Embed Size (px)
Citation preview
The ABCs of Children’s Health and Federal Reform: Understanding the
Potential Impact of PPACA
Jean Marie Abraham, Ph.D.
Division of Health Policy & Management
School of Public Health
University of Minnesota
October 15, 2010
Outline
• Access to Coverage by Children – Why is it important for children’s health?– What are the attributes of uninsured children and their
families?– How will the coverage expansion and mandate parameters
under PPACA affect them?• Burden of Health Care Costs
– How should we think about health care spending, underinsurance, and burden?
– How might PPACA provisions likely affect these outcomes?• Care Provision
– What is the potential effect of expanding coverage on demand for care by previously uninsured children?
– What are some other PPACA provisions likely to affect children’s receipt of health care and outcomes?
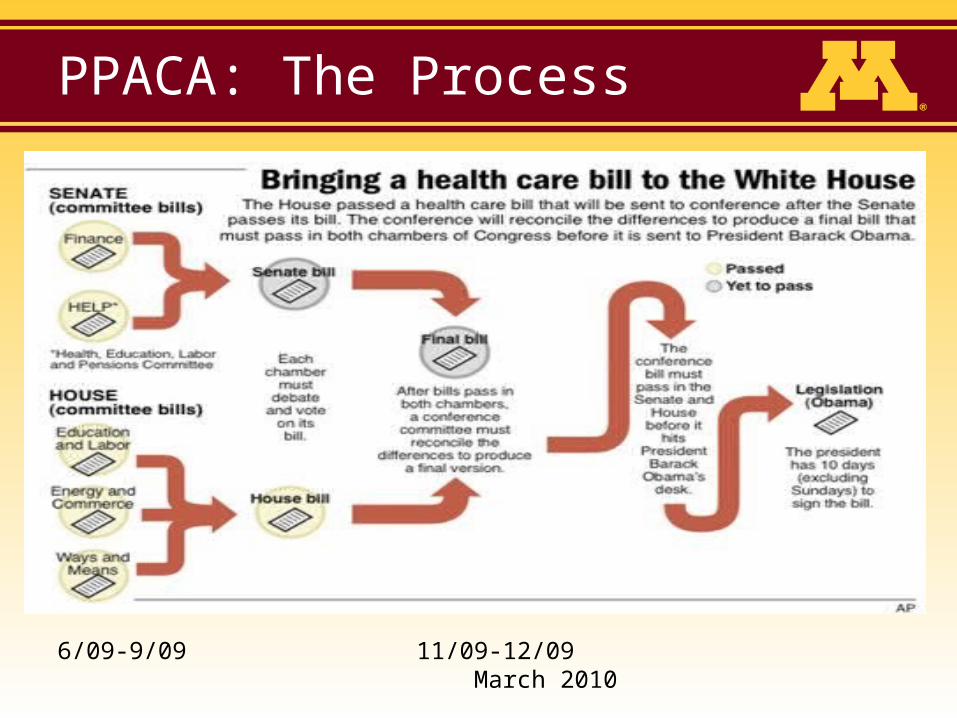
PPACA: The Process
6/09-9/09 11/09-12/09 March 2010

Widespread Impact
• Uninsured
• Individuals who buy health insurance on their own
• People with employer-sponsored insurance
• Medicare beneficiaries
• Healthcare providers
• Health insurers
• Taxpayers
Access to Coverage by Children
Why is insurance important?
• Financial Access to Care– Preventive care for children
• Well-child visits– Assessing development– Administering immunizations– Educating parents and children about safety, lifestyle, and
development
– Acute care• More timely access
– Potential for reduced morbidity • Asthma, Mental health, Diabetes
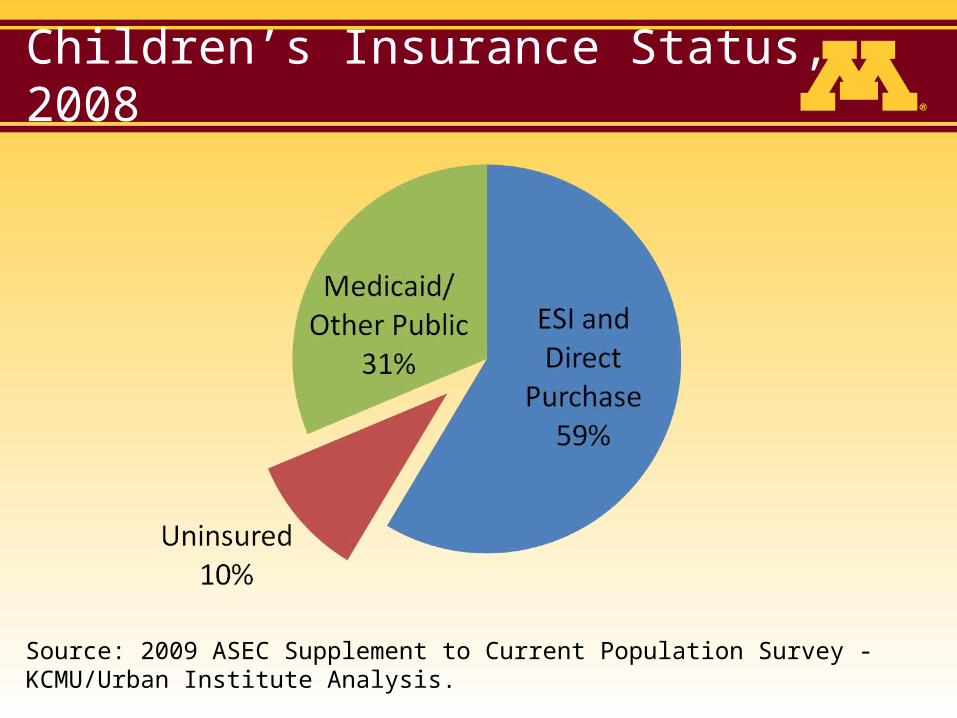
Children’s Insurance Status, 2008
Source: 2009 ASEC Supplement to Current Population Survey - KCMU/Urban Institute Analysis.
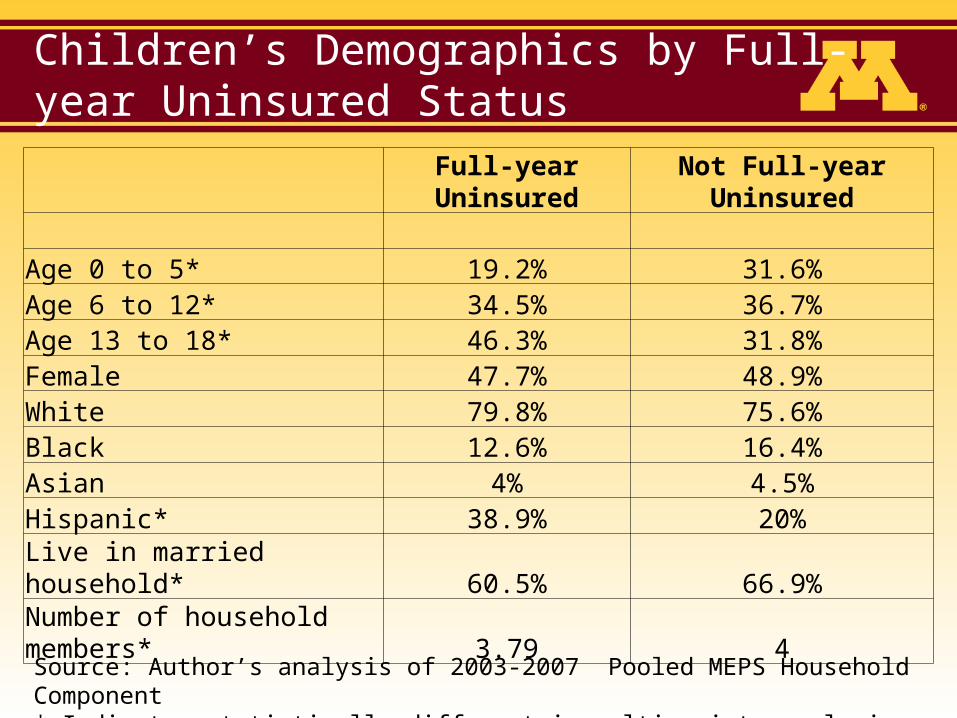
Children’s Demographics by Full-year Uninsured Status
Full-year Uninsured Not Full-year Uninsured
Age 0 to 5* 19.2% 31.6%Age 6 to 12* 34.5% 36.7%Age 13 to 18* 46.3% 31.8%Female 47.7% 48.9%White 79.8% 75.6%Black 12.6% 16.4%Asian 4% 4.5%Hispanic* 38.9% 20%
Live in married household* 60.5% 66.9%Number of household members* 3.79 4
Source: Author’s analysis of 2003-2007 Pooled MEPS Household Component* Indicates statistically different in multivariate analysis of Prob(FY uninsured)
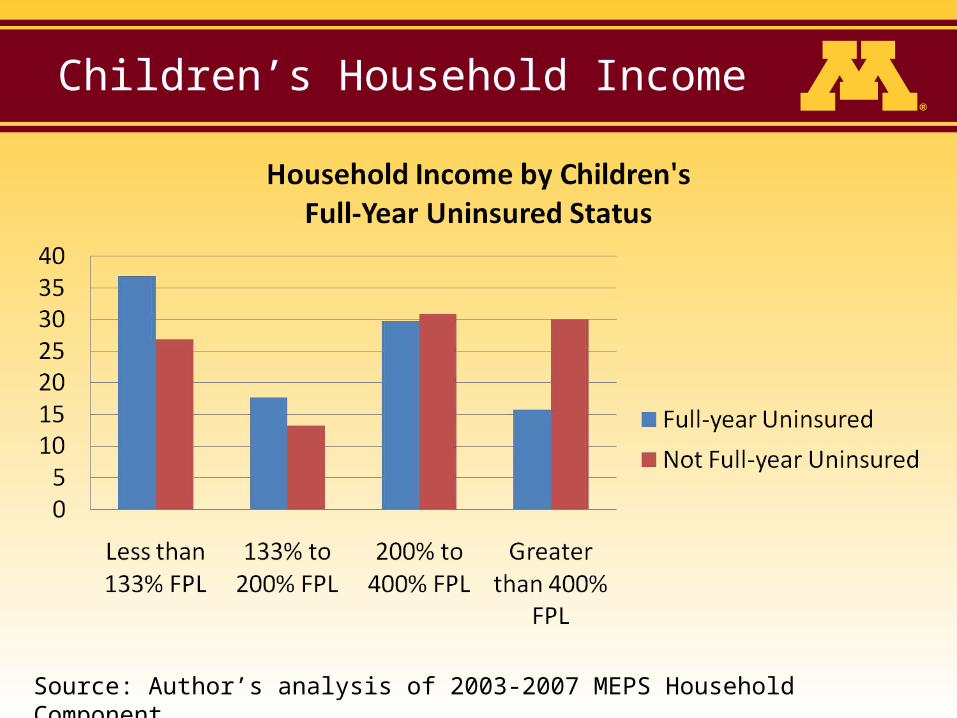
Children’s Household Income
Source: Author’s analysis of 2003-2007 MEPS Household Component
Coverage Expansion in 2014
• Medicaid– Expand eligibility to all individuals in families
earning less than 133% FPL– Children
• Current eligibility varies by state, ranging from 100% FPL to 300% FPL
• 20 states directly affected
– Adults• Eligibility varies by pregnancy, working parents, childless
adults (not covered in 45 states)
– CBO projected net increase of 16 million by 2019
Coverage Expansion in 2014
• Exchanges– Organized marketplace for individually purchased
and small employer coverage– Functions
• Certify qualified health plans (e.g., marketing, provider choice, quality)
• Determine open enrollment period• Review premium rate increases• Standardize enrollment process• Provide employers with price and quality information on available
plans in standard format• Create a web portal to shop
Coverage Expansion in 2014
• Exchange-based premium assistance credits – Individuals with family incomes of 133% FPL– 400% FPL
who do not have an offer of employer-sponsored insurance
– Subsidies based on a sliding-scale• 3%-9.5% of income is maximum dollar amount families
would pay for coverage• Tied to the “Silver plan” (70% actuarial value)
– Premium rating reforms• Modified community rating• Guaranteed issue and renewability
– CBO projects a net increase of 24 million in Exchanges
Individual Mandate in 2014
• U.S. citizens and legal residents must have qualifying health coverage
• Tax penalty the greater of $695 per year up to 3 times that amount for a family or 2.5% of household income
• Phased in through 2016• Exemptions
– Financial hardship waiver if lowest cost plan is more than 8% of income
– < 3 month gaps – Religious objections, – Prisoners– Undocumented immigrants
Increased Regulation of Private Insurance (2010)
• No lifetime limits on benefits
• No ‘unreasonable’ annual limits
• No exclusions or delays in coverage for particular services for children with pre-existing conditions
• Require qualified health plans to provide certain preventive services with zero cost-sharing.
Burden of Health Care Spending for Families with Children
Spending on Health Care
• Types – Medical care and Premiums
• Research literature– Underinsurance
• “Adequacy” of coverage• Spending on medical care relative to income
– Financial Burden• Spending on medical care and insurance premiums relative to income
• Challenges– No consensus on measurement– Heterogeneity by family attributes and over time
Underinsurance
• Kogan et al., NEJM, 2010
– National Survey of Children’s Health in 2007
– Stated response regarding• Does child’s health insurance offer benefits or cover services that
meet his or her needs?
• Does child see providers he/she needs?
• How often are costs reasonable, conditional on answering that they pay money for care?
– Findings• 22.7% of U.S. children underinsured
– Older, Hispanic, Private Insurance, Special Needs
• Of those underinsured– 11.6% had no preventive care visit
– 32% reported difficulty obtaining referrals for needed care (among those who needed them)
Financial Burden
• Banthin, Cunningham, and Bernard, Health Affairs, 2008– Methods
• 2001-2004 MEPS• Doesn’t restrict to families with children• High out-of-pocket burden as spending more than
10% of after-tax family income on medical expenses and premiums
– Findings• 17.0% of employer-based population in 2004
PPACA Provisions Affecting Burden
• Privately Insured– Exchange-based enrollment
• OOP cost-sharing subsidies for families earning less than 200% FPL
• Higher income levels may obtain coverage given the mandate, but face increased burden
– Family of 4 making 300% FPL ($66,000) paying $6,270 for a family coverage plan.
– Employer-based coverage• Annual real growth in premiums is about 5%• Cost-sharing provisions are increasing • Financial burden will likely continue to rise given existing trends
and because of increased regulation on benefit design
Provision of Medical Care
Increased demand for services
• How much additional care will uninsured children demand once they get coverage?– Evidence from state coverage expansions of Medicaid
and CHIP (Buchmueller et al. 2005)• Outpatient visits (Banthin & Selden, 2003; Currie,
2000; Marquis & Long, 1995)– +1 visit per year on average
• Inpatient utilization– Small demand response
» Medicaid eligibility raises the probability of inpatient hospitalization by 4%
Potential increase in children’s demand for medical care given PPACA
• Hofer, Abraham, and Moscovice (working paper, 2010)– Estimate an empirical model of utilization for primary care
visits using 2006-2007 MEPS– Predict impact of the coverage expansion on visits
• Overall increase in U.S. in 2019– 23.3 million visits (7.5% increase)
» 20 million by adults» 3.3 million are visits by children
• Large state variation
– 5,900 additional primary care providers
Other Provisions Affecting Care
• Medicaid– Medicaid payment rates increased in
2013/2014 to Medicare levels• Improve access
– Quality Measurement Program• Compare provider performance
– Pediatric Accountable Care Organization Demonstration
• Alignment of providers’ incentives across continuum of care
Other Provisions
• Maternal, Infant, and Early Childhood Home Visitation Programs (Sec. 2951)– Statewide needs assessment– State grants
Other Provisions
• School-based health centers (Sec. 4101)– Comprehensive primary health services
during school hours to children and adolescents and 24 hour on-call system
– $50 million/ year for 2010-2013– Priority communities
• High barriers to access• High per capita numbers of children who are
uninsured, underinsured, or enrolled in public insurance
Concluding Remarks
• PPACA is going to “change the game” – Coverage expansion will improve financial access for over 7
million full-year uninsured children– Population-specific burden effects– Expected increase in demand for care
• Uncertainty regarding implementation and impact– Administrative rule-making– State government responses– Insurers, Providers, and Consumers
– Constitutionality of the mandate and Medicaid expansion
• Coverage first, cost second approach
Resources on PPACA
• Official Federal government website– www.healthcare.gov
• Kaiser Family Foundation– www.kff.org
• Democratic Policy Committee (U.S. Senate)– www.dpc.senate.gov
• U.S. Chamber of Commerce– http://www.uschamber.com/healthcare.htm
Thank you!
Jean Marie Abraham, Ph.D.Division of Health Policy and Management
School of Public HealthUniversity of Minnesota
Email: [email protected]: (612) 625-4375