Embed Size (px)
Citation preview

The ABCDs of Obesity “Adipose Based Chronic Disease”
Michael A. Bush, M.D. Clinical Chief, Division of Endocrinology
Cedars-Sinai Medical Center Clinical Associate Professor, Geffen School of Medicine, UCLA
President, CA-AACE
The ABCDs of Obesity “Adipose Based Chronic Disease”
Michael A. Bush, M.D. Clinical Chief, Division of Endocrinology
Cedars-Sinai Medical Center Clinical Associate Professor, Geffen School of Medicine, UCLA
President, CA-AACE

3
Classification of Weight by BMI
(Must A, et al. JAMA. (1999) 282: 1523-29) (NIH. Obes Res. 1998) (World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO Consultation presented at: the World Health Organization; June 3-5, 1997; Geneva, Switzerland. Publication WHO/NUT/NCD/98.1)
with co-morbidities

4
•MULTIPLY WEIGHT IN POUNDS BY 705
•DIVIDE BY HEIGHT IN INCHES
•DIVIDE BY HEIGHT IN INCHES AGAIN
CALCULATING BODY MASS INDEX Wt (kg) / Ht (m)2
5
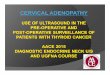
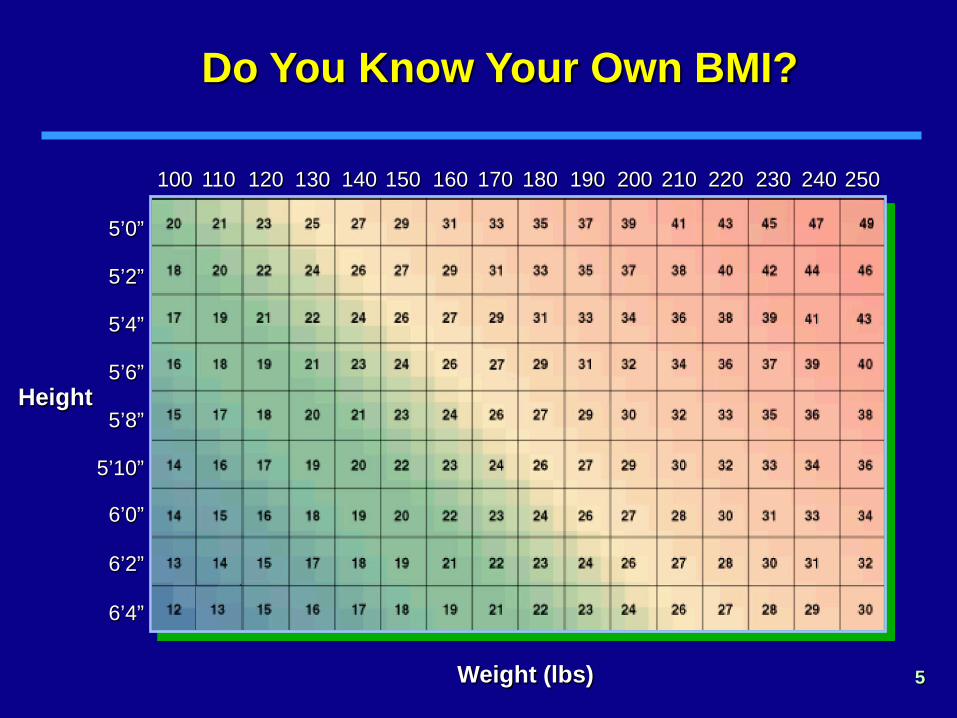
Do You Know Your Own BMI?
5’4”
Height
Weight (lbs)
5’2”
5’0”
5’10”
5’8”
5’6”
6’0”
6’2”
6’4”
100 110 120 130 140 150 160 170 180 190 200 210 220 230 240 250

6
OBESITY IN THE UNITED STATES A Growing Epidemic
N/A
<10%
10-15%
>15%
2000 2014

7
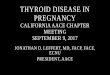
Compared with Caucasians, Asians have Higher Levels of Body Fat vs BMI
• SUBJECTS: Hong Kong Chinese, Indonesians (Malays and Chinese), Singaporean (Chinese, Malays and Indians)
• Generally, for the same BMI, Asians’ Body Fat was 3-5% higher compared to Caucasians.
• Results can be partly explained by differences in body build, i.e. trunk-to-leg-length ratio and slenderness. Differences in muscularity may also contribute.
Obesity Reviews (2002), 3: 141-146.

Compared with Caucasians, South Asian Indians have Lower Insulin Sensitivity vs Body Fat
8 Chandalia M, et sl. JCEM (1999). 842329-2335
Asians have Lower Insulin Sensitivity for Any Degree of
Body Fat

9
Abdominal Obesity
10
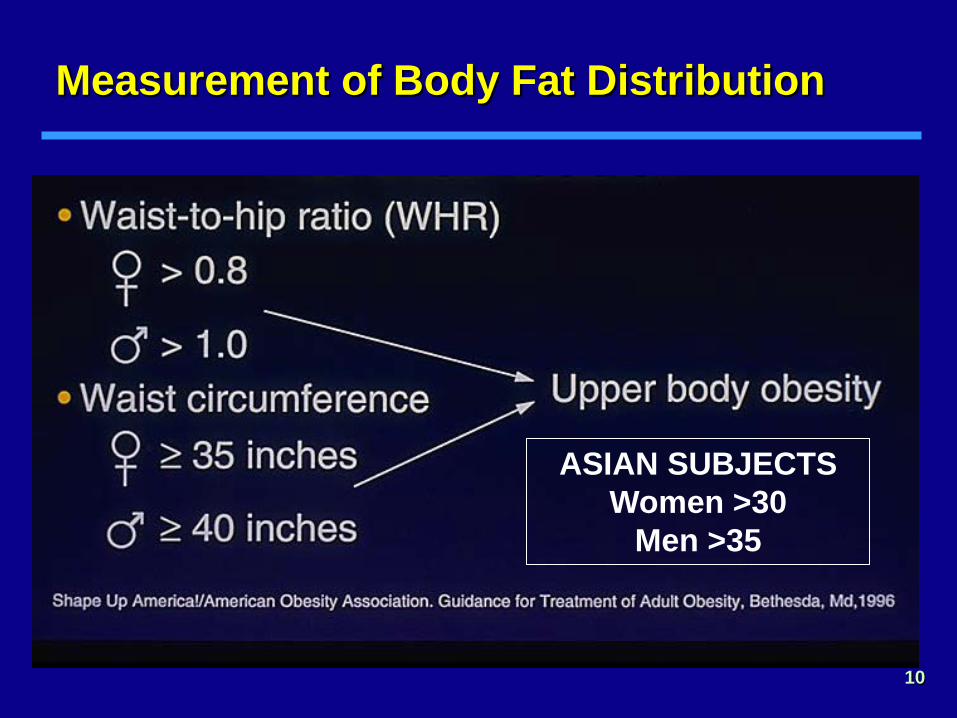
Measurement of Body Fat Distribution
ASIAN SUBJECTS Women >30
Men >35
11
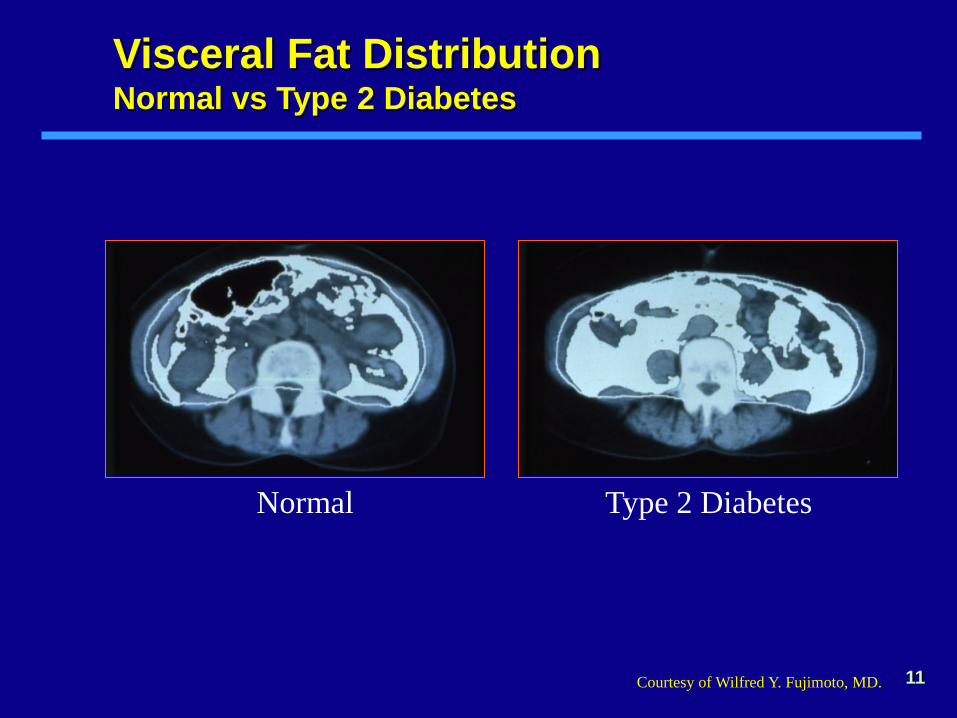
Normal Type 2 Diabetes
Courtesy of Wilfred Y. Fujimoto, MD.
Visceral Fat Distribution Normal vs Type 2 Diabetes

Obesity is a Chronic and Multifaceted disease

13
McTigue et al. Annals Int Med (2002) 136:857-864
Born in 1964
Born in 1957
The Natural History of the Development of Obesity in a Cohort of Young U.S. Adults between 1981 and 1998
(“National Longitudinal Study of Youth”)

Prevalence of Overweight and Obesity Among US Adults
47
32
15
56
33
23
64
34 31
0
20
40
60
80 Overweight or obese Overweight Obese(BMI ≥25.0) (BMI 25.0-29.9) (BMI ≥30.0)
Increased 100% in 20 years %
NHANES II 1976-1980 (n=11,207)
NHANES † 1999-2000 (n=3601)
NHANES III 1988-1994 (n=14,468)
US Bureau of the Census estimates using the age groups 20-34, 35-44, 45-54, 55-64, and 65-74 years †Flegal KM et al. JAMA. 2002;288:1723-1727.

Obesity Evaluation:
Take Obesity Seriously Take the time and make it a priority
Deal with it as you would other Diseases “Adipose-Based Chronic Disease”

Obesity Meets AMA Criteria for a Disease
16
Impairment of Normal Function
• Physical impairments • Altered physiologic
function (inflammation, insulin resistance, dyslipidemia, etc)
• Altered regulation of satiety in the hypothalamus
Characteristic Signs or Symptoms
• Increased body fat mass
• Joint pain • Impaired mobility • Low self-esteem • Sleep apnea • Altered metabolism
Harm or Morbidity
• Cardiovascular disease • Type 2 diabetes • Metabolic syndrome • Cancer • Death
AMA, American Medical Association. Mechanick JI, et al. Endocr Pract. 2012;18:642-648.

Percent of Patients Receiving PCP Advice by Obesity Classification
Simkin-Silverman LR et al. Prev Med 2005;40:71-82.
The Office Environment An Appropriate Setting for Overweight Patients

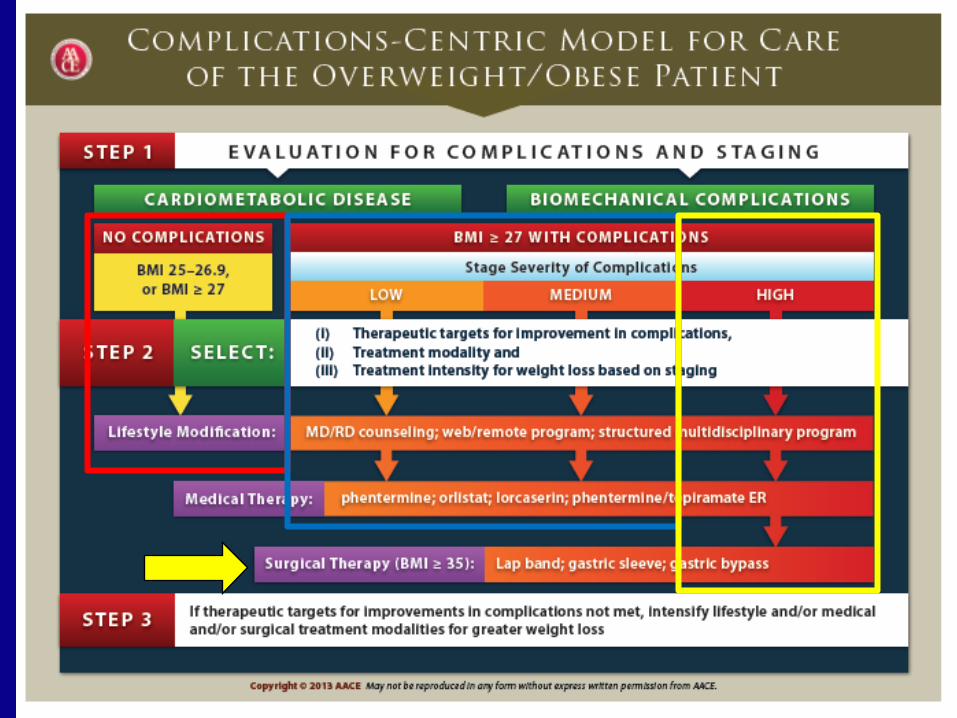
EVALUATE BMI and COMPLICATIONS Treatment is “Complications-Centric”
19

Take a Disease-focused Medical, Social, and Emotional History
• MEDICAL CAUSES OF OBESITY — Hypothyroidism, Cushing’s Syndrome, Depression, Medications
• MEDICAL/MECHANICAL/EMOTIONAL COMPLICATIONS OF OBESITY
• SOCIAL AND FAMILIAL FACTORS — Clustering, genetics, availability of resources
• EMOTIONAL FACTORS — Psych history, binge eating, comfort eating, eating disorder
• HISTORY OF OBESITY TREATMENT
Pregnant
Weight Watchers
Exercise Class,
Low Carb Diet
No $ for classes
Set agreed-upon Goals!

DISCUSS LOTS OF OPTIONS FOR WEIGHT CONTROL
21
YOUR DIET
DIETITIAN DIET
DELIVERED DIET
WW/JENNY DIET
VLCD DIET
MEDICATIONS, LONG-TERM: (Brand:) Qsymia, Belviq, Contrave, Saxenda
BARIATRIC SURGERY: Gastric Band, Bypass, Reversals, J-I, Devices
X
23
TREATMENT OF OBESITY Failure of Diet Therapy
My doctor told me I was really in trouble, so I gave up smoking, stopped drinking and started a really good diet ...
… and in 2 weeks I lost 14 days.

24
25
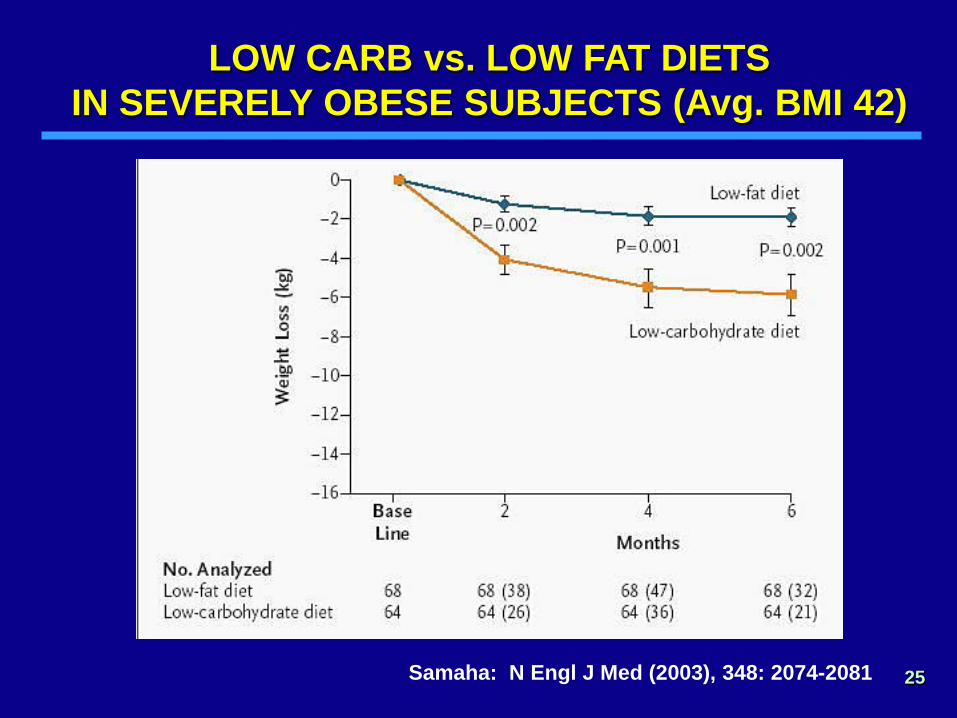
LOW CARB vs. LOW FAT DIETS IN SEVERELY OBESE SUBJECTS (Avg. BMI 42)
Samaha: N Engl J Med (2003), 348: 2074-2081
26
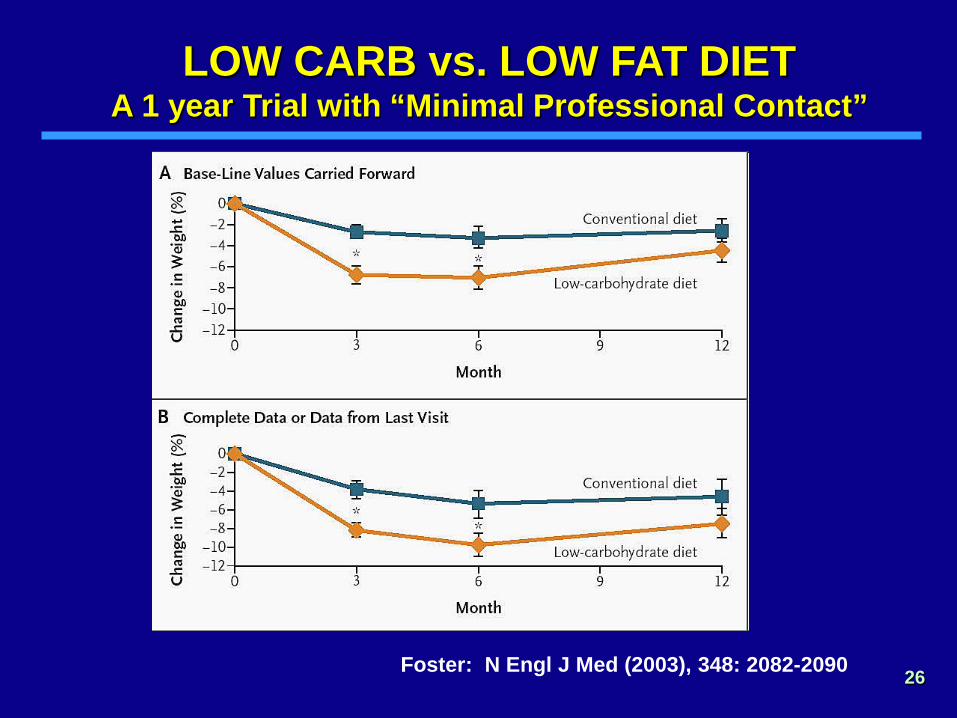
LOW CARB vs. LOW FAT DIET A 1 year Trial with “Minimal Professional Contact”
Foster: N Engl J Med (2003), 348: 2082-2090

27
LOW CARB vs. LOW FAT DIET A 1 year Trial with “Minimal Professional Contact”
Triglycerides HDL Cholesterol
Foster: N Engl J Med (2003), 348: 2082-2090

28
LOW CARB vs. LOW FAT DIET A 1 year Trial with “Minimal Professional Contact”
Foster: N Engl J Med (2003), 348: 2082-2090
LDL Cholesterol Total Cholesterol
29 Dansinger: JAMA, Volume 293(1).January 5, 2005.43–53:
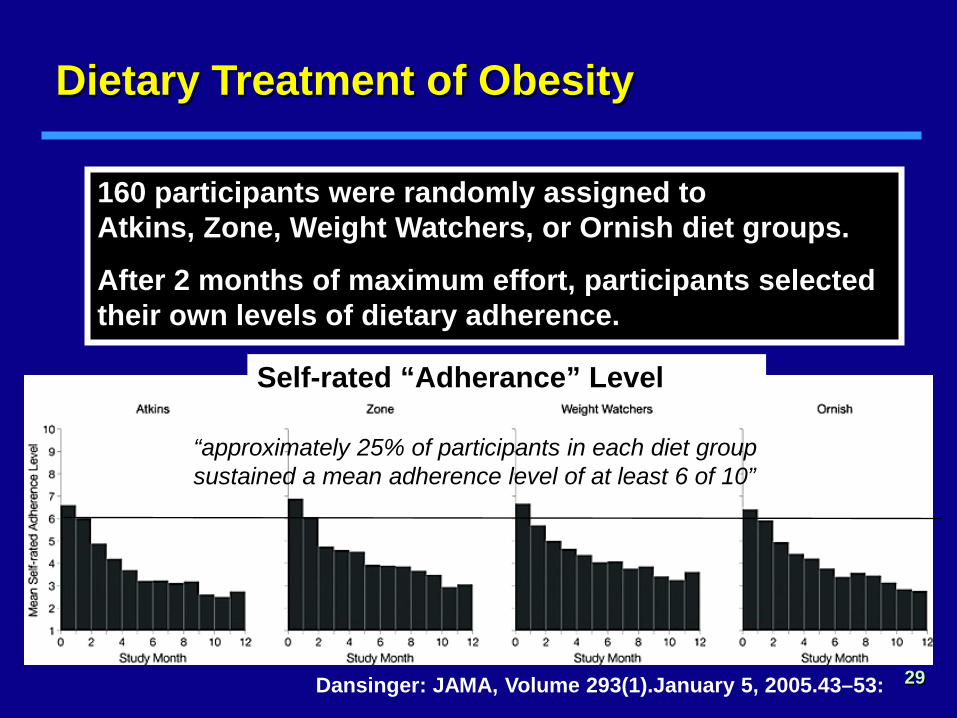
160 participants were randomly assigned to Atkins, Zone, Weight Watchers, or Ornish diet groups.
After 2 months of maximum effort, participants selected their own levels of dietary adherence.
Dietary Treatment of Obesity
Self-rated “Adherance” Level
“approximately 25% of participants in each diet group sustained a mean adherence level of at least 6 of 10”
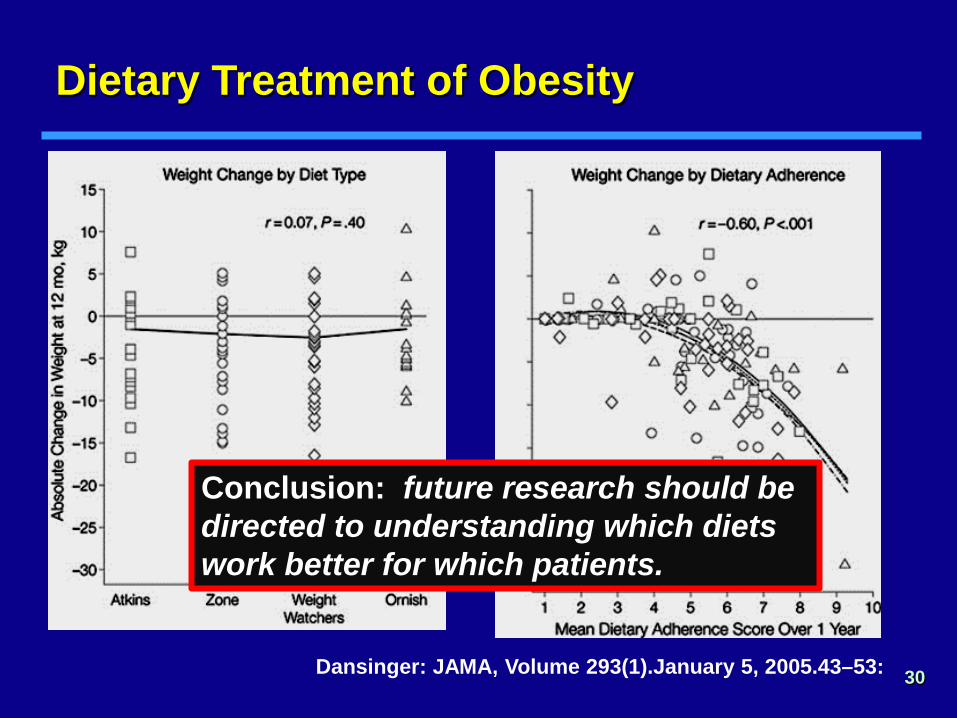
30 Dansinger: JAMA, Volume 293(1).January 5, 2005.43–53:
Dietary Treatment of Obesity
Conclusion: future research should be directed to understanding which diets work better for which patients.
V(ery) L(ow) C(alorie) D(iets)
31 .

32 Wadden: Ann Int Med (1989) 119:688-693
TREATMENT OF OBESITY Diet with Behavior Modification

33
MEDICATIONS FOR THE TREATMENT OF OBESITY HISTORICAL PERSPECTIVE
• 1893-1946 Thyroid Hormone • 1935 Dinitrophenol & Amphetamines • 1950s Norepinephrine analogues (phentermine) • 1973 Serotonin effectors (fenfluramine) • 1980s-90s Dexfenfluramine • 1990s Serotonin/Norepinephrine (sibutramine) • 1990s Lipase inhibitor (orlistat) • 2000 s [Wellbutrin, Topomax, Glucophage,
GLP1 RAs] • 2010s [SGLT2i’s]; Phentermine/Topiramate ER;
Lorcaserin; Bupropion ER/Naltrexone ER; Liraglutide
• Future CCK; B3 Agonists; Gene Therapy; PYY
approved for chronic weight management

Phentermine Use Persists in the Marketplace
34

35
MEDICATIONS FOR OBESITY Orlistat Mechanism of Action
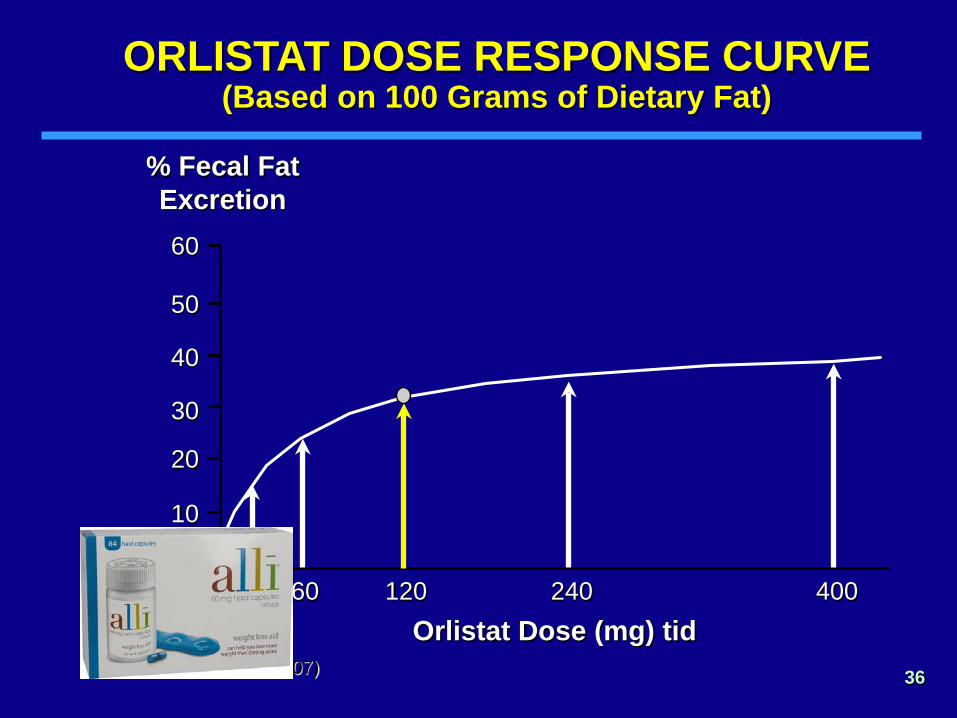
36
ORLISTAT DOSE RESPONSE CURVE (Based on 100 Grams of Dietary Fat)
Data on file. (Ref. 038-007)
% Fecal Fat Excretion
Orlistat Dose (mg) tid 30 120 240 400 60
60
50
40
30
20
10
0

37
-12
-10
-8
-6
-4
-2
0
0 32 48 64 80 104 16 -4
Week
% c
hang
e fro
m in
itial
wei
ght
Placebo/Placebo
120/120
120/60
120/Placebo
Year 2: Eucaloric diet
Year 1: Hypocaloric diet
JAMA, Jan 20, 1999
MEDICATIONS FOR OBESITY Orlistat: Body Weight Change After 2 Years

38
3.9
3.8
3.7
3.6
3.5
3.4
−4 0 24 52 76 104
mmol/L
Week
LDL-cholesterol
p=0.0002
Weight loss
Mildly hypocaloric diet
Eucaloric diet
−4 0 20 40 60 80 104
0
−2
−4
−6
−8
−10
−12
%
Week
Orlistat 120 mg tid Placebo
Lancet (1998) 352:167
MEDICATIONS FOR OBESITY Orlistat: Effect on LDL Cholesterol

39
40
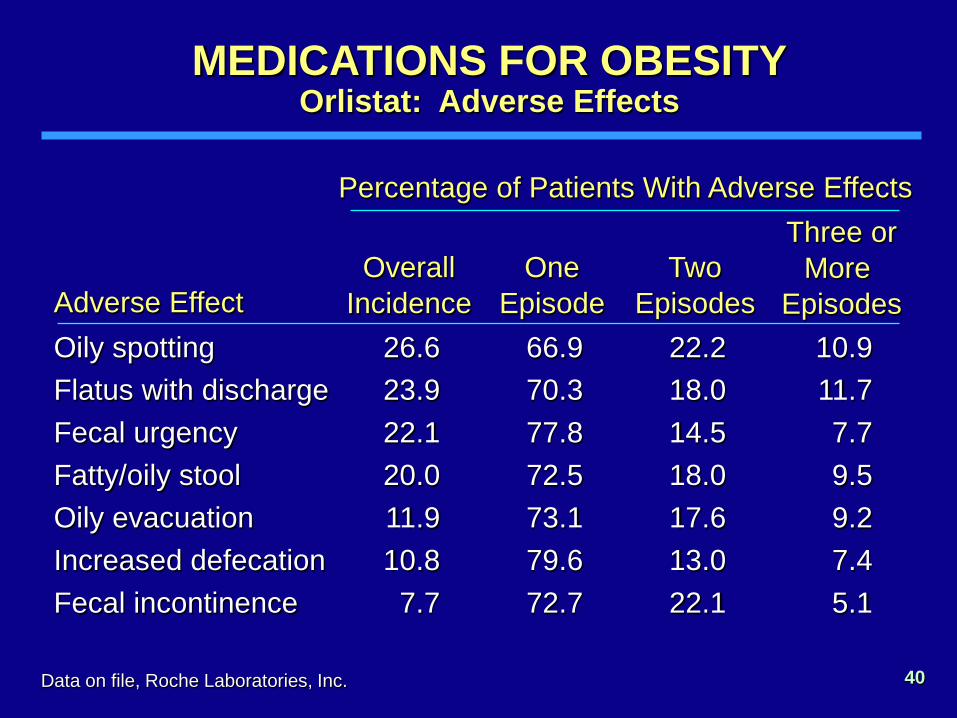
Oily spotting Flatus with discharge Fecal urgency Fatty/oily stool Oily evacuation Increased defecation Fecal incontinence
Adverse Effect 26.6 23.9 22.1 20.0 11.9 10.8
7.7
Overall Incidence
Percentage of Patients With Adverse Effects
Data on file, Roche Laboratories, Inc.
66.9 70.3 77.8 72.5 73.1 79.6 72.7
One Episode
22.2 18.0 14.5 18.0 17.6 13.0 22.1
Two Episodes
10.9 11.7 7.7 9.5 9.2 7.4 5.1
Three or More
Episodes
MEDICATIONS FOR OBESITY Orlistat: Adverse Effects

NEWER MEDICATIONS FOR WEIGHT LOSS COMBINATION PHENTERMINE/TOPIRAMATE
from the PI …
42
Indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management in adults with an initial body mass index (BMI) of 30 kg/m or greater or 27 kg/m2 or greater in the presence of at least one weight-related comorbidity such as hypertension, type 2 diabetes mellitus, or dyslipidemia
• If <3% weight loss after 12 weeks on usual dose, either discontinue medication or advance to maximum dose
• If <5% weight loss after 12 weeks on maximum dose, then discontinue the medication (to discontinue take every other day for one week)
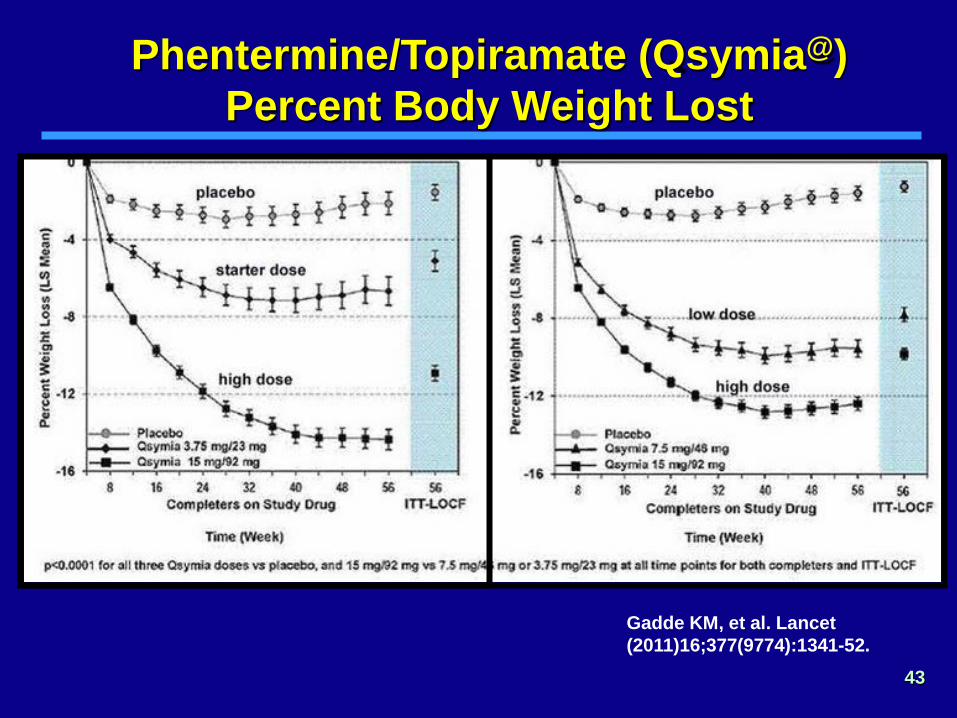
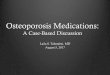
Phentermine/Topiramate (Qsymia@) Percent Body Weight Lost
43
Gadde KM, et al. Lancet (2011)16;377(9774):1341-52.

Phentermine/Topiramate (Qsymia@) CONQUER Study: Weight Loss at 1 Year
Lancet (2011). 377: 1341 - 1352
SEQUEL Extension CONQUER Trial
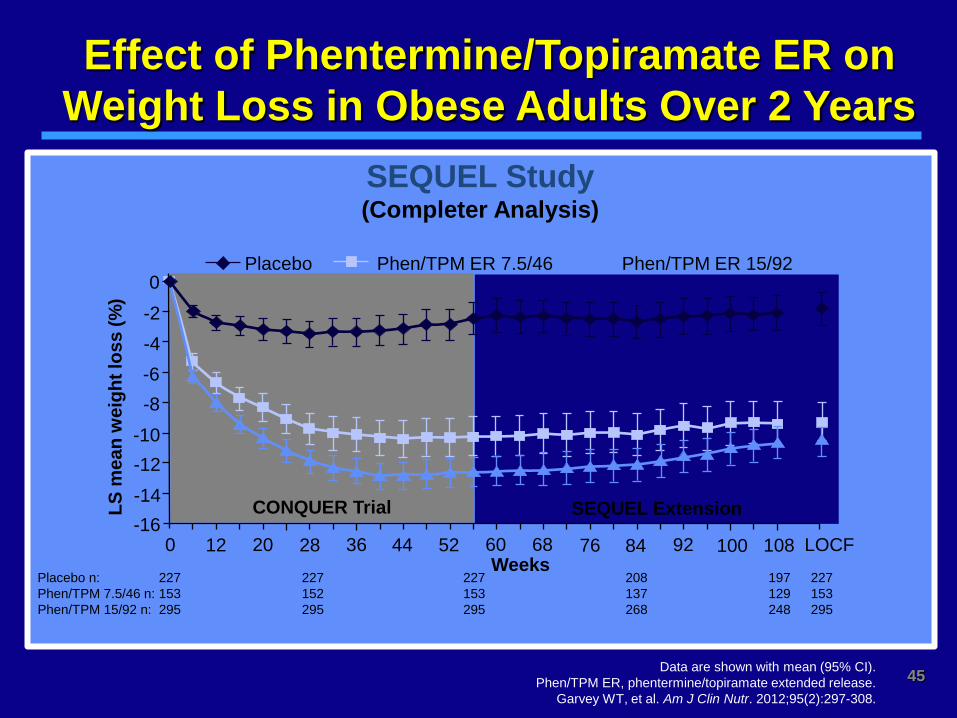
Effect of Phentermine/Topiramate ER on Weight Loss in Obese Adults Over 2 Years
Data are shown with mean (95% CI). Phen/TPM ER, phentermine/topiramate extended release.
Garvey WT, et al. Am J Clin Nutr. 2012;95(2):297-308.
SEQUEL Study (Completer Analysis)
Placebo Phen/TPM ER 7.5/46 Phen/TPM ER 15/92
LS m
ean
wei
ght l
oss
(%)
-2 -4 -6 -8
-10 -12 -14 -16
0 12 20 92
0
Weeks 28 36 44 52 60 68 76 84 100 108 LOCF
Placebo n: 227 227 227 208 197 227 Phen/TPM 7.5/46 n: 153 152 153 137 129 153 Phen/TPM 15/92 n: 295 295 295 268 248 295
45
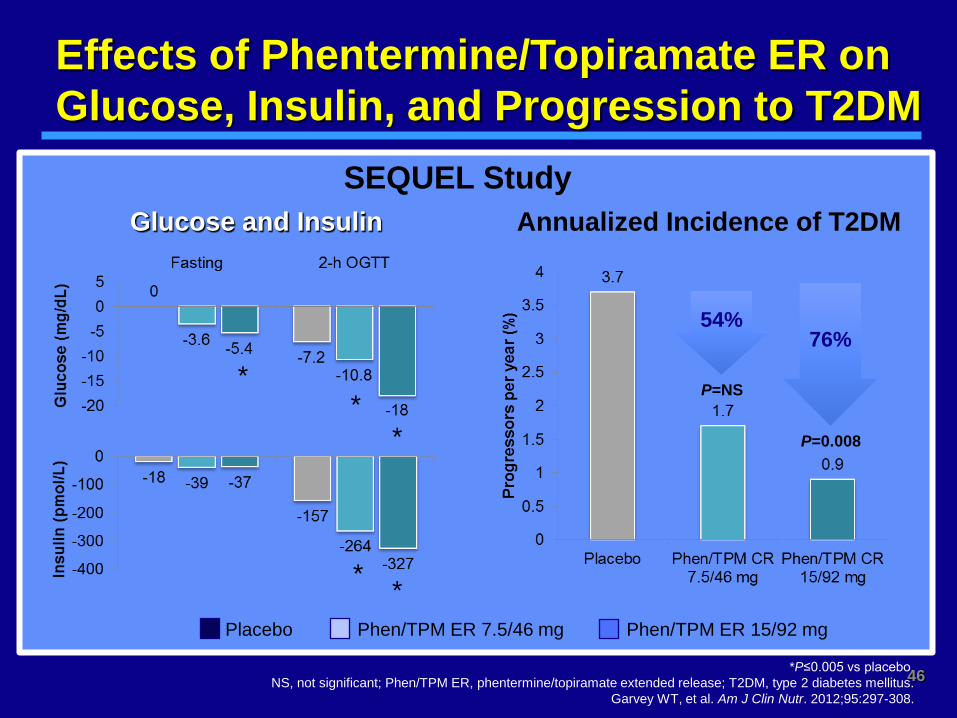
Effects of Phentermine/Topiramate ER on Glucose, Insulin, and Progression to T2DM
Glucose and Insulin
*P≤0.005 vs placebo. NS, not significant; Phen/TPM ER, phentermine/topiramate extended release; T2DM, type 2 diabetes mellitus.
Garvey WT, et al. Am J Clin Nutr. 2012;95:297-308.
* *
* *
*
Placebo Phen/TPM ER 7.5/46 mg Phen/TPM ER 15/92 mg
SEQUEL Study Annualized Incidence of T2DM
P=0.008
76%
P=NS
54%
46
Phentermine/Topiramate (Qsymia@) Adverse Effects
• Increase in heart rate or blood pressure • Dry mouth, dysgeusia, constipation • Insomnia, irritability, anxiety • Disturbances in attention, lack of concentration
• CONTRA-INDICATIONS
— Pregnancy — Glaucoma
47
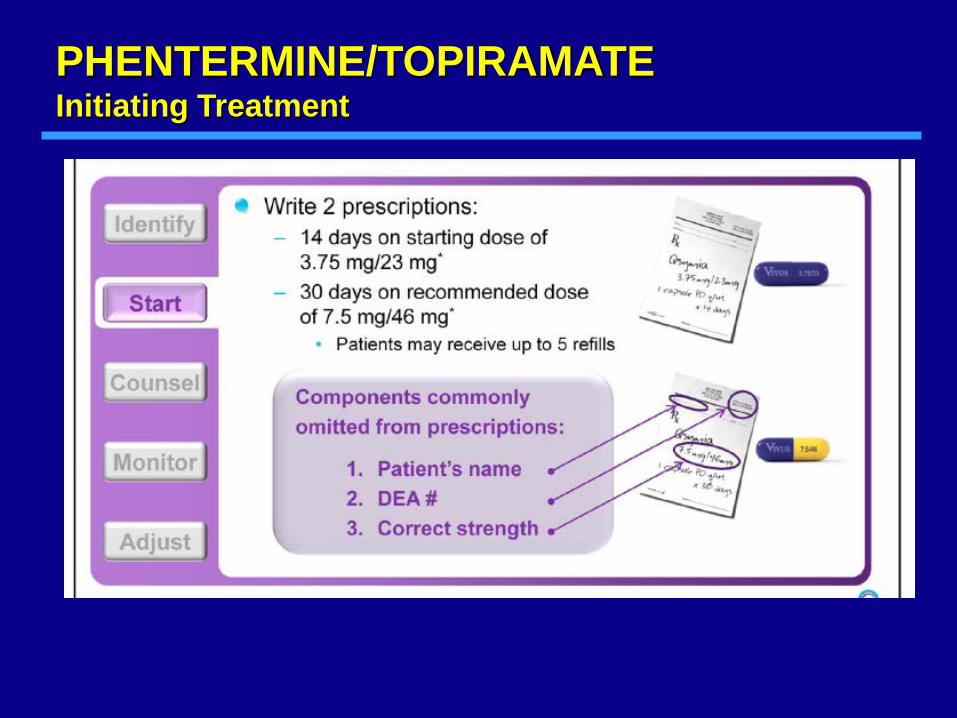
PHENTERMINE/TOPIRAMATE Initiating Treatment
LORCASERIN FOR WEIGHT LOSS
• Lorcaserin (Belviq) is a selective 5-HT2C (Serotonin) Receptor Agonist.
— 5-HT2C receptors are located almost exclusively in the brain in many sites, including the hypothalamus.
• Clinical Use
— Schedule IV Controlled Substance — 10 mg twice daily — Discontinue if 5% weight loss is not achieved within 12
weeks
49

Lorcaserin Adverse Events
Event occurring in ≥5% of patients and more frequently than with placebo, %
Lorcaserin 10 mg BID (N=3195)
Placebo (N=3185)
Headache 16.8 10.1 Upper respiratory tract infection 13.7 12.3
Nasopharyngitis 13.0 12.0
Dizziness 8.5 3.8 Nausea 8.3 5.3 Fatigue 7.2 3.6 Urinary tract infection 6.5 5.4
Diarrhea 6.5 5.6
Back pain 6.3 5.6
Constipation 5.8 3.9 Dry mouth 5.3 2.3
Belviq (lorcaserin HCl) prescribing information. Woodcliff Lake, NJ: Eisai Inc.; 2012.
50

51
Effect of Lorcaserin on Body Weight in Obese Adults Over 2 Years
Smith SR, et al. N Engl J Med. 2010;363:245-256.
BLOOM Study
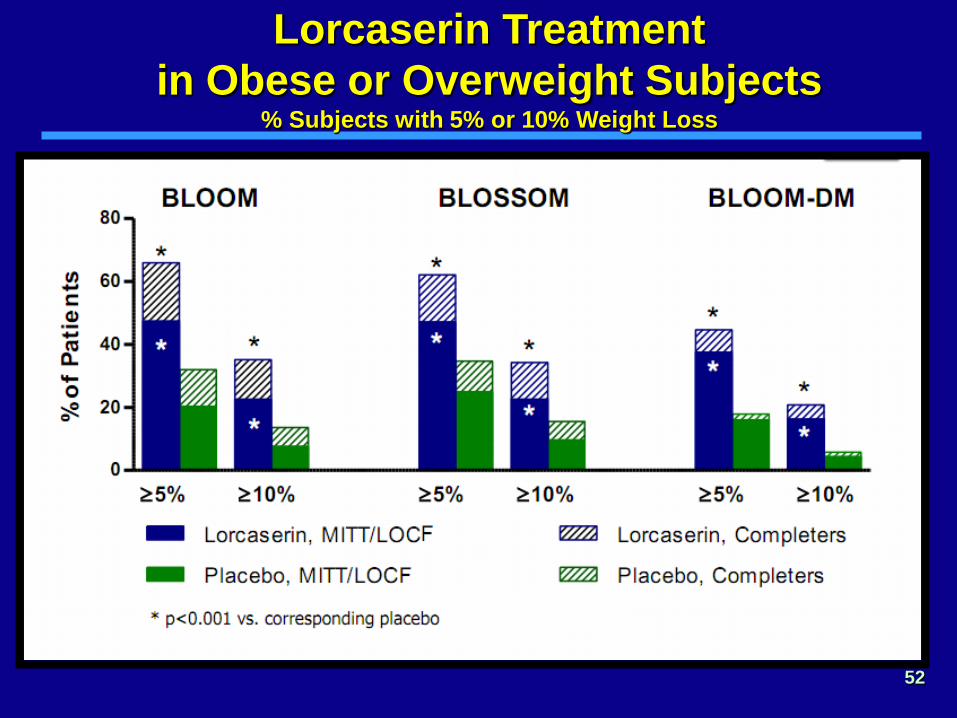
Lorcaserin Treatment in Obese or Overweight Subjects
% Subjects with 5% or 10% Weight Loss
52

Combined Lorcaserin + Phentermine Treatment for Weight Loss
53
NOT FDA APPROVED!
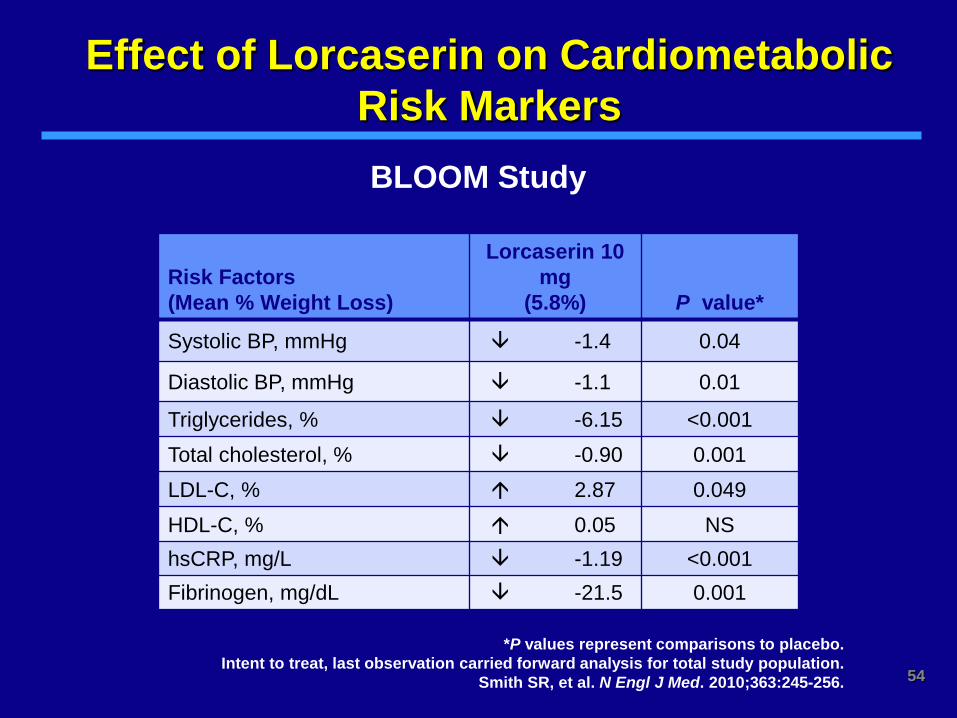
Effect of Lorcaserin on Cardiometabolic Risk Markers
Risk Factors (Mean % Weight Loss)
Lorcaserin 10 mg
(5.8%) P value*
Systolic BP, mmHg -1.4 0.04
Diastolic BP, mmHg -1.1 0.01
Triglycerides, % -6.15 <0.001 Total cholesterol, % -0.90 0.001 LDL-C, % 2.87 0.049 HDL-C, % 0.05 NS hsCRP, mg/L -1.19 <0.001 Fibrinogen, mg/dL -21.5 0.001
*P values represent comparisons to placebo. Intent to treat, last observation carried forward analysis for total study population.
Smith SR, et al. N Engl J Med. 2010;363:245-256.
BLOOM Study
54

Effect of Lorcaserin on Progression to T2DM
55
P=0.003
Patie
nts
with
A1C
≥6.
5% (
%)
Proportion of BLOOM and BLOSSOM Patients With Newly Diagnosed Diabetes After 52 Weeks of Treatment
Lorcaserin hydrochloride briefing document for FDA Advisory Committee. Woodcliff Lake, NJ: Eisai Inc.; 2012. Available at: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM303200.pdf.

Bupropion/Naltrexone (Contrave)
• Bupropion: — stimulates POMC neurons —Has been used for “binge” activities, smoking
cessation • Naltrexone:
— Blocks POMC auto-inhibition —Presumably works at the “hedonistic” centers of
the brain Adverse Effects: -- nausea, constipation -- headache, paresthesias -- dry mouth
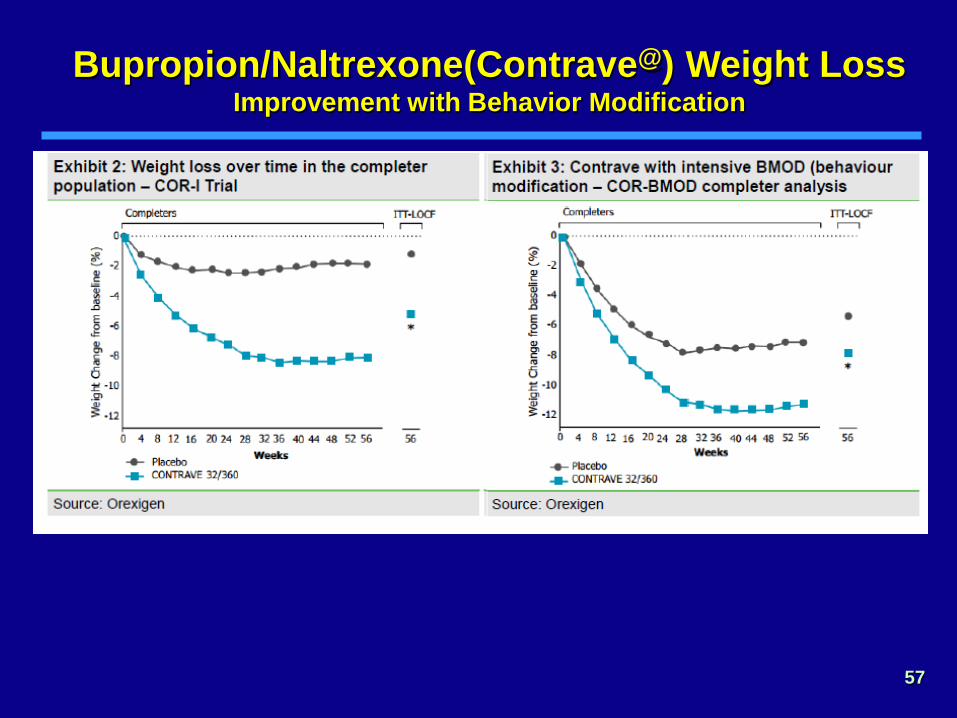
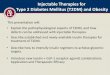
Bupropion/Naltrexone(Contrave@) Weight Loss Improvement with Behavior Modification
57

Bupropion/Naltrexone(Contrave) 5%, 10%, and 15% Weight Loss
Greenway FL, Fujioka K, Plodkowski RA et al.
Lancet. 2010; 376: 595-605
LOCF
COMPLETERS
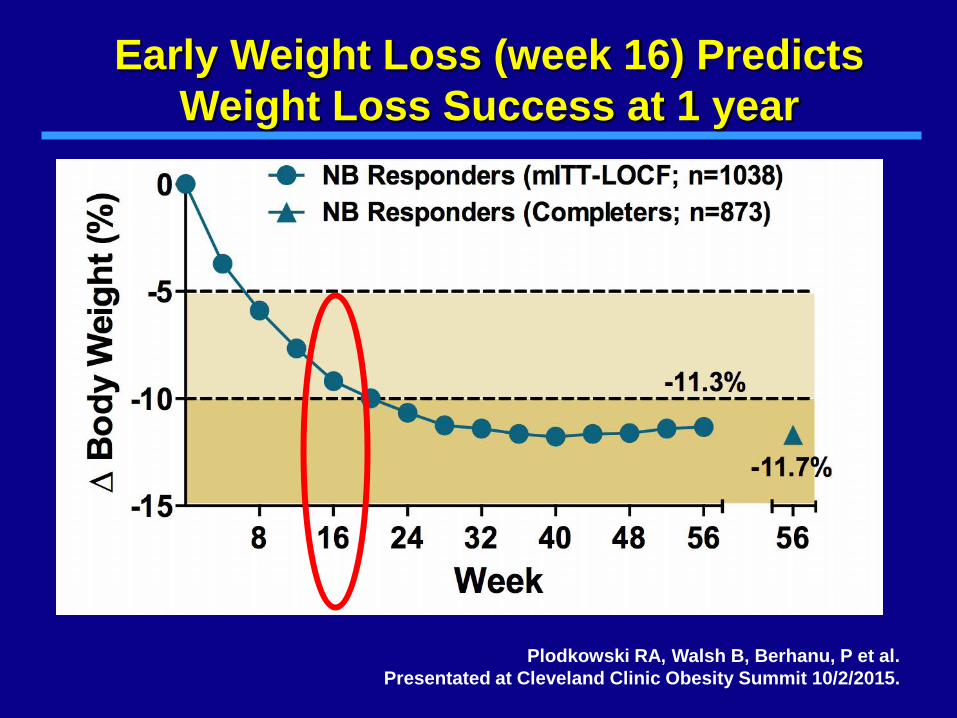
Early Weight Loss (week 16) Predicts Weight Loss Success at 1 year
Plodkowski RA, Walsh B, Berhanu, P et al. Presentated at Cleveland Clinic Obesity Summit 10/2/2015.

VICTOZA AND SAXENDA What’s the Difference?
“VICTOZA” • Liraglutide • Indicated for Type 2 DM • Doses range from 0.6 (starter
dose) to 1.2 to 1.8 mg • Pen contains 3 ml, 6 mg/ml • 2 Pens/month for 1.2 daily,
3 Pens/month for 1.8 daily. • Slows stomach emptying,
reduces appetite, improves pancreatic function
• May cause nausea
“SAXENDA” • Liraglutide • Indicated for Obesity • Doses range from 0.6 (starter
dose) to 1.2, 1.8, 2.4, & 3.0 mg • Pen contains 3 ml, 6 mg/ml • 5 Pens/month for 3.0 daily.
• Slows stomach emptying,
reduces appetite • May cause nausea
60

Weight Loss wtith Liraglutide (Saxenda)
Pi-Sunyer X, Astrup A, Fujioka K et al. NEJM.2015; 373(1):11-22.

Weight Loss with Liraglutide (Saxenda) 5% and 10% Weight Loss
Pi-Sunyer X, Astrup A, Fujioka K et al. NEJM.2015; 373(1):11-22.

Liraglutide After Successful Low Calorie Diet
63 The SCALE Maintenance randomized study.
Int J Obesity. 2013 Nov;37(11):1443-51.
-5.8%
-5.4%
-5.6%

MEDICATIONS FOR CHRONIC WEIGHT MANAGEMENT
Composite of Completer Data
Plodkowski RA, McGarvey ME, Nguyen QT et al. Federal Practitioner. In press Jan 2015.

Combined Lifestyle Intervention and Pharmacotherapy
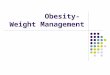
65 Wadden TA, et al. N Engl J Med. 2005;353:2111-2120.
Wei
ght l
oss
(kg)
2
4
6
8
10
12
14
16 0 3 6 10 18 40 52
0
Weeks
Drug alone Extensive lifestyle modification alone Drug + brief lifestyle counseling Drug + extensive lifestyle modification
66
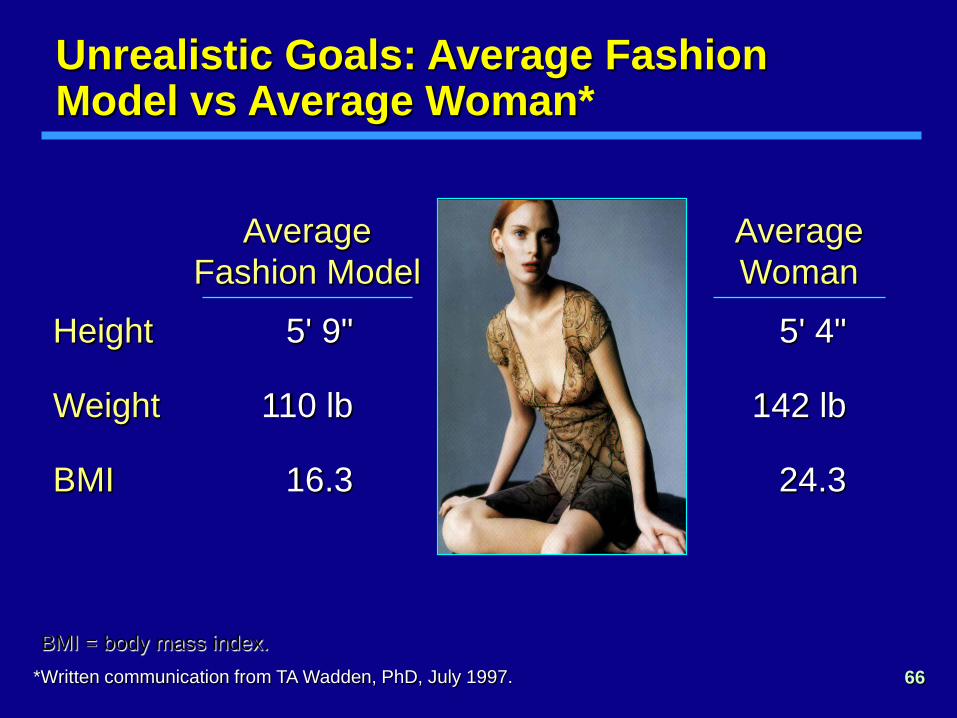
Unrealistic Goals: Average Fashion Model vs Average Woman*
BMI = body mass index.
Height
Weight
BMI
5' 4"
142 lb
24.3
Average Woman
*Written communication from TA Wadden, PhD, July 1997.
Average Fashion Model
5' 9"
110 lb
16.3
67
• Each kg of weight loss
— lowers blood pressure by 2.5/1.7 mm Hg
— lowers total cholesterol by 1.93 mg/dl
— lowers LDL cholesterol by 0.77 mg/dl
— lowers triglycerides by 1.33 mg/dl
— increases survival in Type 2 diabetes by 3 - 4 months
Benefits of Modest Weight Loss in Patients With Hypertension, Hyperlipidemia and Diabetes
Schotte et al. Arch Intern Med. 1990;150:1701-1704. Dattilo et al. Am J Clin Nutr. 1992;56:320-328 Seim et al. Fam Pract Res J. 1992;12:411-419. Lean et al. Diabet Med. 1989;7:228-233 Wing et al. Arch Intern Med. 1987;147:1749-1753.

68
GOAL WEIGHT IN THE TREATMENT OF OBESITY

TREATING OBESITY IN YOUR PRACTICE
• With the increase in obesity and co-morbid conditions, obese patients need access to quality care
• Small differences in approach and attitude related to weight and weight loss can have a huge impact
• The treatment of obesity can be easily integrated into any primary care setting.
• Increase your communication with patients who are obese and take aggressive steps to treat this serious disease.