Embed Size (px)
Citation preview

1
The ABC’s of LUMBAR SPINE DISEASE
The ABC’s of LUMBAR SPINE DISEASE
Susan O. Smith ANP-BC
University of Rochester
Department of Neurological Surgery
Susan O. Smith ANP-BC
University of Rochester
Department of Neurological Surgery
Diagnosis/Imaging/Surgery of Lumbar Spine Disorders
ObjectivesObjectives
Identify the most common pathology that leads to spine surgery
Describe the key exam findings that will be assessed pre and post op
Describe the most common elective surgery techniques
Identify the most common pathology that leads to spine surgery
Describe the key exam findings that will be assessed pre and post op
Describe the most common elective surgery techniques

2
Conflicts of InterestConflicts of Interest
none none
AJNR addition to reportsAJNR addition to reports

3
FACET JOINT
LAMINA
SPINOUS PROCESS
Diagnosis & Imaging of Common Causes of Back Pain
Lumbar Disc HerniationLumbar Disc Herniation
Diagnosis & Imaging of Common Causes of Back Pain
Nerve Sac
Disc & Pinched Nerve
4
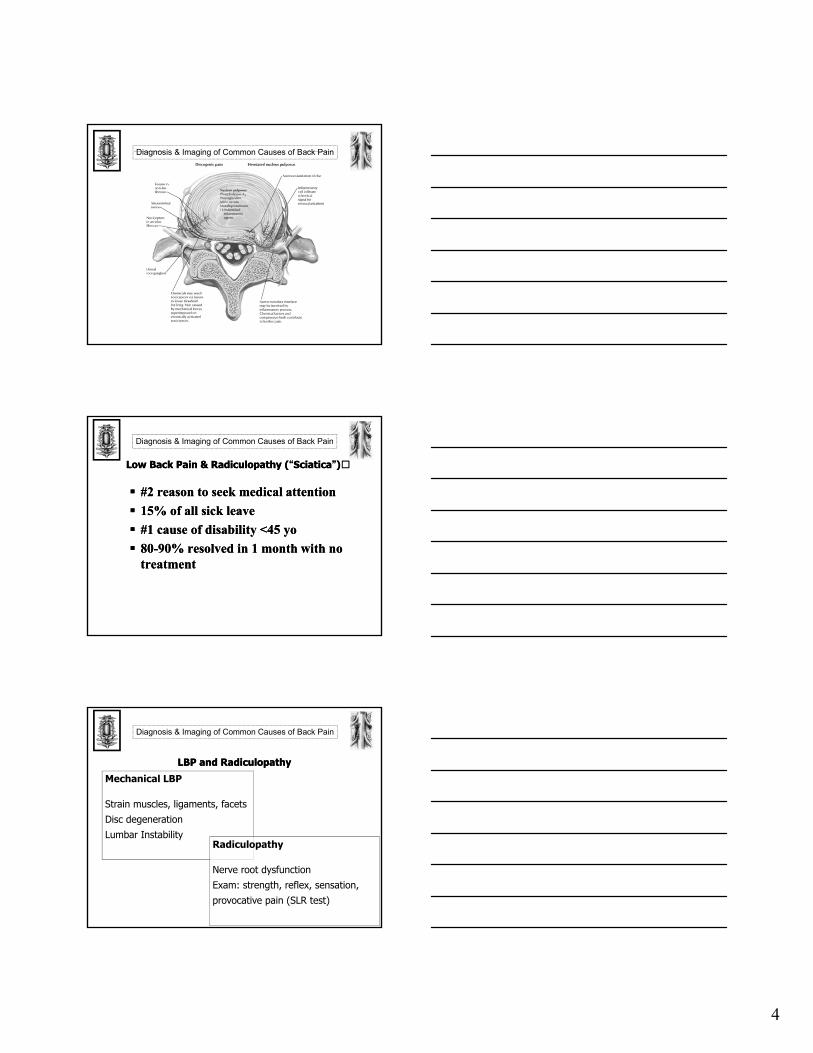
Diagnosis & Imaging of Common Causes of Back Pain
Low Back Pain & Radiculopathy (“Sciatica”)Low Back Pain & Radiculopathy (“Sciatica”)
Diagnosis & Imaging of Common Causes of Back Pain
#2 reason to seek medical attention
15% of all sick leave
#1 cause of disability <45 yo
80-90% resolved in 1 month with no treatment
#2 reason to seek medical attention
15% of all sick leave
#1 cause of disability <45 yo
80-90% resolved in 1 month with no treatment
LBP and RadiculopathyLBP and RadiculopathyMechanical LBP
Strain muscles, ligaments, facetsDisc degenerationLumbar Instability
Radiculopathy
Nerve root dysfunctionExam: strength, reflex, sensation, provocative pain (SLR test)
Diagnosis & Imaging of Common Causes of Back Pain

5
Differential Diagnosis: LBPDifferential Diagnosis: LBP
• Mechanical LBP majority of patients
• Radiculopathy 1%, only 1-3% HNP
• “Red Flags” neurogenictumorinfection fracture
Diagnosis & Imaging of Common Causes of Back Pain
Diagnosis & Imaging of Common Causes of Back Pain
Diagnosis & Imaging of Common Causes of Back Pain
6
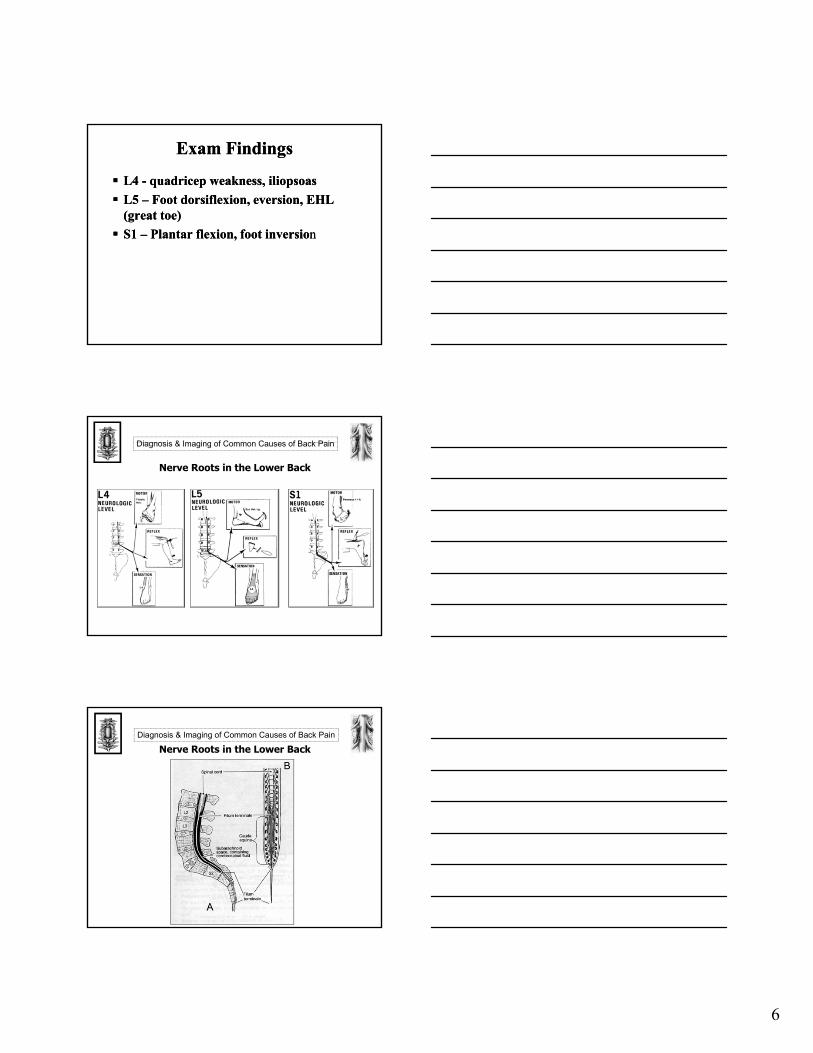
Exam FindingsExam Findings
L4 - quadricep weakness, iliopsoas
L5 – Foot dorsiflexion, eversion, EHL (great toe)
S1 – Plantar flexion, foot inversion
L4 - quadricep weakness, iliopsoas
L5 – Foot dorsiflexion, eversion, EHL (great toe)
S1 – Plantar flexion, foot inversion
Diagnosis & Imaging of Common Causes of Back Pain
Nerve Roots in the Lower Back
Nerve Roots in the Lower BackDiagnosis & Imaging of Common Causes of Back Pain

7
Conservative TreatmentConservative Treatment
NSAIDS
Physical Therapy
Chiropractic Care
Aqua Therapy
Epidural/trigger point steroid injections
NSAIDS
Physical Therapy
Chiropractic Care
Aqua Therapy
Epidural/trigger point steroid injections
SURGERY INDICATIONSSURGERY INDICATIONSLumbar Disc Herniation
(laminectomy/discectomy)Lumbar Stenosis
(lumbar decompression/bilateral laminectomy, foraminotomies
Spondylolisthesis = slippage of alignmentSpondylolysis = pars fracture/pedicle fractureRX - Fusion if dynamic movement
Lumbar Disc Herniation(laminectomy/discectomy)
Lumbar Stenosis(lumbar decompression/bilateral laminectomy, foraminotomies
Spondylolisthesis = slippage of alignmentSpondylolysis = pars fracture/pedicle fractureRX - Fusion if dynamic movement
Diagnosis & Imaging of Common Causes of Back Pain
6 months of conservative treatment, severe pain, unable to work, WHY?
8
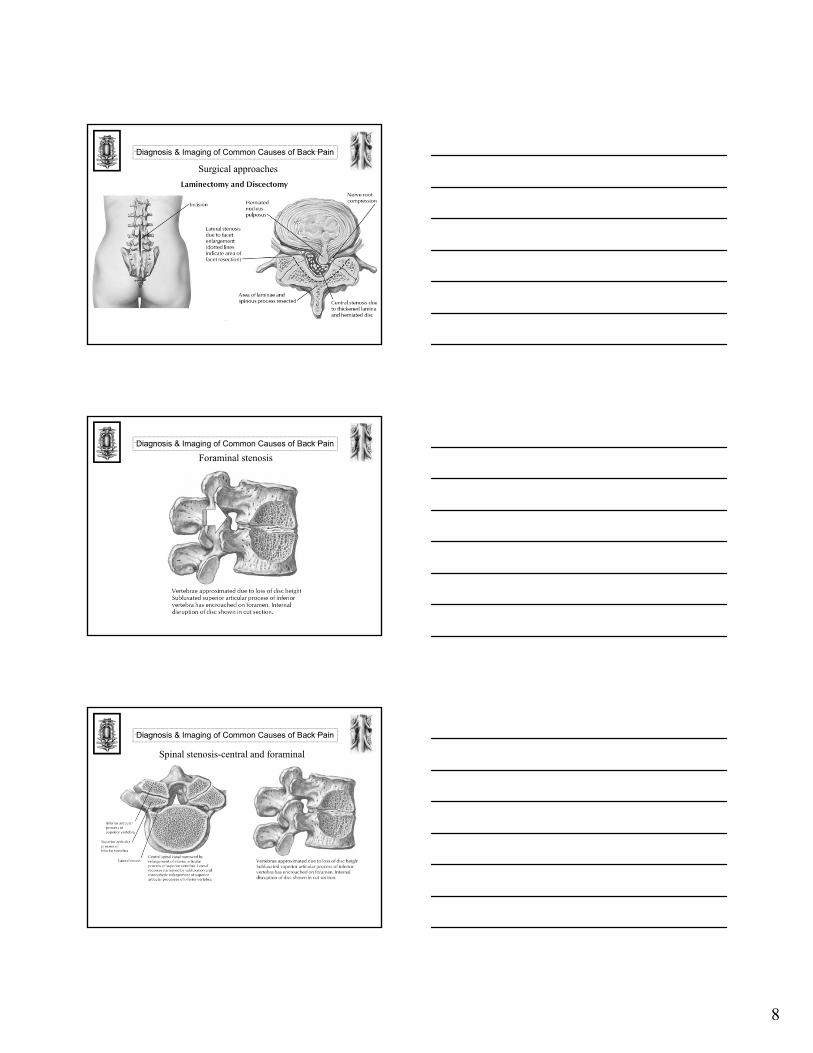
Diagnosis & Imaging of Common Causes of Back Pain
Surgical approaches
Diagnosis & Imaging of Common Causes of Back Pain
Foraminal stenosis
Diagnosis & Imaging of Common Causes of Back Pain
Spinal stenosis-central and foraminal
9
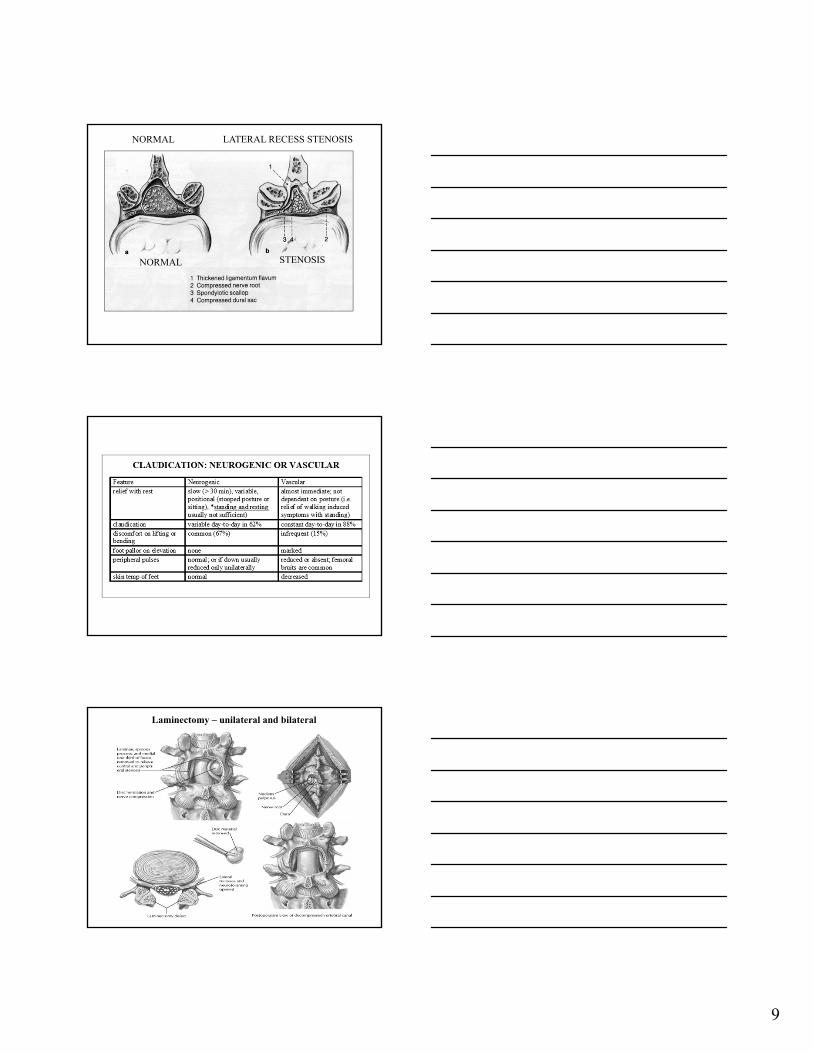
NORMAL LATERAL RECESS STENOSIS
NORMAL STENOSIS
Laminectomy – unilateral and bilateral

10
LUMBAR STENOSISLUMBAR STENOSIS
R.O. 72 yo male with 3 year history of LBP and L > R LE pain; epidural steroids X12 ineffective
EXAM: LEFT EHL 5/3+, Bilateral hypesthesiafrom ankles to toes, KJ tr/0, AJ0/0
MYELO/CT: Congenital stenosis, diffuse disc bulging, ligamentum flavum hypertrophy, severe facet hypertrophy
R.O. 72 yo male with 3 year history of LBP and L > R LE pain; epidural steroids X12 ineffective
EXAM: LEFT EHL 5/3+, Bilateral hypesthesiafrom ankles to toes, KJ tr/0, AJ0/0
MYELO/CT: Congenital stenosis, diffuse disc bulging, ligamentum flavum hypertrophy, severe facet hypertrophy
Myelogram - Lumbar StenosisMyelogram - Lumbar Stenosis
Post Myelo CT - Lumbar StenosisPost Myelo CT - Lumbar Stenosis
11
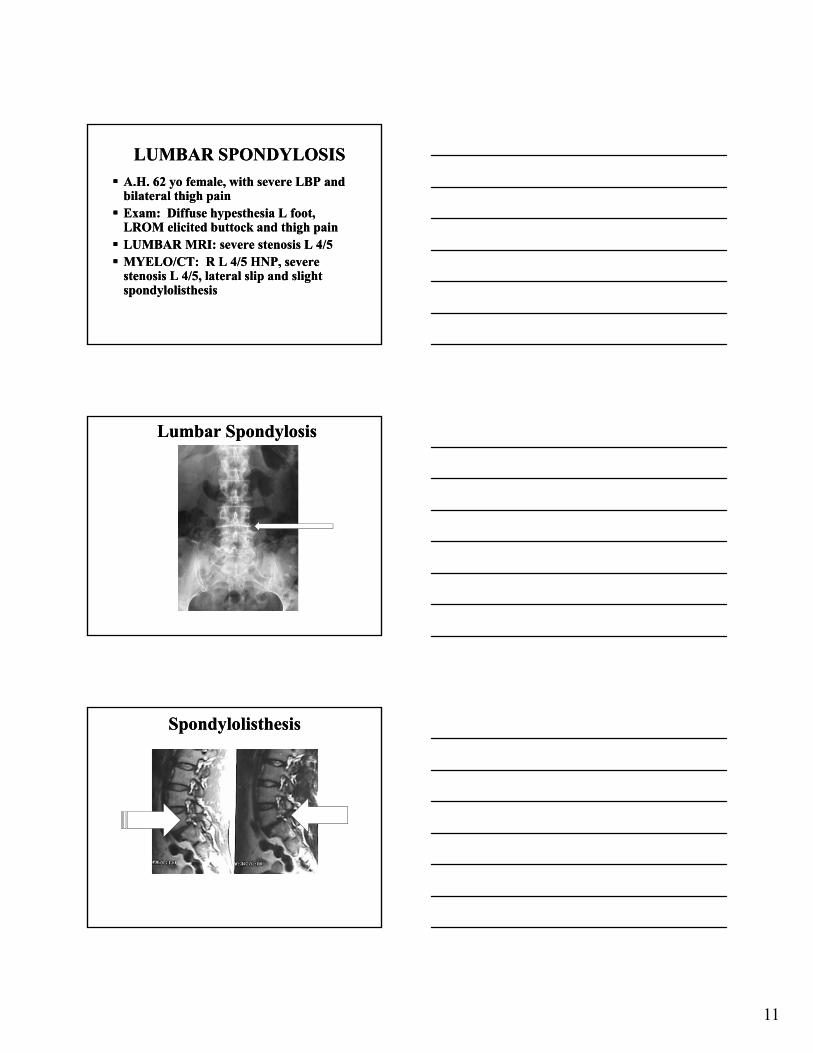
LUMBAR SPONDYLOSISLUMBAR SPONDYLOSIS
A.H. 62 yo female, with severe LBP and bilateral thigh pain Exam: Diffuse hypesthesia L foot,
LROM elicited buttock and thigh pain LUMBAR MRI: severe stenosis L 4/5 MYELO/CT: R L 4/5 HNP, severe
stenosis L 4/5, lateral slip and slight spondylolisthesis
A.H. 62 yo female, with severe LBP and bilateral thigh pain Exam: Diffuse hypesthesia L foot,
LROM elicited buttock and thigh pain LUMBAR MRI: severe stenosis L 4/5 MYELO/CT: R L 4/5 HNP, severe
stenosis L 4/5, lateral slip and slight spondylolisthesis
Lumbar SpondylosisLumbar Spondylosis
SpondylolisthesisSpondylolisthesis
12
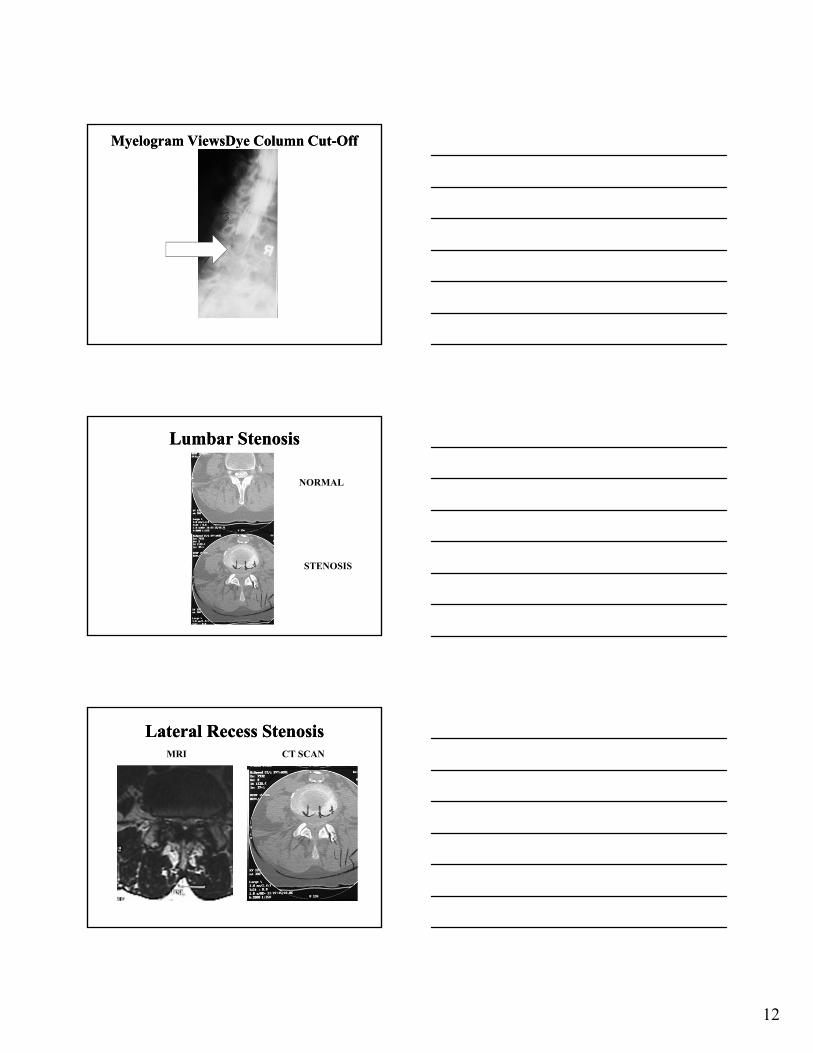
Myelogram ViewsDye Column Cut-OffMyelogram ViewsDye Column Cut-Off
Lumbar StenosisLumbar Stenosis
NORMAL
STENOSIS
Lateral Recess StenosisLateral Recess StenosisMRI CT SCAN

13
Lumbar Congenital StenosisLumbar Congenital Stenosis
Lumbar DecompressionPedicle Screw Fusion Interbody Graft
Lumbar DecompressionPedicle Screw Fusion Interbody Graft
SpondylolysisSpondylolysis Repetitive exposure to simultaneous forces of muscle
contraction, gravity and rotational forces
Repeated micro fractures of the pars interarticularis
Classic imaging - discontinuity of the neck of the “scotty dog”, extra facets on CT
Often associated with spondylolisthesis
10 - 15% unilateral defects
Repetitive exposure to simultaneous forces of muscle contraction, gravity and rotational forces
Repeated micro fractures of the pars interarticularis
Classic imaging - discontinuity of the neck of the “scotty dog”, extra facets on CT
Often associated with spondylolisthesis
10 - 15% unilateral defects

14
PARS DEFECT IS A SPONDYLOLYSIS
SpondylolysisSpondylolysis
15
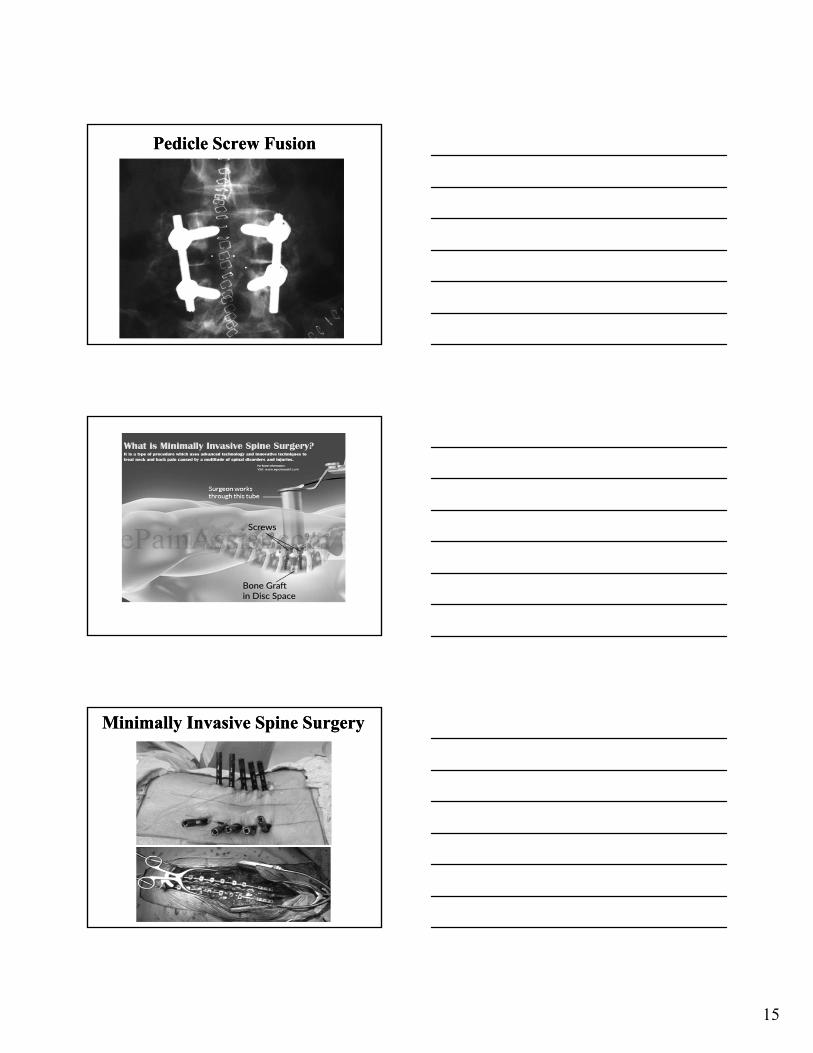
Pedicle Screw FusionPedicle Screw Fusion
Minimally Invasive Spine SurgeryMinimally Invasive Spine Surgery

16
MISSMISS
MISSMISS
Cauda Equina SyndromeCauda Equina Syndrome Sphincter disturbance - Anal 60-80%, urinary
retention 90% sensitivity Saddle Anesthesia - sensitivity 75% Significant Motor Weakness*Large Central Disc Herniation with compression of
the thecal sac (1-2% of disc herniations) Cauda Equina syndrome outcome following
surgery is clearly correlated with timing of surgery within 48 hours of syndrome onset.
Sphincter disturbance - Anal 60-80%, urinary retention 90% sensitivity
Saddle Anesthesia - sensitivity 75% Significant Motor Weakness*Large Central Disc Herniation with compression of
the thecal sac (1-2% of disc herniations) Cauda Equina syndrome outcome following
surgery is clearly correlated with timing of surgery within 48 hours of syndrome onset.
Neurosurg Focus 16 (6): 2004

17
Post op AssessmentPost op Assessment Any new weakness?
Urinary retention? Muscle relaxants can contribute to high PVR
Pain control – meds are only meant to take the “edge” off of pain, not to have pain freedom.
Wound drainage that is excessive
SOB or low O2 Sat that could signify PE or respiratory distress
Any new weakness?
Urinary retention? Muscle relaxants can contribute to high PVR
Pain control – meds are only meant to take the “edge” off of pain, not to have pain freedom.
Wound drainage that is excessive
SOB or low O2 Sat that could signify PE or respiratory distress
18
Thank you, any Questions?Thank you, any Questions?
Scarlett, Sherman, Simon, Samson, Spencer, Sophie, Sydney