Embed Size (px)
Citation preview

The 4Kscore® Test Accurately Identifies Risk for Aggressive Prostate Cancer
and Reduces Unnecessary Prostate Biopsies (April 2017)
Prepared by:
BioReference Laboratories, Inc. An OPKO Health, Inc. Company
481 Edward H. Ross Drive Elmwood Park, New Jersey 07407
http://bioreference.com

2
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
TableofContents
ExecutiveSummary.................................................................................................................3
IntendedUseandTargetPopulation.................................................................................5
ClinicalScenario........................................................................................................................5CurrentStandardofCare.................................................................................................................5PublicHealthImportance................................................................................................................6ThresholdPSAValueof1.5ng/mLforFurtherEvaluation.................................................7
EvidenceSupportingtheIntendedUseofthe4KscoreTest......................................8AnalyticalValidityofthe4KscoreTest.......................................................................................8ClinicalValidityintheDecisiontoPerformProstateBiopsy.............................................9ClinicalUtilityintheDecisiontoPerformaProstateBiopsy..........................................12ClinicalUtilitybyDecisionCurveAnalysis(DCA)................................................................13ReviewsinMedicalLiterature....................................................................................................14
IndependentRecommendationsandGuidelines.......................................................15NCCNGuidelinesforProstateCancerEarlyDetection.......................................................15EuropeanAssociationofUrology(EAU)ProstateCancerGuidelines...........................16
RegulationandCPTCode....................................................................................................16FederalLaboratoryRegulation..................................................................................................16StatePermits.....................................................................................................................................16LaboratoryAccreditation.............................................................................................................174KscoreTestCategoryICPTCode.............................................................................................17
Discussion................................................................................................................................17Developmentofthe4KscoreTest..............................................................................................17TheAbilityofthe4KscoreTesttoPredicttheRiskofDistantMetastasis..................18
Conclusions..............................................................................................................................19
References................................................................................................................................21

3
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
ExecutiveSummary
Widespreadscreeningforprostatecancerwiththeprostate‐specificantigen(PSA)testbeganintheUnitedStatesinthelate1980s,andsubsequentlya45%declineinprostatecancermortalityhasbeenobserved.OwingtothelowspecificityofPSA,unnecessaryprostatebiopsiesandovertreatmentofindolentcancerhaveledtosignificantmorbidityandharm.Prostatebiopsyisapainfulprocedureassociatedwithupto4%ofmenexperiencingsignificantcomplicationssuchasbleeding,infectionandbacterialsepsis.Prostatebiopsycanalsoleadtoovertreatmentofindolent(Gleasonscore6)prostatecancerwithsurgeryorradiationtherapy.
AsaresultofthisandthefailureofaU.S.randomizedclinicalstudyofPSAscreeningtodemonstratebenefit,theUnitedStatesPreventativeServicesTaskForce(USPSTF)in2012advisedagainstroutinePSAscreeningforprostatecancer.Consequently,fewernumbersofmenarebeingscreenedanddiagnosed,butproportionallymoremenarebeingdiagnosedwithmoreadvanceddisease,reversingpasttrends.
InordertoavoidthedilemmacausedbythelowspecificityofthePSAtest,ofeitheroverdiagnosingprostatecancerormissingaggressiveprostatecancerduetoreducedscreening,amoreaccurateandnoninvasivetestisneeded.ThistestwouldbeperformedasaseconddecisionpointafterfindinganabnormalPSAresultand/ordigitalrectalexamination(DRE),butbeforeadecisiontoproceedwithaprostatebiopsy.
The4Kscoretestisdesignedtominimizethepotentialharmsstemmingfromunnecessaryprostatebiopsies,whilestillallowingfortheaccuratedetectionofaggressive,high‐grade(Gleasonscore7andhigher)prostatecancerintimetointervenewitheffectivetreatment.The4Kscoretestisanalgorithm‐basedtestcombiningthebloodlevelsoffourkallikreinproteinsandapatient’sclinicalinformationtoprovideaman’sriskforaggressiveprostatecanceronprostatebiopsy.Itisintendedtobeusedinmenaged45‐75yearswithaPSAbetween1.5and10ng/mLand/oranabnormaldigitalrectalexaminationpriortoprostatebiopsy.
Theclinicalvalidityofthe4Kscoretestwasdemonstratedinaprospective,doubleblinded,1012patientclinicaltrialconductedin2013‐14,at26centersacrosstheUnitedStates.All1012mensubmittedtheirbloodsamplespriortoaprostatebiopsyandtheinvestigatorsandpathologistswereblindedtothe4Kscoreresults.Theareaunderthereceiveroperatorcurve(AUC)fordiscriminatingthepresenceofGleasonscore7andhigherprostatecancerwas0.821forthe4Kscoretestvs.0.694fortotalPSAand0.713for%freePSA.Thedataalsoindicatedthatuseofthe4Kscoretestcouldresultinasignificantreductionofthenumberofunnecessarybiopsies(30‐58%),whilestillidentifyingaveryhighpercentageofthosemenwhomaybeathigherriskforaggressiveprostatecancer.
4
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
Furthersub‐analysisofthiscohortshowedthatinmen45‐75yearsofagewithaPSAbetween1.5‐10ng/mL,the4KscoredemonstratedanAUCof0.774vs0.676for%freePSAand0.607fortPSA.Inthisgroup,therewasapotentialbiopsyreductionof35%usinga4Kscorecutoffof7.5%.
ArecentprospectivestudywithintheVeteran’sAffairs(VA)HealthSystemhasfurthervalidatedthe4KscorewithinacohortincludingalargesubsetofAfricanAmericanmen.AfricanAmericanmenhaveahigherincidenceandhigherriskofaggressiveprostatecancer,makingitimperativetohaveanaccuratetesttoevaluatetheriskforthispopulation.Of366menat8siteswith4Kscoreandcompletedata,205(56%)wereAfricanAmerican.TheAUCof4Kscore(0.81)outperformedthebasemodel(0.74)anddemonstratedhigherutilityondecisionanalysis.TherewasnosignificantdifferenceintheAUCofthe4KscoretestbetweenAfricanAmericanandnon‐AfricanAmericanmen(0.80and0.84respectively,p=0.32).
Theclinicalutilityofthe4Kscoretestwasconfirmedinaretrospective611patientstudyperformedatU.S.basedcommunityandacademicurologycenters.Theresultsdemonstrateda64.6%overallreductioninprostatebiopsies.Menwithalowrisk4Kscore(<7.5%)hada94%reductioninprostatebiopsies,whilemenwithahighrisk4Kscore(20%orhigher)hadonlya19%reduction.
The4KscoretesthasbeenincludedintheNCCN2015and2016guidelinesforProstateCancerEarlyDetectionwithlevel2Aevidenceasameanstoimprovetheselectionofmenathigherriskforclinicallysignificant,aggressiveprostatecancerwhoshouldundergoprostatebiopsyduetoanabnormalPSAtestand/orDREfinding.Itisalsoincludedinthe2016EuropeanAssociationofUrologyProstateCancerGuidelines.TheAmericanMedicalAssociation(AMA)hasapprovedthe4KscoretestforaCategoryICPTcode,effectiveJanuary2017.
ThescientificbasisofresearchontheuseofthefourkallikreinproteinstoenhancethesensitivityandspecificityofdetectingaggressiveprostatecancerwasledbyateamofinvestigatorsfromMemorialSloanKetteringCancerCenter.Thecommerciallyavailable4Kscoretestincorporatedtheirscientificknowledge,andwasfurtherrefined,developedandvalidatedbyOPKOinitsownclinicallaboratoryandwhollyownedsubsidiary,BioReferenceLaboratories.
The4Kscoretestisanon‐invasivebloodbasedtestthatprovidesaseconddecisionpointpriortoaprostatebiopsyformenaged45‐75years,withaPSAbetween1.5and10ng/mLand/oranabnormalDRE.Itprovidesanaccurateriskofaggressiveprostatecancer,allowingforearlydetectionofhighriskmen,whilereducingthenumberofunnecessaryprostatebiopsies.ItcorrelateswithlongtermriskofdistantmetastasisinmenwithanelevatedPSA,andisincludedinNCCNguidelinesforProstateCancerEarlyDetection.Useofthe4Kscorewillreducethecostsandcomplicationsofunnecessaryprostatebiopsies,whileidentifyingmenatahigherriskofaggressivecancer,whowouldbenefitfrommoreextensiveevaluation.

5
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
IntendedUseandTargetPopulation
The4Kscoretestprovidesaman’spercentagerisk(reportedonascaleoflessthan1%togreaterthan95%)ofhavingaGleasonscore7orhigherprostatecancerdiagnosedifheweretohaveaprostatebiopsyperformed.The4Kscoretestisintendedtobeusedasaseconddecisionpointinmenaged45‐75yearswithaPSAbetween1.5and10ng/mLand/oranabnormalDRE,priortoperformingaprostatebiopsyinbiopsynaïvemenandmenwithaprevioushistoryofbenign(negative)biopsies.
The4Kscoretestisnotascreeningtest.Theinformationprovidedbythe4Kscoretestallowstheclinicianandpatienttomakeamoreinformeddecisiononwhetherornotaprostatebiopsyiswarranted.Theevidencetosupportthisintendeduseisprovidedinthisdossier.
The4Kscoretestincorporatesbothlaboratorybloodtestdataandthepatient’sclinicaldata.Thelaboratorybloodtestsareperformedoneitherserumorplasmatomeasuretheconcentrationsoffourprostatespecifickallikreinproteinsthatareprostatespecific.Twoofthebloodtestsareroutinelyperformedintheclinicallaboratory:totalPSA(tPSA)andfreePSA(fPSA),whiletheothertwotests,intactPSA(iPSA)andhumankallikrein‐relatedpeptidase2(hK2),areproprietarytoOPKOandessentialfortheintegrityandpredictiveaccuracyofthe4Kscoretestforhigh‐grade(Gleasonscore7andhigher)prostatecancer.Amongtheclinicaldataincorporatedinthe4Kscoretestarethepatient’sage,DREfindingsifavailable,andconsiderationofanypreviousbenign(negative)prostatebiopsyfinding.
OPKOHealth,Inc.developedthe4Kscoretestandoffersthe4KscoretestservicethroughBioReferenceLaboratories,Inc.,itswhollyownedsubsidiary.The4KscoretesthasbeendevelopedandvalidatedatBioReferenceinstrictcompliancewithCLIAregulations,andisperformedinasinglefacilityinaccordancewiththeLaboratoryDevelopedTest(LDT)regulations.
ClinicalScenario
CurrentStandardofCare
CurrentclinicalpracticeforprostatecancerearlydetectionisbasedonPSAtestingand/orDRE,typicallyperformedbyaprimarycarephysician(PCP).ThediscoveryofanabnormalPSAtestand/orDREistheprimaryindicationforreferraltoaurologistforfurtherevaluationthatcouldleadtoaprostatebiopsytodiagnoseprostatecancer.Thiscurrentparadigmleadstoanestimated1millionprostatebiopsiesbeingperformedeachyearintheUnitedStates.However,75%oftheseprostatebiopsiesperformedareunnecessary,astheyshoweithernocancerorlowgrade(Gleasonscore6)prostatecancer,1anindolentformofprostatecancerthatisage‐associatedandhighlyunlikelytocauseharm.2,3Becauseofconcernthatamoreserious,high‐gradecancercouldbemissedbythebiopsy,manymenwithadiagnosisofGleasonscore6prostatecancerchoosetohavetreatment(radical
6
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
prostatectomyorradiation).However,66%ofGleasonscore6cancersdetectedbybiopsyareconfirmedasGleasonscore6intheradicalprostatectomysurgicalspecimen,renderingtheaggressivetreatmentforthesemenunnecessary.4Consequently,inthecurrentparadigmwithanoverrelianceonthePSAtest,manymenareneedlesslyexposedtotheharmsofbiopsy(bleeding,infection,andhospitalization)5andsufferlongtermimpairedurologicalfunctionfromunnecessaryradicalprostatectomyorradiationtherapy.6
Theultimategoalofprostatecancerscreeningistodiagnoseandtreathigh‐grade,aggressiveprostatecancerwhenitisorganconfinedandwhensuccessfultreatmentispossible,whileminimizingtheharmsofunnecessarybiopsiesandovertreatmentofindolentcancers.Itisapparentthattoachievethisgoal,physiciansrequireatestthatismoresensitiveandspecificforidentificationofthesubsetofmenwithhigherriskforaggressiveprostatecancer.Anewtestthatcouldbetterselectthosemenwhoshouldhaveaprostatebiopsywouldbeextremelyvaluable.The4Kscoretestwasdevelopedtofulfillthisclinicalneed.
PublicHealthImportance
Prostatecanceristhesecondleadingcauseofcancerdeathsinmen,with26,000deathsprojectedintheUSin2016.7SincetheadventofPSAscreeningin1991,a45%declineinoverallprostatecancermortalityhasbeenobserved,withmuchofthisdeclineattributabletoPSAscreening.8In2009,theEuropeanRandomizedStudyofScreeningforProstateCancer(ERSPC)reporteda29%reductionindeathfromprostatecancerinmenundergoingroutinePSAscreening.9However,nobenefittoscreeningwasobservedintheU.S.basedProstate,Lung,Colorectal,andOvarianCancerScreeningTrial(PLCO),10butthiswaslikelyduetocontaminationofthecontrolgroup(whoweretohavenoPSAscreening)withPSAtesting.Areviewofthestudydeterminedthat80%ofthemeninthePLCOcontrolgrouphadatleastonePSAtestduringthetrial.11Nevertheless,becauseofthePLCOstudyresults,thenetphysicalandpsychologicalharmsthatresultfromunnecessaryprostatebiopsies,theuncertaintyofprostatebiopsiesundergradingormissingprostatecancer,andtheovertreatmentofnon‐lifethreateningprostatecancer,in2012theUSPSTFadvisedagainstusingthePSAtestforroutineprostatecancerscreeninginmen.12
A2012systematicanalysisofavailableliteratureonactivesurveillanceofprostatecancersuggestedthatupto60%ofprostatecancersdiagnosedincontemporarystudiesmightbesafelyobservedwithoutaneedforimmediateintervention.13Currently,about40%oflowriskpatientsareonactivesurveillance,whiletherestundergomoreaggressivetherapy.14
Theharmsassociatedwithunnecessaryprostatebiopsyandovertreatmentoflow‐gradeprostatecancerarewelldocumented.Apopulation‐basedstudyrevealedafour‐foldincreasefrom1996to2005intheincidenceofhospitaladmissionsafter
7
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
prostatebiopsy,toanoverallrateof4.1%,with72%oftheseadmissionsduetobiopsy‐relatedbacterialsepticemia.5Theprimarypostsurgicalandpost‐radiationtherapycomplicationsincludeerectiledysfunction,urinaryincontinence,anddeclineinhealth‐relatedqualityoflifeinthedomainsofsexual,urinary,andpsychologicalfunction.6,15‐18
TheimpactoftheUSPSTFhasbeenadecreaseinoverallbiopsyrates,andasaconsequence,adecreaseinthedetectionoftheaggressiveGleasonscore7‐10prostatecancers.19EvidenceisnowmountingthatwithreducedlevelsofPSAscreening,menwhowouldhavebeenfoundtohaveaggressiveprostatecancerfollowinganabnormalPSAlevel,andsubsequentlyreferredtoaurologist,areremainingundetectedlonger,andpresentingwithmoreadvanceddiseaseandwithreducedlikelihoodforcure.20‐22
Insummary,thereisaneedtoaddressthelimitationsofPSAscreeningwithoutabandoningthisveryeffectivetoolfortheearlyidentificationofmenatriskforprostatecancer.The4KscoretestoffersaseconddecisionpointafteranabnormalPSAtestand/orDRE,usinganon‐invasivebloodsample,toreducethenumberofunnecessaryprostatebiopsiesinmenatalowerriskforaggressiveprostatecancer(Gleasonscore7andhigher).Theuseofthe4Kscoretestwilldistinguishthosemenatriskforaggressivediseasefrommenatlowrisk,therebyreducingunnecessaryprostatebiopsies,unnecessarytreatment,andtheharmsthatresultfromboth.
ThresholdPSAValueof1.5ng/mLforFurtherEvaluation
The4KscoreisafollowuptestafteranabnormalPSAand/orDRE.OneofthedifficultiesofusingPSAasascreeningtoolforprostatecanceristhelackofconsensusonwhatPSAthresholdisappropriateforfurtherevaluation.Severalstudieshaveexaminedtheriskofprostatecanceratathresholdof1.5ng/mL,showinganincreasedriskabovethisvalue.
Aprospectivestudyof5,855menexaminedthecancerdetectionrateatvariousPSAvaluestodetermineatwhatpointmorefrequentPSAtestingcouldberecommended.23Ofthesemen,539(9.2%)developedprostatecancer,withamedianfollowupof7.6years.TheyfoundaverylowriskofdetectionformenwithaPSAbelow1.0ng/mL(0‐0.9%).TherateshowedasignificantriseformenwithaPSAof1.50‐1.99ng/mL(12.3%)versusfor1.00‐1.49ng/mL(4.7%).Regular,shorterintervalswererecommendedforPSAtestinginmenwithaPSAgreaterthan1.5ng/mL.
Aretrospectivestudyof21,502menwithPSAof0‐4ng/mL,whoinmanycaseswillbeconsiderednormalrisk,evaluatedtheprostatecancerriskoverafour‐yearperiod.24Prostatecancerrateswere15‐foldhigher(19‐foldforAfricanAmericanmen)inpatientswithaPSAof1.5‐4.0ng/mLversusthosewithaPSA<1.5ng/mL.MenwithabaselinePSAof<1.5ng/mLshowedlittleprogressionoverthestudyperiod,withastartingPSAmeanof0.70ng/mLandanendingmeanof0.88ng/mL.MenwithaPSAbetween1.5‐4.0ng/mL,however,progressedfromameanof2.44
8
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
ng/mLto3.24ng/mL.TheauthorsconcludedthatmenwithaPSAof1.5‐4.0ng/mLshouldbeconsideredinanEarly‐WarningPSAZone,withanincreasedriskasopposedtomenwithalowerPSA.
ArecentdiscussionofhowtoapproachmenwithaPSAgreaterthan1.5ng/mLdiscussedtheuseoffollowuptests,includingthe4Kscoretobetterstratifymen.25RecognizingthedifficultieswithPSAscreening,especiallyinminimizingunnecessaryprocedures,theauthorsproposedutilizingnextgenerationtestsfollowinganabnormalPSA,toimprovethespecificityofdetectinghigh‐riskdisease.Thiscombinationreducestheunnecessaryevaluationoflow‐riskmen,whileprovidingasimplealgorithmthatidentifieshigherriskmenforfurtherworkup,includingaprostatebiopsy.
EvidenceSupportingtheIntendedUseofthe4KscoreTest
AnalyticalValidityofthe4KscoreTest
Thedifferentmolecularformsofprostatespecificantigen(PSA)andhumankallikreinrelatedpeptidase2(hK2)arederivedfromtheprostate.26Inmenwithnoorbenignconditionsoftheprostate,mostPSAisfoundastheenzymaticallyinactiveformsofeithercomplexedPSAordegraded(nicked)freePSA,withverylowlevelsofhK2andtheenzymaticallyactiveintactPSAform(iPSA).27AsignificantincreaseinlevelsofhK2andiPSAinserumisassociatedwithaggressivecancerpathologyatbiopsyandradicalprostatectomy.28‐30
The4Kscoretestutilizesthelaboratoryresultsoffourbloodbiomarkers:totalPSA(tPSA),freePSA(fPSA),intactPSA(iPSA)andhumankallikrein‐relatedpeptidase2(hK2).ThetPSAandfPSAassaysareFDA‐approvedandpurchasedfromRocheDiagnostics(Indianapolis,IN).ThespecifickitsusedaretheElecsys®totalPSA(FDAPMAP990056)andtheElecsys®freePSA(FDAPMAP000027).BothassaysareperformedontheRochecobas®analyzerinaccordancewiththeinstructionsprovidedbyRocheDiagnostics.TheplasmaorserumconcentrationsofiPSAandhK2,whichare1/100thto1/1000thoftPSA,aredeterminedusinglaboratorymethodsdevelopedbyOPKOHealth,anddesignedtorunonthePerkinElmerDiagnostics(Waltham,MA)AutoDELFIA®instrument.31TheAutoDELFIAimmunoassaysystem,whichutilizestime‐resolvedfluorescencetechnology,isFDAclearedforuseinseveralIVDkitssoldintheU.S.byPerkinElmer.
TheanalyticalvalidationforiPSAandhK2assayswasperformedatBioReferenceLaboratoriesandincludedtheanalyticallimitofquantitation(LoQ),reportingrange,precision(intra‐labandinter‐lab),referencerangeforeachinbenignprostateconditionsversusprostatecancer,invitrostability,invivostabilityoftheanalytes,andinterferingsubstances(exclusioncriteria).
TheRochecobasinstrumentandthePerkinElmerAutoDELFIAinstrumentarevalidatedforusewiththe4KscoretestaccordingtotheBioReferenceLaboratories“4KscoreAnalyticalPerformanceVerificationPlan”,whicharedesignedtobein

9
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
substantialcompliancewithFDAstandardsaswell.AppropriatevalidationreportsaremaintainedatBioReferenceLaboratories.
Insummary,thelaboratorymeasurementofthefourkallikreinbiomarkersthatarepartofthe4Kscoretesthavebeenfullyvalidatedandarerobustlaboratoryassaysforuseundertheconditionsemployedforthe4Kscoretest.
ClinicalValidityintheDecisiontoPerformProstateBiopsy
2015USValidationStudy:
The2015U.S.validationtrialfor4Kscorewasadoubleblinded,prospectivestudythatassessedtheaccuracyofthe4Kscoretesttopredictthepresenceofhigh‐grade(Gleasonscore7andhigher)prostatecancerpriortoprostatebiopsy.1Patientswereenrolledintheclinicaltrialat26sitesacrosstheUnitedStatesfromOctober2013toApril2014.Theclinicaltrialwasdesignedtotargettheintendedusepopulationofmenaged40to80yearsoldwhowerescheduledtoreceiveadiagnosticprostatebiopsy,andassuch,placednorestrictiononPSAlevelsorDREresults.Furthermore,thestudyenrolledmenregardlessofwhetherthiswastheirfirstprostatebiopsy,orarepeatprostatebiopsyafterpreviousbiopsieswerebenign(negative)forprostatecancer.AsthiscohortrepresentedacontemporaryU.S.populationofmen,atleasta10‐coretransrectalultrasoundguided(TRUS)prostatebiopsywasperformedonallpatientsandcurrentGleasongradingcriteriawereusedforthehistology.
Thestudywasadouble‐blindeddesign,i.e.OPKOperformedthefourkallikreinimmunoassaysandgeneratedthe4Kscoreresultblindedtothebiopsyoutcome,theurologistandpatientdidnotknowthe4Kscoretestresultspriortothebiopsy,andtheanatomicpathologistgradingthebiopsyspecimenwasblindedtothe4Kscoretestresult.AnindependentbiostatisticianthenanalyzedthecombineddatatoassesstheAUC,sensitivity,specificity,negativepredictivevalue(NPV),positivepredictivevalue(PPV),riskcalibrationandclinicalutilitybydecisioncurveanalysisofthe4Kscoretestinthispopulation.
ThestudywasIRB‐approvedandallmenwerepreviouslyscheduledforandreceivedbothaprostatebiopsyanda4Kscoretestresult.The4Kscoretestwasperformedwithin30dayspriortotheprostatebiopsy.Thestudywasconductedintwoparts:first,a300patientcalibrationcohortconfirmedthediscriminationandcorrelationoftheOPKO4Kscoretestresultagainsttheactualbiopsydataobtainedforthese300patients.Thestatisticalalgorithmusedtoestimatetheriskofhigh‐gradecanceronthebasisofthekallikreinmarkerswas“lockeddown”beforeanalysisofthe1012patientvalidationcohort.The4Kscoretestresultshowedanearperfectcorrelationwiththeactualbiopsydataforthe1012patientclinicalvalidationcohort(Figure1).
10
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
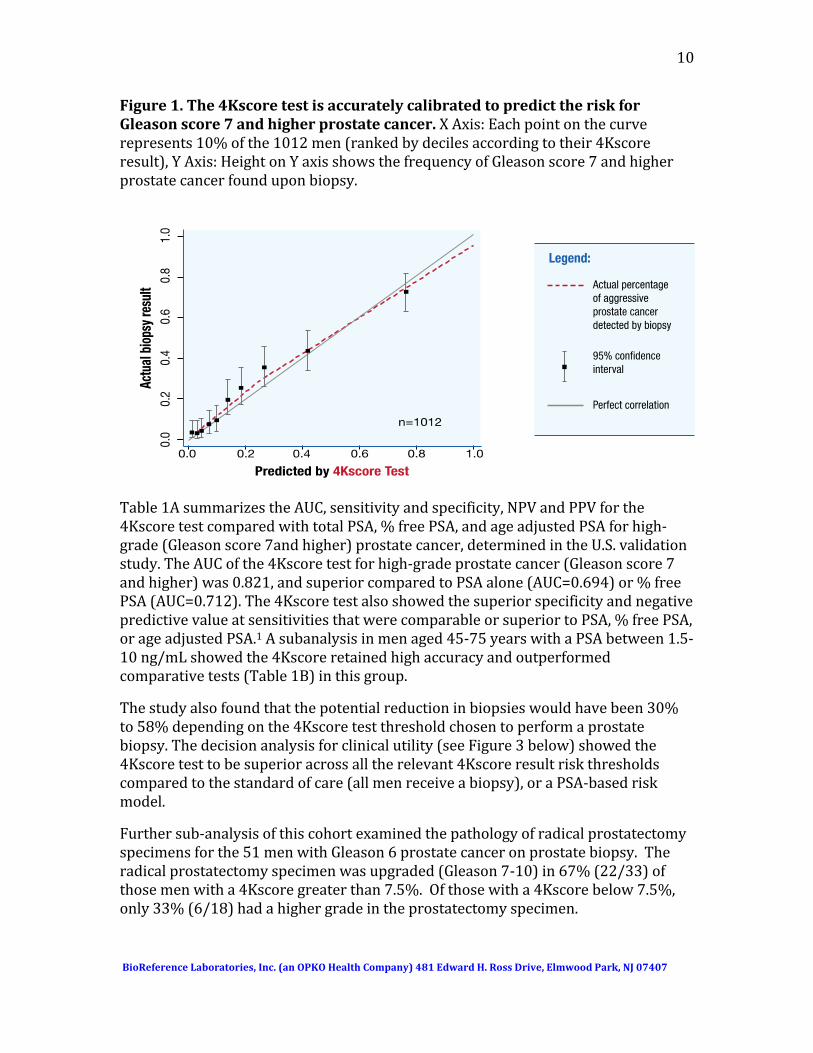
Figure1.The4KscoretestisaccuratelycalibratedtopredicttheriskforGleasonscore7andhigherprostatecancer.XAxis:Eachpointonthecurverepresents10%ofthe1012men(rankedbydecilesaccordingtotheir4Kscoreresult),YAxis:HeightonYaxisshowsthefrequencyofGleasonscore7andhigherprostatecancerfounduponbiopsy.
Table1AsummarizestheAUC,sensitivityandspecificity,NPVandPPVforthe4KscoretestcomparedwithtotalPSA,%freePSA,andageadjustedPSAforhigh‐grade(Gleasonscore7andhigher)prostatecancer,determinedintheU.S.validationstudy.TheAUCofthe4Kscoretestforhigh‐gradeprostatecancer(Gleasonscore7andhigher)was0.821,andsuperiorcomparedtoPSAalone(AUC=0.694)or%freePSA(AUC=0.712).The4KscoretestalsoshowedthesuperiorspecificityandnegativepredictivevalueatsensitivitiesthatwerecomparableorsuperiortoPSA,%freePSA,orageadjustedPSA.1Asubanalysisinmenaged45‐75yearswithaPSAbetween1.5‐10ng/mLshowedthe4Kscoreretainedhighaccuracyandoutperformedcomparativetests(Table1B)inthisgroup.
Thestudyalsofoundthatthepotentialreductioninbiopsieswouldhavebeen30%to58%dependingonthe4Kscoretestthresholdchosentoperformaprostatebiopsy.Thedecisionanalysisforclinicalutility(seeFigure3below)showedthe4Kscoretesttobesuperioracrossalltherelevant4Kscoreresultriskthresholdscomparedtothestandardofcare(allmenreceiveabiopsy),oraPSA‐basedriskmodel.
Furthersub‐analysisofthiscohortexaminedthepathologyofradicalprostatectomyspecimensforthe51menwithGleason6prostatecanceronprostatebiopsy.Theradicalprostatectomyspecimenwasupgraded(Gleason7‐10)in67%(22/33)ofthosemenwitha4Kscoregreaterthan7.5%.Ofthosewitha4Kscorebelow7.5%,only33%(6/18)hadahighergradeintheprostatectomyspecimen.
11
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
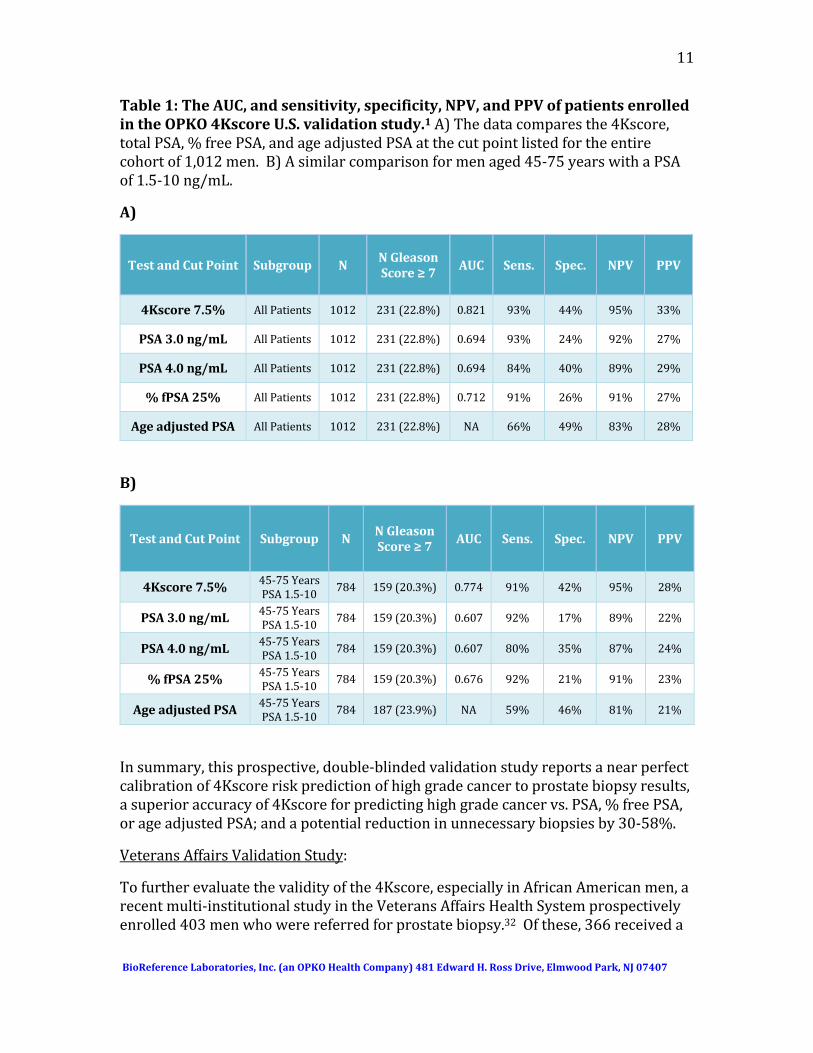
Table1:TheAUC,andsensitivity,specificity,NPV,andPPVofpatientsenrolledintheOPKO4KscoreU.S.validationstudy.1A)Thedatacomparesthe4Kscore,totalPSA,%freePSA,andageadjustedPSAatthecutpointlistedfortheentirecohortof1,012men.B)Asimilarcomparisonformenaged45‐75yearswithaPSAof1.5‐10ng/mL.
A)
TestandCutPoint Subgroup NNGleasonScore≥7 AUC Sens. Spec. NPV PPV
4Kscore7.5% AllPatients 1012 231(22.8%) 0.821 93% 44% 95% 33%
PSA3.0ng/mL AllPatients 1012 231(22.8%) 0.694 93% 24% 92% 27%
PSA4.0ng/mL AllPatients 1012 231(22.8%) 0.694 84% 40% 89% 29%
%fPSA25% AllPatients 1012 231(22.8%) 0.712 91% 26% 91% 27%
AgeadjustedPSA AllPatients 1012 231(22.8%) NA 66% 49% 83% 28%
B)
TestandCutPoint Subgroup NNGleasonScore≥7 AUC Sens. Spec. NPV PPV
4Kscore7.5% 45‐75YearsPSA1.5‐10
784 159(20.3%) 0.774 91% 42% 95% 28%
PSA3.0ng/mL 45‐75YearsPSA1.5‐10
784 159(20.3%) 0.607 92% 17% 89% 22%
PSA4.0ng/mL 45‐75YearsPSA1.5‐10
784 159(20.3%) 0.607 80% 35% 87% 24%
%fPSA25% 45‐75YearsPSA1.5‐10
784 159(20.3%) 0.676 92% 21% 91% 23%
AgeadjustedPSA 45‐75YearsPSA1.5‐10
784 187(23.9%) NA 59% 46% 81% 21%
Insummary,thisprospective,double‐blindedvalidationstudyreportsanearperfectcalibrationof4Kscoreriskpredictionofhighgradecancertoprostatebiopsyresults,asuperioraccuracyof4Kscoreforpredictinghighgradecancervs.PSA,%freePSA,orageadjustedPSA;andapotentialreductioninunnecessarybiopsiesby30‐58%.
VeteransAffairsValidationStudy:
Tofurtherevaluatethevalidityofthe4Kscore,especiallyinAfricanAmericanmen,arecentmulti‐institutionalstudyintheVeteransAffairsHealthSystemprospectivelyenrolled403menwhowerereferredforprostatebiopsy.32Ofthese,366receiveda
12
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
4Kscoretestandhadcompletedataavailableforanalysis.Therewere205(56%)AfricanAmericanmen,ofwhich82(40%)hadhighgradeprostatecancer.Therewere161(44%)non‐AfricanAmericanmen,ofwhom49(31%)hadhighgradeprostatecancer.
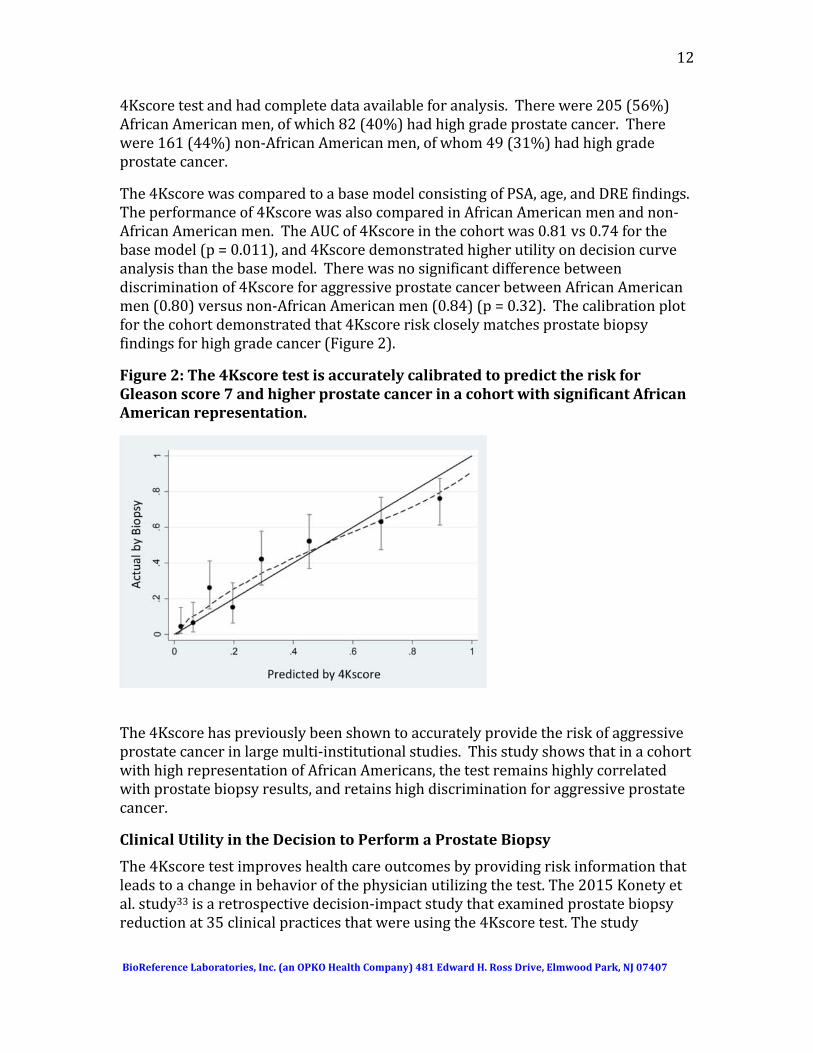
The4KscorewascomparedtoabasemodelconsistingofPSA,age,andDREfindings.Theperformanceof4KscorewasalsocomparedinAfricanAmericanmenandnon‐AfricanAmericanmen.TheAUCof4Kscoreinthecohortwas0.81vs0.74forthebasemodel(p=0.011),and4Kscoredemonstratedhigherutilityondecisioncurveanalysisthanthebasemodel.Therewasnosignificantdifferencebetweendiscriminationof4KscoreforaggressiveprostatecancerbetweenAfricanAmericanmen(0.80)versusnon‐AfricanAmericanmen(0.84)(p=0.32).Thecalibrationplotforthecohortdemonstratedthat4Kscoreriskcloselymatchesprostatebiopsyfindingsforhighgradecancer(Figure2).
Figure2:The4KscoretestisaccuratelycalibratedtopredicttheriskforGleasonscore7andhigherprostatecancerinacohortwithsignificantAfricanAmericanrepresentation.
The4Kscorehaspreviouslybeenshowntoaccuratelyprovidetheriskofaggressiveprostatecancerinlargemulti‐institutionalstudies.ThisstudyshowsthatinacohortwithhighrepresentationofAfricanAmericans,thetestremainshighlycorrelatedwithprostatebiopsyresults,andretainshighdiscriminationforaggressiveprostatecancer.
ClinicalUtilityintheDecisiontoPerformaProstateBiopsy
The4Kscoretestimproveshealthcareoutcomesbyprovidingriskinformationthatleadstoachangeinbehaviorofthephysicianutilizingthetest.The2015Konetyetal.study33isaretrospectivedecision‐impactstudythatexaminedprostatebiopsyreductionat35clinicalpracticesthatwereusingthe4Kscoretest.Thestudy
13
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
involvedatotalof611menwithanabnormalPSAtestand/orDRE.Eachurologistusedthe4Kscoretestandhisorherownclinicaljudgmenttodecidehowbesttomanage(i.e.toproceedwithaprostatebiopsyornot)thepatient.Theurologistswereaskedviaaquestionnairetoevaluatetheimpactofthe4Kscoretestontheirpatientmanagementdecisions.
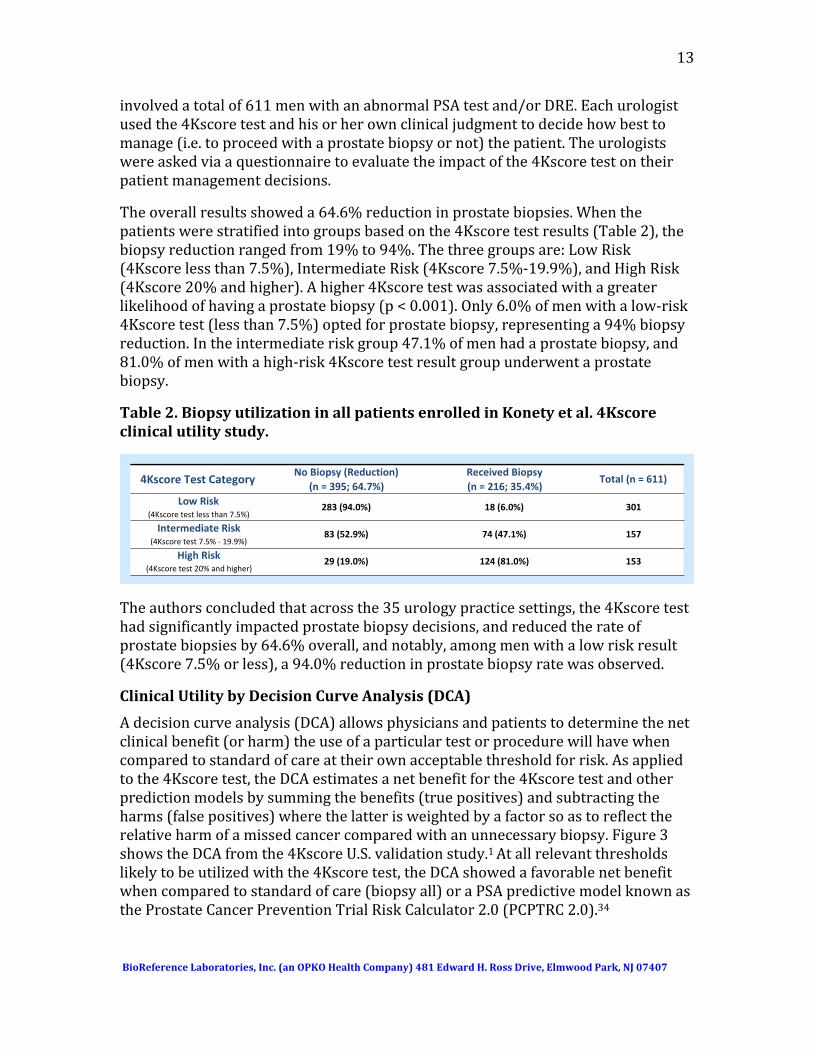
Theoverallresultsshoweda64.6%reductioninprostatebiopsies.Whenthepatientswerestratifiedintogroupsbasedonthe4Kscoretestresults(Table2),thebiopsyreductionrangedfrom19%to94%.Thethreegroupsare:LowRisk(4Kscorelessthan7.5%),IntermediateRisk(4Kscore7.5%‐19.9%),andHighRisk(4Kscore20%andhigher).Ahigher4Kscoretestwasassociatedwithagreaterlikelihoodofhavingaprostatebiopsy(p<0.001).Only6.0%ofmenwithalow‐risk4Kscoretest(lessthan7.5%)optedforprostatebiopsy,representinga94%biopsyreduction.Intheintermediateriskgroup47.1%ofmenhadaprostatebiopsy,and81.0%ofmenwithahigh‐risk4Kscoretestresultgroupunderwentaprostatebiopsy.
Table2.BiopsyutilizationinallpatientsenrolledinKonetyetal.4Kscoreclinicalutilitystudy.
Theauthorsconcludedthatacrossthe35urologypracticesettings,the4Kscoretesthadsignificantlyimpactedprostatebiopsydecisions,andreducedtherateofprostatebiopsiesby64.6%overall,andnotably,amongmenwithalowriskresult(4Kscore7.5%orless),a94.0%reductioninprostatebiopsyratewasobserved.
ClinicalUtilitybyDecisionCurveAnalysis(DCA)
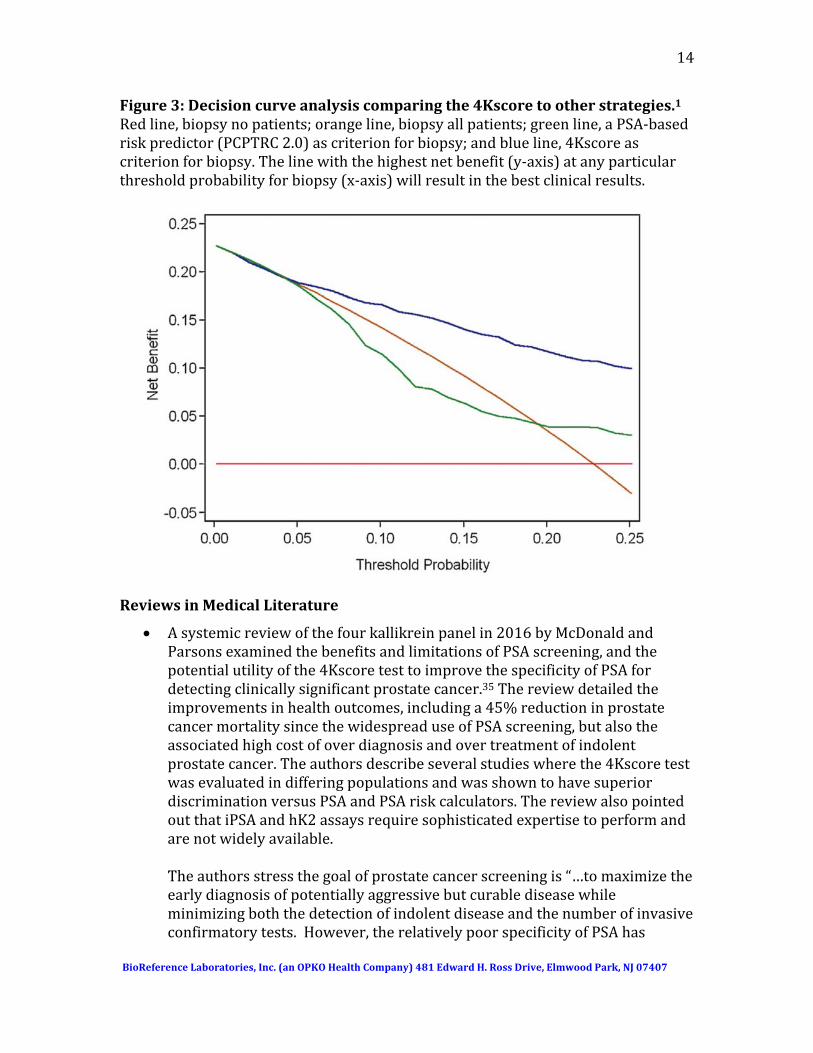
Adecisioncurveanalysis(DCA)allowsphysiciansandpatientstodeterminethenetclinicalbenefit(orharm)theuseofaparticulartestorprocedurewillhavewhencomparedtostandardofcareattheirownacceptablethresholdforrisk.Asappliedtothe4Kscoretest,theDCAestimatesanetbenefitforthe4Kscoretestandotherpredictionmodelsbysummingthebenefits(truepositives)andsubtractingtheharms(falsepositives)wherethelatterisweightedbyafactorsoastoreflecttherelativeharmofamissedcancercomparedwithanunnecessarybiopsy.Figure3showstheDCAfromthe4KscoreU.S.validationstudy.1Atallrelevantthresholdslikelytobeutilizedwiththe4Kscoretest,theDCAshowedafavorablenetbenefitwhencomparedtostandardofcare(biopsyall)oraPSApredictivemodelknownastheProstateCancerPreventionTrialRiskCalculator2.0(PCPTRC2.0).34
4Kscore Test CategoryNo Biopsy (Reduction)
(n = 395; 64.7%)Received Biopsy(n = 216; 35.4%)
Total (n = 611)
Low Risk(4Kscore test less than 7.5%)
Intermediate Risk(4Kscore test 7.5% ‐ 19.9%)
High Risk(4Kscore test 20% and higher)
283 (94.0%) 18 (6.0%) 301
83 (52.9%) 74 (47.1%) 157
29 (19.0%) 124 (81.0%) 153
14
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
Figure3:Decisioncurveanalysiscomparingthe4Kscoretootherstrategies.1Redline,biopsynopatients;orangeline,biopsyallpatients;greenline,aPSA‐basedriskpredictor(PCPTRC2.0)ascriterionforbiopsy;andblueline,4Kscoreascriterionforbiopsy.Thelinewiththehighestnetbenefit(y‐axis)atanyparticularthresholdprobabilityforbiopsy(x‐axis)willresultinthebestclinicalresults.
ReviewsinMedicalLiterature
Asystemicreviewofthefourkallikreinpanelin2016byMcDonaldandParsonsexaminedthebenefitsandlimitationsofPSAscreening,andthepotentialutilityofthe4KscoretesttoimprovethespecificityofPSAfordetectingclinicallysignificantprostatecancer.35Thereviewdetailedtheimprovementsinhealthoutcomes,includinga45%reductioninprostatecancermortalitysincethewidespreaduseofPSAscreening,butalsotheassociatedhighcostofoverdiagnosisandovertreatmentofindolentprostatecancer.Theauthorsdescribeseveralstudieswherethe4KscoretestwasevaluatedindifferingpopulationsandwasshowntohavesuperiordiscriminationversusPSAandPSAriskcalculators.ThereviewalsopointedoutthatiPSAandhK2assaysrequiresophisticatedexpertisetoperformandarenotwidelyavailable.Theauthorsstressthegoalofprostatecancerscreeningis“…tomaximizetheearlydiagnosisofpotentiallyaggressivebutcurablediseasewhileminimizingboththedetectionofindolentdiseaseandthenumberofinvasiveconfirmatorytests.However,therelativelypoorspecificityofPSAhas
15
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
contributedtotheoverdetectionofindolentdisease.Onepotentialsolutionistofocusonthedetectionofclinicallysignificantprostatecancerbyusingtestswithenhancedspecificity.”Theauthorsfoundthatthe4Kscoretestiseffectiveby“…providinganindividualizedpredictionofclinicallysignificantcancerregardlessofpriorscreeningorpreviousbiopsy.”Theyconcludedthatitwouldhaveutilityintheprocessofshareddecisionmakingforprostatebiopsiesandintheearlydetectionofprostatecancer.Thiscouldleadtoa41‐71%reductioninprostatebiopsies,withaminimalriskfordelayeddiagnosisofsignificantprostatecancer.
Inanothersystematicreviewofthe4Kscoretest,theauthorsreviewedthe
clinicalstudiesfortencohortsconsistingofover15,000menfrompeer‐reviewedmedicaljournals.36Theauthorsfoundthatthe4Kscoretestiseffectiveforaccuratelyidentifyingmenathighriskforaggressivediseaseandisappropriatetoselectthosemenwhowouldbenefitfromaprostatebiopsyandpreventapotentiallylethaloutcomefromprostatecancer.Theauthorsconcludethat30‐58%ofmenwithalow4Kscoretestresultcouldsafelydeferprostatebiopsybecauseofhavinganegligibleriskofhavingmissedaggressiveprostatecancer.
ArecentreviewbyBrattetal.37examinedthepotentialforblood‐based
biomarkerstodetectprostatecancer.TheauthorshighlightedtheimportanceofPSAscreeningfollowedbyafourkallikreinpanelformenwithevenmodestlyelevatedPSAvaluespriortoconsideringabiopsy.Theauthorsnotedthatstatisticalmodelsbasedonthebiomarkersinthe4KscoretestimprovethespecificityofelevatedPSA(2.0‐10.0 ng/mL),reduceunnecessaryprostatebiopsies,andbetteridentifymenatriskofaggressiveprostatecancerwhoshouldhaveabiopsyoradditionalimaging.
Filellaetal.publishedacomprehensivereviewofemergingbiomarkersfor
detectionofaggressiveprostatecancerinbloodandurine.38Thereviewincludedadiscussionoftheclinicalworkunderlyingthe4KscoreaswellasotherbloodandurinetestsincludingPCA3andphi.ItconcludedthatthesebiomarkersoutperformthespecificityoftPSAandpercentfPSA.
IndependentRecommendationsandGuidelines
NCCNGuidelinesforProstateCancerEarlyDetection
The4Kscoretestisincludedinthemostrecent2016NCCNGuidelinesforProstateCancerEarlyDetectionbasedonlevel2Aevidence,andisindicatedasatesttobeusedafterafindingofanabnormalPSAtestorDRE:39ThespecificNCCNpanelrecommendationshighlightthe4Kscoretestinthefollowingway,consistentwith
16
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
itsintendeduseinbiopsynaïvepatientsorinpatientswithpreviousbenign(negative)biopsies:
“Biomarkersthatimprovethespecificityof(prostatecancerearly)detectionarenotrecommendedasfirstlinescreeningtests.However,theremaybesomepatientswhomeeteitherPSAstandardsforconsiderationofprostatebiopsy,butforwhomthepatientand/orthephysicianwishtofurtherdefinetheprobabilityofhigh‐gradecancer.4Kscore(whichprovidesanestimateoftheprobabilityofprostatecancer)ispotentiallyinformativeinpatientswhohaveneverundergonebiopsyorafteranegativebiopsy”.
TheNCCNguidelinesgoontofurthercommentonthemanagementofbiopsyresults:
“Itiswellknownthatanegativeprostatebiopsydoesnotprecludeadiagnosisofprostatecanceronsubsequentbiopsy.ThosepatientswithnegativebiopsiesshouldbefollowedwithDREandPSA.Testswhichimprovespecificityinthepost‐biopsystate—including4Kscoreshouldbeconsideredinpatientsthoughttobeatahigherriskdespiteanegativebiopsy.”
EuropeanAssociationofUrology(EAU)ProstateCancerGuidelines
The4Kscoreisincludedinthe2016EAU‐ESTRO‐SIOGGuidelinesonProstateCancer,40withthefollowingrecommendation:
“UsetheadditionaldiagnosticoptionsinasymptomaticmenwithanormalDREandaPSAbetween2.0and10ng/mL(riskcalculator,oranadditionalserumorurine‐basedtest[4Kscore]orimaging).”
Theguidelinesalsomentionthat4Kscorehasbeenshowntoout‐performfree/totalPSAprostatecancerdetection,“withanimprovedpredictionofclinicallysignificantprostatecancer,inmenwithaPSAbetween2‐10ng/mL.”
RegulationandCPTCode
FederalLaboratoryRegulation
The4KscoretesthasbeendevelopedandvalidatedatBioReferenceLaboratories,Inc.,awhollyownedsubsidiaryofOPKOHealth,Inc.The4KscoretestwasvalidatedinstrictcompliancewithCLIAregulations,andisperformedinasinglefacilityinaccordancewiththefederalregulationsregardingLaboratoryDevelopedTests(LDTs).
StatePermits
InadditiontoNewJersey,BioReferenceLaboratoriesislicensedbyallstatesrequiringout‐of‐statediagnosticlabstohavepermits,includingCalifornia,Connecticut,Florida,Maryland,NewYork,Pennsylvania,RhodeIsland,Vermont,andWestVirginia.
17
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
The4KscoretestalsohasconditionalapprovalbyNewYorkStateunderitsClinicalLaboratoryEvaluationProgram.MostclinicalpathologistsconsiderthisprogramasrepresentingthehigheststandardforevaluatingtheperformanceofnewLDTs.
LaboratoryAccreditation
BioReferenceLaboratoriesislicensedbyCMSandisCLIAcertifiedasahighcomplexitylaboratoryunderCLIA88regulations.TheBioReferenceLaboratoriesteamofboard‐certified,fellowship‐trainedpathologistsislicensedinall50states.TheBioReferenceLaboratoriesfacilityisalsoaCollegeofAmericanPathologists(CAP)‐accreditedlaboratory.
4KscoreTestCategoryICPTCode
InOctober2015,theAmericanMedicalAssociation(AMA)determinedthatthe4KScoremettherequirementsforaCategoryICPTcode.BelowistheCPTcodeassignedandthedescriptionofthetestinthe2017AMACPTbookeffectiveJanuary2017.Thetestdescriptorisasfollows:
81539‐Oncology(high‐gradeprostatecancer),biochemicalassayoffourproteins(TotalPSA,FreePSA,IntactPSAandhumankallikrein‐2[hK2]),utilizingplasmaorserum,prognosticalgorithmreportedasaprobabilityscore
Discussion
Developmentofthe4KscoreTest
ScientistsandcliniciansfromMemorialSloanKetteringCancerCenterledtheinitialclinicalresearchonthefourkallikreinbiomarkers,andthedevelopmentofalgorithmsthatcombinedthebiomarkerswithclinicalinformation,laterfinalizedasthe4Kscoretest.Thisteampublishedaseriesofarticles41‐45thatdemonstratedtherepeatedabilityofafourkallikreinbiomarkerandclinicalinformationalgorithmtopredicttheriskofhigh‐grade(Gleasonscore7andhigher)prostatecancerandreduceunnecessaryprostatebiopsies.ThemenwereallenrolledintheEuropeanRandomizedStudyofScreeningforProstateCancer(ERSPC)andunderwentprostatebiopsyduetoanelevatedPSAlevel(3.0ng/mLandhigher)detectedbyPSAscreening.Multiplecohortswerestudied,includingmenwithnopriorPSAscreening,priorPSAscreening,andmenwhohadapriorbenign(negative)prostatebiopsy.ThispioneeringeffortservedasthescientificbasisforthedevelopmentofthecommerciallyavailableOPKO4Kscoretest.
IntheyearsfollowingthecollectionoftheERSPCsamples,theprostatebiopsystandardprocedurechangedfroma6‐core(sextant)biopsytoa10‐corebiopsyandnewcriteriaforGleasongradingwerealsointroducedthatbroadenedthecriteriaforinclusionintoGleasongrade4.46Also,therewasgrowingevidencethatGleasonscore6prostatecancer,thoughhavingthehistopathologicalfeaturesofadenocarcinoma,wasunlikelytometastasizeandcausedeath.2,3Thesechangesinclinicalpracticewerereflectedinthedevelopmentofthecommercialized4Kscore

18
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
test,validatedbyOPKO1inadoubleblinded,prospectivestudyofacontemporaryU.S.populationof1012menat26urologycentersacrosstheU.S.in2013‐14,anddescribedindetailbelow.
TheProstateTestingforCancerandTreatment(ProtecT)study,anongoingprospective,randomized,controlledclinicaltrial,providedanadditionalopportunitytoevaluatethediagnosticaccuracyandbiopsyreductionpotentialofthe4Kscoretestina2015publishedreport.47Allavailablecryopreservedbloodsamplesfromthosemenwhoagreedtoundergoprostatebiopsywereretrieved,resultinginasamplesetconsistingofEDTAplasmafrom4765men,serumfrom1860men,andbothplasmaandserumfrom496menwhohadundergoneaprostatebiopsy.Thelaboratoryperformingthetestingofthefourkallikreinsbiomarkerswasblindedtothebiopsypathologydataandviceversa.
Theplasmasamplesassessedwiththe4KscoretestagainstprostatebiopsyhistologyhadanAUC=0.820fordiscriminationofhigh‐grade(Gleasonscore7andhigher)prostatecancerandsuperiorperformancecomparedtoaPSA‐basedmodel(AUC=0.738).TheAUCinthiscohortwasvirtuallyidenticalcomparedwiththeU.S.validationstudyofParekhetal.1(discussedabove),andtheauthorsreportedthattheplasmaandserumsamplesprovidedequivalentAUCperformanceforthe4Kscoretest.Adecisioncurvedemonstratedclinicalutilityacrossrelevantriskthresholdsforhigh‐grade(Gleasonscore7andhigher)prostatecancer,withabiopsyreductionpotentialof43%ata6%riskthreshold.
The4Kscorewasfurthershowntoaccuratelypredictriskofhigh‐gradediseaseinapopulationscreenedwithfreetototalPSAratio.Braunetal.48studiedthe4Kscoretestinacohortof749whoallreceivedaprostatebiopsyduetoalowfreetototalPSAratio(<20%)orasuspiciousDRE.Theauthorsanalyzedarangeof4Kscorecutpoints(4‐12%)andprojectedthatupto38%ofprostatebiopsiescouldbeavoided.
TheAbilityofthe4KscoreTesttoPredicttheRiskofDistantMetastasis
The4KscoretestwasalsoevaluatedbyStattinetal.49inalong‐termclinicaloutcomesstudypublishedin2015,withanendpointofdistantprostatecancermetastasis.PSAand4Kscoretestresultswereobtainedfrombankedplasmasamplesinagroupofmenwhohadmorethan15yearsoffollowup.Duringthistimeframe,themenwerenotsubjecttoPSAscreening,thusthisstudyexaminedthenaturalhistoryofmetastaticprostatecanceroccurrenceobservedinmenasafunctionoftheirPSAandthe4Kscoretestresultsmeasuredover15yearsearlier.
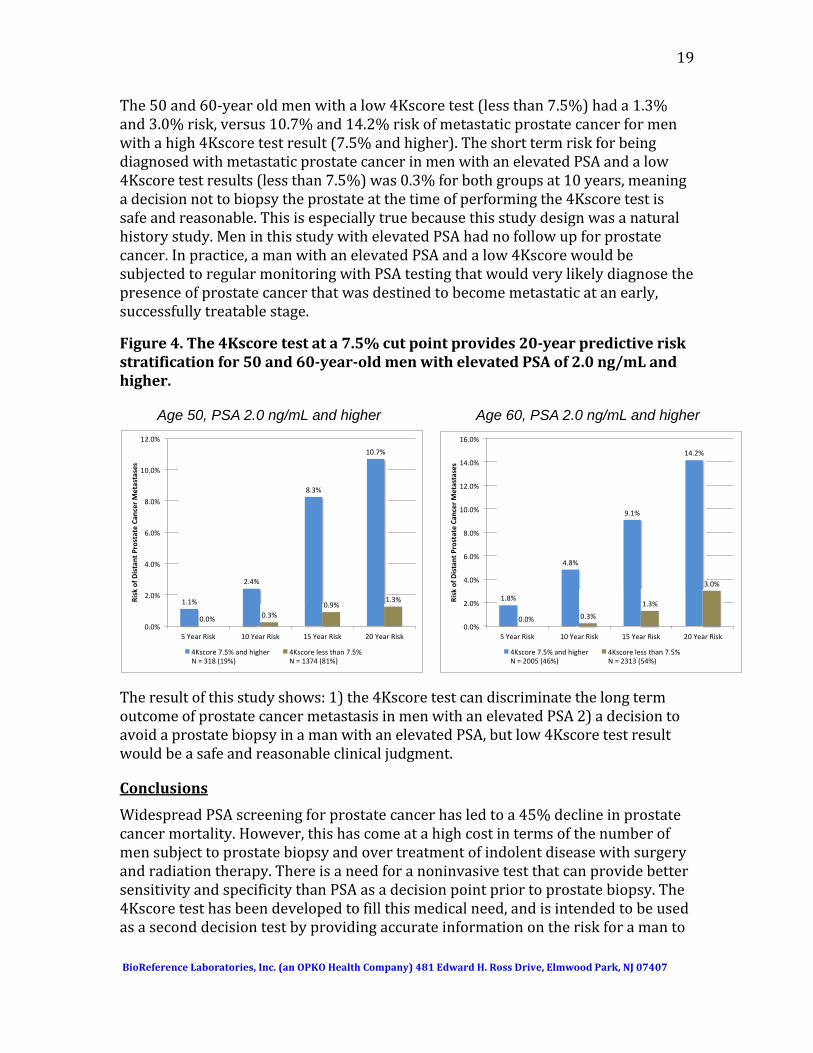
Theplasmasamplesfromthesemenweretestedwiththe4KscoretestinadditiontoPSA.Thedatashowedthatafter20years,a4Kscoretestperformedatage50or60onamanwithaPSAlevelof2.0ng/mLandhigherprovidedclearriskstratificationforsubsequentdevelopmentofmetastaticprostatecancer(seeFigure4).
19
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
The50and60‐yearoldmenwithalow4Kscoretest(lessthan7.5%)hada1.3%and3.0%risk,versus10.7%and14.2%riskofmetastaticprostatecancerformenwithahigh4Kscoretestresult(7.5%andhigher).TheshorttermriskforbeingdiagnosedwithmetastaticprostatecancerinmenwithanelevatedPSAandalow4Kscoretestresults(lessthan7.5%)was0.3%forbothgroupsat10years,meaningadecisionnottobiopsytheprostateatthetimeofperformingthe4Kscoretestissafeandreasonable.Thisisespeciallytruebecausethisstudydesignwasanaturalhistorystudy.MeninthisstudywithelevatedPSAhadnofollowupforprostatecancer.Inpractice,amanwithanelevatedPSAandalow4KscorewouldbesubjectedtoregularmonitoringwithPSAtestingthatwouldverylikelydiagnosethepresenceofprostatecancerthatwasdestinedtobecomemetastaticatanearly,successfullytreatablestage.
Figure4.The4Kscoretestata7.5%cutpointprovides20‐yearpredictiveriskstratificationfor50and60‐year‐oldmenwithelevatedPSAof2.0ng/mLandhigher.
Theresultofthisstudyshows:1)the4KscoretestcandiscriminatethelongtermoutcomeofprostatecancermetastasisinmenwithanelevatedPSA2)adecisiontoavoidaprostatebiopsyinamanwithanelevatedPSA,butlow4Kscoretestresultwouldbeasafeandreasonableclinicaljudgment.
Conclusions
WidespreadPSAscreeningforprostatecancerhasledtoa45%declineinprostatecancermortality.However,thishascomeatahighcostintermsofthenumberofmensubjecttoprostatebiopsyandovertreatmentofindolentdiseasewithsurgeryandradiationtherapy.ThereisaneedforanoninvasivetestthatcanprovidebettersensitivityandspecificitythanPSAasadecisionpointpriortoprostatebiopsy.The4Kscoretesthasbeendevelopedtofillthismedicalneed,andisintendedtobeusedasaseconddecisiontestbyprovidingaccurateinformationontheriskforamanto
Age 50, PSA 2.0 ng/mL and higher Age 60, PSA 2.0 ng/mL and higher
1.1%
2.4%
8.3%
10.7%
0.0% 0.3% 0.9%
1.3%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
5 Year Risk 10 Year Risk 15 Year Risk 20 Year Risk
Risk of D
istant P
rostate Can
cer Metastases
4Kscore 7.5% and higher N = 318 (19%)
4Kscore less than 7.5% N = 1374 (81%)
1.8%
4.8%
9.1%
14.2%
0.0% 0.3%
1.3%
3.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
5 Year Risk 10 Year Risk 15 Year Risk 20 Year Risk
Risk of D
istant P
rostate Can
cer Metastases
4Kscore 7.5% and higher N = 2005 (46%)
4Kscore less than 7.5% N = 2313 (54%)
20
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
beharboringhigh‐grade(Gleasonscore7andhigher)prostatecancerbeforeproceedingtoaprostatebiopsy.
The4Kscoretest:
Isanon‐invasive,blood‐basedtest,offeredasanLDTbyBioReferenceLaboratories,awhollyownedsubsidiaryofOPKOHealth
Intendedtobeusedasaseconddecisiontoolbeforeperformingaprostatebiopsyinmenaged45‐75yearswithaPSAbetween1.5‐10ng/mLand/oranabnormalDRE.
Providesthenecessarydiscriminationforhigh‐grade,GleasonScore7andhigherprostatecancer(AUC=0.821)determinedinaprospective,doubleblinded,26‐centerclinicaltrialof1012menintheU.S.
HassuperioraccuracytoPSA,%fPSA,andPSAbasedriskcalculatorsforpredictinghighgradeprostatecancer
Hasbeenshowntominimizetheriskofover‐diagnosisandovertreatmentofprostatecancerbyreducingunnecessaryprostatebiopsiesasmuchas64.6%
Isincludedinthe2016NCCNguidelinesforprostatecancerearlydetectioninbothbiopsynaïveandmenwithapriorbenign(negative)biopsy
IsapprovedforaCategoryICPTcodebytheAMA
21
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
References
1. ParekhDJ,PunnenS,SjobergDD,etal.Amulti‐institutionalprospectivetrialintheUSAconfirmsthatthe4Kscoreaccuratelyidentifiesmenwithhigh‐gradeprostatecancer.EurUrol.2015Sep;68(3):464‐70.
2. RossHM,KryvenkoON,CowanJE,etal.DoadenocarcinomasoftheprostatewithGleasonscore(GS)≤6havethepotentialtometastasizetothelymphnodes?AmJSurgPathol.2012September;36(9):1346–1352.
3. EggenerSE,BadaniK,BarocasDA,etal.Gleason6prostatecancer:translatingbiologyintopopulationhealth.JUrol.2015Sep;194(3):626‐34.
4. JallohM,MyersF,CowanJE,etal.Racialvariationinprostatecancerupgradingandupstagingamongmenwithlow‐Riskclinicalcharacteristics.EurUrol.2015Mar;67(3):451‐7.
5. NamRK,SaskinR,LeeY,etal.Increasinghospitaladmissionratesforurologicalcomplicationsaftertransrectalultrasoundguidedprostatebiopsy.JUrol.2013Jan;189(1Suppl):S12‐7.
6. ResnickMJ,KoyamaT,FanKH,etal.Long‐termfunctionaloutcomesaftertreatmentforlocalizedprostatecancer.NEnglJMed.2013January31;368(5):436–445.
7. SiegelRL,MillerKD,JemalA.Cancerstatistics,2016.CACancerJClin.2016Jan‐Feb;66(1):7‐30.
8. EtzioniR,TsodikovA,MariottoA,etal.QuantifyingtheroleofPSAscreeningintheUSprostatecancermortalitydecline.CancerCausesControl.2008Mar;19(2):175‐81.
9. SchröderFH,HugossonJ,RoobolMJ,etal.Screeningandprostate‐cancermortalityinarandomizedEuropeanstudy.NEnglJMed.2009Mar26;360(13):1320‐8.
10. AndrioleGL,CrawfordED,GrubbRL3rd,etal.ProstatecancerscreeningintherandomizedProstate,Lung,Colorectal,andOvarianCancerScreeningTrial:mortalityresultsafter13yearsoffollow‐up.JNatlCancerInst.2012Jan18;104(2):125‐32.
11. ShoagJE,MittalS,HuJC.ReevaluatingPSAtestingratesinthePLCOtrial.NEnglJMed.2016May5;374(18):1795‐6.
12. MoyerVA,USPreventiveServicesTaskForce.Screeningforprostatecancer:U.S.PreventiveServicesTaskForcerecommendationstatement.AnnInternMed.2012Jul;157(2):120‐34.
22
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
13. Dall'EraMA,AlbertsenPC,BangmaC,etal.Activesurveillanceforprostatecancer:asystematicreviewoftheliterature.EurUrol.2012Dec;62(6):976‐83.
14. CooperbergMRandCarrollPR.TrendsinManagementforPatientswithLocalizedProstateCancer,1990‐2013.JAMA2015Jul;314(1):80‐82.
15. BarryMJ,GallagherPM,SkinnerJS,etal.Adverseeffectsofrobotic‐assistedlaparoscopicversusopenretropubicradicalprostatectomyamonganationwiderandomsampleofMedicare‐agemen.JClinOncol.2012Feb;30(5):513‐8.
16. PunnenS,CowanJE,ChanJM,etal.Long‐termhealth‐relatedqualityoflifeafterprimarytreatmentforlocalizedprostatecancer:resultsfromtheCaPSUREregistry.EurUrol.2015Oct;68(4):600‐8.
17. ResnickMJ,PensonDF.Functionaloutcomesaftertreatmentforprostatecancer.NEnglJMed.2013Apr25;368(17):1654.
18. WatsonE,ShinkinsB,FrithE,etal.Symptoms,unmetneeds,psychologicalwell‐beingandhealthstatusinsurvivorsofprostatecancer:implicationsforredesigningfollow‐up.BJUInt.2016Jun;117(6B):E10‐19.
19. BhindiBM,MamdaniM,KalkarniGSetal.ImpactoftheU.S.PreventiveServicesTaskForcerecommendationsagainstprostatespecificantigenscreeningonprostatebiopsyandcancerdetectionrates.JUrol.2015May;193(5):1519‐24.
20. BarocasDA,MallinK,GravesAJ,etal.EffectoftheUSPSTFGradeDrecommendationagainstscreeningforprostatecanceronincidentprostatecancerdiagnosesintheUnitedStates.JUrol.2015Dec;194(6):1587‐93
21. HallMD,SchultheissTE,FarinoG,etal.IncreaseinhigherriskprostatecancercasesfollowingnewscreeningrecommendationbytheUSPreventiveServicesTaskForce(USPSTF).JClinOncol.2015March;33(7)_suppl.(Mar.1Supplement),2015:143.
22. WeinerAB,MatulewiczRS,EggenerSE,etal.IncreasingincidenceofmetastaticprostatecancerintheUnitedStates(2004‐2013).ProstateCancerProstaticDis.2016Dec;19(4):395‐397.
23. AusG.,DamberJE,Khatam,A,etal.Individualizedscreeningintervalforprostatecancerbasedonprostate‐specificantigenlevel:resultsofaprospective,randomized,population‐basedstudy.ArchInternMed2005Sep;165(16):1857‐1861.
24. CrawfordED,MoulJW,RoveKO,etal.Prostate‐specificantigen1.5‐4.0ng/mL:adiagnosticchallengeanddangerzone.BJUInt2011Dec;108(11):1743‐1749.
23
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
25. CrawfordED,RosenbergMT,PartinAW,etal.AnApproachUsingPSALevelsof1.5ng/mLastheCutoffforProstateCancerScreeninginPrimaryCare.Urology2016Oct;96:116‐120.
26. LiljaH,OldbringJ,RannevikG,etal.Seminalvesicle‐secretedproteinsandtheirreactionsduringgelationandliquefactionofhumansemen.JClinInvest1987;80:281‐285.
27. LiljaH,UlmertD,VickersAJ.Prostate‐specificantigenandprostatecancer:prediction,detectionandmonitoring.NatRevCancer.2008Apr;8(4):268‐78.
28. SteuberT,VickersAJ,SerioAM,etal.Comparisonoffreeandtotalformsofserumhumankallikrein2andprostate‐specificantigenforpredictionoflocallyadvancedandrecurrentprostatecancer.ClinChem.2007Feb;53(2):233‐40.
29. WenskeS,KoretsR,CroninAM,etal.Evaluationofmolecularformsofprostate‐specificantigenandhumankallikrein2inpredictingbiochemicalfailureafterradicalprostatectomy.IntJCancer.2009Feb1;124(3):659‐63.
30. PeltolaMT,NiemeläP,VäisänenV,etal.Intactandinternallycleavedfreeprostate‐specificantigeninpatientswithprostatecancerwithdifferentpathologicstagesandgrades.Urology2011Apr;77(4):1009.e1‐8.
31. VaisanenV,PeltolaMT,LiljaH,etal.Intactfreeprostate‐specificantigenandfreeandtotalhumanglandularkallikrein2.EliminationofassayinterferencebyenzymaticdigestionofantibodiestoF(ab')2fragments.AnalChem2006Nov;78(22):7809‐7815.
32. PunnenS,FreedlandSJ,PolascikTJ,etal.Anindependent,Multi‐Institutional,ProspectivestudyintheVeteransAffairsHealthSystemconfirmsthe4Kscoreaccuratelypredictsaggressiveprostatecancer.ABSTRACT:AmericanUrologicalAssociationAnnualMeeting2017.
33. KonetyB,ZappalaSM,ParekhDJ,etal.The4Kscoretestreducesprostatebiopsyratesincommunityandacademicurologypractices.RevUrol.2015;17(4):231‐240.
34. ThompsonIM,AnkerstDP,ChiC,etal.Assessingprostatecancerrisk:resultsfromtheProstateCancerPreventionTrial.JNatlCancerInst.2006Apr;98(8):529‐534.
35. McDonaldML,ParsonsJK.4‐Kallikreintestandkallikreinmarkersinprostatecancerscreening.UrolClinNorthAm.2016Feb;43(1):39‐46.
24
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
36. PunnenS,PavanN,Parekh,D.J.Findingthewolfinsheep'sclothing:the4Kscoreisanovelbloodtestthatcanaccuratelyidentifytheriskofaggressiveprostatecancer.RevUrol.2015;17(1):3‐13.
37. BrattO,LiljaH.Serummarkersinprostatecancerdetection.CurOpinUrol.2015
Jan;25(1):59‐64.
38. FilellaX,FojL.Emergingbiomarkersinthedetectionandprognosisofprostatecancer.ClinChemLabMed.2015Jun;53(7):963‐973.
39. NationalComprehensiveCancerNetwork(NCCN).ProstateCancerEarlyDetection(Version2.2016).https://www.nccn.org/professionals/physician_gls/pdf/prostate_detection.pdf
40. MottetN,BellmuntJ,BriersEetal.EAU‐ESTRO‐SIOGGuidelinesonProstate
Cancer.http://uroweb.org/wp‐content/uploads/EAU‐Guidelines‐Prostate‐Cancer‐2016.pdf
41. VickersAJ,CroninAM,AusGetal.Apanelofkallikreinmarkerscanreduceunnecessarybiopsyforprostatecancer:datafromtheEuropeanRandomizedStudyofProstateCancerScreeninginGöteborg,Sweden.BMCMed.2008Jul;6:19.
42. VickersAJ,CroninAM,AusGetal.Impactofrecentscreeningonpredictingtheoutcomeofprostatecancerbiopsyinmenwithelevatedprostate‐specificantigen:datafromtheEuropeanRandomizedStudyofProstateCancerScreeninginGothenburg,Sweden.Cancer.2010Jun1;116(11):2612‐20.
43. VickersA,CroninA,RoobolMetal.Reducingunnecessarybiopsyduringprostatecancerscreeningusingafour‐kallikreinpanel:anindependentreplication.JClinOncol.2010May20;28(15):2493‐8.
44. VickersAJ,CroninAM,RoobolMJetal.Afour‐kallikreinpanelpredictsprostatecancerinmenwithrecentscreening:datafromtheEuropeanRandomizedStudyofScreeningforProstateCancer,Rotterdam.ClinCancerRes.2010Jun15;16(12):3232‐9.
45. GuptaA,RoobolMJ,SavageCJetal.Afour‐kallikreinpanelforthepredictionofrepeatprostatebiopsy:datafromtheEuropeanRandomizedStudyofProstateCancerscreeninginRotterdam,Netherlands.BrJCancer.2010Aug;103(5):708‐14.
46. EpsteinJI,AllsbrookWC,AminMBetal.The2005InternationalSocietyofUrologicalPathology(ISUP)consensusconferenceonGleasongradingofprostaticcarcinoma.AmJSurgPathol.2005Sep;29(9):1228‐42.

25
BioReferenceLaboratories,Inc.(anOPKOHealthCompany)481EdwardH.RossDrive,ElmwoodPark,NJ07407
47. BryantRJ,SjobergDD,VickersAJetal.Predictinghigh‐gradecanceratten‐coreprostatebiopsyusingfourkallikreinmarkersmeasuredinbloodintheProtecTstudy.JNatlCancerInst.2015Apr11;107(7).
48. BraunK,SjobergDD,VickersAJ,etal.AFour‐kallikreinPanelPredictsHigh‐gradeCanceronBiopsy:IndependentValidationinaCommunityCohort.EurUrol2016Mar;69(3):505‐511.
49. StattinP,VickersAJ,SjobergDDetal.Improvingthespecificityofscreeningforlethalprostatecancerusingprostate‐specificantigenandapanelofkallikreinmarkers:anestedcase–controlstudy.EurUrol.2015Aug;68(2):207‐13.





























