Embed Size (px)
Citation preview
ARTICLE IN PRESS
Respiratory Medicine (2007) 101, 957–962
0954-6111/$ - see frodoi:10.1016/j.rmed.
�Corresponding au
E-mail address: m1Present address:
Respiratory Diseases
The additive effect of theophylline on a combinationof formoterol and tiotropium in stable COPD:A pilot study
Mario Cazzolaa,�,1, Maria Gabriella Materab
aDepartment of Respiratory Medicine, Unit of Pneumology and Allergology, A. Cardarelli Hospital, Naples, ItalybDepartment of Experimental Medicine, Unit of Pharmacology, 2nd University of Naples, Naples, Italy
Received 30 August 2006; accepted 9 September 2006Available online 23 October 2006
KEYWORDSCOPD;Tiotropium;Formoterol;Theophylline;Combination therapy
nt matter & 20062006.09.012
thor.
cazzola@qubisoftDepartment of
, University of Rom
SummaryWe explored the additive effect of titrated oral theophylline in patients with stablechronic obstructive pulmonary disease (COPD) who received both tiotropium, 18 mg od, andformoterol, 12 mg bid. Thirty-six patients with moderate-to-severe COPD were enrolled inthis two-period trial. They were initially treated with formoterol+tiotropium for 4 weeks.After this first period, they were divided in two groups of 18 patients. Both groupscontinued with the initial treatment for further 4 weeks, but the first group received alsoplacebo whereas the second group received oral theophylline. The combination therapywith formoterol+tiotropium induced a significant improvement in mean predose FEV1 andFVC at the end of the first period, and a significant reduction in dyspnea score as measureby a visual analogic scale and in use of rescue salbutamol. The second period of treatmentelicited a significant further improvement in lung function and reduction in dyspnea scoreand salbutamol use in both groups. On the contrary, differences in improvements in FEV1and FVC and reduction in dyspnea score and salbutamol use between theophylline andplacebo arms at the end of the second treatment period were not significant, although 5patients reported an important relief in dyspnea during the theophylline administrationperiod. These findings question the importance of adding theophylline in stable COPDpatients already treated with two long-acting bronchodilators, but also indicate thepossibility that some of them can benefit from theophylline because of a symptomaticimprovement.& 2006 Published by Elsevier Ltd.
Published by Elsevier Ltd.
.it (M. Cazzola).Internal Medicine, Unit ofe Tor Vergata, Rome, Italy.
Introduction
Current evidence supports the recommendation of theGlobal Initiative for chronic obstructive lung disease (GOLD)guidelines1 and American Thoracic Society/European

ARTICLE IN PRESS
M. Cazzola, M.G. Matera958
Respiratory Society position paper2 of at least one of the twoclasses of long-acting inhaled bronchodilators, either once-daily tiotropium or twice-daily salmeterol or formoterol, asinitial maintenance therapy for symptomatic chronic ob-structive pulmonary disease (COPD). There is no datasupporting the superiority of one of the families of inhaledbronchodilators (i.e., b2 agonists and anti-cholinergicagents) over the other. Thus, the choice has to be basedon the individual symptomatic response. In patients who donot respond satisfactorily to tiotropium or a long-actinginhaled b-agonist as the initially prescribed single main-tenance agent, the GOLD guidelines recommend the addi-tion of the alternate class of long-acting inhaledbronchodilator as the next step. In effect, an increasingbody of evidence3–7 indicates that the combination of along-acting b2-agonsit and a long-acting anti-muscarinicagent is an effective therapeutic approach for patientssuffering from moderate-to-severe COPD.
Unfortunately treatments prescribed for COPD patientsdo not always follow current guidelines, particularly in theprimary care setting. Recently, Taskin et al.8 have examinedthe adherence to GOLD guidelines recommendation amongpatients entering UPLIFT, a global trial evaluating theefficacy of tiotropium in slowing COPD progression and haveobserved that the percentage of patients receiving long-acting bronchodilators increased as COPD severity in-creased; however, a substantial number of patients werenot receiving long-acting bronchodilators in accordance withGOLD guidelines. In particular, long-acting bronchodilators(anti-cholinergics and/or b-agonists) were used in 67.3% and69.3% of patients. The use of theophylline in 34.9% and36.1% patients suffering from severe and very severe COPD,respectively, was another unexpected finding.
Theophylline, which used to be part of the mainstay oftreatment for COPD, has been relegated to third-linetherapy in COPD because of the frequency of side effectsand relative low efficacy.9 Nonetheless, it is inexpensive andstill has its role. In fact, theophylline tends to be added tothese inhaled bronchodilators in more severe patients andhas been shown to give additional clinical improvementwhen added to a long-acting b2-agonist.
10,11 Moreover,increasing evidence shows that theophylline has significantanti-inflammatory effects in COPD at lower plasma concen-trations.12 In particular, Barnes12 has highlighted that it isthe only therapy currently available that is anti-inflamma-tory in patients with COPD.
These findings are important and might justify the body ofevidence that supports the use of theophylline together with ab2-agonist and an anti-cholinergic because a number ofpatients with COPD may respond subjectively to theophylline.In effect, GOLD guidelines1 report that the combination of ab2-agonist, an anti-cholinergic, and theophylline may produceadditional improvements in lung function and heath status.
We examined the additive effect of oral theophylline inpatients with stable COPD who received both tiotropium,18 mg od, and formoterol, 12 mg bid in a regular manner.
Patients and methods
Thirty-six patients with well-controlled moderate-to-verysevere COPD were enrolled. All of them were 50 years of age
or older, and were current or former smokers with a 20 pack-year or more history. Inclusion criteria required a baselineFEV1 of less than 70% of predicted but more than 0.50 L, anda postbronchodilator FEV1/FVC o70% following salbutamol,400mg. Exclusion criteria were as follows: current evidenceof asthma as primary diagnosis; unstable respiratory diseaserequiring oral/parenteral corticosteroids within 4 weeksprior to beginning the study; upper or lower respiratorytract infection within 4 weeks of the screening visit;unstable angina or unstable arrhythmias; concurrent use ofmedications that affected COPD or interacted with methyl-xanthine products, such as macrolides or fluoroquinolones;and evidence of alcohol abuse. All patients were not takingtheophylline at the time of recruitment in order to avoid thewell-known effects of theophylline withdrawal in COPD.13
Table 1 outlines some characteristics and the smokinghistory of the population studied.
This was a single-blind, placebo-controlled, randomized,two-period trial. Following an initial screening visit, alleligible patients entered a 7 days inhaled placebo run-induring which their regular treatment for COPD was stoppedand they received salbutamol for relief of breakthroughsymptoms and inhaled corticosteroids when already used.Thereafter, all patients were treated with formoterol 12 mgbid+tiotropium 18 mg od for 4 weeks. After this first period,they were divided in two groups of 18 patients each in arandom manner. Both groups continued with the initialtreatment for further 4 weeks, but the first group also oralreceived placebo twice whereas the second group receivedoral theophylline (i.e., 200 or 300mg twice daily throughoutthe 4 weeks [the 300-mg dose was only for patientsweighing480 kg, and these patients received 200mg bidfor first week and the higher 300-mg dose bid for theremaining 3 weeks]). The patients were blinded to thenature of the oral medications.
After the initial screening visit, patients returned to theclinic at the end of the 7-day placebo run-in period for visit2, at which time they started the treatment regimen withformoterol+tiotropium. Afterwards, they attended the clinicafter 4 weeks of treatment when they were randomized toplacebo or theophylline, and after 4 further weeks oftreatment for evaluations of pulmonary function. Patientswithheld from taking their study medication on the morningof each visit, so all measurements were made at trough(i.e., approximately 12 h after their preceding evening dosewas received). At each visit, three FEV1 and FVC measure-ments were taken, and the highest of each was recorded.Changes in the perception of dyspnea assessed through useof a bipolar visual anagogic scale (VAS), and supplementalsalbutamol use were also monitored at each visit. The VASconsisted of a 20-cm horizontal line scoring between 0 (verymuch better) at the left end, and 10 (very much worse) atthe right, with ‘no change’ in the middle. All patients werefamiliarized with the VAS before the study. The supple-mental salbutamol use was recorded by the patient dailythroughout the 2-month treatment period. At the end of thesecond 4-week-treatment, we checked the serum theophyl-line concentration in all patients included in the theophyl-line arm.
Adverse events were collected through non-specificquestioning or direct observation by investigators at eachclinic visit and through spontaneous reports by patients.

ARTICLE IN PRESS
Table 1 Demographics of the population studied.
Variables Placebo arm Theophylline arm
Age (year) 63.873.1 66.274.0Sex (no.) 15 M–3 F 17 M–1 FSmoking (pack-year) 4874.7 5575.2Current smokers, n (%) 12 (72) 11 (61)FEV1, predicted (%) 42 (1.7) 39 (1.4)FEV1/FVC ratio (before bronchodilator) 5073.2 5173.7Inhaled corticosteroid use, n (%) 9 (50) 11 (61)Tiotropium use, n (%) 7 (39) 6 (33)Long-acting b2-agonist use, n (%) 18 (100) 18 (100)Theophylline use, n (%) 2 (11) 1 (6)
Data are presented as mean7SE unless otherwise indicated. M, male; F, female.
Effect of theophylline on a combination of formoterol and tiotropium in stable COPD 959
Patients who experienced exacerbation resulting in hospi-talization or, at least, treatment with an oral corticosteroidand/or antibiotic during the study period were withdrawn.The definition of exacerbation used in the present study was‘‘a worsening of respiratory symptoms, which requirestreatment with oral corticosteroids or antibiotics, orboth’’.14
This was a pilot study and the first known evaluation ofthe additive effect of theophylline on a combination offormoterol and tiotropium in stable COPD. In view of thelack of previous experiences, no statistical hypotheses weredrawn and consequently no formal sample size calculationwas made. The use of a pilot study such as the current studyin clinical research is a well-established scientific procedureand only through the use of a pilot study can statisticiansclarify data distributions and determine appropriate samplesizes for full-scale clinical trials.3
The primary efficacy measure was the mean change frombaseline in predose FEV1 at the end of the study. Secondaryefficacy measures included change from baseline in FVC, VASscore assessing dyspnea and in supplemental salbutamol.Student’s t-test for paired data and repeated ANOVAmeasurements were used for statistical analysis. Values ofpo0:05 were considered as significant.
Results
All patients completed the first treatment period withformoterol+tiotropium. Thirty-three patients completed thesecond treatment period: 17 patients in the placebo arm,and 16 patients in the theophylline arm. The patient in theplacebo arm was withdrawn for COPD exacerbation resultingin hospitalization. The two patients in the theophylline werewithdrawn for severe headache and rhythm disturbances,respectively. There was no significant difference among thepost run-in baseline spirometric values of the two treatmentgroups (FEV1, P40.05)).
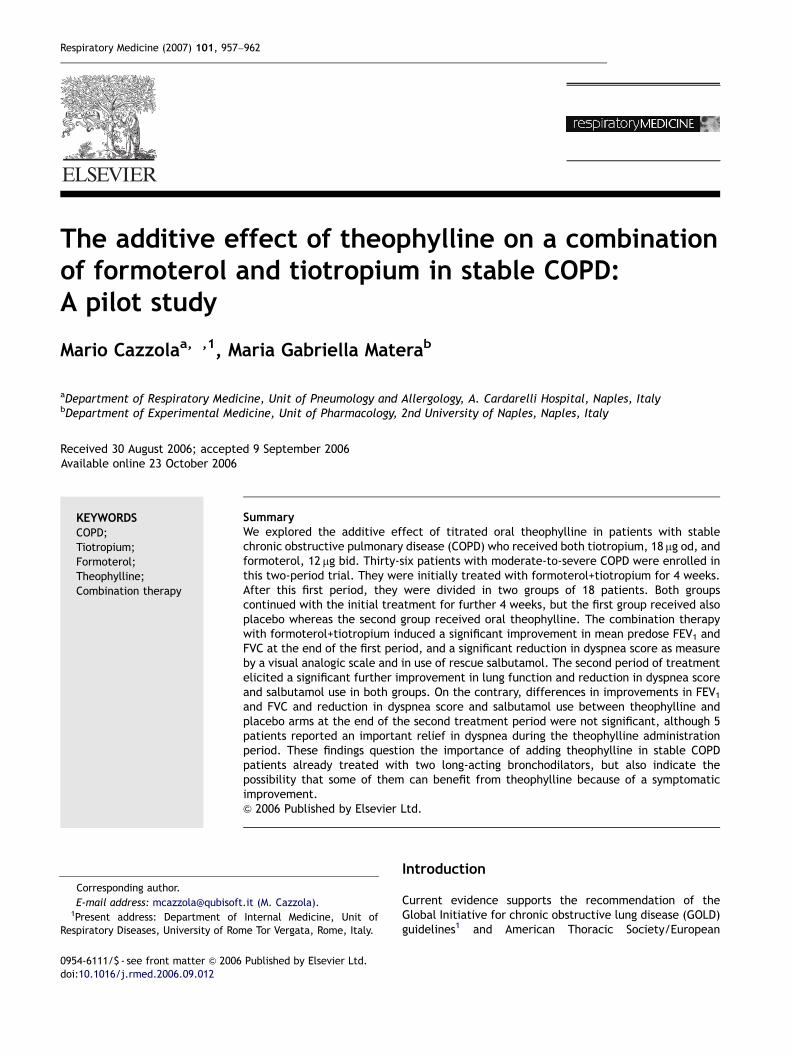
The mean7SE baseline FEV1 and FVC at the start of thetreatment periods were 1.01770.07 L and 1.99270.130 L,respectively in the placebo arm and 0.94170.07 L and1.86470.129 L, respectively, in the theophylline arm. Meanpredose FEV1 and FVC values significantly (Po0.001)improved compared to baseline at the end of the first 4-week treatment in both arms (Fig. 1). At the end of the
second 4-week treatment, FEV1 (Po0.001 both in theplacebo arm and in the theophylline arm, respectively)and FVC (Po0.05 in the placebo arm and Po0.001 in thetheophylline arm, respectively) values further significantlyimproved in both arms (Fig. 1). On the contrary, differencesin improvements in FEV1 and FVC between theophylline andplacebo arms at the end of the second treatment periodwere not significant (P ¼ 0.779 and P ¼ 0.638, respec-tively).
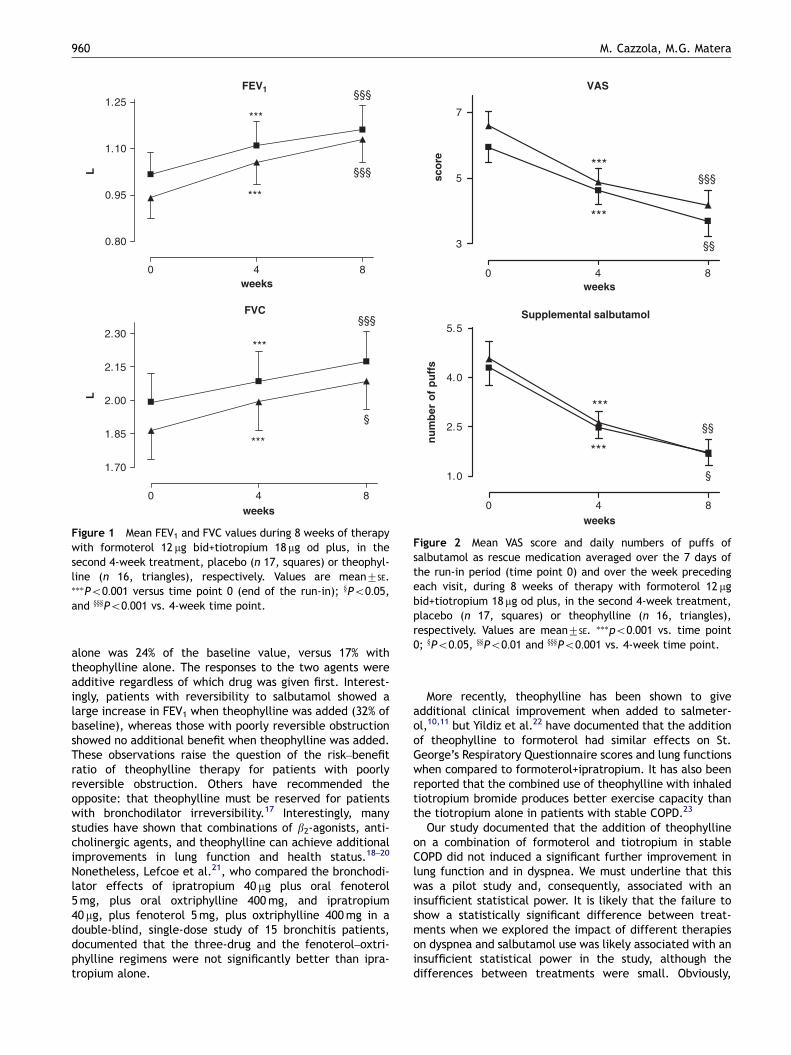
The initial 4-week treatment with formoterol+tiotropiuminduced a significant (Po0.001) improvement in dyspneaand induced a significant (Po0.001) reduction in the use ofsupplemental salbutamol (Fig. 2). At the end of the second4-week treatment with formoterol+tiotropium, we observedan additional significant improvement in dyspnea (Po0.01 inthe placebo arm and Po0.001 in the theophylline arm,respectively) and a further significant (Po0.05, both in theplacebo arm and in the theophylline arm) reduction in theuse of salbutamol as rescue medication (Fig. 2). Differencesin changes in dyspnea score and use of supplementalsalbutamol between theophylline and placebo arms at theend of the second treatment period were not significant(P ¼ 0.436 and P ¼ 0.975, respectively). In any case, 5patients reported an important relief in dyspnea at the endthe theophylline administration period.
Ten out of 16 patients had a theophylline concentrationabove the lower limit of 10 mg/mL, only one had a serumtheophylline concentration 420 mg/mL, and in the otherfive patients theophylline concentration was in the 7–10 mg/mL range.
A part the three patients that were withdrawn for severeadverse events, two patients in the theophylline armsuffered from a mild gastrointestinal adverse event andanother from insomnia.
Discussion
Theophylline is still widely used as a bronchodilator in COPD,although inhaled bronchodilators are preferred.1,2 Usuallytheophylline tends to be added to these inhaled broncho-dilators in patients with more severe COPD.15 In a crossoverstudy, 16 patients with severe COPD received high-dosesalbutamol followed by high-dose theophylline, and theopposite regimen.16 The increase in FEV1 with salbutamol
ARTICLE IN PRESS
0 4 8
3
5
7
§§§
§§
sco
re
Supplemental salbutamol
0 4 8
1.0
2.5
4.0
5.5
nu
mb
er o
f p
uff
s§§
§
VAS
weeks
weeks
Figure 2 Mean VAS score and daily numbers of puffs ofsalbutamol as rescue medication averaged over the 7 days ofthe run-in period (time point 0) and over the week precedingeach visit, during 8 weeks of therapy with formoterol 12 mgbid+tiotropium 18mg od plus, in the second 4-week treatment,placebo (n 17, squares) or theophylline (n 16, triangles),respectively. Values are mean7SE. ���po0:001 vs. time point0; yPo0:05, yyPo0:01 and yyyPo0:001 vs. 4-week time point.
FEV1
0 4 8
0.80
0.95
1.10
1.25
weeks
L §§§
§§§
FVC
0 4 8
1.70
1.85
2.00
2.15
2.30§§§
§
weeks
L
Figure 1 Mean FEV1 and FVC values during 8 weeks of therapywith formoterol 12 mg bid+tiotropium 18mg od plus, in thesecond 4-week treatment, placebo (n 17, squares) or theophyl-line (n 16, triangles), respectively. Values are mean7SE.���Po0:001 versus time point 0 (end of the run-in); yPo0:05,and yyyPo0:001 vs. 4-week time point.
M. Cazzola, M.G. Matera960
alone was 24% of the baseline value, versus 17% withtheophylline alone. The responses to the two agents wereadditive regardless of which drug was given first. Interest-ingly, patients with reversibility to salbutamol showed alarge increase in FEV1 when theophylline was added (32% ofbaseline), whereas those with poorly reversible obstructionshowed no additional benefit when theophylline was added.These observations raise the question of the risk–benefitratio of theophylline therapy for patients with poorlyreversible obstruction. Others have recommended theopposite: that theophylline must be reserved for patientswith bronchodilator irreversibility.17 Interestingly, manystudies have shown that combinations of b2-agonists, anti-cholinergic agents, and theophylline can achieve additionalimprovements in lung function and health status.18–20
Nonetheless, Lefcoe et al.21, who compared the bronchodi-lator effects of ipratropium 40 mg plus oral fenoterol5mg, plus oral oxtriphylline 400mg, and ipratropium40 mg, plus fenoterol 5mg, plus oxtriphylline 400mg in adouble-blind, single-dose study of 15 bronchitis patients,documented that the three-drug and the fenoterol–oxtri-phylline regimens were not significantly better than ipra-tropium alone.
More recently, theophylline has been shown to giveadditional clinical improvement when added to salmeter-ol,10,11 but Yildiz et al.22 have documented that the additionof theophylline to formoterol had similar effects on St.George’s Respiratory Questionnaire scores and lung functionswhen compared to formoterol+ipratropium. It has also beenreported that the combined use of theophylline with inhaledtiotropium bromide produces better exercise capacity thanthe tiotropium alone in patients with stable COPD.23
Our study documented that the addition of theophyllineon a combination of formoterol and tiotropium in stableCOPD did not induced a significant further improvement inlung function and in dyspnea. We must underline that thiswas a pilot study and, consequently, associated with aninsufficient statistical power. It is likely that the failure toshow a statistically significant difference between treat-ments when we explored the impact of different therapieson dyspnea and salbutamol use was likely associated with aninsufficient statistical power in the study, although thedifferences between treatments were small. Obviously,

ARTICLE IN PRESS
Effect of theophylline on a combination of formoterol and tiotropium in stable COPD 961
there was a possibility of a type II error, which supported thelack of significance that we have repeatedly observed24 and,perhaps, a study with a larger sample would likely havereached statistical significance.
In any case, our study questions the importance of addingtheophylline in stable COPD patients already treated withtwo long-acting bronchodilators, although it indicates thepossibility that some of them can benefit from theophyllinebecause of a symptomatic improvement. A systematicreview and meta-analysis of efficacy of theophylline inpeople with stable COPD has documented that beneficialeffects may be obtained in individuals who remain sympto-matic from COPD, despite first-line bronchodilator ther-apy.25 We cannot confirm this finding because we haveobserved improvement in dyspnea in both groups, butdifferences between theophylline and placebo groups werenot significant. In any case, the fact that five patientsreported an important relief in dyspnea during the theophyl-line administration period and these patients were betweenthose with more severe dyspnea at the end of the first4-week treatment with formoterol+tiotropium supports thisopinion.
It is evident that larger parallel, randomized-controlledtrials with explicit clinical and diagnostic criteria, sufficientduration of follow-up and description of all relevant clinicaloutcome measures are warranted in order to understandwhen the addition of theophylline is really needed. In anycase, theophylline possesses anti-inflammatory and immu-nomodulatory effects in addition to its well-recognizedeffects as a bronchodilator when administered at doses thatare not associated with unacceptable side effects and whichmay be used in selected patients without serum monitor-ing.26,27 Therefore, we believe that a combination therapywith tiotropium and a long-acting b2-agonist may serve as abasis for improved ‘triple therapy’ combinations with low-dose theophylline with the aim of delivering three com-plementary therapeutic effects for patients with COPD. Inorder to explore this possibility, a trial of longer duration (atleast 1 year) is mandatory.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Globalstrategy for the diagnosis, management, and prevention ofchronic obstructive pulmonary disease, 2005 [accessed August26, 2006]. Available at: /http://www.goldcopd.comS.
2. Celli BR, MacNee W. Standards for the diagnosis and treatmentof patients with COPD: a summary of the ATS/ERS positionpaper. Eur Respir J 2004;23:932–46.
3. Cazzola M, Di Marco F, Santus P, Boveri B, Verga M, Matera MG,et al. The pharmacodynamic effects of single inhaled doses offormoterol, tiotropium and their combination in patients withCOPD. Pulm Pharmacol Ther 2004;17:35–9.
4. Cazzola M, Centanni S, Santus P, Verga M, Mondoni M, di Marco F,et al. The functional impact of adding salmeterol andtiotropium in patients with stable COPD. Respir Med 2004;98:1214–21.
5. Cazzola M, Noschese P, Salzillo A, De Giglio C, D’Amato G,Matera MG. Bronchodilator response to formoterol after regulartiotropium or to tiotropium after regular formoterol in COPDpatients. Respir Med 2005;99:524–8.
6. van Noord JA, Aumann JL, Janssens E, Smeets JJ, Verhaert J,Disse B, et al. Comparison of tiotropium once daily, formoterol
twice daily and both combined once daily in patients withCOPD. Eur Respir J 2005;26:214–22.
7. van Noord JA, Aumann JL, Janssens E, Verhaert J, Smeets JJ,Mueller A, et al. Effects of tiotropium with and withoutformoterol on airflow obstruction and resting hyperinflation inpatients with COPD. Chest 2006;129:509–17.
8. Tashkin D, Celli B, Decramer M, Burkhart D, Kesten S, Cassino C.Prescribing patterns according to COPD treatment guidelines inpatients enrolled in a global clinical trial [abstract]. Proc AmThorac Soc 2006;3:A111.
9. Cazzola M, Matera MG, Donner CF. Long-acting b2 agonists andtheophylline in stable chronic obstructive pulmonary disease.Thorax 1999;54:730–6.
10. Cazzola M, Di Lorenzo G, Di Perna F, Calderaro F, Testi R,Centanni S. Additive effects of salmeterol and fluticasone ortheophylline in COPD. Chest 2000;118:1576–81.
11. ZuWallack RL, Mahler DA, Reilly D, Church N, Emmett A, RickardK, et al. Salmeterol plus theophylline combination therapy inthe treatment of COPD. Chest 2001;119:1661–70.
12. Barnes PJ. Theophylline in chronic obstructive pulmonarydisease: new horizons. Proc Am Thorac Soc 2005;2:334–9.
13. Kirsten DK, Wegner RE, Jorres RA, Magnussen H. Effects oftheophylline withdrawal in severe chronic obstructive pulmon-ary disease. Chest 1993;104:1101–7.
14. Burge PS, Calverley PM, Jones PW, Spencer S, Anderson JA,Maslen TK. Randomised, double blind, placebo controlled studyof fluticasone propionate in patients with moderate to severechronic obstructive pulmonary disease: the ISOLDE trial. Br MedJ 2000;320:1297–303.
15. Donohue JF. Combination therapy for chronic obstructivepulmonary disease: clinical aspects. Proc Am Thorac Soc 2005;2:272–81.
16. Filuk RB, Easton PA, Anthonisen NR. Responses to large doses ofsalbutamol and theophylline in patients with chronicobstructive pulmonary disease. Am Rev Respir Dis 1985;132:871–4.
17. Thomas P, Pugsley JA, Stewart JH. Theophylline and salbutamolimprove pulmonary function in patients with irreversiblechronic obstructive pulmonary disease. Chest 1992;101:160–5.
18. Nishimura K, Koyama H, Ikeda A, Izumi T. Is oral theophyllineeffective in combination with both inhaled anticholinergicagent inhaled b2-agonist in the treatment of stable COPD?Chest 1993;104:179–84.
19. Karpel JP, Kotch A, Zinny M, Pesin J, Alleyne W. A comparison ofinhaled ipratropium, oral theophylline plus inhaled b-agonist,and the combination of all three in patients with COPD. Chest1994;105:1089–94.
20. Nishimura K, Koyama H, Ikeda A, Sugiura N, Kawakatsu K, IzumiT. The additive effect of theophylline on a high-dose combina-tion of inhaled salbutamol and ipratropium bromide in stableCOPD. Chest 1995;107:718–23.
21. Lefcoe NM, Toogood JH, Blennerhassett G, Baskerville J,Paterson NA. The addition of an aerosol anticholinergic to anoral beta agonist plus theophylline in asthma and bronchitis: adouble-blind single dose study. Chest 1982;82(3):300–5.
22. Yildiz F, Basyigit I, Yildirim E, Boyaci H, Ilgazli A. Differentbronchodilator combinations have similar effects on healthstatus in COPD. Pulm Pharmacol Ther 2006;19:101–6.
23. Hanaoka Y, Teramoto S, Yamamoto H, Yamaguchi Y, Ouchi Y.Effects of the sustained release of theophylline, UnifilR,and tiotropium bromide on pulmonary function andexercise performance in patients with stable chronic obstruc-tive pulmonary disease [abstract]. Proc Am Thorac Soc 2006;3:A114.
24. Freiman JA, Chalmers TC, Smith H, Kuebler RR. The importanceof b, the type II error, and sample size in the design andinterpretation of the randomized controlled trial. In: Bailar JC,

ARTICLE IN PRESS
M. Cazzola, M.G. Matera962
Mosteller F, editors. Medical uses of statistics. Boston, USA:NEJM Books; 1992. p. 357–73.
25. Ram FS, Jardin JR, Atallah A, Castro AA, Mazzini R, Goldstein R,et al. Efficacy of theophylline in people with stable chronicobstructive pulmonary disease: a systematic review and meta-analysis. Respir Med 2005;99:135–44.
26. Sullivan P, Bekir S, Jaffar Z, Page C, Jeffery P, Costello J. Anti-inflammatory effects of low-dose oral theophylline in atopicasthma. Lancet 1994;343:1006–8.
27. Boswell-Smith V, Cazzola M, Page CP. Are phosphodiesterase 4inhibitors just more theophylline? J Allergy Clin Immunol2006;117:1237–43.

![Efficacy of Tiotropium/Olodaterol Compared with Tiotropium as a … · 2 days ago · quality of life versus tiotropium and placebo [9]. In addition, in a recent post hoc analysis](https://img.pdfslide.us/doc/110x75/5faeda3c9b2c197f7d4a9e73/efficacy-of-tiotropiumolodaterol-compared-with-tiotropium-as-a-2-days-ago-quality.jpg)



























