Embed Size (px)
Citation preview
TheActionGroup
onFrailty
Story2012-2014
Part of the European Innovation Partnershipon Active and Healthy Ageing

AcknowledgementsThis report has been prepared by the European Commission, Directorate General for Health andConsumers, Unit 02: Innovation for Health and Consumers, led by Jorge Pinto Antunes. Ines García-Sánchez and Anna Carta where responsible for the drafting in collaboration with the coordinators andtask facilitators of the European Innovation Partnership on Active and Healthy Ageing, Frailty ActionGroup, who stimulated and followed-up di�erent activities of the common work and responded to allour queries.Michael Veale has been responsible for the graphical editing of the manuscript.
Disclaimer
By the European Commission.
The information and views set out in this publication are those of the authors and do not necessarilyre�ect the o�cial opinion of the Commission. The Commission does not guarantee the accuracy ofthe data included. Neither the Commission nor the Action Groups may be held responsible for the usewhich may be made of the information contained therein.
© European Union, 2014. All rights reserved. Certain parts are licensed under conditions to the EU.
Reproduction is authorised provided the source is acknowledged.
Cover picture © iStock.
Executive Summary
The European Innovation Partnership on Activeand Healthy Ageing (hereafter EIP AHA, or thePartnership) was launched in 2012 as a Commis-sion response to demographic changes in the EU.Three years since it was launched, the Partnershipis helping to identify and develop new approachesfor supporting change, placing patients at the cen-tre of health and social care systems, and mov-ing away from hospital-centred, reactive, disease-focused care, and instead towards a proactive, com-munity based model of prevention and continu-ous care management, with the participation ofthe patient and informal care-givers. Furthermore,health and care services supported by ICT systemscan provide alternative ways for better and moretargeted care and more e�cient use of resources.The Action Group on Prevention and Early Diag-nosis of Frailty and Functional Decline, which in-cludes both physical and cognitive decline, in olderpeople (henceforth referred to as Frailty group)wascreated in June 2012 as part of the EIP on AHA.Its aim is to facilitate the work of stakeholders aim-ing to improve the current situation and achieve asupportive organisational context that can remedythe problems of everyday life and clinical practiceencountered by frail older people and their care-givers.
Their objectives and activities address the chal-lenges that fall in any of the following domains:Frailty in general; Cognitive decline; Functionaldecline; Nutrition; Care givers and Dependency;and Physical activity.
It is not easy to disentangle the speci�c impactof the frailty group itself, but it is important thatdi�erent European, national and regional initia-tivesmove in the same direction and build up a crit-
ical mass in the areas of most importance. In thisrespect, framing the idea of the “frailty preventionapproach” has been the most fundamental out-come of the work done by the Frailty group. Un-dertaking actions on advocacy, screening, researchand coordination of care, they have contributedto establishing a common European approach totackle frailty in older people. Furthermore, someof their preliminary results, and the collection ofgood practices can be a source of inspiration forfurther management improvement and policy de-velopment.
This booklet aims to o�er an overview of thefrailty group process, starting from the reasonsthat urged the creation of the group until the cur-rent organisation. In the second part the resultsachieved so far will be analysed. We have chosen topresent them following the same logic that appliesto the frailty group work structure:
• Individual commitmentdeliverables’ results
• Collaborative work achievements
In the coming years e�orts aimed at raising ef-fectiveness of care delivery will be crucial. Workingclosely and sharing ideas and solutions can help theEuropean Union (EU) as a whole to �nd and im-plement new strategies to tackle frailty. The frailtygroup can play a fundamental role in building anEU policy on frailty prevention. This report exam-ines its work process and experiences and pointsout how it can contribute to it.
1

Contents
Contents 2
1 The demographic change in Europe and the EIP AHA 3
2 The Action Group on frailty prevention (frailty group) 52.1 The role of the frailty Action Group . . . . . . . . . . . . . . . . . . . . . . . . . 52.2 The structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52.3 Governance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62.4 Work development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Yammer platform . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8AGMeetings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8TheMarketplace . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8The Conference of Partners . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
3 Actions of the Frailty Group by Domain 93.1 Advocacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93.2 Screening & Prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93.3 Care management & assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . 93.4 Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
4 What has been achieved? 104.1 General outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104.2 Speci�c deliverables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Individual commitments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Common work and deliverables . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
5 Conclusions and the way forward 14
6 Appendix of deliverables and annexes 15
2
1The demographic change inEurope and the EIP AHA
Demographic ageing is one of the most seriouschallenges Europe is facing. Supporting active andhealthy ageing is important both to improve thequality of life of elderly citizens and help them con-tribute to society as they grow older; and to reduceunsustainable pressure on health systems. The Eu-ropean Commission (hereafter EC or the Commis-sion) has launched, among other initiatives, theEuropean Innovation Partnerships within the In-novation Union, one of the �agship initiatives ofthe Europe 2020 strategy, with the objective ofaccelerating innovation to address a well-de�nedtarget within a grand societal challenge. The ECidenti�ed active and healthy ageing as a major soci-etal challenge common to all EUMember States(MS), and as an area presenting considerable poten-tials for Europe to act as a global leader inprovidinginnovative responses.
The EIP on AHA is one of the Commission’sanswers to the demographic challenges that Eu-rope is facing, under the framework of Europe2020 strategy. It sets a target of increasing thehealthy lifespan of EU citizens by 2 years by 2020,and aims to pursue a triple win for Europe by im-proving the quality of life of older people and en-able them to stay active for longer, through activeageing and independent living; improving the sus-tainability and e�ciency of social and health caresystems; and the enhanced competitiveness of Eu-ropean industry through new markets and busi-ness expansion. The Partnership is neither a newfunding programme or instrument nor a new le-gal entity, and does not replace existing decision-making processes.
The EIP AHA re�ects a growing awarenessthat better care and sustainability of health ser-
vices calls for innovative ways to address the needsof the elderly. It has encouraged a wide range ofstakeholders to join forces, to improve coopera-tion, and to foster political commitment, so as toencourage innovative solutions towards a betterquality of life as citizens grow older. It identi�ed aset of actions that could start as early as 2012 anddelivermeasurable outcomeswithin the 2012-2015timeframe.
The Strategic Implementation Plan (SIP) thatwas adopted by the Partnership’s Steering Groupin November 2011, focuses on actions developedaround 3 pillars: A) prevention, screening andearly diagnosis; B) care and cure; and C) activeageing and independent living. Within each pillar,it sets out a limited number of speci�c actions tobe implemented from 2012. These thematic pil-lars are complemented with a set of cross-cuttingpriorities, such as framework conditions, evidenceand funding.
About frailtyFrailty is a complex syndrome ofincreased vulnerability, determinedby life course events, social andpsychological environments. Itrequires timely interventions.Because frailty is not an inevitableconsequence of ageing, we need astronger focus on early diagnosisand screening.An emphasis on prevention canreduce the incidence of frailty andpostpone its onset.
3

CHAPTER 1. THEDEMOGRAPHIC CHANGE IN EUROPE ANDTHE EIP AHA 4
The partners involved in the EIP AHA areorganised in six Action Groups (AG) created inJune 2012. These groups have agreed action planswith concrete activities, deliverables, objectives, re-sources and timeframe to implement successfullythe speci�c actions. They focus on collaborativeprocess of sharing information and solutions onhow to overcome a bottleneck, undertaking ac-tions together andbrainstorming together towardsshared goals. They were built up on the basis oftwo calls for commitment launched by the Euro-pean commission on 2012 and 2013; in total morethan 500 commitments were submitted from upto 300 leading organisations actively forming coali-tions and consortia, covering stakeholders from allEUMS.
One of these six AGs is Action Group on pre-vention of frailty, the frailty group, which aimsto improve the current situation and achieve asupportive organisational context that can remedythe problems of everyday life and clinical practiceencountered by frail older people and their care-givers.
2The Action Group on frailtyprevention (frailty group)
2.1 The role of the frailty Ac-tion Group
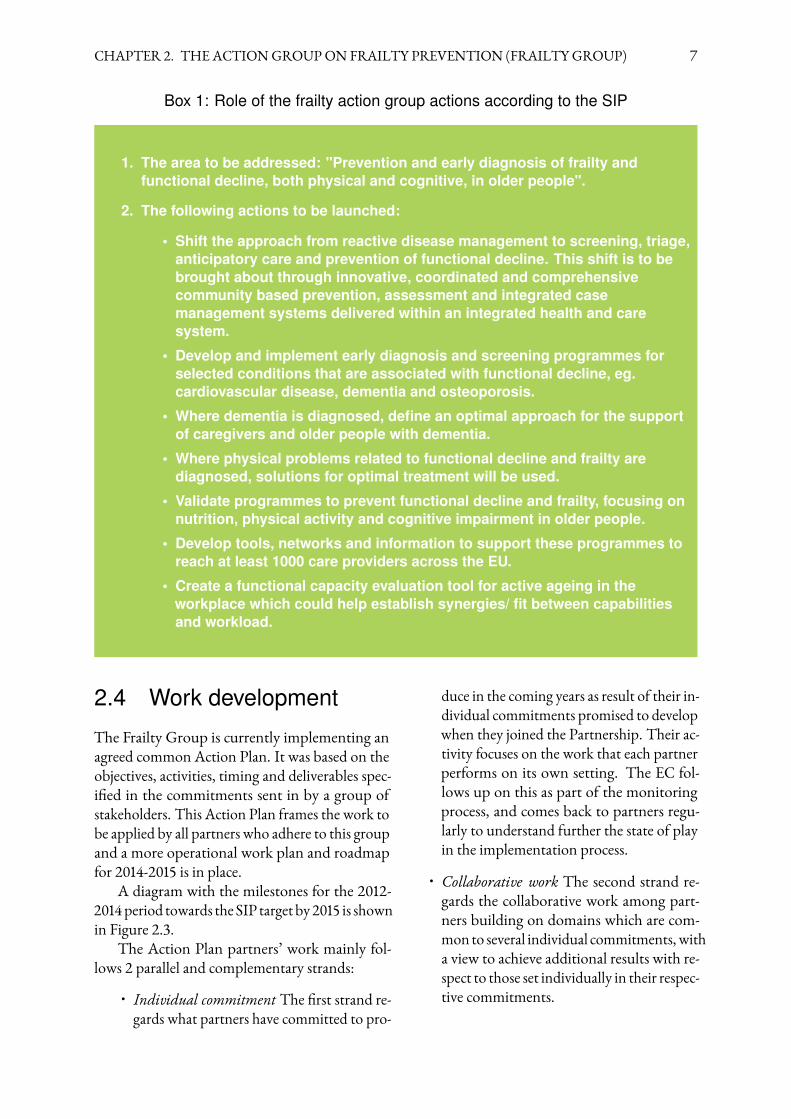
Under pillar on Prevention of the SIP, an Actionon "implementing integrated programmes for pre-vention, early diagnosis and management of func-tional decline, both physical and cognitive, in olderpeople" was identi�ed and ready to start in 2012.The partners who responded to the call committedto the following actions. See Box 1.
2.2 The structure
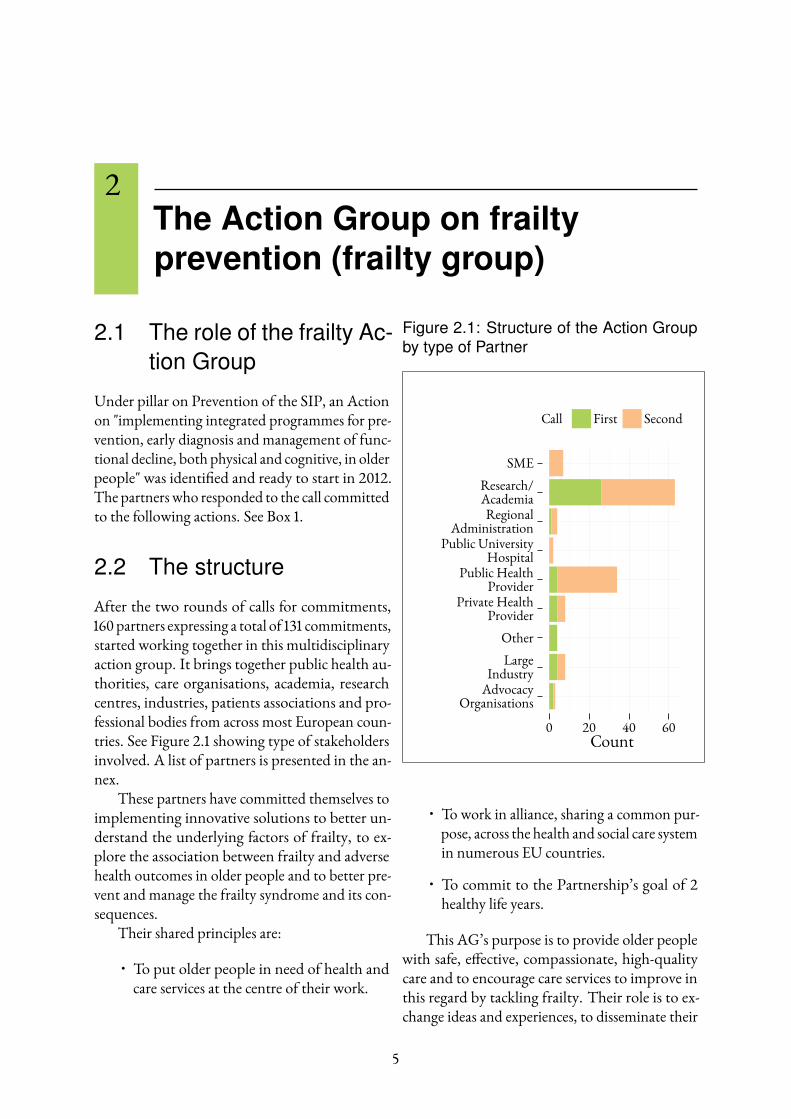
After the two rounds of calls for commitments,160 partners expressing a total of 131 commitments,started working together in this multidisciplinaryaction group. It brings together public health au-thorities, care organisations, academia, researchcentres, industries, patients associations and pro-fessional bodies from across most European coun-tries. See Figure 2.1 showing type of stakeholdersinvolved. A list of partners is presented in the an-nex.
These partners have committed themselves toimplementing innovative solutions to better un-derstand the underlying factors of frailty, to ex-plore the association between frailty and adversehealth outcomes in older people and to better pre-vent and manage the frailty syndrome and its con-sequences.
Their shared principles are:
• To put older people in need of health andcare services at the centre of their work.
Figure 2.1: Structure of the Action Groupby type of Partner
AdvocacyOrganisations
LargeIndustry
Other
Private HealthProvider
Public HealthProvider
Public UniversityHospital
RegionalAdministration
Research/Academia
SME
0 20 40 60Count
Call First Second
• To work in alliance, sharing a common pur-pose, across the health and social care systemin numerous EU countries.
• To commit to the Partnership’s goal of 2healthy life years.
This AG’s purpose is to provide older peoplewith safe, e�ective, compassionate, high-qualitycare and to encourage care services to improve inthis regard by tackling frailty. Their role is to ex-change ideas and experiences, to disseminate their
5
CHAPTER 2. THE ACTIONGROUPON FRAILTY PREVENTION (FRAILTY GROUP) 6
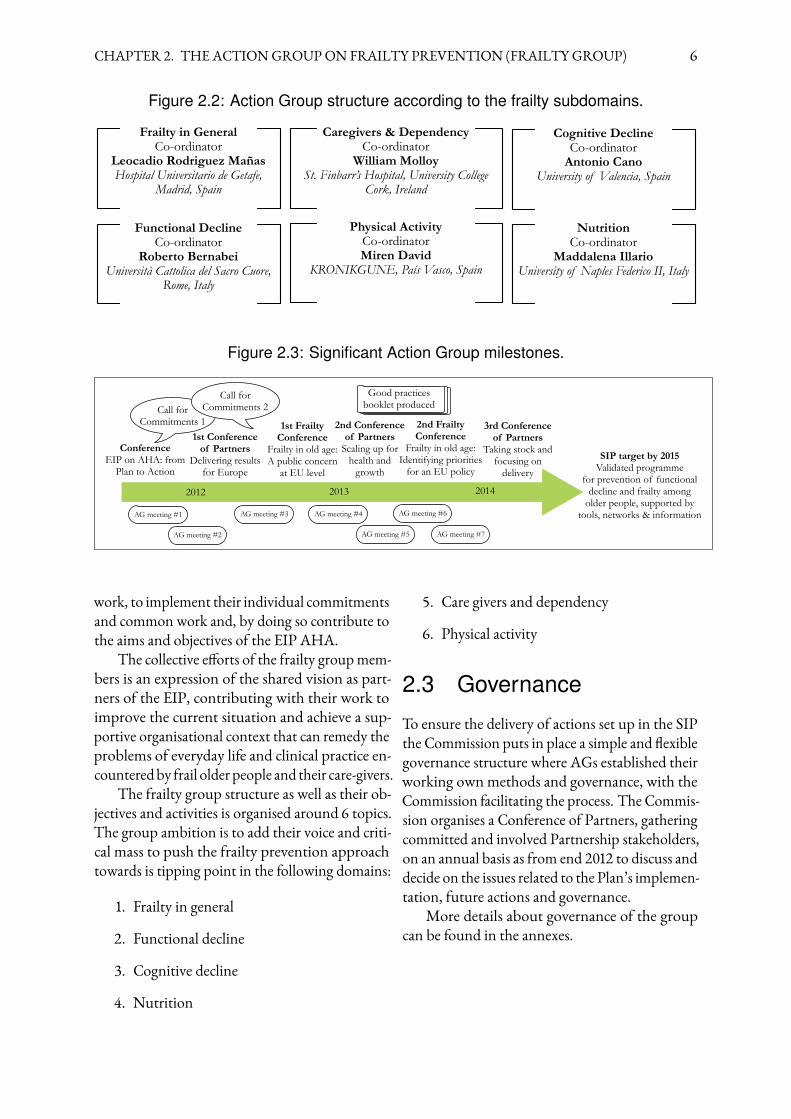
Figure 2.2: Action Group structure according to the frailty subdomains.
Frailty in GeneralCo-ordinator
Leocadio Rodriguez MañasHospital Universitario de Getafe,
Madrid, Spain
Cognitive DeclineCo-ordinator
Antonio CanoUniversity of Valencia, Spain
Functional DeclineCo-ordinator
Roberto BernabeiUniversità Cattolica del Sacro Cuore,
Rome, Italy
NutritionCo-ordinator
Maddalena IllarioUniversity of Naples Federico II, Italy
Caregivers & DependencyCo-ordinator
William MolloySt. Finbarr’s Hospital, University College
Cork, Ireland
Physical ActivityCo-ordinatorMiren David
KRONIKGUNE, País Vasco, Spain
Figure 2.3: Significant Action Group milestones.
ConferenceEIP on AHA: from
Plan to Action
1st Conferenceof Partners
Delivering resultsfor Europe
1st FrailtyConference
Frailty in old age:A public concern
at EU level
2nd Conferenceof Partners
Scaling up forhealth and
growth
2nd FrailtyConference
Frailty in old age:Identifying priorities
for an EU policy
3rd Conference of Partners
Taking stock andfocusing on
delivery
SIP target by 2015Validated programme
for prevention of functionaldecline and frailty among
older people, supported bytools, networks & information
2012 2013 2014
AG meeting #1
AG meeting #2
AG meeting #3 AG meeting #4
AG meeting #5
AG meeting #6
AG meeting #7
Good practices booklet producedCall for
Commitments 1
Call for Commitments 2
work, to implement their individual commitmentsand common work and, by doing so contribute tothe aims and objectives of the EIP AHA.
The collective e�orts of the frailty groupmem-bers is an expression of the shared vision as part-ners of the EIP, contributing with their work toimprove the current situation and achieve a sup-portive organisational context that can remedy theproblems of everyday life and clinical practice en-counteredby frail older people and their care-givers.
The frailty group structure as well as their ob-jectives and activities is organised around 6 topics.The group ambition is to add their voice and criti-cal mass to push the frailty prevention approachtowards is tipping point in the following domains:
1. Frailty in general
2. Functional decline
3. Cognitive decline
4. Nutrition
5. Care givers and dependency
6. Physical activity
2.3 Governance
To ensure the delivery of actions set up in the SIPthe Commission puts in place a simple and �exiblegovernance structure where AGs established theirworking ownmethods and governance, with theCommission facilitating the process. The Commis-sion organises a Conference of Partners, gatheringcommitted and involved Partnership stakeholders,on an annual basis as from end 2012 to discuss anddecide on the issues related to the Plan’s implemen-tation, future actions and governance.
More details about governance of the groupcan be found in the annexes.
CHAPTER 2. THE ACTIONGROUPON FRAILTY PREVENTION (FRAILTY GROUP) 7
Box 1: Role of the frailty action group actions according to the SIP
1. The area to be addressed: "Prevention and early diagnosis of frailty andfunctional decline, both physical and cognitive, in older people".
2. The following actions to be launched:
• Shift the approach from reactive disease management to screening, triage,anticipatory care and prevention of functional decline. This shift is to bebrought about through innovative, coordinated and comprehensivecommunity based prevention, assessment and integrated casemanagement systems delivered within an integrated health and caresystem.
• Develop and implement early diagnosis and screening programmes forselected conditions that are associated with functional decline, eg.cardiovascular disease, dementia and osteoporosis.
• Where dementia is diagnosed, define an optimal approach for the supportof caregivers and older people with dementia.
• Where physical problems related to functional decline and frailty arediagnosed, solutions for optimal treatment will be used.
• Validate programmes to prevent functional decline and frailty, focusing onnutrition, physical activity and cognitive impairment in older people.
• Develop tools, networks and information to support these programmes toreach at least 1000 care providers across the EU.
• Create a functional capacity evaluation tool for active ageing in theworkplace which could help establish synergies/ fit between capabilitiesand workload.
2.4 Work development
The Frailty Group is currently implementing anagreed common Action Plan. It was based on theobjectives, activities, timing and deliverables spec-i�ed in the commitments sent in by a group ofstakeholders. This Action Plan frames the work tobe applied by all partners who adhere to this groupand a more operational work plan and roadmapfor 2014-2015 is in place.
A diagram with the milestones for the 2012-2014period towards the SIP target by2015 is shownin Figure 2.3.
The Action Plan partners’ work mainly fol-lows 2 parallel and complementary strands:
• Individual commitment The �rst strand re-gards what partners have committed to pro-
duce in the coming years as result of their in-dividual commitments promised to developwhen they joined the Partnership. Their ac-tivity focuses on the work that each partnerperforms on its own setting. The EC fol-lows up on this as part of the monitoringprocess, and comes back to partners regu-larly to understand further the state of playin the implementation process.
• Collaborative work The second strand re-gards the collaborative work among part-ners building on domains which are com-mon to several individual commitments, witha view to achieve additional results with re-spect to those set individually in their respec-tive commitments.

CHAPTER 2. THE ACTIONGROUPON FRAILTY PREVENTION (FRAILTY GROUP) 8
Strategic implementation plan(SIP) target“implementing integratedprogrammes for prevention, earlydiagnosis and management offunctional decline, both physical andcognitive, in older people”
The strength of their work within the Part-nership is that every member contributes to theachievement of common objectives. On the samewavelength, together they explore common solu-tions for the key challenges related to frailty, physi-cal decline, cognitive decline as well as risks factorssuch as malnutrition or lack of physical activity forolder people.
Both strands focus on certain areas where ac-tions related to frailty have to advance such as ad-vocacy, care management and assessment, and re-search. They are summarised in the next section.
In addition to this, a wide variety of di�erenttools to support work implementation are in place.
Yammer platformA collaborative platform called “Yammer” is themain communication tool among the Commis-sion the Frailty group partners; documents andfollow-up news are regularly posted on it. It isalso the place to post individual comments andfollow-up discussions among the group members.Partners are invited to use it as much as possibleto exchange information, comments, documents,and anything else that could be useful to the activ-ities of the Group.
AG MeetingsAt least twice a year, partners are invited to at-tend meetings in Brussels. Two group meetingsare scheduled yearly. The main objectives are theexchange of information according to the agreedagenda between the Commission and the Partners,and the reinforcement of the AG dynamic.
No �nancial aid is available for attending thesemeetings
The MarketplaceTheMarketplace is an online platform for informa-tion about the Partnership and to help exchangeviews, �nd partners for speci�c projects or for in-teraction among the partners and outside stake-holders interested in the topic.
The Conference of PartnersThe Conference of Partners is a gathering eventorganised by the Commission on an annual ba-sis to discuss and decide on issues related to theimplementation of the action plans and future ac-tions. Between 2012 and 2013, three Conferencesof Partners have been held in Brussels.
How to reach the SIP target?
• Developing individualcommitments in action groupsand incorporating new partnersthat fill in identified gaps.
• Peer-review validation ofcommon work deliverables andmaking them accessible to EIPAHA partners and the widerpublic.
• Open the process toincorporate new interventions,good practices and newevidence into the action groupwork.
• Find support from theCommission to facilitate aprocess that allows coachingbetween partners’ experiencesand sharing outcomes.
• Access to funding to supportproject proposals and ongoingactivities.
3Actions of the Frailty Group byDomain
This section summarises the main actions of thefrailty group, ordering them by the domain inwhich they fall.
3.1 Advocacy
• Informing the opinion on frailty interven-tions at levelswherepriorities are determinedand decisions are taken.
• Bringing attention to the issue of frailty inolder people being a common EU publichealth problem.
3.2 Screening & Prevention
• Preventing occurrence of frailty and avoid-ing its predictable negative consequences.
• Preventing factors, such as malnutrition orlack of regular physical activity, which haveimpact ondi�erent components of the frailtysyndrome.
• Supporting adequate nutrition and physicalactivity.
• Prevention, screening and early assessmentof risk factors.
3.3 Care management & as-sessment
• Supporting evidencebased interventions throughappropriate pathways of health and socialcare to avoid frailty, its progression to dis-ability and its negative consequences.
• Diminishing avoidable and recurrent hospi-talizations.
• Trainingprofessionals to improve their knowl-edge and skills andkeeppacewithnewneeds.
• Supporting care-givers in their tasks of car-ing for their dependant relatives.
• Identifying those patients whose outcomeshave the higher costs for the health system.
• Identifying thosemost at risk and thosewhowill bene�t most from the interventions.
• Supporting a multi-disciplinary approachto care and management.
• Evaluating current interventions, and sup-porting what really works.
• Supporting care and preventive interven-tions that can be delivered within the com-munity.
• Sharing good practices ready to scale up.• Implementing guidelines to improve man-agement and prevention of frailty.
3.4 Research
• Finding solutions to new challenges.• Looking for new and e�cient ways of solv-ing old problems.
• Improving methodology for the screeningand identi�cation of pre-frail status.
• Basic research development on any of thesix content domains of frailty.
9
4What has been achieved?
4.1 General outcomes
In almost 3 years of collaboration the AG partnershave managed to establish a common approachto provide older people with safe, e�ective, com-passionate, high-quality care and to encourage careservices to improve in this regard by tackling frailtyin older people. Although the activities are still inearly stages, the action group has already achievedsome results, such as:
• Amore comprehensive and clear understand-ing of frailty and its priorities. The exchangeof knowledge and expertise among partnershas resulted in the identi�cation of clearbenchmark on 6 main areas of intervention:frailty in general, physical decline, cogni-tive decline, nutrition, dependency and caregivers, physical activity.
• Contribution to the policy debate at EU level,providing technical inputs to theECon frailtyand functional decline in particular throughthe international conferences on frailty or-ganised by the Commission. OnApril 2013,an international conference on frailty in oldage, addressing the issue from the perspec-tive of a public health concern for the EUand in 18th June 2014, a second one focus-ing on identifying priorities for an EU pol-icy on frailty. Both conferences have beenuseful to give visibility to the work of thefrailty group and building up the supportof the convenience of addressing frailty pre-vention at EU level.
• More reliable trials, many partners had theopportunity to test their protocols and tools
in broader settings, allowing strengtheningthe reliability of both protocols and tools.(e,g: see deliverables from sub-group em-powerment and care-givers)
• Shaping a new model for screening, treat-ment and monitoring of frailty and func-tional decline in community and clinical set-tings. (eg: See deliverables of sub-group onfrailty and physical decline)
• A more suitable training o�ering for health-care professionals. Di�erent groupmembershave proposed improved training coursesfor nurses, social workers and PhD studentson frailty topics. (e.g: see speci�c individu-als commitments annex)
• A collection of good practices in frailty pre-vention. The �nal text gathers 98 good prac-tices coming from 14Member States. It of-fers a grasp of what are the main achieve-ments and what kind of experiences are be-ing carried out in some European regionsaround the topic of frailty and functionaldecline. The numerous and varied examplesof Good Practices, promote the visibility ofa wide range of interventions undertakenin clinical settings, research centres and inthe community, aimed to reduce age-relatedfrailty, disability and su�ering associated toit. (see Good practices booklet publication)
• Specific deliverables and potentially trans-ferable results from either individual com-mitments or common work. (see followingsections and annexes)
10
CHAPTER 4. WHATHAS BEENACHIEVED? 11
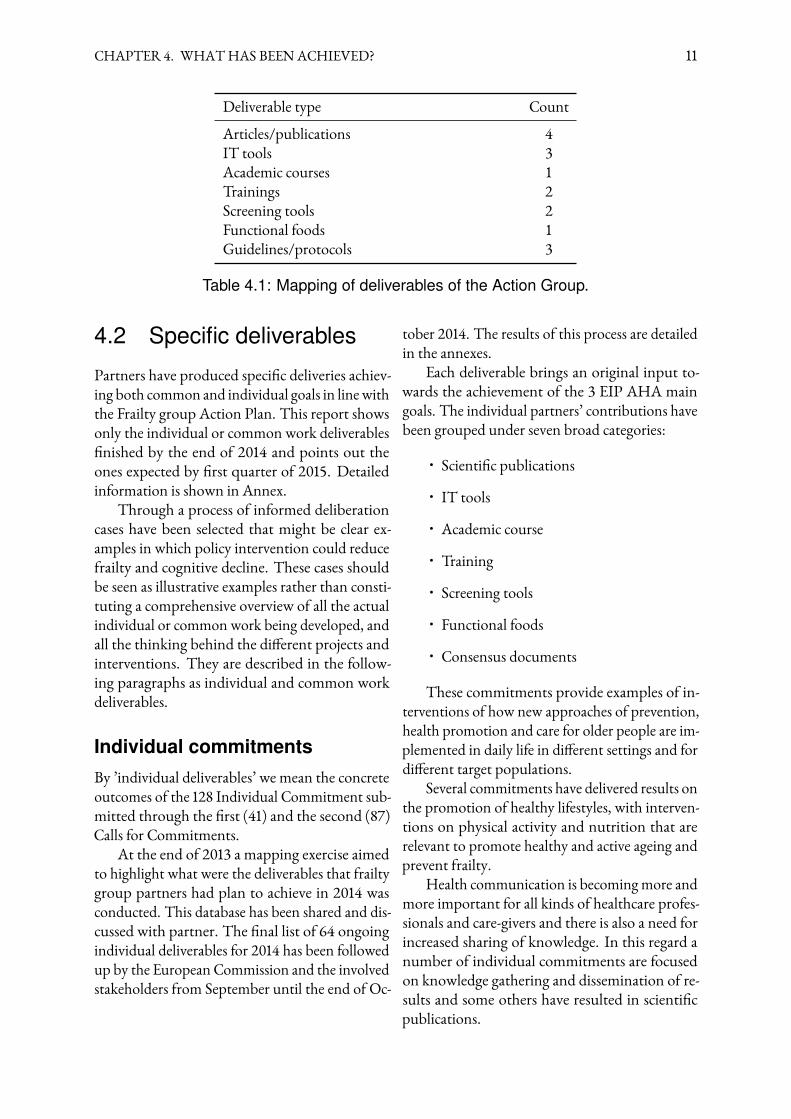
Deliverable type CountArticles/publications 4IT tools 3Academic courses 1Trainings 2Screening tools 2Functional foods 1Guidelines/protocols 3
Table 4.1: Mapping of deliverables of the Action Group.
4.2 Specific deliverables
Partners have produced speci�c deliveries achiev-ing both common and individual goals in linewiththe Frailty group Action Plan. This report showsonly the individual or common work deliverables�nished by the end of 2014 and points out theones expected by �rst quarter of 2015. Detailedinformation is shown in Annex.
Through a process of informed deliberationcases have been selected that might be clear ex-amples in which policy intervention could reducefrailty and cognitive decline. These cases shouldbe seen as illustrative examples rather than consti-tuting a comprehensive overview of all the actualindividual or common work being developed, andall the thinking behind the di�erent projects andinterventions. They are described in the follow-ing paragraphs as individual and common workdeliverables.
Individual commitmentsBy ’individual deliverables’ we mean the concreteoutcomes of the 128 Individual Commitment sub-mitted through the �rst (41) and the second (87)Calls for Commitments.
At the end of 2013 a mapping exercise aimedto highlight what were the deliverables that frailtygroup partners had plan to achieve in 2014 wasconducted. This database has been shared and dis-cussed with partner. The �nal list of 64 ongoingindividual deliverables for 2014 has been followedup by the European Commission and the involvedstakeholders from September until the end of Oc-
tober 2014. The results of this process are detailedin the annexes.
Each deliverable brings an original input to-wards the achievement of the 3 EIP AHA maingoals. The individual partners’ contributions havebeen grouped under seven broad categories:
• Scienti�c publications
• IT tools
• Academic course
• Training
• Screening tools
• Functional foods
• Consensus documents
These commitments provide examples of in-terventions of how new approaches of prevention,health promotion and care for older people are im-plemented in daily life in di�erent settings and fordi�erent target populations.
Several commitments have delivered results onthe promotion of healthy lifestyles, with interven-tions on physical activity and nutrition that arerelevant to promote healthy and active ageing andprevent frailty.
Health communication is becomingmore andmore important for all kinds of healthcare profes-sionals and care-givers and there is also a need forincreased sharing of knowledge. In this regard anumber of individual commitments are focusedon knowledge gathering and dissemination of re-sults and some others have resulted in scienti�cpublications.

CHAPTER 4. WHATHAS BEENACHIEVED? 12
Core achievements of thegroup so far
• Shaping a new model forscreening, treatment andmonitoring of frailty anddunctional decline incommunity and clinicalsettings.
• Scaling up of screeningactivities
• International and interregionalcollaboration (e.g. ondeliverables)
• A more comprehensive andclear understanding of frailtyand its EU policy priorities.
Anumber of partners have delivered results onprevention tools on frailty, malnutrition, and anassessment instrument to predict survival, health-related outcomes and to forecast health resourceuse and costs after discharging frail patients fromhospital.
One partner has developed a new functionalfood rich in bioactive compounds with plant andalgae ingredients. The food is currently under pro-duction at lab scale.
Detailed information on all individual com-mitments delivered until date can be consulted inthe annexes.
Common work and deliverablesCommonworkhas been engaged in since July 2013.The purposes of starting this strand of work areshow below:
• Develop a group with a common approachto speci�c issues e.g. how to promote screen-ing in clinical settings or how to interveneto prevent malnutrition.
• Work on a proactive approach instead ofreactive way.
• Putting together a commonway of thinkingon speci�c frailty related topics.
• Map experiences where knowledge has beenput into practice.
• Map existing useful interventions that aremaking a di�erence at local level (althoughtime is needed to assess results of real changes).
• Identify what has to be done or has to bedone di�erently in speci�c topics.
• Achieve additional results with respect tothose set individually in their respective com-mitments.
• Clarify “state of art” on best interventionson frailty related topics.
Although it is an ongoing activity, a great dealof progress has been made in areas of commoninterest and yields potentially transferable resultsto other settings and target populations.
The common work deliverables re�ect the cur-rent challenges on frailty prevention and treatmentand are evidence based; there are enough articlespublished in scienti�c journals to support the state-ments in which the sub-groups based their activi-ties and recommendations. The deliverables trans-late partners’ knowledge and experience on causesand mechanisms of the ageing process into strate-gies and comprehensive guidelines to prevent andtreat frailty in older people. Furthermore, they aresuitable ways of bringing evidence and providingkey answers on tackling frailty to the attention ofpolicymakers, clinicians and health and social caremanagers.
Key messages resulting from the frailty groupdiscussions, deliverables andpublications are shownin Box 2.
CHAPTER 4. WHATHAS BEENACHIEVED? 13
Box 2: Key messages from EIP AHA group on frailty prevention
• Frailty is a complex syndrome of increased vulnerability, determined by lifecourse events, social and psychological environment, which requires timelyinterventions. Because frailty is not an inevitable consequence of ageing, weneed a stronger focus on early diagnosis and screening.
• Frailty, functional, and cognitive decline are highly prevalent in old age andconstitute major public health problems. Understanding frailty is a particularchallenge from a clinical, research and public health perspective. There is aneed to improve the understanding around frailty for healthcare professionals,care personnel, informal and family care-givers and patients.
• An emphasis on prevention can reduce the incidence of frailty and postpone itsonset. People who are fit when they become old and who remain physically andmentally active have a better chance of avoiding or postponing frailty, and areoften also better at managing functional decline when it occurs.
• Older people aged 65 can expect less than half of their remaining years to befree from conditions affecting their ability to manage daily living activities andrequiring both medical and social care on a continuing basis. The risk ofneeding long-term care (LTC) rises steeply from the age of 80. Our ability tomanage it will have major implications for the wellbeing of individuals andfamilies and for public expenditure.
• There is a need to start focusing our attention on function. Efforts should bemade to help people live independently. To achieve this, we need increased useof innovative, coordinated and comprehensive community based prevention,delivered within an integrated health and care system. Furthermore, there is aneed to distinguish between chronic diseases and frailty despite their commongrounds which usually ends in treating them as a unique problem.
• The impact of frailty in health and social services made it clear the importanceand the urgency of tackling and modernising our health and social services.There is a need to shift from reactive disease management to screening,anticipatory care and prevention of frailty and functional decline in old people.Well-planned, coordinated and effective health and social service interventionsin the frail older population can have a significant impact on health outcomes;on quality of life; and on the sustainability of resources.
• There is need not only to prevent frailty, functional decline, malnutrition,cognitive decline and other issues by strengthening prevention and screeningpolicies, but also to find alternative solutions to the institutionalisation ofpatients. These alternatives should include care-givers support, housingadaptations, tele-healthcare networks, professionals training. They willstrengthen the independency of frail people and may act as a brake on thefunctional and cognitive decline of older people.
• Frail older adults require a proactive, multimodal, coordinatedmulti-disciplinary and multiagency approach, preferably delivered in anintegrated health and care system.
5Conclusions and the way forward
The need to tackle frailty in the older people acrossthe EU is now accepted by a large number of stake-holders spanning policy makers, professionals, re-searchers and academics across EUMember States.It can be assume that the focus will be to concen-trate in supporting scaling-up good practices andon the process of developing an EU frailty policy.
The Frailty group partners are committed towork towards solutions that can be easily imple-mented and replicated by others in Europe. Thisaspect emphasises the spirit of the Partnership in abroader context and strengthens the work alreadydone bymany of them. These 3 years of work haveestablished a solid ground on which to build com-mon and e�ective approaches to tackle frailty inolder age. But still further work, policy supportand resources are needed so that tackling frailty inolder people is no longer an issue of public debate.
The work of the Frailty group provides thenecessary input regarding examples of innovativepractices that can improve the quality of life of frailolder people and help reduce the burden of inef-�ciency in care delivery. The on-going work pro-vides a practical illustration of the main elementsupon which to base a future policy on frailty.
Finding new tools and strategies to preventand treat frailty in all its dimensions will not onlyimprove the quality of life of older people dramat-ically, but will also reduce both the number andthe length of hospitalisation and institutionalisa-tion. The �nal results potentially will alleviate thebudgetary pressure of our health and social caresystems, allowing EUMembers States to allocatemore e�ciently the resources for the health andcare of their citizens.
EUMember States need to move from a pri-
marily reactive to an increasingly proactive policyapproach, which seeks both to reduce care demandand toboost cost-e�ective care provision. Such a re-sponse has to be led byMember States’ authorities.The Partnership provides a platform for nationaland regional authorities and key stakeholders tocoordinate and mobilise actions in strategic areas,identify good and relevant practices, �nally repli-cate and scale-up the most needed and successfulsolutions.
In the coming years e�orts aimed at raising ef-fectiveness of care delivery will be crucial. Workingclosely and sharing ideas and solutions can help theEU as a whole to �nd and implement new strate-gies to tackle frailty. This report shows the workprocess and some experiences of the Frailty groupthat could support an EU policy. Through imple-mentation of innovative solutions and new waysof thinking and doing, the Partnership can sup-port to make the needed changes happen fasterand wider.
There is a case for tackling frailty in older peo-ple at EU level: the causes and high prevalence; thenumerous and costly consequences and the rela-tively in-expensive interventions are common to allMember States. Furthermore, this common chal-lenge and its solutions fall across multiple policyspheres; that is why a concerted action is needed, aswell as coordination amongst di�erent stakehold-ers, intervening in 3main areas: screening/assessment;management and research. The work of the Frailtygroup of the EIP on AHA can play a role in sup-porting the building process of an EU policy onfrailty prevention that will support these changes.
14
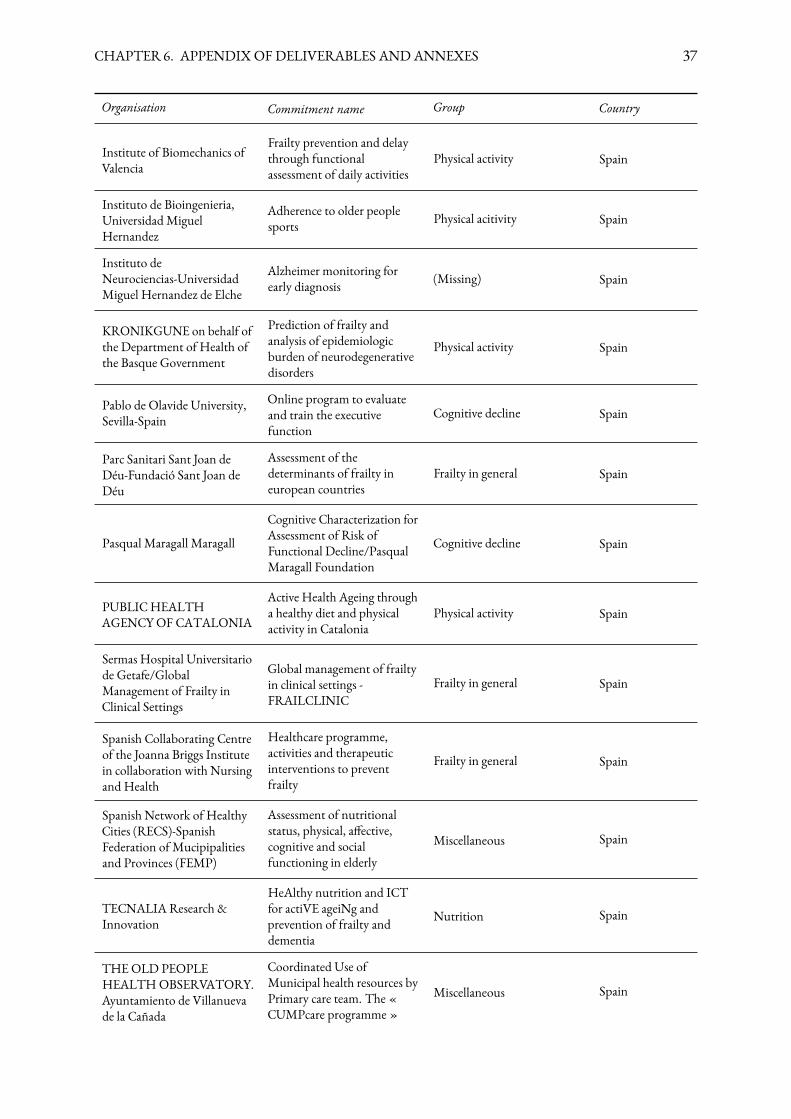
6Appendix of deliverables andannexes
The appendix contains speci�c information on the collaborative deliverables produced by subgroups.These include:
• Physical Activity Subgroup: Deliverables produced by common work
• Nutrition Subgroup: Deliverables produced by common work
• Frailty & Physical Decline Subgroup: Deliverables produced by common work
• Cognitive Decline Subgroup: Deliverables produced by common work
• Dependency and Caregivers Subgroup: Deliverables produced by common work
It also contains two relevant annexes:
1. The Action Group Partners
2. Individual Commitment Deliverables 2014
15
Physical Activity Subgroup:Deliverables produced bycommon work
Product
White paper on physical activity and its relation with frailty in older people.
Description
Document aiming to disseminate up to date information to clinicians, researchers andmanagers lookingto �nd their way into physical activity and frailty.It looks at: A) what we mean by physical activity, B) how it is operationalized or measured, C) mostrelevant current research issues and D) builds on a structured overview of developing interventions inEurope, under the umbrella of the EIP AHA.
Added value
Increased standardisation of physical activity screening methods, and re�nement of research ques-tions such as: A) the di�erence between measurement of frailty through physical activity and themeasurement of physical function, B)What measuring frailty through physical activity is and what it isnot.
What follows
Publishing the white paper and distribution on the EIP AHA Summit in 1Q of 2015 as an outcome ofthe collaborative work of frailty Action Group.
Comments
The sub-group is working (ongoing activity) also on two other products:1. A research paper on screening of frailty through physical activity. They have has collected structuredinformation on 25 regional commitments related with the measurement of frailty through physicalactivity. This has been done through a custom designed Table of contents distributed via Yammerand email. Preliminary results show that commitments use di�erent batteries of indicators to measurefrailty and pre-frailty status. A pool of over 2000 frail patients from which indicators on physical
16

CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 17
activity that have been or are being collected all around Europe has been identi�ed and analysed. Ameta-analysis of the results of 25 European studies on screening, monitoring or implementing physicalactivity interventions will contribute to achieve a higher statistical power for the measurements andoutcomes of interest. The paper will be designed during the �rst half of 2015 but key informationwill be collected during the second half of 2015 when most of the interventions under the umbrella ofPhysical Activity Action Area will already have been �nished and published. They have produced abaseline report on strategies for screening, monitoring and managing frailty through physical activityin Europe.2. A European Database onManagement of Frailty, comprising information on screening, monitoringand intervening on frail patients. Well de�ned but poorly standardized frailty indicators and patientselection criteria for interventions have been identi�ed by the group as important barriers for thegeneralization and understanding of the management of frailty in Europe. A population (strati�cation)or individual (targeted screening) approach for the management of frail patients remains nowadays atopic of discussion between healthcare professionals interested in the management of frailty as it refersto a condition for which consensus between experts still needs to be achieved. A European Database onthe management of frailty would serve as a reference for European healthcare professionals that aim to�nd their way through the myriads of documents published on the topic. More likely to be based onthe European reality rather than the easier available North-American literature, the proposed Europeandatabase would help answer current research questions such as: A) 150 minutes of physical activity foreveryone is the standard in the US but can we relate this number for the European reality? B) Are ourfrail populations equal? C) Do we have access to the same facilities? D) Do we share equal bene�ts?The database would build on the results of the EIP AHA Frailty Action Group, not exclusively thephysical activity sub-group. It would be a web based access database starting by collecting informationon a literature search (agreed by all coordinators of Frailty AG on the 22 of October 2014).
Nutrition Subgroup: Deliverablesproduced by common work
Product
1. Consensus Document “Testing and implementing an integrated approach to nutrition: fromassessment to personalized interventions”.2. Organization of an international EIP-AHANutrition workshop in Rome, 17th October 2014.
Description
1. The document presents a common understanding of malnutrition looking at both elderly peoplewho have undernutrition and those with obesity, including those with sarcopenic obesity. It supportsa common vision where e�ective intervention should take into account the entirety of needs thatin�uence the adequacy of nutrition and has a strong focus on primary prevention.2. The workshop was the opportunity to present the consensus document and discuss on di�erentprojects and interventions that individual partners are developing, either as oral sessions or as posterpresentations. It was organized under the auspices of the Mattone Internationale project.
Added value
The group has worked out a consensus document on nutrition with a common vision that brings up anovel integrated nutritional approach with a strong focus on primary prevention. The new aspect offood support will provide new evidence for primary prevention of malnutrition and also create an EUwide change for agriculture, food supply, new jobs and will o�er new economic perspectives.The aim is to improve the chain of care by translating the group knowledge on mechanisms of theageing process, food and culinary innovations, and dietary recommendations into comprehensiveguidelines and strategies to prevent and treat malnutrition in older people.
What follows
The document will be published in the Journal of Aging Research in response to the open call on“Active and Healthy Ageing and Independent Living” by the end 2014.
18

CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 19
Comments
Partners have also been working on two additional areas which will be further developed in followingyears:1. Nutrition dissemination events e.g: Optimal Nutritional Care for All Implementation ENHAConference, Brussels 2014 or the Health campus events in di�erent regions in Italy.2. Functional Foods and supplements Innovative products development; e.g: Vit. D forti�ed extravirginolive oil (Mataluni); Flavonoid fraction of Bergamot juice; polyphenolic compounds extracted fromgreen lettuce (Lactuca sativa L.; var. Maravilla de Verano).
Frailty & Physical DeclineSubgroup: Deliverables producedby common work
Product
1. Guidelines on instruments for screening and diagnosis of frailty and functional decline.2. Pathways for the management of older people based on their functional status and setting of care
Description
1. The Guidelines analyses frailty and functional impairment assessment tools considering if thesetools have been validated and in which settings they have been used. Furthermore, frailty is a dynamicfunctional state and as frailty, functional decline and disability are di�erent, although they can bepresent at the same time in an older adult, it is necessary to use di�erent tools to assess them. They aredescribed separately in the document2. The pathways document A) gives indications on simple, feasible and brief care approaches andpathways and B) Provides a repository of quality indicators that can be used in di�erent settings inrelation to frailty and physical decline.
Added value
Provides an easy-to-use instrument for decision taking to health professionals that need to assess frailtyin daily practice in clinical and social settings.Provides a framework for the development of integrated care systems for older people and guidelineson levels and ways of care and support that should be provided for each older person according to theirfunctional status and setting of care.Provides a common vision on what an e�ective intervention should take into account.
What follows
Advocacy for using the available instruments in a uniform way so that the likelihood of having homo-geneous and interchangeable data from all the EU regions will increase signi�cantly.Advocacy for implementing this approach in clinical and social care settings.
20

CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 21
Comments
The work of this sub-group adds to the growing interest on the topic of healthy ageing. It has beenpresented in a symposium in theWorld Congress on Gynaecological Oncology (Florence 2014) andwill be in the coming European Congress of EMAS inMadrid (2015).The sub-group is also working (ongoing activity) on three other products that will be ready for Q12015:1. The use of a serious games platform in screening for mild cognitive decline. Validation of the tooland large scale screening on people older than 50 years living in the community. It links 3D virtualtasks to the assessment of cognitive function, giving close consideration to usability and validation.2. Revision of biomarkers to follow-up cognitive decline and dementia. Based on a critical approach tothe role of biomarkers from biological �uids and magnetic resonance images in the management ofcognitive decline.3. Status of art concerning monitoring of the main forms of cognitive decline. They have prepared anarticle “Functional and structural magnetic resonance for detection of neurological impairment”.4. Analyses of datasets fromongoing longitudinal studies in the trajectories of cognitive decline betweenfour longitudinal studies in England [English Longitudinal Study of Ageing (ELSA)], Ireland [IrishLongitudinal Study on Ageing (TILDA)], Spain [Chronic Ailment Reduction after Menopause(CARMEN)] and the smaller scale Extra Care data in England. It will facilitate sharing of analyses andmodelling delivering insights into the predictors of transitions. It will give anthropometric data ofwomen from 4 di�erent European countries.
Cognitive Decline Subgroup:Deliverables produced bycommon work
Product
Scienti�c publication
Description
It is the �rst result of a common task developed by this sub-group. A review of evolution of MCI(mild cognitive impairment) to dementia will be published in complete issue of the scienti�c journalMaturitas (1st quartile in the JSR), which will be entitled: “Personalized healthcare for midlife andbeyond” is being prepared, the editors being Prof. AntonioCano and Prof. Tommasso Simoncini, fromthe University of Pisa, Italy. The contents will include 15 papers, whose authors, already con�rmed andlisted, are �rst-rank scientists from all over the globe. Together with the inclusion in EIP AHA of theeditor, the common work of the group is represented by the participation of Prof. L Calzá as author ofthe paper number 13 (Should we screen. . . ?, see below). The publication is due for the 1Q 2015.
Added value
The impact on the scienti�c community with interest on ageing: Maturitas is a high impact journalread around the world, but more particularly in Europe and North America. The scope of the journalis all aspects related with ageing.
What follows
The publication will increase the interest on aspects related with EIPAHA, and has involved theparticipation of EMAS (European Society of Menopause and Andropause) in one application to oneof the recent Horizon Calls (PHC26), where several members of the cognitive decline group wereparticipating
Comments
The work of this sub-group adds to the growing interest on the topic of healthy ageing. It has beenpresented in a symposium in theWorld Congress on Gynaecological Oncology (Florence 2014) and
22

CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 23
will be in the coming European Congress of EMAS inMadrid (2015).The sub-group is also working (ongoing activity) on three other products that will be ready for Q12015:1. The use of a serious games platform in screening for mild cognitive decline. Validation of the tooland large scale screening on people older than 50 years living in the community. It links 3D virtualtasks to the assessment of cognitive function, giving close consideration to usability and validation.2. Revision of biomarkers to follow-up cognitive decline and dementia. Based on a critical approach tothe role of biomarkers from biological �uids and magnetic resonance images in the management ofcognitive decline.3. Status of art concerning monitoring of the main forms of cognitive decline. They have prepared anarticle “Functional and structural magnetic resonance for detection of neurological impairment”.4. Analyses of datasets fromongoing longitudinal studies in the trajectories of cognitive decline betweenfour longitudinal studies in England [English Longitudinal Study of Ageing (ELSA)], Ireland [IrishLongitudinal Study on Ageing (TILDA)], Spain [Chronic Ailment Reduction after Menopause(CARMEN)] and the smaller scale Extra Care data in England. It will facilitate sharing of analyses andmodelling delivering insights into the predictors of transitions. It will give anthropometric data ofwomen from 4 di�erent European countries.
Dependency and CaregiversSubgroup: Deliverables producedby common work
Product
CARTS programme ( Community Assessment of Risk and Treatment Strategies)Short screening tool (RISC) and Community Assessment of Risk Tool (CART) tools
Description
Screening for Frailty as a state of vulnerability that causes risks of institutionalisation, hospitalisationand death. Short screening tool (RISC), this short screening tool scores concerns in three domains,mental state, ADL and medical issues.It also scores concerns, their severity and caregiver capacity to manage these concerns. Finally, it scoresglobal risk of three adverse outcomes nursing home placement, hospitalization and death. It uses asimple score sheet, developed in Ireland as part of the CARTS programme, within the framework ofthe 3 star reference site COLLAGE. . . . and tested in Portugal, Spain, Northern Ireland and Australia.In Ireland, 803 people were screened in 2012 and followed. The one-year incidence of institutionali-sation, hospitalisation and death was determined and the accuracy of the RISC was compared to theClinical Frailty Scale (CFS).This study looks at high-risk individuals only, so fundamentally looks at a di�erent group of peoplethan the CFS. High-risk individuals in this methodology, interestingly, have a higher risk of adverseoutcomes, and the model of frailty here, looking at these outcomes of interest, is better than the CFS.The fundamental point is that a major contribution to risk is the caregiver network, rather than theperson themselves. The ability of the caregiver network to manage issues is a bigger predictor of theseadverse outcomes than the problems themselves.Screening in other countries using theRISC tool: Ireland 803/Portugal 1318/ Spain, Barcelona 374/Aus-tralia 468/Northern Ireland 294.
Added value
This innovative approach will screen large numbers of individuals quickly to provide a pro�le of riskin the community and identify associated causes. A central outcome of this work will be to provide arisk pro�le of this community, document the natural history of risk with various outcomes e.g. frailty,hospitalization, nursing home placement and death. At the same time, it will identify the healthcareneeds of this vulnerable population, to build capacity and inform service planning to make healthcare
24

CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 25
systems more e�cient, safe and sustainable.The programme is standardized, with rigorous administration and scoring guidelines and trainingprograms that are standardized and validated. It has shown versatility across other EU regions and caneasily be customised and up-scaled.
What follows
An application for Horizon 2020 has been submitted to Implement and evaluate the CommunityAssessment of Risk and Treatment Strategies (CARTS) programme. This project will study the e�ectsof an innovative multifactorial screening, triage with targeted interventions on adverse outcomes(hospitalisation, institutionalisation and death) in community dwelling older adults. The primaryobjective of the I.E.CARTS research programme is to evaluate and compare new detailed screeningand assessment tools together with treatment strategies, to guide primary healthcare professionals toidentify community dwelling older adults (>70 years) at high risk of adverse outcomes and to testinterventions that may decrease the risk of adverse outcomes in nine countries (Ireland, UK, Spain,Portugal, Germany, the Netherlands, Australia, Canada and Turkey).We are continuing to screen and follow older adults in the community, in the UK, Australia, Portugaland Spain. In Ireland, high risk people have been identi�ed and a comprehensive targeted geriatricassessment is being piloted in a subsample.There are two students currently doing PhD’s on the CARTS in University of Oporto, supervised byProfessor Costanca Paul.An application for a 3 year Health Research Board fellowship award has been submitted to fund amedical PhD student to develop the interventions care pathways for those identi�ed as high risk ofadverse outcomes.
Comments
Provides an example of collaborativeworkwithin the EIPAHA.Based on anewparadigmand approachto frailty screening and management. In this research “frailty” has been operationalized as “risk ofadverse events” (hospitalization, death and nursing home placement)The RISC tool has been translated into Portuguese and Spanish. Training in Porto, Ireland, Australia,Northern Ireland, and Barcelona. This included nurses, physicians, GPs, psychologists and allied healthprofessionals. A “train the trainer”model was applied where up to 50 people received the initial trainingprogramme and education tools through face-to-face workshops.This included didactic lectures on risk with practical sessions using training cases. The duration oftraining was 2 days.Focus groups and problems using the tool were identi�ed. Focus groups have been conducted withhealthcare professionals who have used the screening tool, in practice. Professionals interviewed werepublic health nurses, social workers, consultants, GPs. Five countries were involved; Ireland (n=5),UK (n=8), Portugal (n=4), Australia (n=4) and Spain (n=7). A publication on this experience hasbeen drafted and is due for submission to Age and aging (Multidisciplinary Health Care Professionals’experiences of using the Risk Instrument for Screening in the Community (RISC): A cross culturalperspective).Three papers have been published/accepted on the data collected to date:1. Rónán O’Caoimh, Yang Gao, Anton Svendrovski, Elizabeth Healy, Elizabeth O’Connell, GabrielleO’Kee�e, Eileen O’Herlihy, Una Cronin, Nicola Cornally, and William D. Molloy. "Screening formarkers of frailty and perceived risk of adverse outcomes using the Risk Instrument for Screening in

CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 26
the Community (RISC)." BMC geriatrics 14, no. 1 (2014): 104. http://www.biomedcentral.com/1471-2318/14/1042. The Community Assessment of Risk Instrument: Investigation of Inter-rater Reliability of anInstrument Measuring Risk of Adverse Outcomes. Journal of Frailty and Aging, 2014, epub ahead ofpress, see http://www.jfrailtyaging.com/current-issue.html3. Leahy-Warren P, O’Caoimh R, Fitzgerald C, Cochrane A, Svendrovski A, Cronin U, O’Herlihy E,Cornally N, FitzGerald C, Gao Y, Healy E, O’Connell E, O’Kee�e G, Coveney S, McGlynn J, ClarnetteR, Molloy DW. Components of the Risk Instrument for Screening in the Community (RISC) thatpredict Public Health Nurses’ perception of risk. Journal of Frailty and Aging 2014, in press.
Annex 1: The Action GroupPartners
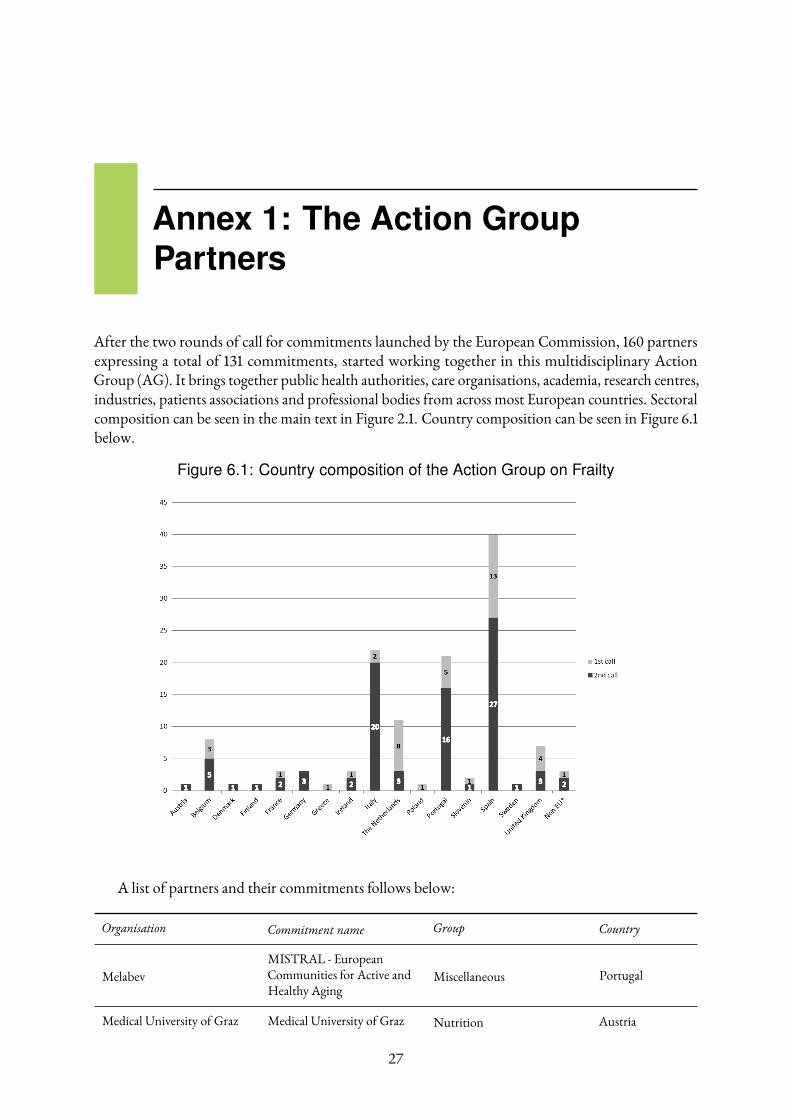
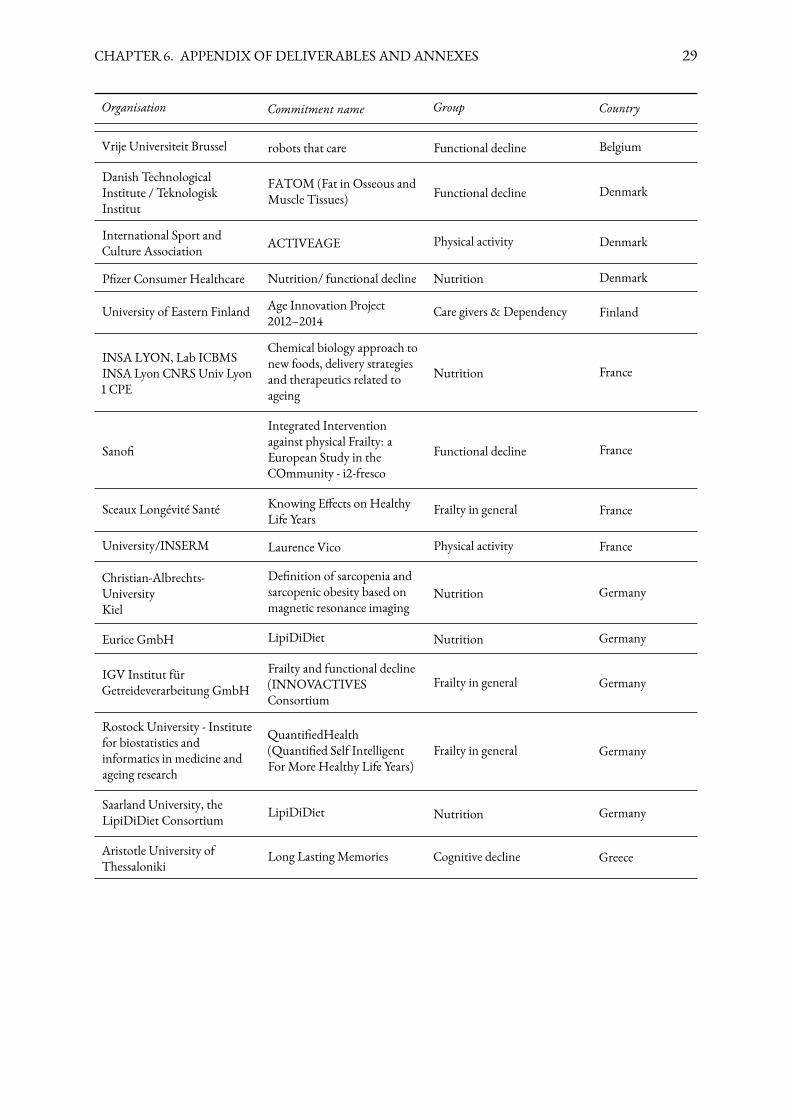
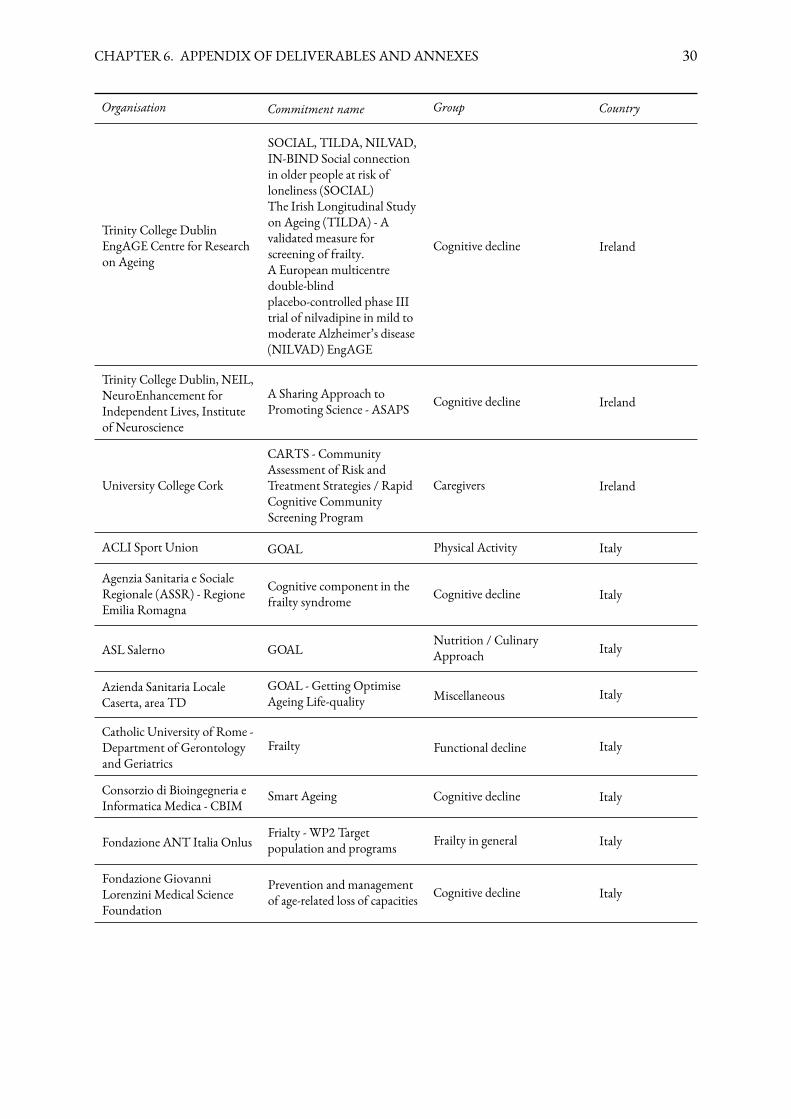
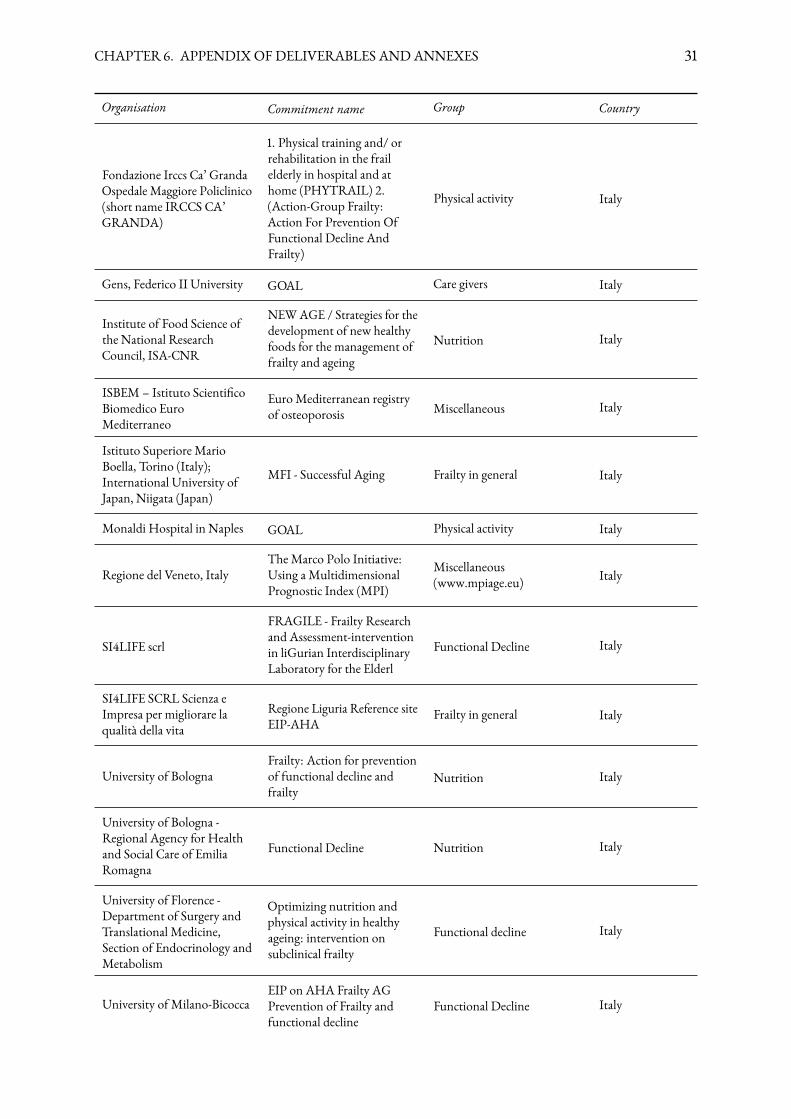
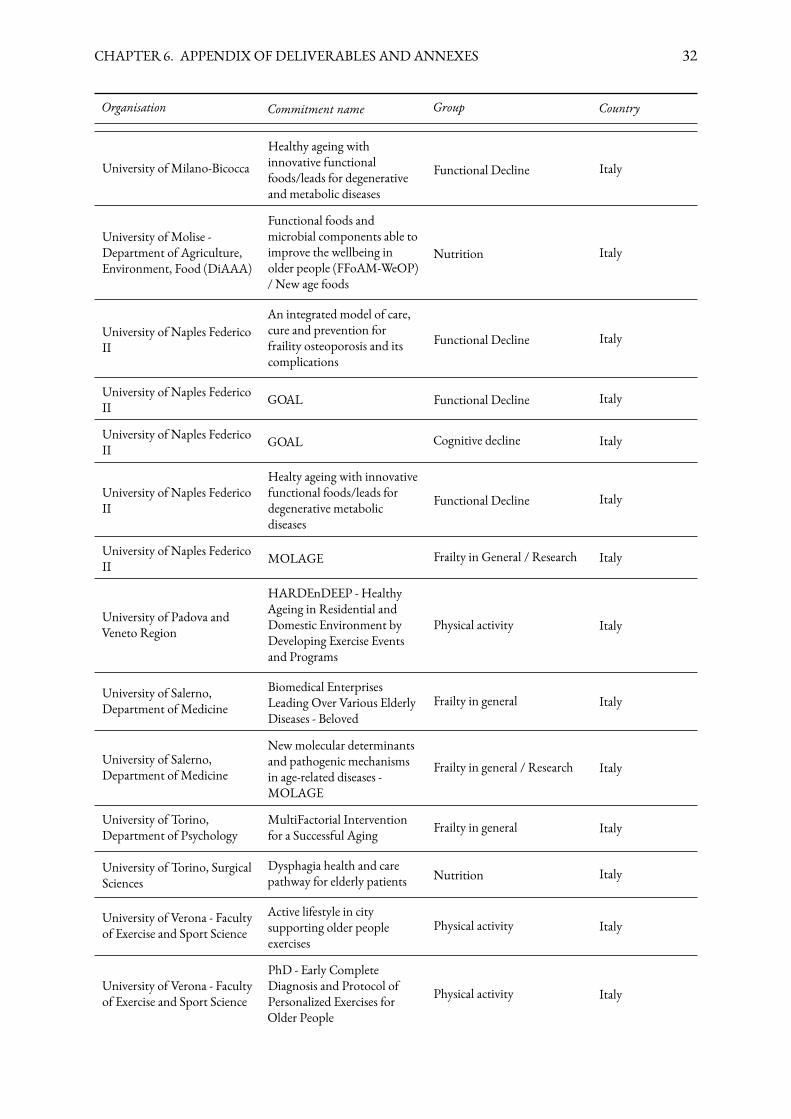
After the two rounds of call for commitments launched by the European Commission, 160 partnersexpressing a total of 131 commitments, started working together in this multidisciplinary ActionGroup (AG). It brings together public health authorities, care organisations, academia, research centres,industries, patients associations and professional bodies from across most European countries. Sectoralcomposition can be seen in the main text in Figure 2.1. Country composition can be seen in Figure 6.1below.
Figure 6.1: Country composition of the Action Group on Frailty
!
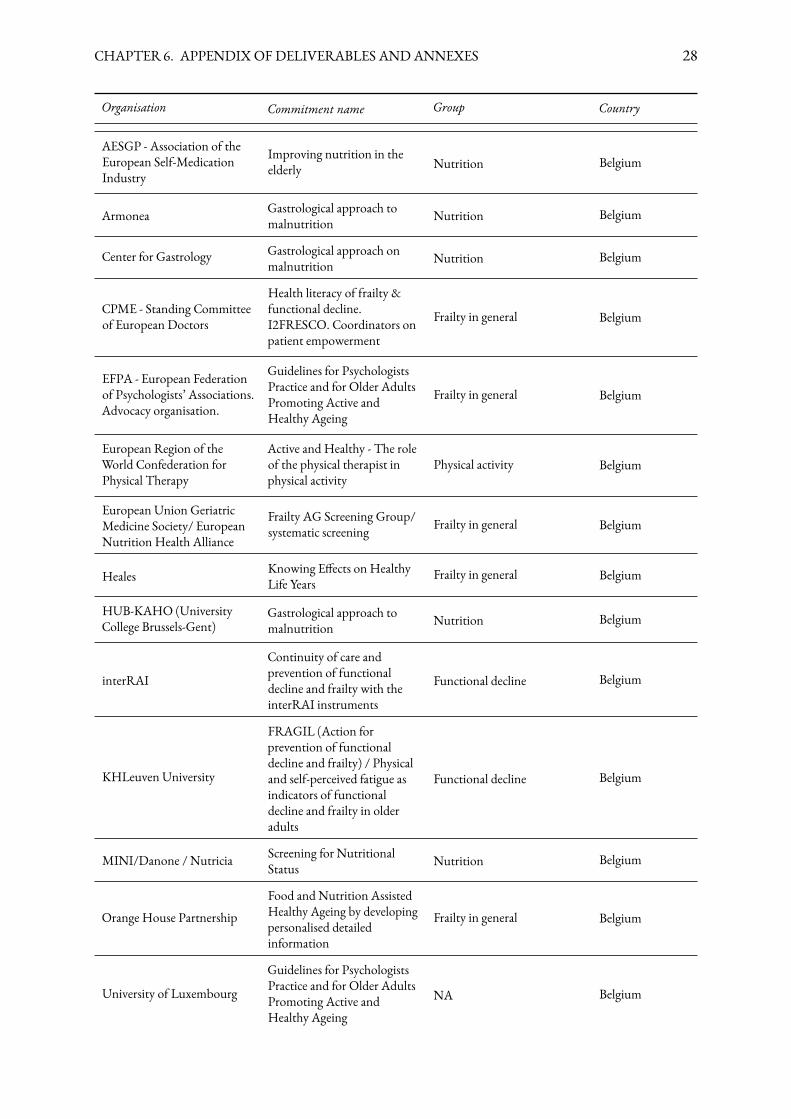
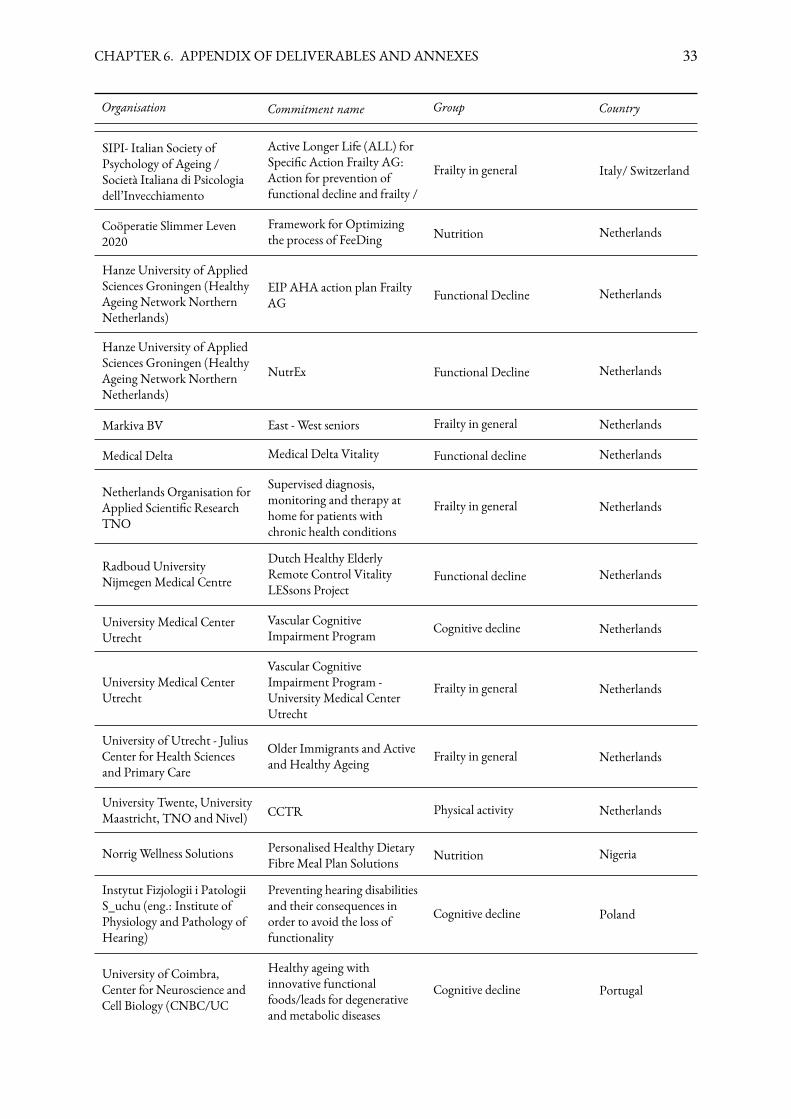
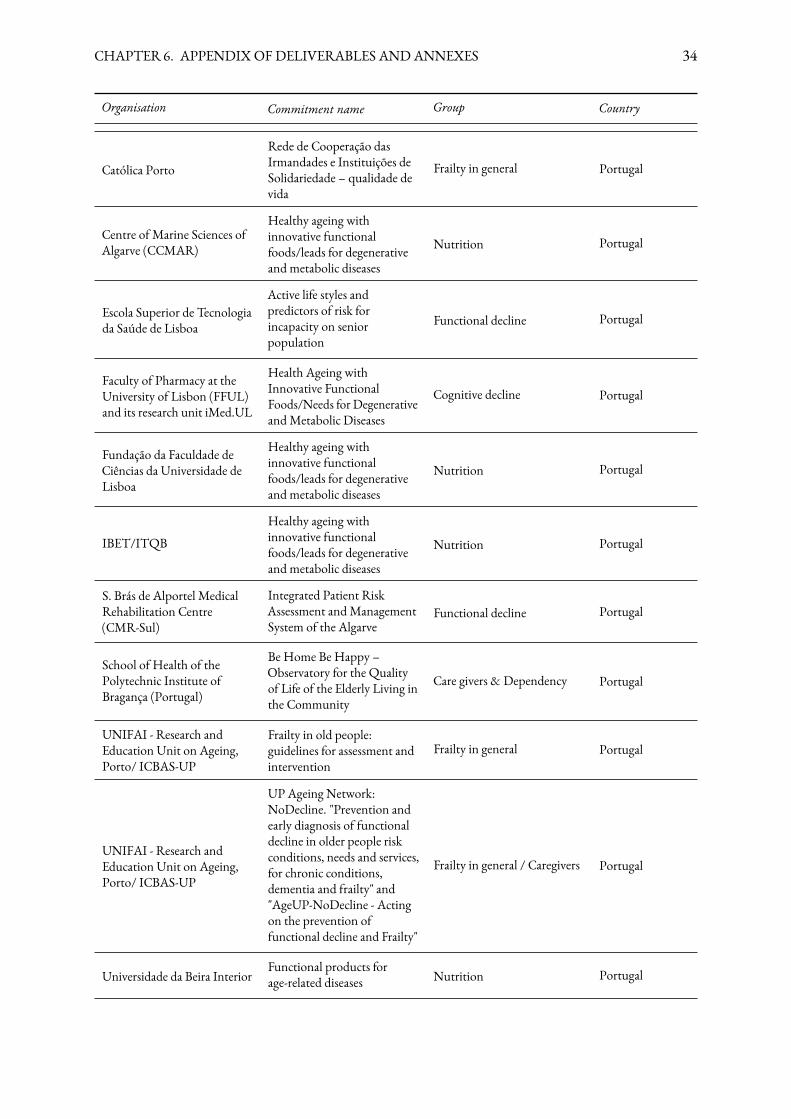
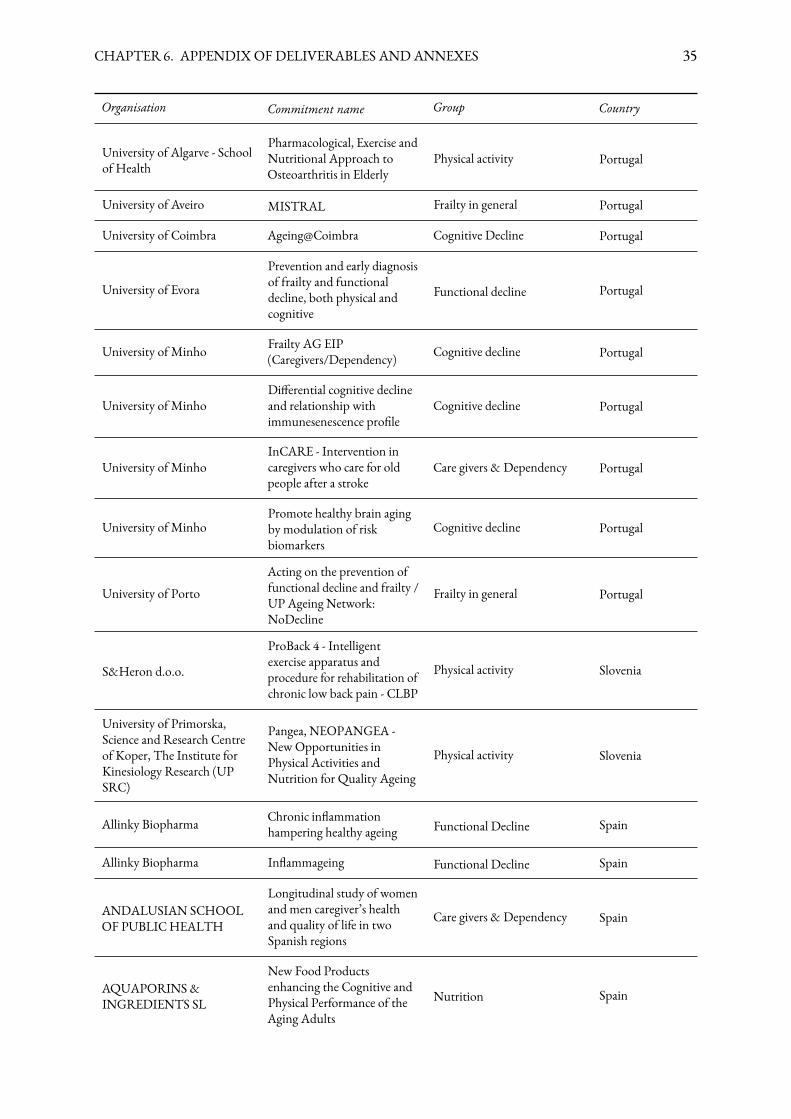
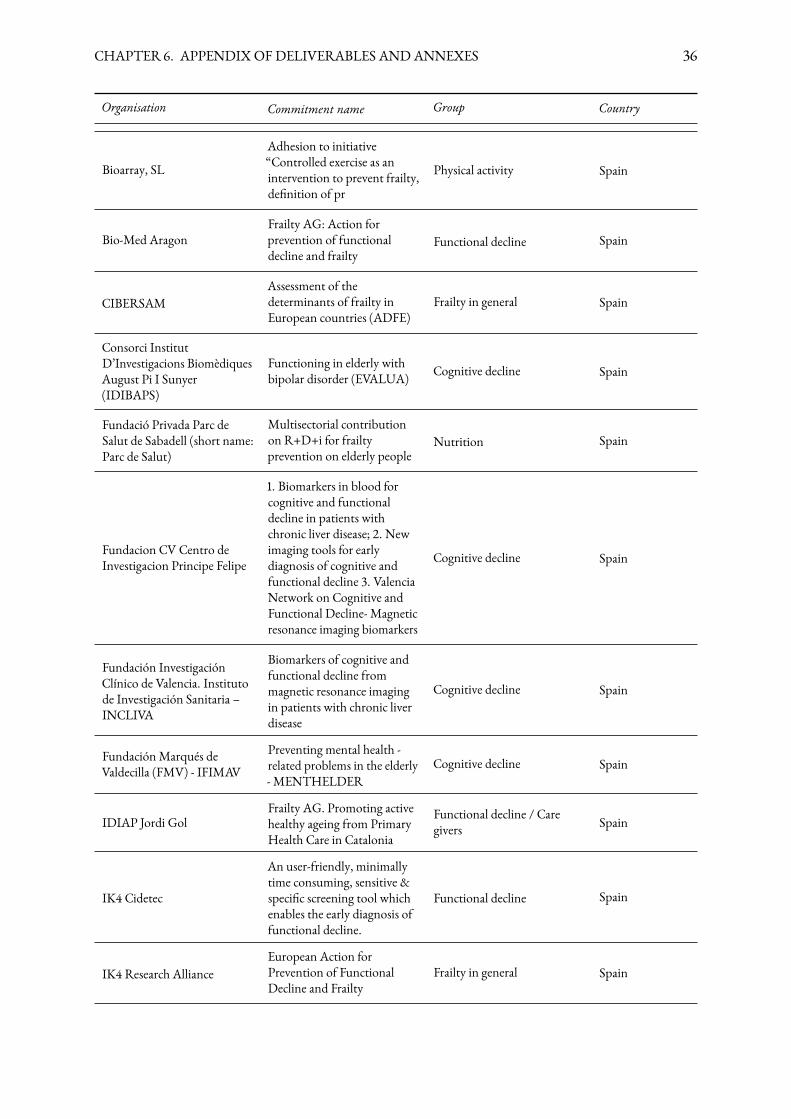
A list of partners and their commitments follows below:
Organisation Commitment name Group Country
MelabevMISTRAL - EuropeanCommunities for Active andHealthy Aging
Miscellaneous Portugal
Medical University of Graz Medical University of Graz Nutrition Austria
27
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 28
Organisation Commitment name Group Country
AESGP - Association of theEuropean Self-MedicationIndustry
Improving nutrition in theelderly Nutrition Belgium
Armonea Gastrological approach tomalnutrition Nutrition Belgium
Center for Gastrology Gastrological approach onmalnutrition Nutrition Belgium
CPME - Standing Committeeof European Doctors
Health literacy of frailty &functional decline.I2FRESCO. Coordinators onpatient empowerment
Frailty in general Belgium
EFPA - European Federationof Psychologists’ Associations.Advocacy organisation.
Guidelines for PsychologistsPractice and for Older AdultsPromoting Active andHealthy Ageing
Frailty in general Belgium
European Region of theWorld Confederation forPhysical Therapy
Active and Healthy - The roleof the physical therapist inphysical activity
Physical activity Belgium
European Union GeriatricMedicine Society/ EuropeanNutrition Health Alliance
Frailty AG Screening Group/systematic screening Frailty in general Belgium
Heales Knowing E�ects on HealthyLife Years
Frailty in general Belgium
HUB-KAHO (UniversityCollege Brussels-Gent)
Gastrological approach tomalnutrition Nutrition Belgium
interRAI
Continuity of care andprevention of functionaldecline and frailty with theinterRAI instruments
Functional decline Belgium
KHLeuven University
FRAGIL (Action forprevention of functionaldecline and frailty) / Physicaland self-perceived fatigue asindicators of functionaldecline and frailty in olderadults
Functional decline Belgium
MINI/Danone / Nutricia Screening for NutritionalStatus Nutrition Belgium
Orange House PartnershipFood and Nutrition AssistedHealthy Ageing by developingpersonalised detailedinformation
Frailty in general Belgium
University of Luxembourg
Guidelines for PsychologistsPractice and for Older AdultsPromoting Active andHealthy Ageing
NA Belgium
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 29
Organisation Commitment name Group Country
Vrije Universiteit Brussel robots that care Functional decline Belgium
Danish TechnologicalInstitute / TeknologiskInstitut
FATOM (Fat in Osseous andMuscle Tissues) Functional decline Denmark
International Sport andCulture Association ACTIVEAGE Physical activity Denmark
P�zer Consumer Healthcare Nutrition/ functional decline Nutrition Denmark
University of Eastern Finland Age Innovation Project2012–2014
Care givers & Dependency Finland
INSA LYON, Lab ICBMSINSA Lyon CNRS Univ Lyon1 CPE
Chemical biology approach tonew foods, delivery strategiesand therapeutics related toageing
Nutrition France
Sano�
Integrated Interventionagainst physical Frailty: aEuropean Study in theCOmmunity - i2-fresco
Functional decline France
Sceaux Longévité Santé Knowing E�ects on HealthyLife Years
Frailty in general France
University/INSERM Laurence Vico Physical activity France
Christian-Albrechts-UniversityKiel
De�nition of sarcopenia andsarcopenic obesity based onmagnetic resonance imaging
Nutrition Germany
Eurice GmbH LipiDiDiet Nutrition Germany
IGV Institut fürGetreideverarbeitung GmbH
Frailty and functional decline(INNOVACTIVESConsortium
Frailty in general Germany
Rostock University - Institutefor biostatistics andinformatics in medicine andageing research
Quanti�edHealth(Quanti�ed Self IntelligentFor More Healthy Life Years)
Frailty in general Germany
Saarland University, theLipiDiDiet Consortium LipiDiDiet Nutrition Germany
Aristotle University ofThessaloniki
Long Lasting Memories Cognitive decline Greece
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 30
Organisation Commitment name Group Country
Trinity College DublinEngAGE Centre for Researchon Ageing
SOCIAL, TILDA, NILVAD,IN-BIND Social connectionin older people at risk ofloneliness (SOCIAL)The Irish Longitudinal Studyon Ageing (TILDA) - Avalidated measure forscreening of frailty.A European multicentredouble-blindplacebo-controlled phase IIItrial of nilvadipine in mild tomoderate Alzheimer’s disease(NILVAD) EngAGE
Cognitive decline Ireland
Trinity College Dublin, NEIL,NeuroEnhancement forIndependent Lives, Instituteof Neuroscience
A Sharing Approach toPromoting Science - ASAPS Cognitive decline Ireland
University College Cork
CARTS - CommunityAssessment of Risk andTreatment Strategies / RapidCognitive CommunityScreening Program
Caregivers Ireland
ACLI Sport Union GOAL Physical Activity Italy
Agenzia Sanitaria e SocialeRegionale (ASSR) - RegioneEmilia Romagna
Cognitive component in thefrailty syndrome Cognitive decline Italy
ASL Salerno GOALNutrition / CulinaryApproach Italy
Azienda Sanitaria LocaleCaserta, area TD
GOAL - Getting OptimiseAgeing Life-quality Miscellaneous Italy
Catholic University of Rome -Department of Gerontologyand Geriatrics
Frailty Functional decline Italy
Consorzio di Bioingegneria eInformatica Medica - CBIM
Smart Ageing Cognitive decline Italy
Fondazione ANT Italia OnlusFrialty - WP2 Targetpopulation and programs Frailty in general Italy
Fondazione GiovanniLorenzini Medical ScienceFoundation
Prevention and managementof age-related loss of capacities Cognitive decline Italy
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 31
Organisation Commitment name Group Country
Fondazione Irccs Ca’ GrandaOspedale Maggiore Policlinico(short name IRCCS CA’GRANDA)
1. Physical training and/ orrehabilitation in the frailelderly in hospital and athome (PHYTRAIL) 2.(Action-Group Frailty:Action For Prevention OfFunctional Decline AndFrailty)
Physical activity Italy
Gens, Federico II University GOAL Care givers Italy
Institute of Food Science ofthe National ResearchCouncil, ISA-CNR
NEWAGE / Strategies for thedevelopment of new healthyfoods for the management offrailty and ageing
Nutrition Italy
ISBEM – Istituto Scienti�coBiomedico EuroMediterraneo
EuroMediterranean registryof osteoporosis Miscellaneous Italy
Istituto Superiore MarioBoella, Torino (Italy);International University ofJapan, Niigata (Japan)
MFI - Successful Aging Frailty in general Italy
Monaldi Hospital in Naples GOAL Physical activity Italy
Regione del Veneto, ItalyTheMarco Polo Initiative:Using a MultidimensionalPrognostic Index (MPI)
Miscellaneous(www.mpiage.eu) Italy
SI4LIFE scrl
FRAGILE - Frailty Researchand Assessment-interventionin liGurian InterdisciplinaryLaboratory for the Elderl
Functional Decline Italy
SI4LIFE SCRL Scienza eImpresa per migliorare laqualità della vita
Regione Liguria Reference siteEIP-AHA
Frailty in general Italy
University of BolognaFrailty: Action for preventionof functional decline andfrailty
Nutrition Italy
University of Bologna -Regional Agency for Healthand Social Care of EmiliaRomagna
Functional Decline Nutrition Italy
University of Florence -Department of Surgery andTranslational Medicine,Section of Endocrinology andMetabolism
Optimizing nutrition andphysical activity in healthyageing: intervention onsubclinical frailty
Functional decline Italy
University of Milano-BicoccaEIP on AHA Frailty AGPrevention of Frailty andfunctional decline
Functional Decline Italy
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 32
Organisation Commitment name Group Country
University of Milano-BicoccaHealthy ageing withinnovative functionalfoods/leads for degenerativeand metabolic diseases
Functional Decline Italy
University of Molise -Department of Agriculture,Environment, Food (DiAAA)
Functional foods andmicrobial components able toimprove the wellbeing inolder people (FFoAM-WeOP)/ New age foods
Nutrition Italy
University of Naples FedericoII
An integrated model of care,cure and prevention forfraility osteoporosis and itscomplications
Functional Decline Italy
University of Naples FedericoII GOAL Functional Decline Italy
University of Naples FedericoII GOAL Cognitive decline Italy
University of Naples FedericoII
Healty ageing with innovativefunctional foods/leads fordegenerative metabolicdiseases
Functional Decline Italy
University of Naples FedericoII MOLAGE Frailty in General / Research Italy
University of Padova andVeneto Region
HARDEnDEEP - HealthyAgeing in Residential andDomestic Environment byDeveloping Exercise Eventsand Programs
Physical activity Italy
University of Salerno,Department of Medicine
Biomedical EnterprisesLeading Over Various ElderlyDiseases - Beloved
Frailty in general Italy
University of Salerno,Department of Medicine
Newmolecular determinantsand pathogenic mechanismsin age-related diseases -MOLAGE
Frailty in general / Research Italy
University of Torino,Department of Psychology
MultiFactorial Interventionfor a Successful Aging Frailty in general Italy
University of Torino, SurgicalSciences
Dysphagia health and carepathway for elderly patients Nutrition Italy
University of Verona - Facultyof Exercise and Sport Science
Active lifestyle in citysupporting older peopleexercises
Physical activity Italy
University of Verona - Facultyof Exercise and Sport Science
PhD - Early CompleteDiagnosis and Protocol ofPersonalized Exercises forOlder People
Physical activity Italy
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 33
Organisation Commitment name Group Country
SIPI- Italian Society ofPsychology of Ageing /Società Italiana di Psicologiadell’Invecchiamento
Active Longer Life (ALL) forSpeci�c Action Frailty AG:Action for prevention offunctional decline and frailty /
Frailty in general Italy/ Switzerland
Coöperatie Slimmer Leven2020
Framework for Optimizingthe process of FeeDing Nutrition Netherlands
Hanze University of AppliedSciences Groningen (HealthyAgeing Network NorthernNetherlands)
EIP AHA action plan FrailtyAG Functional Decline Netherlands
Hanze University of AppliedSciences Groningen (HealthyAgeing Network NorthernNetherlands)
NutrEx Functional Decline Netherlands
Markiva BV East - West seniors Frailty in general Netherlands
Medical Delta Medical Delta Vitality Functional decline Netherlands
Netherlands Organisation forApplied Scienti�c ResearchTNO
Supervised diagnosis,monitoring and therapy athome for patients withchronic health conditions
Frailty in general Netherlands
Radboud UniversityNijmegenMedical Centre
Dutch Healthy ElderlyRemote Control VitalityLESsons Project
Functional decline Netherlands
University Medical CenterUtrecht
Vascular CognitiveImpairment Program Cognitive decline Netherlands
University Medical CenterUtrecht
Vascular CognitiveImpairment Program -University Medical CenterUtrecht
Frailty in general Netherlands
University of Utrecht - JuliusCenter for Health Sciencesand Primary Care
Older Immigrants and Activeand Healthy Ageing Frailty in general Netherlands
University Twente, UniversityMaastricht, TNO and Nivel) CCTR Physical activity Netherlands
Norrig Wellness Solutions Personalised Healthy DietaryFibre Meal Plan Solutions Nutrition Nigeria
Instytut Fizjologii i PatologiiS_uchu (eng.: Institute ofPhysiology and Pathology ofHearing)
Preventing hearing disabilitiesand their consequences inorder to avoid the loss offunctionality
Cognitive decline Poland
University of Coimbra,Center for Neuroscience andCell Biology (CNBC/UC
Healthy ageing withinnovative functionalfoods/leads for degenerativeand metabolic diseases
Cognitive decline Portugal
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 34
Organisation Commitment name Group Country
Católica Porto
Rede de Cooperação dasIrmandades e Instituições deSolidariedade – qualidade devida
Frailty in general Portugal
Centre of Marine Sciences ofAlgarve (CCMAR)
Healthy ageing withinnovative functionalfoods/leads for degenerativeand metabolic diseases
Nutrition Portugal
Escola Superior de Tecnologiada Saúde de Lisboa
Active life styles andpredictors of risk forincapacity on seniorpopulation
Functional decline Portugal
Faculty of Pharmacy at theUniversity of Lisbon (FFUL)and its research unit iMed.UL
Health Ageing withInnovative FunctionalFoods/Needs for DegenerativeandMetabolic Diseases
Cognitive decline Portugal
Fundação da Faculdade deCiências da Universidade deLisboa
Healthy ageing withinnovative functionalfoods/leads for degenerativeand metabolic diseases
Nutrition Portugal
IBET/ITQBHealthy ageing withinnovative functionalfoods/leads for degenerativeand metabolic diseases
Nutrition Portugal
S. Brás de Alportel MedicalRehabilitation Centre(CMR-Sul)
Integrated Patient RiskAssessment andManagementSystem of the Algarve
Functional decline Portugal
School of Health of thePolytechnic Institute ofBragança (Portugal)
Be Home Be Happy –Observatory for the Qualityof Life of the Elderly Living inthe Community
Care givers & Dependency Portugal
UNIFAI - Research andEducation Unit on Ageing,Porto/ ICBAS-UP
Frailty in old people:guidelines for assessment andintervention
Frailty in general Portugal
UNIFAI - Research andEducation Unit on Ageing,Porto/ ICBAS-UP
UP Ageing Network:NoDecline. "Prevention andearly diagnosis of functionaldecline in older people riskconditions, needs and services,for chronic conditions,dementia and frailty" and"AgeUP-NoDecline - Actingon the prevention offunctional decline and Frailty"
Frailty in general / Caregivers Portugal
Universidade da Beira InteriorFunctional products forage-related diseases Nutrition Portugal
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 35
Organisation Commitment name Group Country
University of Algarve - Schoolof Health
Pharmacological, Exercise andNutritional Approach toOsteoarthritis in Elderly
Physical activity Portugal
University of Aveiro MISTRAL Frailty in general Portugal
University of Coimbra Ageing@Coimbra Cognitive Decline Portugal
University of Evora
Prevention and early diagnosisof frailty and functionaldecline, both physical andcognitive
Functional decline Portugal
University of Minho Frailty AG EIP(Caregivers/Dependency) Cognitive decline Portugal
University of MinhoDi�erential cognitive declineand relationship withimmunesenescence pro�le
Cognitive decline Portugal
University of MinhoInCARE - Intervention incaregivers who care for oldpeople after a stroke
Care givers & Dependency Portugal
University of MinhoPromote healthy brain agingby modulation of riskbiomarkers
Cognitive decline Portugal
University of PortoActing on the prevention offunctional decline and frailty /UP Ageing Network:NoDecline
Frailty in general Portugal
S&Heron d.o.o.
ProBack 4 - Intelligentexercise apparatus andprocedure for rehabilitation ofchronic low back pain - CLBP
Physical activity Slovenia
University of Primorska,Science and Research Centreof Koper, The Institute forKinesiology Research (UPSRC)
Pangea, NEOPANGEA -NewOpportunities inPhysical Activities andNutrition for Quality Ageing
Physical activity Slovenia
Allinky Biopharma Chronic in�ammationhampering healthy ageing Functional Decline Spain
Allinky Biopharma In�ammageing Functional Decline Spain
ANDALUSIAN SCHOOLOF PUBLICHEALTH
Longitudinal study of womenand men caregiver’s healthand quality of life in twoSpanish regions
Care givers & Dependency Spain
AQUAPORINS&INGREDIENTS SL
New Food Productsenhancing the Cognitive andPhysical Performance of theAging Adults
Nutrition Spain
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 36
Organisation Commitment name Group Country
Bioarray, SL
Adhesion to initiative“Controlled exercise as anintervention to prevent frailty,de�nition of pr
Physical activity Spain
Bio-Med AragonFrailty AG: Action forprevention of functionaldecline and frailty
Functional decline Spain
CIBERSAMAssessment of thedeterminants of frailty inEuropean countries (ADFE)
Frailty in general Spain
Consorci InstitutD’Investigacions BiomèdiquesAugust Pi I Sunyer(IDIBAPS)
Functioning in elderly withbipolar disorder (EVALUA) Cognitive decline Spain
Fundació Privada Parc deSalut de Sabadell (short name:Parc de Salut)
Multisectorial contributionon R+D+i for frailtyprevention on elderly people
Nutrition Spain
Fundacion CV Centro deInvestigacion Principe Felipe
1. Biomarkers in blood forcognitive and functionaldecline in patients withchronic liver disease; 2. Newimaging tools for earlydiagnosis of cognitive andfunctional decline 3. ValenciaNetwork on Cognitive andFunctional Decline- Magneticresonance imaging biomarkers
Cognitive decline Spain
Fundación InvestigaciónClínico de Valencia. Institutode Investigación Sanitaria –INCLIVA
Biomarkers of cognitive andfunctional decline frommagnetic resonance imagingin patients with chronic liverdisease
Cognitive decline Spain
FundaciónMarqués deValdecilla (FMV) - IFIMAV
Preventing mental health -related problems in the elderly- MENTHELDER
Cognitive decline Spain
IDIAP Jordi GolFrailty AG. Promoting activehealthy ageing from PrimaryHealth Care in Catalonia
Functional decline / Caregivers Spain
IK4 Cidetec
An user-friendly, minimallytime consuming, sensitive &speci�c screening tool whichenables the early diagnosis offunctional decline.
Functional decline Spain
IK4 Research AllianceEuropean Action forPrevention of FunctionalDecline and Frailty
Frailty in general Spain
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 37
Organisation Commitment name Group Country
Institute of Biomechanics ofValencia
Frailty prevention and delaythrough functionalassessment of daily activities
Physical activity Spain
Instituto de Bioingenieria,UniversidadMiguelHernandez
Adherence to older peoplesports Physical acitivity Spain
Instituto deNeurociencias-UniversidadMiguel Hernandez de Elche
Alzheimer monitoring forearly diagnosis (Missing) Spain
KRONIKGUNE on behalf ofthe Department of Health ofthe Basque Government
Prediction of frailty andanalysis of epidemiologicburden of neurodegenerativedisorders
Physical activity Spain
Pablo de Olavide University,Sevilla-Spain
Online program to evaluateand train the executivefunction
Cognitive decline Spain
Parc Sanitari Sant Joan deDéu-Fundació Sant Joan deDéu
Assessment of thedeterminants of frailty ineuropean countries
Frailty in general Spain
Pasqual Maragall Maragall
Cognitive Characterization forAssessment of Risk ofFunctional Decline/PasqualMaragall Foundation
Cognitive decline Spain
PUBLICHEALTHAGENCYOF CATALONIA
Active Health Ageing througha healthy diet and physicalactivity in Catalonia
Physical activity Spain
Sermas Hospital Universitariode Getafe/GlobalManagement of Frailty inClinical Settings
Global management of frailtyin clinical settings -FRAILCLINIC
Frailty in general Spain
Spanish Collaborating Centreof the Joanna Briggs Institutein collaboration with Nursingand Health
Healthcare programme,activities and therapeuticinterventions to preventfrailty
Frailty in general Spain
Spanish Network of HealthyCities (RECS)-SpanishFederation of Mucipipalitiesand Provinces (FEMP)
Assessment of nutritionalstatus, physical, a�ective,cognitive and socialfunctioning in elderly
Miscellaneous Spain
TECNALIA Research &Innovation
HeAlthy nutrition and ICTfor actiVE ageiNg andprevention of frailty anddementia
Nutrition Spain
THEOLD PEOPLEHEALTHOBSERVATORY.Ayuntamiento de Villanuevade la Cañada
Coordinated Use ofMunicipal health resources byPrimary care team. The «CUMPcare programme »
Miscellaneous Spain
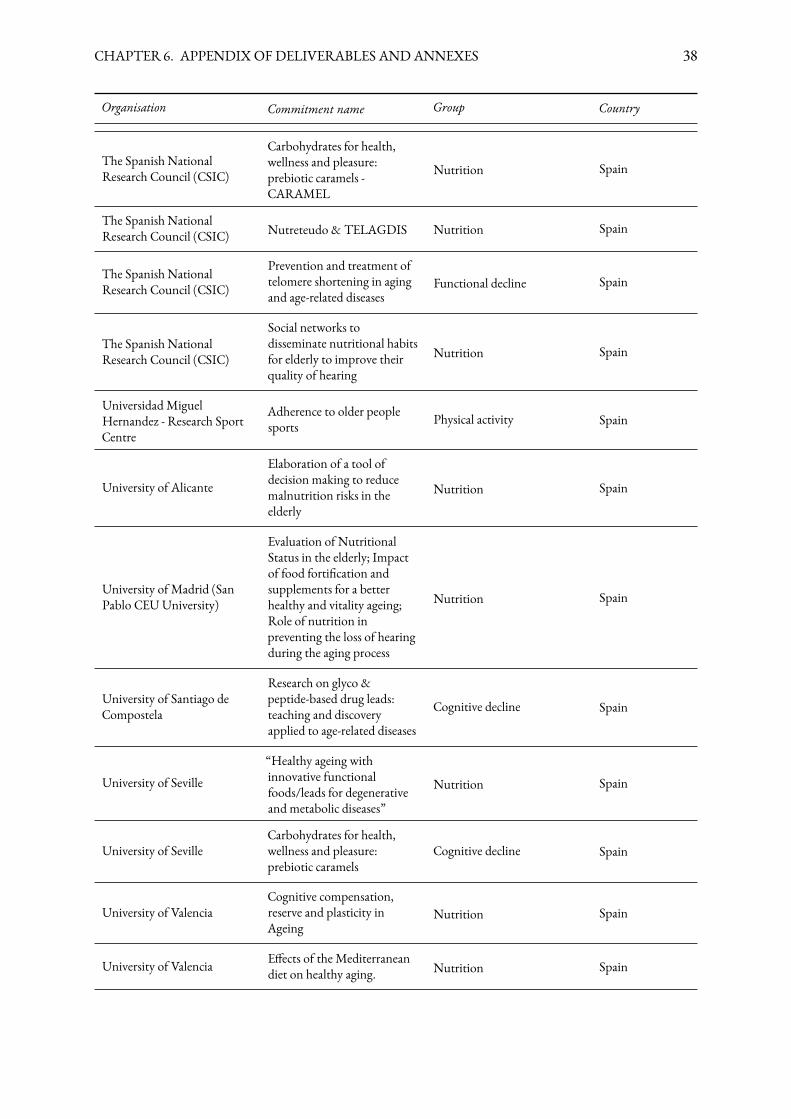
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 38
Organisation Commitment name Group Country
The Spanish NationalResearch Council (CSIC)
Carbohydrates for health,wellness and pleasure:prebiotic caramels -CARAMEL
Nutrition Spain
The Spanish NationalResearch Council (CSIC) Nutreteudo & TELAGDIS Nutrition Spain
The Spanish NationalResearch Council (CSIC)
Prevention and treatment oftelomere shortening in agingand age-related diseases
Functional decline Spain
The Spanish NationalResearch Council (CSIC)
Social networks todisseminate nutritional habitsfor elderly to improve theirquality of hearing
Nutrition Spain
UniversidadMiguelHernandez - Research SportCentre
Adherence to older peoplesports Physical activity Spain
University of Alicante
Elaboration of a tool ofdecision making to reducemalnutrition risks in theelderly
Nutrition Spain
University of Madrid (SanPablo CEUUniversity)
Evaluation of NutritionalStatus in the elderly; Impactof food forti�cation andsupplements for a betterhealthy and vitality ageing;Role of nutrition inpreventing the loss of hearingduring the aging process
Nutrition Spain
University of Santiago deCompostela
Research on glyco &peptide-based drug leads:teaching and discoveryapplied to age-related diseases
Cognitive decline Spain
University of Seville“Healthy ageing withinnovative functionalfoods/leads for degenerativeand metabolic diseases”
Nutrition Spain
University of SevilleCarbohydrates for health,wellness and pleasure:prebiotic caramels
Cognitive decline Spain
University of ValenciaCognitive compensation,reserve and plasticity inAgeing
Nutrition Spain
University of Valencia E�ects of the Mediterraneandiet on healthy aging. Nutrition Spain
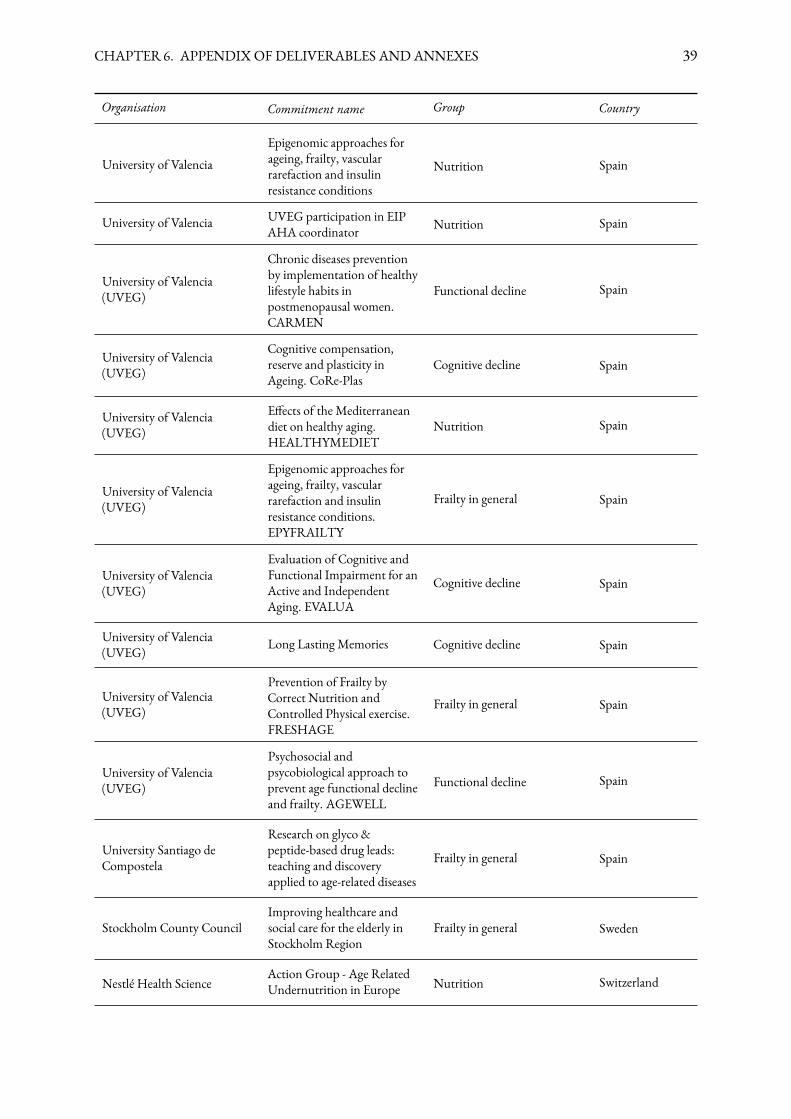
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 39
Organisation Commitment name Group Country
University of ValenciaEpigenomic approaches forageing, frailty, vascularrarefaction and insulinresistance conditions
Nutrition Spain
University of Valencia UVEG participation in EIPAHA coordinator Nutrition Spain
University of Valencia(UVEG)
Chronic diseases preventionby implementation of healthylifestyle habits inpostmenopausal women.CARMEN
Functional decline Spain
University of Valencia(UVEG)
Cognitive compensation,reserve and plasticity inAgeing. CoRe-Plas
Cognitive decline Spain
University of Valencia(UVEG)
E�ects of the Mediterraneandiet on healthy aging.HEALTHYMEDIET
Nutrition Spain
University of Valencia(UVEG)
Epigenomic approaches forageing, frailty, vascularrarefaction and insulinresistance conditions.EPYFRAILTY
Frailty in general Spain
University of Valencia(UVEG)
Evaluation of Cognitive andFunctional Impairment for anActive and IndependentAging. EVALUA
Cognitive decline Spain
University of Valencia(UVEG) Long Lasting Memories Cognitive decline Spain
University of Valencia(UVEG)
Prevention of Frailty byCorrect Nutrition andControlled Physical exercise.FRESHAGE
Frailty in general Spain
University of Valencia(UVEG)
Psychosocial andpsycobiological approach toprevent age functional declineand frailty. AGEWELL
Functional decline Spain
University Santiago deCompostela
Research on glyco &peptide-based drug leads:teaching and discoveryapplied to age-related diseases
Frailty in general Spain
Stockholm County CouncilImproving healthcare andsocial care for the elderly inStockholm Region
Frailty in general Sweden
Nestlé Health ScienceAction Group - Age RelatedUndernutrition in Europe Nutrition Switzerland
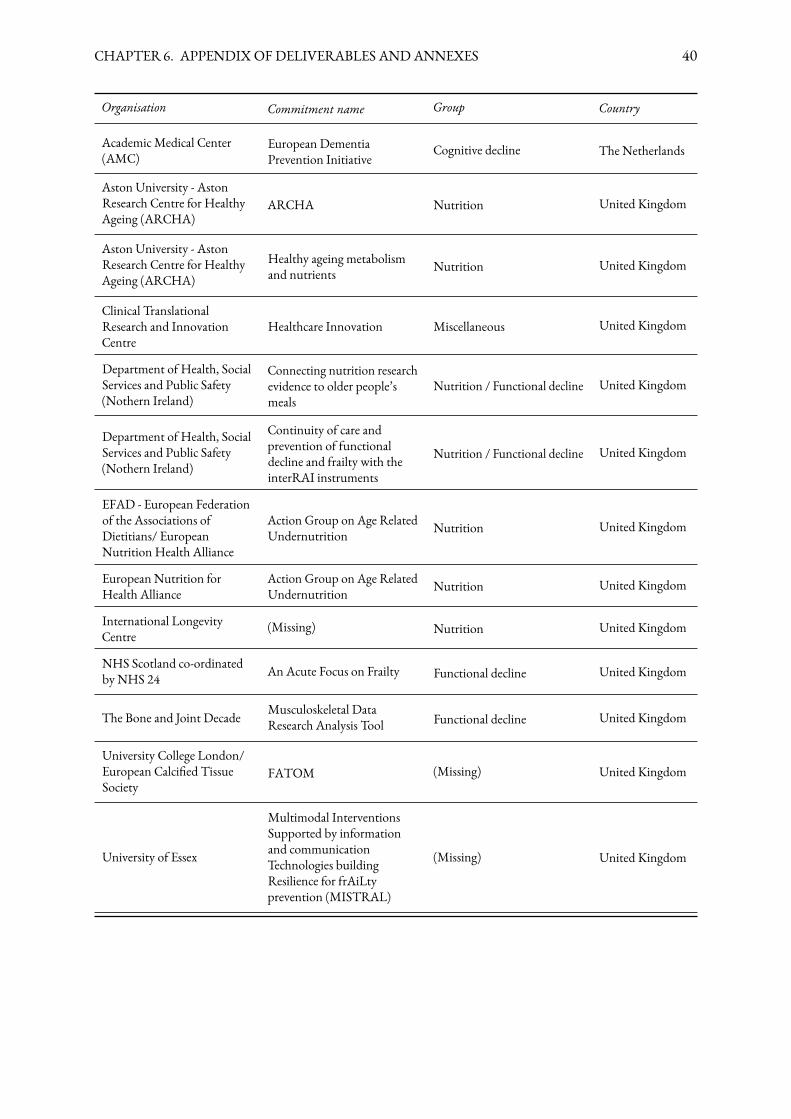
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 40
Organisation Commitment name Group Country
Academic Medical Center(AMC)
European DementiaPrevention Initiative
Cognitive decline The Netherlands
Aston University - AstonResearch Centre for HealthyAgeing (ARCHA)
ARCHA Nutrition United Kingdom
Aston University - AstonResearch Centre for HealthyAgeing (ARCHA)
Healthy ageing metabolismand nutrients Nutrition United Kingdom
Clinical TranslationalResearch and InnovationCentre
Healthcare Innovation Miscellaneous United Kingdom
Department of Health, SocialServices and Public Safety(Nothern Ireland)
Connecting nutrition researchevidence to older people’smeals
Nutrition / Functional decline United Kingdom
Department of Health, SocialServices and Public Safety(Nothern Ireland)
Continuity of care andprevention of functionaldecline and frailty with theinterRAI instruments
Nutrition / Functional decline United Kingdom
EFAD - European Federationof the Associations ofDietitians/ EuropeanNutrition Health Alliance
Action Group on Age RelatedUndernutrition Nutrition United Kingdom
European Nutrition forHealth Alliance
Action Group on Age RelatedUndernutrition Nutrition United Kingdom
International LongevityCentre
(Missing) Nutrition United Kingdom
NHS Scotland co-ordinatedby NHS 24 An Acute Focus on Frailty Functional decline United Kingdom
The Bone and Joint Decade Musculoskeletal DataResearch Analysis Tool Functional decline United Kingdom
University College London/European Calci�ed TissueSociety
FATOM (Missing) United Kingdom
University of Essex
Multimodal InterventionsSupported by informationand communicationTechnologies buildingResilience for frAiLtyprevention (MISTRAL)
(Missing) United Kingdom
Annex 2: Individual CommitmentDeliverables 2014
Promotion of healthy lifestyles.
1. TheUniversity of Valencia produced a validated protocol to prevent osteoporosis in post-menopausalwomen. It includes a risk strati�cation tool and a follow up programme based on physical exercise withan elastic thera-band.
2. Another running protocol, issued by the Institute of Biomechanics of Valencia, aims to delayfrailty status through the improvement of balance in older people. As in the previous example, theexercised proposed can be performed in private houses as well as in nursing home.
3. Another department of the University of Valencia has published a study result on the capacity toevaluate and analyse retirement predictors a second one on the motivation to keep older people activeat work have been carried out and their �ndings published in a scienti�c journal.
4& 5. Two di�erent training activities have been organisedwith the aim to improve healthy lifestyle.The �rst one, from the U.S.ACLI Italy, concerns the promotion of physical activities among olderpeople; in the �rst six months of 2014 alone, 47 "Walking for Health" events were organised. Thesecond training, organised by the Centre for Gastrology, targeted chefs committed to maintain andimprove well-being and health of old people providing themwith safer and healthier foods. Knowledgegathering and dissemination
Almost 40% of the individual deliverables targeted knowledge gathering and dissemination, al-though they took a variety of approaches.
1. The need of integrate current healthcare professional educations with new topics and subjectshas been highlighted by many A3 partners. In response to this concern, the Faculty of Pharmacy ofthe University of Lisbon organised four new courses of Biopharmaceutical Sciences structured withinmaster and doctoral programs. Twenty students enrolled in the following courses: Development andOrganization of the Nervous System, Brain Barriers in Drug Development, Neuropathology andNeuropharmacology and Pathophysiology of Neuroin�ammation.
2. A data platform to collect risk biomarkers has been set up by the University of Minho alongwith the Life and Health Science Research Institute. The data are elaborated to allow a strati�cation ofthe risk of cognitive decline to promote early detection of the high risk patients. Thanks to this speci�cinformation, tailored and more e�cient prevention approached are identi�ed.
3. The International Sport and Culture Association published a guide on capacity building ofstrategies and programs in sport organisations speci�c for older people (Active Age Handbook).
4. An ad hoc questionnaire to test the relation between engagement into cultural and social activitiesand well-being has been developed and administered by the Federico II University together with theNGOGENS. Preliminary analysis indicates that there is a direct and signi�cant correlation betweenwell-being and cultural and social engagement in over 60 years old subjects.
41
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 42
5. The Agencia Estatal Consejo Superior de Investigaciones Cientí�cas opened a Twitter accountto increased awareness on the importance of hearing impairment for active ageing, and on the impactof nutrition on hearing loss has been created. The ultimate goal of the project is to improve diet habitsin order to prevent/delay the onset of age-related hearing loss, while having an impact on the risk offalling.
Scientific publications
Two partners published in scienti�c international journals their research results. The Aston Universityon the prevention of progression from pre-frailty to frailty status in older people through the study ofthe nutrient status with particular focus on fatty acids and antioxidant nutrients. The Veneto regionpublished the results of aMultidimensional Prognostic Index -MPI testing phase carried out in geriatricwards. In an e�ort to boost the added value of telemedicine for physical rehabilitation the RoessinghResearch and Development produced a scienti�c dissertation now publicly available.
Better prevention tools
1. The Research and Education Unit on Ageing of UNIFAI conducted a literature review for thepurpose of adapting existing instruments to measure frailty and estimating the prevalence of frailty inthe population in Portugal. As a result using the phenotypes of frailty (Fried et al, 2001) as a goldenpattern the following two instruments have been adapted:
i. Groningen Frailty Indicator (GFI) (Schuurmans, H., Steverink, N., Lindenberg, S., Frieswijk, N.,& Slates, J., 2004).
ii. Tilburg Frailty Indicator (TFI) (Gobbens, van Assen, Luijkx, Wijnen-Sponselee, & Schols,2010).
2. Hanze University of Applied Science Groningen develop an app as a means to conduct a quickand easy assessment of malnutrition and frailty (risk). The tool aims to enhance patient empowerment,promotion of independent living, early detection of (pre-) frailty or malnutrition (risk) and promptingtimely interventions.
3. VenetoRegion employed a prognostic index (MPI) as aMultidimensional assessment instrumentto discharging frail patients from Geriatric wards to predict survival, health-related outcomes and toforecast health resource use and costs. The results drive the choice of health interventions for frailindividuals that present the best cost-e�ectiveness pro�le.
New functional foods
Finally, Aquaporins & Ingredients SL developed a new functional food rich in bioactive compoundswith plant and algae ingredients. The food is currently under production at lab scale.
List of 2014 Individual deliverables
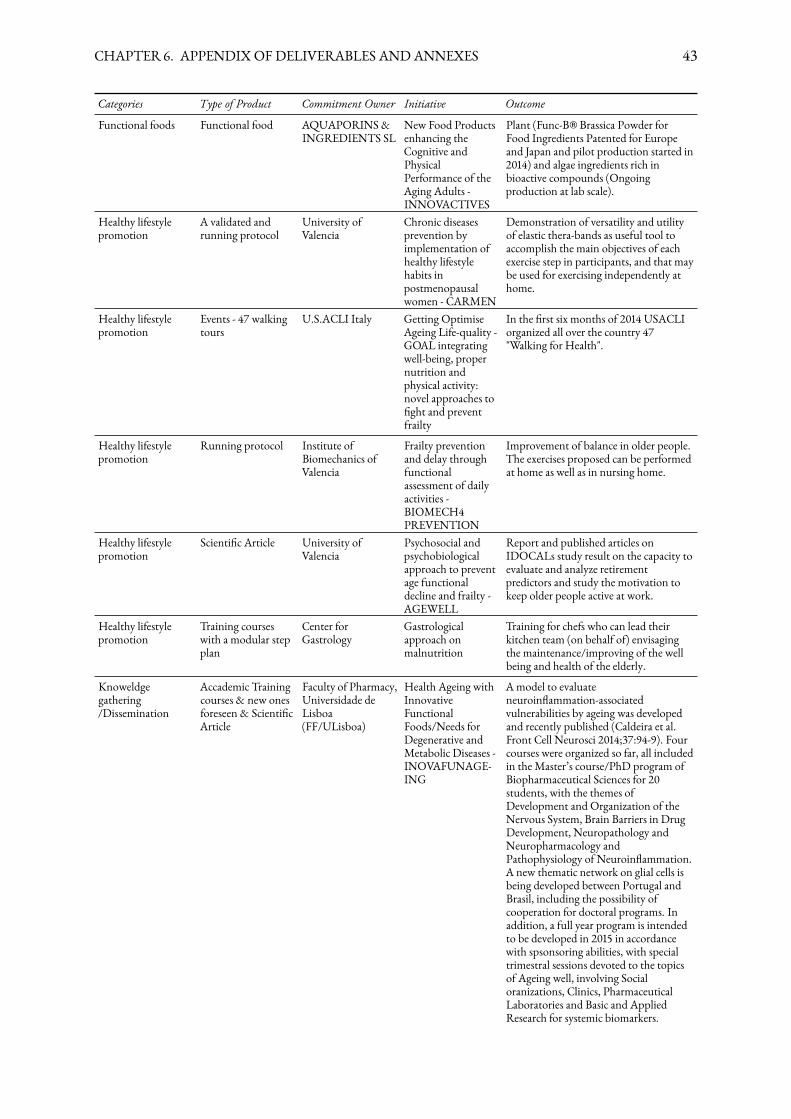
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 43
Categories Type of Product Commitment Owner Initiative Outcome
Functional foods Functional food AQUAPORINS&INGREDIENTS SL
New Food Productsenhancing theCognitive andPhysicalPerformance of theAging Adults -INNOVACTIVES
Plant (Func-B® Brassica Powder forFood Ingredients Patented for Europeand Japan and pilot production started in2014) and algae ingredients rich inbioactive compounds (Ongoingproduction at lab scale).
Healthy lifestylepromotion
A validated andrunning protocol
University ofValencia
Chronic diseasesprevention byimplementation ofhealthy lifestylehabits inpostmenopausalwomen - CARMEN
Demonstration of versatility and utilityof elastic thera-bands as useful tool toaccomplish the main objectives of eachexercise step in participants, and that maybe used for exercising independently athome.
Healthy lifestylepromotion
Events - 47 walkingtours
U.S.ACLI Italy Getting OptimiseAgeing Life-quality -GOAL integratingwell-being, propernutrition andphysical activity:novel approaches to�ght and preventfrailty
In the �rst six months of 2014 USACLIorganized all over the country 47"Walking for Health".
Healthy lifestylepromotion
Running protocol Institute ofBiomechanics ofValencia
Frailty preventionand delay throughfunctionalassessment of dailyactivities -BIOMECH4PREVENTION
Improvement of balance in older people.The exercises proposed can be performedat home as well as in nursing home.
Healthy lifestylepromotion
Scienti�c Article University ofValencia
Psychosocial andpsychobiologicalapproach to preventage functionaldecline and frailty -AGEWELL
Report and published articles onIDOCALs study result on the capacity toevaluate and analyze retirementpredictors and study the motivation tokeep older people active at work.
Healthy lifestylepromotion
Training courseswith a modular stepplan
Center forGastrology
Gastrologicalapproach onmalnutrition
Training for chefs who can lead theirkitchen team (on behalf of) envisagingthe maintenance/improving of the wellbeing and health of the elderly.
Knoweldgegathering/Dissemination
Accademic Trainingcourses & new onesforeseen & Scienti�cArticle
Faculty of Pharmacy,Universidade deLisboa(FF/ULisboa)
Health Ageing withInnovativeFunctionalFoods/Needs forDegenerative andMetabolic Diseases -INOVAFUNAGE-ING
Amodel to evaluateneuroin�ammation-associatedvulnerabilities by ageing was developedand recently published (Caldeira et al.Front Cell Neurosci 2014;37:94-9). Fourcourses were organized so far, all includedin the Master’s course/PhD program ofBiopharmaceutical Sciences for 20students, with the themes ofDevelopment and Organization of theNervous System, Brain Barriers in DrugDevelopment, Neuropathology andNeuropharmacology andPathophysiology of Neuroin�ammation.A new thematic network on glial cells isbeing developed between Portugal andBrasil, including the possibility ofcooperation for doctoral programs. Inaddition, a full year program is intendedto be developed in 2015 in accordancewith spsonsoring abilities, with specialtrimestral sessions devoted to the topicsof Ageing well, involving Socialoranizations, Clinics, PharmaceuticalLaboratories and Basic and AppliedResearch for systemic biomarkers.
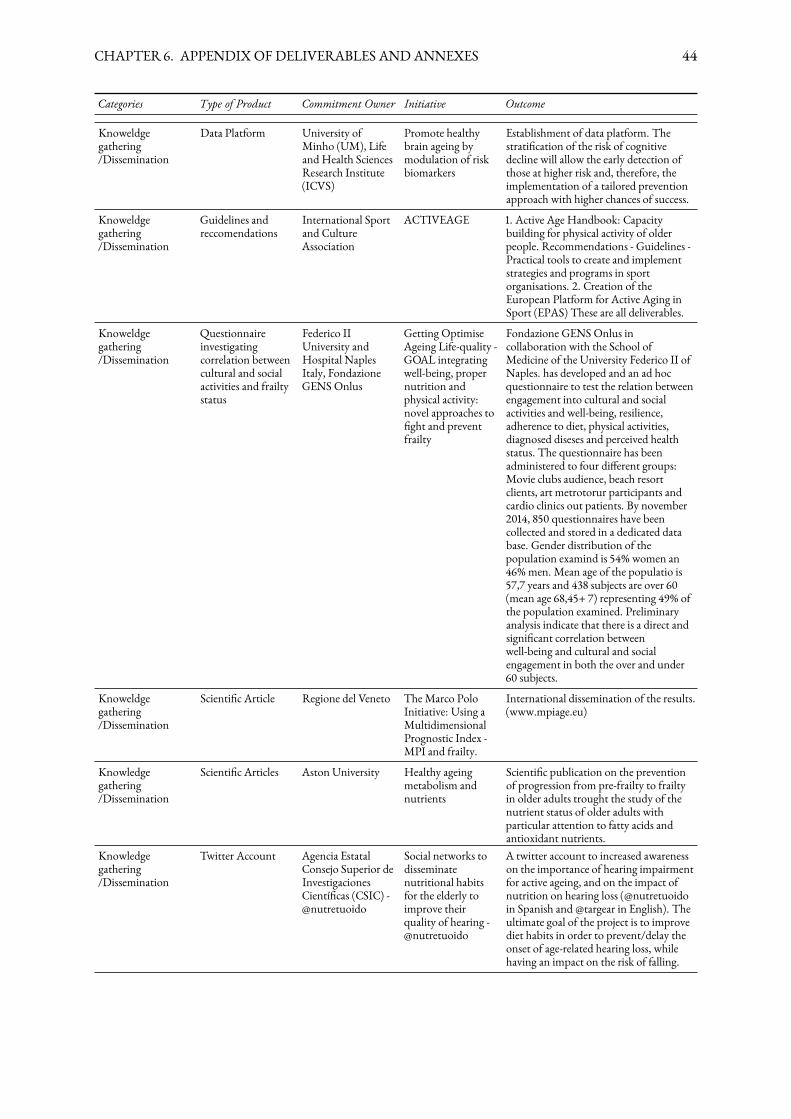
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 44
Categories Type of Product Commitment Owner Initiative Outcome
Knoweldgegathering/Dissemination
Data Platform University ofMinho (UM), Lifeand Health SciencesResearch Institute(ICVS)
Promote healthybrain ageing bymodulation of riskbiomarkers
Establishment of data platform. Thestrati�cation of the risk of cognitivedecline will allow the early detection ofthose at higher risk and, therefore, theimplementation of a tailored preventionapproach with higher chances of success.
Knoweldgegathering/Dissemination
Guidelines andreccomendations
International Sportand CultureAssociation
ACTIVEAGE 1. Active Age Handbook: Capacitybuilding for physical activity of olderpeople. Recommendations - Guidelines -Practical tools to create and implementstrategies and programs in sportorganisations. 2. Creation of theEuropean Platform for Active Aging inSport (EPAS) These are all deliverables.
Knoweldgegathering/Dissemination
Questionnaireinvestigatingcorrelation betweencultural and socialactivities and frailtystatus
Federico IIUniversity andHospital NaplesItaly, FondazioneGENS Onlus
Getting OptimiseAgeing Life-quality -GOAL integratingwell-being, propernutrition andphysical activity:novel approaches to�ght and preventfrailty
Fondazione GENS Onlus incollaboration with the School ofMedicine of the University Federico II ofNaples. has developed and an ad hocquestionnaire to test the relation betweenengagement into cultural and socialactivities and well-being, resilience,adherence to diet, physical activities,diagnosed diseses and perceived healthstatus. The questionnaire has beenadministered to four di�erent groups:Movie clubs audience, beach resortclients, art metrotorur participants andcardio clinics out patients. By november2014, 850 questionnaires have beencollected and stored in a dedicated database. Gender distribution of thepopulation examind is 54% women an46%men. Mean age of the populatio is57,7 years and 438 subjects are over 60(mean age 68,45+ 7) representing 49% ofthe population examined. Preliminaryanalysis indicate that there is a direct andsigni�cant correlation betweenwell-being and cultural and socialengagement in both the over and under60 subjects.
Knoweldgegathering/Dissemination
Scienti�c Article Regione del Veneto TheMarco PoloInitiative: Using aMultidimensionalPrognostic Index -MPI and frailty.
International dissemination of the results.(www.mpiage.eu)
Knowledgegathering/Dissemination
Scienti�c Articles Aston University Healthy ageingmetabolism andnutrients
Scienti�c publication on the preventionof progression from pre-frailty to frailtyin older adults trought the study of thenutrient status of older adults withparticular attention to fatty acids andantioxidant nutrients.
Knowledgegathering/Dissemination
Twitter Account Agencia EstatalConsejo Superior deInvestigacionesCientí�cas (CSIC) -@nutretuoido
Social networks todisseminatenutritional habitsfor the elderly toimprove theirquality of hearing -@nutretuoido
A twitter account to increased awarenesson the importance of hearing impairmentfor active ageing, and on the impact ofnutrition on hearing loss (@nutretuoidoin Spanish and @targear in English). Theultimate goal of the project is to improvediet habits in order to prevent/delay theonset of age-related hearing loss, whilehaving an impact on the risk of falling.
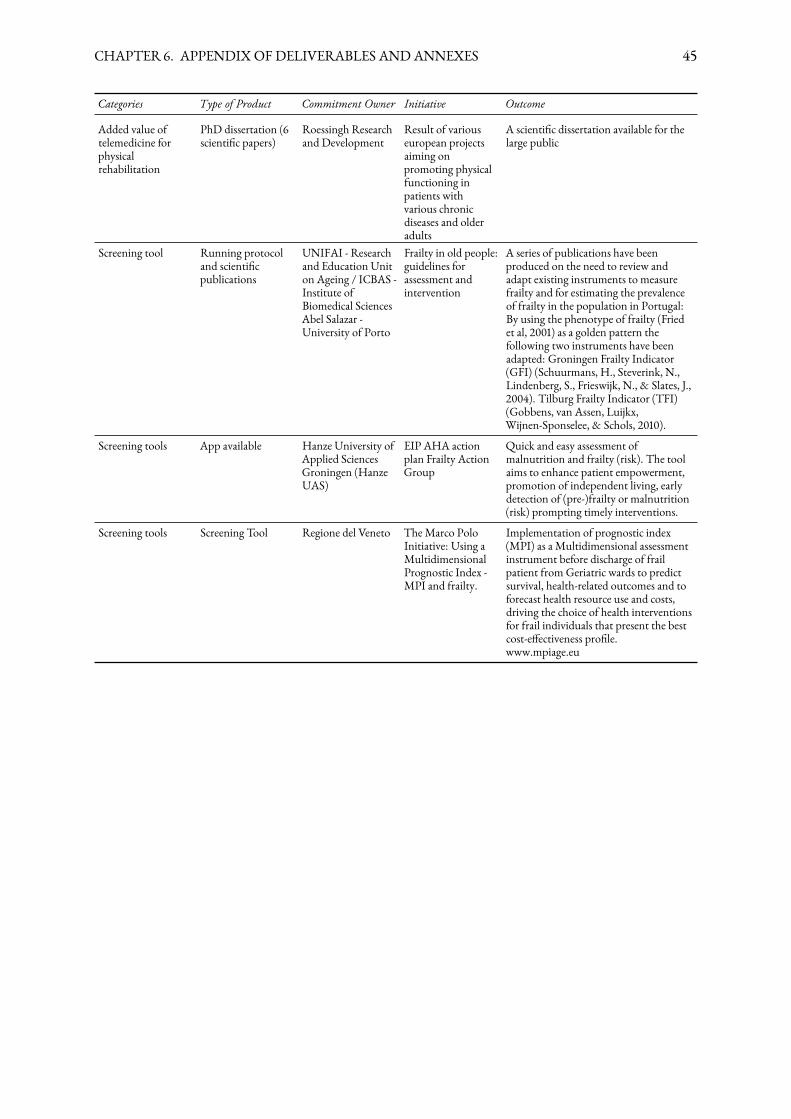
CHAPTER 6. APPENDIXOFDELIVERABLES ANDANNEXES 45
Categories Type of Product Commitment Owner Initiative Outcome
Added value oftelemedicine forphysicalrehabilitation
PhD dissertation (6scienti�c papers)
Roessingh Researchand Development
Result of variouseuropean projectsaiming onpromoting physicalfunctioning inpatients withvarious chronicdiseases and olderadults
A scienti�c dissertation available for thelarge public
Screening tool Running protocoland scienti�cpublications
UNIFAI - Researchand Education Uniton Ageing / ICBAS -Institute ofBiomedical SciencesAbel Salazar -University of Porto
Frailty in old people:guidelines forassessment andintervention
A series of publications have beenproduced on the need to review andadapt existing instruments to measurefrailty and for estimating the prevalenceof frailty in the population in Portugal:By using the phenotype of frailty (Friedet al, 2001) as a golden pattern thefollowing two instruments have beenadapted: Groningen Frailty Indicator(GFI) (Schuurmans, H., Steverink, N.,Lindenberg, S., Frieswijk, N., & Slates, J.,2004). Tilburg Frailty Indicator (TFI)(Gobbens, van Assen, Luijkx,Wijnen-Sponselee, & Schols, 2010).
Screening tools App available Hanze University ofApplied SciencesGroningen (HanzeUAS)
EIP AHA actionplan Frailty ActionGroup
Quick and easy assessment ofmalnutrition and frailty (risk). The toolaims to enhance patient empowerment,promotion of independent living, earlydetection of (pre-)frailty or malnutrition(risk) prompting timely interventions.
Screening tools Screening Tool Regione del Veneto TheMarco PoloInitiative: Using aMultidimensionalPrognostic Index -MPI and frailty.
Implementation of prognostic index(MPI) as a Multidimensional assessmentinstrument before discharge of frailpatient from Geriatric wards to predictsurvival, health-related outcomes and toforecast health resource use and costs,driving the choice of health interventionsfor frail individuals that present the bestcost-e�ectiveness pro�le.www.mpiage.eu
















![Action of almond emulsin on the phenyl glycosides of ... · Pigman] Action oj Enzymes on Glycosides 199 The action of the almond emulsin on a number of methyl hepto sides has been](https://img.pdfslide.us/doc/110x75/5eac6b92ca221e1a974d6e71/action-of-almond-emulsin-on-the-phenyl-glycosides-of-pigman-action-oj-enzymes.jpg)