Embed Size (px)
Citation preview
J7ournal ofNeurology, Neurosurgery, and Psychiatry 1996;61:47-51
The A to G transition at nt 3243 of themitochondrial tRNALeu(uuR) may cause an MERRFsyndrome
Gian Maria Fabrizi, Elena Cardaioli, Gaetano Salvatore Grieco, Tiziana Cavallaro,Alessandro Malandrini, Letizia Manneschi, Maria Teresa Dotti, Antonio Federico,Giancarlo Guazzi
Istituto di ScienzeNeurologiche,Universita di Siena,ItalyG M FabriziE CardaioliG S GriecoA MalandriniL ManneschiM T DottiA FedericoG GuazziIstituto di Neurologia,Universita di Verona,ItalyT CavallaroCorrespondence to:Dr G M Fabrizi, Istituto diScienze Neurologiche,Universiti di Siena, VialeBracci, 53100 Siena, Italy.Received 31 October 1995and in final revised form19 February 1996Accepted 23 February 1996
AbstractObjective-To verify the phenotype togenotype correlations of mitochondrialDNA (mtDNA) related disorders in anatypical maternally inherited encephalo-myopathy.Methods-Neuroradiological, morpholog-ical, biochemical, and molecular geneticanalyses were performed on the affectedmembers of a pedigree harbouring theheteroplasmic A to G transition atnucleotide 3243 of the mitochondrialtRNAI-u(UR), which is usually associatedwith the syndrome of mitochondrialencephalomyopathy, lactic acidosis, andstroke-like episodes (MELAS).Results-The proband was affected by afullblown syndrome of myoclonicepilepsy with ragged red fibres(MERRF), severe brain atrophy, andbasal ganglia calcifications, without theMRI T2 hyperintense focal lesions whichare pathognomonic of MELAS. Oligo-symptomatic relatives were variablyaffected by lipomas, goitre, brain atro-phy, and basal ganglia calcifications.Muscle biopsies in the proband and hismother showed a MELAS-like patternwith cytochrome c oxidase hyperreactiveragged red fibres and strongly succinatedehydrogenase reactive vessels.Quantification of the A3243G mutationdisclosed 78% and 70% of mutatedmtDNA in the muscle of the severelyaffected proband and of his oligosympto-matic mother respectively. Nucleotidesequencing of the mitochondrialtRNAIeu(UUR) and tRNALYs in the proband'smuscle failed to show any additionalnucleotide change which could accountfor the clinical oddity of this pedigree bymodulating the expression of the primarypathogenic mutation.Conclusion-So far, MERRF has beenassociated with mutations of themitochondrial tRNALYS, and MELAS withmutations of the mitochondrialtRNALeu(UuR). Now MERRF may also beconsidered among the clinical syndromesassociated with the A to G transition at nt3243 of the tRNALeu(uuR).
(7 Neurol Neurosurg Psychiatry 1996;61:45-5 1)
Keywords: MERRF; MELAS; mitochondrial DNA
Two distinct maternally inherited encephalo-myopathies with ragged red fibres have beenrecognised on clinical grounds: MERRF,which is characterised by myoclonic epilepsy,skeletal myopathy, neural deafness, and opticatrophy,' and MELAS, which is defined bystroke-like episodes in young age, episodicheadache and vomiting, seizures, dementia,lactic acidosis, skeletal myopathy, and shortstature.2 Molecular genetic studies later con-firmed the nosological distinction between thetwo disorders, showing that MERRF is strictlyassociated with two mutations of the mito-chondrial tRNALYs at nucleotides 83443 and8356,4 and MELAS with three point muta-tions of the mitochondrial tRNAIxu(UUR) atnucleotides 3243, 3271, and 3291; the 3243 Ato G transition (A3243G) is the most commoncause ofMELAS.5We discuss here the clinical, neuroradiolog-
ical, morphological, biochemical, and molecu-lar genetic findings in the affected members ofa clinically atypical pedigree harbouring theheteroplasmic A3243G "MELAS" mutation.
Patients and methodsPEDIGREE ANALYSISFamily member III-1 probandThe proband, an 18 year old man, was thefirstborn of non-consanguineous parents (fig1). Since the age of 5 years, he had had
I
Figure 1 Pedigree: black symbol indicates the severelyaffected proband; grey symbols indicate theoligosymptomatic members. Percentage of the mutatedmtDNA in muscle is given as m; percentage of the mutatedmtDNA in blood is given as b.
47 on D
ecember 11, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.1.47 on 1 July 1996. D
ownloaded from
Fabrizi, Cardaioli, Grieco, Cavallaro, Malandrini, Manneschi, et al
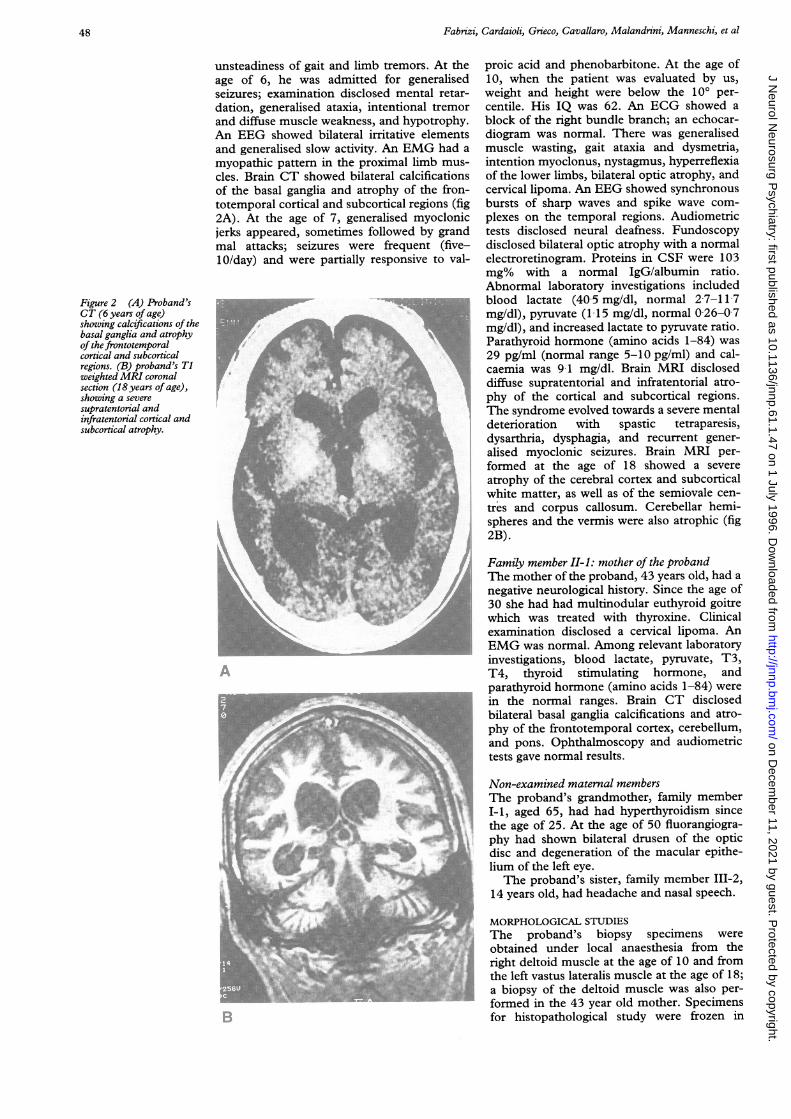
unsteadiness of gait and limb tremors. At theage of 6, he was admitted for generalisedseizures; examination disclosed mental retar-dation, generalised ataxia, intentional tremorand diffuse muscle weakness, and hypotrophy.An EEG showed bilateral irritative elementsand generalised slow activity. An EMG had amyopathic pattern in the proximal limb mus-cles. Brain CT showed bilateral calcificationsof the basal ganglia and atrophy of the fron-totemporal cortical and subcortical regions (fig2A). At the age of 7, generalised myoclonicjerks appeared, sometimes followed by grandmal attacks; seizures were frequent (five-10/day) and were partially responsive to val-
Figure 2 (A) Proband'sCT (6 years of age)showing calcifications of thebasal ganglia and atrophyof the frontotemporalcortical and subcorticalregions. (B) proband's Tiweighted MRI coronalsection (18 years of age),showing a severesupratentorial andinfratentorial cortical andsubcortical atrophy.
proic acid and phenobarbitone. At the age of10, when the patient was evaluated by us,weight and height were below the 100 per-centile. His IQ was 62. An ECG showed ablock of the right bundle branch; an echocar-diogram was normal. There was generalisedmuscle wasting, gait ataxia and dysmetria,intention myoclonus, nystagmus, hyperreflexiaof the lower limbs, bilateral optic atrophy, andcervical lipoma. An EEG showed synchronousbursts of sharp waves and spike wave com-plexes on the temporal regions. Audiometrictests disclosed neural deafness. Fundoscopydisclosed bilateral optic atrophy with a normalelectroretinogram. Proteins in CSF were 103mg% with a normal IgG/albumin ratio.Abnormal laboratory investigations includedblood lactate (405 mg/dl, normal 2 7-11 7mg/dl), pyruvate (115 mg/dl, normal 026-07mg/dl), and increased lactate to pyruvate ratio.Parathyroid hormone (amino acids 1-84) was29 pg/ml (normal range 5-10 pg/ml) and cal-caemia was 9-1 mg/dl. Brain MRI discloseddiffuse supratentorial and infratentorial atro-phy of the cortical and subcortical regions.The syndrome evolved towards a severe mentaldeterioration with spastic tetraparesis,dysarthria, dysphagia, and recurrent gener-alised myoclonic seizures. Brain MRI per-formed at the age of 18 showed a severeatrophy of the cerebral cortex and subcorticalwhite matter, as well as of the semiovale cen-tres and corpus callosum. Cerebellar hemi-spheres and the vermis were also atrophic (fig2B).
Family member II-1: mother of the probandThe mother of the proband, 43 years old, had anegative neurological history. Since the age of30 she had had multinodular euthyroid goitrewhich was treated with thyroxine. Clinicalexamination disclosed a cervical lipoma. AnEMG was normal. Among relevant laboratoryinvestigations, blood lactate, pyruvate, T3,T4, thyroid stimulating hormone, andparathyroid hormone (amino acids 1-84) werein the normal ranges. Brain CT disclosedbilateral basal ganglia calcifications and atro-phy of the frontotemporal cortex, cerebellum,and pons. Ophthalmoscopy and audiometrictests gave normal results.
Non-examined maternal membersThe proband's grandmother, family memberI-1, aged 65, had had hyperthyroidism sincethe age of 25. At the age of 50 fluorangiogra-phy had shown bilateral drusen of the opticdisc and degeneration of the macular epithe-lium of the left eye.The proband's sister, family member 111-2,
14 years old, had headache and nasal speech.
's MORPHOLOGICAL STUDIESThe proband's biopsy specimens wereobtained under local anaesthesia from theright deltoid muscle at the age of 10 and fromthe left vastus lateralis muscle at the age of 18;a biopsy of the deltoid muscle was also per-formed in the 43 year old mother. Specimensfor histopathological study were frozen in
48
.:..i..
'A.
"'
rX
on Decem
ber 11, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.61.1.47 on 1 July 1996. Dow
nloaded from

The A to G transition at nt 3243 of the mitochondrial tRNA'-LtU-RI may cause a MERRF syndrome
Figure 3 ModifiedGomori trichrome stain(A x 140) andcytochrome c oxidasereaction (B x 140) in themother's deltoid mnuscle;asterisks indicate thecorrespondingfibres inserial sections. Ragged redfibres have a strongcytochrome c oxidaseactivity which is moreintense at the periphery.(C) Succinatedehydrogenase stainling onthe proband's second musclebiopsy (x 175) shows asmall artery with denselystained granules in its wall.(D) Electronmicrographyof the proband's secondmtiuscle biopsy, showsaggregates ofi.ntermyofibrillarmitochondria containingparacrystalline inclusions( x 4200).
/I
* \ . \ t.. , .. ,. te,. . s , : .0. V, 0 _ *;v _* X ., .) iM-- w it;; ¢ /e';
_ 4 * ie.
faU'... :A ,,Or_ ) . ; 8* < t8; 2 . '. ,rt ; A _; S . + X 9.X,ttt; 0S4 A; i 4\$S ! ! ;i .j.l,
isopentane cooled with liquid nitrogen. Serial8 pum thick transverse sections were stainedwith haematoxylin and eosin, modifiedGomori trichrome, and a battery of histo-chemical methods including succinate dehy-drogenase, routine ATPase, ATPase withpreincubation at pH 4,6 and 43, andcytochrome c oxidase. Small pieces of thespecimens were fixed in 2-5% glutaraldehydeand postfixed in 1% 0S04 in 01- M phosphatebuffer. After fixation the specimens were dehy-drated and embedded in epoxy resin for elec-tron microscopy
BIOCHEMICAL STUDIESThe mitochondrial fraction was isolated from200-300 mg of frozen muscle samples fromfamily members III-1 and II-1 and the activi-ties of the following respiratory chain enzymeswere determined spectrophotometrically aspreviously described6: NADH cytochrome creductase, succinate cytochrome c reductase,and cytochrome c oxidase. Values wereexpressed as ratios with citrate synthase, anenzyme of the mitochondrial matrix that is areliable index of mitochondrial protein con-tent.
MOLECULAR GENETIC ANALYSISTotal DNA was extracted from blood of familymembers III-1, II-1, and I-1 and from 50 mgof frozen bioptic muscle of members III-1 andII-1, according to standard procedures. Thepresence of the following pathogenic pointmutations of mtDNA were investigated on theproband's muscle mtDNA, by standardRFLP-PCR (polymerase chain reaction)analysis: MERRF A8344G and T8356C atthe tRNALYS; MELAS A3243G, T3271C,T3291C at the tRNALcu(UUR); MELAS T9957Cat the COXIII gene; and NARP (neurogenicataxia and retinitis pigmentosa) T8993G atthe ATPase6 gene.
Quantification of the A3243G mutation inblood from I-1, II-1, and III-1 and musclefrom HI-1 and I-1 was obtained by a routineApaI-RFLP analysis on the PCR amplifiedmitochondrial tRNAIU(ULUR), modified accord-ing to Tanno et a17 to reduce the underestima-tion of mutated mtDNA caused by theformation of heteroduplexes. Direct sequenc-ing of both strands of the mitochondrialtRNAI-eu(UUR) and tRNALys was performed onpolymerase chain reaction (PCR) amplifiedfragments corresponding to nucleotides
49
%;r A.lp
0
.E I '.I
on Decem
ber 11, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.61.1.47 on 1 July 1996. Dow
nloaded from

Fabrizi, Cardaioli, Grieco, Cavallaro, Malandrini, Manneschi, et al
Respiratory chai'n enzyme activities in skeletal mluscle mitochontdria
NADH Succiniatecytochromle cytochronie Cytochrortie Citr-atec reductase c reductase c oxidase sywthase
Pedigree nmemibersIII-1 0 15 0 10 0Q49 719II-1 019 013 062 946controls (n = 50) 0-24 (0 08) 0 19 (0 09) 1.2 (0 45) 690 (229)mean (SD)
Values are nmol/min/mg of mitochondrial proteins.
3150-3369 for the tRNAL' LUU3R) and nucleo-tides 8184-8478 for the tRNA"-S, using the"Sequenase PCR product sequencing kit"(Amersham).
ResultsMORPHOLOGICAL FINDINGS IN SKELETAL
MUSCLE BIOPSIES
The proband's first muscle biopsy (deltoid)showed 8%-10% of ragged red fibres. In thesecond biopsy (vastus lateralis), ragged redfibres were reduced to 1%-2%, but in many
fibres the succinate dehydrogenase stainingwas stronger than that of normal fibres. Theoligosymptomatic mother's muscle biopsyshowed 8%-10% of ragged red fibres. Type Ifibres were preferentially involved in mito-chondrial proliferation. Some ragged red fibreswere completely deficient in cytochrome c oxi-
dase, but most showed cytochrome c oxidasehyperreactivity, which was more evident in theperiphery of the fibres (fig 3 A,B). Blood ves-
sels stained darkly with succinate dehydroge-nase (fig 3C), and were hyperreactive to
cytochrome c oxidase. Ultrastructural exami-nation showed intermyofibrillar and sub-sarcolemmal aggregates of abnormalmitochondria containing paracrystalline inclu-sions (fig 3D). An increased number of mito-chondria were also present in the pericytes ofcapillaries, endothelial cells, and smooth mus-
cle cells of the small arteries.
Figure 4 Autoradiogramti ofPCR products after digestion with Apa I. M anid B indicatemtiuscle and blood of the examined pedigree mnembers. Wild type mitDNA corresponds to the428 bpfragment, which is resolved inzto two fragments of 315 and 113 bp wheni theA3243G mutation is present. A small percentage (5%) of mutant DNA present in bloodfrom I-1 is not visible on the photographic reproduction.
ACTIVITIES OF RESPIRATORY CHAIN ENZYMES
Biochemical analysis on the mitochondrialfraction (table) showed a significant decreaseof the activities of the NADH cytochrome creductase (complexes I + III) and cytochrome coxidase (complex IV) in the skeletal muscle ofthe proband III-1. Values in the mother'smuscle were in the normal range.
MOLECULAR ANALYSIS OF MITOCHONDRIALDNAPCR-RFLP analysis with Apa I showed theheteroplasmic A to G transition at nt 3243 ofthe mitochondrial tRNA'uUUR) in the pro-band's muscle. Quantitative analysis (fig 4)showed that the percentage of the mutatedDNA in muscle was 78% in the severelyaffected proband and 70% in the oligosympto-matic mother. Percentages of mutated DNAin blood were 30%, 20%, and 5% in theproband, mother, and grandmother respec-tively.
Direct nucleotide sequencing of theproband's muscle mtDNA confirmed thepresence of the heteroplasmic A3243G muta-tion and failed to show any other nucleotidechange of the tRNA' ''-'I and tRNA'.
DiscussionThe present pedigree harboured the hetero-plasmic A to G transition at nucleotide 3243of the mtDNA, which is typical of MELAS,although the proband was affected by a full-blown MERRF. The syndrome was charac-terised by seizures, intention myoclonus,ataxia, psychomotor delay, optic atrophy,neural deafness, and cervical lipoma, withoutany sign or symptom of stroke episodes. Adetailed CT and MRI follow up disclosedbasal ganglia calcifications and severe, pro-gressive atrophy of the cortex, subcorticalwhite matter, corpus callosum, and semiovalecentres. Two MRIs, performed at differentstages of disease, did not show the T2 hyperin-tense focal lesions which are pathognomonicof MELAS.5 Basal ganglia calcifications,although often encountered in MELAS, maybe found in various mitochondrial encephalo-myopathies, and they are not specific for thedisease.' The A3243G mutation was firstdescribed in MELAS, but it may also occur inassociation with other two syndromes: chronicprogressive external ophthalmoplegia andmaternally inherited diabetes with deafness.') I"
The same mutation has been also identified ina few cases of MERRF/MELAS overlap." Inthese cases, myoclonus or ataxia were alwaysassociated with clinical or radiological evi-dence of stroke-like episodes. More recently,the A3243G mutation was found in a MERRFpedigree,'5 but the occurrence of focal cerebrallesions could not be ruled out in the reportbecause of the absence of MRI studies.
Clinical findings in the oligosymptomaticmembers of the pedigree also showed atypicalfeatures. The proband's mother had cervicallipoma, euthyroid goitre, basal ganglia calcifi-cations, and atrophy of the frontotemporal
50 on D
ecember 11, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.1.47 on 1 July 1996. D
ownloaded from

The A to G transition at nt 3243 of the mitochondrial tRNA'- UUR may cause a MERRF syndromne
cortex and cerebellum. The grandmother hadretinopathy and hyperthyroidism. So far, lipo-mas have been related to the A to G transitionat nt 8344 of the tRNALs,l7 in associationwith MERRF or with Ekbom's syndrome(MERRF plus lipomas, ataxia, and neuropa-thy), as well as to the autosomal dominantmultiple deletions of the mtDNA." Thyroiddysfunction has been reported in a MERRFcase4 and in a MERRF/MELAS pedigree,'"both associated with a T to C transition at nt8356 of the tRNA'-s. We conclude that lipo-mas and thyroid dysfunction occur in a widerange of molecular lesions of the mtDNA andthey are not specific of any syndrome.
Unlike the clinical phenotype, the morpho-logical abnormalities in muscle followed thepattern seen with the A3243G mutation,which is characterised by ragged red fibreshyperreactive to cytochrome c oxidase andvessels strongly reactive to succinate dehydro-genase.2'
Quantification of the A3243G mutationshowed 78% of mutated muscle mtDNA inthe proband and 70% in the oligosymptomaticmother. Percentages of mutated mtDNA inblood were 30%, 20%, and 5% in theproband, mother, and grandmother respec-tively. Recent surveys showed that the per-centages of the A3243G mutation did notcorrelate with the expression of specificclinical syndromes, although, in the MELASsubgroup, the percentage of mutated mtDNAcorrelated positively with the age of onset ofdisease.9 1" To explain these imperfect cor-relations, additional genetic factors involvingthe mtDNA or the nuclear genome have beenhypothesised to modulate the expression ofthe primary pathogenic mutations of mtDNA.9Nucleotide sequence analysis of the proband'smuscle mtDNA did not show any additionalnucleotide change of the tRNAL-\s andtRNAI'u(UUR), which represent two genetic hotspots in maternally inherited syndromes.2' Wealso excluded the T9957C mutation at thegene for subunit III of cytochrome c oxidasewhich has been recently reported in MELAS.22
In conclusion, the presented pedigreechallenges the known correlations between theclinical phenotype and the genotype of themtDNA related disorders, and it indicates thata pure MERRF syndrome must be actuallyconsidered as a possible phenotype of theA3243G mutation at the tRNAl-u(UUR). Furthermolecular genetic studies are needed to dis-close other alterations of the mtDNA whichcould account for the clinical oddity of thedescribed pedigree.
The financial support of Telethon-Italy is gratefully aknowl-edged (grants to GCG, AF, and GMF).
1 Fukuhara N, Tokiguchi S, Shirakawa K, Tsubaki T.Myoclonus epilepsy associated with ragged-red fibers(mitochondrial abnormalities): disease entity or a syn-drome? Light- and electron-microscopic studies of twocases and review of literature. J Neurol Sci 1980;47:117-33.
2 Pavlakis SG, Phillips PC, DiMauro S, DeVivo DC,Rowland LP. Mitochondrial myopathy, encephalopathy,lactic acidosis, and stroke-like episodes. Ann Neurol1984;16:481-8.
3 Shoffner JM, Lott MT, Lezza AM, Seibel P, Ballinger SW,Wallace DC. Myoclonic epilepsy and ragged-red fiberdisease (MERRF) is associated with a mitochondrialDNA tRNALys mutation. Cell 1991,61:931-7.
4 Silvestri G, Moraes CT, Shanske S, Oh SJ, DiMauro S. Anew mtDNA mutation in the tRNALys gene associatedwith myoclonic epilepsy and ragged-red fibers(MERRF). Am J Husn Genet 1992;51:1213-7.
5 Goto Y. Clinical features of MELAS and mitochondrialDNA mutations. Muscle Nerve 1995;3(suppl): 107-12.
6 Federico A, Manneschi L, Paolimi E. Biochemical differ-ences between intermyofibrillar and subsarcolemmalmitochondria from human muscle. _7 Inherit Metab Dis1987;1O(suppl):242-6.
7 Tanno Y, Yoneda M, Nonaka I, Tanaka K, Miyatake T,Tsuji S. Quantitation of mitochondrial DNA carrying thetRNALys mutation in MERRF patients. Biochenm BiophysRes Commun 199 1;179:880-5.
8 Matthews PM, Phil D, Tampieri D, et al. Magnetic reso-nance imaging shows specific abnormalities in theMELAS syndrome. Neurology 1991 ;41:1043-6.
9 Hammans SR, Sweeney MG, Hanna MG, Brockington M,Morgan-Hughes JA, Harding AE. The mitochondrialDNA transfer RNALeu(UUR) A to G (3243) mutation.A clinical and genetic study. Brain 1995;118:721-34.
10 Mariotti C, Savarese N, Soumalainen A, et al. Genotype tophenotype correlations in mitochondrial encephalomy-opathies associated with the A3243G mutation of mito-chondrial DNA.
_Neurol 1995;242:304-12.
11 Ciafaloni E, Ricci E, Shanske S, et al. MELAS: clinical fea-tures, biochemistry, and molecular genetics. Anni Neurol1992;31:391-8.
12 Hirano M, Ricci E, Koenigsberg MR, et al. MELAS:an original case and clinical criteria for diagnosis.Neuromuscul Disord 1992;2: 125-35.
13 Chen R-S, Huang C-C, Lee C-C, et al. Overlapping syn-drome of MERRF and MELAS: molecular and neurora-diological studies. Acta Neurol Scand 1993;8:494-8.
14 Crimmins D, Morris JCL, Walker GL, et al. Mitochondrialencephalomyopathy: variable clinical expression within asingle kindred. _7 Neurol Neurosurg Psyzchiatry 199356:900-5.
15 Folgero T, Torbergsen T, 0ian P. The 3243 MELASmutation in a pedigree with MERRF. Eur Neurol 1995;35:168-71.
16 Larsson N-G, Tulinius MH, Holme E, Oldfors A.Pathogenetic aspects of the A8344G mutation of mito-chondrial DNA associated with MERRF syndrome andmultiple lipomas. Muscle Nerve 1995;3(suppl): 102-6.
17 Calabresi P, Silvestri G, DiMauro S, Criggs C. Ekbom'ssyndrome: lipomas, ataxia, and neuropathy withMERRF. Musclk Nerve 1994;17:943-5.
18 Ciafaloni E, Shanske S, Apostolski S, et al. Multiple dele-tions of mitochondrial DNA. Neurology 1991 ;41(suppl) :207.
19 Zeviani M, Muntoni F, Savarese N, et al. A MERRF/MELAS overlap syndrome associated with a new pointmutation in the mitochondrial DNA tRNA'' gene. Eur]_Humn Genet 1992;1:80-7.
20 Moraes CT, Ricci E, Bonilla E, DiMauro S, Schon EA.The mitochondrial tRNALeu(UUR) mutation in mito-chondrial encephalomyopathy, lactic acidosis, andstroke-like episodes (MELAS): genetic, biochemical, andmorphological correlations in skeletal muscle. Am 7 HumGenet 1992;50:934-49.
21 Moraes CT, Ciacci F, Bonilla E, et al. Two novel patho-genic mitochondrial DNA mutations affecting organellenumber and protein synthesis. Is the tRNALeu(UUR)gene an etiologic hot spot? _7 Clin Invest 1993;92:2906-15.
22 Manfredi G, Schon EA, Moraes CT, et al. New mutationassociated with MELAS is located in a mitochondrialDNA polypeptide-coding gene. N"euromuscul Disord 1995;5:391-8.
51 on D
ecember 11, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.1.47 on 1 July 1996. D
ownloaded from





























