications. The symptoms of AF can be debilitating and unpredictable. Many AF patients report a dramatic fall in quality of life. As we have learned in previous chapters, many also suffer from a pronounced decline in mental health. At diagnosis, it is common for a patient to have endured a considerable period of time living in fear of symptoms over which they had no control and of which they had no understanding. Treatments such as ablation that achieve the desired symptomatic control by returning the heart to a normal rhythm also offer the potential benefi t of eliminating the threat of long-term complications such as heart failure and stroke.
For these reasons, it is vital that the drugs and proce-dures that treat the underlying AF are used in appropri-ate patients whenever possible.
In a considerable proportion of patients, control of the AF itself proves unsuccessful and treatment becomes entirely targeted at assessing and reducing the risk that a patient will suffer serious long-term consequences of AF, particularly stroke and heart failure.
This chapter reviews current treatments both for AF di-rectly and for managing the risk of long term complica-tions independently of the underlying AF.
Rhythm and clotting
Two treatment approaches underpin the management of AF. One is to correct the faulty heartbeat,178 and the other is to manage the risk of stroke by preventing the formation of clots in the fi brillating heart.
Rate control, rhythm control and cardioversion
Several strategies are commonly used to treat the heart-beat:
Strategies for treating a faulty heart rhythm
Rate control Slowing an excessively fast pulse with sustained drug treatment
Rate control is used to treat symptoms and to relieve stress to the cardiovascular system
Rhythm Returning the heart to a normalcontrol rhythm with sustained drug treatment
Rhythm control is achieved with antiarrhythmic drugs that reduce the fi brillation to control symptoms
Cardio- Resetting the heart rhythm suddenly, version usually with an electric current
Ablation Returning the heart to a normal rhythm permanently by surgically blocking chaotic electrical activity in the atria

The AF Report 27
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Reducing the risk of stroke
Regardless of the course chosen to address the underly-ing heart rhythm problem, AF patients almost always need additional management of stroke risk by prevent-ing clots from forming and blocking blood vessels in the brain.
AF disrupts the blood fl ow through the heart allowing the formation of a blood clot, or thrombus. Most strokes are the result of a thromboembolism which is a clot that travelled to the brain in the bloodstream. Strategies for the prevention of stroke in patients with AF primarily involve the use of anticlotting drug therapy. It is recom-mended that AF patients receiving treatment to correct their for heart rhythm also receive some form of anticlot-ting therapy.82
There are three main classes of ‘blood-thinning’ drugs currently used in the prevention of stroke in patients with AF
The main types of antithrombotic (‘blood thinning’) drugs
Anticoagulants Which interrupt the pathway of chemical reactions that result in the formation of a blood clot
Warfarin is the recommended oral anticoagulant (OAC) for stroke prevention in AF patients
Antiplatelet Which limit the aggregation of drugs platelets; components of the blood that form a signifi cant part of the blood clot
Aspirin is the most widely used antiplatelet agent for the reduction of stroke risk in AF patients
Thrombolytics Which break up blood clots once they are formed. Thrombolytics are generally reserved for use in the acute setting and do not play a role in long-term stroke prevention
Warfarin
Warfarin belongs to a class of drugs called vitamin K antagonists, (VKAs) meaning that they interfere with the normal action of vitamin K which is involved in the blood clotting process. Specifi cally, four proteins that play key roles in the blood coagulation pathway require vitamin K for their production. Warfarin inhibits the action of vita-min K, limiting the production of these four anticoagula-tion proteins.4,17 The anticoagulation pathway is a series of enzyme-controlled chemical reactions that ultimately produces fi brin, an insoluble protein that combines with platelets to form blood clots.
A narrow effective range and a need for monitoring
Despite this useful anticoagulant activity, warfarin has only a narrow range of concentration in the blood in which it is both safe and effective. Maintaining warfarin within this range is also complicated by interactions with food and other drugs18 that can signifi cantly alter blood levels of warfarin regardless of the dose taken.
If the level of warfarin is too low then the patient is not benefi ting from a reduced risk of stroke. If the level is too high, the anticoagulation properties put the patient as an increased risk of bleeding.
Thus, the management of patients on warfarin can be challenging, and frequent monitoring is required so that the dose can be adjusted to maintain effective and safe therapy. For monitoring, a measure of clotting time is taken (called the pro-thrombin time). If clotting takes too long then the dose needs to be reduced. If clotting happens too quickly, the dose of warfarin needs to be increased.
Understanding clotting time and INR
So that all pro-thrombin tests can be compared accu-rately with one another, the result of the test is converted to a ratio between the test result and a standard pro-thrombin time. This ratio is called the international nor-malised ratio (INR). Consequently, it is the INR that a physician and patient will try to keep within a target range to ensure warfarin remains at ideal levels in the blood. A target INR of 2.0 - 3.0 is typically recommend-ed for patients receiving warfarin.8,83 If the INR is too high, a patient is at increased risk of bleeding; too low, and the risk of a blood clot becomes high.

The AF Report28
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Drawbacks of warfarin are not insignifi cant and include
unpredictable interactions with food which often necessi-tate signifi cant lifestyle changes. One of the many drugs with which warfarin interacts is amiodarone, an anti-ar-rhythmic drug used in the treatment of AF.84 The incon-venience of INR monitoring and frequent dose adjust-ment also represents a burden for many patients.
Effi cacy of warfarin in clinical trials
Warfarin has been shown to be very effective at reducing stroke in AF patients. Systematic reviews of clinical trials in patients with AF have shown, compared with no therapy, that warfarin can provide a 62-68% reduction in stroke and a 26-33% reduction in the death rate85,87,88
without signifi cantly increasing the risk of major bleed-ing. This means that for every 1,000 patients treated with warfarin, 31 strokes will be prevented each year.85 Given the cost and harrowing consequences of stroke, this is an equations that strongly favours the use of warfarin.
Importantly for patients with AF, it has been shown that, when the dose is monitored and adjusted, warfarin is effective in preventing both mild and severe strokes.89,90
Warfarin in clinical practice
The practical diffi culties in maintaining the target INR, understandably raise concerns that the effi cacy and safety observed with warfarin in clinical trials might not refl ect what can be achieved in routine clinical practice.91
Clinical trials monitor patients very closely, more than might be practical or possible in routine clinical practice. Also, to meet trial design and ethical requirements, clinical trials often exclude patients at high risk of bleeding while also recruiting relatively few elderly patients.85,91
These concerns were largely refuted by observational studies that reviewed the history of large groups of patients cared for in routine clinical practice. In a large-scale study of more than 11,500 AF patients, warfarin provided a 39-60% reduction in the risk of thrombolem-bolic events (stroke and peripheral embolism) and a 31% reduction in the risk of death compared with either patients taking therapy or patients only taking aspirin.92
The risk of an intracranial bleed was almost doubled with warfarin, but still remained low with no signifi cant asso-ciation between warfarin and non-intracranial bleeding. The authors concluded that the results of clinical trials of warfarin translate well into clinical care for patients with atrial fi brillation.92
Further investigations in the clinical practice setting in Italy and the UK have demonstrated reductions in the risk of stroke of between 26-66% in patients with AF receiving warfarin compared with those not receiving warfarin.93,95
Despite an increased risk of bleeding, the overall rates of ill health and death were signifi cantly lower in the Italian patients receiving warfarin than in those not receiving warfarin.94,95 However, the risk reduction observed in the UK study (26%) was substantially lower than in clinical trials.94 Further analysis has highlighted management differences between anticoagulation clinic care and routine medical care, with patients in routine clinical care spending less time within the target INR range.94,150
While the effi cacy and safety profi les of warfarin do appear to be somewhat less favourable in routine medical practice than in clinical trials, the benefi ts outweigh the risks in the majority of patients.
Improving warfarin use with GRASP-AF
Warfarin is currently recommended in UK and European guidelines as fi rst-line therapy in patients with AF and a moderate or high risk of developing stroke.8,83 Despite evidence that following the guidelines results in improved patient outcomes,106 there is signifi cant under-use of war-farin illustrating that the guidelines are not always followed. Thus, many patients with AF and a moderate-to- high risk of stroke do not receive anticoagulant therapy and therefore remain at high risk for stroke.112,19
As introduced in the previous chapter, GRASP-AF is a tool for GPs that automates the identifi cation of patients for whom warfarin treatment should be started. GRASP-AF data, collected from use in over 1,500 English GP practices, supports the NICE statistics that only around half (55%) of those with AF at high risk are prescribed warfarin.
GRASP-AF is part of a broad NHS Improvement pro-gramme to raise awareness of AF and stroke risk, thereby reducing the number of AF-related strokes. An important element of this work is improving the management of stroke risk in patients with AF by promoting appropri-ate risk assessment, and the prescribing of appropriate anticoagulation. This is achieved through the use of the GRASP-AF tool that is free for GPs to download from the NHS Improvement web site. The GRASP-AF tool identifi es patients with AF, calculates their stroke risk, and also de-tails their current management. This information is simply summarised, allowing GPs easily to audit their current management of AF against best practice guidelines.

The AF Report 29
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875There is also a facility to upload the data to CHART,
a web-based comparative analysis tool. This enables anonymous comparison of data with other practices.
Local and regional analyses are also made possible by comparisons between Primary Care Trusts, Cardiac and Stroke Networks and Strategic Health Authorities. To date, 1,500 GP practices in England have run GRASP and uploaded their data to CHART – this growing data-base is probably the largest AF database in the world.
Illustrating the potential of warfarin to reduce stroke risk, GRASP-AF is already leading to improvements in antico-agulation and management of AF in general practice.
Cost of warfarin in stroke prevention in atrial fi brillation
In a UK study, the cost of preventing one AF-related stroke per year using warfarin was estimated to be £5,260.96 This cost of prevention appears to be favourable when compared with a European average cost of £11,799 for treating a stroke.62 In another study of patients with AF in the UK, the cost of treatment of a stroke over a 10-year period was estimated to be almost four times greater than the estimated 10-year direct costs of anticoagulation,97 further indicating that prevention is a cost effective option, regardless of the costs associated with warfarin and its challenges. Numerous other studies have provided additional evidence that anticoagulation with warfarin is cost-effective in patients with AF at a moderate or high risk of stroke when compared with no therapy or aspirin.105,99
As well as effi cacy and safety, modern health providers also have to take into account the cost-effectiveness of a treatment. This can be challenging as it necessarily puts a price on human health and life. However, done carefully, cost-effectiveness comparisons allow many different treatments to be assessed on a level playing fi eld. In the absence of unlimited funding, cost-effectiveness comparisons allow the NHS to make treatment decisions that will have the greatest benefi t for the most people.
To make these comparisons, health economists use the QALY; a quality-adjusted life-year. To illustrate, a year in perfect health is equal to a QALY of one. A year in less than perfect health would have a QALY less then one. The worse the health, the closer the QALY becomes to zero.
Treatment of AF patients with warfarin has been found to be cost effective, i.e., associated with a low cost per QALY, particularly in patients considered to be at moderate-to-high risk of stroke.99 In one study, the cost of warfarin for AF patients with one additional stroke risk factor was reported to be $8,000 per QALY saved109 well below the threshold of acceptable cost effectiveness of £20,000 - 30,000 per QALY established by NICE in the UK.100
It should be noted that the cost effectiveness of warfarin is dependent on achieving a signifi cant reduction in the risk of stroke. Practical diffi culties in maintaining target INR values may result in warfarin being less cost effective in clinical practice than in clinical trials. INR monitoring in clinical practice may also incur additional costs, to the patient, carer and society, not captured in the cost-effectiveness studies.
Thus, it is important that stroke prevention in clinical practice is improved so that it is as cost effective as in clinical trials. This might be achieved through new strategies that deliver optimal management with warfarin. It might also be achieved following technological advances, or new treatments that overcome the current challenges of warfarin.
Aspirin
One of many actions of aspirin is to reduce the activity of platelets during clotting. Limited platelet aggregation reduces the risk of a clot from forming which, in turn, helps to prevent a stroke.101
In patients with AF, aspirin reduces the risk of all strokes by approximately 22% compared with placebo. For severe, disabling strokes, the reduction in risk with aspirin compared to placebo is smaller (13%).86 Clinical trials directly comparing aspirin with warfarin in the prevention of stroke in AF have shown warfarin to be signifi cantly superior, reducing the risk of a stroke by approximately half compared with aspirin.107,129 Despite perceptions that it may be safer than warfarin, a major drawback of aspirin is that it increases the risk of bleeding, particularly in the gastrointestinal tract.65,104
Aspirin is therefore recommended only in patients with a low risk of stroke and in those who cannot take warfarin.8, 83
It should be noted, however, that there is doubt as to the benefi t of aspirin in patients at low risk of stroke.108, 98

The AF Report30
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Managing other conditions that
increase stroke risk
AF commonly co-exists with other conditions, such as high blood pressure and diabetes, which themselves can contribute to the risk of blood clots and stroke. The risk in patients with several of these conditions is cumulative that is, the more conditions that predispose to stroke, the greater the risk. Even in patients who are receiving antiarrhythmic and anticlotting therapy, effective management of these other conditions can further reduce the risk of stroke.
Blood pressure control is particularly important in the management of AF, as uncontrolled blood pressure increases the risk of stroke three-fold.68,110
AF in patients with diabetes is also associated with a very high risk of stroke. One study in patients with diabetes found that those who also had AF had a more than 60% greater risk of death from all causes than patients without AF; they also had an increased risk of death from stroke and heart failure.111
It is therefore clear that conditions which increase the risk of stroke and that co-exist with AF must be carefully managed.
The outlook for stroke prevention in patients with atrial fi brillation
To summarise, patients with AF should be managed holistically and treated with drugs or other strategies that control the abnormal heart rhythm itself, as well as with anticlotting therapy to reduce the risk of blood clots and, hence, stroke. Warfarin has been shown to reduce the risk of stroke in patients with AF in both clinical trials and clinical practice. Importantly, warfarin has proven effi cacy in reducing the risk of severe, fatal or disabling strokes. In addition, anticoagulation with warfarin has been demonstrated to be cost-effective in patients with AF and a moderate-to-high risk of stroke. Warfarin is, however, associated with major, well-recognised drawbacks. Nevertheless, it remains frontline therapy in this indication. Thus, in the immediate term, improved detection of asymptomatic AF and increased use and optimisation of warfarin therapy is important to reduce the incidence of severe strokes in patients with AF.
In the medium-to-long term, alternative therapies that combine convenience with a effi cacy and safety could help to improve further the prevention of stroke in patients with AF. The development of such treatment promise considerable improvements in the management of patients with AF. Several clinical studies of potential new treatment are ongoing and early indications are positive. New and emerging treatments and recently-published clinical trial results are discussed in more detail in the chapter “New developments for stroke prevention in patients with atrial fi brillation”.

The AF Report 31
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Chapter 7 - The importance of guidelines
Key points• Patients at moderate and high risk of stroke should receive anticoagulation therapy such as warfarin
• Aspirin is currently recommended only for patients at a low risk of stroke
• Robust evidence for the effectiveness of aspirin in AF patients is limited
• Aspirin is associated with major bleeding risks
• While two sets of guidelines are directly applicable to the UK, neither benefi ts from widespread adherence
• In the UK fewer than 55% of at-risk patients receive adequate, guideline-adherent therapy to prevent blood clots
• The drawbacks of current therapies, a lack of physician and patient education, and poor motivation of GPs to change practice, may contribute to this problem
Summary of guidelines
Data show that under-use of anticoagulant therapy in AF patients at a high risk of stroke is associated with a sig-nifi cantly greater rate of thromboembolism, while over-treatment is not associated with a signifi cantly higher risk of bleeding.112 Given this evidence, and that reviewed in the previous chapter, the importance of clinical guide-lines which advocate the use of warfarin in patients at moderate and high risk for stroke cannot be overstated.
Different recommendations in NICE 2006 and ESC 2010 guidelines
Several sets of guidelines exist for the treatment of AF and the prevention of stroke. In the UK, however, there are two guidelines that have direct relevance: those pub-lished by the National Institute for Health and Clinical Excellence (NICE) in 2006 and those published by the European Society of Cardiology (ESC) in 2010.
The ESC 2010 guidelines have replaced many earlier international publications, including those cited by NICE in its 2006 guidelines.113 However, clinical guidance from NICE has a special status in the UK; as the formal guidance that all health professional are expected to take into account when making treatment decisions.114 It is important to note that the NICE guidelines refl ect the start of the art in 2005. However, until and unless NICE updates its guidance to accommodate the more recent ESC 2010 publication, healthcare professionals in England and Wales will remain in the challenging situation of having to decide between two, occasionally confl icting, guidelines.
The clinical guidelines from NICE are based on system-atic reviews and cost-effectiveness analysis.32 This differs from the methodology of expert consensus that was used to produce the ESC 2010 guidelines, as well as most others.115
The guidelines differ in the specifi c treatment recommen-dations that they make regarding stroke prevention in patients with AF. Until the publication of the ESC 2010 guidelines, there was a general agreement between international expert consensus guidelines that patients at low risk of stroke should receive aspirin therapy, those at moderate risk should receive aspirin or oral anticoagu-lant therapy (eg, warfarin) and those at high risk should only receive therapy with warfarin. This raises therapeu-tic uncertainty for the doctor when faced with moderate risk patients; should aspirin or warfarin be given? Stroke risk classifi cation schemes that assign a high proportion of patients to moderate risk compound this therapeutic uncertainty and are less helpful.
New guidance that all ‘low’ and ‘moderate’ risk patients should be on warfarin
In contrast, the ESC 2010 guidelines recommend a risk factor approach and a reduction in emphasis on the artifi cial categories of low, moderate and high, which have been found to be poor predictors of stroke risk. The ESC guidelines recommend that those at genuinely low risk (with a CHA2DS2VASc score of zero) should receive no antithrombotic therapy or, in some cases, aspirin. For those with risk factors for stroke (ie, with a CHA2DS2VASc score of one or higher) most should receive oral anticoagulation therapy.116

The AF Report32
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Treatment implications of not using ESC 2010 guidelines
Risk of stroke NICE 2006 Guidelines ESC 2010 Guidelines Low Aspirin No antithrombotic therapy (or *aspirin) Moderate Aspirin or Warfarin Warfarin (or *aspirin) High Warfarin Warfarin
* indicates the guidelines’ preferred choice
The ESC 2010 guidelines draw upon CHA2DS2VASc, a new method of risk stratifi cation that was introduced in chapter fi ve. CHA2DS2VASc is an evolution of the stroke risk scheme developed by NICE for its 2006 guidance and is more inclusive of common stroke risk factors. One recent analysis of patient registry data (registry data can provide insights into outcomes within routine clinical practice) found that the benefi ts of oral anticoagulation therapy outweigh bleeding risks in all but those patients at genuinely low risk, ie, those with a CHA2DS2VASc score of zero.202
CHADS2 has been found to be easy to use, but still a modest predictor of stroke; similar to earlier schemes, in patients not on anticoagulation treatment.117,118 CHADS2does not take account of several common stroke risk factors, categorising many patients at moderate risk de-spite evidence than many of them would gain signifi cant benefi t from taking an anticoagulant instead of aspirin.116
Until the 2006 NICE AF guidelines are updated to re-fl ect this advance in understanding of stroke risk, many patients will continue to receive aspirin when they could derive a signifi cantly increased reduction in stroke risk, with no additional risk of major bleeding, if they were to take warfarin instead.
Guidelines: theory versus practice
Regardless of the difference between these two authori-tive guidelines, neither is uniformly followed and warfarin treatment remains underused in the UK. Even NICE’s own data shows that of all those with AF who should be on warfarin, almost half are not.119
This is not just a UK problem; in a study conducted in seven European countries, it was found that only 8.4% of patients with AF who had a stroke were receiving anti-coagulants at the time of their stroke, and the propor-tion decreased by 4% per year with increasing age.5 A review of the scientifi c literature from 2000 indicated that only 15–44% of eligible patients with AF were receiving warfarin.23
Yet, when asked, physicians demonstrate both awareness of the guidelines and agreement with them. For exam-ple, a questionnaire was used to examine the adher-ence of Swedish physicians to European and national guidelines.19 Of 498 physicians who responded, more than 94% stated that patients at risk of blood clots with chronic AF should receive long-term anticoagulation therapy. The investigators also evaluated the records of 200 patients hospitalised for AF to check whether or not treatment matched the answers to the questionnaire. In total, 108 patients had chronic AF with one or more risk factor for stroke, and no other reason not to take to war-farin, but only 40% of these patients received warfarin.19 This study further highlights the discrepancy that is often found between guidelines and what happens in clinical practice.
Another study documented the medications being taken by AF patients when they suffered an ischaemic stroke. It found that only 10% of these patients had been taking an effective dose of an anticoagulant. Nearly a third were on no antithrombotic treatment at all (29%). A further 29% were on aspirin and another 29% were on a non-therapeutic dose of warfarin.
Not all studies into the use of warfarin in AF patients provide evidence of under-use.121,143 According to recent surveys in different parts of Europe, the proportion of patients with AF at high risk of stroke who are receiving adequate anticoagulation is most commonly around 54–61%,122,112 but this fi gure is as high as 88% in settings where guidelines are being more successfully applied in the real world.123,124
Reasons for poor adherence to guidelines
Adherence to guidelines for the prevention of stroke in patients with AF may be low for several reasons. These include diffi culties in maintaining INR within the thera-peutic range18 and physicians’ concerns about bleeding risk, particularly in the elderly.125 This section reviews some of these challenges, and also examines the way in which the Department of Health rewards GPs for reach-ing targets, and how that might contribute to poor adher-ence to guidelines in the UK.

The AF Report 33
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875The motivation of general practitioners
When the payment of UK general practitioners was reviewed in 2004, a new scheme was introduced called the Quality Outcomes Framework (QOF).126 QOF was designed to reward GPs for the quality of the care that they provided, instead of for how many patients they treated. The scheme also provided additional resources that could help GPs implement new services to address local needs. Currently, GPs can work to secure up to 1,000 QOF points by meeting predetermined performance targets in four broad areas: Clinical, Organisational, Patient Experience and Additional Services. A total haul of 1,000 points represents an additional payment to GPs of over £13,000.
Specifi cally for AF, within the current QOF scheme, up to 12 points are available for GPs achieving a high per-centage of…
‘… patients with atrial fi brillation who are currently treated with anticoagulation drug therapy or antiplatelet therapy.’126
It is reasonable to expect that many patients diagnosed with AF will already be taking aspirin for another condi-tion. It is also relatively simple to start and manage a patient on aspirin (antiplatelet therapy) compared to war-farin (anticoagulation therapy). Consequently, the way the target is written enables GPs to receive the maximum QOF reward just by having AF patients on aspirin, even if none of them is on warfarin.
Consequently, QOF today provides virtually no motiva-tion for GPs to put patients on warfarin in accordance with the NICE 2006 or the ESC 2010 guidelines.The QOF target described above is, within the scheme, called an indicator. In March of 2011, NICE opened a consultation on proposed revisions to the QOF in-dicators for AF. Encouragingly, the proposed revisions represent the possibility that GPs might become more effectively motivated to adhere to guidelines.128 Specifi -cally, two new indicators were submitted for consultation. If these new indicators are adopted, GPs will receive QOF rewards dependent upon:
• The percentage of patients with Atrial Fibrillation in whom stroke risk has been assessed using the CHADS2 risk stratifi cation scoring system in the previous 15 months
• In those patients with Atrial Fibrillation in whom there is a record of a CHADS2 score of less than one, the percentage of patients who are receiving anticoagulants
Both of these proposals are to be welcomed by those seeking better adherence to clinical guidelines and more effective treatment of UK patients at risk of stroke be-cause of AF. Moreover, the second of the two proposed new indicators specifi cally addresses the failing of the current QOF indicator to provide GPs with motivation to prescribe anticoagulation therapy.
The proposed QOF reward for prescribing an antico-agulant in patients at moderate or high risk appears refl ective of the ESC 2010 guidelines and perhaps demonstrates that UK policy makers are keen to accom-modate the recommendations of the new ESC guidelines even before there is opportunity to accommodate them in revised NICE guidelines.
Diffi culties of keeping warfarin within the thera-peutic range
Many patients fi nd the frequent monitoring and necessary dose adjustments associated with warfarin inconvenient and time consuming, and may miss appointments. Re-search has shown that AF patients in routine clinical care were able to maintain a target INR for over half the time (56%). Of the considerable remaining time, patients were above the target range for 30%, and below the target range for 14%.143
This has unsettling implications. If around half of all patients in need of anticoagulation aren’t prescribed warfarin119 and if those who are have either ineffective or unsafe blood levels of warfarin for nearly half of the time,143 then perhaps only a quarter of patients at any one time is receiving the therapy they need to safely lower their risk of stroke.
This becomes ever more worrisome when remembering experts’ estimates that only about half of all AF patients are actually diagnosed. The vast majority of these undi-agnosed patients would be expected to be at moderate or high risk of stroke,127 and, hence, in need of warfarin therapy according to the ESC 2010 guidelines. As illus-trated in the table below, perhaps only a fi fth of patients in need of warfarin to reduce risk of stroke actually receiving safe and effective anticoagulation treatment at any time.

The AF Report34
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Very few warfarin patients receive effective and safe
treatment
Percentage Of every 100 AF patientsAF patients diagnosed c.60% 60
AF patients at moderate 97%127 58 or high risk
Number anticoagulated 54%119 31
Number in INR range 56%143 18
Even if the estimated for the number diagnosed is in-correct and, for example, only 30% of AF patients are undiagnosed, the estimate for the number of patients receiving safe and effective anticoagulation would rise only to 21%.
When patients do not receive close monitoring, which is not usually available in routine clinical practice, they have been found to be outside the target INR range for longer than when strict monitoring is imposed upon them.142 Clearly patients are facing challenges with their therapy when not under close supervision, and are therefore put at increased risk of a potentially-dangerous blood clot or of uncontrolled bleeding.
Physician concerns about bleeding risk
Many physicians resist the use of warfarin in the elderly, largely on grounds of safety. The evidence, however, strongly favours the use of warfarin in older patients. The incidence of stroke among patients aged 75 years or more with AF is lower in those who are receiving war-farin than in those taking aspirin, without increasing the risk of haemorrhage.129
Despite this, research has demonstrated repeatedly that many physicians over-estimate the risk of bleeding associated with the use of warfarin and under-estimate its benefi ts in preventing thromboembolism and stroke; conversely, they have been shown to under-estimate the bleeding risk of aspirin therapy and over-estimate its benefi ts.20,125,21 As a result, eligible patients are not receiving therapy that could prevent strokes.16 For many physicians, bleeding risk is a particular concern in the elderly, who are more prone to falls, more likely to have suffered previous major bleeds and who are subject to
many additional problematic factors associated with old age.132,134 However, evidence has shown that none of these factors, not previous bleeds, falls or old age itself has any impact on increased risk of bleeding associated with warfarin.
While the bleeding risk with warfarin is no worse than that with aspirin, especially in the elderly, physician experience of major bleeding events associated with warfarin can profoundly reduce prescription of warfa-rin.135 A study investigated the behaviour of physicians treating AF patients who had bleeds while on warfarin. Patients treated in the 90 days after the physician had encountered a bleeding event were signifi cantly less likely to receive a prescription for warfarin than patients treated before the bleed.135 In contrast, having a patient who experienced a stroke while not receiving warfarin did not infl uence prescribing behaviour with subsequent patients.135
In other words, a bleeding event may make a physician less likely to prescribe an anticoagulant but a stroke does not increase the likelihood that a physician will prescribe and anticoagulant.
Two theories have been put forward to explain this phe-nomenon. The fi rst is based upon a theory that when we predict the probability of an event, we are infl uenced by the ease with which those events can be remembered. Since a major bleed is likely to be memorable, this might create a perception among physicians that bleeds are more likely than is actually the case.136 A second theory suggests that when making choices, we tend to select the one we will least regret.137 It is arguable that a decision to add to bleeding risk by making a change (prescribing warfarin) is less appealing than a decision to add to stroke risk by doing nothing. This may also be in keeping with a principle of the Hippocratic oath, to ‘do no harm’.135 While of interest, there is no evidence that an understanding of these two possible infl uences on prescribing behaviour has any impact on the number patients who remain at high risk of stroke despite strong evidence that warfarin would reduce that risk without a prohibitive risk in bleeding.
Discrepancies between patients’ and physicians’ perceptions of stroke and bleeding risk
Much of proposed future NHS policy is founded on a desire to engage patients in the path of treatment recom-mended to them, giving them both choice and control. This is neatly captured in the line, ‘no decision about me, without me’.

The AF Report 35
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875A study that compared patients’ and physicians’ percep-
tions of risk illustrates how such a shift toward patient-centred care might infl uence the prevention of stroke in AF patients.
A group of physicians, and another of patients at high risk of stroke, were asked the same set of questions about when anticoagulation therapy was justifi ed accord-ing to the reduction in stroke risk. Following in-depth explanation of the bleeding risks involved, 74% of the patients were willing to take warfarin if prevented just one stroke in 100 patients over two years. Yet, when confronted with the same question, only 38% of physi-cians were willing to prescribe warfarin for the same risk reduction.138 This result suggests that if patients were suffi ciently informed about, and then involved in, treatment decisions, many more of them would receive stroke-preventing anticoagulation therapy than if just left to the doctors.
The same study also asked questions about the number of bleeds that were acceptable with warfarin and aspirin, having fi rst explained the stroke risk reduction with which each treatment is associated. Of the physicians, 46% were willing to accept more than ten bleeds in 100 patients treated with warfarin over two years. In stark contrast, the patients were much more willing accept bleeds on warfarin given the stroke risk reduction pos-sible. Of the patients, 85% were willing to accept more than ten bleeds in 100 patients over two years.
The study also suggested that physicians perceive the risk of bleeding to be higher with warfarin than with aspirin, perception that we know is not supported by the clinical evidence.129
These results indicate that patients place more value than physicians do on the avoidance of stroke, and less value on the avoidance of bleeding.138 For the effective prevention of strokes, it appears important that the views of the individual patient are taken into account when as-sessing whether to use anticoagulant therapy.
To summarise, adherence to guidelines for the prevention of stroke in patients with AF is often poor. The reasons for this appear to be related primarily to the drawbacks associated with warfarin therapy and to a lack of physi-cian and patient education regarding the benefi t-to-risk ratio of therapy. There is also a clear need for a change in the way that UK GPs are rewarded for treating AF patients. The current system fails to provide motivation to follow guidelines. The proposed change to this system is to be welcomed, as is the indication that UK policy makers appear to endorse elements of the most recent international guidelines from the ESC.

The AF Report36
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Chapter 8 - Current challenges
Key pointsIf the prevention of a silent epidemic of AF-related stroke is to be prevented, it is vital that we address the following barriers to reduced stroke risk:
• Insuffi cient detection and diagnosis strategies
• Low patient awareness and understanding
• Limitations of current treatments
• Incomplete knowledge among healthcare professionals
• Inequity of patient access to effective management
• Insuffi cient communication to ensure a continuum of care for patients
• Guideline differences and low guideline adherence
As has been discussed at length in this report, there are many and varied obstacles to the effective prevention of stroke in AF patients. This chapter identifi es and summa-rises seven major challenges to effective stroke preven-tion among AF patients, as captured above in the key points.
Insuffi cient detection and diagnosis
Without effective detection and diagnosis of AF between a third and a half of patients affected will only be iden-tifi ed once it is too late; having suffered a potentially debilitating or lethal stroke. If a lack of detection and di-agnosis continues, then many patients will be denied the opportunity to benefi t from treatments that can dramati-cally reduce their risk of stroke.
Strategies are urgently needed to improve detection and diagnosis of AF. Existing research suggests that routine pulse screening has a role to play,139 as does public education on the need to investigate an irregular pulse. Any solution will need to involve promoting pulse checks among the general public, and the importance of having an irregular pulse investigated. The role and value of screening programmes will need serious review, espe-cially following the positive results of the SAFE study.139
Many pieces are already in place; NICE already recom-mends that all patients with an irregular pulse receive an
ECG to make a diagnosis and the SAFE study uncovered the marginal additional costs of taking a manual pulse.
The SAFE study also found that GP and practice nurse performance in interpreting ECGs was not encouraging,139
identifying another potential challenge to the effective diagnosis of AF in primary care.
Low patient awareness and under-standing
Wider access to information
Many patients have poor understanding of AF and of the treatments they take because of it. We know from one study that 37% of documented chronic AF patients were unaware that they had AF and nearly half didn’t know why they were taking warfarin. A similar number didn’t know they were at risk of clots that could cause stroke. Sixty percent felt that their underlying condition (AF) was not severe.140
These fi ndings are backed up be other sources including surveys of patients from patient advocacy organisations and from qualitative research among patients.
An extensive international survey conducted by the patient organisation, AntiCoagulation Europe (ACE), revealed that a quarter of the surveyed patients did not remember receiving any information on AF at diagnosis, and over one-third felt that their doctor could have told them more regarding their medication and how it would affect their lives. Particular lack of awareness among pa-tients was noted with regard to the potential interactions of warfarin with common over-the-counter medicines and herbal remedies.141
From a qualitative study of AF patients’ experiences it is clear that the above fi ndings should not have been surprising. The study reported common and disturb-ing patient experiences during particular phases of the pathway of care. All patients involved in the research had AF which was both recurrent and symptomatic. Before being diagnosed, patients reported confusion and fear of symptoms, and were often puzzled during a search to understand what they meant. Patients reported that fre-

The AF Report 37
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875quently no explanation of symptoms was given by health-
care professionals, and that symptoms were dismissed as ‘panic attacks’.
At diagnosis, patients reported relief, hope for the future and validation of their search for understanding of the symptoms. However, the time of diagnosis was also as-sociated with many less positive experiences with health-care professionals:
• Lack of information and support from healthcare professionals
• No education of the course of AF, or information on what to expect in the future
• No acknowledgement of the negative impact that symptoms were having on patients’ lives
• Inadequate education on how to manage symptoms
Following the initiation of management, a new range of negative patient experiences were reported. The unpre-dictable recurrence of symptoms was associated with distress, anxiety and a loss of control. Recurrent symp-toms were commonly associated with a perception of treatment failure and accompanied by a fear of suffering a debilitating stroke.
So not only are patients are not receiving or retaining information during consultations with their doctors, there is also evidence that AF patients feel abandoned, dis-missed, without support and without understanding at the hands of the healthcare professionals charged with the care of their AF.28
Better adherence to therapy
According to AntiCoagulation Europe, adherence to therapy is strongly dependent upon patients’ understand-ing of their condition. Without the proper information or guidance, adherence can be poor, leaving patients at risk of bleeding or stroke. This report is supported by data showing that adherence to warfarin therapy increas-es when patients are supervised and have easy access to professional support.142
We know that AF patients in routine clinical care were able to maintain a target INR for over half the time (56%). Of the considerable remaining time, patients were above the target range for 30%, and below the target range for 14%.143
Insights into these research fi ndings were uncovered by the ACE patients survey. It was found that, while nearly three-quarters of patients knew their target INR, over a
third believed that being outside the target range had no major effect on their health. Only 30% of patients had been in their target INR range in all of their last 5–10 monitoring sessions, and 7% had not been in their target INR range in any of their last 5–10 sessions.141
Greater patient empowerment
Patient empowerment is associated with improved clini-cal outcomes,144 and has been made central to the cur-rent focus of the NHS. For a patient to be empowered, it is necessary that he or she has suffi cient knowledge to be actively engaged in treatment decisions, in the setting of treatment goals and in evaluating the outcomes. Spe-cifi c to the stroke prevention efforts required in AF, patient education and involvement in the management of warfa-rin therapy have been shown to reduce the risk of major bleeding.145 Patients cannot become empowered without access to information which needs to be accurate, con-sistent and easy to understand. Limits on the accessibility should also be removed wherever possible by addressing different levels of literacy, by not relying on a single for-mat (e.g., print or internet) and by making the information available in appropriate languages.
Barriers to patient empowerment extend far beyond the accessibility of information; they include factors such as time pressure on healthcare professionals, their misper-ceptions of patient needs and poor continuity of care between healthcare professionals.
Limitations of current treatments
The limitations of current treatments represent a signifi -cant challenge to the effective reduction of stroke risk in AF patients. Among the group of patients who are diagnosed, and who would benefi t from warfarin, nearly half don’t receive it.119 And that those taking warfarin, are only benefi ting from reduced stroke risk, with no in-crease in bleeding risk, for about half the time.143 As we have see in earlier sections, there are many drawbacks with warfarin and almost all of these can be traced back to the narrow therapeutic range and the ease with which lifestyle choices, foods and other drugs can push blood levels outside of that range.
There is clearly a need for new therapies that treat AF, prevent blood clots and prevent AF-stroke without the in-convenience and disadvantages of warfarin and aspirin. Understandably, AF patients currently taking anticlotting therapy are all to aware of this need. When surveyed, 68% of chronic AF patients expressed their interest in new anticoagulation drugs for which routine monitoring was not needed.151

The AF Report38
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Progress in this area of new therapies is discussed in
more detail in the earlier section but new anticoagulant drugs are in development. Available clinical data sug-gests that some of these new drugs might match the stroke risk reduction of warfarin while being convenient, having more predictable effects and a better safety profi le. These agents they have the potential to increase adherence to therapy and to guidelines, and most im-portantly to the number of AF patients at reduced risk of stroke.
Incomplete knowledge among health-care professionals
The importance of patient empowerment has been stressed already. Unless healthcare professionals are equipped with a high knowledge of AF-patient manage-ment, it will remain almost impossible to engage pa-tients in decision making and target setting for their own management.
Benefi ts of current treatments to prevent stroke
The reasons for poor adherence to guidelines have been reviewed in earlier sections. Many of these reasons are rooted in the degree of understanding and concern that physicians have about the safety and effectiveness of warfarin. We have seen that doctors both underestimate the benefi ts of warfarin and over estimate the risks. There is also evidence that the safety of aspirin and effective-ness is overestimated by prescribers. This highlights an urgent need for improved awareness and understanding among physicians of the existing antithrombotic treat-ments and their essential role in the prevention of stroke among AF patients.
The barriers of low awareness and knowledge among healthcare professionals is also evident from survey data. Physicians have reported that increased training and availability of consultant advice or guidelines specifi cally on managing anticoagulation therapy would increase their willingness to prescribe warfarin.153
Evidence also suggests that healthcare professionals need greater awareness of their patients’ ability to retain information at the point of diagnosis, as well as greater insight into the negative effects that the symptoms of AF have on patients’ lives.
Provision of information
There is a large amount of information for patients to absorb in one consultation with the physician. Physicians
need to understand the enormous value of supplying written information covering critical advice and facts, and that this is vital to ensure patient understanding and engagement. Physicians also need to revisit this informa-tion in subsequent consultations to confi rm and reinforce patient understanding so that patients can become involved in the making of informed decisions about their care.
Physicians need also to recognised the negative impact that symptoms are having on patients lives. Failure to do this results in a feeling of abandonment and dismissal, which will likely undermine efforts to educate and en-gage the patient in the management of AF, achieving the opposite of patient empowerment.
Finally, efforts are required to ensure that always patients receive consistent and accurate information and advice that is uniformly specifi c to individual circumstances. This is only possible if there is effective communication between the various healthcare professionals involved in the patient’s care.
Management of patients receiving warfarin
There is evidence to suggest that patients adhere to warfarin therapy more closely when closely supervised or routinely managed by a dedicated anticoagulation service.152 However, there are great differences between the many dedicated anticoagulation services provided throughout the UK, but a distinct lack of information on the effectiveness, quality and range of services that they provide. Physicians need to become aware of the strengths and limitations of their local anticoagulation clinic, and remain mindful of alternatives such as home testing. The roles of self-management and anticoagula-tion clinics is covered more closely at the end of this chapter under Access to care and information.
Awareness of treatment innovations
Novel anticoagulants currently in advanced stages of development may simplify the management of patients with AF. As with any chronic intervention, however, high-quality guidance and education for doctors, patients and their carers will be essential. Healthcare professionals will need to identify and manage eligible patients and know how to deal with emergency situations. Increased resources for education and rapid dissemination of infor-mation will allow faster introduction and uptake of new therapies.

The AF Report 39
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Inequity of access to effective
management
There is a considerable body of evidence that supports the accuracy and reliability of self-testing.146,147,148,149
There is also high-level endorsement of home testing from NICE which recommends that it is considered in all AF patients in need of long-term anticoagulation, if they would prefer self-management. The Department of Health has committed to help fund home testing and self-management is very much in line with government strategy promoting patient choice and patient empower-ment.
However, there are major disincentives for patients to self-manage their warfarin treatment in the UK. The test-ing machines are not available on the NHS, preventing their use among many patients who would benefi t from a high degree of involvement with their own treatment. Furthermore, while the Department of Health has com-mitted to funding the testing strips that the machines use, many Primary Care Trusts (PCTs) are not currently funding the strips in line with this commitment. The result is that the cost falls to patients who should not have to face this fi nancial burden. Many patients simply can not afford the strips and become failed by the system responsible for their care. This situation also creates imbalance and ‘postcode prescribing’ where patients in one part of the country are denied access to a therapy which is provided routinely elsewhere.
There is need not only for agreed standards of care and service from anticoagulation services, there is also need for much greater consideration and support of home testing for those patients likely to benefi t. When the risks and benefi ts of home testing are properly explained to patients, nearly all (94%) fi nd the option to be accepta-ble.147 In a study that investigated the role of self-testing, 87% of patients reported that they felt it to be straight-forward and that they were confi dent with the results they obtained. Research from outside the UK has also indi-cated that cost benefi ts might also be possible with home testing.155
In further support of home testing and patient empower-ment, there is general agreement among both primary care physicians and specialists that anticoagulation therapy is best managed by general practitioners, rather than hospital doctors to ensure optimal access to, and continuity, of care.153
Anticoagulation clinics – a potential educational resource
Anticoagulation clinics may be run from a hospital or at-tached to a primary care practice. They have sometimes
been considered the gold standard of warfarin manage-ment152 helping to increase the time that a patient’s INR values are within the target range, improve the overall cost-effectiveness of therapy, increase patient adherence and provide valuable information for both healthcare professionals and patients.150,154 However, information of the quality and range of services of these clinics in the UK is poor. When the effectiveness of dedicated clin-ics is compared with home-monitoring, the results are positive for self-testing. 149 Self-testing also avoids much of the time and fi nancial commitment required to make frequent journeys to the clinic, and it frees patients from feeling a need to remain close to their clinic at all times. This can interfere considerably with daily life as patients avoid travel and holidays because of such fears.
If patients are referred to an anticoagulation clinic, communication between all the healthcare professionals involved is crucial: assigning one part of patient care to an external clinic can weaken the relationship between the primary care physician and patient and may lead to disruption of care if communication breaks down.152
Therefore, healthcare providers may need education and support in ensuring a seamless transition between the different strands in the patient pathway. As management of patients receiving anticoagulants evolves, anticoagu-lation clinics will need to adapt.152 The organisation and running of anticoagulation clinics might gain cost and effi ciency benefi ts through the adoption of technology. Computer programs to calculate the required dose ad-justment of warfarin have been found to perform just as well as clinic staff.157,158 Anticoagulation clinic staff may have an increasing role as educators and coordinators of anticoagulation therapy, providing support and commu-nications links for other healthcare providers.
Moves towards patient-centred care
Access to, and the quality of, management of patients with AF is also likely to be greatly improved by a move to more patient-centred care and patient empowerment. Under current Department of Health policies, the con-sideration of patients’ needs, preferences and concerns relating to overall health, rather than just to a specifi c condition will become increasingly important. Although a patient-centred approach is widely advocated, it is not always implemented.159 Instead, health care is typically centred on treating the disorder, rather than consider-ing patients’ individual needs.159,160 There is evidence that anticlotting therapy tailored to patients’ preferences is more cost-effective than giving the same therapy to every patient. 109 There is therefore a need to provide physicians with further education on the benefi ts of pa-tient-centred care and with support in implementing this approach locally.

The AF Report40
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875Interruptions in the continuum of
patient care
Continuity of care, involving timely communication be-tween healthcare providers, is essential for high-quality care. As the provision of health care often involves sever-al different service providers, continuity of care is defi ned as ‘coherent health care with a seamless transition over time between various providers in different settings’.162
By empowering patients and adopting a patient-centred approach to management, many factors that interrupt the continuum of care can be identifi ed and eliminated.
Clinical research supports the need for an optimised continuum of care. In one paper, the defi ning character-istics of an ideal continuum were established; the seven Cs) of optimal continuity of care.162
• Regular contact between patients and healthcare providers.
• Collaboration between healthcare professionals and patients in educating and ‘empowering’ the patient.
• Communication between healthcare providers.
• Coordination of the multidisciplinary teams involved, with clear identifi cation of different roles.
• Contingency plans in the form of access to healthcare professionals out of hours to answer questions and address concerns.
• Convenience – achieved, for example, by avoiding the need for patients to keep repeating information and by considering home monitoring.
• Consistency of the advice provided by different professionals and adherence to clinical practice Guidelines.
The close monitoring required in patients receiving war-farin therapy can be problematic in ensuring continuity of care. When patients are transferred to other healthcare providers or to different settings, such as during hospi-talisation or at discharge from hospital, critical informa-tion can be lost. Comprehensive, timely and appropriate discharge information is essential – possibly in some portable format 163 – so that the primary care practice has all it needs for appropriate follow-up care. Insuf-fi cient discharge information can contribute to hospital readmission.164 Education of carers also plays a key role in the success of therapy, and the availability of a health-care provider to answer questions and address concerns is likely to improve continuity of care.
Confl icting guidelines and GP targets
When guidelines provide confl icting information or when outcomes rewards fail to motivate treatment in accord-ance with guidelines, there is signifi cant opportunity for patient management that falls short of what is ideal. In the UK, healthcare providers have a choice of two con-fl icting sets of authoritative guidelines; those from NICE and those from ESC.
It is essential that the planned review of the existing NICE 2006 guidelines are updated to refl ect not only the exist-ing ESC guidelines, but also to refl ect improvements that the authors of the ESC guidelines are already consider-ing.
It is also necessary to change the current QOF scheme that rewards physicians for achieving targeted patient outcomes. In the previous chapter, this topic was ad-dressed in more detail, but the current scheme provides virtually no motivation for GPs to put patients on war-farin in accordance with either the NICE 2006 or the ESC 2010 guidelines. Proposed changes to this scheme would help eliminate this barrier to effective AF patient management.
Summary of current challenges
In summary, numerous challenges remain in the preven-tion of stroke in patients with AF. Increased detection of AF by physicians is vital, and improved education is needed among patients and healthcare professionals on the benefi t-to-risk profi le of aspirin and warfarin, and on the optimum management of patients receiving warfa-rin. Healthcare professionals need to be aware of new anticoagulants and other therapeutic strategies that are emerging, as well as advances in the treatment of the un-derlying AF. It is also vitally important to encourage pa-tient empowerment and patient-centred care and ensure equity of access to advances such as self-management. Finally, improved adherence to guidelines, consistent recommendations between guidelines and collaborative approaches to the development of revised guidelines are essential, as are revisions to schemes that exist to moti-vate GP to achieve outcome targets among AF patients. All of these factors will contribute to the prevention of stroke in patients with AF.

The AF Report 41
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
Chapter 9 - New treatments in development
Key points• Practical and perceived drawbacks of warfarin are limiting its potential to prevent stroke
• alternative anticoagulants in development aim to offer effi cacy, safety and convenience, without need for monitoring or dose adjustment
• Three oral anticoagulants are in the fi nal stages of development for the prevention of stroke in AF
• Promising minimally-invasive procedures have also been developed for correcting abnormal heart rhythms and eliminating the source of AF-related blood clots
Limitations of warfarin and aspirin restrict their use and effectiveness in the prevention of stroke in patients with AF. These limitations have led to an ongoing search for alternative effective and convenient therapies. In addi-tion, there have been developments in anti-arrhythmic drugs used to treat AF. These developments are dis-cussed in more detail below.
Anticoagulant agents
There are many challenges involved in the effective use of current anticoagulants to prevent stroke. Taken together, they point clearly to what might be the ideal characteristics of an anticoagulant for long-term use in AF.165
• As effective as warfarin
• A large therapeutic window (a wide separation between blood levels that reduce the risk of a blood clot and those that substantially increase the risk of bleeding)
• A good safety profi le in a wide range of patients, including the elderly
• A low tendency to interact with food and other drugs
• No need for regular monitoring and dose adjustment
• Easy and simple to take (i.e., by mouth in pill or capsule form on daily basis)
Warfarin can be very effective, is relatively simple to take, and is somewhat safer than many physicians appear to believe, but it does not fulfi l the remaining criteria for an ideal anticoagulant. Warfarin interacts with food and other drugs in a way that can lead to blood levels far outside a very narrow therapeutic window. Consequently, warfarin requires frequent monitoring and dose adjust-ments. When monitoring and adjustment are lax, both the effectiveness and safety of warfarin are compromised.
Understandably, there has been a long search for alter-native anticoagulants. The clotting process is a compli-cated cascade of biological reactions providing many potential targets for a new drug. Yet it has taken decades of research to uncover new compounds that are effec-tive in tackling some of these targets. The agents that are most advanced in their development act on single proteins in the coagulation pathway; either clotting factor Xa (pronounced ‘ten A’) which is involved in the ampli-fi cation of the clotting response, or on thrombin which enables the fi nal step of the clotting process to take place.165 Today, development of a handful of new oral anticoagulants has advanced to human trials in large numbers of patients.
The below table summarises the new anticoagulation agents which have fi led, or which plan imminently to fi le, applications for European regulatory approval. These and other agents in the fi nal stage of development are discussed below.

The AF Report42
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875New anticoagulant agents offer potential alternative to warfarin in some patientsc
Agent Commercial Name Class Current indications Status of AF indication
Rivaroxaban Xarelto Direct factor Xa inhibitor VTEa Licensed Dec-2011 AFb
Apixaban Eliquis Direct factor Xa inhibitor VTEa Filed 2011
Dabigatran Pradaxa Direct thrombin inhibitor VTEa Licensed 2011 AFb
a The prevention of venous thromboembolism in adults after hip or knee replacementb To prevent strokes and the formation of clots in adults who have an abnormal heart beat called ‘non-valvular atrial fi brillation’ and are considered to be at risk of strokec Accurate at Feb 2012
Oral factor Xa inhibitors
Clotting factor Xa has few functions in the body outside coagulation, making it an excellent target for potential new anticoagulants as this may result in fewer side ef-fects.166 Inhibition of factor Xa inhibits thrombin genera-tion, while allowing existing thrombin to continue its vital role in blood clotting.166 Oral inhibitors of factor Xa in late-stage development include rivaroxaban, apixaban and edoxaban. Two factor Xa inhibitors are currently licensed in the UK by the Medicines and Healthcare products Regulatory Agency (MHRA); rivaroxaban,170 and apixaban.167 Both are available Europe-wide following authorisation from the European Medicines Agency. Both agents are available for the prevention of clotting prob-lems in the veins in adults after hip or knee replacement surgery. For this indication, called venous thromboem-bolism (VTE), rivaroxaban is taken orally, once daily at a fi xed dose; apixaban is taken orally, twice daily at a fi xed dose.
Unlike warfarin, rivaroxaban and apixaban have a wide therapeutic window and do not require routine monitor-ing. The manufactures of rivaroxaban have also now submitted additional indications for licence, including stroke prevention in patients with AF and the treatment of deep vein thrombosis. The manufacturers of apixaban have announced plans to make regulatory fi lings in 2011 for stroke prevention in AF patients.
Rivaroxaban
The pivotal clinical study of rivaroxaban is called ROCKET AF.168,169 The results of the study showed that AF patients taking rivaroxaban had a comparable risk of stroke and a similar risk of bleeding compared to patients taking warfarin.169
ROCKET-AF was a randomised, double-blind study that compared the effi cacy and safety of rivaroxaban 20 mg once daily with warfarin for the prevention of stroke in approximately 14,000 high-stroke-risk patients with AF.168,169
Apixaban
Two pivotal studies of apixaban have recently released results. The AVERROES study compared apixaban with aspirin in 5,599 AF patients who were unable to take warfarin. The study was stopped early having demon-strated clearly that apixaban was associated with a sig-nifi cant reduction in strokes when compared with aspirin. A second pivotal trial, ARISTOTLE, compared apixaban with warfarin in over 18,000 AF patients. Results from this trial show that apixaban was superior to warfarin in preventing stroke or systemic embolism, caused less bleeding, and resulted in lower mortality.
Edoxaban
Pivotal studies of edoxaban have yet to complete but earlier trials indicated that AF patients taking edoxaban had a similar incidence of bleeding to those assigned to warfarin.172 A pivotal phase III study (ENGAGE- AF TIMI 48) is underway to demonstrate the safety and effi cacy profi le of different edoxaban doses compared to warfarin.171
Indirect factor Xa inhibitors
Another group of factor Xa inhibitors are under investiga-tion. These agents, instead of acting directly, limit the ac-tivity of factor Xa via antithrombin. Among these indirect factor Xa inhibitors, biotinylated idraparinux is the most studied and the only example to have been involved in a late-stage clinical study. Unlike the direct Factor Xa

The AF Report 43
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875inhibitors above, biotinylated idraparinux is administered
by subcutaneous injection.165 A study called BOREALIS-AF was evaluating whether subcutaneous biotinylated idraparinux administered once a week was at least as ef-fective as warfarin for the prevention of stroke in patients with AF.171 However, the trial was halted by the sponsor. This is the second trial of biotinylated idraparinux to have been stopped early. However, unlike a predecessor BO-REALIS-AF was not stopped because of a safety concern. This earlier trial, which used a different formulation of the drug, was stopped as a result of bleeding concerns.
Thrombin inhibitors
Dabigatran
Dabigatran etexilate directly inhibits the action of thrombin, blocking the fi nal step of the clotting cascade which converts fi brinogen to fi brin. Similar to apixaban and rivaroxaban, throughout Europe dabigatran has been approved for the prevention of VTE in adults after total hip replacement or total knee replacement sur-gery.173 The pivotal, late-stage clinical study of dabigat-ran is called RE-LY, which compared the effi cacy and safety of dabigatran with warfarin in 18,113 AF patients. RE-LY compared two doses of dabigatran, taken orally, twice daily, to warfarin. The lower dose was associated with a stroke rate comparable to that seen with warfarin, but with a lower rate of major bleeds. The higher dose resulted in a signifi cantly lower rate of stroke compared to warfarin and a similar rate of major bleeds.174 Further studies of dabigatran and other direct thrombin inhibitors are ongoing.176,55
Antiplatelet agents
Clopidogrel is an inhibitor of platelet aggregation. Re-duced platelet aggregation reduces the risk of a blood clot forming. In a study called ACTIVE-A, clopidogrel in combination with aspirin was compared to aspirin alone for the prevention of stroke in AF patients for whom warfarin therapy was unsuitable. While clopidogrel in combination with aspirin signifi cantly reduced the risk of stroke in patients with AF, it was also associated with a signifi cantly greater rate of major bleeding.177
Additional studies are under way to assess the effi cacy and safety of clopidogrel for stroke prevention in patients with AF.171 Clopidogrel is currently licensed for other indications including the prevention of atherothrombotic events in patients suffering from heart attack.185
Alternative strategies
Current strategies are focused on drugs that target the process of clot formation. However, other strategies are emerging for patients with AF. These include:178
• Drugs and procedures that target AF itself
• Drugs and procedures to control heart rhythm and heart rate
• Drugs and procedures to prevent blood clots reaching the brain
New rate and rhythm control drugs
In rhythm control, drugs are used to restore and maintain the sinus rhythm of the heart; in rate control, drugs are used to maintain a suitably low heart rate. Examples of drugs used for rhythm or rate control include amiodar-one, digoxin and beta-blockers.
Dronedarone is a new anti-arrhythmic drug licensed for use in clinically stable patients with non-permanent atrial fi brillation, to prevent recurrence of AF or to lower the pulse rate. In trials dronedarone has been shown to reduce the incidence of death or hospitalisation due to cardiovascular events compared with placebo.188
Non-pharmacological methods
Non-pharmacological interventions for stroke prevention in AF concentrate on eliminating the AF itself; stopping potentially harmful blood clots from reaching the brain, or by preventing the formation of clots.
Non-pharmacological management of abnormal heart rhythm
There are numerous non-pharmacological methods for the management of abnormal heart rhythm.178
These include:
• Electrical cardioversion: the process by which an abnormally fast heart rate or disturbance in heart rhythm is terminated by the delivery of an electric current to the heart at a specifi c moment in the heart cycle
• Radiofrequency (RF) catheter ablation: a minimally- invasive procedure used to correct a faulty electrical pathway in the heart
• Non-RF ablation: open surgical or minimally- invasive procedures that correct the faulty electrical pathways from the heart

The AF Report44
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875• Left atrial appendage (LAA) occlusion: minimally-
invasive procedure that either prevents clots from forming or prevents them from leaving the site of formation in the heart
Current data suggest that catheter ablation is more effective than anti- arrhythmic drug therapy in maintain-ing normal heart rhythm.179 Whether or not this interven-tion affects the incidence strokes requires further evalua-tion in clinical trials.
Procedural interventions to reduce stroke risk
One procedural approach to preventing stroke in AF pa-tients seeks to remove an anatomical contributor to clot formation. More than 90% of blood clots in AF patients form in the left atrial appendage (LAA) of the heart.178
The LAA is a small sac behind an opening the wall of the left atrium. It has been suggested that AF particularly degrades the normal fl ow of blood in the LAA, allowing clot formation.
Sealing the left atrial appendage, isolating it from the main atrial chamber, may therefore prove to be an effec-tive and permanent way to reduce the risk of blood clots and stroke. Several new occlusion devices have been developed that block the LAA. Such devices are designed to be placed permanently, sealing the opening of the LAA. Once in place, potentially harmful blood clots no longer have opportunity to form in the LAA and any thrombotic material in the LAA is prevented from entering the bloodstream and causing stroke.180,181 One of these devices, Watchman, recently received approval for use in Europe.181 The results of a recently published trial, PRO-TECT-AF, showed that closure of the LAA with Watchman was comparable to warfarin for stroke prevention. The study authors noted caution, having observed an overall increase in the rate of adverse events in the LAA group compared to warfarin. However, unlike drugs, device-related interventions frequently demonstrate substantial safety improvements associated with increased operator experience. A subsequent paper from an extension of the same study investigated this effect. A signifi cant reduction in safety events was observed during the second half of the study period compared to the fi rst. It was also noted that the impact of these safety events, as defi ned by sig-nifi cant disability or death, was statistically superior in the Watchman group compared with the warfarin group. The authors concluded that closure of the LAA might provide an alternative strategy to chronic warfarin therapy for stroke prophylaxis in patients with AF.182,183
Summary
To summarise, there are several pharmacological agents in development for use in patients with AF, including the new oral anticoagulants rivaroxaban, dabigatran and apixaban. Minimally-invasive device interventions for the management of arrhythmias and the reduction of stroke risk are also being developed.
Valuable insights into the impact of these new therapies on the prevention of stroke in patients with AF can be gained from real-life registries. A number of registries of AF patients are in existence, most of which are country specifi c or focused on North America.
A new global registry has now been established, the Global Anticoagulant Registry in the FIELD (GARFIELD). GARFIELD will prospectively follow 50,000 newly-diag-nosed AF patients and 5,000 patients with previously-diagnosed AF, over six years.192 Patients will be included and followed, regardless of whether or not they receive appropriate therapy. The GARFIELD registry will docu-ment details such as the risk factors, treatment patterns and clinical events associated with AF, and will provide a picture of the real-life global burden of the condition. It is also hoped that GARFIELD will show how the new advances in therapy can contribute to the prevention of stroke in patients with AF.186
It is hoped that the availability of new therapy options, together with a greater understanding of their impact on the burden of stroke, will pave the way for better management of patients with AF.

The AF Report 45
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875
References
1 Offi ce of National Statistics Health Statistics Quarterly (12) Winter 2001 “Stroke incidence and risk factors in a population based cohort study”; Scottish Stroke Care Audit 2005/2006.
2 Adamson, J., Beswick, A. and Ebrahim, S., “Stroke and Disability” in Journal of Stroke and Cerebrovascular Diseases, Vol 13, No 4, 2004
3 Reducing Brain Damage: Faster access to better stroke care, National Audit Offi ce Report. Department of Health, 2005
4 Marini C, De Santis F, Sacco S et al. Contribution of atrial fi brillation to incidence and outcome of ischemic stroke: results from a population- based study. Stroke 2005;36:1115–19
5 Lamassa M, Di Carlo A, Pracucci G et al. Characteristics, outcome, and care of stroke associated with atrial fi brillation in Europe: data from a multicenter multinational hospital- based registry (The European Community Stroke Project). Stroke 2001;32:392–8
6 Wolfe CD. The impact of stroke. Br Med Bull 2000;56:275–86
7 White CL, Poissant L, Cote-LeBlanc G et al. Long-term caregiving after stroke: the impact on caregivers’ quality of life. J Neurosci Nurs 2006;38:354–60
8 Fuster V, Ryden LE, Cannom DS et al. ACC/AHA/ ESC 2006 Guidelines for the management of patients with atrial fi brillation: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 2006;114:e257–354
9 Lip GYH et al. Stroke 2002;33:238–44
10 Kirchhof P, Auricchio A, Bax J et al. Outcome parameters for trials in atrial fi brillation: recommendations from a consensus conference organized by the German Atrial Fibrillation Competence NETwork and the European Heart Rhythm Association. Europace 2007;9:1006–23
11 Go AS, Hylek EM, Phillips KA et al. Prevalence of diagnosed atrial fi brillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285:2370–5
12 Miyasaka Y, Barnes ME, Gersh BJ et al. Secular trends in incidence of atrial fi brillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119–25
13 Gage BF, Waterman AD, Shannon W et al. Validation of clinical classifi cation schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA 2001;285:2864–70
14 Briffa T, Hickling S, Knuiman M et al. Long term survival after evidence based treatment of acute myocardial infarction and revascularisation: follow- up of population based Perth MONICA cohort, 1984–2005. BMJ 2009;338:b36
15 Wittkowsky AK. Effective anticoagulation therapy: defi ning the gap between clinical studies and clinical practice. Am J Manag Care 2004;10: S297–306
16 Gladstone DJ, Bui E, Fang J et al. Potentially preventable strokes in high-risk patients with atrial fi brillation who are not adequately anticoagulated. Stroke 2009;40: 235–40
17 Hirsh J, Dalen J, Anderson DR et al. Oral anticoagulants: mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest 2001;119:8S–21S
18 Turpie AG. Warfarin replacements: Mechanisms underlying emerging agents. Can J Cardiol 2008;24 Suppl C:56–60C
19 Frykman V, Beerman B, Ryden L et al. Management of atrial fi brillation: discrepancy between guideline recommendations and actual practice exposes patients to risk for complications. Eur Heart J 2001;22:1954–9
20 Man-Son-Hing M, Laupacis A. Anticoagulant- related bleeding in older persons with atrial fi brillation: physicians’ fears often unfounded. Arch Intern Med 2003;163:1580–6

The AF Report46
www.afa.org.uk
www.anticoagulationeurope.org020 8289 687521 Lip GY, Zarifi s J, Watson RD et al. Physician
variation in the management of patients with atrial fi brillation. Heart 1996;75:200–5
22 Daniel K, Wolfe CD, Busch MA et al. What are the social consequences of stroke for working-aged adults? A systematic review. Stroke 2009;40: e431–40
23 Bungard TJ, Ghali WA, Teo KK et al. Why do patients with atrial fi brillation not receive warfarin? Arch Intern Med 2000;160:41–6
24 Lloyd-Jones DM, Wang TJ, Leip EP et al. Lifetime risk for development of atrial fi brillation: the Framingham Heart Study. Circulation 2004;110: 1042–6
25 Eric J. Feuer EJ, Wun LM, Boring CC et al. The Lifetime Risk of Developing Breast Cancer. J Natl Cancer Inst (1993) 85 (11): 892-897
26 Friberg J, Buch P, Scharling H, et al. Rising rates of hospital admissions for atrial fi brillation. Epidemiology 2003;14:666–72.
27 Banach M, Mariscalco G, Urgulan M et al. The signifi cance of preoperative atrial fi brillation in patients undergoing cardiac surgery: preoperative atrial fi brillation – still underestimated opponent. Europace. 2009; 10:1266-70
28 McCabe PJ, Schumacher K, Barnason SA. Living with atrial fi brillation: a qualitative study. J Cardiovasc Nurs. 2011 Jul-Aug;26(4):336-44.
29 Thrall G, Lip GY, Carroll D, Lane D. Depression, anxiety, and quality of life in patients with atrial fi brillation. Chest. 2007 Oct;132(4):1259-64. Epub 2007 Jul 23.
30 AF AWARE. AF AWARE cardiology groups call for greater awareness and better education on atrial fi brillation. Press release 2009. http://www.world- heart-federation.org/press/press- releases/news- details/article/af-aware- cardiology-groups-call-for- greater-awareness-and-better-education-on- atrial- fi brillation/. Accessed 16 June 2009
31 Lip GYH, Kamath S, Jafriet M al. Ethnic Differences in Patient Perceptions of Atrial Fibrillation and Anticoagulation Therapy. Stroke 2002;33:238–44
32 National Institute for Health and Clinical Excellence. Guideline 36 – Atrial fi brillation: the management of atrial fi brillation. http://www.nice. org.uk/ nicemedia/pdf/CG036nice guideline.pdf. Accessed March 200933 National Institute for Health and Clinical Excellence. Understanding NICE guidance: Atrial fi brillation. http://www.nice.org. uk/nicemedia/pdf/ CG036publicinfo. pdf. Accessed May 2009
34 1. American Heart Association. Heart Disease and Stroke Statistics: 2004 Update. Dallas, Tex: American Heart Association; 2003.
35 Aizer A, Gaziano JM, Cook NR et al. Relation of vigorous exercise to risk of atrial fi brillation. Am J Cardiol 2009; 103:1572–7
36 Farrar MW, Bogart DB, Chapman SS et al. Atrial fi brillation in athletes. Mo Med 2006;103:297–301
37 A Ruigómez et al. Incidence of chronic atrial fi brillation in general practice and its treatment pattern. Journal of Clinical Epidemiology 2002 55: 358-363
38 Adamson, J., Beswick, A. and Ebrahim, S., “Stroke and Disability” in Journal of Stroke and Cerebrovascular Diseases, Vol 13, No 4, 2004
39 Easton JD, Saver JL, Albers GW et al. Defi nition and evaluation of transient ischemic attack: a scientifi c statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. Stroke 2009;40:2276–93
40 Stroke Statistics 2009. British Heart Foundation and The Stroke Association.
41 Wolfe, C “The Burden of Stroke” in Wolfe, C, Rudd, T and Beech, R (eds) Stroke Services and Research (1996) The Stroke Association
42 2005 Coronary Heart Disease Statistics. British Heart Foundation
43 World Health Organization. The global burden of disease: 2004 update. http://www.who.int/ healthinfo/global_burden_disease/ 2004_report_ update/en/index.html. Accessed March 2009
44 Boyle P, Ferlay J. Cancer incidence and mortality in Europe, 2004. Ann Oncol 2005;16:481–8
45 Gunarathne A, Patel JV, Gammon B et al. Ischemic stroke in South Asians. A review of the epidemiology, pathophysiology, and ethnicity- related clinical features. Stroke 2009;40;e415–23
46 Mayo NE, Wood-Dauphinee S, Ahmed S et al. Disablement following stroke. Disabil Rehabil 1999;21: 258–68
47 Kappelle LJ, Adams HP Jr, Heffner ML et al. Prognosis of young adults with ischemic stroke. A long-term follow- up study assessing recurrent vascular events and functional outcome in the Iowa Registry of Stroke in Young Adults. Stroke 1994;25:1360–5

The AF Report 47
www.afa.org.uk
www.anticoagulationeurope.org020 8289 687548 Spieler JF, Lanoe JL, Amarenco P. Socioeconomic
aspects of postacute care for patients with brain infarction in France. Cerebrovasc Dis 2002;13: 132–41
49 Chandratheva A, Mehta Z, Geraghty OC et al. Population-based study of risk and predictors of stroke in the fi rst few hours after a TIA. Neurology 2009;72:1941–7
50 Asplund K, Marké L-A, Terént A et al. Costs and gains in stroke prevention: European perspective. Cerebrovasc Dis 1993;3 (Suppl 1):34–42
51 Wattigney WA, Mensah GA, Croft JB. Increased atrial fi brillation mortality: United States, 1980– 1998. Am J Epidemiol 2002;155:819–26
52 Schneck M, Lei X. Cardioembolic stroke. eMedicine Neurology 2008. http://emedicine.medscape.com/ article/1160370-overview. Accessed March 2009
53 Murphy R, Sackley CM, Miller P et al. Effect of experience of severe stroke on subjective valuations of quality of life after stroke. J Neurol Neurosurg Psychiatry 2001;70:679–81
54 Gage BF, Cardinalli AB, Owens DK. The effect of stroke and stroke prophylaxis with aspirin or warfarin on quality of life. Arch Intern Med 1996;156:1829–36
55 Steger C, Pratter A, Martinek-Bregel M et al. Stroke patients with atrial fi brillation have a worse prognosis than patients without: data from the Austrian Stroke registry. Eur Heart J 2004;25:1734–40
56 Wolfe CD, Rudd AG. The Burden of Stroke White Paper: Raising awareness of the global toll of stroke-related disability and death. http://www.safestroke.org/Portals/ 10/ FINAL%20Burden%20of%20 Stroke.pdf. Accessed March 2009
57 Allender S, Scarborough P, Peto V et al. European Cardiovascular Disease Statistics 2008 Edition. http://www. heartstats.org/uploads/documents% 5Cproof30NOV2007.pdf. Accessed March 2009
58 Grant JS, Glandon GL, Elliott TR et al. Caregiving problems and feelings experienced by family caregivers of stroke survivors the fi rst month after discharge. Int J Rehabil Res 2004; 27:105–11
59 Young AJ, Rogers A, Addington-Hall JM. The quality and adequacy of care received at home in the last 3 months of life by people who died following a stroke: a retrospective survey of surviving family and friends using the Views of Informal Carers Evaluation of Services questionnaire. Health Soc Care Community 2008;16:419–28
60 Ferro JM. Cardioembolic stroke: an update. Lancet Neurol 2003;2:177–88
61 The Offi ce of Health Economics Estimating the direct costs of atrial fi brillation to the NHS in the constituent countries of the UK and at SHA level in England, 2008 November 2009, London
62 Bruggenjurgen B, Rossnagel K, Roll S et al. The impact of atrial fi brillation on the cost of stroke: the Berlin acute stroke study. Value Health 2007;10: 137–43
63 Wolf PA, Abbott RD, Kannel WB. Atrial fi brillation: a major contrib- utor to stroke in the elderly. The Framingham Study. Arch Intern Med 1987;147:1561–4
64 Royal College of Physicians. Atrial fi brillation. National clinical guideline for management in primary and secondary care. National Collaborating Centre for Chronic Conditions. http://www.nice.org.uk/ nicemedia/pdf/ cg036fullguideline.pdf. Accessed March 2009
65 Aspirin for the prevention of cardiovascular disease: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2009;150:396–404
66 Murphy NF, Simpson CR, Jhund PS et al. A national survey of the prevalence, incidence, primary care burden and treatment of atrial fi brillation in Scotland. Heart 2007;93:606–12
67 Frost L, Vukelic Andersen L, Godtfredsen J et al. Age and risk of stroke in atrial fi brillation: evidence for guidelines? Neuroepidemiology 2007;28: 109–15
68 Wolf PA, Abbott RD, Kannel WB. Atrial fi brillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983–8
69 Truelsen T, Piechowski-Jozwiak B, Bonita R et al. Stroke incidence and prevalence in Europe: a review of available data. Eur J Neurol 2006;13:581–98
70 Cabin HS, Clubb KS, Hall C et al. Risk for systemic embolization of atrial fi brillation without mitral stenosis. Am J Cardiol 1990;65:1112–16
71 Stewart S, Hart CL, Hole DJ et al. A population- based study of the long- term risks associated with atrial fi brillation: 20-year follow-up of the Renfrew/ Paisley study. Am J Med 2002;113:359–64
72 Jorgensen HS, Nakayama H, Reith J et al. Acute stroke with atrial fi brillation. The Copenhagen Stroke Study. Stroke 1996;27:1765–9
73 Lip GY, Lim HS. Atrial fi brillation and stroke prevention. Lancet Neurol 2007;6:981–93

The AF Report48
www.afa.org.uk
www.anticoagulationeurope.org020 8289 687574 Lip GY, Tse HF. Management of atrial fi brillation.
Lancet 2007;370:604–18
75 Lip GY, Frison L, Halperin JL et al. Identifying patients at high risk for stroke despite anticoagulation: a comparison of contemporary stroke risk stratifi cation schemes in an anticoagulated atrial fi brillation cohort. Stroke 2010;41:2731–8
76 Poli D, Lip GY, Antonucci E et al. Stroke risk stratifi cation in a “real-world” elderly anticoagulated atrial fi brillation population. J Cardiovasc Electrophysiol 2011;22:25–30
77 van Staa TP, Setakis E, Di Tanna GL et al. A comparison of risk stratifi cation schema for stroke in 79884 atrial fi brillation patients in general practice. J Thromb Haemost 2010;9:39–48
78 Singer DE, Albers GW, Dalen JE et al. Antithrombotic therapy in atrial fi brillation: American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th edition). Chest 2008;133:546S–92S
79 Lip GY, Nieuwlaat R, Pisters R et al. Refi ning clinical risk stratifi cation for predicting stroke and thromboembolism in atrial fi brillation using a novel risk factor based approach: The Euro Heart Survey on Atrial Fibrillation. Chest 2010;137:263–72
80 Pisters R, Lane DA, Nieuwlaat R et al. A novel user- friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fi brillation: the Euro Heart Survey. Chest 2010;138:1093–100
81 Olesen JB, Lip GY, Hansen ML. Validation of risk stratifi cation schemes for predicting stroke and thromboembolism in patients with atrial fi brillation: nationwide cohort study. BMJ 2011;342:d124. doi:10.1136/bmj.d124
82 Death rates from stroke, adults aged 65 to 74, 1969 to 2006, England. http://www.heartstats. org/temp/Figsp 1.1fspweb08.xls. Accessed March 2009
83 Ringleb PA, Bousser MG, Ford GA et al. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis 2008;25:457–507
84 Lu Y, Won KA, Nelson BJ et al. Characteristics of the amiodarone- warfarin interaction during long- term follow-up. Am J Health Syst Pharm 2008;65:947–52
85 Singer DE, Albers GW, Dalen JE et al. Antithrombotic therapy in atrial fi brillation: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:429S–56S
86 Hart RG, Pearce LA, Aguilar MI. Meta- analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fi brillation. Ann Intern Med 2007;146:857–67
87 Hart RG, Benavente O, McBride R et al. Antithrombotic therapy to prevent stroke in patients with atrial fi brillation: a meta-analysis. Ann Intern Med 1999;131:492–501
88 Risk factors for stroke and effi cacy of antithrombotic therapy in atrial fi brillation. Analysis of pooled data from fi ve randomized controlled trials. Arch Intern Med 1994;154:1449–57
89 Hart RG, Pearce LA, Miller VT et al. Cardioembolic vs. noncardioembolic strokes in atrial fi brillation: frequency and effect of antithrombotic agents in the stroke prevention in atrial fi brillation studies. Cerebrovasc Dis 2000;10:39–43
90 Miller VT, Pearce LA, Feinberg WM et al. Differential effect of aspirin versus warfarin on clinical stroke types in patients with atrial fi brillation. Stroke Prevention in Atrial Fibrillation Investigators. Neurology 1996;46: 238–40
91 Hylek EM. Contra: ‘Warfarin should be the drug of choice for thrombo- prophylaxis in elderly patients with atrial fi brillation’. Caveats regarding use of oral anticoagulant therapy among elderly patients with atrial fi brillation. Thromb Haemost 2008; 100:16–17
92 Go AS, Hylek EM, Chang Y et al. Anticoagulation therapy for stroke prevention in atrial fi brillation: how well do randomized trials translate into clinical practice? JAMA 2003;290:2685–92
93 Burton C, Isles C, Norrie J et al. The safety and adequacy of antithrombotic therapy for atrial fi brillation: a regional cohort study. Br J Gen Pract 2006;56:697–702
94 Currie CJ, Jones M, Goodfellow J et al. Evaluation of survival and ischaemic and thromboembolic event rates in patients with non-valvar atrial fi brillation in the general population when treated and untreated with warfarin. Heart 2006;92:196–200
95 Monte S, Macchia A, Pellegrini F et al. Antithrombotic treatment is strongly underused despite reducing overall mortality among high-risk elderly patients hospitalized with atrial fi brillation. Eur Heart J 2006;27: 2217–23
96 Abdelhafi z AH, Wheeldon NM. Use of resources and cost implications of stroke prophylaxis with warfarin for patients with nonvalvular atrial fi brillation. Am J Geriatr Pharmacother 2003;1:53–60

The AF Report 49
www.afa.org.uk
www.anticoagulationeurope.org020 8289 687597 Lightowlers S, McGuire A. Cost- effectiveness
of anticoagulation in nonrheumatic atrial fi brillation in the primary prevention of ischemic stroke. Stroke 1998;29:1827–32
98 Baigent C, Blackwell L, Collins R et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009; 373:1849–60
99 Szucs TD, Bramkamp M. Pharmaco- economics of anticoagulation therapy for stroke prevention in atrial fi brillation: a review. J Thromb Haemost 2006;4:1180–5
100 Appleby J, Devlin N, Parkin D. NICE’s cost effectiveness threshold. BMJ 2007;335:358–9
101 Catella-Lawson F. Vascular biology of thrombosis: platelet-vessel wall interactions and aspirin effects. Neurology 2001;57:S5–7
102 Dorsch MP, Lee JS, Lynch DR et al. Aspirin resistance in patients with stable coronary artery disease with and without a history of myocardial infarction. Ann Pharmacother 2007;41:737–41
103 Patel D, Moonis M. Clinical implications of aspirin resistance. Expert Rev Cardiovasc Ther 2007; 5:969–75
104 Palikhe NS, Kim SH, Park HS. What do we know about the genetics of aspirin intolerance? J Clin Pharm Ther 2008; 33:465–72
105 Hughes M, Lip GY. Stroke and thromboembolism in atrial fi brillation: a systematic review of stroke risk factors, risk stratifi cation schema and cost effectiveness data. Thromb Haemost 2008;99:295–304
106 Winter Y, Wolfram C, Schaeg M et al. Evaluation of costs and outcome in cardioembolic stroke or TIA. J Neurol 2009;256:954–63
107 van Walraven C, Hart RG, Singer DE et al. Oral anticoagulants vs aspirin in nonvalvular atrial fi brillation: an individual patient meta-analysis. JAMA 2002;288:2441–8
108 Sato H, Ishikawa K, Kitabatake A et al. Low-dose aspirin for prevention of stroke in low-risk patients with atrial fi brillation: Japan Atrial Fibrillation Stroke Trial. Stroke 2006;37:447–51
109 Gage BF, Cardinalli AB, Albers GW et al. Cost- effectiveness of warfarin and aspirin for prophylaxis of stroke in patients with nonvalvular atrial fi brillation. JAMA 1995;274:1839–45
110 Lip GY, Frison L, Grind M. Effect of hypertension on anticoagulated patients with atrial fi brillation. Eur Heart J 2007;28:752–9
111 Du X, Ninomiya T, de Galan B et al. Risks of cardiovascular events and effects of routine blood pressure lowering among patients with type 2 diabetes and atrial fi brillation: results of the ADVANCE study. Eur Heart J 2009;30:1128–35
112 Nieuwlaat R, Olsson SB, Lip GY et al. Guideline-adherent antithrombotic treatment is associated with improved outcomes compared with under-treatment in high-risk patients with atrial fi brillation. The Euro Heart Survey on Atrial Fibrillation. Am Heart J 2007; 153:1006–12
113 NICE and the National Collaborating Centre for Chronic Conditions. NICE clinical guideline 36: The management of atrial fi brillation. June 2006. http://www.nice.org.uk/nicemedia/ live/10982/30052/30052.pdf
114 National institute for Health and Clinical Excellence. http://www.nice.org.uk/aboutnice/ whatwedo/niceandthenhs/nice_and_the_nhs.jsp
115 Lip GY, Rudolf M. The new NICE guideline on atrial fi brillation management. Heart 2007;93:23
116 The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology. Guidelines for the management of atrial fi brillation. European Heart Journal (2010) 31, 2369–2429
117 Atrial Fibrillation Investigators. Risk factors for stroke and effi cacy of antithrombotic therapy in atrial fi brillation. Analysis of pooled data from fi ve randomized controlled trials. Arch Intern Med 1994;154:1449–57
118 Stroke Prevention in Atrial Fibrillation Investigators. Stroke Prevention in Atrial Fibrillation Study. Final results. Circulation 1991;84:527–39
119 National Institute for Health and Clinical Excellence. Atrial fi brillation: the management of atrial fi brillation. Costing report; Implementing NICE guidance in England. July 2006. www.nice.org.uk /nicemedia/live/10982/30061/30061.pdf
120 Frykman V, Beerman B, Ryden L et al. Management of atrial fi brillation: discrepancy between guideline recommendations and actual practice exposes patients to risk for complications. Eur Heart J 2001;22:1954–9
121 Deplanque D, Leys D, Parnetti L et al. Stroke prevention and atrial fi brillation: reasons leading to an inappropriate management. Main results of the SAFE II study. Br J Clin Pharmacol 2004; 57:798–806
122 Friberg L, Hammar N, Ringh M et al. Stroke prophylaxis in atrial fi brillation: who gets it and who does not? Report from the Stockholm Cohort- study on Atrial Fibrillation (SCAF-study). Eur Heart J 2006;27: 1954–64

The AF Report50
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875123 Nabauer M, Gerth A, Limbourg T et al. The Registry
of the German Competence NETwork on Atrial. Fibrillation: patient characteristics and initial management. Europace 2009;11:423–34
124 Meiltz A, Zimmermann M, Urban P et al. Atrial fi brillation management by practice cardiologists: a prospective survey on the adherence to guidelines in the real world. Europace 2008; 10:674–80
125 Bungard TJ, Ghali WA, McAlister FA et al. Physicians’ perceptions of the benefi ts and risks of warfarin for patients with nonvalvular atrial fi brillation. CMAJ 2001;165:301–2
126 NHS Employers. Quality and Outcomes Framework guidance for GMS contract 2009/10. March 2009. http://www.nhsemployers.org/ Aboutus/Publications/Documents/ QOF_Guidance_2009_fi nal.pdf
127 Baruch L, Gage BF, Horrow J et al. Can patients at elevated risk of stroke treated with anticoagulants be further risk stratifi ed? Stroke 2007;38: 2459–63
128 National Institute for Health and Clinical Excellence. Consultation on potential new indicators for the 2012/13 Quality and Outcomes Framework (QOF) 28/2/2011. http://www.nice.org.uk/media/ 6BC/B1/QOFConsultation.pdf. Accessed 8/7/2011.
129 Mant J, Hobbs FD, Fletcher K et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fi brillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet 2007;370:493–503
130 Anderson DR, Gardner MJ, Putnam W et al. Population-based evaluation of the management of antithrombotic therapy for atrial fi brillation. Can J Cardiol 2005;21:257–66
131 Bravata DM, Rosenbeck K, Kancir S et al. The use of warfarin in veterans with atrial fi brillation. BMC Cardiovasc Disord 2004;4:18132 Maeda K, Sakai T, Hira K et al. Physicians’ attitudes toward anti-coagulant therapy in patients with chronic atrial fi brillation. Intern Med 2004;43:553–60
133 Vasishta S, Toor F, Johansen A et al. Stroke prevention in atrial fi brillation: physicians’ attitudes to anticoagulation in older people. Arch Gerontol Geriatr 2001;33:219–26
134 Hart RG, Aguilar MI. Anticoagulation in atrial fi brillation: selected controversies including optimal anticoagulation intensity, treatment of intracerebral hemorrhage. J Thromb Thrombolysis 2008;25:26–32
135 Choudhry NK, Anderson GM, Laupacis A et al. Impact of adverse events on prescribing warfarin in patients with atrial fi brillation: matched pair analysis. BMJ 2006;332:141–5
136 Tversky A, Kahneman D. Judgment under uncertainty: heuristics and biases. Science 1974;185:1124–31
137 Feinstein AR. The ‘chagrin factor’ and qualitative decision analysis. Arch Intern Med 1985;145:1257–9
138 Devereaux PJ, Anderson DR, Gardner MJ et al. Differences between perspectives of physicians and patients on anticoagulation in patients with atrial fi brillation: observational study. BMJ 2001;323:1218−22
139 Hobbs FD, Fitzmaurice DA, Mant J et al. A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fi brillation in people aged 65 and over. The SAFE study. Health Technol Assess 2005;9:1–74
140 Lip GY, Kamath S, Jafri M et al. Ethnic differences in patient perceptions of atrial fi brillation and anticoagulation therapy: the West Birmingham Atrial Fibrillation Project. Stroke 2002;33: 238–42
141 AntiCoagulation Europe. It’s about time campaign. http://www.anti coagulationeurope.org/abouttime survey.html. Accessed March 2009
142 Dolan G, Smith LA, Collins S et al. Effect of setting, monitoring intensity and patient experience on anticoagulation control: a systematic review and meta-analysis of the literature. Curr Med Res Opin 2008;24:1459–72143 McBride D, Bruggenjurgen B, Roll S et al. Anticoagulation treatment for the reduction of stroke in atrial fi brillation: a cohort study to examine the gap between guidelines and routine medical practice. J Thromb Thrombolysis 2007;24:65–72
144 Trummer U, Mueller U, Nowak P et al. Does physician−patient communication that aims at empowering patients improve clinical outcome? A case study. Patient Educ Couns 2006;61:299–306
145 Beyth RJ, Quinn L, Landefeld CS. A multicomponent intervention to prevent major bleeding complications in older patients receiving warfarin. A randomized, controlled trial. Ann Intern Med 2000;133:687–95
146 Heneghan C et al. Review: self testing and self management increase the benefi ts and reduce the harms of anticoagulant therapy. The Lancet, 2006; 367: 404-11

The AF Report 51
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875147 MHRA Guidance, 2004 www.mhra.gov.uk
148 Gardiner C et al. Patient self-testing is a reliable and acceptable alternative to laboratory INR monitoring. British Journal of Haematology. 2004; 128: 242-247.
149 Fitzmaurice DA et al. Self-management of oral anticoagulation: randomised trial. British Medical Journal. 2005; 331(7524): 1057.
150 Ansell J, Hollowell J, Pengo V et al. Descriptive analysis of the process and quality of oral anticoagulation management in real-life practice in patients with chronic non-valvular atrial fi brillation: the international study of anticoagulation management (ISAM). J Thromb Thrombolysis 2007;23:83–91
151 Lip GY, Agnelli G, Thach AA et al. Oral anticoagulation in atrial fi brillation: A pan- European patient survey. Eur J Intern Med 2007;18:202–8
152 Macik BG. The future of anticoagulation clinics. J Thromb Thrombolysis 2003;16:55–9
153 Rodgers H, Sudlow M, Dobson R et al. Warfarin anticoagulation in primary care: a regional survey of present practice and clinicians’ views. Br J Gen Pract 1997;47:309–10
154 Chiquette E, Amato MG, Bussey HI. Comparison of an anticoagulation clinic with usual medical care: anticoagulation control, patient outcomes, and health care costs. Arch Intern Med 1998;158:1641–7
155 Taborski U, Wittstamm FJ, Bernardo A. Cost- effectiveness of self-managed anticoagulant therapy in Germany. Semin Thromb Hemost 1999;25:103–7
156 Murray E, Fitzmaurice D, McCahon D et al. Training for patients in a randomised controlled trial of self management of warfarin treatment. BMJ 2004;328:437–8
157 Poller L, Keown M, Ibrahim S et al. A multicentre randomised clinical endpoint study of PARMA 5 computer-assisted oral anticoagulant dosage. Br J Haematol 2008;143: 274–83
158 Poller L, Keown M, Ibrahim S et al. An international multicenter randomized study of computer-assisted oral anti-coagulant dosage vs. medical staff dosage. J Thromb Haemost 2008; 6:935–43
159 Groene O, Lombarts M, Klazinga N et al. Is patient-centredness in European hospitals related to existing quality improvement strategies? Analysis of a cross-sectional survey (MARQuIS study). Qual Saf Health Care 2009;18:i44–i50
160 Ellis S. The patient-centred care model: holistic/ multiprofessional/ refl ective. Br J Nurs 1999;8:296–301
161 Gage BF, Cardinalli AB, Owens DK. Cost- effectiveness of preference- based antithrombotic therapy for patients with nonvalvular atrial fi brillation. Stroke 1998;29:1083–91
162 Biem HJ, Hadjistavropoulos H, Morgan D et al. Breaks in continuity of care and the rural senior transferred for medical care under regionalisation. Int J Integr Care 2003;3:e03
163 van Bemmel JH, van Ginneken AM, Stam B et al. Virtual electronic patient records for shared care. Stud Health Technol Inform 1998;52 Pt 1: suppl 37–41
164 van Walraven C, Seth R, Austin PC et al. Effect of discharge summary availability during post- discharge visits on hospital readmission. J Gen Intern Med 2002;17:186–92
165 Turpie AG. New oral anticoagulants in atrial fi brillation. Eur Heart J 2007; 29:155–65166 Turpie AG. Oral, direct factor Xa inhibitors in development for the prevention and treatment of thromboembolic diseases. Arterioscler Thromb Vasc Biol 2007;27:1238–47
167 EMEA. European Public Assessment Report for Eliquis. http://www.ema.europa.eu/ema/index. jsp?curl=pages/medicines/human/ medicines/002148/human_med_001449. jsp&murl=menus/medicines/medicines.jsp&mid= WC0b01ac058001d125#
168 Patel MR for ROCKET AF Investigators. Rivaroxaban- once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation: rationale and design of the ROCKET AF study. Am Heart J 2010;159:340–7
169 Mahaffey KW, Fox KAA and ROCKET AF Executive Steering Committee. Stroke prevention using the oral direct Factor Xa inhibitor rivaroxaban compared with warfarin in patients with nonvalvular atrial fi brillation (ROCKET AF). Presented at AHA 2010. http://sciencenews.myamerican heart. org/ sessions/late_breaking.shtml#rocket. Accessed March 2011
170 European Medicines Agency Evaluation of Medicines for HumanUse. CHMP Assessment Report for Xarelto. http://www.emea.europa. eu/ humandocs/PDFs/EPAR/xarelto/ H-944-en6.pdf. Accessed March 2009
171 ClinicalTrials.gov. http://www.clinical trials.gov. Accessed May 2009

The AF Report52
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875172 Weitz JI. Randomized, parallel group, multicenter,
multinational study evaluating safety of DU-176b compared with warfarin in subjects with non- valvular atrial fi brillation. 50th Annual Meeting of the American Society of Hematology, 5–9 December 2008, San Francisco: Abstract 33
173 European Medicines Agency. Pradaxa Annex 1 Summary of Product Characteristics. http://www.emea. europa.eu/humandocs/PDFs/ EPAR/ pradaxa/emea-combined-h829en.pdf. Accessed November 2009
174 Connolly SJ, Ezekowitz MD, Yusuf S et al. Dabigatran versus warfarin in patients with atrial fi brillation. N Engl J Med 2009;361:10.1056/ nejmoa 0905561
175 Reddy VY, Holmes D, Shephal K et al. Safety of Percutaneous Left Atrial Appendage Closure: Results from the Watchman Left Atrial Appendage System for Embolic Protection in Patients With AF (PROTECT AF) Clinical Trial and the Continued Access Registry Circulation DOI: 10.1161/ CIRCULATIONAHA.110.976449. Jan 17, 2011
176 ClinicalTrials.gov. RELY-ABLE long term multi-center extension of dabigatran treatment in patients with atrial fi brillation Who Completed RE-LY Trial. 2010. http://clinicaltrials.gov/ct2/show/ NCT00808067. Accessed February 2011
177 The ACTIVE Investigators. Effect of clopidogrel added to aspirin in patients with atrial fi brillation. N Engl J Med 2009;360:2066–78
178 Iqbal MB, Taneja AK, Lip GY et al. Recent developments in atrial fi brillation. BMJ 2005;330:238–43
179 Lee R, Kruse J, McCarthy PM. Surgery for atrial fi brillation. Nat Rev Cardiol 2009;6:505–13
180 Sick PB, Schuler G, Hauptmann KE et al. Initial worldwide experience with the WATCHMAN left atrial appendage system for stroke prevention in atrial fi brillation. J Am Coll Cardiol 2007;49:1490–5
181 AtriCure reports fi rst human implant of the Cosgrove–Gillinov left atrial appendage occlusion system. www.bio-medicine.org. Accessed October 2009
182 Holmes DR, Reddy VY, Turi ZG et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fi brillation: a randomised non-inferiority trial. Lancet 2009;374: 534–42
183 McCabe DJ, Kinsella JA, Tobin WO. Left atrial appendage occlusion in non-valvular atrial fi brillation. Lancet 2009;374:504–6
184 Khoo CW, Tay KH, Shantsila E et al. Novel oral anticoagulants. Int J Clin Pract 2009;63:630–41
185 European Medicines Agency. Clopidogrel Annex 1 Summary of Product Characteristics. http://www.emea.europa.eu/human docs/PDFs/ EPAR/clopidogrelbms/ H-974-PI-en.pdf. Accessed March 2009
186 PR Newswire. Largest registry to date to provide the fi rst-ever picture of the real global burden of atrial fi brillation (AF). Barcelona, Spain, 30 August 2009. http://pharmalicensing.com. Accessed October 2009
187 Siddique A, Butt M, Shantsila E et al. New antiplatelet drugs: beyond aspirin and clopidogrel. Int J Clin Pract 2009;63:776–89
188 Hohnloser SH, Crijns HJ, van Eickels M et al. Effect of dronedarone on cardiovascular events in atrial fi brillation. N Engl J Med 2009; 360:668–78
189 Connolly SJ, Crijns HJ, Torp-Pedersen C et al. Analysis of stroke in ATHENA: a placebo-controlled, double-blind, parallel-arm trial to assess the effi cacy of dronedarone 400 mg BID for the prevention of cardiovascular hospitalization or death from any cause in patients with atrial fi brillation/atrial fl utter. Circulation 2009;120:1174–80
190 Nabauer M, Gerth A, Limbourg T et al. The Registry of the German Competence NETwork on Atrial Fibrillation: patient characteristics and initial management. Europace 2009;11:423–34
191 Kirchhof P, Bax J, Blomstrom- Lundquist C et al. Early and comprehensive management of atrial fi brillation: executive summary of the proceedings from the 2nd AFNET- EHRA consensus conference ‘research perspectives in AF’. Eur Heart J 2009;doi:10.1093/eurheartj/ehp235
192 Kakkar AK, Lip GYH, Breithardt G. The importance of real-world registries in the study of AF-related stroke. http://www.theheart.org/documents/ sitestructure/en/content/programs/ 1003241/ transcript.pdf. Accessed October 2009
193 Kannel WB, Wolf PA, Benjamin EJ et al. Prevalence, incidence, prognosis, and predisposing conditions for atrial fi brillation: population-based estimates. Am J Cardiol 1998; 82:2N–9N
194 Lin LY, Lee CH, Yu CC, Tsai CT, Lai LP, Hwang JJ, Chen PC, Lin JL. Risk factors and incidence of ischemic stroke in Taiwanese with nonvalvular atrial fi brillation. A nationwide database analysis. Atherosclerosis 2011 doi:10.1016/ j.atherosclerosis.2011.03.033

The AF Report 53
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875195 Lip GY, Beevers DG, Singh SP et al. ABC of atrial
fi brillation. Aetiology, pathophysiology, and clinical features. BMJ 1995;311:1425–8
196 Ghatnekar O, Glader EL. The effect of atrial fi brillation on stroke-related inpatient costs in Sweden: a 3-year analysis of registry incidence data from 2001. Value Health 2008; 11:862–8
197 Rasmussen LH, Larsen TB, Due KM, Tjønneland A, Overvad K, Lip GY. Impact of vascular disease in predicting stroke, and death in patients with atrial fi brillation: The Danish Diet, Cancer and Health (DCH) cohort study. J Thromb Haemost. 2011 Apr 19. doi: 10.1111/j.1538-7836.2011.04308.x
198 Cairns JA, Connolly S, McMurtry S, Stephenson M, Talajic M; CCS Atrial Fibrillation Guidelines Committee. Canadian Cardiovascular Society atrial fi brillation guidelines 2010: prevention of stroke and systemic thromboembolism in atrial fi brillation and fl utter. Can J Cardiol. 2011 Jan-Feb;27(1):74-90.
199 Gudbjartsson DF, Arnar DO, Helgadottir A et al. Variants conferring risk of atrial fi brillation on chromosome 4q25. Nature 2007;448:353–7
200 Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fi brillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/ Alcohol Concomitantly) score. J Am Coll Cardiol. 2011 Jan 11;57(2):173-80. Epub 2010 Nov 24.
201 Olesen JB, Lip GY, Hansen PR, Lindhardsen J, Ahlehoff O, Andersson C, Weeke P, Hansen ML, Gislason GH, Torp-Pedersen C. Bleeding risk in ‘real world’ patients with atrial fi brillation: comparison of two established bleeding prediction schemes in a nationwide cohort. J Thromb Haemost. 2011 Aug;9(8):1460-7. doi: 10.1111/ j.1538-7836.2011.04378.x.
202 Olesen JB, Lip GY, Lindhardsen J, Lane DA, Ahlehoff O, Hansen ML, Raunsø J, Tolstrup JS, Hansen PR, Gislason GH, Torp-Pedersen C. Risks of thromboembolism and bleeding with thromboprophylaxis in patients with atrial fi brillation: A net clinical benefi t analysis using a ‘real world’ nationwide cohort study. Thromb Haemost. 2011 Jul 20;106(4). [Epub ahead of print] PMID: 2178933
203 Potpara TS, Lip GHY. Lone atrial fi brillation: what is known and what is to come. Int J Clin Pract. 2011 Apr;65(4):446-57. doi: 10.1111/ j.1742-1241.2010.02618.x. Epub 2011 Jan 11

The AF Report54
www.afa.org.uk
www.anticoagulationeurope.org020 8289 6875


Atrial Fibrillation: Preventing A Stroke Crisis
www.afa.org.ukwww.afa.org.uk www.anticoagulationeurope.org
Access an online version of the AF Report
www.preventaf-strokecrisis.org
Calculate your personal risk of stroke because of AF
www.afstrokerisk.org
This report was developed by the Atrial Fibrillation Association (AFA) and AntiCoagulation Europe (ACE), both of which are charities engaged in patient advocacy, support and education. The report content is based upon a Working Group Report prepared by Action for Stroke Prevention.
This revision has been updated and rewritten specifi cally for online access by UK patients and those who care for them. Development of this report was supported by an unrestricted grant provided to the AFA and ACE by Bayer Healthcare. © Copyright AFA and ACE 2011.