Embed Size (px)
Citation preview

The addition of soft tissuereplacement grafts in plasticperiodontal and implant surgery:critical elements in design andexecutionZuhr O, B€aumer D, H€urzeler M. The addition of soft tissue replacement grafts inplastic periodontal and implant surgery: critical elements in design and execution. JClin Periodontol 2014; 41 (Suppl. 15): S123–S142. doi: 10.1111/jcpe.12185.
AbstractSoft tissue replacement grafts have become a substantial element to increase tissuevolume in plastic periodontal and implant surgery. Autogenous subepithelial con-nective tissue grafts are increasingly applied in aesthetic indications like soft tissuethickening, recession treatment, ridge preservation, soft tissue ridge augmentationand papilla re-construction. For the clinical performance of connective tissuegraft harvesting and transplantation, a fundamental understanding of the anat-omy at the donor sites and a sound knowledge of tissue integration and re-vascu-larization processes are required. Possible donor sites are the anterior andposterior palate including the maxillary tuberosity, providing grafts of distinctgeometric shape and histologic composition. The selective clinical application ofdifferent grafts depends on the amount of required tissue, the indication and thepersonal preference of the treating surgeon. One of the main future challenges isto volumetrically evaluate and compare the efficacy and long-term stability of softtissue autografts and their prospective substitutes. The aim of this review was todiscuss the advantages and shortfalls of different donor sites, substitute materialsand harvesting techniques. Although standardized recommendations regardingtreatment choice and execution can hardly be given, guidelines for predictableand successful treatment outcomes are provided based on clinical experience andthe available scientific data.
Otto Zuhr1,2, Daniel B€aumer1 andMarkus H€urzeler1,3
1Private Practice H€urzeler/Zuhr, Munich,
Germany; 2Department of Periodontology,
Centre for Dental, Oral, and Maxillofacial
Medicine (Carolinum), Johann Wolfgang
Goethe-University Frankfurt/Main, Frankfurt,
Germany; 3Department of Operative Dentistry
and Periodontology, University Dental
School, University of Freiburg, Freiburg,
Germany
Key words: donor sites; graft harvesting; soft
tissue augmentation; soft tissue replacement
graft; soft tissue substitute; subepithelial
connective tissue graft
Accepted for publication 16 October 2013
The use of soft tissue replacementgrafts has become a substantial ele-ment in plastic periodontal andimplant surgery. The application of
soft tissue autografts has character-ized the last 50 years of clinical peri-odontology, and till today – morethan ever – a variety of soft tissuegrafting interventions is carried outwith two different targets being pur-sued: increasing the width of kerati-nized tissue and increasing soft tissuevolume. In the beginning of the eraof mucogingival surgery, surgicalinterventions were performed based
on the belief that a minimal width ofkeratinized gingiva would berequired to maintain the periodontaltissues healthy and stable (Nabers1954, Ochsenbein 1960, Friedman &Levine 1964, Sullivan & Atkins1969, Carranza & Carraro 1970,Hall 1981, Matter 1982). A mini-mum of 1 mm to 3 mm of kerati-nized gingiva was believed to bemandatory (Corn 1962, Bowers
Conflict of interest and source offunding statement
The authors declare that they have noconflict of interest. This review articlehas been self-funded by the authors.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd S123
J Clin Periodontol 2014; 41 (Suppl. 15): S123–S142 doi: 10.1111/jcpe.12185

1963, Lang & Loe 1972). In the1960s, it was assumed that the tissuearound teeth adapts to functionalrequirements when subjected tophysical impacts during mastication(Ivancie 1957, Orban 1957, Bradleyet al. 1959, Pfeifer 1963). As a conse-quence, denudation techniques (Och-senbein 1960, Bohannan 1962, Corn1962, Wilderman 1964), periostealretention procedures (Staffileno et al.1962) and apical repositioned flaps(Friedman 1962) were recommendedto increase the width of the kerati-nized gingiva. As the role of inherentfactors regarding genetic determina-tion of gingival tissues became clearlater on (Karring et al. 1971, 1974,1975), the use of pedicle grafts andin particular free epithelializedgrafts, usually referred to as free gin-gival grafts (FGG), was proposedinstead (Haggerty 1966, Nabers1966, Sullivan & Atkins 1968, Edel1974).
When it was subsequently real-ized that the biological significanceof a sufficient wide keratinized gin-giva was doubtlessly overrated in thepast (Miyasato et al. 1977, Hangor-sky & Bissada 1980, Lindhe &Nyman 1980, de Trey & Bernimou-lin 1980, Dorfman et al. 1982, Schoo& van der Velden 1985, Kisch et al.1986, Salkin et al. 1987), the clinicalimportance of FGGs to increase thewidth of the keratinized gingivamore and more decreased. Insteadperiodontists started to use the FGGfor aesthetic corrections like soft tis-sue recession coverage (Bernimoulinet al. 1975, Miller 1982) and soft tis-sue ridge augmentation (Seibert1983) as well as for socket preserva-tion in aesthetically relevant areas(Landsberg & Bichacho 1994). Theseadvancements of soft tissue augmen-tation procedures were marked by asense of aesthetics among patients,which had not been present in thedental community in this formbefore. This meant a fundamentalchange regarding the indications ofsoft tissue autografts in periodontol-ogy. However, as much as the FGGhad proven for increase in the widthof keratinized gingiva, as much itslimitations, both regarding the quan-titative (volume augmentation) andqualitative outcomes (aesthetic inte-gration, surface, colour, scarring),were obvious when it was appliedfor soft tissue re-construction in aes-
thetic indications. In search of betteralternatives it soon became clear thatthe predictability regarding the aes-thetic outcome was much higherwhen using a subepithelial connec-tive tissue graft (SCTG) (Langer &Calagna 1980, Langer & Langer1985, Raetzke 1985, Nelson 1987,Harris 1992, Allen 1994, Bruno1994). The further development ofsoft tissue autografts from the FGGto the SCTG represents a paradigmshift, which is conceptually anchoredin the literature by the transitionfrom classical mucogingival surgeryto plastic periodontal surgery. Todaysoft tissue augmentation only occa-sionally means widening of the gin-giva or peri-implant mucosa in thecontext of plastic periodontal andimplant surgery. It is rather indi-cated for soft tissue recession treat-ment at teeth (Cairo et al. 2008,Chambrone et al. 2010, 2012, Cortel-lini & Pini Prato 2012) or implants(Burkhardt et al. 2008, Roccuzzoet al. 2013, Zucchelli et al. 2013), forridge preservation procedures withimmediate implants or fixed partialdentures (Esposito et al. 2012, Langet al. 2012), for soft tissue ridge aug-mentation associated with implantsor fixed partial dentures (Thomaet al. 2009, Schneider et al. 2011,Sanz et al. 2012) and for papillareconstruction (Nemcovsky 2001,Nordland et al. 2008). Furthermore,it might be recommended for softtissue thickening to stabilize the gin-giva, for example. before orthodon-tic (Steiner et al. 1981, Wennstromet al. 1987) or restorative (Ericsson& Lindhe 1984) treatment and tomask discoloured roots or shiningthrough implant components (Junget al. 2007).
Considering the challenges ofsoft tissue augmentation proceduresin plastic periodontal and implantsurgery today, the FGG has conse-quently disappeared from the aes-thetic zone and its scope ofapplication has been limited to pro-cedures increasing the keratinizedtissue around teeth and implants inaesthetically irrelevant zones. Forthat reason, this review dispensesFGGs and concentrates on SCTGsand their potential substitutes forsoft tissue recession treatment andsoft tissue volume increase. Theaim of this review was therefore toanalyse the dental literature regard-
ing soft tissue grafting techniquesin plastic periodontal and implantsurgery and to provide clinicalstrategies for soft tissue replacementgraft procedures. Based on scientificevidence and clinical experience itis supposed to (I) analyse and dis-cuss the advantages and shortfallsof different donor sites and har-vesting techniques as related toautogenous soft tissue grafts and(II) to provide clinical guidelinesfor predictable and successful treat-ment outcomes and (III) give aglobal perspective on current andfuture possibilities with soft tissuesubstitutes.
Anatomical landmarks
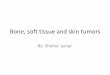
The oral mucosa can be divided intothree portions: the specialized sen-sory mucosa (taste buds on dorsumof the tongue), the lining mucosa(lips, cheeks, vestibule, floor of themouth, base of the tongue and softpalate) and the masticatory mucosa(gingiva and hard palate) (Orban &Sicher 1945). The masticatorymucosa of the hard palate is com-posed of three histologic layers: theepithelium, and the subepithelialconnective tissue with the laminapropria and the submucosa (Fig. 1).The epithelium is characterized byorthokeratinization and about300 lm thick, its structure basicallycorresponding to that of the gingivalepithelium. The lamina propriabelow the palatal epithelium is verycoarse tissue. It contains a high pro-portion of inter-cellular substance,which is produced by fibroblasts.This extracellular matrix is responsi-
Fig. 1. Clinical view of a thick free epi-thelialized graft without periosteum har-vested from the lateral palate to illustratethe histological composition of the pala-tal masticatory mucosa: covering epithe-lium and subepithelial connective tissueincluding lamina propria and submucosa.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S124 Zuhr et al.

ble for the mechanical properties ofthe tissue layer. It consists predomi-nantly of collagen fibrils mainly withtype I and II and few type V and VIcollagen. Elastic fibres are hardlypresent. The lamina propria isdivided into the papillary portionand the reticular portion. The papil-lary portion shows finger-like projec-tions that inter-lock with theoverlying epithelium whereas thereticular portion consists of thickand dense reticular fibres. The sub-mucosa is a connective tissue layer,which attaches the lamina propria tothe periosteum of the underlyingbone. Numerous glands, nerves andadipose tissue are present in this tis-sue layer. Its thickness can varybetween patients and within thesame individual (Muller et al. 2000).The submucosa is characterized by arather fatty zone in the anterior andcopious glands (Gll. Palatinae) in theposterior area whereas it is in gen-eral less pronounced in the posteriorthan in the anterior part of the pal-ate. In a histologic evaluation ofhuman SCTGs from the anteriorpalate by Harris, large differences inthe histologic composition werefound: some grafts consisted almostonly of lamina propria and in somegrafts the greatest proportion wassubmucosa with mainly adipose tis-sue (Harris 2003). The portion of thelamina propria varied between 21.1and 100% of the graft (mean65.2%). These results confirm theclinical observation that the dimen-sions of the different subepithelialconnective tissue layers vary substan-tially from patient to patient.
The thickness of the masticatorymucosa at the palate has been evalu-ated in different studies. Eger andM€uller determined the thickness withultrasonic devices (Eger et al. 1996,Muller et al. 2000). They found thatthe soft tissue thickness at the tuber-osity area was highest with morethan 4 mm, followed by the palatalmasticatory mucosa at the secondmolars and pre-molars with an aver-age of 3 mm. In general, the thick-ness was found to be higher in menthan in women. In a computertomo-graphic study by Song and cowork-ers, it was found to be3.83 � 0.58 mm with females havinga thinner (3.66 � 0.52 mm) mucosathan men (3.95 � 0.60 mm) and anincreasing thickness with increasing
age (Song et al. 2008). Furthermore,there was a tendency for an increasefrom the canine to the second pre-molar, a decrease at the first molarand an increase again at the secondmolar. The second pre-molar regionshowed to be thickest with a meanof 3.81 � 0.75 mm and the firstmolar region the thinnest with3.13 � 0.69 mm. In a cadaver studyby Gapski and coworkers, the softtissue thickness at the tuberositycame out to be 2.5–4 mm (Gapskiet al. 2006). Apparently, the subepi-thelial connective tissue from thetuberosity area is a very dense,coarse and collagen-rich tissue thatseems to contain less fat and glandu-lar tissue, but much more collagenthan that from the anterior lateralpalate.
The arterial blood supply of thepalate is provided by the greater pal-atine artery (GPA), a branch of themaxillary artery, which emergesfrom the greater palatine foramen. Itruns through a groove lateral to thegreater palatine nerve (GPN) andsubmits branches to the palatalmucosa and the gingiva, continu-ously decreasing its diameter andends at the incisive canal, where itanastomoses with the sphenopalatineartery. The innervation of themucosa and gingiva at the hard pal-ate is provided by the GPN, whichemerges also through the greater pal-atine foramen and traverses medialto the GPA, subdividing into severalbranches, which are becoming thin-ner towards the epithelial layer.Between the GPA and the GPN, acrest is present, which can in mostcases be palpated clinically (Bennin-ger et al. 2012).
With respect to potential compli-cations of harvesting SCTGs fromthe palate, the palatine neurovascu-lar bundle is a very important andclinically relevant anatomical struc-ture to be protected. Therefore, hav-ing a general idea of the possiblecourse of the palatine artery isessential. For this reason, differentanatomical studies were set up withthe objective to work out reliablereference points and guidelines thatcan be used by clinicians to preventdamage to the GPA during SCTGharvesting in a given clinical situa-tion. In an anatomical study of theGPA and related bony structures ofthe hard palate in 41 cadavers, Klo-
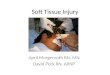
sek and Rungruang found that theGPF was most frequently found inthe region near the apices of thesecond and third molars, in the areawhere the vertical and horizontalsegments of the palatine bone cometogether (Klosek & Rungruang2009). Ikuta and coworkers foundin a cone beam computed tomogra-phy study that the GPF was locatedin 92 of 100 cases in the third molarregion and in an average distance of7.9 mm from the alveolar ridge (Ik-uta et al. 2013), whereas a study inIndian skulls observed the GPF tobe in the third molar region in only73% of the cases (Sharma & Garud2013). Monnet-Corti and coworkers,who measured the distance of themain branches of the GPA from thepalatal gingival margin in 198 plas-ter models of periodontally healthypatients, found that the average dis-tance from the gingival margin tothe GPA ranged from approxi-mately 12 mm in the canine area toroughly 14 mm at the second molarlevel (Monnet-Corti et al. 2006).The authors concluded that itshould be possible to harvest aSCTG measuring 5 mm in height inall patients and 8 mm in height in93% of patients without a risk ofdamaging the GPA. However, acadaver study by Fu and coworkersrevealed that the predicted locationof the GPA based on the aforemen-tioned study cast measurementstended to be inaccurate and that thepredicted distance between the GPAand the cementoenamel junction ofthe first molars and pre-molarstended to be underestimated (Fuet al. 2011). This is in correspon-dence to findings by Benninger andcoworkers, who measured an aver-age distance of 12 mm (range 9–16 mm) between the first molar andthe GPA (Benninger et al. 2012). Toestablish a guideline for clinicians tolocalize the GPA, the authorsassumed that in most cases theGPA would be found at a distanceof 76% of the palatal height mea-suring from the cementoenameljunction of the first molar. Otherevidence suggests that the height ofthe palatal vault is related to thecourse of the greater palatine artery:The shallower the palatal vault, thecloser the palatine artery gets to thepalatal gingival margin (Reiser et al.1996) (Fig. 2).
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S125

Donor site selection
It is beyond all question that amongsuitable donor sites for intra-oralSCTG harvesting only those comeinto consideration that promise anadequate amount of obtainable tis-sue. They should not be associatedwith major health risks and go alongwith acceptable patient morbidity.Under these requirements and inconsequence of the anatomical softtissue conditions in the oral cavitytwo areas of interest for autograftharvesting have emerged as the areasof choice: the anterior and theposterior palate, whereas in the pos-terior area the tuberosity and the lat-eral palate can be distinguished.
In general, the grafts from the dif-ferent eligible sites differ in their geo-metric shape: grafts from thetuberosity are more voluminous,those from the posterior lateral palaterather thin, whereas those from theanterior palate can often be extensivewith a large surface. This has an influ-ence on the indication they areintended for. For example, an alveo-
lar ridge augmentation is rather per-formed with a voluminous graft fromthe tuberosity area whereas a reces-sion coverage can also be done with athin and small dimensioned graftfrom the posterior lateral palate.Should the clinical situation requirechanging the geometry of a givengraft, the transplant can be modifiedby folding and suturing grafts fromthe lateral palate or by slicing andunfolding grafts from the tuberosityarea. As the dimensions of the masti-catory mucosa at the palate vary sub-stantially from patient to patient(Eger et al. 1996, Muller et al. 2000,Harris 2003, Gapski et al. 2006, Songet al. 2008), it is important for the cli-nician to quickly overview theamount of available tissue at the pos-sible donor sites. To do so, a goodand simple option is using an end-odontic needle with a silicon discapplied to it (Studer et al. 1997, Pao-lantonio et al. 2002, da Silva et al.2004, Joly et al. 2007). In this con-text, Zucchelli and coworkersassumed that in addition to measur-ing soft tissue thickness at the palateendodontic needles might also beused to estimate the composition ofthe subepithelial connective tissue.The authors believed that due to dif-ferent penetration resistances towardsthe needle the transition between lam-ina propria and the adipose submu-cosa could be felt in many situations(Zucchelli et al. 2010).
Besides their geometry, graftsfrom different donor sites vary intheir histologic composition (Harris2003). It may be speculated thatthese differences not only accountfor variable volume stability but alsoinfluence the physiologic process ofgraft re-vascularization. From clini-cal experience, it seems in this con-text as if subepithelial connectivetissue from the tuberosity and theposterior lateral palate was denserand firmer than that from the ante-rior palate. It can be assumed that itis therefore less susceptible to post-operative shrinkage. On the otherhand, this very dense and coarseconnective tissue appears to undergonecrosis more easily than that fromthe anterior palate. It may behypothesized that compared to therather loose formation of the subepi-thelial connective tissue from theanterior palate, the dense tissue fromthe posterior area does not comply
as good with the requirements forgraft survival in the course of plas-matic circulation and re-vasculariza-tion during the early postoperativephase. As a clinical consequenceSCTGs from the posterior palateseem – in contrast to SCTGs fromthe anterior area – to need beingfully covered by a flap to ensurehealing by primary intention. It ispresently unclear to what extent itmight play an additional role in thiscontext if, depending on theemployed harvesting technique, theperiosteum covering the palatal boneis included in the graft or not.
SCTGs can also be harvestedfrom the palate with covering epithe-lium according to FGGs, providedthat they are deepithelialized extrao-rally. This approach has the advan-tage that SCTGs can also be takenin situations with a very thin masti-catory mucosa and that the graftpreparation itself can be performedmore superficially, thereby not vio-lating blood vessels and nerve fibresrunning in deeper layers. In thisway, transplants with more extensivesurfaces can be gained in a shortamount of time and the allegedlyhigh-quality tissue layer of the lam-ina propria can be used to fullextent as no parts of it remain in theflap at the donor site like in under-mining harvesting techniques. Onthe other hand, this procedure mightadversely affect patient morbidity:In several clinical studies it could bedemonstrated that a more painfulpost-operative course could beobserved in FGG patients with apalatal wound healing by secondaryintention in contrast to SCTGpatients where a flap was raised, thegraft harvested internally and thewound allowed to heal by primaryintention (Farnoush 1978, Jahnkeet al. 1993, Del Pizzo et al. 2002,Griffin et al. 2006, Wessel & Tatakis2008). However, these results arecontrary to a recent clinical studyidentifying influencing factors forpain sensation after FGG removal(Burkhardt et al. in preparation)and a randomized controlled clinicaltrial (RCT) comparing patient mor-bidity after FGG and SCTG har-vesting procedures (Zucchelli et al.2010). In both studies it could bedemonstrated that post-operativepain was rather influenced by thethickness of the graft and the
Fig. 2. The blood vessels that supply thelateral palate region can be seen in thisanatomical specimen. The greater pala-tine artery emerges from the greater pala-tine foramen and extends along thelateral palate in an anterior direction.Due to its size, injury to the greater pala-tine artery, particularly in its distal seg-ment, can be expected to result inmassive bleeding. It is therefore crucial totake precautions to prevent damage tothe artery when subepithelial connectivetissue grafts are harvested from thepalate.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S126 Zuhr et al.

remaining soft tissue at the palate,but by primary or secondary woundhealing at the donor site. It can bementioned as an aside that in thelatter study, the deepithelializedautografts consisting of lamina pro-pria only led to a statistically signifi-cant higher increase in buccalgingival thickness following reces-sion coverage (Zucchelli et al. 2010).These findings support the afore-mentioned clinical observation thatSCTGs containing presumed densersubepithelial connective tissue arecomparatively less prone to postop-erative shrinkage. The clinical expe-rience that using SCTGs that areharvested with epithelium and deepi-thelialized outside the oral cavityseem to bear an increased risk forpostoperative scar tissue formationat the recipient site should not beneglected, though. At this point oftime any attempted explanationwould be speculative in nature,although it would be possible that incontrast to SCTGs from deep sub-epithelial connective tissue zonesSCTGs consisting mainly of a super-ficial layer of subepithelial connec-tive tissue behave more similar toFGGs with all the negative conse-quences for the qualitative treatmentoutcomes outlined above (aestheticintegration, surface, colour, scar-ring). This might potentially becaused by isolated fragments of epi-thelium that are left in the graftafter deepithelialization, especiallydue to the papillary inter-lockingbetween the epithelium and the lam-ina propria. In a study by Harris,SCTGs were manually deepithelial-ized at the best optical control bythe surgeon (Harris 2003). Thesubsequent histological analysis,though, could demonstrate remain-ing epithelium in 80% of the grafts.In addition, “more aggressive” mor-phogenetic stimuli regarding the dif-ferentiation of the coveringepithelium at the recipient site couldbe suspected in more superficial lay-ers of subepithelial connective tissue(Ouhayoun et al. 1988). If it wouldmake a difference for this reason toposition the superficial side of thegraft inwards or outwards in therecipient bed could be an interestingfield of future research (Fig. 3).
In summary, it can be stated that– although the actual reasons arelargely unknown up to date – grafts
from different donor sites seem tohave different characteristics thatmight require selective clinical appli-cation and well thought out surgicalprotocols. The clinical decisionwhere to harvest soft tissue auto-grafts from is presently hardly basedon written evidence, but rather relieson clinical experience and dependson the amount of available tissue atthe eligible donor sites, the indica-tion in which the transplant is sup-posed to be used and last, but notleast on the personal preference ofthe treating surgeon.
Harvesting techniques
The clinical procedure of SCTG har-vesting from the palate is often char-acterized by the remarkablechallenge of obtaining the largestvolume of tissue possible on one sidewhile minimizing post-operative painand reducing the risk of complica-tions on the other side. To meetthese requirements, various proce-dures for soft tissue autograft har-vesting in plastic periodontal andimplant surgery have been developedand described in the literature:
SCTG harvesting from the lateral palate
The different SCTG harvesting tech-niques from the lateral palate vary
basically in the particular positionof the donor site, the number andtype of surface incisions and in theflap design for gaining access to thegraft. In principle, they can be sub-divided into techniques that provideSCTGs with or without a remainingcollar of keratinized epithelium.Relating to the group of SCTGswith epithelium, Langer and Cala-gna as well as Langer and Langerintroduced a harvesting methodbased on a rectangular incisiondesign with two horizontal and twovertical incisions resulting in SCTGs
with an epithelial collar of about2 mm width (Langer & Calagna1980, 1982, Langer & Langer 1985).Subsequently, Harris used a verysimilar approach and modified thetechnique by limiting the verticalincisions to a minimal dimension,barely enough to get access to theunderlying donor tissue (Harris1992). Raetzke, finally, abstainedfrom vertical incisions completelyand used two converging horizontalcrescent-shaped incisions resulting ina wedge-shaped SCTG with an epi-thelial collar (Raetzke 1985). How-ever, the disadvantage of all thesetechniques obtaining SCTGs includ-ing parts of the epithelium was –beside the aforementioned negativeconsequences for the qualitative-aes-
(a) (b)
(c) (d)
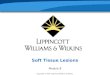
Fig. 3. Clinical view of soft tissue grafts harvested from the different possible donorsites with varying geometric shape and histologic composition: from the anterior lat-eral palate (a), from the posterior lateral palate (b), from the lateral palate, deepitheli-alized extraorally (c) and from the maxillary tuberosity (d).
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S127

thetic treatment outcomes – that thedonor site could not be completelycovered with the flap and was there-fore partially healing by secondaryintention. Due to the rigidity of thepalatal masticatory mucosa thiscould only be avoided if SCTGswere harvested without epithelium.In consequence, Edel introduced atrap-door approach without remov-ing epithelium from the donor site(Edel 1974). By undertaking onehorizontal and two vertical inci-sions, an access flap could beraised, the graft removed and com-plete wound closure achieved. How-ever, particularly in cases withunfavourable relations between flapbase and pedicle length flap slough-ing could be observed causingunnecessary discomfort for thepatient (Edel 1974, Harris 1994,1997). This is why H€urzeler andWeng proposed a single-incisiontechnique for SCTG harvestingfrom the lateral palate later on(Hurzeler & Weng 1999). The exe-cution of only one horizontal sur-face incision followed by anundermining flap preparationseemed to positively affect post-operative healing and patient mor-bidity compared with the trap-doortechnique (Del Pizzo et al. 2002,Wessel & Tatakis 2008). In the fol-lowing, three distinct and obviouslyfrequently applied techniques toharvest SCTGs from the lateral pal-ate will be proposed: SCTG har-vesting from the anterior palate,SCTG harvesting from the posteriorlateral palate and SCTG harvestingfrom the lateral palate by obtaininga graft with epithelium correspond-ing to a FGG that is deepithelial-ized extraorally. In this respectideally those surgical protocolsshould be picked out that have sci-entifically proven to be the presentlybest possible treatment options.However, at the time being it is inthis context hardly possible tochoose one approach over the otherone based on scientific evidence.For this reason, those clinical proce-dures were selected that seem toreflect a contemporary mindset andpresently seem to be based uponsound clinical experience if SCTGsare harvested from the lateral pal-ate. The subsequent SCTG harvest-ing step by step descriptions arebased on clinical recommendations
given in two recently published text-books (Zuhr & H€urzeler 2012, Zuc-chelli 2013).
SCTG harvesting from the anterior palate
The procedure starts according tothe single-incision technique with ahorizontal incision along the row ofteeth starting from the mesial borderof the first molar to the lateral inci-sor, 2.0 mm apical to the gingivalmargin, 1.0–1.5 mm deep. All theremaining incisions are underminingbelow the mucosal surface. Withregard to post-operative pain, itseems to be the main challenge froma surgical point of view to achieveprimary wound healing at the palataldonor site. In this context, it appearsto be essential to guarantee an ade-quate postoperative blood supply forthe access flap and therefore preparea partial-thickness flap of uniformthickness and proper dimension. Forthis reason, it is mandatory to per-form the initial horizontal incisionwith a scalpel held strictly perpendic-ular to the palatal surface. To ensurethat the following split-thickness flappreparation will provide a flap ofsufficient dimension throughout, it isimportant to gradually increase theangle of the blade until it is parallelto the palatal surface by makingrepeated distal to mesial movements,mainly with the tip of the scalpel.Care must be taken to ensure thatthe flap preparation is not substan-tially extended more than 10 mmapical from the cementoenamel junc-tion of the maxillary posterior teeth.If placed roughly 2 mm from the ce-mentoenamel junction, the initialincision can be safely extended api-cally to a depth of approximately8 mm without a risk of damagingthe great palatine artery. As the cut-ting portion of a No. 15 scalpelblade is approximately 8 mm inlength, it can serve as a gauge forsafe graft harvesting on this occa-sion. After that the size of the graftis defined by executing two horizon-tal and two vertical incisions insidethe created envelope. They should beextended to the bone and overlap atintersections. It might be advisableto place the coronal internal incisionroughly 1.0–1.5 mm apical to the ini-tial horizontal incision. This ensuresthat the access flap will rest on awell-perfused connective tissue sur-
face instead of on bone or perios-teum after surgery, which mightimprove the predictability to achievehealing by primary intention.Depending on the clinical indicationand how much tissue is available,SCTGs can be obtained with orwithout periosteum. Grafts withperiosteum are harvested by bluntdissection using a periosteal elevator.For graft removal without perios-teum, an additional offset incision iscarried out above the periosteum bysharp dissection with a scalpel blade.Although leaving periosteum on thebone has probably positive conse-quences in terms of post-operativewound healing, clinical experiencehas shown that SCTGs with perios-teum have superior mechanical sta-bility, which might be an advantagerelating to the clinical handling ofthose grafts in certain situations. Forthe following wound closure paralleland crossed horizontal sling suturesare recommended. The placement ofthis type of sutures around the max-illary posterior teeth has a woundcompressing effect that might bebeneficial particularly in terms ofpromoting hemostasis and primaryadaptation of the wound margins(Zuhr & H€urzeler 2012) (Fig. 4).
SCTG harvesting from the posterior
lateral palate
The harvesting procedure is carriedout at the first and second maxillarymolars and usually contains one hor-izontal and two vertical incisionsaccording to the trap-door approach.Depending on the soft tissue thick-ness at the donor site and the size ofthe graft to be harvested one or inindividual cases even both verticalincisions can be omitted. While thehorizontal incision is performed 1–2 mm apical of the gingival margin,the two vertical incisions shouldextend 1 mm further than theintended apicocoronal dimension ofthe graft offering access to the apicalincision line in the connective tissuelater on. A split-thickness flap isthen prepared parallel to the externalmucosal surface by watching theblade working from outside underthe flap. By doing so, the goal is tocreate a flap of uniform thickness,whereby the releasing incisions canbe used as flap thickness guides.Now the horizontal incision of the
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S128 Zuhr et al.

graft is made along the horizontalincision of the flap perpendicular tothe underlying bone and the mesialand distal internal incisions aredone. Consequently, the blade isrotated to be parallel to the externalsurface and a second underminingincision with the scalpel is performedattempting to maintain uniform graftdimensions in the aspired graftthickness. Then the connective tissueis freed apicocoronally and mesiodis-tally before making the apical inci-sion almost perpendicular to thebone surface to completely detachthe SCTG. At the end, single inter-rupted sutures can be used to pri-marily adapt the wound margins andtherefore provide the donor site forhealing by primary intention (Zucch-elli 2013) (Fig. 5).
SCTG harvesting from the lateral palate
with a FGG that is deepithelialized
extraorally
At first, two horizontal and two verti-cal incisions are performed accordingto the size of the area to be grafted,
perpendicular to the mucosal surface,1.0–1.5 mm deep. Now the blade isrotated to be almost parallel to themucosal surface and moved apicallyas far as a FGG of uniform thicknessis mobilized being 0.5 mm thickerthan actually needed. Subsequently,compressive sling sutures anchored tothe soft tissue apical to the palatalwound area are applied. The graft isthen positioned on sterile gauze,moistened with a saline solution anddeepithelialized with a sharp scalpelblade held parallel to the externalgraft surface. To distinguish betweenepithelium und subepithelial connec-tive tissue and therefore make surethat the epithelium is completelyremoved from the graft the use ofmagnification aids is recommended(Zucchelli 2013) (Fig. 6).
SCTG harvesting from the maxillary
tuberosity
Technically, the clinical procedurefor harvesting SCTGs from the max-illary tuberosity corresponds to thatfor the distal wedge technique in re-
sective periodontal surgery. It is eas-ier to perform if the terminal toothis the first molar, but it can also beaccomplished with second or thirdmolars present. The procedure startswith two converging incisions per-pendicular to the tissue surface and1.0–1.5 mm deep as far distal to thelast molar as possible while remain-ing within the masticatory mucosa.Then, an undermining partial-thick-ness incision buccal and palatal upto the mesial surface of the lastmolar is made. The scalpel is guidedsuccessively parallel to the buccal orpalatal soft tissue surfaces to yield apartial-thickness flap of uniformthickness throughout. After a supra-periosteal incision is made thewedge-shaped graft is removed fromthe donor site by sharp dissection.The covering epithelium on theupper part of the graft is conse-quently removed extraorally. Thedonor site is closed with an externalhorizontal mattress suture anchoredto the periosteum. Additional singleinterrupted sutures can be used tocompletely close the wound (Zuhr &H€urzeler 2012) (Fig. 7).
Independently of the selecteddonor site and the applied SCTGharvesting technique, it takes a cer-tain amount of time from themoment when the graft is takenfrom the palate until the wound atthe palatal donor site is closed. Inthe meantime care should be takento prevent graft dehydration, forexample by storing the SCTG ingauze soaked in physiologic salineuntil further use. Extraoral modifica-tion in SCTGs is often necessary. Aproven way to do this is to firstspread and press the graft on a wetglass slab using a surgical forceps. Afresh scalpel blade is then applied tocut the graft to the desired size andshape and to thin the SCTG asneeded. Due to the possibility to actas a barrier to plasmatic circulationand re-vascularization during theearly phase of healing fat and glan-dular tissue remnants detected onthe graft should be removed (Sulli-van & Atkins 1968).
The routine use of surgical stentsafter harvesting SCTGs from the lat-eral palate is recommended for manyreasons. First, the stent applies pres-sure to the wound, which seems topromote post-operative flap adapta-tion and wound healing. Second, the
(a) (b)
(c) (d)
Fig. 4. (a) If the initial incision is placed approximately 2 mm from the gingival mar-gin of the maxillary posterior teeth, the current scientific evidence suggests that itwould be virtually impossible to damage the greater palatine artery or its majorbranches if the subepithelial connective tissue graft is harvested no more than 8 mmapical to the initial incision line. Because the cutting portion of a No. 15 scalpel bladeis roughly 8 mm in length, it can serve as a gauge for safe graft harvesting. (b) Clinicalexperience has shown that it is much easier to achieve primary wound healing if theinitial and coronal harvesting incisions are slightly offset to create a small shelf of softtissue on which the palatal access flap can rest postoperatively. (c) Subepithelial con-nective tissue grafts from the anterior lateral palate can be comparatively extensiveand include to some extent fatty tissue. (d) Postoperative situation after wound closureby application of parallel and crossed horizontal sling sutures.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S129

stent enables a rapid and effectiveresponse to intra-operative or post-
operative bleeding. Third, the stentnot only protects the palatal donor
site from mechanical irritation butalso seems to enhance patient com-fort considerably during the firstpostoperative days. The results of aRCT by Thoma and coworkers indi-cate that the application of a colla-gen matrix at the palatal woundmight additionally enhance soft tis-sue healing and re-epithelization atearly time points if an extraorallydeepithelialized FGG was harvested(Thoma et al. 2012). The use of asurgical stent is not required afterSCTG harvesting from the maxillarytuberosity.
The amount of tissue needed fordefect re-construction is potentiallygreater than the amount of tissueavailable, even if harvested fromboth sides of the palate. Therefore,it is sometimes necessary to harvestsubepithelial connective tissue fromthe palate at two different times.Harris and coworkers could demon-strate that this approach causes nosignificant problems if the secondprocedure is performed after a 2- to3-month interval (Harris et al. 2007).
Tissue integration and volume
stability
In contrary to vascular or pediclegrafts, free grafts are avascular andhave no direct blood supply. There-fore, the survival of vital, tissue-spe-cific cells in a free autologous graftdepends on an early and adequateblood supply from the recipient bedand the overlying flap by means ofplasmatic circulation and, later on,by means of re-vascularization of thegraft.
The healing of FGGs has beenstudied in a variety of animal experi-ments (Oliver et al. 1968, Jansenet al. 1969, Nobuto 1986, 1987,Nobuto et al. 1988). It can beassumed that their results regardingthe basic concepts of soft tissueautograft integration can at leastprincipally be transferred to thehealing process of SCTGs: Duringthe initial phase of healing, thegrafted tissue survives exclusively byavascular plasmatic circulation fromthe recipient bed. Apart from theirlimited intra-cellular energyresources, the grafts are entirelydependent on the influx of oxygenand metabolites within the extracel-lular fluid, the driving force behindthis diffusion process being the con-
(a) (b)
(c) (d)
Fig. 5. (a) The harvesting procedure at the posterior lateral palate equals a trap-doorapproach: it usually contains one horizontal and two vertical incisions. (b) A split-thickness flap is then prepared parallel to the external mucosal surface creating a flapof uniform thickness, whereby the releasing incisions can be used as flap thicknessguides. (c) Subepithelial connective tissue grafts from the posterior lateral palate arelimited in size compared to those from the anterior palate, but are suggestive to con-tain less fatty tissue. (d) Horizontal sling sutures can be used to compress the woundarea and adapt the flap margins as good as possible.
(a) (b)
(c) (d)
Fig. 6. (a) Two horizontal and two vertical incisions are performed according to thesize of the area to be grafted, perpendicular to the mucosal surface, 1.0 to 1.5 mmdeep. Then the blade is rotated in order to be almost parallel to the mucosal surfaceand moved apically. (b) A free gingival graft of uniform thickness is mobilized being0.5 mm thicker than actually needed. c The graft is then positioned on a sterile glassplate, moistened with a saline solution and deepithelialized with a sharp scalpel bladeheld parallel to the external graft surface. To distinguish between epithelium und sub-epithelial connective tissue and therefore make sure that the epithelium is completelyremoved from the graft the use of magnification aids is recommended. (d) The donorsite is left for healing by secondary intention.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S130 Zuhr et al.

centration gradient between thenative and the transplanted tissues.The thinner the initially formed exu-date between bed and graft and themore immobile the graft is, the eas-ier plasmatic circulation can occurand the more living cells can survive.From the third to fourth post-opera-tive day on the re-vascularizationphase begins. During this time, Nob-uto and coworkers observed a medi-ator-stimulated ingrowth ofcapillaries from the wound bed intothe graft and the formation of anas-tomoses between blood vessels of therecipient bed and the transplantedtissues – the blood circulation isreestablished by reusing the pre-existing vascular network of thegraft (Nobuto 1986, 1987, Nobutoet al. 1988). After the fifth post-operative day, the vessels increasetheir continuity and form a vascularlayer in the graft–bed junction, afinding that coincides with observa-tions in dye-injected sections by Jan-sen and coworkers (Jansen et al.1969). From the seventh day on theconnection of existing vessels by hor-
izontal anastomoses can beobserved. Capillary budding takesplace throughout the graft and afibrous union with the graft bed isestablished. Capillaries proliferateand re-build a dense vascular net-work extending beyond the pre-exist-ing graft margins. Simultaneous tothe re-vascularization process, exfoli-ation of the epithelium on the graftcan be observed and re-epithelializa-tion occurs mainly by proliferationof epithelium from the adjacent tis-sues, indicating that the survival ofthe graft depends on the trans-planted connective tissue layer only.Subsequent to the re-vascularizationphase, from the 11th post-operativeday on, the maturation phase sets in.At this point of time, the amount ofblood vessels is gradually reduced toa number that is usually found inthe oral mucosa, whereas the epithe-lium simultaneously matures withthe formation of a keratin layer.Only few changes can be observed inthe following time and after about3 weeks the demarcation zonesbetween graft and flap or periosteum
cannot be detected anymore (Gargi-ulo & Arrocha 1967). The results ofthe above-quoted animal experi-ments could partially be confirmedin a clinical study by M€ormann andcoworkers (Mormann et al. 1975).Under the use of fluorescein angiog-raphy, the post-operative diffusionand re-establishment of capillaryblood circulation could be investi-gated. The authors observed the for-mation of capillary loops betweenthe seventh and 14th post-operativeday and concluded that blood circu-lation in FGGs is re-established pri-marily by capillary budding.
Wound healing and clinical outcomes in
avascular beds
When using SCTGs to cover soft tis-sue recessions at teeth or implants,part of the recipient site will be theavascular root or implant surface.Consequently, graft survival dependson a sufficient blood supply originat-ing from the vascular recipient bedadjacent to the recession defect andthe covering flap (Fig. 8). In anexperimental study by Guiha andcoworkers, artificially created gingi-val recessions were treated under theuse of SCTGs harvested from thepalate (Guiha et al. 2001). Histologi-cal evaluation was performed at 7,14, 28 and 60 days after surgerydemonstrating re-vascularization ofthe grafts by capillary proliferationoriginating from the periodontalplexus, the supraperiosteal plexusand the overlying flap. The trans-planted tissues seemed to be vascu-larized completely after 14 days andafter 28 and 60 days demarcationzones between graft and flap or peri-osteum could not be identified any-more. In contrary, a few 2-weekspecimens showed a bigger dimen-sioned blood clot at the interfacebetween graft and recipient bed and/or graft and flap obviously notallowing blood vessels to penetrateto the graft. The authors assumedthe re-vascularization and healingprocess to have been delayed in theseareas presumably due to a less thanoptimal adaptation of the graft tothe recipient bed. Those parts of thegraft not being in contact with theroot surface and not covered by theflap were not vascularized at all.Basically, small areas of SCTGs notcompletely covered by an overlying
(a) (b)
(c) (d)
Fig. 7. (a) Two converging incisions are made with a No. 15 scalpel blade. Theyshould start at the distal surface of the last molar and extend as far distally as possiblewhile remaining in the masticatory mucosa. The incisions should be made perpendicu-lar to the surface to a depth of approximately 1.0 to 1.5 mm. To harvest as large avolume of tissue as possible, the incisions should include all of the soft tissue aroundthe distal tooth surface. (b) After a supraperiosteal incision was made, the graft isremoved from the donor site by sharp dissection. (c) The wedge-shaped connective tis-sue graft immediately after harvesting. To prevent dehydration, the graft should bestored in gauze soaked in physiologic saline until further use. (d) The donor site isclosed with a crossed periosteal suture. Anchorage of the suture in this manner (by theperiosteum buccally and by the masticatory mucosa palatally) serves two purposes:apical flap repositioning and wound compression. Interrupted sutures can be used toclose the remaining wound areas in the distal region.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S131

flap – a practice occasionally per-formed based on experimental (Kar-ring et al. 1974) and clinical studies(Donn 1978, Mackenzie & Fusenig1983, Ouhayoun et al. 1988, Bor-ghetti & Louise 1994, Bouchardet al. 1994, Cordioli et al. 2001) toenlarge the width of keratinized tis-sue particularly in root coverageprocedures – though, seem not toentail an increased risk for graftnecrosis (Raetzke 1985). In this con-text, Yotnuengnit and coworkersinvestigated 15 patients scheduledfor recession treatment (Yotnuengnitet al. 2004) based on the envelopetechnique (Raetzke 1985). They mea-sured the areas of the SCTGs beingcovered by a flap in relation to theareas left exposed over the originallydenuded root surfaces and identifieda minimum ratio of 11:1 that shouldnot be substandarded if the goal wascomplete root coverage. The resultsof a clinical investigation by Al-Zah-rani and coworkers indicated that inthis connection the surface orienta-tion of the SCTG had no significanteffect on the clinical outcomes ofeither root coverage or height of ker-atinized tissue (Al-Zahrani et al.2004). Burkhardt and Lang assessedthe outcomes of gingival recessioncoverage using SCTGs in a clinicalstudy (Burkhardt & Lang 2005). Ina split-mouth design, root coveragewas accomplished by conventionalmacrosurgery on one side and bymicrosurgery on the other. Fluores-cence angiography was performed toevaluate the course of healing imme-diately after surgery and 3 and7 days later. The authors could show
that the vascularization of the micro-surgically treated sites was superiorto that of the macrosurgically trea-ted ones immediately after surgeryand after 3 and 7 days post-opera-tively. They could also demonstratea statistically significant superiorityof the microsurgical technique, basedon the percentage of root coverageone year after treatment. As it canbe assumed that the re-vasculariza-tion process is driven by numeroussignalling pathways, more recentresearch focused on the question towhat extent growth factors mightimprove the healing process ofSCTGs. In a clinical study, Lafziand coworkers evaluated the use ofvascular epithelial growth factor inconjunction with SCTGs from thepalate for gingival recession treat-ment (Lafzi et al. 2012). In fact theyobserved better clinical outcomeswhen the growth factors were used,although not statistically significant.A study by Jankovic and coworkerscomparing platelet-rich membraneswith SCTGs for recession treatmentobserved enhanced wound healing inthe first group with similar treatmentoutcomes except for less gain in ker-atinized tissue width (Jankovic et al.2012). Although Cheung andcoworkers also found similar out-come measures for platelet-concen-trated grafts (Cheung & Griffin2004), a RCT by McGuire andcoworkers resulted in statisticallysignificant recession depth reduction,root coverage and recession widthreduction favouring the SCTG(McGuire et al. 2009a). Two otherstudies (Huang et al. 2005, Keceliet al. 2008), in which platelet-richplasma was added to SCTGs inrecession coverage, found no differ-ence in clinical outcomes comparedwith SCTGs alone, except for moregain of keratinized tissue under theimplementation of growth factors inthe study by Keceli and coworkers.
Up to date, the knowledge aboutthe physiologic proceedings of graftre-vascularization is mainly based onhistological studies. This has recentlychanged due to the availability ofnew technologies in combinationwith innovative scientific models tofurther investigate the healing pro-cess of free soft tissue autografts.One promising, forward-lookingmodel was introduced by Lindenblattand coworkers allowing to perform
continuous in vivo monitoring ofskin graft healing by repetitive intra-vital microscopy (Lindenblatt et al.2008). In an experimental study, theauthors were able to show for thefirst time a temporary angiogenicresponse within the capillaries of theskin graft obviously representing areaction to reperfusion and supply ofthe hypoxic graft with proangiogenicfactors (Lindenblatt et al. 2010). Inanother animal experiment of thesame working group, an early in-growth of angiogenic wound bed ves-sels into the existing vascular chan-nels of the skin graft and subsequentcentripetal replacement of the exist-ing graft vessels could be indicated(Calcagni et al. 2011).
Soft tissue healing against a cov-ered root or implant surface typi-cally results in healthy gingival ormucosal conditions without clinicalsigns of inflammation and pocketformation. Different scientific inves-tigations studied the quality and nat-ure of the new tissue attachment topreviously denuded root surfacesafter a combined therapy with pedi-cle soft tissue grafts and SCTGs.While only a few experimental stud-ies (Weng et al. 1998) and humanhistologies (Harris 1999, Goldsteinet al. 2001) could demonstrate a truenew connective tissue attachmentwith new cementum, new bone andinserting PDL fibres in larger quanti-ties, the majority of scientific evalua-tions found that only the mostapical and lateral parts of the reces-sion defects healed by regenerationwith new connective tissue attach-ment, whereas the main body of thepreviously exposed root surfaceshealed with a long junctional epithe-lium and connective tissue adhesion(Harris 1999, Bruno & Bowers 2000,Guiha et al. 2001, Majzoub et al.2001, McGuire & Cochran 2003,Cummings et al. 2005, McGuireet al. 2009a,b). High effort wastaken in the past to develop chemicalroot conditioning agents promotingwound healing outcomes with morenew connective tissue attachment.Citric acid, tetracyclin HCL, fibringlue associated with tetracyclin HCLand sodium hypochlorite were usedin combination with scaling and rootplaning to demineralize the root sur-face and – in doing so– to exposethe collagen fibres of the dentinematrix and allow their inter-locking
Fig. 8. When using subepithelial connec-tive tissue grafts to cover soft tissuerecessions at teeth or implants, part ofthe recipient site will be the avascularroot or implant surface. Consequently,graft survival depends on a sufficientblood supply originating from the vascu-lar recipient bed adjacent to the recessiondefect and the covering flap.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S132 Zuhr et al.

with those in the covering connectivetissue. However, the results of ani-mal experiments and controlled clini-cal trials indicated that chemicalroot surface demineralization cannotimprove wound healing outcomesand cannot be considered as benefi-cial for root coverage procedurescompared to mechanical biofilmremoval only (Roccuzzo et al. 2002,Oates et al. 2003, Cortellini & PiniPrato 2012). Whether the combina-tion of SCTG and root surfaceconditioning with ethylenediamine-tetraacetic acid before application ofenamel matrix derivate (EMD) caninfluence the type of attachment onthe root surface after gingival reces-sion treatment is presently unclearand needs further scientific verifica-tion (Rasperini et al. 2000, Carnioet al. 2002). The clinical observationof a so-called “creeping attachment”which refers to a soft tissue matura-tion process with a certain coronalmigration of the gingival margin atSCTG-treated sites over time, cannotnot be explained at present. (Agudioet al. 2009, Pini Prato et al. 2010).Two clinical case documentationsreported on external root resorptionafter root coverage with SCTGs(Hokett et al. 2002, Carnio et al.2003). The fact that this is indeed asevere but not a common complica-tion after gingival recession treat-ment might be explained by theearly formation of a root-protectivebarrier, namely a new connective tis-sue attachment in the most apicalpart and a long junctional epithe-lium in the more coronal part of thetreated root surfaces.
It goes without saying that ifinstead of natural roots SCTGs areplaced against artificial surfaces ofimplants or restored teeth new con-nective tissue attachment cannot beexpected. It can be assumed thatthe established type of attachmentis slightly different between restoredtooth and implant and from mate-rial to material, and is character-ized by connective tissue adhesionand – primarily – by a long junc-tional epithelium (Berglundh et al.1991, Abrahamsson et al. 1998,Gomes et al. 2005, Martins et al.2007). Although subgingival resto-ration margins seem to be detri-mental to gingival and periodontalhealth over a long period of time(Schatzle et al. 2001), short-term
data from clinical studies could notreveal more pronounced gingivalinflammation and plaque accumula-tion if class V restorations made ofdifferent tooth coloured filling mate-rials were covered with coronallyadvanced pedicle flaps (Lucchesiet al. 2007, Santamaria et al. 2008).Santamaria and coworkers evalu-ated in a RCT the treatment ofgingival recessions associated withnon-carious cervical lesions bySCTGs with a coronally advancedflap alone or in combination withthe fabrication of resin-modifiedglass ionomer restorations. Sixmonths after surgery there was nostatistically significant differencebetween test and control regardingpercentage of root coverage. Fur-thermore, no clinical signs ofinflammation could be detected inboth groups. The authors creditedthe results with the biocompatibilityof the filling material, the well fab-ricated and polished restorationsand the good compliance and oralhygiene of the patients (Santamariaet al. 2009).
In gingival recession treatment,the combination of coronallyadvanced flaps and SCTGs is pres-ently recommended as the treatmentmodality of choice (Cairo et al.2008, Chambrone et al. 2012, Cortel-lini & Pini Prato 2012), whereas onthe other hand uncertainty existsabout the real effect of the graft:Cortellini and coworkers comparedin a RCT coronally advanced flapsfor gingival recession treatment withand without the additional applica-tion of SCTGs (Cortellini et al.2009). The presence of a SCTGunder the flap was associated with areduced soft tissue contraction dur-ing the early phase of healing lead-ing to a significantly greater amountof sites completely covered at6 months. These results can be inter-preted in a way that the presence ofa SCTG might stabilize the flap in acoronal position and therefore serveas an “anchor” for the covering flapduring the initial wound healing per-iod. A variety of clinical conse-quences would follow if thishypothesis was confirmed: SCTGharvesting for gingival recessiontreatment would be less demandingfor the surgeon in the majority ofthe cases and go along with adecreased risk of damaging the GPA
during the harvesting procedure. Inaddition, more recessions could betreated at the same time if necessaryas the required grafts per recessioncould be comparatively small andrather thin. Furthermore, the nutri-tional exchange between wound bed,SCTG and covering flap might beimproved during the early woundhealing period by this type of grafts– an aspect that might in particularplay a role if the covering flap is thin(Hwang & Wang 2006). In this senseZucchelli and coworkers modifiedposition, size and thickness ofSCTGs and recommended the use ofabout 1 mm thick grafts that werepositioned in a distance apical of thecementoenamel junction that corre-sponds to the pre-operative width ofkeratinized tissue with a mesiodistalextension of the recession width plus6 mm and an apicocoronal dimen-sion calculated as the distance fromthe cementoenamel junction to thebone crest minus the pre-operativeheight of keratinized gingiva. In aRCT using coronally advanced flapsin combination with SCTGs forrecession treatment, the authorscompared the conventional type ofgraft with the novel approach.Although differences between thetwo treatment modalities were notstatistically significant regarding per-centage of root coverage, aestheticresults and patient-centred outcomeswere superior with the small dimen-sioned and apically positioned graft(Zucchelli et al. 2003). If for any rea-son the SCTG failed to anchor theoverlying flap and undesired flapretraction occured during the earlywound healing phase the SCTGmight, on condition that it is posi-tioned at the level of the cemento-enamel junction, act as a “protector”beyond it and still allow healing byprimary intention and successfulroot coverage. This clinical presump-tion can be supported by the resultsof a clinical study by Bouchard andcoworkers comparing coronallyadvanced and envelope flaps in com-bination with SCTGs for gingivalrecession treatment (Bouchard et al.1994). Although treatment outcomeswere similar with respect to rootcoverage a significant increase inkeratinized tissue height was surpris-ingly observed in both groups. Thesefindings could be expected in theenvelope flap group where the most
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S133

coronal parts of the SCTGs werenot covered by the flaps, but not inthe coronally advanced flap groupwhere instead the overlying flapscovered the SCTGs completely(Mackenzie & Fusenig 1983, Ouha-youn et al. 1988, Borghetti & Louise1994, Cordioli et al. 2001). Theauthors assumed that these resultsmight be caused by a tendency offlap retraction during wound healingin the coronally advanced flap groupleaving the most coronal parts of thegraft uncovered. The fact thatslightly exposed areas of a SCTGusually do not undergo necrosis andmaintain primary adhesion to theroot surface might explain theobserved gain in keratinized tissueheight and elucidate the possiblyexisting protector effect of SCTGs(Yotnuengnit et al. 2004). Currentscientific investigations seem to fur-thermore suggest a positive SCTGeffect by “increasing marginal softtissue thickness”. Zuhr and cowork-ers compared in a RCT a modifiedtunnel technique with SCTG fromthe anterior palate versus a coronallyadvanced flap with EMD for rootcoverage (Zuhr et al. accepted forpublication). The application of aninnovative three-dimensional mea-suring technology for treatment out-come evaluation allowed inparticular to quantify the thicknessof the marginal soft tissues estab-lished above the formerly exposedroot surfaces and in this way analyseits influence on recession treatmentoutcomes. Twelve months after sur-gery, mean soft tissue thickness was1.69 � 0.63 mm and 0.91�0.18 mm,respectively, increased gingival thick-ness was clearly associated with bet-ter surgical outcomes in terms ofrecession reduction and root cover-age, whereas a mean marginal softtissue thickness of 1.44 mm was nec-essary to achieve complete root cov-erage with a confidence of 95%(Rebele et al. submitted for publica-tion). In a cohort of six SCTGpatients within the same study popu-lation healing dynamics were evalu-ated by means of volumetricobservations with the post-operativevolume gain at 1 month beingregarded as baseline value. The trea-ted sites showed a mean shrinkageof 1/4 of the augmented volume after3 months, amounting to 1/3 after12 months corresponding to a mean
maintenance of 74% of the aug-mented volume after 3 months and64% after 12 months respectively.With regard to post-operative softtissue volume changes, the healingprocess seemed to be accomplishedafter 6 months (Rebele et al. submit-ted for publication). With respect tolong-term stability after recessiontreatment it can further be specu-lated if the SCTG can provide apositive contribution by “thickeningthe marginal soft tissues” (Nickleset al. 2010, Pini Prato et al. 2010),by the long-term effect of a “creep-ing attachment” (Agudio et al. 2009,Pini Prato et al. 2010) or by a com-bination of both. Anchoring theoverlying flap, protecting healing byprimary intention, increasing mar-ginal soft tissue thickness or induc-ing creeping attachment – furtherprogress regarding soft tissue reces-sion treatment with combined proce-dures will, to some extent, definitelybe dependent on a better under-standing of the true SCTG effect. Itis beyond all doubt that more trans-parency in this context will substan-tially influence future research andclinical developments.
Wound healing and clinical outcomes in
vascular beds
If in contrast to soft tissue recessiontreatment SCTGs are used for softtissue volume build-ups in terms ofridge preservation procedures, softtissue ridge augmentations or papillare-constructions, the pre-requisitesfor uneventful and fast wound heal-ing processes are comparativelyfavourable as the blood supply forgraft integration is provided by both– the overlying flap and the recipientbed (Fig. 9). Although the terms os-teoconduction, osteoinduction andosteogenesis originate from conceptsof bone regeneration and bone heal-ing, the underlying principles mightalso be used to qualify the healingand regeneration processes associ-ated with soft tissue grafting. Equalto bone grafts the “ideal” soft tissuegraft should exhibit an optimalpotential for tissue-specific conduc-tion and induction as well and con-tain the largest number of co-transplanted vital cells possible. Inprinciple, SCTGs seem to have goodcharacteristics with respect to theabove-mentioned requirements for
grafting materials. The organicextracellular matrix could serve as aspace-holder and the relativelyloosely arranged collagen fibreswithin the matrix might ensure thatplasmatic circulation in the initialpost-operative period and the subse-quent re-vascularization process canstart early and proceed relativelyunimpeded (tissue-conductive char-acter). Consequently, the chancesthat a large number of living fibro-blasts in the graft will survive (tis-sue-genetic potential) and continueto produce tissue-specific endoge-nous proteins (tissue-inductive prop-erties) by receiving an adequatesupply of oxygen and nutrientsquickly enough seem to be relativelygood. This thinking model might atleast in part allow to explain the suc-cessful application of SCTGs in plas-tic periodontal and implant surgerytoday. It might in addition be usedto elucidate the aforementioned clini-cal observation that SCTGs fromdifferent donor sites and harvestedwith different techniques seem toprovide different properties regard-ing healing response and volume sta-bility. Furthermore, the clinicalpresumption can be supported thatamong the available SCTGs thoseappear to have a better wound heal-ing response that seem to undergoremarkable shrinkage, and viceversa. Considering its significance forsoft tissue augmentation proceduresin plastic periodontal and implantsurgery, it is remarkable that volu-metric aspects have been hardly eval-uated in the literature. Thus, to thebest of our knowledge only two clin-
Fig. 9. If subepithelial connective tissuegrafts are used for soft tissue volumebuildups like soft tissue ridge augmenta-tions, the prerequisites for uneventfuland fast wound healing processes arecomparatively favourable as the bloodsupply for graft integration is providedby both - the overlying flap and the reci-pient bed.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S134 Zuhr et al.

ical studies on volumetric changesafter soft tissue ridge augmentationprocedures with a follow-up periodof 3.5 months (Studer et al. 2000)and 12 months (Schneider et al.2011) presently exist. Studer andcoworkers compared in a controlledclinical study SCTGs and FGGs forsoft tissue ridge augmentation byquantitative volume assessment.Impressions were made before treat-ment and also at 1 and 3.5 monthsafter surgery to measure the volumechanges on dental casts with a vali-dated projection Moir�e system. Vol-umetric assessment after 3.5 monthsrevealed significantly greater volumegain with SCTGs in comparison toFGGs (Studer et al. 2000). Schneiderand coworkers evaluated the dimen-sional changes of peri-implant tissuesobtained by hard and soft tissueaugmentation. Impressions weretaken before treatment, after implantplacement and guided bone regener-ation, after soft tissue augmentationwith SCTGs, immediately aftercrown insertion and 1 year later.After the cast models were scannedand digitally superimposed, amean buccal tissue gain of 1.27 �0.67 mm could be determined afterthe surgical procedures. One yearafter crown insertion, a mean loss of0.04 � 0.31 mm in the labial direc-tion was recorded. Guided boneregeneration conducted more to vol-ume gain than soft tissue grafting.Moreover, in one-third of theimplants, the soft tissue augmenta-tion did not contribute to theincreased buccal volume at all(Schneider et al. 2011). Besides thatlong-term data on volumetric stabil-ity of soft tissue augmentations aremissing completely. This mightpartly be explained by the fact thatin the past only very complicatedmeasurement technologies like theoptical projection Moir�e methodused by Studer and coworkers wereavailable (Studer et al. 2000). How-ever, the introduction of the afore-mentioned recently developed newmeasuring methods employing three-dimensional optical scanning andsubsequent virtual superimposingprocedures with a previously unfore-seen precision in the quantitativeevaluation of volumetric changes(Windisch et al. 2007, Fickl et al.2008, Strebel et al. 2009, Thomaet al. 2010, Schneider et al. 2011,
Thalmair et al. 2013, Zuhr et al.accepted for publication, Rebeleet al. submitted for publication)offers new perspectives in this con-nection: If ongoing progress anddevelopment regarding soft tissueaugmentation procedures in plasticperiodontal and implant surgery isthe goal, to volumetrically evaluateand compare the efficacy and long-term stability of eligible soft tissuereplacement grafts will be one of themain challenges for the future(Fig. 10).
The above-mentioned scientificinvestigations give a deep insightinto the fundamental physiologicprocesses and the healing chronologyof free autogenous soft tissue grafts.In this respect, some factors of clini-cal relevance can be identified thatshould be respected to accomplishsuccessful and predictable treatmentoutcomes if SCTGs are used in plas-tic periodontal and implant surgery.In the first place, the best possibleblood supply from the recipient bedand the covering flap should be pro-vided for graft survival: incision-and flap-design (Mormann & Cian-cio 1977), thickness of the flap(Hwang & Wang 2006), completegraft coverage (Harris 1994, Studeret al. 2000) and an atraumatic surgi-cal proceeding (Burkhardt & Lang2005) seem to play an important
role. Furthermore, it should be keptin mind that the risk of graft necro-sis might increase with graft thick-ness (Miller 1985, Borghetti &Gardella 1990). Besides, those careshould be taken that the blood clotbetween wound bed and trans-planted tissue is post-operatively asthin as possible to minimize diffu-sion distance and capillary prolifera-tion length, and that the graft isembedded stable and immobile inthe recipient site by tension-free flapsand appropriate suturing techniques(Allen & Miller 1989, Pini Pratoet al. 2000). In this context, a gentlewound compression immediately fol-lowing surgery might have a positiveeffect and in-depth patient instruc-tions on post-operative physical restof the intra-oral wound area mightalso play a role.
Soft tissue substitutes
Soft tissue augmentation procedureswith autogenous grafting materialshave significant disadvantages. Firstand foremost, the amount of avail-able tissue is limited and in themajority of clinical situations, a sec-ond surgical site is needed to obtaina sufficient quantity of autograftmaterial, which increases the burdenon the patient and the morbidity ofthe surgical procedure considerably(Farnoush 1978, Del Pizzo et al.2002, Griffin et al. 2006, Soileau &Brannon 2006). Against this back-ground, it is quite evident that thesearch for suitable soft tissue substi-tutes is currently at the centre ofenormous efforts by scientists andmanufacturers, for the good of thepatient.
Yet, the development of adequatesoft tissue substitutes turns out to becomplicated: SCTGs are undoubt-edly considered as the gold standardfor soft tissue volume augmentationsin plastic periodontal and implantsurgery to date. However, the term“gold standard” suggests a well-defined, consistent standard of har-vesting procedure. However, in factthere seems to be no standardizedprotocol for SCTG removal fromthe palate. As elucidated above dif-ferent available donor sites and har-vesting techniques result ininconsistent types of SCTGs thatvary in their histological composi-tion potentially influencing their clin-
Fig. 10. For future research it will beimportant to generate more three-dimen-sional data after soft tissue augmentationprocedures. Innovative methods usingdigital superimposing of models allowprecise volumetric evaluation.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S135

ical characteristics. Furthermore, itis difficult to develop alternatives toSCTGs as long as their true impacton successful treatment outcomes isnot entirely clear. In some indica-tions the actual role of the graft isobviously the volume increasingeffect, for example. in soft tissueridge augmentation procedures. Inother applications like, for examplein soft tissue recession treatment incontrast the true nature of theSCTG is – as mentioned before –not quite as clear. As long as theSCTG is not clearly defined and aslong as important informationregarding the true effect of theSCTG is lacking it will be very diffi-cult to develop substitutes that aresupposed to measure up with thecurrent gold standard. Not least onthese grounds it needs to be realizedthat for the time being the develop-ment of SCTG substitute materialsis still in its infancy.
In principal, three basic soft tis-sue substitute materials of differentorigin can be distinguished: alloge-neic (of human origin), xenogeneic(from another species, e.g. of porcineor bovine origin), and alloplastic (ofartificial origin) materials. At themoment a variety of available prod-ucts are on the market, whereby itneeds to be mentioned restrictivelythat only a few of them have provedscientifically documented success.
In the late 1980s acellular dermalsubstitutes were introduced to thedental market. The best-researchedtype is the acellular dermal matrix(ADM), an allogeneic substitute thatconsists of a freeze-dried connectivetissue matrix, without epitheliumand cellular components, which isobtained from tissue banks by astandardized, controlled manufactur-ing process. It contains type I- andIII- collagen bundles and elasticfibres, which seem to be degradedand replaced by host tissues duringthe wound healing and integrationprocess (Wei et al. 2002, Cummingset al. 2005, Scarano et al. 2009).With respect to root coverage proce-dures, a systematic review by Cairoand coworkers revealed considerableheterogeneity in clinical outcomemeasures after 6–12 months andconcluded that adding ADM to cor-onally advanced pedicle flaps did notimprove clinical results comparedwith coronally advanced flaps alone
and was inferior to the combinationof coronally advanced flap andSCTG (Cairo et al. 2008). Eventhough, in addition, sufficient long-term data are missing it needs to bestated that the application of acellu-lar dermal substitutes seems to bepresently widespread and acceptedby many clinicians as an approvedalternative to SCTGs in gingivalrecession treatment (Gapski et al.2005, Cairo et al. 2008, Moslemiet al. 2011, Schlee & Esposito 2011).As on the other hand, only fewshort-term observations from clinicalcase series exist, scientific evidence isweak if ADM is supposed to be usedfor soft tissue ridge augmentationprocedures (Thoma et al. 2009).Care needs to be taken, moreover, ifbigger dimensioned grafts arerequired: Folded or layered ADMmight impede vascularization andlead to extensive shrinkage (Batistaet al. 2001, Wei et al. 2002). Ethicalconcerns being an allograft fromhuman cadavers and the pretendedrisk of disease transmission areremarkable counterpoints of thematerial frequently subjected bypatients.
Later on tissue-engineered cellu-lar dermal substitutes, including cel-lular components and tissue-inducingsubstances, came to the centre of sci-entific attention. Wilson andcoworkers investigated the safetyand effectiveness of living human fi-broblasts cultivated on polymer scaf-folds compared with autogenousSCTGs for gingival recession treat-ment (Wilson et al. 2005). The6-month results were promising withno statistically significant differencesbetween control and test group. Jha-veri and coworkers, who appliedautologous fibroblasts on ADMscaffolds, found similar outcomescompared with SCTGs in theirinvestigation (Jhaveri et al. 2010).Despite these promising findings, thecritical cost-benefit ratio seems topresently interfere with furtherinvestments in this type of substitutematerial. To what extent in the con-text of tissue-engineered soft tissuesubstitutes growth factors in theform of platelet-rich fibrin mem-branes or platelet-concentrated graftscould be applied to replace SCTGsfor gingival recession treatment isalso a matter of current scientificinvestigations (Cheung & Griffin
2004, Murata et al. 2008, Arocaet al. 2009, Griffin & Cheung 2009).Carney and coworkers investigatedthe combined effect of recombinanthuman platelet-derived growth factor(rhPDGF) applied on ADM, withthe aim to promote faster re-vascu-larization of the ADM network(Carney et al. 2012). After a 6-month healing period, they found nostatistically significant differences inthe clinical outcomes, showing nobenefit from adding PDGF toADM. McGuire and coworkers con-ducted a RCT to compare coronallyadvanced flap procedures for gingi-val recession treatment through agrowth factor-mediated approachwith either beta-tricalcium phosphate(b-TCP) + 0.3 mg/ml rhPDGF-BBwith a bioabsorbable collagenwound healing dressing or SCTG.Moreover, recession defects were cre-ated in six teeth, each requiringextraction for orthodontic therapy,and treated with the same treatmentmodalities. Nine months after surgi-cal correction, en bloc resectionswere obtained and examinedhistologically and by the use ofmicro-CT. In the RCT, statisticallysignificant results favouring theSCTG were found regarding reces-sion depth reduction 6 months aftersurgery. Histologic and microcom-puted tomography examinationrevealed evidence of new cementum,PDL with inserting connective tissuefibres and supporting alveolar bonein all sites treated with rhPDGF-BB+ b-TCP, whereas neither SCTG-treated site exhibited any signs ofperiodontal regeneration (McGuireet al. 2009a).
Recently, xenogeneic soft tissuesubstitutes in the shape of bilayeredporcine-derived collagen-basedmatrices were introduced. Althoughthese materials were originally intro-duced to promote keratinized tissueregeneration (Sanz et al. 2009, Her-ford et al. 2010, Nevins et al. 2011,Lorenzo et al. 2012), they were sub-sequently adopted for root coverageprocedures. Clinical outcome mea-sures were promising in short-termview and a certain potential for softtissue thickening was observed,although a lower percentage of rootcoverage was recorded comparedwith coronally advanced flaps incombination with SCTGs (Cardaro-poli & Cardaropoli 2009, McGuire
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S136 Zuhr et al.

& Scheyer 2010, Cardaropoli et al.2012, Jepsen et al. 2013) (Fig. 11). Anew type of collagen matrix intendedto be used as a SCTG substitute forlarge volume augmentations wasrecently investigated in an experi-mental study by Thoma and cowork-ers (Thoma et al. 2010). Soft tissueridge augmentation was performedwith either the substitute or SCTGsfrom the lateral palate. Impressionswere taken before augmentation andat 28 and 84 days. In a forward-looking way, the obtained casts wereoptically scanned and the digitalimages analysed. As volumetricanalysis demonstrated no statisticallysignificant differences between bothgroups the authors concluded thatthe experimental collagen matrixmight be a suitable device for softtissue volume augmentation andmight serve as a substitute for autog-enous soft tissue to augment local-ized alveolar ridge defects. Moreclinical and in particular long-termstudies will be needed to confirmthese promising results.
Finally, eligible soft tissue substi-tutes must be non-infectious andbiocompatible. They should providegood tissue integration behaviourwith tissue-conductive characteris-tics. Their mechanical propertiesshould assure good clinical handlingand physical stability. They shouldbe economically efficient and docu-mented success must be given. It willundoubtedly be of great importanceto develop soft tissue substitutes thatcan replace autogenous grafts in thenear future. However, to completelydispense with the need of autograftsfor soft tissue volume augmentationin plastic periodontal and implant
surgery, future substitutes should inaddition feature tissue-genetic andtissue-inductive properties. Theextent to which these propertiesmight be improved, for example byadding autogenous cells and syn-thetic growth proteins or bioactivesubstances and the degree to whichinnovative medical technologies suchas tissue engineering might allow touse substitute materials more than todate remain to be seen. The nextgeneration technology should aimfor soft tissue substitutes that are atleast as good as or even better thanSCTGs for soft tissue volume aug-mentation by vascularizing quickly,for instance by implementation of apre-fabricated vascular network(Calcagni et al. 2011), by allowingfor healing by secondary intention,and ideally by showing no post-oper-ative shrinkage at all. Like SCTGsfrom different donor sites are at thisstage utilized in various indications,it is conceivable that there is a needto develop a variety of substitutematerials with distinct propertiesdeployed in varying clinical situa-tions at the end.
Summary and conclusions
The predominant interventions inplastic periodontal and implant sur-gery are augmentation proceduresfrequently performed by the use ofsoft tissue replacement grafts.Although written evidence lacks rele-vant data for the most part, thepresent review demonstrates clearlythat among available augmentationmaterials autologous SCTGs areconsidered as the gold standard forsoft tissue volume augmentation todate. However, there is a restrictivecore of critical elements that couldbe identified within the scope of thisarticle and that can be summarizedas follows:
• The term “gold standard” impliesa well-defined and consistentstandard of harvesting procedure.Different donor sites at the palatethat can be selected and varyingharvesting techniques that can beapplied, though, result in differ-ent kinds of SCTGs that vary intheir histological compositionobviously leading to differentcharacteristics that might requireselective clinical application.
• Up to date, the clinical decisionwhere to harvest SCTGs from ishardly based on scientific evi-dence but rather depends on theamount of available tissue at theeligible donor sites, the indicationin which the transplant is sup-posed to be used and in particu-lar on the personal preference ofthe treating surgeon.
• Independent of the selecteddonor site the clinical procedureof SCTG harvesting from thepalate is basically characterizedby the challenge of obtaining anadequate amount of tissue whileminimizing postoperative painand reducing the risk of compli-cations at its best.
• The limited amount of graftingtissue and the increased patientmorbidity are substantial disad-vantages of autogenous SCTGs.For this reason, the search forsuitable soft tissue substitutes iscurrently at the centre of numer-ous efforts by scientists and man-ufacturers and will be animportant field of future research– for the good of the patient.
• Many questions with regard tograft healing and volumetric sta-bility remain presently unknown– this relates to soft tissue substi-tutes, but to autologous SCTGsas well. Patient-centred outcomemeasures, quantitative three-dimensional and qualitative-aes-thetic assessment of treatmentresults as well as long-term fol-low-up data are hardly availableat present.
• Thus, more research is needed tofurther progress and increaseknowledge regarding soft tissuevolume augmentation proceduresin plastic periodontal andimplant surgery. At the end, thegoal cannot be considerably dif-ferent from developing appropri-ate soft tissue substitutes for allconceivable indications and bydoing so rendering soft tissueautografts unnecessary and elimi-nating their clinical applicationto the best possible extent.
References
Abrahamsson, I., Berglundh, T., Glantz, P. O. &Lindhe, J. (1998) The mucosal attachment atdifferent abutments. An experimental study in
Fig. 11. Scanning electron microscopeimage of a commercially available xeno-geneic collagen matrix. The bilayereddesign is supposed to provide tissue-con-ductive properties and good clinical han-dling (courtesy of Peter Sch€upbach).
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S137

dogs. Journal of Clinical Periodontology 25,721–727.
Agudio, G., Nieri, M., Rotundo, R., Franceschi,D., Cortellini, P. & Pini Prato, G. P. (2009)Periodontal conditions of sites treated with gin-gival-augmentation surgery compared tountreated contralateral homologous sites: a 10-to 27-year long-term study. Journal of Peri-odontology 80, 1399–1405.
Allen, A. L. (1994) Use of the supraperiostealenvelope in soft tissue grafting for root cover-age. I. Rationale and technique. The Interna-tional journal of periodontics & restorativedentistry 14, 216–227.
Allen, E. P. & Miller, P. D. Jr (1989) Coronalpositioning of existing gingiva: short termresults in the treatment of shallow marginal tis-sue recession. Journal of Periodontology 60,316–319.
Al-Zahrani, M. S., Bissada, N. F., Ficara, A. J. &Cole, B. (2004) Effect of connective tissue graftorientation on root coverage and gingival aug-mentation. The International journal of peri-odontics & restorative dentistry 24, 65–69.
Aroca, S., Keglevich, T., Barbieri, B., Gera, I. &Etienne, D. (2009) Clinical evaluation of amodified coronally advanced flap alone or incombination with a platelet-rich fibrin mem-brane for the treatment of adjacent multiplegingival recessions: a 6-month study. Journal ofPeriodontology 80, 244–252.
Batista, E. L. Jr, Batista, F. C. & Novaes, A. B.Jr (2001) Management of soft tissue ridgedeformities with acellular dermal matrix. Clini-cal approach and outcome after 6 months oftreatment. Journal of Periodontology 72,265–273.
Benninger, B., Andrews, K. & Carter, W. (2012)Clinical measurements of hard palate andimplications for subepithelial connective tissuegrafts with suggestions for palatal nomencla-ture. Journal of Oral and Maxillofacial Surgery70, 149–153.
Berglundh, T., Lindhe, J., Ericsson, I., Marinello,C. P., Liljenberg, B. & Thomsen, P. (1991) Thesoft tissue barrier at implants and teeth. Clini-cal Oral Implants Research 2, 81–90.
Bernimoulin, J. P., Luscher, B. & Muhlemann, H.R. (1975) Coronally repositioned periodontalflap. Clinical evaluation after one year. Journalof Clinical Periodontology 2, 1–13.
Bohannan, H. M. (1962) Studies in the alterationof vestibular depth. I. Complete denudation.Journal of Periodontology 33, 120–128.
Borghetti, A. & Gardella, J. P. (1990) Thick gingi-val autograft for the coverage of gingival reces-sion: a clinical evaluation. The Internationaljournal of periodontics & restorative dentistry10, 216–229.
Borghetti, A. & Louise, F. (1994) Controlled clini-cal evaluation of the subpedicle connective tis-sue graft for the coverage of gingival recession.Journal of Periodontology 65, 1107–1112.
Bouchard, P., Etienne, D., Ouhayoun, J. P. &Nilveus, R. (1994) Subepithelial connective tis-sue grafts in the treatment of gingival reces-sions. A comparative study of 2 procedures.Journal of Periodontology 65, 929–936.
Bowers, G. M. (1963) A study of the width ofattached gingiva. Journal of Periodontology 34,201–209.
Bradley, R. E., Gant, J. C. & Ivancie, G. P.(1959) Histologic evaluation of mucogingivalsurgery. Oral Surgery, Oral Medicine, and OralPathology 12, 1184–1199.
Bruno, J. F. (1994) Connective tissue graft tech-nique assuring wide root coverage. The Interna-
tional journal of periodontics & restorativedentistry 14, 126–137.
Bruno, J. F. & Bowers, G. M. (2000) Histologyof a human biopsy section following the place-ment of a subepithelial connective tissue graft.The International journal of periodontics &restorative dentistry 20, 225–231.
Burkhardt, R., Joss, A. & Lang, N. P. (2008) Softtissue dehiscence coverage around endosseousimplants: a prospective cohort study. ClinicalOral Implants Research 19, 451–457.
Burkhardt, R. & Lang, N. P. (2005) Coverage oflocalized gingival recessions: comparison ofmicro- and macrosurgical techniques. Journalof Clinical Periodontology 32, 287–293.
Cairo, F., Pagliaro, U. & Nieri, M. (2008)Treatment of gingival recession with coronallyadvanced flap procedures: a systematicreview. Journal of Clinical Periodontology 35,136–162.
Calcagni, M., Althaus, M. K., Knapik, A. D.,Hegland, N., Contaldo, C., Giovanoli, P. &Lindenblatt, N. (2011) In vivo visualization ofthe origination of skin graft vasculature in awild-type/GFP crossover model. MicrovascularResearch 82, 237–245.
Cardaropoli, D. & Cardaropoli, G. (2009) Heal-ing of gingival recessions using a collagenmembrane with a hemineralized xenograft: arandomized controlled clinical trial. The Inter-national journal of periodontics & restorativedentistry 29, 59–67.
Cardaropoli, D., Tamagnone, L., Roffredo, A. &Gaveglio, L. (2012) Treatment of gingivalrecession defects using coronally advanced flapwith a porcine collagen matrix compared tocoronally advanced flap with connective tissuegraft: a randomized controlled clinical trial.Journal of Periodontology 83, 321–328.
Carney, C. M., Rossmann, J. A., Kerns, D. G.,Cipher, D. J., Rees, T. D., Solomon, E. S., Ri-vera-Hidalgo, F. & Beach, M. M. (2012) Acomparative study of root defect coverageusing an acellular dermal matrix with and with-out a recombinant human platelet-derivedgrowth factor. Journal of Periodontology 83,893–901.
Carnio, J., Camargo, P. M. & Kenney, E. B.(2003) Root resorption associated with a sub-epithelial connective tissue graft for root cover-age: clinical and histologic report of a case.The International journal of periodontics &restorative dentistry 23, 391–398.
Carnio, J., Camargo, P. M., Kenney, E. B. &Schenk, R. K. (2002) Histological evaluation of4 cases of root coverage following a connectivetissue graft combined with an enamel matrixderivative preparation. Journal of Periodontol-ogy 73, 1534–1543.
Carranza, F. A. Jr & Carraro, J. J. (1970) Muco-gingival techniques in periodontal surgery.Journal of Periodontology 41, 294–299.
Chambrone, L., Pannuti, C. M., Tu, Y. K. &Chambrone, L. A. (2012) Evidence-based peri-odontal plastic surgery. II. An individual datameta-analysis for evaluating factors in achiev-ing complete root coverage. Journal of Peri-odontology 83, 477–490.
Chambrone, L., Sukekava, F., Araujo, M. G., Pu-stiglioni, F. E., Chambrone, L. A. & Lima, L.A. (2010) Root-coverage procedures for thetreatment of localized recession-type defects: aCochrane systematic review. Journal of Peri-odontology 81, 452–478.
Cheung, W. S. & Griffin, T. J. (2004) A compara-tive study of root coverage with connective tis-sue and platelet concentrate grafts: 8-month
results. Journal of Periodontology 75, 1678–1687.
Cordioli, G., Mortarino, C., Chierico, A., Gruso-vin, M. & Majzoub, Z. (2001) Comparison of 2techniques of subepithelial connective tissuegraft in the treatment of gingival recessions.Journal of Periodontology 72, 1470–1476.
Corn, H. (1962) Periosteal separation - its clinicalsignificance. Journal of Periodontology 33, 144–152.
Cortellini, P. & Pini Prato, G. (2012) Coronallyadvanced flap and combination therapy forroot coverage. Clinical strategies based on sci-entific evidence and clinical experience. Peri-odontology 2000 59, 158–184.
Cortellini, P., Tonetti, M., Baldi, C., Francetti,L., Rasperini, G., Rotundo, R., Nieri, M.,Franceschi, D., Labriola, A. & Prato, G. P.(2009) Does placement of a connective tissuegraft improve the outcomes of coronallyadvanced flap for coverage of single gingivalrecessions in upper anterior teeth? A multi-cen-tre, randomized, double-blind, clinical trial.Journal of Clinical Periodontology 36, 68–79.
Cummings, L. C., Kaldahl, W. B. & Allen, E. P.(2005) Histologic evaluation of autogenousconnective tissue and acellular dermal matrixgrafts in humans. Journal of Periodontology 76,178–186.
Del Pizzo, M., Modica, F., Bethaz, N., Priotto, P.& Romagnoli, R. (2002) The connective tissuegraft: a comparative clinical evaluation ofwound healing at the palatal donor site. A pre-liminary study. Journal of Clinical Periodontol-ogy 29, 848–854.
Donn, B. J. Jr (1978) The free connective tissueautograft: a clinical and histologic wound heal-ing study in humans. Journal of Periodontology49, 253–260.
Dorfman, H. S., Kennedy, J. E. & Bird, W. C.(1982) Longitudinal evaluation of free autoge-nous gingival grafts. A four year report. Jour-nal of Periodontology 53, 349–352.
Edel, A. (1974) Clinical evaluation of free connec-tive tissue grafts used to increase the width ofkeratinised gingiva. Journal of Clinical Peri-odontology 1, 185–196.
Eger, T., Muller, H. P. & Heinecke, A. (1996)Ultrasonic determination of gingival thickness.Subject variation and influence of tooth typeand clinical features. Journal of Clinical Peri-odontology 23, 839–845.
Ericsson, I. & Lindhe, J. (1984) Recession in siteswith inadequate width of the keratinized gin-giva. An experimental study in the dog. Journalof Clinical Periodontology 11, 95–103.
Esposito, M., Maghaireh, H., Grusovin, M. G.,Ziounas, I. & Worthington, H. V. (2012) Softtissue management for dental implants: whatare the most effective techniques? A Cochranesystematic review. European Journal of OralImplantology 5, 221–238.
Farnoush, A. (1978) Techniques for the protec-tion and coverage of the donor sites in free softtissue grafts. Journal of Periodontology 49, 403–405.
Fickl, S., Zuhr, O., Wachtel, H., Bolz, W. & Hu-erzeler, M. (2008) Tissue alterations after toothextraction with and without surgical trauma: avolumetric study in the beagle dog. Journal ofClinical Periodontology 35, 356–363.
Friedman, N. (1962) Mucogingival surgery: Theapically repositioned flap. Journal of Periodon-tology 33, 328–340.
Friedman, N. & Levine, H. L. (1964) Mucogingi-val surgery. Current status. Journal of Peri-odontology 35, 5–21.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S138 Zuhr et al.

Fu, J. H., Hasso, D. G., Yeh, C. Y., Leong, D.J., Chan, H. L. & Wang, H. L. (2011) Theaccuracy of identifying the greater palatineneurovascular bundle: a cadaver study. Journalof Periodontology 82, 1000–1006.
Gapski, R., Parks, C. A. & Wang, H. L. (2005)Acellular dermal matrix for mucogingival sur-gery: a meta-analysis. Journal of Periodontology76, 1814–1822.
Gapski, R., Satheesh, K. & Cobb, C. M. (2006)Histomorphometric analysis of bone density inthe maxillary tuberosity of cadavers: a pilotstudy. Journal of Periodontology 77, 1085–1090.
Gargiulo, A. W. & Arrocha, R. (1967) Histo-clini-cal evaluation of free gingival grafts. Periodon-tics 5, 285–291.
Goldstein, M., Boyan, B. D., Cochran, D. L. &Schwartz, Z. (2001) Human histology of newattachment after root coverage using subepithe-lial connective tissue graft. Journal of ClinicalPeriodontology 28, 657–662.
Gomes, S. C., Miranda, L. A., Soares, I. & Op-permann, R. V. (2005) Clinical and histologicevaluation of the periodontal response torestorative procedures in the dog. The Interna-tional journal of periodontics & restorative den-tistry 25, 39–47.
Griffin, T. J. & Cheung, W. S. (2009) Guided tis-sue regeneration-based root coverage with aplatelet concentrate graft: a 3-year follow-upcase series. Journal of Periodontology 80, 1192–1199.
Griffin, T. J., Cheung, W. S., Zavras, A. I. &Damoulis, P. D. (2006) Postoperative complica-tions following gingival augmentation proce-dures. Journal of Periodontology 77, 2070–2079.
Guiha, R., el Khodeiry, S., Mota, L. & Caffesse,R. (2001) Histological evaluation of healingand revascularization of the subepithelial con-nective tissue graft. Journal of Periodontology72, 470–478.
Haggerty, P. C. (1966) The use of a free gingivalgraft to create a healthy environment for fullcrown preparation. Case history. Periodontics4, 329–331.
Hall, W. B. (1981) The current status of mucogin-gival problems and their therapy. Journal ofPeriodontology 52, 569–575.
Hangorsky, U. & Bissada, N. F. (1980) Clinicalassessment of free gingival graft effectivenesson the maintenance of periodontal health.Journal of Periodontology 51, 274–278.
Harris, R. J. (1992) The connective tissue andpartial thickness double pedicle graft: a predict-able method of obtaining root coverage. Jour-nal of Periodontology 63, 477–486.
Harris, R. J. (1994) The connective tissue withpartial thickness double pedicle graft: theresults of 100 consecutively-treated defects.Journal of Periodontology 65, 448–461.
Harris, R. J. (1997) A comparison of twotechniques for obtaining a connective tissuegraft from the palate. The International journalof periodontics & restorative dentistry 17, 260–271.
Harris, R. J. (1999) Human histologic evaluationof root coverage obtained with a connective tis-sue with partial thickness double pedicle graft.A case report. Journal of Periodontology 70,813–821.
Harris, R. J. (2003) Histologic evaluation of con-nective tissue grafts in humans. The Interna-tional journal of periodontics & restorativedentistry 23, 575–583.
Harris, R. J., Harris, L. E., Harris, C. R. & Har-ris, A. J. (2007) Evaluation of root coveragewith two connective tissue grafts obtained from
the same location. The International journal ofperiodontics & restorative dentistry 27, 333–339.
Herford, A. S., Akin, L., Cicciu, M., Maiorana,C. & Boyne, P. J. (2010) Use of a porcine col-lagen matrix as an alternative to autogenoustissue for grafting oral soft tissue defects.Journal of Oral and Maxillofacial Surgery 68,1463–1470.
Hokett, S. D., Peacock, M. E., Burns, W. T.,Swiec, G. D. & Cuenin, M. F. (2002) Externalroot resorption following partial-thickness con-nective tissue graft placement: a case report.Journal of Periodontology 73, 334–339.
Huang, L. H., Neiva, R. E., Soehren, S. E., Gian-nobile, W. V. & Wang, H. L. (2005) The effectof platelet-rich plasma on the coronallyadvanced flap root coverage procedure: a pilothuman trial. Journal of Periodontology 76,1768–1777.
Hurzeler, M. B. & Weng, D. (1999) A single-inci-sion technique to harvest subepithelial connec-tive tissue grafts from the palate. TheInternational journal of periodontics & restor-ative dentistry 19, 279–287.
Hwang, D. & Wang, H. L. (2006) Flap thicknessas a predictor of root coverage: a systematicreview. Journal of Periodontology 77, 1625–1634.
Ikuta, C. R., Cardoso, C. L., Ferreira-Junior, O.,Lauris, J. R., Souza, P. H. & Rubira-Bullen, I.R. (2013) Position of the greater palatine fora-men: an anatomical study through cone beamcomputed tomography images. Surgical andRadiologic Anatomy 35, 837–842.
Ivancie, G. P. (1957) Experimental and histologi-cal investigation of gingival regeneration in ves-tibular surgery. Journal of Periodontology 28,259–263.
Jahnke, P. V., Sandifer, J. B., Gher, M. E., Gray,J. L. & Richardson, A. C. (1993) Thick freegingival and connective tissue autografts forroot coverage. Journal of Periodontology 64,315–322.
Jankovic, S., Aleksic, Z., Klokkevold, P., Lekovic,V., Dimitrijevic, B., Kenney, E. B. & Camargo,P. (2012) Use of platelet-rich fibrin membranefollowing treatment of gingival recession: a ran-domized clinical trial. The International journalof periodontics & restorative dentistry 32, e41–e50.
Jansen, W. A., Ruben, M. P., Kramer, G. M.,Bloom, A. A. & Turner, H. (1969) Develop-ment of the blood supply to split-thickness freegingival autografts. Journal of Periodontology39, 707–716.
Jepsen, K., Jepsen, S., Zucchelli, G., Stefanini,M., de Sanctis, M., Baldini, N., Greven, B.,Heinz, B., Wennstrom, J., Cassel, B., Vigno-letti, F. & Sanz, M. (2013) Treatment of gingi-val recession defects with a coronally advancedflap and a xenogeneic collagen matrix: a multi-center randomized clinical trial. Journal of Clin-ical Periodontology 40, 82–89.
Jhaveri, H. M., Chavan, M. S., Tomar, G. B.,Deshmukh, V. L., Wani, M. R. & Miller, P.D. Jr (2010) Acellular dermal matrix seededwith autologous gingival fibroblasts for thetreatment of gingival recession: a proof-of-concept study. Journal of Periodontology 81,616–625.
Joly, J. C., Carvalho, A. M., da Silva, R. C., Cio-tti, D. L. & Cury, P. R. (2007) Root coveragein isolated gingival recessions using autograftversus allograft: a pilot study. Journal of Peri-odontology 78, 1017–1022.
Jung, R. E., Sailer, I., Hammerle, C. H., Attin, T.& Schmidlin, P. (2007) In vitro color changes
of soft tissues caused by restorative materials.The International journal of periodontics &restorative dentistry 27, 251–257.
Karring, T., Cumming, B. R., Oliver, R. C. &Loe, H. (1975) The origin of granulation tissueand its impact on postoperative results of mu-cogingival surgery. Journal of Periodontology46, 577–585.
Karring, T., Lang, N. R. & Loe, H. (1974) Therole of gingival connective tissue in determiningepithelial differentiation. Journal of PeriodontalResearch 10, 1–11.
Karring, T., Ostergaard, E. & Loe, H. (1971)Conservation of tissue specificity after hetero-topic transplantation of gingiva and alveolarmucosa. Journal of Periodontal Research 6,282–293.
Keceli, H. G., Sengun, D., Berberoglu, A. & Kar-abulut, E. (2008) Use of platelet gel with con-nective tissue grafts for root coverage: arandomized-controlled trial. Journal of ClinicalPeriodontology 35, 255–262.
Kisch, J., Badersten, A. & Egelberg, J. (1986)Longitudinal observation of “unattached”,mobile gingival areas. Journal of Clinical Peri-odontology 13, 131–134.
Klosek, S. K. & Rungruang, T. (2009) Anatomi-cal study of the greater palatine artery andrelated structures of the palatal vault: consider-ations for palate as the subepithelial connectivetissue graft donor site. Surgical and RadiologicAnatomy 31, 245–250.
Lafzi, A., Faramarzi, M., Shirmohammadi, A.,Behrozian, A., Kashefimehr, A. & Khashabi,E. (2012) Subepithelial connective tissue graftwith and without the use of plasma rich ingrowth factors for treating root exposure. Jour-nal of Periodontal & Implant Science 42, 196–203.
Landsberg, C. J. & Bichacho, N. (1994) A modi-fied surgical/prosthetic approach for optimalsingle implant supported crown. Part I–Thesocket seal surgery. Practical Periodontics andAesthetic Dentistry 6, 11–17; quiz 19.
Lang, N. P. & Loe, H. (1972) The relationshipbetween the width of keratinized gingiva andgingival health. Journal of Periodontology 43,623–627.
Lang, N. P., Pun, L., Lau, K. Y., Li, K. Y. &Wong, M. C. (2012) A systematic review onsurvival and success rates of implants placedimmediately into fresh extraction sockets afterat least 1 year. Clinical Oral Implants Research23 (Suppl 5), 39–66.
Langer, B. & Calagna, L. (1980) The subepithelialconnective tissue graft. Journal of ProstheticDentistry 44, 363–367.
Langer, B. & Calagna, L. J. (1982) The subepithe-lial connective tissue graft. A new approach tothe enhancement of anterior cosmetics. TheInternational journal of periodontics & restor-ative dentistry 2, 22–33.
Langer, B. & Langer, L. (1985) Subepithelial con-nective tissue graft technique for root coverage.Journal of Periodontology 56, 715–720.
Lindenblatt, N., Calcagni, M., Contaldo, C.,Menger, M. D., Giovanoli, P. & Vollmar, B.(2008) A new model for studying the revascu-larization of skin grafts in vivo: the role ofangiogenesis. Plastic and Reconstructive Surgery122, 1669–1680.
Lindenblatt, N., Platz, U., Althaus, M., Hegland,N., Schmidt, C. A., Contaldo, C., Vollmar, B.,Giovanoli, P. & Calcagni, M. (2010) Tempo-rary angiogenic transformation of the skingraft vasculature after reperfusion. Plastic andReconstructive Surgery 126, 61–70.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S139

Lindhe, J. & Nyman, S. (1980) Alterations of theposition of the marginal soft tissue followingperiodontal surgery. Journal of Clinical Peri-odontology 7, 525–530.
Lorenzo, R., Garcia, V., Orsini, M., Martin, C. &Sanz, M. (2012) Clinical efficacy of a xenoge-neic collagen matrix in augmenting keratinizedmucosa around implants: a randomizedcontrolled prospective clinical trial. ClinicalOral Implants Research 23, 316–324.
Lucchesi, J. A., Santos, V. R., Amaral, C. M., Pe-ruzzo, D. C. & Duarte, P. M. (2007) Coronallypositioned flap for treatment of restored rootsurfaces: a 6-month clinical evaluation. Journalof Periodontology 78, 615–623.
Mackenzie, I. C. & Fusenig, N. E. (1983) Regener-ation of organized epithelial structure. The Jour-nal of Investigative Dermatology 81, 189s–194s.
Majzoub, Z., Landi, L., Grusovin, M. G. &Cordioli, G. (2001) Histology of connective tis-sue graft. A case report. Journal of Periodontol-ogy 72, 1607–1615.
Martins, T., Bosco, A., Nobrega, F., Nagata, M.,Garcia, V. & Fucini, S. (2007) Periodontal tis-sue response to coverage of root cavitiesrestored with resin materials: A histomorpho-metric study in dogs. Journal of Periodontology78, 1075–1082.
Matter, J. (1982) Free gingival grafts for the treat-ment of gingival recession. A review of sometechniques. Journal of Clinical Periodontology9, 103–114.
McGuire, M. K. & Cochran, D. L. (2003) Evalua-tion of human recession defects treated withcoronally advanced flaps and either enamelmatrix derivative or connective tissue. Part 2:Histological evaluation. Journal of Periodontol-ogy 74, 1126–1135.
McGuire, M. K. & Scheyer, E. T. (2010) Xenoge-neic collagen matrix with coronally advancedflap compared to connective tissue with coro-nally advanced flap for the treatment of dehis-cence-type recession defects. Journal ofPeriodontology 81, 1108–1117.
McGuire, M. K., Scheyer, E. T. & Schupbach, P.(2009a) Growth factor-mediated treatment ofrecession defects: a randomized controlled trialand histologic and microcomputed tomographyexamination. Journal of Periodontology 80,550–564.
McGuire, M. K., Scheyer, T., Nevins, M. &Schupbach, P. (2009b) Evaluation of humanrecession defects treated with coronallyadvanced flaps and either purified recombinanthuman platelet-derived growth factor-BB withbeta tricalcium phosphate or connective tissue:a histologic and microcomputed tomographicexamination. The International journal of peri-odontics & restorative dentistry 29, 7–21.
Miller, P. D. Jr (1982) Root coverage using a freesoft tissue autograft following citric acid applica-tion. Part 1: Technique. The International journalof periodontics & restorative dentistry 2, 65–70.
Miller, P. D. Jr (1985) Root coverage using thefree soft tissue autograft following citric acidapplication. III. A successful and predictableprocedure in areas of deep-wide recession. TheInternational journal of periodontics & restor-ative dentistry 5, 14–37.
Miyasato, M., Crigger, M. & Egelberg, J. (1977)Gingival condition in areas of minimal andappreciable width of keratinized gingiva. Jour-nal of Clinical Periodontology 4, 200–209.
Monnet-Corti, V., Santini, A., Glise, J. M., Fou-que-Deruelle, C., Dillier, F. L., Liebart, M. F.& Borghetti, A. (2006) Connective tissue graftfor gingival recession treatment: assessment of
the maximum graft dimensions at the palatalvault as a donor site. Journal of Periodontology77, 899–902.
Mormann, W., Bernimoulin, J. P. & Schmid, M.O. (1975) Fluorescein angiography of free gin-gival autografts. Journal of Clinical Periodontol-ogy 2, 177–189.
Mormann, W. & Ciancio, S. G. (1977) Blood sup-ply of human gingiva following periodontalsurgery. A fluorescein angiographic study.Journal of Periodontology 48, 681–692.
Moslemi, N., Mousavi Jazi, M., Haghighati, F.,Morovati, S. P. & Jamali, R. (2011) Acellulardermal matrix allograft versus subepithelialconnective tissue graft in treatment of gingivalrecessions: a 5-year randomized clinical study.Journal of Clinical Periodontology 38, 1122–1129.
Muller, H. P., Schaller, N., Eger, T. & Heinecke,A. (2000) Thickness of masticatory mucosa.Journal of Clinical Periodontology 27, 431–436.
Murata, M., Okuda, K., Momose, M., Kubo, K.,Kuroyanagi, Y. & Wolff, L. F. (2008) Root cov-erage with cultured gingival dermal substitutecomposed of gingival fibroblasts and matrix: acase series. The International journal of periodon-tics & restorative dentistry 28, 461–467.
Nabers, C. L. (1954) Repositioning the attachedgingiva. Journal of Periodontology 25, 38–39.
Nabers, J. M. (1966) Free gingival grafts. Peri-odontics 4, 243–245.
Nelson, S. W. (1987) The subpedicle connectivetissue graft. A bilaminar reconstructive proce-dure for the coverage of denuded root surfaces.Journal of Periodontology 58, 95–102.
Nemcovsky, C. E. (2001) Interproximal papillaaugmentation procedure: a novel surgicalapproach and clinical evaluation of 10 consecu-tive procedures. The International journal ofperiodontics & restorative dentistry 21, 553–559.
Nevins, M., Nevins, M. L., Kim, S. W., Schup-bach, P. & Kim, D. M. (2011) The use of mu-cograft collagen matrix to augment the zone ofkeratinized tissue around teeth: a pilot study.The International journal of periodontics &restorative dentistry 31, 367–373.
Nickles, K., Ratka-Kruger, P., Neukranz, E.,Raetzke, P. & Eickholz, P. (2010) Ten-yearresults after connective tissue grafts and guidedtissue regeneration for root coverage. Journalof Periodontology 81, 827–836.
Nobuto, T. (1986) Microvascularization of thefree gingival autograft using corrosion casts.Journal of Dental Research 65, 528.
Nobuto, T. (1987) Experimental study on micro-vascularization following free gingival auto-graft–process of the recirculation to grafts.Nihon Shishubyo Gakkai Kaishi 29, 352–364.
Nobuto, T., Imai, H. & Yamaoka, A. (1988) Mi-crovascularization of the free gingival auto-graft. Journal of Periodontology 59, 639–646.
Nordland, W. P., Sandhu, H. S. & Perio, C.(2008) Microsurgical technique for augmenta-tion of the interdental papilla: three casereports. The International journal of periodontics& restorative dentistry 28, 543–549.
Oates, T. W., Robinson, M. & Gunsolley, J. C.(2003) Surgical therapies for the treatment ofgingival recession. A systematic review. Annalsof Periodontology 8, 303–320.
Ochsenbein, C. (1960) Newer concept of mucogin-gival surgery. Journal of Periodontology 31,175–185.
Oliver, R. C., Loe, H. & Karring, T. (1968)Microscopic evaluation of the healing andrevascularization of free gingival grafts. Journalof Periodontal Research 3, 84–95.
Orban, B. J. (1957) Oral Histology and Embryol-ogy. St. Louis: C.V. Mosby Company.
Orban, B. & Sicher, H. (1945) The oral mucosa.Journal of Dental Education 10, 94–103.
Ouhayoun, J. P., Sawaf, M. H., Gofflaux, J. C.,Etienne, D. & Forest, N. (1988) Re-epithelial-ization of a palatal connective tissue grafttransplanted in a non-keratinized alveolarmucosa: a histological and biochemical studyin humans. Journal of Periodontal Research 23,127–133.
Paolantonio, M., Dolci, M., Esposito, P., D’Ar-chivio, D., Lisanti, L., Di Luccio, A. & Peri-netti, G. (2002) Subpedicle acellular dermalmatrix graft and autogenous connective tissuegraft in the treatment of gingival recessions: acomparative 1-year clinical study. Journal ofPeriodontology 73, 1299–1307.
Pfeifer, J. S. (1963) The growth of gingival tissueover denuded bone. Journal of Periodontology34, 10–16.
Pini Prato, G. P., Cairo, F., Nieri, M., France-schi, D., Rotundo, R. & Cortellini, P. (2010)Coronally advanced flap versus connective tis-sue graft in the treatment of multiple gingivalrecessions: a split-mouth study with a 5-yearfollow-up. Journal of Clinical Periodontology37, 644–650.
Pini Prato, G., Pagliaro, U., Baldi, C., Nieri, M.,Saletta, D., Cairo, F. & Cortellini, P. (2000)Coronally advanced flap procedure for rootcoverage. Flap with tension versus flap withouttension: a randomized controlled clinical study.Journal of Periodontology 71, 188–201.
Raetzke, P. B. (1985) Covering localized areas ofroot exposure employing the “envelope” tech-nique. Journal of Periodontology 56, 397–402.
Rasperini, G., Silvestri, M., Schenk, R. K. &Nevins, M. L. (2000) Clinical and histologicevaluation of human gingival recession treatedwith a subepithelial connective tissue graft andenamel matrix derivative (Emdogain): a casereport. The International journal of periodontics& restorative dentistry 20, 269–275.
Reiser, G. M., Bruno, J. F., Mahan, P. E. & Lar-kin, L. H. (1996) The subepithelial connectivetissue graft palatal donor site: anatomic consid-erations for surgeons. The International journalof periodontics & restorative dentistry 16, 130–137.
Roccuzzo, M., Bunino, M., Needleman, I. &Sanz, M. (2002) Periodontal plastic surgery fortreatment of localized gingival recessions: a sys-tematic review. Journal of Clinical Periodontol-ogy 29 Suppl 3, 178–194; discussion 195–176.
Roccuzzo, M., Gaudioso, L., Bunino, M. &Dalmasso, P. (2013) Surgical treatment of buc-cal soft tissue recessions around singleimplants: 1-year results from a prospective pilotstudy. Clinical Oral Implants Research doi: 10.1111/clr.12149. [Epub ahead of print].
Salkin, L. M., Freedman, A. L., Stein, M. D. &Bassiouny, M. A. (1987) A longitudinal studyof untreated mucogingival defects. Journal ofPeriodontology 58, 164–166.
Santamaria, M. P., Ambrosano, G. M., Casati,M. Z., Nociti Junior, F. H., Sallum, A. W. &Sallum, E. A. (2009) Connective tissue graftplus resin-modified glass ionomer restorationfor the treatment of gingival recession associ-ated with non-carious cervical lesion: a ran-domized-controlled clinical trial. Journal ofClinical Periodontology 36, 791–798.
Santamaria, M. P., Suaid, F. F., Casati, M. Z.,Nociti, F. H., Sallum, A. W. & Sallum, E. A.(2008) Coronally positioned flap plus resin-modified glass ionomer restoration for the
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S140 Zuhr et al.

treatment of gingival recession associated withnon-carious cervical lesions: a randomized con-trolled clinical trial. Journal of Periodontology79, 621–628.
Sanz, I., Garcia-Gargallo, M., Herrera, D., Mar-tin, C., Figuero, E. & Sanz, M. (2012) Surgicalprotocols for early implant placement in post-extraction sockets: a systematic review. ClinicalOral Implants Research 23 (Suppl 5), 67–79.
Sanz, M., Lorenzo, R., Aranda, J. J., Martin, C.& Orsini, M. (2009) Clinical evaluation of anew collagen matrix (Mucograft prototype) toenhance the width of keratinized tissue inpatients with fixed prosthetic restorations: arandomized prospective clinical trial. Journal ofClinical Periodontology 36, 868–876.
Scarano, A., Barros, R. R., Iezzi, G., Piattelli, A.& Novaes, A. B. Jr (2009) Acellular dermalmatrix graft for gingival augmentation: a preli-minary clinical, histologic, and ultrastructuralevaluation. Journal of Periodontology 80, 253–259.
Schatzle, M., Land, N. P., Anerud, A., Boysen,H., Burgin, W. & Loe, H. (2001) The influenceof margins of restorations of the periodontaltissues over 26 years. Journal of Clinical Peri-odontology 28, 57–64.
Schlee, M. & Esposito, M. (2011) Human dermisgraft versus autogenous connective tissue graftsfor thickening soft tissue and covering multiplegingival recessions: 6-month results from apreference clinical trial. European Journal ofOral Implantology 4, 119–125.
Schneider, D., Grunder, U., Ender, A., Hammer-le, C. H. & Jung, R. E. (2011) Volume gainand stability of peri-implant tissue followingbone and soft tissue augmentation: 1-yearresults from a prospective cohort study. Clini-cal Oral Implants Research 22, 28–37.
Schoo, W. H. & van der Velden, U. (1985) Mar-ginal soft tissue recessions with and withoutattached gingiva. A five year longitudinalstudy. Journal of Periodontal Research 20, 209–211.
Seibert, J. S. (1983) Reconstruction of deformed,partially edentulous ridges, using full thicknessonlay grafts. Part II. Prosthetic/periodontalinterrelationships. Compendium of ContinuingEducation in Dentistry 4, 549–562.
Sharma, N. A. & Garud, R. S. (2013) Greaterpalatine foramen–key to successful hemimaxil-lary anaesthesia: a morphometric study andreport of a rare aberration. Singapore MedicalJournal 54, 152–159.
da Silva, R. C., Joly, J. C., de Lima, A. F. & Ta-takis, D. N. (2004) Root coverage using thecoronally positioned flap with or without asubepithelial connective tissue graft. Journal ofPeriodontology 75, 413–419.
Soileau, K. M. & Brannon, R. B. (2006) A histo-logic evaluation of various stages of palatalhealing following subepithelial connective tis-sue grafting procedures: a comparison of eightcases. Journal of Periodontology 77, 1267–1273.
Song, J. E., Um, Y. J., Kim, C. S., Choi, S. H.,Cho, K. S., Kim, C. K., Chai, J. K. & Jung,U. W. (2008) Thickness of posterior palatalmasticatory mucosa: the use of computerizedtomography. Journal of Periodontology 79,406–412.
Staffileno, H., Wentz, F. M. & Orban, B. (1962)Histologic study of healing of split thickness
flap surgery in dogs. Journal of Periodontology33, 56–69.
Steiner, G. G., Pearson, J. K. & Ainamo, J.(1981) Changes of the marginal periodontiumas a result of labial tooth movement inmonkeys. Journal of Periodontology 52, 314–320.
Strebel, J., Ender, A., Paque, F., Krahenmann,M., Attin, T. & Schmidlin, P. R. (2009) In vivovalidation of a three-dimensional opticalmethod to document volumetric soft tissuechanges of the interdental papilla. Journal ofPeriodontology 80, 56–61.
Studer, S. P., Allen, E. P., Rees, T. C. & Kouba,A. (1997) The thickness of masticatory mucosain the human hard palate and tuberosity aspotential donor sites for ridge augmentationprocedures. Journal of Periodontology 68, 145–151.
Studer, S. P., Lehner, C., Bucher, A. & Scharer,P. (2000) Soft tissue correction of a single-tooth pontic space: a comparative quantitativevolume assessment. Journal of Prosthetic Den-tistry 83, 402–411.
Sullivan, H. C. & Atkins, J. H. (1968) Free autog-enous gingival grafts. III. Ultilzation of graftsin the treatment of gingival recession. Periodon-tics 6, 152–160.
Sullivan, H. C. & Atkins, J. H. (1969) The role offree gingival grafts in periodontal therapy. Den-tal Clinics of North America 13, 133–148.
Thalmair, T., Fickl, S., Schneider, D., Hinze,M. & Wachtel, H. (2013) Dimensional altera-tions of extraction sites after different alveolarridge preservation techniques - a volumetricstudy. Journal of Clinical Periodontology 40,721–727.
Thoma, D. S., Benic, G. I., Zwahlen, M., Ham-merle, C. H. & Jung, R. E. (2009) A systematicreview assessing soft tissue augmentation tech-niques. Clinical Oral Implants Research 20(Suppl 4), 146–165.
Thoma, D. S., Jung, R. E., Schneider, D., Coch-ran, D. L., Ender, A., Jones, A. A., Gorlach,C., Uebersax, L., Graf-Hausner, U. & Ham-merle, C. H. (2010) Soft tissue volume augmen-tation by the use of collagen-based matrices: avolumetric analysis. Journal of Clinical Peri-odontology 37, 659–666.
Thoma, D. S., Sancho-Puchades, M., Ettlin, D.A., Hammerle, C. H. & Jung, R. E. (2012)Impact of a collagen matrix on early healing,aesthetics and patient morbidity in oral muco-sal wounds - a randomized study in humans.Journal of Clinical Periodontology 39, 157–165.
de Trey, E. & Bernimoulin, J. P. (1980) Influenceof free gingival grafts on the health of the mar-ginal gingiva. Journal of Clinical Periodontology7, 381–393.
Wei, P. C., Laurell, L., Lingen, M. W. & Geivelis,M. (2002) Acellular dermal matrix allografts toachieve increased attached gingiva. Part 2. Ahistological comparative study. Journal of Peri-odontology 73, 257–265.
Weng, D., H€urzeler, M., Quinones, C., Pechstadt,B., Mota, L. & Caffesse, R. (1998) Healing pat-terns in recession defects treated with ePTFEmembranes and with free connective tissuegrafts. A histologic and histometric study inthe beagle dog. Journal of Clinical Periodontol-ogy 25, 238–245.
Wennstrom, J. L., Lindhe, J., Sinclair, F. & Thi-lander, B. (1987) Some periodontal tissue reac-
tions to orthodontic tooth movement inmonkeys. Journal of Clinical Periodontology 14,121–129.
Wessel, J. R. & Tatakis, D. N. (2008) Patient out-comes following subepithelial connective tissuegraft and free gingival graft procedures. Journalof Periodontology 79, 425–430.
Wilderman, M. N. (1964) Exposure of bone inperiodontal surgery. Dental Clinics of NorthAmerica 8, 23–31.
Wilson, T. G. Jr, McGuire, M. K. & Nunn, M.E. (2005) Evaluation of the safety and efficacyof periodontal applications of a living tissue-engineered human fibroblast-derived dermalsubstitute. II. Comparison to the subepithelialconnective tissue graft: a randomized controlledfeasibility study. Journal of Periodontology 76,881–889.
Windisch, S. I., Jung, R. E., Sailer, I., Studer, S.P., Ender, A. & Hammerle, C. H. (2007) Anew optical method to evaluate three-dimen-sional volume changes of alveolar contours: amethodological in vitro study. Clinical OralImplants Research 18, 545–551.
Yotnuengnit, P., Promsudthi, A., Teparat, T., Lao-hapand, P. & Yuwaprecha, W. (2004) Relativeconnective tissue graft size affects root coveragetreatment outcome in the envelope procedure.Journal of Periodontology 75, 886–892.
Zucchelli, G. (2013) Mucogingival Esthetic Sur-gery. Milan: Quintessenza Ediziono S.r.l.
Zucchelli, G., Amore, C., Sforza, N. M., Monte-bugnoli, L. & De Sanctis, M. (2003) Bilaminartechniques for the treatment of recession-typedefects. A comparative clinical study. Journalof Clinical Periodontology 30, 862–870.
Zucchelli, G., Mazzotti, C., Mounssif, I., Mele,M., Stefanini, M. & Montebugnoli, L. (2013)A novel surgical-prosthetic approach for softtissue dehiscence coverage around singleimplant. Clinical Oral Implants Research 24,957–962.
Zucchelli, G., Mele, M., Stefanini, M., Mazzotti,C., Marzadori, M., Montebugnoli, L. & deSanctis, M. (2010) Patient morbidity and rootcoverage outcome after subepithelial connectivetissue and de-epithelialized grafts: a compara-tive randomized-controlled clinical trial. Jour-nal of Clinical Periodontology 37, 728–738.
Zuhr, O. & H€urzeler, M. (2012) Plastic-EstheticPeriodontal and Implant Surgery - A Microsur-gical Approach. Ltd: Quintessence PublishingCo.
Zuhr, O., Rebele, S., Schneider, D., Jung, R. &H€urzeler, M. (2013) Tunnel technique withconnective tissue graft versus coronallyadvanced flap with enamel matrix derivate forroot coverage: a RCT using 3D digital measur-ing methods. Part I. Clinical and patient-cen-tered outcomes. Journal of ClinicalPeriodontology doi: 10.1111/jcpe.12178. [Epubahead of print].
Address:Otto ZuhrPrivate Practive H€urzeler/ZuhrRosenkavalierplatz 1881925 MunichGermanyE-Mail: [email protected]
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Soft tissue replacement grafts S141

Clinical relevance
Scientific rationale: Soft tissue aug-mentation procedures are increas-ingly performed in plasticperiodontal and implant surgery.Standardized guidelines regardingdonor sites and harvesting tech-niques can hardly be given to date,but recommendations for predict-able treatment outcomes can bedeveloped. The aim was to providea narrative review of the literature
concerning the use of soft tissuereplacement grafts.Principal findings: Subepithelial con-nective tissue grafts are consideredas gold standard. Many questionsregarding graft healing and volumet-ric stability are presently unknown.The limited amount of grafting tis-sue and the increased patient mor-bidity make the search for suitablesoft tissue substitutes an importantfield of future research.
Practical implications: The avail-able donor sites provide grafts ofdistinct shape and composition.Which donor site is chosen dependson the amount of required tissueand the indication. Harvesting andtransplantation procedures shouldfollow certain advices to allow thebest healing and tissue integrationpossible.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
S142 Zuhr et al.