Embed Size (px)
Citation preview

T H E 2 01 6R U S H N E U R O S C I E N C E R E V I E W

“ Medicine is a science, but there is also an art, and
the approach has to be customized depending on
the patient, their background, and where they are
in their lives. We help them understand what’s in
the future, and we help walk this path with them.” – Aikaterini Kompoliti, MD, movement disorders specialist

T H E 2 0 16 R U S H N E U R O S C I E N C E R E V I E WFaculty editors Sepehr Sani, MD Aimee Szewka, MD
CHAIRPERSONS’ LETTER 2
NEUROSCIENCES AT RUSH: AT A GLANCE 4
PRIMARY AND ASSOCIATED FACULTY
Department of Neurological Sciences 6
Department of Neurological Surgery 9
RESIDENTS AND FELLOWS
Department of Neurological Sciences 10
Department of Neurological Surgery 11
ORIGINAL ARTICLES
Stem Cell Therapy for Traumatic Spinal Cord Injury 12Christopher D. Witiw, MD; Richard G. Fessler, MD, PhD
The Join App for Acute Stroke: Mobile Real-Time Tracking of Patients 17 With Instant Interteam CommunicationDaniel J. DiLorenzo, MD, PhD, MBA; Lee A. Tan, MD; Danilo Marques Nogueira, MD; Kiffon M. Keigher, ACNP; Demetrius K. Lopes, MD
Deep Brain Stimulation for Major Depression 22Joshua T. Wewel, MD; Ryan B. Kochanski, MD; Sepehr Sani, MD
SELECT PUBLISHED ARTICLES
Outcome Following Intracranial Hemorrhage Associated With Novel Oral Anticoagulants 26Manish K. Kasliwal, MBBS, MCh; Nicholas G. Panos, PharmD, BCPS; Lorenzo F. Muñoz, MD; Roham Moftakhar, MD; Demetrius K. Lopes, MD; Richard Byrne, MD
Resecting Critical Nodes From an Epileptogenic Circuit in Refractory Focal-Onset 31 Epilepsy Patients Using Subtraction Ictal SPECT Coregistered to MRIAbhijay Jalota, MD; Marvin A. Rossi, MD, PhD; Volodymyr Pylypyuk, CNMT, NMTCB, ARRT(N); Michael Stein, MD; Travis Stoub, PhD; Antoaneta Balabanov, MD; Donna Bergen, MD; Adriana Bermeo, MD; Esmeralda Park, MD; Michael Smith, MD; Richard Byrne, MD
Exercise Improves Cognition in Parkinson Disease: The PRET-PD Randomized Clinical Trial 41Fabian J. David, PhD; Julie A. Robichaud, PT, PhD; Sue E. Leurgans, PhD; Cynthia Poon, PhD; Wendy M. Kohrt, PhD; Jennifer G. Goldman, MD, MS; Cynthia L. Comella, MD; David E. Vaillancourt, PhD; Daniel M. Corcos, PhD
VOLUME AND QUALITY DATA
Volumes, neurology and neurological surgery 48
Mortality, neurology and neurological surgery 49
Quality indicators, stroke 49
PUBLICATIONS 50
RESEARCH GRANTS 61
LEGACY INTERVIEW: Offering the Best Service 63Retired neurology chairperson Jacob Fox, MD, and fellow general neurologist Allison Weathers, MD, talk about the ingredients for a successful neurological sciences department.

2 THE 2016 RUSH NEUROSCIENCE REVIEW
Chairpersons’ Letter
You may notice something different about this year’s letter: After 26 years of distinguished service to Rush, our esteemed colleague Jacob Fox has retired. (See page 63 for an interview with Dr Fox.) And I am pleased to introduce you to my new fellow chairperson and coauthor, Igor Koralnik, who has accepted the position of chairperson for the Department of Neurological Sciences.
If you will permit me, a brief introduction: Koralnik has spent the last 25 years studying how viruses affect the nervous system in immunosuppressed individuals, with an emphasis on progressive multifocal leukoencephalopathy. In bringing his clinical expertise in neuroimmunology, along with his research laboratory and fellowship to Rush, he will continue Rush’s strong tradition of patient care, education, and translational research.
As you know, this intersection of education, patient care, and research is particularly critical now as we face an aging population and a national focus on cost-effective health management strategies. Neuroscientists are critical to the management of complex chronic conditions—and to spreading this expertise to the many areas in our country and
beyond that lack neurologists and neurosurgeons. Rush’s focus on translational research, in particular, is a key component to fulfilling these needs.
Here are several examples from the last year at Rush of clinical progress toward these goals:
Movement disorders fellowship and research: Our movement disorders program is one of the few that focuses on the nonmotor aspects of Parkinson’s disease along with the motor aspects, including training interns and residents in both aspects of the disease. In recognition of our program’s strengths, the Michael J. Fox Foundation recently announced that Rush was one of only six academic medical centers selected to host a Safra Fellowship in Movement Disorders. The fellowship is designed to further the growth of movement disorders specialists and potential clinical breakthroughs.
Telehealth access to epilepsy specialists: Rush’s epilepsy program, in collaboration with the Epilepsy Foundation of North/Central Illinois, is developing portable communication technologies that will allow epileptologists to take specialized epilepsy care to refractory patients in rural communities that lack this expertise—and to help these patients avoid going to the ER. Two examples of these technologies are micro-EEGs that can be put on a patient’s head within minutes and relay information remotely, and biosensors that can be placed on the body to watch a patient walk around in their own homes in case of falls.
The program is also developing implantable nanotechnology the size of a pin tip. Currently in preclinical stages, this patented technology can be injected into the brain to facilitate sensing early seizure activity. This technology can amplify both stimulation therapy in tandem with therapeutic drug delivery to stabilize otherwise uncontrolled seizures.
Expanding quick access to stroke neurologists: For the last 5 years, our stroke program has been busy demonstrating the great possibilities for raising the health of a whole community through telemedicine. The TeleStroke program will soon have 13 affiliated hospitals participating in its stroke network, the largest such network in the Chicago area.
Igor Koralnik, MD (left) and Richard Byrne, MD (right).

Chairpersons’ Letter 3
Stroke neurologists from Rush have remotely examined more than 2700 stroke patients at community hospitals across Chicago—an indication of the tremendous need for stroke neurologists not only in rural areas, but in urban settings as well.
The team has honed their processes for quickly treating these emergencies to the point where their door-to-needle times are routinely under one-third of the national average for this measure. (See page 17 for more on the stroke team’s processes and page 49 for quality data.)
Alzheimer’s NIA research funding: The National Institute on Aging has recently awarded the Rush Alzheimer’s Disease Center $14.3 million over the next 5 years. This award is a renewal of continuous grant funding—now extending to 30 years—for the center that has supported the collection of pathology samples and health data from longitudinal research of individuals with and without Alzheimer’s.
This information is available to researchers at Rush, 11 strategic partner programs at other major academic medical centers, and other researchers worldwide. In the last 5 years alone, researchers in the Alzheimer’s center have published more than 225 papers in peer-reviewed journals.
Extending neurosurgery access: Our Department of Neurological Surgery has strengthened its affiliation with John H. Stroger, Jr Hospital, Chicago’s public hospital and Rush’s neighbor in the Illinois Medical District. The affiliation involves a collaboration as the primary academic partner of the Stroger Division of Neurosurgery. In the spirit of the larger academic affiliation between Rush and Stroger, Rush neurosurgery plans to offer more subspecialty clinical services to patients at this safety net hospital while improving the educational experience for Rush neurosurgery residents.
And our faculty continue to further their respective fields in a variety of other ways:
• Neurologist Neelum Aggarwal, MD, received the 2016 Women in Science Award from the American Medical Women’s Association in recognition of her exceptional contributions to medical science, and specifically women’s health, through her research and leadership. Among Aggarwal’s research interests is the intersection between cognitive decline and cardiology among women, an interest that is manifest in the neurocognitive cardiology clinic that is part of the Rush Heart Center for Women.
• Rush hosted several conferences last year, including the first World Live Neurovascular conference to be held in the United States in June 2015. Co-directed by neuroendovascular surgeon Demetrius Lopes, MD, the conference showcased new developments in neurointerventional and cerebrovascular surgery. Rush also hosted the American Association of Neurological Surgeons annual conference and the First International Brain Mapping Course.
• Our spine neurosurgeons continue to pursue new treatment possibilities for spine patients, particularly in the area of spinal cord injuries. Richard Fessler, MD, PhD, is leading an exciting stem cell therapy trial for traumatic spinal cord injuries (see page 12 for more).
We invite you to read more about the contributions of our departments to further the reach of translational research so that it is truly bench to bedside—whether the bedside is at Rush, in community hospitals, in rural communities across Illinois, or even around the world.
Regards,
Richard Byrne, MDChairperson, Department of Neurological Surgery
The Roger C. Bone, MD, Presidential Chair
Igor Koralnik, MDChairperson, Department of Neurological Sciences
The Jean Schweppe Armour Professor of Neurology

4 THE 2016 RUSH NEUROSCIENCE REVIEW
Neurosciences at Rush: At a Glance
32 28 67 54 10 General Neuro Psychiatric Rehabilitation Epilepsy neurology ICU (adult)
Beds
Inpatient Facilities
For additional volume and quality data, see pages 48-49.
Department of Neurological Sciences•Rush Alzheimer’s Disease Center
•Section of Cerebrovascular Disease
•Section of Clinical Neurophysiology and Epilepsy
•Section of Cognitive Neurosciences
•Section of Critical Care Neurology
•Section of General Neurology
•Section of Movement Disorders
•Rush Multiple Sclerosis Center
•Section of Pediatric Neurology
•Section of Neuromuscular Diseases
•Section of Neuro-oncology
•Section of Neuro-ophthalmology
Department of Neurological Surgery•Neuroendovascular Surgery Center
•Skull Base and Pituitary Surgery Center
•Spine and Back Care
Attending physicians
120Residents and fellows
57Advanced practice nursesand physician assistants
25
Neurology outpatient visits28 709
Neurology inpatient discharges2 717
Neurological surgery outpatient visits (brain)3 638
Neurological surgery outpatient visits (spine)5 068

Neurosciences at Rush: At a Glance 5
NIA-designated Alzheimer’s research center: The Rush Alzheimer's Disease Center is a designated Alzheimer's disease research center, funded by the National Institute on Aging of the U.S. National Institutes of Health.
No. 2 in the Nation: In 2015, Rush received the University HealthSystem Consortium’s Quality Leadership Award, ranking No. 2 among more than 100 academic medical centers.
Comprehensive Stroke Center: The Rush stroke program is certified by the Joint Commission as a comprehensive stroke center.
CARF accreditation: Rush’s rehabilitation program, including general inpatient and stroke specialty rehab, is fully accredited by the Commission on Accreditation of Rehabilitation Facilities.
Nursing Excellence: Rush has earned Magnet status—the highest honor in nursing—four times from the American Nurses Credentialing Center.
AAHRPP accreditation: Rush’s research program is fully accredited by the Association for the Accreditation of Human Research Protection Programs.
Huntington’s Disease Center of Excellence: The Huntington’s Disease Society of America named Rush one of its Centers of Excellence for 2015.

6 THE 2016 RUSH NEUROSCIENCE REVIEW
Primary and Associated Faculty (2015)
Department of Neurological SciencesChairperson: Igor Koralnik, MD
Alzheimer’s disease
Neelum Aggarwal, MD Konstantinos Arfanakis, PhD Zoe Arvanitakis, MD Lisa Barnes, PhD David Bennett, MD Patricia Boyle, PhD
Aron Buchman, MD Ana Capuano, PhD Robert Dawe, PhD Debra Fleischman, PhD S. Duke Han, PhD Bryan James, PhD
Sue Leurgans, PhD Sukriti Nag, MD, PhD Julie Schneider, MD Raj Shah, MD Rita Shapiro, DO Robert Wilson, PhD
Lei Yu, PhD
Cerebrovascular disease
Laurel Cherian, MD James Conners, MD, MS Shawna Cutting, MD Michael Kelly, MD Vivien Lee, MD Sarah Song, MD
Clinical neurophysiology and epilepsy
Antoaneta Balabanov, MD Donna Bergen, MD Lawrence Bernstein, MD Adriana Bermeo-Ovalle, MD Thomas Hoeppner, PhD Maggie McNulty, MD
Serge Pierre-Louis, MD Marvin Rossi, MD, PhD Michael Smith, MD
Not pictured: Esmeralda Park, MD Travis Stoub, PhD
Not pictured: Denis Evans, MDChristopher Gaiteri, PhDJingyun Yang, PhD

Faculty (2015) 7
Critical care neurology
Thomas Bleck, MD Torrey Boland, MD Katharina Busl, MD Rajeev Garg, MD Diana Goodman, MD Sayona John, MD
George Lopez, MD, PhD Sebastian Pollandt, MD
General neurology
Jonathan Cheponis, MD Jacob Fox, MD Carrie Grouse, MD Steven Lewis, MD Megan Shanks, MD Jordan Topel, MD
Allison Weathers, MD Felise Zollman, MD
Movement disorders
Sharlet Anderson, PhD Brandon Barton, MD, MS Bryan Bernard, PhD Cynthia Comella, MD Christopher Goetz, MD Jennifer Goldman, MD, MS
Deborah Hall, MD, PhD Aikaterini Kompoliti, MD Gian Pal, MD, MS Kathleen Shannon, MD Glenn Stebbins, PhD Leonard Verhagen, MD, PhD
Multiple sclerosis
Roumen Balabanov, MD Rajendra Goswami, PhD Dusan Stefoski, MD
Not pictured: Robert Wright, MD
Not pictured: Melany Danehy, MD Bichun Ouyang, PhD
Not pictured: Michael Ko, MD

8 THE 2016 RUSH NEUROSCIENCE REVIEW
Neurobiology
Yaping Chu, PhD Bin He, PhD Jeffrey Kordower, PhD Kalipada Pahan, PhD Sylvia Perez, PhD
Neuroinfectious disease
Igor Koralnik, MD
Neuromuscular disease
Rabia Malik, MD Matthew Meriggioli, MD Irwin Siegel, MD Madhu Soni, MD
Neuro-oncology
Nina Paleologos, MD
Neuro-ophthalmology
Thomas Mizen, MD Aimee Szewka, MD
Pediatric neurology
Elizabeth Berry-Kravis, MD, PhD Peter Heydemann, MD Lubov Romantseva, MD
Associated faculty at Rush University Medical Center
Christopher Grote, PhD Neha Kramer, MD Richard Peach, PhD Neuropsychology Neuropalliative care Audiology and speech language pathology
Not pictured: Malabendu Jana, PhD Susanta Mondal, PhD Elliott Mufson, PhD Dan Nicholson, PhD Avik Roy, PhD Dustin Wakeman, PhD

Faculty (2015) 9
Primary and Associated Faculty (2015)
Department of Neurological SurgeryChairperson: Richard Byrne, MD
Richard Byrne, MD Michael Chen, MD R. Webster Crowley, MD Harel Deutsch, MD Richard Fessler, MD, PhD Ricardo Fontes, MD, PhD
Demetrius Lopes, MD Lorenzo Muñoz, MD John O’Toole, MD, MS Sepehr Sani, MD Vincent Traynelis, MD
Research faculty
Roberta Glick, MD Terry Lichtor, MD, PhD Richard Penn, MD
Associated faculty at Rush University Medical Center
Pete Batra, MD Aidnag Diaz, MD, MPH Sheila Dugan, MD R. Mark Wiet, MD Otorhinolaryngology Radiation oncology Physical medicine Neurotology and rehabilitation
Associated clinical faculty*
Jerry Bauer, MD Tibor Boco, MD George Bovis, MD Martin Herman, MD, PhD Juan Jimenez, MD
Martin Luken, MD Patricia Raksin, MD Szymon Rosenblatt, MD John Ruge, MD Andrew Zelby, MD
*Primary appointment is not at Rush University Medical Center
Not pictured: David Rothenberg, MD, anesthesiology Mary Sturaitis, MD, anesthesiology

10 THE 2016 RUSH NEUROSCIENCE REVIEW
Residents and Fellows (2015)
Department of Neurological Sciences
Residents
Zeeshan Ali, MDMedical school: Indiana University School of Medicine
Bahar Beaver, MDMedical school: University of Oklahoma College of Medicine at Tulsa
Ankush Bhatia, MDMedical school: Rush Medical College
Hunan Chaudhry, MDMedical school: Rush Medical College
Christine Chuck, MDMedical school: Indiana University School of Medicine
Dana Cooper, MDMedical school: Loyola University Chicago Stritch School of Medicine
Kathryn Ess, MDMedical school: Indiana University School of Medicine
Avram Fraint, MDMedical school: Rush Medical College
Sabreena Gillow, MDMedical school: University of Colorado School of Medicine
Breyanna Grays, MDMedical school: Indiana University School of Medicine
Ryan Hanson, MDMedical school: Rush Medical College
Christian Hernandez, MDMedical school: Louisiana State University School of Medicine–
New Orleans
Emily Hill, MDMedical school: Rush Medical College
Zehra Husain, MDMedical school: Wayne State University School of Medicine
Samantha LoRusso, MDMedical school: Wake Forest University School of Medicine
Brian Marcus, MDMedical school: Medical College of Wisconsin
Colin McLeod, MDMedical school: University of Florida College of Medicine
Michael Mercurio, MDMedical school: State University of New York Upstate College of
Medicine
Kristin Miller, MDMedical school: George Washington University School of
Medicine and Health Sciences
Jeremy Pruzin, MDMedical school: The Chicago Medical School at Rosalind Franklin
University of Medicine and Science
Benjamin Savage, DOMedical school: Chicago College of Osteopathic Medicine,
Midwestern University
Dan Schachter, MDMedical school: New York Medical College
Ruby Upadhyay, MDMedical school: Rush Medical College
David Whitney, MDMedical school: Temple University School of Medicine
Fellows
Justin Abraham, MDMedical school: Penn State College of Medicine Residency: Thomas Jefferson University Hospital
Hesham Allam, MDMedical school: Ain Shams University Faculty of MedicineResidency: Saint Louis University Hospital
Ameer Al Wafai, MDMedical school: Beirut Arab University School of MedicineResidency: University of Tennessee Health Science Center
Fatmah Al Zahmi, MBBSMedical school: United Arab Emirates University Residency: University of Connecticut
Meagan Bailey, MDMedical school: Texas Tech University Health Sciences CenterResidency: Wake Forest School of Medicine
Ian Bledsoe, MDMedical school: University of Pittsburgh School of MedicineResidency: Stanford Hospital and Clinics
Kyle Carpenter, DOMedical school: Des Moines University College of Osteopathic
MedicineResidency: University of Kansas Medical Center
Mohamad Ezzeldin, MDMedical school: Cairo University Faculty of MedicineResidency: University of Texas Medical Branch

Residents and Fellows (2015) 11
Mineshkumar Morker, MDMedical school: Northwestern University Feinberg School of
MedicineResidency: Northwestern University Feinberg School of Medicine
Nicholas Osteraas, MDMedical school: George Washington University School of
Medicine and Health SciencesResidency: Rush University Medical Center
Atul Ramesh, MDMedical school: University of Toledo College of MedicineResidency: Albert Einstein College of Medicine
Kapil Sachdeva, MDMedical school: Northwestern University Feinberg School of
MedicineResidency: Northwestern University Feinberg School of Medicine
Varoon Thavapalan, MDMedical school: John A. Burns School of MedicineResidency: Thomas Jefferson University Hospital
Jessica Walter, MDMedical school: Georgetown University School of Medicine Residency: Mount Sinai Hospital, New York
Department of Neurological Surgery
Residents
Owoicho Adogwa, MDMedical school: Vanderbilt University School of Medicine
Sumeet Ahuja, MDMedical school: Indiana University School of Medicine
Bledi Brahimaj, MDMedical school: University of Cincinnati College of Medicine
Daniel DiLorenzo, MD, PhD, MBAMedical school: Harvard Medical School
Daniel Eddelman, MDMedical school: Indiana University School of Medicine
Carter Gerard, MDMedical school: University of Louisville School of Medicine
Manish Kasliwal, MBBS, MCh Medical school: All India Institute of Medical Sciences
Mena Kerolus, MDMedical school: University of Missouri–Kansas City School of
Medicine
Ryan Kochanski, MDMedical school: Wayne State University School of Medicine
Joseph Molenda, MDMedical school: Johns Hopkins University School of Medicine
Stephan Munich, MDMedical school: University at Buffalo School of Medicine and
Biomedical Sciences
Ravi Nunna, MDMedical school: University of Cincinnati College of Medicine
Lee Tan, MDMedical school: Indiana University School of Medicine
Joshua Wewel, MDMedical school: University of Nebraska College of Medicine
Fellow
Danilo Marques Nogueira, MDMedical school: Federal University of Grande Dourados, BrazilResidency: Hospital de Base do Distrito Federal, Brazil

12 THE 2016 RUSH NEUROSCIENCE REVIEW
STEM CELL THERAPY FOR TRAUMATIC SPINAL CORD INJURY
Christopher D. Witiw, MD; Richard G. Fessler, MD, PhD
Author Affiliations: Department of Neurological Surgery, Rush University Medical Center, Chicago, Illinois (Drs Witiw and Fessler), and Division of Neurosurgery, Department of Surgery, University of Toronto, Toronto, Ontario, Canada (Dr Witiw).
Corresponding Author: Richard G. Fessler, MD, PhD, Department of Neurological Surgery, Rush University Medical Center, 1725 W Harrison St, Suite 855, Chicago, IL 60612 ([email protected]).
Introduction
The personal and societal impact of traumatic spinal cord injury (SCI) is often tremendous.1 Affected individuals are disproportionately young and healthy, and this devastating injury is common. Recent estimates suggest an annual incidence of 30 to 49 cases per million in North America.2 This incidence has compelled clinicians and basic scientists to search for strategies to optimize neurological recovery after these life-changing events. One area of active research is stem cell transplantation therapy, which holds promise to enhance sensorimotor recovery and improve functional outcomes through multiple mechanisms of neural protection and plasticity.
In this review, we summarize the current state of knowledge and outline recent developments in stem cell therapy for SCI. The Department of Neurological Surgery at Rush University Medical Center is actively leading research in this important domain, and we conclude with a description of Rush’s current contribution to this important area of research.
Current State of Knowledge
Presently, stem cell therapy for traumatic SCI is focused on 3 specific cell types: (1) mesenchymal stem cells (MSCs), (2) embryonic stem cells (ESCs), and (3) induced pluripotent stem cells (IPSCs). Each has been shown to hold promise for enhancing recovery through neuroprotection, axonal regeneration, and cellular replacement at the injury site.
Mesenchymal Stem Cells
The sources of adult mesenchymal stem cells (MSCs) are numerous, but they are most commonly derived from bone marrow and after appropriate processing may be stimulated for neuroglial differentiation.3 These differentiated cells may then be transplanted into the injured spinal cord of the same patient from whom they came. It is generally thought that MSCs act primarily through modulation of the immunogenic response, a part of the secondary injury phase of SCI that occurs after the initial traumatic insult. By preventing the deleterious effects of T-cell activation at the injury site, MSCs exert a neuroprotective effect at the cellular level. This theory is supported by observations of significantly higher levels of neuron preservation and axonal myelination in animal models of traumatic SCI treated with MSCs.4,5 These findings suggest a potential for the enhancement of neurological function after injury, and a number of studies conducted on rat models have identified this effect after implantation of MSCs in the acute and subacute phases after injury.6
Richard Fessler, MD, PhD

Stem Cell Therapy for Traumatic Spinal Cord Injury 13
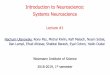
Figure 1. The generation of oligodendrocytes, neurons, and astrocytes through differentiation of embryonic stem cells to unipotent cells. Adapted with permission from Nandoe Tewarie et al.10
The encouraging results of animal investigations have been translated into a number of human trials. Here, the results have been mixed, but some have found clinically meaningful improvement in neurological function in certain patients after MSC therapy. The neuroprotectant properties of MSCs are likely to have the greatest benefit during the early phases of the secondary injury process, but because most human studies have focused on the chronic phase of injury, the full potential of MSCs may not have been observed.7,8 The authors of 1 particular trial reported that nearly one-third of their study cohort with loss of all sensorimotor function treated in the acute or subacute period with MSCs regained a clinically significant amount of neurological function.9 This finding suggests that timing of administration may be an important factor, although the results should be interpreted with caution because the single-arm nature of the study does not allow for a clear distinction between gains attributable to therapy and those resulting from the evolution of and recovery from the injury. At present, the efficacy of MSCs for treatment of SCI remains to be fully defined, and further study is needed.
Embryonic Stem Cells
ESCs are generally classified as those of the inner cell mass within a blastocyst. These cells are pluripotent cells that differentiate into multipotent cells of the 3 germ layers: ectodermal (the origin of neural tissue), mesodermal, and endodermal.10 During the differentiation process, progenitor cells that are capable of self-renewal are formed. Neural progenitors become the neuron and glial cells of the central nervous system, and it is these cells that are of specific interest for SCI therapies. The process of differentiation is illustrated in Figure 1.10
Implanted progenitor ESCs have been shown to have neuroprotectant properties by acting to reduce inflammation and mitigate cell death, along with axonal regeneration through remyelination following the injury.11,12 Although these effects have been noted with MSCs, a further and potentially substantial advantage of ESCs over adult MSCs is their potential to act as cellular replacements. Whereas adult MSCs do not appear to harbor this ability,13 ESC-derived neurons have been shown to survive and integrate after injection into animal models of SCI.14
The synergistic combination of neuroprotective effects in the earlier stages of injury coupled with cellular replacement has led to excitement and active research in both animal models and human trials of ESCs for the treatment of SCI. However, the use of these cells is not without challenges. One particular issue with ESCs is immunogenicity. ESCs are not autologous (adult MSCs are), and thus transplantation of ESCs stimulates an immune response that places the transplanted cells at risk for rejection. For this reason, all patients receiving ESCs require immunosuppression. Furthermore, there have been concerns regarding the potential for teratogenicity with ESC implantation because of uncontrolled cellular proliferation.15 However, this concern has been greatly reduced through differentiation of the ESCs to neural progenitor cells prior to implantation. Ethical dilemmas are also commonplace when discussing ESCs. The concerns largely focus on the creation of human embryos specifically for scientific research and the identification of the point when a human life begins.16
Notwithstanding these challenges, the effects of ESCs on inflammation, axonal remyelination, and cellular replacement have led to significant neurological improvement after SCI in animal models.17 This finding has spurred active research in human SCI. A phase I/IIa study of ESC therapy for traumatic thoracic SCI (ClinicalTrials.gov identifier NCT01321333) was initiated in 2011 and reached completion in mid-2015, but the publication of the results is pending. Around the time of completion of this trial, another study of ESC therapy following traumatic SCI was initiated. Rush University Medical Center is currently involved with this promising phase I/IIa multicenter study, and the details are outlined in the final section of this review.
Trophoblast Inner Cell Mass
Blastocyst
EmbryonicStem Cell
Progenitor
Neural Progenitor
Neuroblast Glioblast
Oligodendrocyte
Self-renewal
Transdifferentiation?
Astrocyte
Totipotent:can become any but a placenta cell
Pluripotent:can become any cell within a germ layer
Multipotent:can become any cell within a lineage
Unipotent:can become one specific cell
Neuron

14 THE 2016 RUSH NEUROSCIENCE REVIEW
Induced Pluripotent Stem Cells
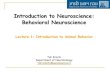
IPSCs are derived from adult cells that are “reprogrammed” to behave as immature stem cells, which differentiate into cells of any germ line, including neurons, oligodendrocytes, and astrocytes.18 Figure 2 summarizes the harvesting and reprogramming process.19 The cells are easily accessible, and because they are autologous, immunosuppression is not needed. The ethical issues inherent with embryonic cells are avoided because IPSCs are derived from adult cells instead. Because these cells appear to behave similarly to ESCs, they may offer the same benefits. Encouraging results suggest improved motor function after IPSC therapy in animal models of SCI.20,21 Currently, no human trials are underway to assess the role of IPSCs in SCI; however, future research in this area is likely.
The Role of Rush University Medical Center
The Department of Neurological Surgery at Rush University Medical Center is currently at the forefront of clinical trials of stem cell therapy in traumatic SCI. Rush is actively recruiting patients as a part of the SCiStar study (ClinicalTrials.gov identifier NCT02302157). This multicenter phase I/IIa open-label, single-arm study is testing AST-OPC1, a population
of oligodendrocyte progenitor cells derived from human ESCs, as a potential therapy to enhance neurological recovery following SCI.
Potential Reparative Mechanisms
Oligodendrocyte progenitor cells have been shown to enhance survival and regrowth of axons following SCI through neurotrophic factor production, stimulation of vascularization, and remyelination of denuded axons.22,23 Specific testing involving AST-OPC1 cells injected in rodent models 7 days after SCI revealed appropriate in situ differentiation into mature oligodendrocytes and encouraging findings of reduced spinal cord cavitation, remyelination, and, most important, enhanced functional recovery.12
Study Recruitment
The overall aim of the SCiStar study is to test the safety of stem cell therapy with AST-OPC1 and to evaluate if the neurological gains observed in animal models may be translated to humans. To this end, 13 participants will be recruited, each between 18 and 65 years of age. Those with a blunt traumatic SCI within the past 14 to 30 days are eligible. The clinical neurological
Figure 2. Derivation of induced pluripotent stem cells. Autologous cells from multiple sources from the injured patient may be used to prepare neural cells for reimplantation into the injured spinal cord through the use of reprogramming factors. Adapted with permission from Khazaei et al.19
Somatic Cells
Fibroblasts
Keratinocytes
Blood Cells
Adipose Stem Cells
Neural Progenitor Cells
IPSC-Derived Cells
Patient With Spinal Cord Injury
Neural Progenitor Cells
Oligodendrocytes
Neurons
Astrocytes
Mesenchymal Stromal Cells

Stem Cell Therapy for Traumatic Spinal Cord Injury 15
exam must be consistent with a sensorimotor complete traumatic spinal cord injury, and the last fully preserved single neurological level must be between C5 and C7. In effect, this requirement represents a state of absent neurological function below the level of injury in the cervical spine. These individuals are profoundly affected by the injury, and it is here where the greatest potential gains are thought to be achievable.
Stem Cell Transplantation
These progenitor cells are differentiated from an undifferentiated population of human embryonic stem cells after a controlled and specialized differentiation protocol.24 The early-stage oligodendrocyte progenitor cells are cryopreserved, forming the AST-OPC1 investigational product. AST-OPC1 is injected directly into the spinal cord parenchyma at the site of injury. This procedure requires surgical removal of the lamina overlying the injured segment of the spinal cord and opening of the dura mater to provide access for administration of AST-OPC1 through a single-use, sterile syringe (Figure 3). Each participant will receive a single dose, and the study will follow a sequential dose escalation protocol, testing 3 escalated dose cohorts ranging from 2 million cells to 20 million cells.
Outcomes and Follow-up
The treatment and observation period is set for 12 months, and the total duration of the study is planned to be approximately 3 years. The primary end points are focused on safety and include tracking the incidence and severity of adverse events as well as untoward changes in serum laboratory values and changes at the injection site through monitoring with periodic magnetic resonance imaging studies. The secondary end points pertain to efficacy of the treatment and are focused on changes in sensorimotor neurological function. Finally, exploratory testing will include changes in aspects of daily living and lower urinary tract and bowel function over the 12-month follow-up period. The participants will then be enrolled in a separate long-term safety protocol that is planned for a duration of 14 years.
Conclusions
Stem cells hold tremendous promise to enhance functional neurological recovery after traumatic SCI through mechanisms of neuroprotection, axonal regeneration, and cellular
replacement. Future SCI management is quite likely to involve stem cell transplantation therapies; however, much more remains to be learned. Investigations such as the SCiStar study and the contributions made by the Department of Neurological Surgery at Rush may play an important role in mitigating the devastating impact of the injury.
Figure 3. Transplantation of AST-OPC1 into the spinal cord parenchyma at the site of injury through the surgical exposure with a fixed-position sterile syringe.

16 THE 2016 RUSH NEUROSCIENCE REVIEW
References1. Ackery A, Tator C, Krassioukov A. A global perspective on spinal cord injury epidemiology. J Neurotrauma. 2004;21(10):1355-1370.
2. Cripps RA, Lee BB, Wing P, Weerts E, Mackay J, Brown D. A global map for traumatic spinal cord injury epidemiology: towards a living data repository for injury prevention. Spinal Cord. 2011;49(4):493-501.
3. Bossolasco P, Cova L, Calzarossa C, et al. Neuro-glial differentiation of human bone marrow stem cells in vitro. Exp Neurol. 2005;193(2):312-325.
4. Beyth S, Borovsky Z, Mevorach D, et al. Human mesenchymal stem cells alter antigen-presenting cell maturation and induce T-cell unresponsiveness. Blood. 2005;105(5):2214-2219.
5. Ankeny DP, McTigue DM, Jakeman LB. Bone marrow transplants provide tissue protection and directional guidance for axons after contusive spinal cord injury in rats. Exp Neurol. 2004;190(1):17-31.
6. Tetzlaff W, Okon EB, Karimi-Abdolrezaee S, et al. A systematic review of cellular transplantation therapies for spinal cord injury. J Neurotrauma. 2011;28(8):1611-1682.
7. Bhanot Y, Rao S, Ghosh D, Balaraju S, Radhika CR, Satish Kumar KV. Autologous mesenchymal stem cells in chronic spinal cord injury. Br J Neurosurg. 2011;25(4):516-522.
8. Kishk NA, Gabr H, Hamdy S, et al. Case control series of intrathecal autologous bone marrow mesenchymal stem cell therapy for chronic spinal cord injury. Neurorehabil Neural Repair. 2010;24(8):702-708.
9. Yoon SH, Shim YS, Park YH, et al. Complete spinal cord injury treatment using autologous bone marrow cell transplantation and bone marrow stimulation with granulocyte macrophage-colony stimulating factor: phase I/II clinical trial. Stem Cells. 2007;25(8):2066-2073.
10. Nandoe Tewarie RS, Hurtado A, Bartels RH, Grotenhuis A, Oudega M. Stem cell-based therapies for spinal cord injury. J Spinal Cord Med. 2009;32(2):105-114.
11. Salewski RP, Mitchell RA, Shen C, Fehlings MG. Transplantation of neural stem cells clonally derived from embryonic stem cells promotes recovery after murine spinal cord injury. Stem Cells Dev. 2015;24(1):36-50.
12. Keirstead HS, Nistor G, Bernal G, et al. Human embryonic stem cell-derived oligodendrocyte progenitor cell transplants remyelinate and restore locomotion after spinal cord injury. J Neuroscience. 2005;25(19):4694-4705.
13. Alexanian AR, Kwok WM, Pravdic D, Maiman DJ, Fehlings MG. Survival of neurally induced mesenchymal cells may determine degree of motor recovery in injured spinal cord rats. Restor Neurol Neurosci. 2010;28(6):761-767.
14. Deshpande DM, Kim YS, Martinez T, et al. Recovery from paralysis in adult rats using embryonic stem cells. Ann Neurol. 2006;60(1):32-44.
15. Shiras A, Chettiar ST, Shepal V, Rajendran G, Prasad GR, Shastry P. Spontaneous transformation of human adult nontumorigenic stem cells to cancer stem cells is driven by genomic instability in a human model of glioblastoma. Stem Cells. 2007;25(6):1478-1489.
16. de Miguel-Beriain I. The ethics of stem cells revisited. Adv Drug Deliv Rev. 2015;82-83:176-180.
17. Bottai D, Cigognini D, Madaschi L, et al. Embryonic stem cells promote motor recovery and affect inflammatory cell infiltration in spinal cord injured mice. Exp Neurol. 2010;223(2):452-463.
18. Park IH, Zhao R, West JA, et al. Reprogramming of human somatic cells to pluripotency with defined factors. Nature. 2008;451(7175):141-146.
19. Khazaei M, Siddiqui AM, Fehlings MG. The potential for iPS-derived stem cells as a therapeutic strategy for spinal cord injury: opportunities and challenges. J Clin Med. 2014;4(1):37-65.
20. Salewski RP, Mitchell RA, Li L, et al. Transplantation of induced pluripotent stem cell-derived neural stem cells mediate functional recovery following thoracic spinal cord injury through remyelination of axons. Stem Cells Transl Med. 2015;4(7):743-754.
21. Romanyuk N, Amemori T, Turnovcova K, et al. Beneficial effect of human induced pluripotent stem cell-derived neural precursors in spinal cord injury repair. Cell Transplant. 2015;24(9):1781-1797.
22. Zhang YW, Denham J, Thies RS. Oligodendrocyte progenitor cells derived from human embryonic stem cells express neurotrophic factors. Stem Cells Dev. 2006;15(6):943-952.
23. Faulkner J, Keirstead HS. Human embryonic stem cell-derived oligodendrocyte progenitors for the treatment of spinal cord injury. Transpl Immunol. 2005;15(2):131-142.
24. Nistor GI, Totoiu MO, Haque N, Carpenter MK, Keirstead HS. Human embryonic stem cells differentiate into oligodendrocytes in high purity and myelinate after spinal cord transplantation. Glia. 2005;49(3):385-396. ◆

The Join App for Acute Stroke 17
THE JOIN APP FOR ACUTE STROKE:Mobile Real-Time Tracking of Patients With Instant Interteam Communication
Daniel J. DiLorenzo, MD, PhD, MBA; Lee A. Tan, MD; Danilo Marques Nogueira, MD; Kiffon M. Keigher, ACNP; Demetrius K. Lopes, MD
Author Affiliations: Department of Neurological Surgery, Rush University Medical Center, Chicago, Illinois.
Corresponding Author: Daniel J. DiLorenzo, MD, PhD, MBA, Rush University Medical Center, Department of Neurological Surgery, 1725 W Harrison St, Suite 855, Chicago, IL 60612 ([email protected]).
Introduction
Concurrent with technological advances in therapy for acute emergencies has been the development of an infrastructure to support time-efficient delivery of care and the education of physicians, patients, and other stakeholders on the need and availability of promptly delivered therapy. Prompt treatment is particularly important in the management of ischemic conditions, such as myocardial infarction and stroke, in which irreversible organ damage begins shortly after onset of the condition. Over the past decade, to address this growing need, our institution has designed and implemented a multidisciplinary and multi-institutional workflow and infrastructure to support streamlined treatment of stroke patients. One novel component of this process is a mobile smartphone software application (app), the features, functionality, and benefits of which are the focus of this article.
More than two-thirds of physicians now regularly use smartphones,1 and mobile smartphone applications are beginning to be used broadly in disease management, in a variety of indications and spanning the chronology from prevention to management to long-term follow-up.2 In the cardiovascular and stroke space, recent promise has been shown across this time frame, including the use of digital health interventions in the reduction of vascular stroke risk factors,3 prevention of cardiovascular disease,4 diagnosis of stroke in telestroke centers,5 and postdischarge follow-up with automated assessment of modified Rankin scores.6 With the refinement of streamlined acute stroke management workflows and the realization that improved
interinstitutional communication, such as telestroke processes, improves outcomes, the time has come for the introduction of a new wave of technologies and processes that further improve communication and reduce time to treatment delivery.
Figure 1. A time series of screenshots from the Join app (Allm Inc) is shown, beginning with A and progressing in time from A to F. Each screenshot has a time stamp in the upper center. A mobile beacon with GPS tracking communicates the location of the patient. In this series, a patient is picked up and tagged by emergency medical services at 10:46 pm (A), followed by rapid transport from the suburbs by helicopter, over the congested Chicago highway and street system, to a helipad in the Illinois Medical District by 10:59 pm and then via ambulance to Rush University Medical Center minutes later (F).
A
D
B
E
C
F

18 THE 2016 RUSH NEUROSCIENCE REVIEW
Methods
Clinical Workflow for Acute Stroke Management
Our Stroke60 acute stroke workflow begins with a call or page from a physician from an outside facility who has a patient in whom a stroke is suspected. This communication is early and usually occurs immediately after the physician’s assessment of the patient, often before computed tomography (CT) imaging is performed. Our stroke neurologist receives the call, discusses the patient, reviews the imaging when available, and discusses
the case with the neurosurgeon or interventional neurologist to decide whether the patient meets criteria and would benefit from an intervention such as mechanical thrombectomy. Immediately upon an affirmative decision, a page is sent to the entire on-call stroke team, which includes the neurology and neurological surgery stroke fellows, the circulating nurse, the scrub technician, and the room technician. The procedure is scheduled emergently in the neurointerventional suite, and the anesthesia team on call is immediately notified. Others who are notified or paged include the neuroscience intensive care unit (NSICU) charge nurse to facilitate timely staffing and
bed availability for the patient after the procedure. This notification typically occurs 45 minutes prior to the arrival of the patient at our institution. A series of subsequent pages are sent at specific time points, including confirmation of the name and date of birth of the patient, an update with the medical record number of the patient, notification of the arrival of the transport team (helicopter or ambulance) to the referring facility, and a heads-up usually 15 minutes and then several minutes prior to arrival.
The patient is admitted upon entry through the emergency department bay doors with prompt placement of a wristband. A rapid neurological assessment, including the National Institutes of Health Stroke Scale, is performed; orders for emergent computed tomography (CT), CT arthrography, and CT perfusion study are entered; and the patient is wheeled directly to the CT scanner. On the basis of the examination, the patient’s ASPECTS (Alberta Stroke Program Early CT Score) assessment, the presence of large-vessel occlusion, and other factors including medical comorbidities, a decision whether to perform mechanical thrombectomy is made, and the patient is taken immediately to the neurointerventional suite or NSICU.
Figure 2. A, A time-stamp sequence for a Stroke60 patient from arrival at Rush University Medical Center to recanalization is shown, including the following events: arrival to hospital, start of CT/MRI imaging, end of CT/MRI imaging, entrance into angiography suite, and recanalization. B, The Rush University Medical Center stroke team, after waiting in the emergency department (ED) before arrival of the ambulance, meets the ambulance in the ED bay before the patient is unloaded, and assists in the unloading and expeditious transport of the patient through the ED directly to the CT scanner. C, The team in the neurointerventional suite after successful thrombectomy. D, Close-up photograph depicts the retrieved thrombus and the stent retriever.
A
C
B
D

The Join App for Acute Stroke 19
Mobile Smartphone Application
A customized mobile application called Join (Allm Inc) has been developed to further streamline our acute stroke workflow. The app provides the following helpful features: (1) real-time secure communication among team members, (2) automated time-stamping of events, (3) generation of a summary document in PDF for uploading into the electronic medical record (EMR), and (4) real-time monitoring and communication of patient’s exact position during transport using GPS. All events receive a time stamp that is visible to all team members, obviating the need for a recording person to be appointed and a specific clock to be chosen. Time-stamped events include “Time of Onset / Last Known Well,” “Time of tPA Administration,” “Time Consent Obtained,” “Time of Arrival / Door Time,” “Imaging Complete Time,” “Procedure Start Time,” “First Pass Time,” and “Recanalization Time.”
After the treatment process is completed and the patient is admitted to the NSICU, the information that was transmitted, with associated time stamps, is summarized in a document, outputted as a PDF, and uploaded to the patient’s EMR. A unique feature of this application and our workflow is the incorporation of a real-time GPS-based patient tracking system. A precise estimated
time of arrival for a patient is difficult to determine because of the multiple stages in evaluation and transport, each of which has considerable variability. Therefore, to best inform the stroke team of the patient’s status, a graphical representation of the patient’s position in the city or surrounding region is transmitted.
Figure 1 shows a series of screenshots of the Join app during a Stroke60 event. In Figure 2, a set of time stamps from the Join app is shown along with corresponding components of the workflow in our institution, including the team awaiting and greeting the arriving ambulance and patient, rapid transport to the CT (or MRI) scanner and then to the neurointerventional suite for thrombectomy. Figure 3 depicts the interrelated stroke response team entities.
Results
We have found the Join app to be a helpful tool in providing real-time communication among team members, all of whom are on call and may be up to 60 minutes away from the hospital. The secure text communication feature facilitates rapid delegation of tasks and confirmation of their completion to the entire team. Automated time-stamping eliminates inefficient
Rush UniversityMedical Center
Home
Text link
Patient
Physician and staff transportation
Physician and staff
Emergency medical services and patient transportation
OutsideHospital
Figure 3. Diagram representing the coordinated communication and transportation in the Stroke60 response. The patient is picked up and brought to an outside hospital, where a preliminary diagnosis of acute ischemic stroke is made, the Stroke60 process is activated, and confirmatory imaging is obtained at the outside hospital and reviewed by outside hospital physicians and the on-call Rush University Medical Center neurologist and neurosurgeon or neurointerventionalist. A decision is made regarding transfer to Rush University Medical Center, and, if affirmative, the patient is brought via ambulance or helicopter to Rush University Medical Center. Immediately upon Stroke60 activation, all on-call team members indicate (via call, text, or Join app) that they are available and en route or on site, and team members ensure that all elements are in house and ready before the arrival of the patient in the emergency department bay.

20 THE 2016 RUSH NEUROSCIENCE REVIEW
scribing of times and the risk of losing paper time-stamp notes. Automated generation of a summary report provides further robust documentation of time stamps and communication. Real-time patient location tracking with GPS is valuable to on-call and in-house team members in ensuring that appropriate personnel are ready prior to the arrival of the patient, thereby minimizing delay in delivery of therapy.
Discussion
The Rush University Medical Center Stroke60 workflow and associated mobile application represent, to our knowledge, the first integration of a mobile application with GPS functionality that coordinates the activities and travel logistics of all stakeholders in acute stroke treatment, including the patient, the staff at the initial presenting hospital, the transportation service (ambulance or helicopter service), and the receiving hospital and associated physicians and on-call team members.
In real time, we are able to receive text and image updates, delegate responsibility for tasks (scheduling the procedure in the interventional suite, calling the anesthesia team, obtaining telephone consent from family, obtaining patient handoff from the transferring hospital, and others) and confirm their completion, and ensure that all on-call staff are on site and systems are ready before arrival of the patient. Rather than utilizing an estimated time of arrival with an unknown level of uncertainty, the visual GPS tracking, with an icon trail showing the trajectory history and velocity, provides a clear big-picture view of the patient’s present location and likely time to arrival. Usually, the stroke neurointerventional team has 45 to 60 minutes of advance notice from the first page to arrival of the patient at the emergency department bay, but the variability is large, and occasionally less than 30 minutes of notice has been given. A real-time visual representation is helpful so that the need for backup staff may be quickly appreciated and their activation commenced if needed.
Static use of GPS has been described in stroke treatment. Nam et al7 described a consumer mobile smartphone application that provides guided questioning to enable patients to self-diagnose acute ischemic stroke and uses GPS in a static fashion to calculate distances to hospitals to determine the closest hospital offering thrombectomy services. Demaerschalk et al5 described the use of a smartphone application, ResolutionMD, to facilitate secure remote viewing of neuroradiological images from an outside hospital for stroke diagnosis.
Conclusion
In our pilot study, the Join app has provided reliable real-time communication among Stroke60 team members, reliable graphical representation of patient location during transport, time-efficient time-stamping, and summaries of these and other metrics for uploading into the EMR. This pilot experience is
qualitative in nature, and further quantitative study with metrics is planned. This is the first reported use of real-time GPS tracking of patient transfer for acute stroke treatment. Our experience has been positive, and further quantitative evaluation of this and other mobile applications is warranted and planned.
Acknowledgments
We would like to acknowledge Allm Inc (Tokyo, Japan) for providing the Join app.

The Join App for Acute Stroke 21
References1. Thomairy NA, Mummaneni M, Alsalamah S, Moussa N, Coustasse A. Use of smartphones in hospitals. Health Care Manag (Frederick). 2015;34(4):297-307.
2. Cohen AB, Nahed BV, Sheth KN. Mobile medical applications in neurology. Neurol Clin Pract. 2013;3(1):52-60.
3. Seo WK, Kang J, Jeon M, et al. Feasibility of using a mobile application for the monitoring and management of stroke-associated risk factors. J Clin Neurol. 2015;11(2):142-148.
4. Widmer RJ, Collins NM, Collins CS, West CP, Lerman LO, Lerman A. Digital health interventions for the prevention of cardiovascular disease: a systematic review and meta-analysis. Mayo Clin Proc. 2015;90(4):469-480.
5. Demaerschalk BM, Vargas JE, Channer DD, et al. Smartphone teleradiology application is successfully incorporated into a telestroke network environment. Stroke. 2012;43(11):3098-3101.
6. Cooray C, Matusevicius M, Wahlgren N, Ahmed N. Mobile phone-based questionnaire for assessing 3 months modified Rankin score after acute stroke: a pilot study. Circ Cardiovasc Qual Outcomes. 2015;8(6)(suppl 3): S125-S130.
7. Nam HS, Heo J, Kim J, et al. Development of smartphone application that aids stroke screening and identifying nearby acute stroke care hospitals. Yonsei Med J. 2014;55(1):25-29. ◆

22 THE 2016 RUSH NEUROSCIENCE REVIEW
DEEP BRAIN STIMULATION FOR MAJOR DEPRESSION
Joshua T. Wewel, MD; Ryan B. Kochanski, MD; Sepehr Sani, MD
Author Affiliations: Department of Neurological Surgery, Rush University Medical Center, Chicago, Illinois.
Corresponding Author: Sepehr Sani, MD, Department of Neurological Surgery, Rush University Medical Center, 1725 W Harrison St, Suite 855, Chicago, IL 60612 ([email protected]).
Introduction
Major depressive disorder (MDD) is a ubiquitous affective disorder with debilitating symptoms that severely hampers quality of life. Population studies have reported the lifetime prevalence of MDD to be 16.2%.1 Symptoms of depression include depressed mood, changes in sleep patterns, loss of interest in daily activities, fatigue, excessive guilt, and suicidal ideation. Pharmacotherapy is commonly effective; however, 20% to 30% of patients remain refractory to medical treatment.2,3
In addition to pharmacotherapy, contemporary noninvasive treatments for MDD include psychotherapy and electroconvulsive therapy. Surgical treatments in the form of ablation, including anterior capsulotomy, anterior cingulotomy, and subcaudate tractotomy, have been reported with varying degrees of success.4-7 Neuromodulation therapies including vagal nerve stimulation and epidural cortical stimulation have also been trialed.8,9 With increasing interest and improvement in reported outcomes, deep brain stimulation (DBS) for MDD is becoming a field of heightened interest.
The departments of neurological surgery, neurological sciences, and psychiatry at Rush University Medical Center are high-volume clinical practices with the requisite patient population and resources to conduct continued research regarding DBS for MDD. In this review we intend to illustrate how Rush is in a unique position to advance the field of neuromodulation for psychiatric conditions and improve the quality of life for those with refractory MDD.
Current State of Knowledge
MDD is a multifactorial disease process predicated around the monoamine and catecholamine hypotheses for affective disorders.10 Simply stated, affective disorders such as MDD are observed to exist in a state of relative amine deficiency (serotonin and norepinephrine). Conversely, drugs or therapies that potentiate amine availability produce an antidepressant effect. Additional factors contributing to MDD include stress, neurodegeneration, and possibly genetic components.11-13
Neurocircuitry
The neurocircuitry relating to MDD and other affective disorders is complex. Previous studies have implicated various components of the cortico-striato-thalamo-cortical (CSTC) pathway and subcomponents thereof.14-18 The CSTC pathway can be subcategorized into dorsal, modulatory, and ventral components.16 The dorsal component consists of the thalamus, prefrontal cortices, premotor cortex, dorsal cingulate cortex, dorsal striatum, and dorsal pallidum. The dorsal structures are believed to contribute to the cognitive and motor symptoms of MDD. The ventral compartment consists of the thalamus, orbitofrontal cortex, subgenual cingulate cortex (SCC), insular cortex, ventral striatum, and ventral pallidum. These structures contribute to the vegetative state observed in MDD. The modulatory component, consisting of the hippocampus, amygdala, and hypothalamic-pituitary-adrenal axis, completes the circuit and aids in communication and relaying information between the dorsal and ventral structures.16
Review of DBS for MDD
A total of six stimulation sites have been trialed for the treatment of MDD, including the SCC, nucleus accumbens (NAcc), ventral capsule/ventral striatum (VA/VS), lateral habenula (LHb), inferior thalamic peduncle, and medial forebrain bundle (MFB). In a series of patients undergoing DBS

Deep Brain Stimulation for Major Depression 23
of the NAcc, long-term follow-up revealed that approximately 50% of the cohort had a successful response.19,20 DBS of the VA/VS has been reported with a response rate of 71% in 1 trial of 17 patients with a mean follow-up of 37.4 months.21 Response rates have ranged from 29% to 92% across multiple studies.22-24 However, despite success with open-label VA/VS DBS, a prospective randomized trial failed to show significant improvement in the VA/VS stimulation group when compared with the sham stimulation group.25 Stimulation of the SCC was initially described in 1997, and, more recently, a single-blinded study of 17 patients with bipolar disorder and MDD demonstrated a response rate of 92% with full remission in 58% of patients.15,22 However, a multicenter, prospective, randomized trial for DBS of the SCC was initiated by St. Jude Medical and stopped early because the 6-month results failed to show utility.16
At Rush, current efforts to treat MDD are focused on targeting of the LHb and MFB. DBS of the LHb has been reported with success in a single patient with therapy-refractory MDD, and increased activation of the LHb has been implicated in the downregulation of serotonergic, noradrenergic, and dopaminergic systems and stimulation of the HPA axis.26,27 An increase in peripheral brain-derived neurotrophic factor, a neuronal growth factor involved in maintenance of synaptic function and neural plasticity, with long-term DBS of the LHb has also been demonstrated.28 At Rush, we have utilized MRI tractography to identify the major afferent pathway to the LHb, the stria medullaris thalami, in 5 patients, which could provide utility for direct targeting in DBS surgery (Figure 1).
The MFB (Figure 2) interconnects various centers of the reward pathway, including the NAcc, ventral tegmental area (VTA), hypothalamus, and amygdala. The VTA is central to the processing of inputs from various parts of the brain to generate motivated behavior based on reward designation and is believed to be dysfunctional in patients with MDD.29 Therefore, it stands to reason that stimulation of the MFB may alter the function of the VTA, leading to improvement in mood. This hypothesis has
undergone preliminary testing in Germany, where 7 patients underwent bilateral DBS implantation of the superolateral branch of the medial forebrain bundle (slMFB), a structure with proven convergence on the prefrontal cortex and close functional connection to the anterior limb of the internal capsule and the NAcc.30-34 Preliminary results show that 6 of 7 patients studied achieved a 50% decrease in the Montgomery-Asberg Depression Rating Scale, a very encouraging result so far.
The Role of Rush University Medical Center
The departments of neurological surgery, neurological sciences, and psychiatry at Rush are at the forefront of researching new and evolving uses of DBS. In addition to efforts targeting the LHb via the stria medullaris using MRI tractography, Rush is also currently recruiting patients with refractory MDD for treatment with DBS targeting the slMFB in a randomized, blinded, placebo-controlled trial.
Study Design
Twenty patients age 18 to 70 years with refractory MDD will be identified by the Department of Psychiatry at Rush. Those included in the study must carry the diagnosis of MDD as defined by DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th ed) standards. Symptoms must be present for greater than 2 years, with a current episode lasting longer than 12 months. Standardized Hamilton Depression Rating Scale (HDRS) and computerized adaptive testing (CAT) will be used for inclusion criteria, and all patients must have exhausted trials of at least 3 antidepressants used independently or in combination with each other. Lifetime failure or intolerance of electroconvulsive therapy is also required. Both patients with bipolar disorder and those with MDD will be included.
Excluded from the study are those with concomitant nonaffective psychiatric disorders such as schizophrenia,
Figure 1. Diffusion tensor imaging of the stria medullaris in axial (A), sagittal (B), and coronal (C) views.
A B C

24 THE 2016 RUSH NEUROSCIENCE REVIEW
schizoaffective disorder, or personality disorders. Organic neurologic disorders such as dementia, stroke, or medical illness affecting brain function will preclude enrollment in the study. Additionally, previous brain surgery or abnormal preoperative cranial imaging will negate enrollment.
Initial baseline testing will take place 3 weeks after DBS implantation within the slMFB. Patients will be randomized into 2 groups (10 patients each). The DBS system will be turned on for 1 cohort and kept off for the other cohort, and no changes will be made over a 6-month period during the blinded evaluation phase. Following the blinded evaluation phase, the open-label phase, during which all patients will have their DBS system turned on and settings optimized over an 18-month period, will ensue.
Outcome Measures
The primary outcome measure will be evaluated by CAT scoring, which will be used to record response and remission rates. Response to stimulation will be defined as a CAT severity score of moderate or better, while remission will be defined as a severity score of mild or better. Secondary outcome measures will be defined by HDRS scoring. A response in HDRS measures will be defined as a 50% change in HDRS score compared with the baseline score. Remission will be defined as an HDRS score of 8 or less at the end point.
Conclusions
Treatment-refractory MDD is a common clinical occurrence with debilitating symptomatology. A variety of stimulation targets exist for select patients with refractory MDD. At Rush, the departments of neurological surgery, neurological sciences, and psychiatry are changing the way MDD is managed and will continue do so in the prospective, randomized clinical trial of DBS of the slMFB.
Figure 2. Diffusion tensor imaging of the medial forebrain bundle in axial (A), sagittal (B), and coronal (C) views.
A B C

Deep Brain Stimulation for Major Depression 25
References1. Kessler RC, Berglund P, Demler O, et al; National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095-3105.
2. Fava M. Diagnosis and definition of treatment-resistant depression. Biol Psychiatry. 2003;53(8):649-659.
3. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163(11):1905-1917.
4. Christmas D, Eljamel MS, Butler S, et al. Long term outcome of thermal anterior capsulotomy for chronic, treatment refractory depression. J Neurol Neurosurg Psychiatry. 2011;82:594-600.
5. Dougherty DD, Weiss AP, Cosgrove GR, et al. Cerebral metabolic correlates as potential predictors of response to anterior cingulotomy for treatment of major depression. J Neurosurg. 2003;99(6):1010-1017.
6. Kelly D, Richardson A, Mitchell-Heggs N, Greenup J, Chen C, Hafner RJ. Stereotactic limbic leucotomy: a preliminary report on forty patients. Br J Psychiatry. 1973;123(573):141-148.
7. Ström-Olsen R, Carlisle S. Bi-frontal stereotactic tractotomy: a follow-up study of its effects on 210 patients. Br J Psychiatry. 1971;118(543):141-154.
8. Kopell BH, Halverson J, Butson CR, et al. Epidural cortical stimulation of the left dorsolateral prefrontal cortex for refractory major depressive disorder. Neurosurgery. 2011;69(5):1015-1029, discussion 1029.
9. Rush AJ, George MS, Sackeim HA, et al. Vagus nerve stimulation (VNS) for treatment-resistant depressions: a multicenter study. Biol Psychiatry. 2000;47(4):276-286.
10. Schildkraut JJ, Kety SS. Biogenic amines and emotion. Science. 1967;156(3771):21-37.
11. Bewernick BH, Schlaepfer TE. Chronic depression as a model disease for cerebral aging. Dialogues Clin Neurosci. 2013;15(1):77-85.
12. Frodl T, O’Keane V. How does the brain deal with cumulative stress? a review with focus on developmental stress, HPA axis function and hippocampal structure in humans. Neurobiol Dis. 2013;52:24-37.
13. Hartmann N, Boehner M, Groenen F, Kalb R. Telomere length of patients with major depression is shortened but independent from therapy and severity of the disease. Depress Anxiety. 2010;27(12): 1111-1116.
14. Kopell BH, Greenberg B, Rezai AR. Deep brain stimulation for psychiatric disorders. J Clin Neurophysiol. 2004;21(1):51-67.
15. Mayberg HS. Limbic-cortical dysregulation: a proposed model of depression. J Neuropsychiatry Clin Neurosci. 1997;9(3):471-481.
16. Morishita T, Fayad SM, Higuchi MA, Nestor KA, Foote KD. Deep brain stimulation for treatment-resistant depression: systematic review of clinical outcomes. Neurotherapeutics. 2014;11(3):475-484.
17. Rauch SL. Neuroimaging and neurocircuitry models pertaining to the neurosurgical treatment of psychiatric disorders. Neurosurg Clin N Am. 2003;14(2):213-223, vii-viii.
18. Shah DB, Pesiridou A, Baltuch GH, Malone DA, O’Reardon JP. Functional neurosurgery in the treatment of severe obsessive compulsive disorder and major depression: overview of disease circuits and therapeutic targeting for the clinician. Psychiatry (Edgmont). 2008;5(9):24-33.
19. Schlaepfer TE, Cohen MX, Frick C, et al. Deep brain stimulation to reward circuitry alleviates anhedonia in refractory major depression. Neuropsychopharmacology. 2008;33(2):368-377.
20. Bewernick BH, Kayser S, Sturm V, Schlaepfer TE. Long-term effects of nucleus accumbens deep brain stimulation in treatment-resistant depression: evidence for sustained efficacy. Neuropsychopharmacology. 2012;37(9):1975-1985.
21. Malone DA Jr, Dougherty DD, Rezai AR, et al. Deep brain stimulation of the ventral capsule/ventral striatum for treatment-resistant depression. Biol Psychiatry. 2009;65(4):267-275.
22. Holtzheimer PE, Kelley ME, Gross RE, et al. Subcallosal cingulate deep brain stimulation for treatment-resistant unipolar and bipolar depression. Arch Gen Psychiatry. 2012;69(2):150-158.
23. Lozano AM, Giacobbe P, Hamani C, et al. A multicenter pilot study of subcallosal cingulate area deep brain stimulation for treatment-resistant depression. J Neurosurg. 2012;116(2):315-322.
24. Lozano AM, Mayberg HS, Giacobbe P, Hamani C, Craddock RC, Kennedy SH.. Subcallosal cingulate gyrus deep brain stimulation for treatment-resistant depression. Biol Psychiatry. 2008;64(6):461-467.
25. Underwood E. Short-circuiting depression. Science. 2013;342(6158):548-551.
26. Sartorius A, Henn FA. Deep brain stimulation of the lateral habenula in treatment resistant major depression. Med Hypotheses. 2007;69(6):1305-1308.
27. Sartorius A, Kiening KL, Kirsch P, et al. Remission of major depression under deep brain stimulation of the lateral habenula in a therapy-refractory patient. Biol Psychiatry. 2010;67(2):e9-e11.
28. Hoyer C, Kranaster L, Sartorius A, Hellweg R, Gass P. Long-term course of brain-derived neurotrophic factor serum levels in a patient treated with deep brain stimulation of the lateral habenula. Neuropsychobiology. 2012;65(3):147-152.
29. Martin-Soelch C. Is depression associated with dysfunction of the central reward system? Biochem Soc Trans. 2009;37(pt 1):313-317.
30. Schlaepfer TE, Bewernick BH, Kayser S, Mädler B, Coenen VA. Rapid effects of deep brain stimulation for treatment-resistant major depression. Biol Psychiatry. 2013;73(12):1204-1212.
31. Schoene-Bake JC, Parpaley Y, Weber B, Panksepp J, Hurwitz TA, Coenen VA. Tractographic analysis of historical lesion surgery for depression. Neuropsychopharmacology. 2010;35(13):2553-2563.
32. Coenen VA, Schlaepfer TE, Maedler B, Panksepp J. Cross-species affective functions of the medial forebrain bundle—implications for the treatment of affective pain and depression in humans. Neurosci Biobehav Rev. 2011;35(9):1971-1981.
33. Coenen VA, Panksepp J, Hurwitz TA, Urbach H, Mädler B. Human medial forebrain bundle (MFB) and anterior thalamic radiation (ATR): imaging of two major subcortical pathways and the dynamic balance of opposite affects in understanding depression. J Neuropsychiatry Clin Neurosci. 2012;24(2):223-236.
34. Coenen VA, Honey CR, Hurwitz T, et al. Medial forebrain bundle stimulation as a pathophysiological mechanism for hypomania in subthalamic nucleus deep brain stimulation for Parkinson’s disease. Neurosurgery. 2009;64(6):1106-1114, discussion 1114-1115. ◆

26 THE 2016 RUSH NEUROSCIENCE REVIEW
OUTCOME FOLLOWING INTRACRANIAL HEMORRHAGE ASSOCIATED WITH NOVEL ORAL ANTICOAGULANTS
Manish K. Kasliwal, MBBS, MCh; Nicholas G. Panos, PharmD, BCPS; Lorenzo F. Muñoz, MD; Roham Moftakhar, MD; Demetrius K. Lopes, MD; Richard Byrne, MD
Author Affiliations: Department of Neurological Surgery, Case Western Reserve University (Dr Kasliwal), Cleveland, Ohio; Department of Neurological Surgery, Rush University Medical Center (Drs Panos, Muñoz, Lopes, and Byrne), Chicago, Illinois; and Department of Neurological Surgery, University of South Carolina (Dr Moftakhar), Columbia, South Carolina.
Corresponding Author: Manish K. Kasliwal, MBBS, MCh, Department of Neurological Surgery, Case Western Reserve University School of Medicine, 11100 Euclid Ave, Mailstop HAN 5042, Cleveland, OH 44106 ([email protected]).
Previous Publication: This article was previously published in J Clin Neurosci 2015;22(1):212-215. Minor edits have been made.
Introduction
Anticoagulants are frequently used for various indications, including prevention of venous thromboembolism after orthopedic surgery, treatment of acute venous thromboembolism, and prevention of arterial thromboembolism in atrial fibrillation.1-3 Warfarin has been the most commonly prescribed anticoagulant to treat and prevent thrombosis for many decades. Three novel oral anticoagulants (NOAC), dabigatran, rivaroxaban, and apixaban, have recently been approved by the US Food and
Drug Administration for the prevention of arterial thromboembolic events in nonvalvular atrial fibrillation as an alternative to warfarin.4-6 As the use of these NOAC increases over time, neurosurgeons will be confronted with managing patients receiving these medications more often, secondary to the risk of development of intracranial hemorrhage (ICH) while on these NOAC.7 We report our experience in 2 patients who sustained ICH while on NOAC, along with a review of the literature.
Case Descriptions
Patient 1
An 83-year-old man presented with acute onset of weakness for 1 day. Computed tomography (CT) scan of the head revealed an ICH involving the left basal ganglia (Figure 1). Past medical history was significant for well-controlled hypertension and nonvalvular atrial fibrillation for which he was receiving rivaroxaban 20 mg daily, the last dose being taken about 12 hours prior to the onset of symptoms. Neurological examination at presentation was within normal limits except for a subtle right-sided pronator drift. Laboratory analysis showed serum creatinine, prothrombin time/international normalized ratio (PT/INR), and activated partial thromboplastin time (APTT) to be within normal limits. He was immediately treated with factor VIII inhibitor bypassing activity (FEIBA) 30 international units/kg in consultation with a hematologist and monitored in the neuroscience intensive care unit. Repeat CT scan performed 24 hours after admission showed no expansion in the size of the hematoma with stable neurological exam. He was subsequently discharged home and was doing well at last follow-up at 3 months.
Patient 2
An 80-year-old man with a significant past medical history of deep vein thrombosis on dabigatran 150 mg every 12 hours presented to an outside hospital after 2 days of altered mental
Figure 1. Axial noncontrast CT scan of the head showing an acute hemorrhage in the left thalamus measuring 2×1 cm in axial section with no significant mass effect or midline shift (A). Repeat CT scan done after 24 hours demonstrating stable hemorrhage (B).
A B

Outcome Following Intracranial Hemorrhage Associated With Novel Oral Anticoagulants 27
status and right-sided weakness. He was taking dabigatran as prescribed, with the most recent dose taken the morning of presentation. CT scan of the head showed a left-sided acute-on-chronic subdural hematoma (SDH) with significant mass effect and midline shift (Figure 2). Laboratory analysis showed serum creatinine within normal limits with PT, INR, and APTT on admission being 14.8 seconds (normal range, 9.5-13.2 seconds), 1.48 (normal range, 0.8-1.2), and 45.8 seconds (normal range, 23-33 seconds) respectively. Surgical treatment was deemed appropriate, but because he recently took dabigatran, it was deferred considering his good neurological examination apart from minimal right pronator drift. The family was informed about the risk and benefits, and a collective decision to delay the surgery (reserving it for acute deterioration) was made. He was closely monitored in the neuroscience intensive care unit with repeat CT scan of the head performed at 6 and 24 hours after admission showing stable SDH (Figure 2) with no worsening of neurological examination. Because he was more than 96 hours out from his last dose of dabigatran and his PT/INR and APTT normalized, surgery was performed with successful removal of the SDH through a mini craniotomy. Excessive bleeding was not encountered during surgery, and hemostasis was achieved without difficulty. Throughout the inpatient stay, he did not experience neurological deterioration attributable to rebleeding, and subsequent postoperative CT scans showed good decompression with resolution of the mass effect and midline shift. However, he experienced a prolonged postoperative recovery and required a tracheostomy because he could not be weaned off the ventilator. He was finally transferred to a nursing home.
Discussion
Neurosurgeons and neurointensivists are frequently involved in the management of anticoagulant-related ICH. Pharmacologic strategies are available to reverse the effect of traditional anticoagulants such as warfarin, unfractionated heparin, and
low-molecular-weight heparin, which may improve the overall outcome by reducing hematoma expansion, related mass effect, and midline shift.1,2,8 This may involve reversal with fresh frozen plasma, phytonadione, prothrombin complex concentrates (PCC), and recombinant activated factor VII (rVIIa). Regardless of the availability of reversal agents and their efficacy in reversing the anticoagulation effect of warfarin, reversal of anticoagulation may not always translate to good clinical outcome, which is probably related to the severity of initial hemorrhage.9 Likewise, even though platelets are often administered in patients who sustain ICH on antiplatelet agents such as aspirin and clopidogrel, there is no true antidote for these agents either. As compared to warfarin, where reversal strategies for preventing expansion of ICH in the event of bleeding are well defined, pharmacologic strategies to reverse NOAC in cases of life-threatening hemorrhage are lacking and experience is limited mostly to animal studies, in vitro studies, and case reports.7,10-21 In addition, coagulation assays used to confirm the anticoagulant effect of NOAC are limited to clinical studies and not commercially available at this time.22 This makes it very difficult to confirm the effect of the various pharmacologic agents used to reverse these agents in clinical practice.
Upon our review of all the reported cases of NOAC-associated ICH at the time of writing (total 18 patients, including this study), there were 7 deaths, leading to an overall mortality rate of 39% (7 of 18 patients).10-12,15,16,19-21 Previous reports have focused mainly on dabigatran-associated hemorrhages. The management of these patients who sustained ICH while on dabigatran varied among institutions and reflects the problems associated with incomplete dabigatran reversal (Table 1). Even though various pharmacologic agents such as PCC and rVIIa have been administered to patients who sustained a dabigatran-associated ICH, it is unknown whether they are effective in fully reversing the anticoagulant effect of dabigatran.10,12,13,20,23 Dialysis is an alternative for drug clearance and can remove approximately 35% to 60% of the drug in 2 to 3 hours and at present may be the only option to enhance the removal of
Figure 2. Axial noncontrast CT scan of the head demonstrating left-sided acute-on-chronic subdural hematoma, with significant mass effect and midline shift (A). Also seen is the ventricular end of the shunt from prior surgery. Repeat axial CT scans performed at 6 hours (B) and 24 hours (C) showing no increase in the size of the hematoma. Postoperative axial CT scan of the head (D) demonstrating good decompression with improvement in mass effect and midline shift and no hemorrhagic complication.
A B C D

28 THE 2016 RUSH NEUROSCIENCE REVIEW
dabigatran.11 However, it is not proven whether patients with normal renal function should undergo hemodialysis to expedite clearance of dabigatran.23,24 Since the patient receiving dabigatran was conscious with very subtle pronator drift and had normal renal function, we elected not to proceed with the emergent surgery to allow time for dabigatran to be fully excreted. The use of dabigatran did delay the surgery in this case and could have precipitated an adverse outcome if the hematoma expanded with subsequent deterioration of the neurological examination.
On the other hand, there is growing evidence that PCC may be beneficial and have been found to reverse the anticoagulant activity of rivaroxaban.14,17,23,25 Our patient receiving rivaroxaban prior to admission was treated with FEIBA, which may have contributed to his favorable outcome. He maintained his neurological examination status throughout the hospital stay without evidence of hematoma expansion on serial imaging at 6 and 24 hours and was discharged home.
No. Authors (Year) Age/Sex Anticoagulant Type of ICH Reversal Strategy
Outcome
1 Garber et al (2012)16
83/M Dabigatran Parenchymal/subdural/ subarachnoid
rFVIIa Death
2 Chen et al (2012)12
80/M Dabigatran Subdural Phytonadione Stable hemorrhage
3 Chang et al (2013)11
94/M Dabigatran Subdural FEIBA, hemodialysis
Stable hemorrhage
4 Awad et al (2013)10
85/F Dabigatran Subdural Hemodialysis attempted
Surgery due to hemorrhage expansion; neurologically intact at discharge
5 Faust and Peterson (2014)15
85/M Dabigatran Parenchymal FEIBA Death secondary to ischemic stroke; hemorrhage stable
6 Wassef et al (2013)21
79/F Dabigatran Parenchymal None Death secondary to expansion of hemorrhage
7 Wassef et al (2013)21
72/M Dabigatran Chronic subdural
None Surgery; discharged home
8 Wassef et al (2013)21
72/M Dabigatran Subarachnoid None Stable hemorrhage; discharged home
9 Ross et al (2014)19
NR Dabigatran NR None Stable hemorrhage; discharged home
10 Ross et al (2014)19
NR Dabigatran NR FFP, platelets Death
11 Ross et al (2014)19
NR Dabigatran NR None Stable hemorrhage; discharged home
12 Ross et al (2014)19
NR Dabigatran NR FFP, platelets, dialysis
Surgery; death
13 Ross et al (2014)19
NR Dabigatran NR None Stable hemorrhage; discharged home
14 Ross et al (2014)19
NR Dabigatran NR FFP, vitamin K, rFVIIa, dialysis
Surgery; death
15 Ross et al (2014)19
NR Dabigatran NR None Stable hemorrhage; rehabilitation
16 Simonsen et al (2014)20
75/M Dabigatran Parenchymal None Death due to hematoma expansion
17 Present study 83/M Rivaroxaban Parenchymal FEIBA Stable hemorrhage; discharged home
18 Present study 80/M Dabigatran Subdural None Surgery; rehabilitation
Table 1. Summary of Reported Cases of Intracranial Hemorrhage in Patients Treated With Novel Oral Anticoagulants
Abbreviations: F, female; FEIBA, factor VIII inhibitor bypassing activity; FFP, fresh frozen plasma; ICH, intracranial hemorrhage; M, male; NR, not reported; PCC, prothrombin complex concentrates; rFVIIa, coagulation factor VIIa (recombinant).

Conclusion
With the introduction of NOAC, the low risk of ICH provides a favorable alternative to warfarin. The use of NOAC comes with a greater risk for hematoma expansion and death if suitable reversal agents are not found. Current strategies to reverse the NOAC with PCC, fresh frozen plasma, and rVIIa are limited by the inability to measure their clinical effect with the available coagulation assays. The need to develop antidotes for NOAC and reliable laboratory tests to measure anticoagulation effects related to them cannot be overemphasized. Understanding the potential salvaging reversal strategies and knowledge of the outcome following ICH in patients receiving NOAC is of utmost importance for any practicing neurosurgeon and neurointensivist to envisage the expected outcome and prognosticate following this catastrophic event.
Conflict of Interest
The authors M.K.K., N.G.P., and L.F.M. have no disclosures or conflict of interest. R.W.B. is a consultant for Integra and Stryker. R.M. is a consultant for Covidien and Penumbra Inc. D.K.L. has financial and research relationships with Penumbra, Covidien, and Stryker.
Neurosurgery at Rush University Medical Center, lead by Richard Byrne, MD (center).
Outcome Following Intracranial Hemorrhage Associated With Novel Oral Anticoagulants 29

30 THE 2016 RUSH NEUROSCIENCE REVIEW
References1. Flibotte JJ, Hagan N, O’Donnell J, Greenberg SM, Rosand J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology. 2004;63(6):1059-1064.
2. Schulman S, Crowther MA. How I treat with anticoagulants in 2012: new and old anticoagulants, and when and how to switch. Blood. 2012;119(13):3016-3023.
3. Sinnaeve PR, Brueckmann M, Clemens A, Oldgren J, Eikelboom J, Healey JS. Stroke prevention in elderly patients with atrial fibrillation: challenges for anticoagulation. J Intern Med. 2012;271(1):15-24.
4. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139-1151.
5. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992.
6. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891.
7. Teddy P, Nair G. Anti-stroke prophylaxis—the ethics of collateral damage. J Clin Neurosci. 2012;19(6):792-794.
8. Provencio JJ, Da Silva IR, Manno EM. Intracerebral hemorrhage: new challenges and steps forward. Neurosurg Clin N Am. 2013;24(3):349-359.
9. Dowlatshahi D, Butcher KS, Asdaghi N, et al. Poor prognosis in warfarin-associated intracranial hemorrhage despite anticoagulation reversal. Stroke. 2012;43(7):1812-1817.
10. Awad AJ, Walcott BP, Stapleton CJ, Yanamadala V, Nahed BV, Coumans JV. Dabigatran, intracranial hemorrhage, and the neurosurgeon. Neurosurg Focus. 2013;34(5):E7.
11. Chang DN, Dager WE, Chin AI. Removal of dabigatran by hemodialysis. Am J Kidney Dis. 2013;61(3):487-489.
12. Chen BC, Viny AD, Garlich FM, et al. Hemorrhagic complications associated with dabigatran use. Clin Toxicol (Phila). 2012;50(9):854-857.
13. Dager WE, Gosselin RC, Roberts AJ. Reversing dabigatran in life-threatening bleeding occurring during cardiac ablation with factor eight inhibitor bypassing activity. Crit Care Med. 2013;41(5):e42-e46.
14. Eerenberg ES, Kamphuisen PW, Sijpkens MK, Meijers JC, Buller HR, Levi M. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation. 2011;124(14):1573-1579.
15. Faust AC, Peterson EJ. Management of dabigatran-associated intracerebral and intraventricular hemorrhage: a case report. J Emerg Med. 2014;46(4):525-529.
16. Garber ST, Sivakumar W, Schmidt RH. Neurosurgical complications of direct thrombin inhibitors-catastrophic hemorrhage after mild traumatic brain injury in a patient receiving dabigatran. J Neurosurg. 2012;116(5):1093-1096.
17. Marlu R, Hodaj E, Paris A, Albaladejo P, Cracowski JL, Pernod G. Effect of non-specific reversal agents on anticoagulant activity of dabigatran and rivaroxaban: a randomised crossover ex vivo study in healthy volunteers. Thromb Haemost. 2012;108(2):217-224.
18. Pernod G, Albaladejo P, Godier A, et al. Management of major bleeding complications and emergency surgery in patients on long-term treatment with direct oral anticoagulants, thrombin or factor-Xa inhibitors: proposals of the working group on perioperative haemostasis (GIHP)—March 2013. Arch Cardiovasc Dis. 2013;106(6-7):382-393.
19. Ross B, Miller MA, Ditch K, Tran M. Clinical experience of life-threatening dabigatran-related bleeding at a large, tertiary care, academic medical center: a case series. J Med Toxicol. 2014;10(2):223-228.
20. Simonsen CZ, Steiner T, Tietze A, Damgaard D. Dabigatran-related intracerebral hemorrhage resulting in hematoma expansion. J Stroke Cerebrovasc Dis. 2014;23(2):e133-e134.
21. Wassef SN, Abel TJ, Grossbach A, et al. Traumatic intracranial hemorrhage in patients taking dabigatran: report of 3 cases and review of the literature. Neurosurgery. 2013;73(2):E368-E373, discussion E373-E374.
22. Miyares MA, Davis K. Newer oral anticoagulants: a review of laboratory monitoring options and reversal agents in the hemorrhagic patient. Am J Health Syst Pharm. 2012;69(17):1473-1484.
23. Mittal MK, Rabinstein AA. Anticoagulation-related intracranial hemorrhages. Curr Atheroscler Rep. 2012;14(4):351-359.
24. van Ryn J, Stangier J, Haertter S, et al. Dabigatran etexilate—a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Thromb Haemost. 2010;103(6):1116-1127.
25. Steiner T, Böhm M, Dichgans M, et al. Recommendations for the emergency management of complications associated with the new direct oral anticoagulants (DOACs), apixaban, dabigatran and rivaroxaban. Clin Res Cardiol. 2013;102(6):399-412. ◆

Resecting Critical Nodes From an Epileptogenic Circuit in Refractory Focal-Onset Epilepsy Patients 31
Author Affiliations: Rush Epilepsy Center, Department of Neurological Sciences (Drs Jalota, Rossi, Stein, Stoub, Balabanov, Bergen, Bermeo, Park, and Smith), Department of Diagnostic Radiology and Nuclear Medicine (Dr Rossi and Mr Pylypyuk), and Department of Neurological Surgery (Dr Byrne), Rush University Medical Center, Chicago, Illinois.
Corresponding Author: Marvin A. Rossi, MD, PhD, Rush University Medical Center, Department of Neurological Sciences, 1725 W Harrison St, Suite 885, Chicago, IL 60612 ([email protected]).
Previous Publication: This article was previously published in J Neurosurg [published online March 18, 2016; doi:10.3171/2015.6.JNS141719]. Minor edits have been made.
Epilepsy is estimated to affect between 2.5 and 3 million people in the United States, with a prevalence of 5 to 10 persons per 1 000.1 It has been shown that about 47% of patients with a new diagnosis of focal-onset epilepsy are successfully treated with the first antiepileptic drug (AED) prescribed.2 Therapeutic failure of 2 AEDs is defined as drug-resistant epilepsy.3,4 Approximately 20% to 40% of patients with epilepsy are likely to have drug-resistant epilepsy.5-7 Patients with a unilateral lesion on high-resolution MRI that is concordant with the electroencephalography (EEG) findings and seizure semiology have the best outcomes after resection.8-10 Unfortunately, 20% to 30% of temporal lobe epilepsy (TLE) patients and 20% to 50% of extratemporal lobe epilepsy (ETLE) patients demonstrate the absence of an underlying lesion on high-resolution MRI.11-13 Resective targeting of the ictal onset zone (IOZ) is most challenging in patients with nonlesional MRI and focal-onset epilepsy. Previous postresection outcome studies report seizure freedom to be the greatest after resection in lesional TLE patients, whereas 75% to 85% of patients achieve Engel Class I after 2 years of follow-up (Engel classification: Class I, seizure free; Class II, rare disabling seizures; Class III, worthwhile improvement; and Class IV, no worthwhile improvement).14,15 Patients with lesional ETLE have seizure-free rates (Engel Class I) of around 60% (at 1-year follow-up).9 In contrast, patients with nonlesional TLE demonstrate outcomes with seizure-free rates (Engel Class I) ranging from 41% to 65% (at 2-year follow-up).16-19 Patients with nonlesional ETLE have the lowest seizure-free outcomes, ranging from 24% to 42%
(at 2-year follow-up).20-22 A better understanding is necessary to evolve our approach toward recognizing the IOZ as a critical node in a larger epileptogenic network in order to achieve better seizure-free rates, particularly in nonlesional focal-onset epilepsy.
In the present study, we retrospectively analyzed the clinical history profiles including duration of epilepsy, video EEG (noninvasive and invasive) and MRI findings, subtraction ictal SPECT coregistered to MRI (SISCOM) data, seizure semiology, sites and sizes of resection, pathological findings, and postsurgical seizure outcomes in a cohort of patients with lesional and nonlesional ETLE and TLE. The aim of our study was to assess the positive predictive value of resecting SISCOM regions of transient hyperperfusion that were associated with the IOZ. Also, the long-term postsurgical outcomes in patients with both MRI-positive and MRI-negative ETLE and TLE were compared.
Methods
Patients
A total of 567 presurgical SPECT studies (243 patients) were performed at our center between 2002 and 2013. Our study included a cohort of 44 patients from this presurgical group who underwent resective epilepsy surgery. The mean age of the patients in our cohort was 29 years (range, 11-57 years; SEM, 1.8) (Table 1). Patients underwent follow-up for a mean of 5 years (range, 2-10 years). All patients in our cohort were assessed using chronic intracranial electrocorticography (ECoG) monitoring and/or acute intraoperative electrocorticography (aECoG). The placement of the electrodes for invasive monitoring was determined during the epilepsy surgery management conference at our institution. Multiple factors were analyzed to generate the hypothesis for intracranial electrode placement and targeting the IOZ. To facilitate localization of the IOZ, we employed seizure semiology, MRI,
RESECTING CRITICAL NODES FROM AN EPILEPTOGENIC CIRCUIT IN REFRACTORY FOCAL-ONSET EPILEPSY PATIENTS Using Subtraction Ictal SPECT Coregistered to MRI
Abhijay Jalota, MD; Marvin A. Rossi, MD, PhD; Volodymyr Pylypyuk, CNMT, NMTCB, ARRT(N); Michael Stein, MD; Travis Stoub, PhD; Antoaneta Balabanov, MD; Donna Bergen, MD; Adriana Bermeo, MD; Esmeralda Park, MD; Michael Smith, MD; Richard Byrne, MD

32 THE 2016 RUSH NEUROSCIENCE REVIEW
chronic noninvasive scalp video-EEG monitoring, magnetoencephalography, SISCOM, positron emission tomography, and neurocognitive testing (Table 2).
We included patients based on the following inclusion criteria: (1) diagnosis of drug-resistant, focal-onset epilepsy based on the presurgical evaluation that included SISCOM; and (2) resective epilepsy surgery performed with a postoperative follow-up of at least 24 months (mean follow-up, 5 years). The predominant reasons for exclusion from the study were (1) patient underwent less than 24 months of follow-up (except patients who remained as Engel Class IV), or (2) no interictal SPECT was acquired. Forty-four patients met all of the inclusion criteria and were analyzed in this study. One ETLE patient in the study had undergone a previous resection prior to a second resection. In 25 patients (61%), postresection MRI was performed. Preresection subtraction ictal SPECT was coregistered to the patient’s postresection MRI study, which was acquired at least 12 months postoperatively. This strategy was used to determine the regions of transient hyperperfusion in comparison with the extent of resection.
High-Resolution MRI
High-resolution, gapless, pregadolinium and postgadolinium, volumetric, spoiled gradient recalled (SPGR) MR images of the brain were obtained for each patient. The MRI examination was performed using a 1.5-T or 3-T scanner (Siemens). A gapless, SPGR, T1-weighted sequence data set for each patient was acquired at a slice thickness of 1.0 or 1.6 mm.
Noninvasive Video-EEG Monitoring
Chronic, noninvasive video-EEG monitoring was performed in each patient using the International 10-20 system for electrode placement, including anterior temporal and sphenoidal
electrodes if appropriate. AEDs were lowered during chronic monitoring, all patients were electrographically monitored to record the typical seizures, and video recordings were generated to monitor semiology.
SISCOM
SPECT was performed on each patient during video-EEG monitoring using Ceretec (99mTc-HMPAO) or Neurolite (99mTc-ECD) at a dose of 24 to 26 mCi (adjusted for body weight). The radiotracer was injected for the ictal SPECT studies with an autoinjector (MedRad) used by a specially trained nuclear medicine technologist (V.P.) while at the patient’s bedside during seizure onset. The technologist was trained to inject at the clinical and/or electroencephalographic seizure onset, whichever came first. The seizure-onset and ending times were always noted. Also, the time from the beginning of injection up to the complete depression of the syringe plunger was noted. We retrospectively calculated the time of the radiotracer injection following seizure onset by reviewing the video-EEG recordings for all patients. To avoid injection during the postictal state, a minimum of 15 seconds was required between the end of radiotracer injection and the end of the seizures, as described above. Baseline SPECT was obtained by performing an interictal injection after a seizure-free period of at least 24 hours. Brain SPECT scans were obtained within 2 hours after injection using a Siemens E.CAM Dual-Detector gamma camera with BiOCORE fan beam collimators. Thirty-two views per detector (total 64) were acquired using 80 000 counts per view, circular orbit, and “step and shoot” mode. Images were reconstructed by Syngo Siemens AG software using a 128x128 matrix with a Butterworth filter. DICOM isotropic datasets with a voxel size of 3.9 mm were created and transferred to Analyze software (AnalyzeDirect). Analyze version 10 was used to perform ictal and interictal SPECT thresholding, normalization, subtraction, and coregistration to the patient’s MRI study. Finally, the brain was segmented from the extracerebral structures, as identified on the patient’s volumetric MRI study. The cerebral surface of the binary ictal SPECT was matched to the cerebral surface of the binary MRI. The resulting registered transformation matrix was then applied to the subtraction SPECT data set in order to coregister it to the processed MRI study. Complete, gapless, SISCOM image sets were presented to a blinded, board-certified epilepsy neurologist (M.A.R.), who determined the SISCOM region of transient hyperperfusion for each patient in this study.
Invasive Recording
The ECoG electrode placement plan (subdural grid electrodes and/or depth electrodes) was confirmed using head CT. In 41 patients, chronic bedside ECoG monitoring was performed to investigate the clinical electrocerebral IOZ based on the patient’s stereotypic seizure. For 3 patients, aECoG monitoring alone provided enough information to establish the IOZ.
Characteristic Valuea
Resections, n 44
Age, y
Range 11-57
Mean 29
Male 23 (52%)
Female 21 (48%)
Right-handed 38 (86%)
Lesional temporal epilepsy 17 (38%)
Nonlesional temporal epilepsy 1 (2%)
Lesional extratemporal epilepsy 14 (32%)
Nonlesional extratemporal epilepsy 12 (27%)
Table 1. Characteristics of the Study Participants
a Values are shown as n (%) unless otherwise stated.

Pathology
A pathological diagnosis of the resected specimens, such as gliosis, focal cortical dysplasia, heterotopias, tumor, or mesial temporal sclerosis, was determined for 38 of 44 patients (86%) (Table 2).
Postoperative Seizure Outcomes
Postoperative outcomes were determined by following 38 patients for a period greater than 24 months (mean follow-up, 5 years; range, 2-10 years) after resection. We classified the postresection outcomes into 4 classes and subclasses according to Engel’s classification (Table 3).23 At the time of our analysis, 5 patients in our study received a follow-up period of 17 to 18 months. However, these patients remained classified as Engel Class IV. One of the patients in our study was observed for only 12 months. However, this patient remained Engel Class IVc (no worthwhile improvement, worsening of seizures after surgery).
Postresection MRI
We obtained postresection MRIs for 34 of 44 patients (77%). We coregistered the preresection SISCOM on postresection MRI in order to evaluate the extent of resection of the identified SISCOM region of hyperperfusion. Using traditional SISCOM processing with Analyze, we could not achieve accurate registration of the preresection SISCOM signals on the postresection MRI studies for all patients. Postresection MRI findings were considerably different from preresection MRI findings because of the creation of new cortical boundaries, particularly in the area of resection. In addition, the craniotomy flap altered the skull shape in some patients. Consequently, clean object extraction could not be achieved in several postresection MRI data sets, resulting in poor registration. To solve this problem, we employed a different postprocessing method. We performed 3-dimensional voxel registration using Analyze between the original fused preresection SISCOM, which was used as the base, and the postresection MRI, which was used as the match. We first performed manual registration
to achieve similar alignment in all 3 planes (transverse, coronal, and sagittal). We then performed autoregistration using the register tab in the 3-dimensional voxel registration window in Analyze. This process perfectly aligned the 2 3-dimensional objects, so that the each voxel in the new fused image represented the same voxel of the base (preresection SISCOM) and match (postresection MRI).
The intensities of the base and match were modified as follows. The minimum intensity of the base image was increased in order to make the preresection MRI disappear and reduce the maximum of the base in order to improve the SPECT signal. This technique prevented the preresection brain tissue boundary from filling the resection site. Thus, the fused image demonstrated the properties of the SPECT signal of the base, but not the MRI properties of the base. Lastly, we reduced the maximum intensity of the match to intensify the postresection MRI. This technique enabled us to better visualize the resection site. This process resulted in the accurate
Resecting Critical Nodes From an Epileptogenic Circuit in Refractory Focal-Onset Epilepsy Patients 33
All Subjects(n=44)
SISCOM & lesional MRIconcordant with ECoG/aECoG
(n=8)
SISCOM concordant, lesional MRI nonconcordant with
ECoG/aECoG(n=3)
SISCOM concordant, lesional MRI nonconcordant with
ECoG/aECoG(n=2)
SISCOM nonconcordant, lesional nonconcordant with
ECoG/aECoG(n=0)
SISCOM nonconcordant, lesional MRI concordant with
ECoG/aECoG(n=2)
SISCOM nonconcordant, lesional MRI nonconcordant
with ECoG/aECoG(n=4)
SISCOM nonconcordant, lesional MRI concordant with
ECoG/aECoG(n=5)
SISCOM concordant withECoG/aECoG nonlesional MRI
(n=2)
SISCOM concordant withECoG/aECoG nonlesional MRI
(n=11)
SISCOM & lesional MRIconcordant with ECoG/aECoG
(n=6)
SISCOM concordant withECoG/aECoG &
overlapping the resection site
(n=32)
SISCOM nonconcordant with ECoG/aECoG & not
overlapping the resection site
(n=11)
SISCOM nonconcordant with ECoG/aECoG &
overlapping the resection site
(n=1)
TLE(n=13)
TLE(n=5)
ETLE(n=19)
ETLE(n=6)
Figure 1. Classification hierarchy of patient outcomes after resective epilepsy surgery. Three main groups are repre-sented: (1) subtraction ictal SPECT coregistered to MRI (SISCOM) concordant with electrocorticography (ECoG) and overlapping with the resection site; (2) SISCOM nonconcordant with ECoG and nonoverlapping with the resection site in temporal lobe epilepsy (TLE) patients; and (3) SISCOM nonconcordant with ECoG and overlapping with the resection site. aECoG, acute intraoperative electrocorticography.

34 THE 2016 RUSH NEUROSCIENCE REVIEW
Pt No.
Age, y/Sex
Hand- edness
Duration of Epilepsy, y
MRI Finding Pathology Scalp EEG ECoG Onset Injection Time, s
No. of Seizures During Injection
SISCOM Focus Surgery EcoG/SISCOM Concordance
Complete/Partial Resection
Outcome (Engel Class)a
1 32/M Rt 31 Normal Gliosis Bilat frontal (1) Lt mesiofrontal, lt orbitofrontal; (2) surrounding prior resection
11 3 Lt ant cingluate cortex
(1) SFG, MFG, sparing lt MFG; (2) lt anterior frontal
No NA IVb
2 45/F Rt 38 Cavernoma, Lt H Gliosis Rt frontal Rt mesiofrontal 62 11 Rt post supramarginal gyrus/STG
Rt frontal, IFG, MFG, SFG
No NR Ia
3 50/M Rt 45 Lt MTS MTS Lt temp Lt ant temp NA 2 Lt ant temp/H Lt ant temp; STG, MTG, ITG, AHC
Yes Complete Id
4 12/M Rt 5 Normal Inflammation Bilat frontal Rt mesiofrontal, rt posteroinferior frontal
21 1 Rt ant insula Rt frontal, SFG + ant corpos callostomy
Yes NA lb
5 27/M Rt 26 Rt frontoparietal cortical effacement
FCD Bilat frontal (rt>lt) Rt mesiofrontal 20 2 Rt basal frontal Rt basal frontal Yes Partial IVb
6 29/M Rt 8 Lt temp tumor Epidermoid cyst
Lt temp Lt ant temp, lt post temp
12 4 Lt ant temp Lt ant temp; STG, MTG, ITG, tumorectomy, AHC
Yes Partial Ia
7 51/F Rt 45 Normal Hemorrhage Bilat frontal, lt temp
Lt mesiofrontal 8 2 Lt mesiofrontal Lt mesiofrontal Yes Partial Ic
8 24/F Rt 17 Normal Heterotopia Rt temp, rt frontal H
Rt orbitofrontal 44 8 Rt frontal Rt SFG, IFG + partial MFG + ant mesio-temp + rt ant temp
Yes Complete IVb
9 31/M Rt 14 Rt frontal tumor FCD Lt temp & lt frontal
Lt ant inferior temp 72 2 Lt anterobasal temp
Lt ant temp; STG, MTG, ITG, AHC
Yes Partial la
10 57/M Lt 50 Lt-sided tumor Inflammation Lt frontal Lt mesial frontal 11 16 Lt mesiofrontal Lt hemispherectomy
Yes Partial IVa
11 40/F Rt 21 Lt MTS + tumor MTS, heterotopia
Lt temp & midpost rt frontal
Lt temp 23 1 Lt hippocampus Lt temp; STG, MTG, ITG, AHC
Yes Partial Ia
12 39/0 Rt 19 Rt frontal tumor Gliosis Rt temp & rt basal frontal
Rt ant, middle temp, rt basal frontal
22 1 Rt basofrontal, rt temp
Rt ant temp; STG, MTG, ITG, AHC
Yes Complete IVa
13 14/F Rt 3 Normal Hemorrhage Bilat frontal Rt lateral frontal, rt orbitofrontal
11 1 Lt paramesial premotor cortex
Rt frontal No Partial Ia
14 41/F Rt 36 Rt FCD FCD Nonlocalizable Rt mesial frontal 54 10 Rt mesiofrontal Rt frontal; SFG Yes Complete Ia
15 11/M Rt 2 Lt cingulate tumor
Neurocytoma Lt temp Lt frontal, SFG 330 5 Lt mesiofrontal Lt frontal; SFG, lt parietal tumorectomy
Yes Partial Ia
16 28/M Lt 27 Normal FCD Lt frontal Lt basal frontal 41 3 Lt basal frontal Lt frontal; SFG, MFG, IFG
Yes Complete Ib
17 50/F Rt 46 Lt MTS MTS Lt frontal Lt mesial temp, lt ant frontal
17 6 Lt ant temp Lt temp; STG, MTG, ITG, AHC
Yes Partial la
18 36/F Rt 30 Rt frontal tumor Giant cell astrocytoma
Bilat frontoparietotemp multifocal
Rt ant mesial frontal 11 1 Rt post frontal Rt ant frontal, tumorectomy
No NA IVb
19 17/F Rt 15 Ischemia or demyelination
Gliosis Lt temp Lt basal temp 40 1 Lt basal temp Lt ant temp; STG, MTG, ITG, AHC
Yes NR IIIa
20 33/F Rt 25 Normal Gliosis Rt temp Rt ant temp 3 NA Rt ant temp Rt ant temp, AHC Yes Partial IIIb
21 10/F Lt 3 Lt frontal tumor Meningioma Bilat frontal, rt frontopolar
Lt ant frontal 22 1 Rt hippocampal frontal
Lt frontal tumor No NR la
22 49/M Rt 46 Rt MTS Rt MTS + heterotopia
Rt H, post quadrant
Rt posterolateral temp
21 1 Rt posterolateral temp
Rt ant temp; STG, MTG, ITG, AHC
Yes NA Ia
23 27/M Rt 4 Rt MTS MTS Rt ant temp, lt frontotemp
Rt ant temp 21 3 Bilat temp Rt temp; STG, MTG, ITG, AHC
No NR Ia
24 16/F Lt 15 Lt temp tumor Inflammation Lt post quadrant; rt frontal
Lt frontocentrotemp 10 1 Lt post basal temp
Lt AHC & resection of scar around the prior stroke cavity
Yes NR IIIa
25 23/F Rt 12 Bilat FCD (It occipital lobe) MTS
Gliosis Lt occipital/lt temp Lt anterior mesial temporal
12 3 Lt ant temp Lt ant temp; STG, MTG, ITG, AHC
Yes NA IIa
26 25/M Rt 15 Normal Gliosis Rt mesiofrontal, rt temp
Rt mesial frontal 87 3 Rt basal frontal Rt frontal Yes Partial IVc
27 13/M Rt 4 Ischemia or demyelination
Inflammation Rt frontal Rt lateral frontal 3 NA Rt lateral frontal Rt frontal back to the area of precentral sulcus
Yes NR IVc
28 27/M Rt 14 Normal Gliosis Bilat frontal Rt mesial frontal 375 NA Rt basal frontal, rt mesiofrontal
Rt SFG, cingulate sulcus
Yes NR Ia
29 27/M Rt 14 Normal NA NA Rt orbitofrontal 11 10 Rt orbitofrontal Rt orbitofrontal, MFG
Yes Partial Ia
30 37/F Rt 10 Ischemia or demyelination
NA Rt frontal, lt post quadrant
Rt mesial frontal 9 4 Rt mesiofrontal MST, leg area over to the lateral convexity rt frontal
Yes NA Ic
31 20/F Rt 3 Normal MTS Rt mesiotemporal Rt temp 3 NA Rt basal temp Rt temp Yes NA Ib
32 24/F Rt 19 Rt FCD Gliosis Nonlocalizable rt mesiofrontal, also bilat frontal spikes
Rt mesial frontal 129 3 Rt dorsolateral frontal
Rt frontal-SFG using bipolar & resection
No NA IIIa
Table 2. Clinical Data of All Patients Included in the Study

Resecting Critical Nodes From an Epileptogenic Circuit in Refractory Focal-Onset Epilepsy Patients 35
registration of the preresection, SISCOM hyperperfusion signals over the postresection MRI, and, at the same time, improved the intensity of the resection site.
Analysis and Statistics
Concordance was determined between SISCOM localization and ECoG on the basis of an overlapping IOZ and called “concordance with the ECoG.” Concordance was also determined between SISCOM localization and the resection site, or “concordance with the resection site.” Two different concordance types are designated since resection usually involves a larger area than the IOZ, as determined by ECoG. Strict concordance criteria were used, where greater than 90% of the resected area must overlap with the SISCOM signal to be considered concordant. Concordance was determined by a blinded, board-certified epilepsy neurologist (M.A.R.).
We coregistered preresection and subtracted ictal SPECT on postresection MRI to determine if the SISCOM signal was completely or partially removed. We determined if complete or partial resection impacted postoperative outcomes.
Our cohort of 44 patients underwent resective epilepsy surgery. All patients underwent follow-up for at least 2 years (mean follow-up, 5.0 years; range, 2-10 years). Five patients received
only 17 to 18 months of follow-up at the time of our analysis, but these patients demonstrated Engel Class IV outcomes. One of the patients completed a follow-up of only 12 months, but achieved Engel Class IVc. The mean radiotracer injection time for all patients was 45 seconds (SEM, 11.4) after electrocerebral seizure onset. In our cohort, all SPECT studies were performed during the patient’s stereotypic seizures, as measured electrographically or clinically.
Results
ECoG Monitoring
ECoG concordant tissue was completely resected from all 44 patients. Of these 44 patients, 24 of 44 (55%) became seizure free (Engel Class I) after at least 2 years of follow-up after resection.
SISCOM Concordance
SISCOM was concordant with ECoG and the resection site in 32 of 44 patients (73%), and 20 of these 32 (63%) became seizure free (Engel Class I after greater than 2 years of follow-up). Of these, 32 patients, 19 of 32 (59%) had ETLE and 13 of 32 (41%) had TLE (Figure 1). The mean injection time was 46 seconds in the SISCOM ECoG concordant group (SEM, 14.5).
Abbreviations: aECoG, acute intraoperative electrocorticography; AHC, amygdalohippocampectomy; ant, anterior; bilat, bilateral; ECoG, electro-corticography; FCD, focal cortical dysplasia; H, hemisphere; HF, hippocampus; IFG, inferior frontal gyrus; ITG, inferior temporal gyrus; lt, left; MFG, middle frontal gyrus; midpost, midposterior; MST, multiple subpial transection; MTG, middle temporal gyrus; MTS, mesial temporal sclerosis; NA, not available; NR, not resected; post, posterior; pt, patient; rt, right; SFG, superior frontal gyrus; SISCOM, subtraction ictal SPECT coregistered to MRI; STG, superior temporal gyrus; temp, temporal.a Engel classification: Ia, completely seizure free since surgery; Ib, nondisabling, simple partial seizures only after surgery; Ic, some disabling seizures after surgery, but free of disabling seizures for at least 2 years; Id, generalized convulsions with antieptileptic drug discontinuation only; IIa, initially free of disabling seizures, but has rare seizures now; IIIa, worthwhile seizure reduction; IIIb, prolonged, seizure-free intervals amounting to greater than half of the follow-up period, but for less than 2 years; IVa, significant seizure reduction; IVb, no appreciable change; IVc, seizures worse after surgery.
33 41/F Rt 39 Rt temp, rt occipital, & rt parietal FCD
FCD Rt parietal quadrant
Rt temp, seizure foci in rt parietal & rt occipital
28 2 Rt parietal Rt temp, rt parietooccipital
Yes Complete Ib
34 25/M Rt 6 Lt temp tumor Old hemorrhage
Lt temp, rt frontal Lt temporal 76 5 Rt STG (1) Lt temp; (2) Rt neurospace concordant w/SISCOM
No NR IIc
35 15/M Rt 8 Normal Subdural hematoma
Rt frontal Rt mesial frontal 15 5 Rt mesiofrontal Rt mesiofrontal Yes NA Ib
36 35/F Rt 29 Bilat MTS Gliosis Rt frontotemp Rt anterior frontal, rt temp
NA 5 Nonlocalizing/nonlateralizing
Rt frontal; MFG, IFG
No NR Ib
37 20/M Rt 12 Rt H w/ double cortex
NA Nonlocalizable rt parietal sharp waves
Rt parietal 13 5 Rt parietal NA Yes NR IVa
38 11/F Rt 10 Lt frontal FCD NA Lt frontal Lt lateral frontal 12 2 Rt mesiofrontal NA No Complete IIIb
39 32/M Rt 25 Normal NA Lt temp Lt temp, ant temp 3 NA Lt ant temp Lt basal temp Yes Partial Ia
40 24/F Lt 19 Normal, sinus disease
Gliosis Nonlocalizable bilat frontal slowing
Rt mesiofrontal 11 13 Rt mesiofrontal Rt mesial frontal Yes NA IVb
41 31/F Rt 24 MTS MTS Lt frontotemp Lt ant temp 9 5 Lt anterobasal temp region
Lt ant temp STG, MTG, ITG
Yes Complete Ia
42 44/M Rt 41 Lt MTS MTS Nonlocalizable Lt ant temp & lt basal temp
30 6 Lt basal frontal region
Lt ant temp STG, MTG, ITG, AHC
No NR Ia
43 20/M Rt 5 Rt frontal encephalomalacia
NA Bilat mesial frontal Rt prefrontal cortex 118 42 Rt basal frontal Rt frontal & STG Yes Partial Ic
44 24/M Rt 4 Rt arachnoid cyst Gliosis Lt temp Lt ant polar temp region
39 2 Lt basal temp region
Lt temp STG, MTG, ITG
Yes NA IVb

36 THE 2016 RUSH NEUROSCIENCE REVIEW
SISCOM Concordant ETLE Group
In 19 ETLE patients with concordant SISCOM and ECoG results, ECoG delineated the epileptogenic source or focus, which was completely resected in all patients; 11 of 19 patients (58%) became seizure free (Engel Class I) (Table 3).
Among these 19 ETLE patients, 8 patients exhibited a lesion on MRI (focal cortical dysplasia, tumor, double cortex, or encephalomalacia). Only 6 of these 8 patients exhibited an MRI lesion and SISCOM focus that were both concordant with the ECoG results; only 3 of these 6 patients (50%) became seizure free (Engel Class I) (Table 3).
Also, among these 19 ETLE patients, 11 patients were MRI negative for lesions. For these patients, SISCOM facilitated the placement of the intracranial electrodes; 7 patients (64%) became seizure free (Engel Class I) (Table 3).
SISCOM Concordant TLE Group
In the 13 TLE patients with concordant SISCOM and ECoG results, the indicated ECoG focus was completely resected; 9 of 13 patients (69%) became seizure free (Engel Class I) (Table 3).
Among these 13 TLE patients, 11 patients had a lesion (mesial temporal sclerosis, focal cortical dysplasia, or tumor) on MRI.
Figure 2. Presentation of patients with subtraction ictal SPECT coregistered to MRI (SISCOM) foci localizing with the resection site. These patients demonstrated poor surgical outcomes (Engel Class IV) and at least 1 SISCOM region did not overlap with the resection site.
26
8
24
5
19
12
PatientNumber
Preresection SISCOM Preresection SISCOM co-registered to postresection MRI
Preresection acquired SISCOM
Engel Class ETLE TLE
SISCOM & Lesional MRI
Concordant w/ aECoG/ECoG
(n=6)
SISCOM Concordant, Lesional MRI
Nonconcordant w/ aECoG/ECoG
(n=2)
SISCOM Concordant w/ aECoG/ECoG,
Nonlesional MRI (n=11)
SISCOM & Lesional MRI
Concordant w/ aECoG/ECoG
(n=8)
SISCOM Concordant, Lesional MRI
Nonconcordant w/ aECoG/ECoG
(n=3)
SISCOM Concordant w/ aECoG/ECoG,
Nonlesional MRI (n=2)
I 3 (50%) 1 (50%) 7 (64%) 7 (88%) 1 (33%) 1 (50%)
II 0 0 0 0 1 (33%) 0
III & IV 3 (50%) 1 (50%) 4 (36%) 1 (12%) 1 (33%) 1 (50%)
Table 3. SISCOM Concordant With ECoG and Overlapping With the Resection Site in ETLE Patients (n=19) and TLE Patients (n=13)a
Abbreviations: aECoG, acute intraoperative electrocorticography; ECoG, electrocorticography; ETLE, extratemporal lobe epilepsy; SISCOM, subtraction ictal SPECT coregistered to MRI; TLE, temporal lobe epilepsy.a Values are shown as n (%).

Resecting Critical Nodes From an Epileptogenic Circuit in Refractory Focal-Onset Epilepsy Patients 37
Only 8 of these 11 patients demonstrated an MRI lesion and SISCOM focus that were both concordant with the ECoG results; 7 of these 8 patients (88%) became seizure free (Engel Class I) (Table 3).
Also, among these 13 TLE patients, 2 patients were MRI negative. For these patients, SISCOM guided the placement of the intracranial electrodes; 1 patient (50%) became seizure free (Engel Class I) (Table 3).
Nonconcordant Group
SISCOM was nonconcordant with ECoG but overlapped with the resection site in only 1 of 44 patients. This patient was diagnosed with nonlesional ETLE but did not have a lesion on MRI. This patient demonstrated a worse outcome after resection and achieved Engel Class IV (greater than 2 years of follow-up, Figure 1).
SISCOM was nonconcordant with ECoG and nonoverlapping with the resection site in 11 of 44 patients (Figure 1). In the nonconcordant group, 4 of 11 patients (36%) achieved Engel Class I, 1 of 11 patients (9%) achieved Engel Class II (rare disabling seizures), 2 of 11 patients (18%) achieved Engel Class III (worthwhile improvement), and 4 of 11 patients (36%) achieved Engel Class IV. All of these 11 patients exhibited lesions on MRI (Table 4).
For the SISCOM nonconcordant group, the average injection time was 37 seconds (SEM, 11.3).
Resection of SISCOM Focus
We coregistered the preresection subtraction ictal SPECT to each patient’s postresection MRI in order to determine if the SISCOM signal(s) used to guide the placement of the intracranial electrodes preresection was completely, partially, or not resected. A 10% shifting of the adjacent brain postresection was assumed in the postresection MRI coregistrations. Postresection MRI studies were completed in 35 of 44 patients (80%).
Complete resection of the SISCOM signal was found in 7 of 34 patients (21%). Of these 7 patients, 5 patients (72%) were seizure free (Engel Class I). Partial resection of the SISCOM signal was found in 16 of 34 patients (47%); 10 of these 16 patients (62%) were seizure free (Engel Class I) after more than 24 months of follow-up (Table 5).
The SISCOM signal was not resected in 11 of 34 patients (32%). Four of these 11 patients (36%) were seizure free (Engel Class I) after more than 24 months of follow-up.
Pathology
The pathological findings (gliosis and focal cortical dysplasia) were not significantly correlated with the outcomes of epilepsy surgery (P=.1007; Table 2).
Discussion
The success of epilepsy surgery depends on the accurate anatomical localization of the IOZ, which is indispensable to contributing to favorable outcomes. The IOZ is a component of the ictal circuitry that is critically involved in the initiation of seizures. Scalp EEG and semiology are often not sensitive enough to accurately delineate the IOZ in rapidly propagating seizures. Consequently, the development of novel neuroimaging approaches is required to facilitate visualizing the IOZ, particularly in patients with ETLE. SISCOM can help identify the IOZ, though its limitations as an indirect measure of increased metabolic demand in the nearby epileptogenic cortex must be kept in mind. The probability of seizure freedom in our cohort is highest for lesions identified on MRI. Patients with MRI findings showing lesions in 1 temporal lobe that are concordant with ipsilateral ictal activity on EEG have the highest rate of seizure freedom after resective epilepsy surgery.8,9 In our cohort, 7 patients demonstrated underlying lesions in 1 temporal lobe (predominantly mesial temporal sclerosis), and a concordant abnormality on scalp EEG was noted in 6 of these patients; all 7 of 7 patients (100%) achieved Engel Class I with longer than 3 years of follow-up (mean follow-up, 4.9 years).
Engel Class ETLE TLE
SISCOM Nonconcordant,
Lesional MRI Concordant w/ aECoG/ECoG
(n=2)
SISCOM Nonconcordant,
MRI Lesional Nonconcordant w/ aECoG/ECoG
(n=4)
SISCOM Nonconcordant,
MRI Lesional concordant w/ aECoG/ECoG
(n=5)
SISCOM Nonconcordant,
Lesional MRI Nonconcordant w/ aECoG/ECoG
(n=0)
I 1 (50%) 1 (25%) 2 (40%) 0
II 0 0 1 (20%) 0
III & IV 1 (50%) 3 (75%) 2 (40%) 0
Table 4. Outcomes for SISCOM Nonconcordant With aECoG/ECoG and Nonoverlapping With the Resection Site (n=11)a
Abbreviations: aECoG, acute intraoperative electrocorticography; ECoG, electrocorticography; ETLE, extra-temporal lobe epilepsy; SISCOM, subtraction ictal SPECT coregistered to MRI; TLE, temporal lobe epilepsy.a Values are shown as n (%).

38 THE 2016 RUSH NEUROSCIENCE REVIEW
SISCOM was concordant with the resection site in 6 of 8 (75%) of these patients.
It has been previously shown that the probability of seizure freedom (Engel Class I) at the 12-month follow-up after surgery is 2.7 times higher in TLE patients with MRI lesions in comparison with TLE patients without MRI lesions.9 Moreover, the probability of seizure freedom (Engel Class I) at the 12-month follow-up after surgery is 2.9 times higher in ETLE patients with MRI lesions in comparison with ETLE patients without MRI lesions.9 SISCOM impacted our postresection outcomes in the nonlesional ETLE and TLE patient groups. Also, the complete or partial resection of the SISCOM region of transient hyperperfusion plays a role in seizure freedom; 5 of 7 patients (72%) were seizure free after complete resection of SISCOM hyperperfusion-related signaling, and 10 of 16 patients (63%) were seizure free after the partial resection of similar SISCOM signals. In our study, 6 patients exhibited SISCOM signal foci localized with the resection site; these patients demonstrated poor surgical outcomes (Engel Class IV), and at least 1 SISCOM region not overlapping with the resection site (Figure 2). Concordance between SISCOM and
ECoG had a sensitivity of 72.7%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 14.3%.
Improved outcomes were seen with earlier surgery for intractable frontal lobe epilepsy.24 In our study, the mean duration of frontal lobe epilepsy was 19.17 years. When the duration of frontal lobe epilepsy was less than 5 years, 75% became seizure free (n=4; 3 MRI lesion-positive patients and 1 MRI lesion-negative patient) (Engel Class I, mean year of follow-up postresection, 7.7 years; range, 6-10 years; SD, 2.08). However, when the duration of frontal lobe epilepsy was at least 5 years, 59% became seizure free (n=17; 7 MRI lesion-positive and 10 MRI lesion-negative patients) (Engel Class I, mean year of follow-up postresection, 7.3 years; range, 3-11; SD, 2.8).
According to previously published success rates for partial frontal lobectomy, favorable outcomes (Engel Class I) range from 15% to 35% in these trials.21,25-29 The only variable that was significantly associated with a favorable surgical outcome was a focal MRI abnormality in frontal lobe epilepsy.8 Elsharkawy et al published a retrospective study investigating 97 patients with lesional frontal lobe epilepsy who underwent
Marvin Rossi, MD, PhD (right), in Rush's neuroimaging and neuroengineering laboratory.

resection.30 This study reported the seizure freedom rates (Engel Class I) to be 54.6% at 6 months, 49.5% at 2 years, 47% at 5 years, and 41.9% at 10 years.30 In yet another series, 41% of nonlesional TLE patients showed excellent outcomes versus 72% when an MRI abnormality was present.31 Previous studies that report favorable (Engel Class I) outcomes investigated patients with frontal lobe tumors or focal cortical dysplasias.29 Other factors that predict seizure recurrence include incomplete resection of the epileptogenic lesion,25,29,30,32,33 predominantly generalized or poorly localized ictal EEG patterns on surface EEG,30,32,34 the lack of a subdural grid evaluation,30,32 acute postresection seizures,6 postoperative persistence of prolonged auras,30,32 history of febrile seizures,31 and the lack of a distinct MRI lesion.25,30,32-35
The SISCOM results in our study patients influenced the planning of intracranial electrode placement. Therefore, our ECoG results were, in part, influenced by our SISCOM data. Also, all patients in our cohort underwent SISCOM as part of the presurgical evaluation. Therefore, potential selection bias toward patients with more localizable IOZ has to be regarded, and consequently resulted in more favorable postresection outcomes.
Conclusions
The goal of resective epilepsy surgery is long-term seizure freedom (Engel Class I or II). Seizure outcomes are time dependent and dynamic. All prognostic factors converge into one central theme: an epileptogenic zone that is well visualized and also electrically and semiologically restricted, in that its extent offers the best chance of seizure freedom when resected completely. However, SISCOM provides an indirect measure of localizing the IOZ, which often coincides with the critical nodes within the epileptogenic network.
These data confirm previous studies that demonstrate the utility of SISCOM by improving the outcomes of drug-resistant, focal-onset epilepsy in both ETLE and TLE patients. Concordance between SISCOM and ECoG and/or aECoG in this refractory
epilepsy cohort provide useful additional information for predicting postresection outcomes. In addition, the limitations in SPECT scanner technology may contribute to the sensitivity of SISCOM for identifying the maximal extent of the critical nodes or the generators of the epileptogenic circuit. The predominant limitation of conventional SPECT technology is the voxel resolution, which is limited to 8 to 12 mm with inadequate attenuation correction. The limitations of the spatial resolution of SPECT are related to using only 2-head and 3-head photon detectors to record low-energy single-photon events. Next-generation SPECT scanner systems with significantly improved resolution and complementary postprocessing techniques will facilitate identifying a greater extent of critical nodes in the epileptogenic network.36 Such technology will augment guiding of ECoG electrode placement in potentially extensive epileptogenic networks.
Conflict of Interest
Dr Byrne reports that he is a consultant for Stryker and Integra.
Resecting Critical Nodes From an Epileptogenic Circuit in Refractory Focal-Onset Epilepsy Patients 39
Engel Class ETLE TLE
Lesional MRI Concordant w/ aECoG/ECoG
(n=2)
Lesional MRI Nonconcordant w/ aECoG/ECoG
(n=2)
MRI Nonlesional (n=6)
Lesional MRI Concordant with
aECoG/ECOG (n=4)
Lesional MRI Nonconcordant w/
aECoG/ECoG (n=1)
MRI Nonlesional (n=1)
I 1 (50%) 1 (50%) 4 (67%) 3 (75%) 1 0
II 0 0 0 0 0 0
III & IV 1 (50%) 1 (50%) 2 (33%) 1 (25%) 0 1
Table 5. Outcomes in Patients With Partial Resection of the SISCOM Focus in ETLE (n=10) and TLE (n=6)a
Abbreviations: aECoG, acute intraoperative electrocorticography; ECoG, electrocorticography; ETLE, extratemporal lobe epilepsy; SISCOM, subtraction ictal SPECT coregistered to MRI; TLE, temporal lobe epilepsy.a Values are shown as n (%).

40 THE 2016 RUSH NEUROSCIENCE REVIEW
References1. Theodore WH, Spencer SS, Wiebe S, et al. Epilepsy in North America: a report prepared under the auspices of the global campaign against epilepsy, the International Bureau for Epilepsy, the International League Against Epilepsy, and the World Health Organization. Epilepsia. 2006;47(10):1700-1722.
2. Kwan P, Brodie MJ. Effectiveness of first antiepileptic drug. Epilepsia. 2001;42(10):1255-1260.
3. Berg AT, Kelly MM. Defining intractability: comparisons among published definitions. Epilepsia. 2006;47(2):431-436.
4. Brodie MJ, Kwan P: Staged approach to epilepsy management. Neurology. 2002;58 (8)(suppl 5):S2-S8.
5. Brodie MJ, Dichter MA. Antiepileptic drugs. N Engl J Med. 1996;334(3):168-175.
6. Sander JW. Some aspects of prognosis in the epilepsies: a review. Epilepsia. 1993;34(6):1007-1016.
7. Schmidt D, Gram L. Monotherapy versus polytherapy in epilepsy: a reappraisal. CNS Drugs. 1995;3(3):194-208.
8. Ferrier CH, Engelsman J, Alarcón G, Binnie CD, Polkey CE. Prognostic factors in presurgical assessment of frontal lobe epilepsy. J Neurol Neurosurg Psychiatry. 1999;66(3):350-356.
9. Téllez-Zenteno JF, Hernández Ronquillo L, Moien-Afshari F, Wiebe S. Surgical outcomes in lesional and non-lesional epilepsy: a systematic review and meta-analysis. Epilepsy Res. 2010;89(2-3):310-318.
10. Wieshmann UC, Larkin D, Varma T, Eldridge P. Predictors of outcome after temporal lobectomy for refractory temporal lobe epilepsy. Acta Neurol Scand. 2008;118(5):306-312.
11. Carne RP, O’Brien TJ, Kilpatrick CJ, et al. MRI-negative PET-positive temporal lobe epilepsy: a distinct surgically remediable syndrome. Brain. 2004;127(pt 10):2276-2285.
12. Hong KS, Lee SK, Kim JY, Lee DS, Chung CK. Pre-surgical evaluation and surgical outcome of 41 patients with non-lesional neocortical epilepsy. Seizure. 2002;11(3):184-192.
13. Kutsy RL. Focal extratemporal epilepsy: clinical features, EEG patterns, and surgical approach. J Neurol Sci. 1999;166(1):1-15.
14. Berkovic SF, McIntosh AM, Kalnins RM, et al. Preoperative MRI predicts outcome of temporal lobectomy: an actuarial analysis. Neurology. 1995;45(7):1358-1363.
15. Eliashiv SD, Dewar S, Wainwright I, Engel J Jr, Fried I. Long-term follow-up after temporal lobe resection for lesions associated with chronic seizures. Neurology. 1997;48(3):621-626.
16. Bell ML, Rao S, So EL, et al. Epilepsy surgery outcomes in temporal lobe epilepsy with a normal MRI. Epilepsia. 2009;50(9):2053-2060.
17. Holmes MD, Born DE, Kutsy RL, Wilensky AJ, Ojemann GA, Ojemann LM. Outcome after surgery in patients with refractory temporal lobe epilepsy and normal MRI. Seizure. 2000;9(6):407-411.
18. Radhakrishnan K, So EL, Silbert PL, et al. Predictors of outcome of anterior temporal lobectomy for intractable epilepsy: a multivariate study. Neurology. 1998;51(2):465-471.
19. Sylaja PN, Radhakrishnan K, Kesavadas C, Sarma PS. Seizure outcome after anterior temporal lobectomy and its predictors in patients with apparent temporal lobe epilepsy and normal MRI. Epilepsia. 2004;45(7):803-808.
20. Cohen-Gadol AA, Wilhelmi BG, Collignon F, et al. Long-term outcome of epilepsy surgery among 399 patients with nonlesional seizure foci including mesial temporal lobe sclerosis. J Neurosurg. 2006;104(4):513-524.
21. Lee SK, Lee SY, Kim KK, Hong KS, Lee DS, Chung CK. Surgical outcome and prognostic factors of cryptogenic neocortical epilepsy. Ann Neurol. 2005;58(4):525-532.
22. Noe K, Sulc V, Wong-Kisiel L, et al. Long-term outcomes after nonlesional extratemporal lobe epilepsy surgery. JAMA Neurol. 2013;70(8):1003-1008.
23. Engel J Jr, Van NP, Rasmussen TB, Ojemann LM. Outcome with respect to epileptic seizures. In: Engel J Jr, ed. Surgical Treatment of the Epilepsies. New York, NY: Raven Press; 1993:609-621.
24. Simasathien T, Vadera S, Najm I, Gupta A, Bingaman W, Jehi L. Improved outcomes with earlier surgery for intractable frontal lobe epilepsy. Ann Neurol. 2013;73(5):646-654.
25. Chung CK, Lee SK, Kim KJ. Surgical outcome of epilepsy caused by cortical dysplasia. Epilepsia. 2005;46(suppl 1):25-29.
26. Ferrier CH, Alarcon G, Engelsman J, et al. Relevance of residual histologic and electrocorticographic abnormalities for surgical outcome in frontal lobe epilepsy. Epilepsia. 2001;42(3):363-371.
27. Rasmussen T. Tailoring of cortical excisions for frontal lobe epilepsy. Can J Neurol Sci. 1991;18 (4)(suppl):606-610.
28. Swartz BE, Delgado-Escueta AV, Walsh GO, et al. Surgical outcomes in pure frontal lobe epilepsy and foci that mimic them. Epilepsy Res. 1998;29(2):97-108.
29. Zaatreh MM, Spencer DD, Thompson JL, Blumenfeld H, Novotny EJ, Mattson RH, et al. Frontal lobe tumoral epilepsy: clinical, neurophysiologic features and predictors of surgical outcome. Epilepsia. 2002;43(7):727-733.
30. Elsharkawy AE, Alabbasi AH, Pannek H, et al. Outcome of frontal lobe epilepsy surgery in adults. Epilepsy Res. 2008;81(2-3):97-106.
31. Mosewich RK, So EL, O’Brien TJ, et al. Factors predictive of the outcome of frontal lobe epilepsy surgery. Epilepsia. 2000;41(7):843-849.
32. Jeha LE, Najm I, Bingaman W, Dinner D, Widdess-Walsh P, Lüders H. Surgical outcome and prognostic factors of frontal lobe epilepsy surgery. Brain. 2007;130(pt 2):574-584.
33. Wetjen NM, Cascino GD, Fessler AJ, et al. Subtraction ictal single-photon emission computed tomography coregistered to magnetic resonance imaging in evaluating the need for repeated epilepsy surgery. J Neurosurg. 2006;105(1):71-76.
34. Yun CH, Lee SK, Lee SY, Kim KK, Jeong SW, Chung CK. Prognostic factors in neocortical epilepsy surgery: multivariate analysis. Epilepsia. 2006;47(3):574-579.
35. Najm I, Jehi L, Palmini A, Gonzalez-Martinez J, Paglioli E, Bingaman W. Temporal patterns and mechanisms of epilepsy surgery failure. Epilepsia. 2013;54(5):772-782.
36. Jain M, Krug K, Balaguera P, et al. Moving towards new techniques in the evaluation of the ictal onset zone: ratio ictal SPECT (RISCOM) using a 72-detector focused collimator ring SPECT scanner system, Presented at: American Epilepsy Society 68th Annual Meeting, 2014; Seattle, WA. Abstract 2.241. https://www.aesnet.org/meetings_events/annual_meeting_abstracts/view/1868323. Accessed February 1, 2016. ◆

Author Affiliations: Department of Physical Therapy and Human Movement Sciences, Northwestern University (Drs David, Poon, and Corcos), Chicago, Illinois; Department of Physical Therapy, University of Illinois at Chicago, Chicago, Illinois (Dr Robichaud); Departments of Neurological Sciences and Preventive Medicine, Rush University Medical Center, Chicago, Illinois (Dr Leurgans); Division of Geriatric Medicine, University of Colorado School of Medicine, Aurora, Colorado (Dr Kohrt); Department of Neurological Sciences, Section of Parkinson Disease and Movement Disorders, Rush University Medical Center, Chicago, Illinois (Drs Goldman, Comella, and Corcos); Departments of Applied Physiology and Kinesiology, Biomedical Engineering, and Neurology, University of Florida, Gainesville, Florida (Dr Vaillancourt).
Corresponding Author: Fabian J. David, PhD, Department of Physical Therapy and Human Movement Sciences, Northwestern University, 645 N Michigan Ave, Suite 1100, Chicago, IL 60611 ([email protected]).
Previous Publication: This article was previously published in Mov Disord 2015;30(12):1657-1663. Minor edits have been made.
Introduction
Cognitive impairment,1-4 including attention and working memory deficits,5 is frequently observed in Parkinson disease (PD). It is estimated that 78% of patients with PD will develop dementia.6 Treating cognitive impairment is a challenge given that it is often unresponsive to dopaminergic therapies.7 Recent work from the 90+ Study suggests that poor overall physical performance is a strong predictor of cognitive decline.8 The beneficial effects of exercise training on cognitive performance are well recognized in aging,9 as well as in individuals with dementia.10 In PD, preliminary research on the effects of exercise on cognition is promising,11 but long-term randomized controlled trials (RCTs) are needed.12
Recently, the Progressive Resistance Exercise Training in PD (PRET-PD)13 trial reported that, compared to modified Fitness Counts (mFC),14 Progressive Resistance Exercise Training (PRET) reduced the off-medication motor section of the Unified Parkinson’s Disease Rating Scale (UPDRS-III) at the study endpoint of 24 months by 7.3 points. More recently, we also reported our findings associated with physical function, a secondary outcome.15 Here, we examine the cognitive domain
and report the effect of mFC and PRET on cognitive outcomes related to attention and working memory. This article addresses the following questions at the 12-month and 24-month time points: Relative to baseline, does exercise improve cognitive function, and is one type of exercise modality better at improving cognitive function in mild-to-moderate PD? Because of the known benefits of exercise on cognitive performance,9-11 we hypothesized that exercise would improve cognitive function in mild-to-moderate PD.
Patients and Methods
Study Design and Participants
The PRET-PD trial was a prospective, parallel-group, single-center RCT between September 2007 and July 2011.13 Patients with idiopathic PD, confirmed by a movement disorders specialist,16 were self-referred or recruited from Rush University Medical Center (Chicago, IL). Patients were eligible if they were 50 to 67 years of age (the Physical Activity Readiness Questionnaire [PAR-Q],17 a screening tool used for exclusion, was only validated for use with persons younger than 69 years, the maximum age at study completion); on stable dopaminergic therapy; and able to walk for 6 minutes. Patients were ineligible if they had a neurological history other than PD; had significant arthritis; failed the PAR-Q;17 had a Mini–Mental State Examination score less than 23;18 were already exercising; or had deep brain stimulation surgery for PD. Patients were followed every 6 months for 24 months or until they withdrew from the study. Each participant provided written informed consent approved by the local institutional review boards.
Interventions
Details of the exercise intervention used in the PRET-PD trial have been published previously.13 In brief, the mFC was an exercise program recommended by the National Parkinson
EXERCISE IMPROVES COGNITION IN PARKINSON DISEASE: The PRET-PD Randomized Clinical Trial
Fabian J. David, PhD; Julie A. Robichaud, PT, PhD; Sue E. Leurgans, PhD; Cynthia Poon, PhD; Wendy M. Kohrt, PhD; Jennifer G. Goldman, MD, MS; Cynthia L. Comella, MD; David E. Vaillancourt, PhD; Daniel M. Corcos, PhD
Exercise Improves Cognition in Parkinson Disease 41

42 THE 2016 RUSH NEUROSCIENCE REVIEW
Foundation and focused on stretches, balance exercises, breathing, and nonprogressive strengthening (manual chapters 2 and 3).14 PRET was a weight-lifting program in which the load against which the muscle worked was systematically and progressively increased. The PRET program consisted of strengthening exercises that were directed at all the major muscle groups.19 The programs were identical in all aspects (duration of exercise, number of exercise sessions, and time with the personal trainer), except for the specific exercises. Patients participated in their respective interventions twice a week19 for 24 months. One-on-one exercise with a certified personal trainer was provided for both weekly exercise sessions during the first 6 months; the trainer-assisted sessions were reduced to once per week after 6 months. Patients in the mFC and PRET groups were instructed not to engage in additional exercise.
Study Procedures
All cognitive assessments were performed after 12-hour overnight withdrawal of dopaminergic medication20 by individuals trained in administering standardized cognitive assessments and blinded to group assignments at the clinical motor control laboratory at the University of Illinois at Chicago. Off-medication assessment was completed in the morning. The cognitive outcomes were one of many outcome domains tested; they were clinical status, the primary outcome, and bradykinesia and strength, tremor, physical function15 and gait, quality of life, and cognition, which were secondary outcomes. The order of testing was pseudorandomized between outcome domains and between cognitive outcomes. The off-medication testing session lasted for approximately 3 hours. It was followed by ingestion of antiparkinsonian medication, a break for lunch, confirmation of a clinical response to the medication, and then repetition of the entire testing procedure while on antiparkinsonian medication. In this article, we report findings related to the cognitive outcomes only while off medication for the following reasons: first, the effects of antiparkinsonian medication on cognitive outcomes are not well understood;21 second, antiparkinsonian medication could possibly mask the effects of exercise; and third, because on-medication testing was always conducted in the afternoon after off-medication testing in the morning, fatigue was a potential confound with respect to cognitive performance.
Cognitive Outcomes
The cognitive outcomes were the Digit Span Forwards and Backwards to assess working memory,22 which had a sum score that ranged from 0 to 30; the Stroop Color-Word Interference to measure selective attention and conflict resolution,23 which had a T score, a standardized normative metric, with a mean of 50 and a standard deviation (SD) of 10; and the Brief Test of Attention (BTA) to assess selective attention,24 which had a sum score that ranged from 0 to 20.
Follow-up
Patients in the mFC and PRET groups returned to the laboratory at 6, 12, 18, and 24 months for follow-up. The entire baseline assessment procedure was repeated at each follow-up visit.
Randomization and Blinding
The statistician matched the enrolled patients in pairs by sex and off-medication UPDRS-III scores,25 and randomly assigned one member of each pair to PRET and the other member to mFC using a random-length permuted block design.26
Randomization resulted in a parallel-group design with a 1:1 allocation ratio. Patients started exercising within 1 month of randomization. Research personnel involved in data collection were blinded to group assignment. The patients knew their treatment assignment but were unaware of the study hypothesis and were explicitly instructed not to discuss their exercise program with the raters.
Jennifer Goldman, MD, MS (right) is part of the multidisciplinary movement disorders care team at Rush.

Exercise Improves Cognition in Parkinson Disease 43
Table 1. Characteristics of Patients at Baselinea
Treatment groups
mFC PRET PRET vs mFC (95% CI) P Valueb
Demographic
Age, y 58.6 ± 5.6 59.0 ± 4.6 −0.4 (−2.6 to 3.4) 0.78c
Education, y 15.9 ± 2.7 16.8 ± 3.5 0.9 (−1.0 to 2.7) 0.37c
Sex, n (%) 1d
Male 14 (58.3) 14 (58.3)
Female 10 (41.7) 10 (41.7)
Ethnicity, n (%) 0.19d
Hispanic or Latino 5 (20.8) 1 (4.2)
Not Hispanic or Latino 19 (79.2) 23 (95.8)
Race, n (%) 0.49d
African American 0 (0) 2 (8.3)
Native American 0 (0) 0 (0)
White 24 (100) 22 (91.7)
Handedness, n (%) 1d
Right 22 (91.7) 23 (95.8)
Left 2 (8.3) 1 (4.2)
Clinical
Years since diagnosis 6.5 ± 4.7 6.5 ± 4.1 0.0 (−2.5 to 2.6) 0.97c
MMSE 29.1 ± 1.4 29.3 ± 1.1 −0.2 (−0.9 to 0.5) 0.56c
Most affected side, n (%) 0.5 (0.2 to 1.6) 0.37d
Right 17 (70.8) 13 (54.2)
Left 7 (29.2) 11 (45.8)
Motor status
Unified Parkinson Disease Rating Scale, part III, motor subscale score (range, 0-108) (off medication)
34.7 ± 11.5 34.5 ± 11.9 −0.2 (−7.0 to 6.6) 0.95c
Hoehn and Yahr Staging Scale (disability; range, 0-5; off medication)
2 (2, 2.5) 2 (2, 2.5) 0 (0 to 0)e 0.85f
Medication, n (%)
Dopamine precursors 19 (79) 17 (71) 0.51d
Dopamine agonists 16 (67) 17 (71) 0.76d
Adjuncts 12 (50) 10 (42) 0.56d
Cognitive outcomes, median (IQR)
Digit Span Forwards and Backwards Sum Score (range, 0-30; off medication)
17 (14.5, 19) 17 (15, 19.5) 0 (−2 to 2)e 0.84f
Stroop Color-Word Interference T Score (mean, 50; SD, 10; off medication)
47.5 (41, 53) 41 (33, 51) −3 (−11 to 4)e 0.41f
Brief Test of Attention Sum Score (range, 0-20; off medication)
16 (13, 18.5) 17 (13.5, 18) 0 (−2 to 2)e 0.75f
Abbreviations: CI, confidence interval; IQR, interquartile range; mFC, modified Fitness Counts; MMSE, Mini-Mental State Examination; PRET, Progressive Resistance Exercise Training.a Plus-minus values are mean ± 1 SD.b Representing significance of a test that was performed to determine if values were the same across the mFC and PRET groups.c P values calculated using t test.d P values calculated using chi-square test (expected cell count ≥ 5) or Fisher exact test (expected cell count <5). e Hodges-Lehman estimate of location shift. f P values calculated using Wilcoxon rank-sum test.

44 THE 2016 RUSH NEUROSCIENCE REVIEW
Statistical Analysis
All raw scores were converted to z scores. For the Digit Span22 and the Stroop,23 published norms were used to calculate z scores. For the BTA, the pooled baseline mean and SD was used to calculate z scores. To reduce type I errors, we used only the 12- and 24-month change from baseline z scores. The distributional assumptions for parametric testing were not met; therefore, nonparametric methods were used. The Wilcoxon rank-sum test was used to analyze the differences between the mFC and PRET groups at 12 and 24 months. The Wilcoxon signed-rank test was used to analyze change from baseline at 12 and 24 months. We also calculated correlations of changes in cognitive outcomes with changes in clinical and functional outcomes published previously. In addition, a sensitivity analysis using the last available observation carried forward (LOCF) was performed to evaluate the impact of missing data. Since these outcomes were not used to power the original RCT, we did not adjust the significance level for multiple outcomes. All statistical tests were 2-tailed, with P<.05 for statistical significance.
Results
Of the 51 patients enrolled, 46 patients (mFC, n=23; PRET, n=23) completed the 12-month follow-up and 38 patients (mFC, n=18; PRET, n=20) completed the 24-month follow-up. At baseline, the mFC and PRET groups did not differ on demographic, clinical, and cognitive outcomes (Table 1).
Difference Between mFC and PRET Groups at 12 and 24 Months
There were no differences between the mFC and PRET groups at 12 and 24 months on any of the cognitive outcomes measured in this study (Table 2).
Change From Baseline: The Effect in Each Intervention Arm at 12 and 24 Months
Digit Span Forwards and Backwards Sum Score
The mFC and PRET groups improved their Digit Span scores at 12 (mFC: estimated difference, 0.3; interquartile range [IQR], 0,
0.7; P=.04; PRET: 0.7; IQR, 0.3, 1; P < .01; Table 3; Figure 1A) and at 24 months (mFC: 0.7; IQR, 0.3, 1.7; P < .01; PRET: 0.5; IQR, 0.2, 0.8; P < .01; Table 3; Figure 1A).
Stroop Color-Word Interference T-Score
The mFC group improved performance on the Stroop at 12 months (mFC: 0.3; IQR, 0, 0.6; P=.04; Table 3; Figure 1B), whereas the PRET group presented with no change (0.2; IQR, −0.1, 0.8; P=.08; Table 3; Figure 1B). At 24 months, the mFC and PRET groups improved their Stroop scores (mFC: 0.3; IQR, 0.1, 0.5; P=.03; PRET: 0.2; IQR, −0.1, 0.6; P=.048; Table 3; Figure 1B).
Brief Test of Attention Sum Score
At 12 months, the mFC (0.3; IQR, −0.3, 1; P=.07; Table 3; Figure 1C) and the PRET (0; IQR, −0.3, 0.5; P=.11; Table 3; Figure 1C) groups did not change on the BTA. At 24 months, the mFC group remained unchanged, whereas the PRET group improved on the BTA (mFC: 0.1; IQR, −0.3, 0.8; P=.50; PRET: 0.3; IQR, 0, 0.8; P=.048; Table 3; Figure 1C).
Figure 1. Box plots illustrate the off-medication change from baseline z scores in the modified Fitness Counts (mFC) and Progressive Resistance Exercise Training (PRET) for (A) the Digit Span Forwards and Backwards, (B) the Stroop Color-Word Interference, and (C) the Brief Test of Attention at 12, and 24 months. Positive z scores indicate improvement in the Digit Span Forwards and Backwards sum score, the Stroop Color-Word Interference T score, and the Brief Test of Attention sum score.
A B CD
igit
Sp
an
Stro
op
Co
lor-
Wo
rd
Inte
rfer
ence
Bri
ef T
est
o
f A
tten
tio
n
Month Month Month
3
2
1
0
-1
-2
-3
3
2
1
0
-1
-2
-3
3
2
1
0
-1
-2
-3
12 24 12 24 12 24
mFCPRET
Outcome PRET vs mFC (95% CI)a P Value
Digit Span Forwards and Backwards (z score)
12 mo −0.3 (−0.7 to 0.3) 0.32
24 mo 0.3 (−0.3 to 1) 0.27
Stroop Color-Word Interference (z score)
12 mo 0.1 (−0.5 to 0.5) 0.81
24 mo 0 (−0.4 to 0.5) 0.77
Brief Test of Attention (z score)
12 mo 0 (−0.5 to 0.5) 0.77
24 mo 0 (−0.8 to 0.5) 0.83
Table 2. Difference Between Groups in Change From Baseline in Cognitive Outcomes at 12 and 24 Months
Abbreviations: CI, confidence interval; mFC, modified Fitness Counts; PRET, Progressive Resistance Exercise Training.a Hodges-Lehman estimate of location shift and P values calculated using Wilcoxon rank-sum test.

Exercise Improves Cognition in Parkinson Disease 45
Associations of Change in UPDRS-III, Function, and Cognition
There were no significant relationships between change in the cognitive outcomes and the UPDRS-III. With respect to the relationships between change in cognitive outcomes and change in physical function outcomes, only the relationship between the Digit Span and walking speed was significant (rho=0.46, P=.004).
In summary, there are 2 findings of importance at the study endpoint. First, there are no differences between mFC and PRET for all cognitive outcomes measured in this study. Second, the PRET and mFC groups presented with substantial within-group improvement in cognitive performance; that is, at 24 months, relative to baseline, the PRET group improved on all three of the cognitive outcomes (Digit Span, Stroop, and BTA) measured in this study, while the mFC group improved on two of the three cognitive outcomes (Digit Span and Stroop) measured in this study. These results did not change with LOCF sensitivity analyses (Supporting Tables e-1 and e-2 are available in the published version online).
Adverse Events
Adverse events related to this trial have been previously published.13 Of note, there were no neurological or cognitive adverse events reported.
Discussion
This clinical trial demonstrated that 24 months of exercise, twice a week, may be effective in improving attention and working memory in patients with mild-to-moderate PD without
dementia when evaluated off medication. Relative to baseline, mFC and PRET improved performance on the Digit Span and Stroop, whereas PRET also improved performance on the BTA. This study is the first RCT to examine the effects of 24 months of exercise on cognitive functions in patients with mild-to-moderate PD. The findings from this clinical trial extend the previously known cognitive benefits of exercise in Alzheimer’s disease and in normal aging to PD. In addition, improvements in Digit Span scores were associated with improvements in walking speed. Given the recently published finding that physical activity reduces major mobility disability in older adults at risk for disability,27 taken together with our recently published findings that exercise improves motor signs of PD13 and physical function,15 and our current finding that exercise might improve cognitive function, the evidence for the benefits of exercise across domains is accumulating.
This clinical trial demonstrates the likely beneficial effects of 24 months of structured exercise on attention and working memory, which are cognitive domains that are frequently impaired in patients with PD. This finding is especially important for the Stroop because impaired performance on the Stroop has been shown to be associated with greater risk of subsequent dementia in patients with PD without dementia.28,29 Consequently, the finding that structured exercise might improve Stroop scores might indicate that exercise may reduce the risk of subsequent dementia in patients with PD. This possibility is clinically relevant because the cumulative incidence estimates from longitudinal studies indicate that up to 78% of patients with PD will develop dementia.6
PRET was significantly better than mFC at improving motor signs of PD,13 and PRET and mFC were efficacious at improving
Table 3. Cognitive Outcomes at Baseline, 12 Months, and 24 Months, and Change From Baseline at 12 and 24 Months
Abbreviations: IQR, interquartile range; mFC, modified Fitness Counts; PRET, Progressive Resistance Exercise Training.a P values calculated using the Wilcoxon signed-rank test.b Positive change score from baseline is indicative of improvement.
Outcome Z Score at Visit: Median (IQR) Change From Baseline: Median (IQR), P Valuea
mFC PRET mFC PRET
Digit Span Forwards and Backwardsb
Baseline 0 (−0.3, 0.6) 0.3 (−0.3, 0.8)
12 mo 0.3 (−0.3, 1.3) 1 (0, 1.7) 0.3 (0, 0.7), P=0.04 0.7 (0.3, 1), P<0.01
24 mo 1 (0, 2) 1 (0.2, 1.3) 0.7 (0.3, 1.7), P<0.01 0.5 (0.2, 0.8), P<0.01
Stroop Color-Word Interferenceb
Baseline −0.3 (−0.9, 0.3) −0.9 (−1.7, 0.1)
12 mo −0.1 (−0.8, 0.8) −0.2 (−1.2, 0.4) 0.3 (0, 0.6), P=0.04 0.2 (−0.1, 0.8), P=0.08
24 mo −0.1 (−0.8, 0.8) −0.1 (−1.7, 0.4) 0.3 (0.1, 0.5), P=0.03 0.2 (−0.1, 0.6), P=0.048
Brief Test of Attentionb
Baseline 0.1 (−0.7, 0.8) 0.4 (−0.5, 0.7)
12 mo 0.4 (−0.4, 1.2) 0.4 (−0.4, 0.9) 0.3 (−0.3, 1), P=0.07 0 (−0.3, 0.5), P=0.11
24 mo −0.1 (−0.4, 0.9) 0.4 (0.1, 1.2) 0.1 (−0.3, 0.8), P=0.50 0.3 (0, 0.8), P=0.048

46 THE 2016 RUSH NEUROSCIENCE REVIEW
physical function15 and cognitive outcomes in patients with PD, with neither being better than the other. One possible explanation is that because the mFC protocol included nonprogressive resistance exercises, it could be considered a low-dose resistance exercise regimen, whereas the PRET protocol could be considered a high-dose resistance exercise regimen. It has been shown that both low- and high-dose PRET have similar beneficial effects on cognitive outcomes.30 It could be that there is a threshold for a treatment effect on cognitive function. Our findings suggest that PRET and mFC exceeded a threshold for an effect on cognitive function. Further research is needed to understand the mechanisms by which exercise improves cognition and whether different doses of exercise and different types of exercise have the same or different effects on cognition.
In general, repeated administrations of cognitive assessments in healthy individuals are known to have practice effects, and these practice effects are affected by factors such as age, task difficulty,31,32 and IQ.31 We recognize that the improvements observed in this study could have been driven by practice effects. However, there are two arguments that favor the idea that the improvements in cognitive outcomes observed in this study were, at least partially, attributable to the effect of exercise and not simply an effect of practice. First, cognitive function has been shown to decline with increasing age, and the magnitude of this decline is approximated by the improvement in cognitive function owing to repeated testing.33 Second, in patients with PD, the neurodegenerative disease process augments the cognitive decline that accompanies the aging process. In fact, earlier work has shown that when cognitive tests are administered approximately 36 months apart, more cognitive decline occurs in patients with PD than in age-matched controls.34 Consequently, combining the effects of aging and the neurodegenerative disease process, one would expect cognitive function to decline or, at best, remain unchanged over time in patients with PD. However, we observed improvements in performance in the mFC and PRET groups in cognitive outcomes at 12 and 24 months. This finding might be suggestive of an effect of exercise beyond that of practice alone.
Another factor that is a potential confound is the increased social and cognitive engagement by virtue of mere participation in the PRET-PD study. The very fact that these patients went out of their houses to the gyms provides for greater opportunities for social and cognitive engagement with others, including their family, personal trainers, and the study personnel. The extent to which this increased social and cognitive engagement confounds our findings is unknown. This is a limitation of this study. In addition, because the study included a relatively younger group of patients with mild-to-moderate disease and an above-average level of education, the lack of generalizability is a limitation. Given these limitations and the fact that we did not adjust our alpha level for multiple outcomes, our findings should be interpreted with caution. Despite these limitations, the PRET-PD trial is similar to a phase II study that supports the concept of exercise as an adjunct therapy for PD and
demonstrates feasibility,35 thereby providing a rationale for larger-scale, multicenter trials that could extend our findings across geographical locations, clinical practices, and a wider group of patients with PD.
In conclusion, this clinical trial found that 24 months of PRET or mFC exercise may improve cognitive outcomes in patients with mild-to-moderate PD while off medication. Our findings suggest that patients with mild-to-moderate PD without dementia might be able to improve cognitive performance by engaging in either mFC or PRET for two 60- to 90-minute sessions a week.
Supporting Data
Additional supporting information may be found in the online version of this article at the publisher’s website.
Funding
Supported by the National Institutes of Health (NIH; R01-NS28127-12 to 16, R01 NS52318, and R01 NS75012). The sponsors were not involved in the design, conduct, collection, management, analysis, and/or interpretation of the study results and preparation, review, or approval of the manuscript. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the NIH (Clinical Trial Registration: clinicaltrials. gov, NCT00591344).
Conflict of Interest
Nothing to report. Full financial disclosures and author roles may be found in the online version of this article.

References1. Brown RG, Marsden CD. Cognitive function in Parkinson’s disease: from description to theory. Trends Neurosci. 1990;13(1):21-29.
2. Cooper JA, Sagar HJ, Jordan N, Harvey NS, Sullivan EV. Cognitive impairment in early, untreated Parkinson’s disease and its relationship to motor disability. Brain. 1991;114(pt 5):2095-2122.
3. Owen AM. Cognitive dysfunction in Parkinson’s disease: the role of frontostriatal circuitry. Neuroscientist. 2004;10(6):525-537.
4. Kudlicka A, Clare L, Hindle JV. Executive functions in Parkinson’s disease: systematic review and meta-analysis. Mov Disord. 2011;26(13):2305-2315.
5. Owen AM, James M, Leigh PN, et al. Fronto-striatal cognitive deficits at different stages of Parkinson’s disease. Brain. 1992;115(pt 6):1727-1751.
6. Aarsland D, Andersen K, Larsen JP, Lolk A, Kragh-Sorensen P. Prevalence and characteristics of dementia in Parkinson disease: an 8-year prospective study. Arch Neurol. 2003;60(3):387-392.
7. Goldman JG, Litvan I. Mild cognitive impairment in Parkinson’s disease. Minerva Med. 2011;102(6):441-459.
8. Bullain SS, Corrada MM, Shah BA, Mozaffar FH, Panzenboeck M, Kawas CH. Poor physical performance and dementia in the oldest old: the 90+ study. JAMA Neurol. 2013;70(1):107-113.
9. Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci. 2003;14(2):125-130.
10. Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil. 2004;85(10):1694-1704.
11. Uc EY, Doerschug KC, Magnotta V, et al. Phase I/II randomized trial of aerobic exercise in Parkinson disease in a community setting. Neurology. 2014;83(5):413-425.
12. Hindle JV, Petrelli A, Clare L, Kalbe E. Nonpharmacological enhancement of cognitive function in Parkinson’s disease: a systematic review. Mov Disord. 2013;28(8):1034-1049.
13. Corcos DM, Robichaud JA, David FJ, et al. A two-year randomized controlled trial of progressive resistance exercise for Parkinson’s disease. Mov Disord. 2013;28(9):1230-1240.
14. Cianci H. Parkinson Disease: Fitness Counts. 3rd ed. Miami, FL: National Parkinson Foundation; 2006.
15. Prodoehl J, Rafferty MR, David FJ, et al. Two-year exercise program improves physical function in Parkinson’s disease: the PRET-PD randomized clinical trial. Neurorehabil Neural Repair. 2015;29(2):112-122.
16. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55(3):181-184.
17. Canadian Society for Exercise Physiology. Physical activity readiness questionnaire—PAR-Q (revised 2002). http://uwfitness.uwaterloo.ca/PDF/par-q.pdf. Updated 2002. Accessed May 4, 2013.
18. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
19. Feigenbaum MS, Pollock ML. Prescription of resistance training for health and disease. Med Sci Sports Exerc. 1999;31(1):38-45.
20. Langston JW, Widner H, Goetz CG, et al. Core assessment program for intracerebral transplantations (CAPIT). Mov Disord. 1992;7(1):2-13.
21. Cools R, Barker RA, Sahakian BJ, Robbins TW. Enhanced or impaired cognitive function in Parkinson’s disease as a function of dopaminergic medication and task demands. Cereb Cortex. 2001;11(12):1136-1143.
22. Wechsler D. Wechsler Adult Intelligence Scale: Administration and Scoring Manual. 3rd ed. San Antonio, TX: Psychological Corporation; 1997.
23. Golden CJ, Freshwater SM. The Stroop Color and Word Test: A Manual for Clinical and Experimental Uses. Chicago, IL: Stoelting; 2002.
24. Schretlen D. Brief Test of Attention: Professional Manual. Lutz, FL: Psychological Assessment Resources, Inc; 1997.
25. Fahn S, Elton RL, UPDRS Program Members. Unified parkinson’s disease rating scale. In: Fahn S, Marsden CD, Goldstein M, Calne DB, eds. Recent Developments in Parkinson’s Disease. Vol 2. Florham Park, NJ: Macmillan Healthcare Information; 1987:153-163.
26. Friedman LM, Furberg CD, DeMets DL. Fundamentals of Clinical Trials. New York, NY: Springer-Verlag; 1998.
27. Pahor M, Guralnik JM, Ambrosius WT, et al. Effect of structured physical activity on prevention of major mobility disability in older adults: the LIFE study randomized clinical trial. JAMA. 2014;311(23):2387-2396.
28. Mahieux F, Fenelon G, Flahault A, Manifacier MJ, Michelet D, Boller F. Neuropsychological prediction of dementia in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 1998;64(2):178-183.
29. Janvin CC, Aarsland D, Larsen JP. Cognitive predictors of dementia in parkinson’s disease: a community-based, 4-year longitudinal study. J Geriatr Psychiatry Neurol. 2005;18(3):149-154.
30. Liu-Ambrose T, Nagamatsu LS, Graf P, Beattie BL, Ashe MC, Handy TC. Resistance training and executive functions: a 12-month randomized controlled trial. Arch Intern Med. 2010;170(2):170-178.
31. Rabbitt P. Crystal quest: an examination of the concepts of ‘fluid’ and ‘crystallised’ intelligence as explanations for cognitive changes in old age. In: Baddeley AD, Weiskrantz LS, eds. Attention, Selection, Awareness and Control. Oxford, England: Oxford University Press; 1993:197-231.
32. Lowe C, Rabbitt P. Test/re-test reliability of the CANTAB and ISPOCD neuropsychological batteries: theoretical and practical issues. Cambridge Neuropsychological Test Automated Battery. International Study of Post-Operative Cognitive Dysfunction. Neuropsychologia. 1998;36(9):915-923.
33. Rabbitt P, Diggle P, Smith D, Holland F, Mc Innes L. Identifying and separating the effects of practice and of cognitive ageing during a large longitudinal study of elderly community residents. Neuropsychologia. 2001;39(5):532-543.
34. Muslimovic D, Post B, Speelman JD, De Haan RJ, Schmand B. Cognitive decline in Parkinson’s disease: a prospective longitudinal study. J Int Neuropsychol Soc. 2009;15(3):426-437.
35. Rascol O. Physical exercise in Parkinson disease: moving toward more robust evidence? Mov Disord. 2013;28(9):1173-1175. ◆
Exercise Improves Cognition in Parkinson Disease 47

48 THE 2016 RUSH NEUROSCIENCE REVIEW
0
200
400
600
800
1000
1200
894 1009 834 1091 997
2011 2012 2013 2014 2015
Neurological surgery volume of major cases by area, fiscal year 2015
Total:2 974
Surgeries
Volume and Quality Data
0
500
1000
1500
2000
2500
3000
2186 2398 2589 2528 2717
2011 2012 2013 2014 2015
Num
ber
of d
isch
arge
s
Out
pati
ent
visi
ts
Year Year
Neurology volumes*, fiscal years 2011-2015 Neurology outpatient visits, fiscal years 2011-2015
Rush had the highest volume of general neurology discharges in the Chicago region for fiscal years 2014 and 2015.
*Includes neuro-oncology discharges
0
5000
10000
15000
20000
25000
30000
22 736 25 162 26 937 28 986 28 709
2011 2012 2013 2014 2015
Volumes, neurology and neurological surgery
1 000
2 000
3 000
4 000
5 000
6 000
2011 2012 2013 2014 2015
5068
3638
1599
3222
4375
2258
43453666
5086
3420
Out
pati
ent
visi
ts
Case
s of
vid
eo E
EG
mon
itor
ing
for
seiz
ure
clas
sific
atio
n or
loca
lizat
ion
Year Year
Neurological surgery outpatient visits, fiscal years 2011-2015
Volume of patients monitored for epilepsy, calendar years 2011-2015
*Includes all nonspine procedures
Spine Brain*
Rush had the highest volume of neurosurgical discharges in the Chicago region for fiscal years 2011-2015.
Brain tumor 314 (10.56%)
Cerebrospinal fluid treatments 203 (6.83%)
Epilepsy and movement disorders 78 (2.62%)
Functional 165 (5.55%)
Neuroendovascular-diagnostic 460 (15.47%)
Neuroendovascular-interventional 425 (14.29%)
Open cerebrovascular 61 (2.05%)
Other 117 (3.93%)
Spine and nerves 1047 (35.21%)
Trauma 104 (3.50%)

Volume and Quality Data 49
0.0
0.2
0.4
0.6
0.8
1.0
0.87 0.75 0.77 0.95 0.98
2011 2012 2013 2014 20150.0
0.2
0.4
0.6
0.8
1.0
0.56 0.71 0.60 0.79 0.63
2011 2012 2013 2014 2015
Stroke case volumes, fiscal year 2015
Total:1131Cases
Intracerebral hemorrhage 273 (24.14%)
Ischemic stroke 596 (52.70%)
Subarachnoid hemorrhage 158 (13.97%)
Transient ischemic attack (<24 hours) 104 (9.20%)
Year Year
Mor
talit
y in
dex
Mor
talit
y in
dex
Neurological surgery mortality o/e, fiscal years 2011-2015
Source: University HealthSystem Consortium clinical database Source: University HealthSystem Consortium clinical database
Mortality, neurology and neurological surgery
Neurology mortality o/e, fiscal years 2011-2015
Sources: Get With the Guidelines and internal data1Includes all comprehensive stroke centers participating in Get With the Guidelines stroke data registry2Administered at Rush and outside hospitals combined3Includes all U.S. hospitals participating in Get With the Guidelines stroke data registry
Median times to endovascular recanalization treatment at Rush
Stroke IV tPA rate, fiscal year 2015
Stroke inpatient mortality, fiscal year 2015
0
5
10
15
20
25
0
5
10
15
20
25
IV tPA rate for ischemic stroke2
Ischemic stroke
Intracerebral hemorrhage
Subarachnoid hemorrhage
RushU.S. Hospitals3
RushU.S. Hospitals3
RushComparison1
22.22% 16.88% 5.87% 14.56%
Groin torecanalization time
Door to groin time
17.58%5.33% 23.33% 17.17%0
20
40
60
80
100
30 min.
102 min.
32 min.
Unavailable
Quality indicators, stroke

Abner EL, Schmitt FA, Nelson PT, Lou W, Wan L, Gauriglia R, Dodge HH, Woltjer RL, Yu L, Bennett DA, Schneider JA, Chen R, Masaki K, Katz MJ, Lipton RB, Dickson DW, Lim KO, Hemmy LS, Cairns NJ, Grant E, Tyas SL, Xiong C, Fardo DW, Kryscio RJ. The statistical modeling of aging and risk of transition project: data collection and harmonization across 11 longitudinal cohort studies of aging, cognition, and dementia. Obs Stud. 2015;1(2015):56-73.
Aggarwal NT, Everson-Rose SA, Evans DA. Social determinants, race, and brain health outcomes: findings from the Chicago Health and Aging Project. Curr Alzheimer Res. 2015;12(7):622-631.
Aggarwal NT, Shah RC, Bennett DA. Alzheimer’s disease: unique markers for diagnosis & new treatment modalities. Indian J Med Res. 2015;142(4):369-382.
Albers MW, Gilmore GC, Kaye J, Murphy C, Wingfield A, Bennett DA, Boxer AL, Buchman AS, Cruickshanks KJ, Devanand DP, Duffy CJ, Gall CM, Gates GA, Granholm AC, Hensch T, Holtzer R, Hyman BT, Lin FR, McKee AC, Morris JC, Petersen RC, Silbert LC, Struble RG, Trojanowski JQ, Verghese J, Wilson DA, Xu S, Zhang LI. At the interface of sensory and motor dysfunctions and Alzheimer’s disease. Alzheimers Dement. 2015;11(1):70-98.
Alperin N, Loftus JR, Oliu CJ, Bagci AM, Lee SH, Ertl-Wagner B, Sekula R, Lichtor T, Green BA. Imaging-based features of headaches in Chiari malformation type I. Neurosurgery. 2015;77(1):96-103, discussion 103.
Amin AJ, Lewis SL. Clinical reasoning: a 35-year-old man with 2 episodes of meningoencephalitis associated with flu-like illnesses. Neurology. 2015;84(9):e60-e64.
Arvanitakis Z, Brey RL, Rand JH, Schneider JA, Capuano AW, Yu L, Leurgans SE, Bennett DA, Levine SR. Relation of antiphospholipid antibodies to postmortem brain infarcts in older people. Circulation. 2015;131(2):182-189.
Asher R, Mason AE, Weiner J, Fessler RG. The relationship between preoperative general mental health and postoperative quality of life in minimally invasive lumbar spine surgery. Neurosurgery. 2015;76(6):672-679.
Bailey DB Jr, Wheeler A, Berry-Kravis E, Hagerman R, Tassone F, Powell CM, Roche M, Gane LW, Sideris J. Maternal consequences of the detection of fragile X carriers in newborn screening. Pediatrics. 2015;136(2):e433-e440.
Barclay SF, Rand CM, Borch LA, Nguyen L, Gray PA, Gibson WT, Wilson RJ, Gordon PM, Aung Z, Berry-Kravis EM, Ize-Ludlow D, Weese-Mayer DE, Bech-Hansen NT. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation (ROHHAD): exome sequencing of trios, monozygotic twins and tumours. Orphanet J Rare Dis. 2015;10:103.
Barnes LL, Bennett DA. Dementia: cognitive resilience in APOE*ε4 carriers—is race important? Nat Rev Neurol. 2015;11(4):190-191.
Barnes LL, Capuano AW, Aiello AE, Turner AD, Yolken RH, Torrey EF, Bennett DA. Cytomegalovirus infection and risk of Alzheimer disease in older black and white individuals. J Infect Dis. 2015;211(2):230-237.
Barnes LL, Leurgans S, Aggarwal NT, Shah RC, Arvanitakis Z, James BD, Buchman AS, Bennett DA, Schneider JA. Mixed pathology is more likely in black than white decedents with Alzheimer dementia. Neurology. 2015;85(6):528-534.
Barral S, Vardarajan BN, Reyes-Dumeyer D, Faber KM, Bird TD, Tsuang D, Bennett DA, Rosenberg R, Boeve BF, Graff-Radford NR, Goate AM, Farlow M, Lantigua R, Medrano MZ, Wang X, Kamboh MI, Barmada MM, Schaid DJ, Foroud TM, Weamer EA, Ottman R, Sweet RA, Mayeux R; NIA-LOAD/NCRAD Family Study Group. Genetic variants associated with susceptibility to psychosis in late-onset Alzheimer’s disease families. Neurobiol Aging. 2015;36(11):3116.e9-3116.e16.
Bartus RT, Kordower JH, Johnson EM Jr, Brown L, Kruegel BR, Chu Y, Baumann TL, Lang AE, Olanow CW, Herzog CD. Post-mortem assessment of the short and long-term effects of the trophic factor neurturin in patients with α-synucleinopathies. Neurobiol Dis. 2015;78:162-171.
Bennett DA, Yu L, Yang J, Srivastava GP, Aubin C, De Jager PL. Epigenomics of Alzheimer’s disease. Transl Res. 015;165(1):200-220.
Berg D, Postuma RB, Adler CH, Bloem BR, Chan P, Dubois B, Gasser T, Goetz CG, Halliday G, Joseph L, Lang AE, Liepelt-Scarfone I, Litvan I, Marek K, Obeso J, Oertel W, Olanow CW, Poewe W, Stern M, Deuschl G. MDS research criteria for prodromal Parkinson’s disease. Mov Disord. 2015;30(12):1600-1611.
Bermeo-Ovalle AC, Kennedy JD, Schuele SU. Cardiac and autonomic mechanisms contributing to SUDEP. J Clin Neurophysiol. 2015;32(1):21-29.
Berry-Kravis E, Levin R, Shah H, Mathur S, Darnell JC, Ouyang B. Cholesterol levels in fragile X syndrome. Am J Med Genet A. 2015;167A(2):379-384.
Bhalla D, Aziz H, Bergen D, Birbeck GL, Carpio A, Cavalheiro E, Chivorakoun P, Helen Cross J, Houinato D, Newton CR, Odermatt P, Ravat S, Schmutzhard E, Preux PM. Undue regulatory control on phenobarbital—an important yet overlooked reason for the epilepsy treatment gap [published correction appears in Epilepsia. 2015;56(6):985]. Epilepsia. 2015;56(4):659-662.
Boland TA, Lee VH, Bleck TP. Stress-induced cardiomyopathy. Crit Care Med. 2015;43(3):686-693.
* This is a partial list of published works of the faculty from the neurosciences at Rush University Medical Center (indicated in bold). The department gratefully acknowledges the co-authorship of students, nurses, practitioners, therapists, residents, fellows, and other colleagues at Rush.
Select Publications (2015)
Departments of Neurological Sciences and Neurological Surgery*
50 THE 2016 RUSH NEUROSCIENCE REVIEW

Bot M, van den Munckhof P, Bakay R, Sierens D, Stebbins G, Verhagen Metman L. Analysis of stereotactic accuracy in patients undergoing deep brain stimulation using Nexframe and the Leksell frame. Stereotact Funct Neurosurg. 2015;93(5):316-325.
Boyle PA, Yu L, Nag S, Leurgans S, Wilson RS, Bennett DA, Schneider JA. Cerebral amyloid angiopathy and cognitive outcomes in community-based older persons. Neurology. 2015;85(22):1930-1936.
Broer L, Buchman AS, Deelen J, Evans DS, Faul JD, Lunetta KL, Sebastiani P, Smith JA, Smith AV, Tanaka T, Yu L, Arnold AM, Aspelund T, Benjamin EJ, De Jager PL, Eirkisdottir G, Evans DA, Garcia ME, Hofman A, Kaplan RC, Kardia SL, Kiel DP, Oostra BA, Orwoll ES, Parimi N, Psaty BM, Rivadeneira F, Rotter JI, Seshadri S, Singleton A, Tiemeier H, Uitterlinden AG, Zhao W, Bandinelli S, Bennett DA, Ferrucci L, Gudnason V, Harris TB, Karasik D, Launer LJ, Perls TT, Slagboom PE, Tranah GJ, Weir DR, Newman AB, van Duijn CM, Murabito JM. GWAS of longevity in CHARGE consortium confirms APOE and FOXO3 candidacy. J Gerontol A Biol Sci Med Sci. 2015;70(1):110-118.
Buchman AS, Wilson RS, Leurgans SE, Bennett DA, Barnes LL. Change in motor function and adverse health outcomes in older African-Americans. Exp Gerontol. 2015;70:71-77.
Buchman AS, Yu L, Wilson RS, Dawe RJ, VanderHorst V, Schneider JA, Bennett DA. Post-mortem brain pathology is related to declining respiratory function in community-dwelling older adults. Front Aging Neurosci. 2015;7:197.
Burns JM, Bennett DA. Parsing the heterogeneity of mild cognitive impairment: lumpers and splitters. Neurology. 2015;85(19):1646-1647.
Burt RK, Balabanov R, Han X, Sharrack B, Morgan A, Quigley K, Yaung K, Helenowski IB, Jovanovic B, Spahovic D, Arnautovic I, Lee DC, Benefield BC, Futterer S, Oliveira MC, Burman J. Association of nonmyeloablative hematopoietic stem cell transplantation with neurological disability in patients with relapsing-remitting multiple sclerosis. JAMA. 2015;313(3):275-284.
Busl KM. Patient management problem. Continuum (Minneap Minn). 2015;21(5):1503-1523.
Busl KM, Bleck TP. Neurogenic pulmonary edema. Crit Care Med. 2015;43(8):1710-1715.
Busl KM, Ouyang B, Boland TA, Pollandt S, Temes RE. Prolonged mechanical ventilation is associated with pulmonary complications, increased length of stay, and unfavorable discharge destination among patients with subdural hematoma. J Neurosurg Anesthesiol. 2015;27(1):31-36.
Cardoso AC, Fontes RB, Tan LA, Rhoton AL Jr, Roh SW, Fessler RG. Biomechanical effects of the transcondylar approach on the craniovertebral junction. Clin Anat. 2015;28(5):683-689.
Cedarbaum JM, Stephenson D, Rudick R, Carrillo MC, Stebbins G, Kerr D, Heemskerk J, Galpern WR, Kaufmann P, Cella D, Isaac M, Walton MK. Commonalities and challenges in the development of clinical trial measures in neurology [published correction appears in Neurotherapeutics. 2015;12(1):285]. Neurotherapeutics. 2015;12(1):151-169.
Chan G, White CC, Winn PA, Cimpean M, Replogle JM, Glick LR, Cuerdon NE, Ryan KJ, Johnson KA, Schneider JA, Bennett DA, Chibnik LB, Sperling RA, Bradshaw EM, De Jager PL. CD33 modulates TREM2: convergence of Alzheimer loci. Nat Neurosci. 2015;18(11):1556-1558.
Chauhan G, Adams HH, Bis JC, Weinstein G, Yu L, Töglhofer AM, Smith AV, van der Lee SJ, Gottesman RF, Thomson R, Wang J, Yang Q, Niessen WJ, Lopez OL, Becker JT, Phan TG, Beare RJ, Arfanakis K, Fleischman D, Vernooij MW, Mazoyer B, Schmidt H, Srikanth V, Knopman DS, Jack CR Jr, Amouyel P, Hofman A, DeCarli C, Tzourio C, van Duijn CM, Bennett DA, Schmidt R, Longstreth WT Jr, Mosley TH, Fornage M, Launer LJ, Seshadri S, Ikram MA, Debette S. Association of Alzheimer’s disease GWAS loci with MRI markers of brain aging. Neurobiol Aging. 2015;36(4):1765.e7-16.
Chen M, Conners J. Blank space [published correction appears in J Neurointerv Surg. 2015;7(7):548]. J Neurointerv Surg. 2015;7(6):391-392.
Cherian L, Conners J, Cutting S, Lee VH, Song S. Periprocedural risk of stroke is elevated in patients with end-stage renal disease on hemodialysis. Cerebrovasc Dis Extra. 2015;5(3):91-94.
Cherian L, Cutting S, Song S. Intra-arterial thrombectomy: does invasive treatment lead to better outcomes than intravenous thrombolysis alone? Curr Cardiol Rep. 2015;17(10):82.
Chesnut RM, Bleck TP, Citerio G, Classen J, Cooper DJ, Coplin WM, Diringer MN, Grände PO, Hemphill JC III, Hutchinson PJ, Le Roux P, Mayer SA, Menon DK, Myburgh JA, Okonkwo DO, Robertson CS, Sahuquillo J, Stocchetti N, Sung G, Temkin N, Vespa PM, Videtta W, Yonas H. A consensus-based interpretation of the benchmark evidence from South American trials: treatment of intracranial pressure trial. J Neurotrauma. 2015;32(22):1722-1724.
Chibnik LB, Yu L, Eaton ML, Srivastava G, Schneider JA, Kellis M, Bennett DA, De Jager PL. Alzheimer’s loci: epigenetic associations and interaction with genetic factors. Ann Clin Transl Neurol. 2015;2(6):636-647.
Choi M, Thoma M, Tolekidis G, Byrne RW, Diaz AZ. Successful delivery of adjuvant external beam radiotherapy for ependymoma in a patient with Ondine’s curse. Med Dosim. 2015 Winter;40(4):366-371.
Chu Y, Kordower JH. The prion hypothesis of Parkinson’s disease. Curr Neurol Neurosci Rep. 2015;15(5):28.
Clarke PJ, Weuve J, Barnes L, Evans DA, Mendes de Leon CF. Cognitive decline and the neighborhood environment. Ann Epidemiol. 2015;25(11):849-854.
Comella C, Bhatia K. An international survey of patients with cervical dystonia. J Neurol. 2015;262(4):837-848.
Contopoulos-Ioannidis D, Wheeler KM, Ramirez R, Press C, Mui E, Zhou Y, Van Tubbergen C, Prasad S, Maldonado Y, Withers S, Boyer KM, Noble AG, Rabiah P, Swisher CN, Heydemann P, Wroblewski K, Karrison T, Grigg ME, Montoya JG, McLeod R. Clustering of Toxoplasma gondii infections within families of congenitally infected infants. Clin Infect Dis. 2015;61(12):1815-1824.
Select Publications (2015) 51

Corbett GT, Gonzalez FJ, Pahan K. Activation of peroxisome proliferator-activated receptor α stimulates ADAM10-mediated proteolysis of APP. Proc Natl Acad Sci U S A. 2015;112(27):8445-8450.
Corbett GT, Kordower JH. The native form of α-synuclein: monomer, tetramer, or a combination in equilibrium. Mov Disord. 2015;30(14):1870.
Cothran FA, Farran CJ, Barnes LL, Whall AL, Redman RW, Struble LM, Dunkle RE, Fogg L. Demographic and socioenvironmental characteristics of black and white community-dwelling caregivers and care recipients’ behavioral and psychological symptoms of dementia. Res Gerontol Nurs. 2015;8(4):179-187.
David FJ, Robichaud JA, Leurgans SE, Poon C, Kohrt WM, Goldman JG, Comella CL, Vaillancourt DE, Corcos DM. Exercise improves cognition in Parkinson’s disease: the PRET-PD randomized, clinical trial. Mov Disord. 2015;30(12):1657-1663.
Defazio G, Hallett M, Jinnah HA, Stebbins GT, Gigante AF, Ferrazzano G, Conte A, Fabbrini G, Berardelli A. Development and validation of a clinical scale for rating the severity of blepharospasm. Mov Disord. 2015;30(4):525-530.
Dickson DW, Rademakers R, Nicholson AM, Schneider JA, Yu L, Bennett DA. The TMEM106B locus and TDP-43 pathology in older persons without FTLD. Neurology. 2015;85(15):1354-1355.
Dimitrov N, Koenig W, Bosson N, Song S, Saver JL, Mack WJ, Sanossian N. Variability in criteria for emergency medical services routing of acute stroke patients to designated stroke center hospitals. West J Emerg Med. 2015;16(5):743-746.
Dong J, Yang J, Tranah G, Franceschini N, Parimi N, Alkorta-Aranburu G, Xu Z, Alonso A, Cummings SR, Fornage M, Huang X, Kritchevsky S, Liu Y, London S, Niu L, Wilson RS, De Jager PL, Yu L, Singleton AB, Harris T, Mosley TH Jr, Pinto JM, Bennett DA, Chen H. Genome-wide meta-analysis on the sense of smell among US older adults. Medicine (Baltimore). 2015;94(47):e1892.
Doyle KP, Quach LN, Solé M, Axtell RC, Nguyen TV, Soler-Llavina GJ, Jurado S, Han J, Steinman L, Longo FM, Schneider JA, Malenka RC, Buckwalter MS. B-lymphocyte-mediated delayed cognitive impairment following stroke. J Neurosci. 2015;35(5):2133-2145.
Falowski SM, DiLorenzo DJ, Shannon LR, Wallace DJ, Devries J, Kellogg RG, Cozzi NP, Fogg LF, Byrne RW. Optimizations and nuances in neurosurgical technique for the minimization of complications in subdural electrode placement for epilepsy surgery. World Neurosurg. 2015;84(4):989-997.
Filley CM, Brown MS, Onderko K, Ray M, Bennett RE, Berry-Kravis E, Grigsby J. White matter disease and cognitive impairment in FMR1 premutation carriers. Neurology. 2015;84(21):2146-2152.
Fiorella DJ, Fargen KM, Mocco J, Albuquerque F, Hirsch JA, Chen M, Gupta R, Linfante I, Mack W, Rai A, Tarr RW. Thrombectomy for acute ischemic stroke: an evidence-based treatment. J Neurointerv Surg. 2015;7(5):314-315.
Fleischman DA, Yang J, Arfanakis K, Arvanitakis Z, Leurgans SE, Turner AD, Barnes LL, Bennett DA, Buchman AS. Physical activity, motor function, and white matter hyperintensity burden in healthy older adults. Neurology. 2015;84(13):1294-1300.
Fontes RB, Baptista JS, Rabbani SR, Traynelis VC, Liberti EA. Structural and ultrastructural analysis of the cervical discs of young and elderly humans. PLoS One. 2015;10(10):e0139283.
Fraint A, Pal G. Deep brain stimulation in Tourette’s syndrome. Front Neurol. 2015;6:170.
Frisoni GB, Jack CR Jr, Bocchetta M, Bauer C, Frederiksen KS, Liu Y, Preboske G, Swihart T, Blair M, Cavedo E, Grothe MJ, Lanfredi M, Martinez O, Nishikawa M, Portegies M, Stoub T, Ward C, Apostolova LG, Ganzola R, Wolf D, Barkhof F, Bartzokis G, DeCarli C, Csernansky JG, deToledo-Morrell L, Geerlings MI, Kaye J, Killiany RJ, Lehéricy S, Matsuda H, O’Brien J, Silbert LC, Scheltens P, Soininen H, Teipel S, Waldemar G, Fellgiebel A, Barnes J, Firbank M, Gerritsen L, Henneman W, Malykhin N, Pruessner JC, Wang L, Watson C, Wolf H, deLeon M, Pantel J, Ferrari C, Bosco P, Pasqualetti P, Duchesne S, Duvernoy H, Boccardi M; EADC-ADNI Working Group on the Harmonized Protocol for Manual Hippocampal Volumetry and for the Alzheimer’s Disease Neuroimaging Initiative. The EADC-ADNI harmonized protocol for manual hippocampal segmentation on magnetic resonance: evidence of validity. Alzheimers Dement. 2015;11(2):111-125.
Fung VS, Kordower JH. Parkinson’s disease and prion disease: straining the comparison. Mov Disord. 2015;30(13):1727.
Gamble K, Boyle P, Yu L, Bennett D. Aging and financial decision making. Manage Sci. 2015;61(11):2603-2610.
Garcia R Jr, Yue JJ, Blumenthal S, Coric D, Patel VV, Leary SP, Dinh DH, Buttermann GR, Deutsch H, Girardi F, Billys J, Miller LE. Lumbar total disc replacement for discogenic low back pain: two-year outcomes of the activL multicenter randomized controlled IDE clinical trial. Spine (Phila Pa 1976). 2015;40(24):1873-1881.
Gatto RG, Chu Y, Ye AQ, Price SD, Tavassoli E, Buenaventura A, Brady ST, Magin RL, Kordower JH, Morfini GA. Analysis of YFP(J16)-R6/2 reporter mice and postmortem brains reveals early pathology and increased vulnerability of callosal axons in Huntington’s disease. Hum Mol Genet. 2015;24(18):5285-5298.
Gerard CS, Fessler RG. Accurate pedicle screw placement—a perspective statement. World Neurosurg. 2015;83(5):747-749.
Ghani M, Reitz C, Cheng R, Vardarajan BN, Jun G, Sato C, Naj A, Rajbhandary R, Wang LS, Valladares O, Lin CF, Larson EB, Graff-Radford NR, Evans D, De Jager PL, Crane PK, Buxbaum JD, Murrell JR, Raj T, Ertekin-Taner N, Logue M, Baldwin CT, Green RC, Barnes LL, Cantwell LB, Fallin MD, Go RC, Griffith PA, Obisesan TO, Manly JJ, Lunetta KL, Kamboh MI, Lopez OL, Bennett DA, Hendrie H, Hall KS, Goate AM, Byrd GS, Kukull WA, Foroud TM, Haines JL, Farrer LA, Pericak-Vance MA, Lee JH, Schellenberg GD, St George-Hyslop P, Mayeux R, Rogaeva E; Alzheimer’s Disease Genetics Consortium. Association of long runs of homozygosity with Alzheimer disease among African American individuals. JAMA Neurol. 2015;72(11):1313-1323.
52 THE 2016 RUSH NEUROSCIENCE REVIEW

Ghosh A, Jana M, Modi K, Gonzalez FJ, Sims KB, Berry-Kravis E, Pahan K. Activation of peroxisome proliferator-activated receptor α induces lysosomal biogenesis in brain cells: implications for lysosomal storage disorders. J Biol Chem. 2015;290(16):10309-10324.
Gillis CC, Eichholz K, Thoman WJ, Fessler RG. A minimally invasive approach to defects of the pars interarticularis: restoring function in competitive athletes. Clin Neurol Neurosurg. 2015;139:29-34.
Gillow SJ, Lee VH. PFO closure for cryptogenic stroke. Curr Atheroscler Rep. 2015;17(8):525.
Goetz CG, Luo S, Wang L, Tilley BC, LaPelle NR, Stebbins GT. Handling missing values in the MDS-UPDRS. Mov Disord. 2015;30(12):1632-1638.
Goldman JG. Writer’s cramp. Toxicon. 2015;107(pt A):98-104.
Goldman JG, Aggarwal NT, Schroeder CD. Mild cognitive impairment: an update in Parkinson’s disease and lessons learned from Alzheimer’s disease. Neurodegener Dis Manag. 2015;5(5):425-443.
Goldman JG, Holden S, Ouyang B, Bernard B, Goetz CG, Stebbins GT. Diagnosing PD-MCI by MDS Task Force criteria: how many and which neuropsychological tests? Mov Disord. 2015;30(3):402-406.
Goldman JG, Weintraub D. Advances in the treatment of cognitive impairment in Parkinson’s disease. Mov Disord. 2015;30(11):1471-1489.
Gross C, Hoffmann A, Bassell GJ, Berry-Kravis EM. Therapeutic strategies in fragile X syndrome: from bench to bedside and back. Neurotherapeutics. 2015;12(3):584-608.
Gunduz A, Morita H, Rossi PJ, Allen WL, Alterman RL, Bronte-Stewart H, Butson CR, Charles D, Deckers S, de Hemptinne C, DeLong M, Dougherty D, Ellrich J, Foote KD, Giordano J, Goodman W, Greenberg BD, Greene D, Gross R, Judy JW, Karst E, Kent A, Kopell B, Lang A, Lozano A, Lungu C, Lyons KE, Machado A, Martens H, McIntyre C, Min HK, Neimat J, Ostrem J, Pannu S, Ponce F, Pouratian N, Reymers D, Schrock L, Sheth S, Shih L, Stanslaski S, Steinke GK, Stypulkowski P, Tröster AI, Verhagen L, Walker H, Okun MS. Proceedings of the Second Annual Deep Brain Stimulation Think Tank: what’s in the pipeline. Int J Neurosci. 2015;125(7):475-485.
Gupta R, Rai AT, Hirsch JA, Linfante I, Mack W, Mocco J, Albuquerque F, Chen M, Fiorella D, Tarr RW. A research roadmap of future endovascular stroke trials. J Neurointerv Surg. 2015;7(2):82-83.
Gustafson DR, Clare Morris M, Scarmeas N, Shah RC, Sijben J, Yaffe K, Zhu X. New perspectives on Alzheimer’s disease and nutrition. J Alzheimers Dis. 2015;46(4):1111-1127.
Han SD, Boyle PA, James BD, Yu L, Bennett DA. Mild cognitive impairment and susceptibility to scams in old age. J Alzheimers Dis. 2015;49(3):845-851.
Han SD, Boyle PA, James BD, Yu L, Bennett DA. Mild cognitive impairment is associated with poorer decision-making in community-based older persons [published correction appears in J Am Geriatr Soc. 2015;63(6):1286]. J Am Geriatr Soc. 2015;63(4):676-683.
Han SD, Boyle PA, James BD, Yu L, Bennett DA. Poorer financial and health literacy among community-dwelling older adults with mild cognitive impairment. J Aging Health. 2015;27(6):1105-1117.
Herman ST, Abend NS, Bleck TP, Chapman KE, Drislane FW, Emerson RG, Gerard EE, Hahn CD, Husain AM, Kaplan PW, LaRoche SM, Nuwer MR, Quigg M, Riviello JJ, Schmitt SE, Simmons LA, Tsuchida TN, Hirsch LJ; Critical Care Continuous EEG Task Force of the American Clinical Neurophysiology Society. Consensus statement on continuous EEG in critically ill adults and children, I: indications. J Clin Neurophysiol. 2015;32(2):87-95.
Herman ST, Abend NS, Bleck TP, Chapman KE, Drislane FW, Emerson RG, Gerard EE, Hahn CD, Husain AM, Kaplan PW, LaRoche SM, Nuwer MR, Quigg M, Riviello JJ, Schmitt SE, Simmons LA, Tsuchida TN, Hirsch LJ. Consensus statement on continuous EEG in critically ill adults and children, II: personnel, technical specifications, and clinical practice. J Clin Neurophysiol. 2015;32(2):96-108.
Hindman BJ, From RP, Fontes RB, Traynelis VC, Todd MM, Zimmerman MB, Puttlitz CM, Santoni BG. Intubation biomechanics: laryngoscope force and cervical spine motion during intubation in cadavers-cadavers versus patients, the effect of repeated intubations, and the effect of type II odontoid fracture on C1-C2 motion. Anesthesiology. 2015;123(5):1042-1058.
Högl B, Comella C. Therapeutic advances in restless legs syndrome (RLS). Mov Disord. 2015;30(11):1574-1579.
Hohman TJ, Chibnik L, Bush WS, Jefferson AL, De Jaeger PL, Thornton-Wells TA, Bennett DA, Schneider JA. GSK3β interactions with amyloid genes: an autopsy verification and extension. Neurotox Res. 2015;28(3):232-238.
Hutson SL, Wheeler KM, McLone D, Frim D, Penn R, Swisher CN, Heydemann PT, Boyer KM, Noble AG, Rabiah P, Withers S, Montoya JG, Wroblewski K, Karrison T, Grigg ME, McLeod R. Patterns of hydrocephalus caused by congenital Toxoplasma gondii infection associate with parasite genetics. Clin Infect Dis. 2015;61(12):1831-1834.
James BD, Boyle PA, Yu L, Han SD, Bennett DA. Cognitive decline is associated with risk aversion and temporal discounting in older adults without dementia. PLoS One. 2015;10(4):e0121900.
James KA, Hall DA. Groundwater pesticide levels and the association with Parkinson disease. Int J Toxicol. 2015;34(3):266-273.
Jankovic J, Adler CH, Charles D, Comella C, Stacy M, Schwartz M, Manack Adams A, Brin MF. Primary results from the cervical dystonia patient registry for observation of onabotulinumtoxina efficacy (CD PROBE). J Neurol Sci. 2015;349(1-2):84-93.
Jayaraman MV, Hussain MS, Abruzzo T, Albani B, Albuquerque FC, Alexander MJ, Ansari SA, Arthur AS, Baxter B, Bulsara KR, Chen M, Delgado Almandoz JE, Fraser JF, Heck DV, Hetts SW, Kelly M, Lee SK, Leslie-Mawzi T, McTaggart RA, Meyers PM, Prestigiacomo C, Pride GL, Patsalides A, Starke RM, Tarr RW, Frei D, Rasmussen P; Standards and Guidelines Committee of the Society of NeuroInterventional Surgery. Embolectomy for stroke with emergent large vessel occlusion (ELVO): report of the Standards and Guidelines Committee of the Society of NeuroInterventional Surgery [published correction appears in J Neurointerv Surg. 2015;7(8):622]. J Neurointerv Surg. 2015;7(5):316-321.
Select Publications (2015) 53

Jellinger KA, Alafuzoff I, Attems J, Beach TG, Cairns NJ, Crary JF, Dickson DW, Hof PR, Hyman BT, Jack CR Jr, Jicha GA, Knopman DS, Kovacs GG, Mackenzie IR, Masliah E, Montine TJ, Nelson PT, Schmitt F, Schneider JA, Serrano-Pozo A, Thal DR, Toledo JB, Trojanowski JQ, Troncoso JC, Vonsattel JP, Wisniewski T. PART, a distinct tauopathy, different from classical sporadic Alzheimer disease. Acta Neuropathol. 2015;129(5):757-762.
Jette N, Beghi E, Hesdorffer D, Moshé SL, Zuberi SM, Medina MT, Bergen D. ICD coding for epilepsy: past, present, and future—a report by the International League Against Epilepsy Task Force on ICD codes in epilepsy. Epilepsia. 2015;56(3):348-355.
Johnson AK, Munich SA, Tan LA, Heiferman DM, Keigher KM, Lopes DK. Complication analysis in nitinol stent-assisted embolization of 486 intracranial aneurysms. J Neurosurg. 2015;123(2):453-459.
Jost WH, Benecke R, Hauschke D, Jankovic J, Kaňovský P, Roggenkämper P, Simpson DM, Comella CL. Clinical and pharmacological properties of incobotulinumtoxinA and its use in neurological disorders. Drug Des Devel Ther. 2015;9:1913-1926.
Kallmes DF, Hanel R, Lopes D, Boccardi E, Bonafé A, Cekirge S, Fiorella D, Jabbour P, Levy E, McDougall C, Siddiqui A, Szikora I, Woo H, Albuquerque F, Bozorgchami H, Dashti SR, Delgado Almandoz JE, Kelly ME, Turner R IV, Woodward BK, Brinjikji W, Lanzino G, Lylyk P. International retrospective study of the Pipeline Embolization Device: a multicenter aneurysm treatment study [published correction appears in AJNR Am J Neuroradiol. 2015;36(5):E39-E40]. AJNR Am J Neuroradiol. 2015;36(1):108-115.
Kasliwal MK, Dua SG, Harbhajanka A, Nag S, Jhaveri MD, Moftakhar R. Intrasphenoidal Rathke’s cleft cyst. J Clin Neurosci. 2015;22(10):1678-1682.
Kasliwal MK, Dua SG, Mangubat EZ, Lopes DK. Compressive cervical myelopathy secondary to totally extradural spinal arteriovenous fistula. Neurol India. 2015;63(5):790-792.
Kasliwal MK, Moftakhar R, O’Toole JE, Lopes DK. High cervical spinal subdural hemorrhage as a harbinger of craniocervical arteriovenous fistula: an unusual clinical presentation. Spine J. 2015;15(5):e13-e17.
Kasliwal MK, Moore KA, Tan LA, Harbhajanka A, Gattuso P, O’Toole JE. Dialysis-related amyloidosis: an unusual etiology for pathological odontoid fracture. Neurol India. 2015;63(6):965-967.
Kasliwal MK, Panos NG, Muñoz LF, Moftakhar R, Lopes DK, Byrne RW. Outcome following intracranial hemorrhage associated with novel oral anticoagulants. J Clin Neurosci. 2015;22(1):212-215.
Keiser MS, Kordower JH, Gonzalez-Alegre P, Davidson BL. Broad distribution of ataxin 1 silencing in rhesus cerebella for spinocerebellar ataxia type 1 therapy. Brain. 2015;138(pt 12):3555-3566.
Kerolus M, Jeans EB, Fontes RB, Deutsch H, Traynelis VC. Atlantoaxial instability of inflammatory origin in adults: case reports, literature review, and rationale for early surgical intervention. Neurosurgery. 2015;76(2):E226-E232, discussion E232.
Kerolus M, Kasliwal MK, Lopes DK. Persistent aneurysm growth following Pipeline Embolization Device assisted coiling of a fusiform vertebral artery aneurysm: a word of caution! Neurointervention. 2015;10(1):28-33.
Kerr C, Breheny K, Lloyd A, Brazier J, Bailey DB Jr, Berry-Kravis E, Cohen J, Petrillo J. Developing a utility index for the Aberrant Behavior Checklist (ABC-C) for fragile X syndrome. Qual Life Res. 2015;24(2):305-314.
Keshavarzian A, Green SJ, Engen PA, Voigt RM, Naqib A, Forsyth CB, Mutlu E, Shannon KM. Colonic bacterial composition in Parkinson’s disease. Mov Disord. 2015;30(10):1351-1360.
Khanna R, McDevitt JL, McClendon J Jr, Smith ZA, Dahdaleh NS, Fessler RG. Utility of readmission rates as a quality of care measure and predictors of readmission within 30 days after spinal surgery: a single-center, multivariate analysis. Spine (Phila Pa 1976). 2015;40(22):1769-1774.
King-Stephens D, Mirro E, Weber PB, Laxer KD, Van Ness PC, Salanova V, Spencer DC, Heck CN, Goldman A, Jobst B, Shields DC, Bergey GK, Eisenschenk S, Worrell GA, Rossi MA, Gross RE, Cole AJ, Sperling MR, Nair DR, Gwinn RP, Park YD, Rutecki PA, Fountain NB, Wharen RE, Hirsch LJ, Miller IO, Barkley GL, Edwards JC, Geller EB, Berg MJ, Sadler TL, Sun FT, Morrell MJ. Lateralization of mesial temporal lobe epilepsy with chronic ambulatory electrocorticography. Epilepsia. 2015;56(6):959-967.
Kordower JH. Gene therapy for Parkinson’s disease: still a hot topic? Neuropsychopharmacology. 2015;40(1):255-256.
Kotloff RM, Blosser S, Fulda GJ, Malinoski D, Ahya VN, Angel L, Byrnes MC, DeVita MA, Grissom TE, Halpern SD, Nakagawa TA, Stock PG, Sudan DL, Wood KE, Anillo SJ, Bleck TP, Eidbo EE, Fowler RA, Glazier AK, Gries C, Hasz R, Herr D, Khan A, Landsberg D, Lebovitz DJ, Levine DJ, Mathur M, Naik P, Niemann CU, Nunley DR, O’Connor KJ, Pelletier SJ, Rahman O, Ranjan D, Salim A, Sawyer RG, Shafer T, Sonneti D, Spiro P, Valapour M, Vikraman-Sushama D, Whelan TP; Society of Critical Care Medicine/American College of Chest Physicians/Association of Organ Procurement Organizations Donor Management Task Force. Management of the potential organ donor in the ICU: Society of Critical Care Medicine/American College of Chest Physicians/Association of Organ Procurement Organizations consensus statement. Crit Care Med. 2015;43(6):1291-1325.
Kotrotsou A, Schneider JA, Bennett DA, Leurgans SE, Dawe RJ, Boyle PA, Golak T, Arfanakis K. Neuropathologic correlates of regional brain volumes in a community cohort of older adults. Neurobiol Aging. 2015;36(10):2798-2805.
Kurani AS, Seidler RD, Burciu RG, Comella CL, Corcos DM, Okun MS, MacKinnon CD, Vaillancourt DE. Subthalamic nucleus—sensorimotor cortex functional connectivity in de novo and moderate Parkinson’s disease. Neurobiol Aging. 2015;36(1):462-469.
Kwon I, Choi S, Mittman B, Bharmal N, Liu H, Vickrey B, Song S, Araiza D, McCreath H, Seeman T, Oh SM, Trejo L, Sarkisian C. Study protocol of “Worth the Walk”: a randomized controlled trial of a stroke risk reduction walking intervention among racial/ethnic minority older adults with hypertension in community senior centers. BMC Neurol. 2015;15:91.
Lachs MS, Han SD. Age-associated financial vulnerability: an emerging public health issue. Ann Intern Med. 2015;163(11):877-878.
Lamotte G, Rafferty MR, Prodoehl J, Kohrt WM, Comella CL, Simuni T, Corcos DM. Effects of endurance exercise training on the motor and non-motor features of Parkinson’s disease: a review [published correction appears in J Parkinsons Dis. 2015;5(3):621]. J Parkinsons Dis. 2015;5(1):21-41.
54 THE 2016 RUSH NEUROSCIENCE REVIEW

Langbaum JB, Hendrix S, Ayutyanont N, Bennett DA, Shah RC, Barnes LL, Lopera F, Reiman EM, Tariot PN. Establishing composite cognitive endpoints for use in preclinical Alzheimer’s disease trials. J Prev Alzheimers Dis. 2015;2(1):2-3.
Lauryssen C, Jackson RJ, Baron JM, Tallarico RA, Lavelle WF, Deutsch H, Block JE, Geisler FH. Stand-alone interspinous spacer versus decompressive laminectomy for treatment of lumbar spinal stenosis. Expert Rev Med Devices. 2015;12(6):763-769.
Lewis SL. Disorders that strike a cord. Continuum (Minneap Minn). 2015;21(1):11-12.
Lewis SL. For all intensive purposes. Continuum (Minneap Minn). 2015;21(5):1261-1262.
Lewis SL. Neuro-oncology for the masses. Continuum (Minneap Minn). 2015;21(2):299-300.
Lewis SL. Preface: totally psyched. Continuum (Minneap Minn). 2015;21(3):595-596.
Lewis SL. Scintillating discussions. Continuum (Minneap Minn). 2015;21(4):951-952.
Li L, Bao Y, He S, Wang G, Guan Y, Ma D, Wu R, Wang P, Huang X, Tao S, Liu Q, Wang Y, Yang J. The association between apolipoprotein E and functional outcome after traumatic brain injury: a meta-analysis. Medicine (Baltimore). 2015;94(46):e2028.
Lin N, Brouillard AM, Keigher KM, Lopes DK, Binning MJ, Liebman KM, Veznedaroglu E, Magarik JA, Mocco J, Duckworth EA, Arthur AS, Ringer AJ, Snyder KV, Levy EI, Siddiqui AH. Utilization of Pipeline Embolization Device for treatment of ruptured intracranial aneurysms: US multicenter experience. J Neurointerv Surg. 2015;7(11):808-815.
Lugli G, Cohen AM, Bennett DA, Shah RC, Fields CJ, Hernandez AG, Smalheiser NR. Plasma exosomal miRNAs in persons with and without Alzheimer disease: altered expression and prospects for biomarkers. PLoS One. 2015;10(10):e0139233.
Malik R, Irodenko V, Zimmermann L, Green A, Layzer R. Focal amyotrophy in multiple sclerosis. Muscle Nerve. 2015;51(1):137-140.
Mangubat E, Sani S. Acute global ischemic stroke after cranioplasty: case report and review of the literature. Neurologist. 2015;19(5):135-139.
Mangubat EZ, Kellogg RG, Harris TJ Jr, Rossi MA. On-demand pulsatile intracerebral delivery of carisbamate with closed-loop direct neurostimulation therapy in an electrically induced self-sustained focal-onset epilepsy rat model. J Neurosurg. 2015;122(6):1283-1292.
Marsh JC, Goldman S, Ziel E, Bregman C, Diaz A, Byrne R, Fangusaro J. Involvement of the neural stem cell compartment by pediatric and adult gliomas: a retrospective review of 377 cases. J Neurooncol. 2015;122(1):105-110.
Martinez-Martin P, Chaudhuri KR, Rojo-Abuin JM, Rodriguez-Blazquez C, Alvarez-Sanchez M, Arakaki T, Bergareche-Yarza A, Chade A, Garretto N, Gershanik O, Kurtis MM, Martinez-Castrillo JC, Mendoza-Rodriguez A, Moore HP, Rodriguez-Violante M, Singer C, Tilley BC, Huang J, Stebbins GT, Goetz CG. Assessing the non-motor symptoms of Parkinson’s disease: MDS-UPDRS and NMS Scale. Eur J Neurol. 2015;22(1):37-43.
Masood SA, Kazmouz S, Heydemann P, Li H, Kenny D. Under-recognition of low blood pressure readings in patients with Duchenne muscular dystrophy. Pediatr Cardiol. 2015;36(7):1489-1494.
Meriggioli MN. The clinical spectrum of necrotizing autoimmune myopathy: a mixed bag with blurred lines. JAMA Neurol. 2015;72(9):977-979.
Meriggioli MN, Roubenoff R. Prospect for pharmacological therapies to treat skeletal muscle dysfunction. Calcif Tissue Int. 2015;96(3):234-242.
Metman LV, Slavin KV. Advances in functional neurosurgery for Parkinson’s disease. Mov Disord. 2015;30(11):1461-1470.
Mocco J, Fiorella D, Fargen KM, Albuquerque F, Chen M, Gupta R, Hirsch JA, Linfante I, Mack W, Rai AT, Tarr RW. Endovascular therapy for acute ischemic stroke is indicated and evidence based: a position statement. J Neurointerv Surg. 2015;7(2):79-81.
Modi KK, Jana M, Mondal S, Pahan K. Sodium benzoate, a metabolite of cinnamon and a food additive, upregulates ciliary neurotrophic factor in astrocytes and oligodendrocytes. Neurochem Res. 2015;40(11):2333-2347.
Modi KK, Roy A, Brahmachari S, Rangasamy SB, Pahan K. Cinnamon and its metabolite sodium benzoate attenuate the activation of p21rac and protect memory and learning in an animal model of Alzheimer’s disease. PLoS One. 2015;10(6):e0130398.
Mokin M, Lopes DK, Binning MJ, Veznedaroglu E, Liebman KM, Arthur AS, Doss VT, Levy EI, Siddiqui AH. Endovascular treatment of cerebral venous thrombosis: contemporary multicenter experience. Interv Neuroradiol. 2015;21(4):520-526.
Mondal S, Pahan K. Cinnamon ameliorates experimental allergic encephalomyelitis in mice via regulatory T cells: implications for multiple sclerosis therapy. PLoS One. 2015;10(1):e0116566.
Morris MC, Schneider JA, Li H, Tangney CC, Nag S, Bennett DA, Honer WG, Barnes LL. Brain tocopherols related to Alzheimer’s disease neuropathology in humans. Alzheimers Dement. 2015;11(1):32-39.
Morris MC, Tangney CC, Wang Y, Sacks FM, Barnes LL, Bennett DA, Aggarwal NT. MIND diet slows cognitive decline with aging. Alzheimers Dement. 2015;11(9):1015-1022.
Morris MC, Tangney CC, Wang Y, Sacks FM, Bennett DA, Aggarwal NT. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimers Dement. 2015;11(9):1007-1014.
Mufson E, Rubinson K, Scalia F. Walter Riss, PhD, 1925-2015. Brain Behav Evol. 2015;86(2):77-78.
Mufson EJ, Mahady L, Waters D, Counts SE, Perez SE, DeKosky ST, Ginsberg SD, Ikonomovic MD, Scheff SW, Binder LI. Hippocampal plasticity during the progression of Alzheimer’s disease. Neuroscience. 2015;309:51-67.
Mukherjee S, Walter S, Kauwe JS, Saykin AJ, Bennett DA, Larson EB, Crane PK, Glymour MM; Adult Changes in Thought Study Investigators; Religious Orders Study/Memory and Aging Project Investigators; Alzheimer’s Disease Genetics Consortium. Genetically predicted body mass index and Alzheimer’s disease-related phenotypes in three large samples: mendelian randomization analyses. Alzheimers Dement. 2015;11(12):1439-1451.
Select Publications (2015) 55

Nadimpalli SB, James BD, Yu L, Cothran F, Barnes LL. The association between discrimination and depressive symptoms among older African Americans: the role of psychological and social factors. Exp Aging Res. 2015;41(1):1-24.
Nag S, Yu L, Capuano AW, Wilson RS, Leurgans SE, Bennett DA, Schneider JA. Hippocampal sclerosis and TDP-43 pathology in aging and Alzheimer disease. Ann Neurol. 2015;77(6):942-952.
Nation DA, Edmonds EC, Bangen KJ, Delano-Wood L, Scanlon BK, Han SD, Edland SD, Salmon DP, Galasko DR, Bondi MW; Alzheimer’s Disease Neuroimaging Initiative Investigators. Pulse pressure in relation to tau-mediated neurodegeneration, cerebral amyloidosis, and progression to dementia in very old adults. JAMA Neurol. 2015;72(5):546-553.
Neely KA, Kurani AS, Shukla P, Planetta PJ, Wagle Shukla A, Goldman JG, Corcos DM, Okun MS, Vaillancourt DE. Functional brain activity relates to 0-3 and 3-8 Hz force oscillations in essential tremor. Cereb Cortex. 2015;25(11):4191-4202.
Neuman KM, Molina-Campos E, Musial TF, Price AL, Oh KJ, Wolke ML, Buss EW, Scheff SW, Mufson EJ, Nicholson DA. Evidence for Alzheimer’s disease-linked synapse loss and compensation in mouse and human hippocampal CA1 pyramidal neurons. Brain Struct Funct. 2015;220(6):3143-3165.
Nogueira RG, Gupta R, Jovin TG, Levy EI, Liebeskind DS, Zaidat OO, Rai A, Hirsch JA, Hsu DP, Rymer MM, Tayal AH, Lin R, Natarajan SK, Nanda A, Tian M, Hao Q, Kalia JS, Chen M, Abou-Chebl A, Nguyen TN, Yoo AJ. Predictors and clinical relevance of hemorrhagic transformation after endovascular therapy for anterior circulation large vessel occlusion strokes: a multicenter retrospective analysis of 1122 patients. J Neurointerv Surg. 2015;7(1):16-21.
Odland AP, Lammy AB, Perle JG, Martin PK, Grote CL. Reaffirming normal: the high risk of pathologizing healthy adults when interpreting the MMPI-2-RF. Clin Neuropsychol. 2015;29(1):38-52.
O’Keefe JA, Robertson-Dick E, Dunn EJ, Li Y, Deng Y, Fiutko AN, Berry-Kravis E, Hall DA. Characterization and early detection of balance deficits in fragile X premutation carriers with and without fragile X-associated tremor/ataxia syndrome (FXTAS). Cerebellum. 2015;14(6):650-662.
Olanow CW, Bartus RT, Volpicelli-Daley LA, Kordower JH. Trophic factors for Parkinson’s disease: to live or let die. Mov Disord. 2015;30(13):1715-1724.
O’Neill W, Penn R, Werner M, Thomas J. A theory of fine structure image models with an application to detection and classification of dementia. Quant Imaging Med Surg. 2015;5(3):356-367.
O’Toole JE. Guest editorial: high impact spinal surgery articles. Neurosurgery. 2015;76(suppl 1):S1-S3.
Pahan K. Prospects of cinnamon in multiple sclerosis. J Mult Scler (Foster City). 2015;2(3):1000149.
Pahan P, Pahan K. Can cinnamon bring aroma in Parkinson’s disease treatment? Neural Regen Res. 2015;10(1):30-32.
Pal GD, Shaikh M, Forsyth CB, Ouyang B, Keshavarzian A, Shannon KM. Abnormal lipopolysaccharide binding protein as marker of gastrointestinal inflammation in Parkinson disease. Front Neurosci. 2015;9:306.
Park P, Wang MY, Lafage V, Nguyen S, Ziewacz J, Okonkwo DO, Uribe JS, Eastlack RK, Anand N, Haque R, Fessler RG, Kanter AS, Deviren V, La Marca F, Smith JS, Shaffrey CI, Mundis GM Jr, Mummaneni PV; International Spine Study Group. Comparison of two minimally invasive surgery strategies to treat adult spinal deformity. J Neurosurg Spine. 2015;22(4):374-380.
Perez SE, He B, Nadeem M, Wuu J, Ginsberg SD, Ikonomovic MD, Mufson EJ. Hippocampal endosomal, lysosomal, and autophagic dysregulation in mild cognitive impairment: correlation with aβ and tau pathology. J Neuropathol Exp Neurol. 2015;74(4):345-358.
Perez SE, He B, Nadeem M, Wuu J, Scheff SW, Abrahamson EE, Ikonomovic MD, Mufson EJ. Resilience of precuneus neurotrophic signaling pathways despite amyloid pathology in prodromal Alzheimer’s disease. Biol Psychiatry. 2015;77(8):693-703.
Petersen RB, Lissemore FM, Appleby B, Aggarwal N, Boyatzis R, Casadesus G, Cummings J, Jack A, Perry G, Safar J, Sajatovic M, Surewicz WK, Wang Y, Whitehouse P, Lerner A. From neurodegeneration to brain health: an integrated approach. J Alzheimers Dis. 2015;46(1):271-283.
Petruzzelli GJ, Howell JB, Pederson A, Origitano TC, Byrne RW, Muñoz L, Emami B, Clark JI. Multidisciplinary treatment of olfactory neuroblastoma: patterns of failure and management of recurrence. Am J Otolaryngol. 2015;36(4):547-553.
Pivtoraiko VN, Abrahamson EE, Leurgans SE, DeKosky ST, Mufson EJ, Ikonomovic MD. Cortical pyroglutamate amyloid-β levels and cognitive decline in Alzheimer’s disease. Neurobiol Aging. 2015;36(1):12-19.
Planetta PJ, Kurani AS, Shukla P, Prodoehl J, Corcos DM, Comella CL, McFarland NR, Okun MS, Vaillancourt DE. Distinct functional and macrostructural brain changes in Parkinson’s disease and multiple system atrophy. Hum Brain Mapp. 2015;36(3):1165-1179.
Poewe W, Goetz CG. Preface. Mov Disord. 015;30(11):1441.
Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, Obeso J, Marek K, Litvan I, Lang AE, Halliday G, Goetz CG, Gasser T, Dubois B, Chan P, Bloem BR, Adler CH, Deuschl G. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591-1601.
Prodoehl J, Rafferty MR, David FJ, Poon C, Vaillancourt DE, Comella CL, Leurgans SE, Kohrt WM, Corcos DM, Robichaud JA. Two-year exercise program improves physical function in Parkinson’s disease: the PRET-PD randomized clinical trial. Neurorehabil Neural Repair. 2015;29(2):112-122.
Rajan KB, Barnes LL, Skarupski KA, Mendes de Leon CF, Wilson RS, Evans DA. Physical and cognitive activities as deterrents of cognitive decline in a biracial population sample. Am J Geriatr Psychiatry. 2015;23(12):1225-1233.
Rajan KB, Schneider JA, Aggarwal NT, Wilson RS, Everson-Rose SA, Evans DA. Racial differences in cognitive function and risk of incident stroke. J Stroke Cerebrovasc Dis. 2015;24(12):2854-2859.
Rajan KB, Wilson RS, Weuve J, Barnes LL, Evans DA. Cognitive impairment 18 years before clinical diagnosis of Alzheimer disease dementia. Neurology. 2015;85(10):898-904.
56 THE 2016 RUSH NEUROSCIENCE REVIEW

Ralph JW, Malik R, Layzer RB. Cervical myelopathy caused by injections into the neck. Neurohospitalist. 2015;5(4):212-216.
Ramanan VK, Nho K, Shen L, Risacher SL, Kim S, McDonald BC, Farlow MR, Foroud TM, Gao S, Soininen H, Kłoszewska I, Mecocci P, Tsolaki M, Vellas B, Lovestone S, Aisen PS, Petersen RC, Jack CR Jr, Shaw LM, Trojanowski JQ, Weiner MW, Green RC, Toga AW, De Jager PL, Yu L, Bennett DA, Saykin AJ. FASTKD2 is associated with memory and hippocampal structure in older adults. Mol Psychiatry. 2015;20(10):1197-1204.
Ramanan VK, Risacher SL, Nho K, Kim S, Shen L, McDonald BC, Yoder KK, Hutchins GD, West JD, Tallman EF, Gao S, Foroud TM, Farlow MR, De Jager PL, Bennett DA, Aisen PS, Petersen RC, Jack CR Jr, Toga AW, Green RC, Jagust WJ, Weiner MW, Saykin AJ; Alzheimer’s Disease Neuroimaging Initiative (ADNI). GWAS of longitudinal amyloid accumulation on 18F-florbetapir PET in Alzheimer’s disease implicates microglial activation gene IL1RAP. Brain. 2015;138(pt 10):3076-3088.
Ramos-Miguel A, Hercher C, Beasley CL, Barr AM, Bayer TA, Falkai P, Leurgans SE, Schneider JA, Bennett DA, Honer WG. Loss of Munc18-1 long splice variant in GABAergic terminals is associated with cognitive decline and increased risk of dementia in a community sample. Mol Neurodegener. 2015;10:65.
Rangasamy SB, Corbett GT, Roy A, Modi KK, Bennett DA, Mufson EJ, Ghosh S, Pahan K. Intranasal delivery of NEMO-binding domain peptide prevents memory loss in a mouse model of Alzheimer’s disease. J Alzheimers Dis. 2015;47(2):385-402.
Replogle JM, Chan G, White CC, Raj T, Winn PA, Evans DA, Sperling RA, Chibnik LB, Bradshaw EM, Schneider JA, Bennett DA, De Jager PL. A TREM1 variant alters the accumulation of Alzheimer-related amyloid pathology. Ann Neurol. 2015;77(3):469-477.
Rieu I, Martinez-Martin P, Pereira B, De Chazeron I, Verhagen Metman L, Jahanshahi M, Ardouin C, Chéreau I, Brefel-Courbon C, Ory-Magne F, Klinger H, Peyrol F, Schupbach M, Dujardin K, Tison F, Houeto JL, Krack P, Durif F. International validation of a behavioral scale in Parkinson’s disease without dementia. Mov Disord. 2015;30(5):705-713.
Rijpma A, Meulenbroek O, van Hees AM, Sijben JW, Vellas B, Shah RC, Bennett DA, Scheltens P, Olde Rikkert MG. Effects of Souvenaid on plasma micronutrient levels and fatty acid profiles in mild and mild-to-moderate Alzheimer’s disease. Alzheimers Res Ther. 2015;7(1):51.
Rossi MA. Postresective outcome nomograms: a patient-specific prediction tool for the clinic? Epilepsy Curr. 2015;15(5):257-259.
Rossi MA. Regaining white matter integrity and neurocognitive development in rolandic epilepsy after the storm. Epilepsy Curr. 2015;15(1):20-23.
Rossi MA. Where have all the temporal lobe epilepsy surgeries gone? Epilepsy Curr. 2015;15(3):126-128.
Roy A, Jana M, Kundu M, Corbett GT, Rangaswamy SB, Mishra RK, Luan CH, Gonzalez FJ, Pahan K. HMG-CoA reductase inhibitors bind to PPARα to upregulate neurotrophin expression in the brain and improve memory in mice. Cell Metab. 2015;22(2):253-265.
Roy A, Mondal S, Kordower JH, Pahan K. Attenuation of microglial RANTES by NEMO-binding domain peptide inhibits the infiltration of CD8(+) T cells in the nigra of hemiparkinsonian monkey. Neuroscience. 2015;302:36-46.
Roy A, Pahan K. PPARα signaling in the hippocampus: crosstalk between fat and memory. J Neuroimmune Pharmacol. 2015;10(1):30-34.
Sahlein DH, Fouladvand M, Becske T, Saatci I, McDougall CG, Szikora I, Lanzino G, Moran CJ, Woo HH, Lopes DK, Berez AL, Cher DJ, Siddiqui AH, Levy EI, Albuquerque FC, Fiorella DJ, Berentei Z, Marosfoi M, Cekirge SH, Kallmes DF, Nelson PK. Neuroophthalmological outcomes associated with use of the Pipeline Embolization Device: analysis of the PUFS trial results. J Neurosurg. 2015;123(4):897-905.
Samartzis D, Gillis CC, Shih P, O’Toole JE, Fessler RG. Intramedullary spinal cord tumors, I: epidemiology, pathophysiology, and diagnosis. Global Spine J. 2015;5(5):425-435.
Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, Albers GW, Cognard C, Cohen DJ, Hacke W, Jansen O, Jovin TG, Mattle HP, Nogueira RG, Siddiqui AH, Yavagal DR, Devlin TG, Lopes DK, Reddy V, du Mesnil de Rochemont R, Jahan R; SWIFT PRIME Investigators. Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment for Acute Ischemic Stroke (SWIFT PRIME) trial: protocol for a randomized, controlled, multicenter study comparing the Solitaire revascularization device with IV tPA with IV tPA alone in acute ischemic stroke. Int J Stroke. 2015;10(3):439-448.
Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, Albers GW, Cognard C, Cohen DJ, Hacke W, Jansen O, Jovin TG, Mattle HP, Nogueira RG, Siddiqui AH, Yavagal DR, Baxter BW, Devlin TG, Lopes DK, Reddy VK, du Mesnil de Rochemont R, Singer OC, Jahan R; SWIFT PRIME Investigators. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 2015;372(24):2285-2295.
Scheer JK, Auffinger B, Wong RH, Lam SK, Lawton CD, Nixon AT, Dahdaleh NS, Smith ZA, Fessler RG. Minimally invasive transforaminal lumbar interbody fusion (TLIF) for spondylolisthesis in 282 patients: in situ arthrodesis versus reduction. World Neurosurg. 2015;84(1):108-113.
Scheer JK, Khanna R, Lopez AJ, Fessler RG, Koski TR, Smith ZA, Dahdaleh NS. The concave versus convex approach for minimally invasive lateral lumbar interbody fusion for thoracolumbar degenerative scoliosis. J Clin Neurosci. 2015;22(10):1588-1593.
Scheff SW, Price DA, Ansari MA, Roberts KN, Schmitt FA, Ikonomovic MD, Mufson EJ. Synaptic change in the posterior cingulate gyrus in the progression of Alzheimer’s disease. J Alzheimers Dis. 2015;43(3):1073-1090.
Schuster J, Lai RK, Recht LD, Reardon DA, Paleologos NA, Groves MD, Mrugala MM, Jensen R, Baehring JM, Sloan A, Archer GE, Bigner DD, Cruickshank S, Green JA, Keler T, Davis TA, Heimberger AB, Sampson JH. A phase II, multicenter trial of rindopepimut (CDX-110) in newly diagnosed glioblastoma: the ACT III study. Neuro Oncol. 2015;17(6):854-861.
Shannon KM, Fraint A. Therapeutic advances in Huntington’s disease. Mov Disord. 2015;30(11):1539-1546.
Sharp ME, Caccappolo E, Mejia-Santana H, Tang MX, Rosado L, Orbe Reilly M, Ruiz D, Louis ED, Comella C, Nance M, Bressman S, Scott WK, Tanner C, Waters C, Fahn S, Cote L, Ford B, Rezak M, Novak K, Friedman JH, Pfeiffer R, Payami H, Molho E, Factor SA, Nutt J, Serrano C, Arroyo M, Pauciulo MW, Nichols WC, Clark LN, Alcalay RN, Marder KS. The relationship between obsessive-compulsive symptoms and PARKIN genotype: the CORE-PD study. Mov Disord. 2015;30(2):278-283.
Select Publications (2015) 57

Sheft S, Shafiro V, Wang E, Barnes LL, Shah RC. Relationship between auditory and cognitive abilities in older adults. PLoS One. 2015;10(8):e0134330.
Simkin D, Hattori S, Ybarra N, Musial TF, Buss EW, Richter H, Oh MM, Nicholson DA, Disterhoft JF. Aging-related hyperexcitability in CA3 pyramidal neurons is mediated by enhanced A-type K+ channel function and expression. J Neurosci. 2015;35(38):13206-13218.
Smith PY, Hernandez-Rapp J, Jolivette F, Lecours C, Bisht K, Goupil C, Dorval V, Parsi S, Morin F, Planel E, Bennett DA, Fernandez-Gomez FJ, Sergeant N, Buée L, Tremblay MÈ, Calon F, Hébert SS. miR-132/212 deficiency impairs tau metabolism and promotes pathological aggregation in vivo. Hum Mol Genet. 2015;24(23):6721-6735.
Smith TR, Habib A, Rosenow JM, Nahed BV, Babu MA, Cybulski G, Fessler R, Batjer HH, Heary RF. Defensive medicine in neurosurgery: does state-level liability risk matter? Neurosurgery. 2015;76(2):105-113, discussion 113-114.
Snyder HM, Corriveau RA, Craft S, Faber JE, Greenberg SM, Knopman D, Lamb BT, Montine TJ, Nedergaard M, Schaffer CB, Schneider JA, Wellington C, Wilcock DM, Zipfel GJ, Zlokovic B, Bain LJ, Bosetti F, Galis ZS, Koroshetz W, Carrillo MC. Vascular contributions to cognitive impairment and dementia including Alzheimer’s disease. Alzheimers Dement. 2015;11(6):710-717.
Sohail S, Yu L, Bennett DA, Buchman AS, Lim AS. Irregular 24-hour activity rhythms and the metabolic syndrome in older adults. Chronobiol Int. 2015;32(6):802-813.
Srivatsal S, Cholerton B, Leverenz JB, Wszolek ZK, Uitti RJ, Dickson DW, Weintraub D, Trojanowski JQ, Van Deerlin VM, Quinn JF, Chung KA, Peterson AL, Factor SA, Wood-Siverio C, Goldman JG, Stebbins GT, Bernard B, Ritz B, Rausch R, Espay AJ, Revilla FJ, Devoto J, Rosenthal LS, Dawson TM, Albert MS, Mata IF, Hu SC, Montine KS, Johnson C, Montine TJ, Edwards KL, Zhang J, Zabetian CP. Cognitive profile of LRRK2-related Parkinson’s disease. Mov Disord. 2015;30(5):728-733.
Straus D, Takagi I, O’Toole J. Minimally invasive direct lateral approach to the thoracolumbar junction: cadaveric analysis and case illustrations. J Neurol Surg A Cent Eur Neurosurg. 2015;76(1):56-62.
Su X, Chu Y, Kordower JH, Li B, Cao H, Huang L, Nishida M, Song L, Wang D, Federoff HJ. PGC-1α promoter methylation in Parkinson’s disease. PLoS One. 2015;10(8):e0134087.
Sweis RT, Ouyang B, Lopez GA, Bleck TP, Busl KM. Falcine and tentorial subdural hematomas may not routinely require transfer to a tertiary care center. J Emerg Med. 2015;49(5): 679-685.
Tan LA, Ahuja SK, Deutsch H. The “screwed aorta” after spinal deformity surgery. Br J Neurosurg. 2015;29(2):290.
Tan LA, Boco T, Johnson AK, Rivas FF, Ahmed S, Byrd SE, Byrne RW. Magnetic resonance imaging characteristics of typical and atypical/anaplastic meningiomas—case series and literature review. Br J Neurosurg. 2015;29(1):77-81.
Tan LA, Byrne RW. Anterior temporal sulcus: a reliable intraoperative landmark for accurately delineating the superior limit of amygdala resection during anterior temporal lobectomy. Stereotact Funct Neurosurg. 2015;93(5):360-365.
Tan LA, Byrne RW. Bilateral humeral fractures mimicking Todd’s paralysis. Br J Neurosurg. 2015;29(5):733.
Tan LA, Deutsch H. Severe spinal cord compression due to extramedullary hematopoiesis. Br J Neurosurg. 2015;29(5):737-738.
Tan LA, Deutsch H. Thermal injury of thoracic spinal cord after percutaneous cryoablation of spinal tumor—when needles are more dangerous than the knife. Br J Neurosurg. 2015;29(3):443.
Tan LA, Gerard CS, Keigher KM, Moftakhar R, Lopes DK. Ventriculoperitoneal shunt in a patient with ruptured blister aneurysm treated with Pipeline Embolization Device. J Cerebrovasc Endovasc Neurosurg. 2015;17(1):54-58.
Tan LA, Kasliwal MK, Arvanitis LD, Byrne RW. Enlarging scalp mass. J Neurooncol. 2015;122(2):419-420.
Tan LA, Kasliwal MK, Deutsch H. Complications associated with epidural steroid injection. J Neurosurg Spine. 2015;22(5):558-559.
Tan LA, Kasliwal MK, Deutsch H. Rapidly progressive quadriparesis secondary to cervical epidural hematoma—a rare complication of epidural injection. Br J Neurosurg. 2015;29(2):280.
Tan LA, Kasliwal MK, Harbhajanka A, Kellogg RG, Arvanitis LD, Muñoz LF. Hyperdense suprasellar mass: an unusual radiological presentation of intracranial dermoid cyst. J Clin Neurosci. 2015;22(7):1208-1210.
Tan LA, Kasliwal MK, O’Toole JE. Minimally invasive combined direct lateral and posterior transpedicular approach for 360° resection of a lumbar aneurysmal bone cyst with spinal stabilization. Spine J. 2015;15(10):e37-e38.
Tan LA, Keigher KM, Munich SA, Moftakhar R, Lopes DK. Thromboembolic complications with Pipeline Embolization Device placement: impact of procedure time, number of stents and pre-procedure P2Y12 reaction unit (PRU) value. J Neurointerv Surg. 2015;7(3):217-221.
Tan LA, Lopes DK. Surgical management of malignant cerebral edema secondary to immune reconstitution inflammatory syndrome from natalizumab-associated progressive multifocal encephalopathy. J Clin Neurosci. 2015;22(10):1669-1671.
Tan LA, Muñoz LF. Giant pontine capillary telangiectasia. Br J Neurosurg. 2015;29(4):574-575.
Tan LA, Sandler V, Todorova-Koteva K, Levine L, Lopes DK, Moftakhar R. Recovery of pituitary function following treatment of an unruptured giant cavernous carotid aneurysm using Surpass flow-diverting stents. J Neurointerv Surg. 2015;7(6):e20.
Tan LA, Straus DC, Traynelis VC. Cervical interfacet spacers and maintenance of cervical lordosis. J Neurosurg Spine. 2015;22(5):466-469.
Tanner CM, Comella CL. When brawn benefits brain: physical activity and Parkinson’s disease risk. Brain. 2015;138(pt 2):238-239.
Tasaki S, Sauerwine B, Hoff B, Toyoshiba H, Gaiteri C, Chaibub Neto E. Bayesian network reconstruction using systems genetics data: comparison of MCMC methods. Genetics. 2015;199(4):973-989.
Turner AD, Capuano AW, Wilson RS, Barnes LL. Depressive symptoms and cognitive decline in older African Americans: two scales and their factors. Am J Geriatr Psychiatry. 2015;23(6):568-578.
58 THE 2016 RUSH NEUROSCIENCE REVIEW

Uddin OM, Haque R, Sugrue PA, Ahmed YM, El Ahmadieh TY, Press JM, Koski T, Fessler RG. Cost minimization in treatment of adult degenerative scoliosis. J Neurosurg Spine. 2015;23(6):798-806.
VanderHorst VG, Samardzic T, Saper CB, Anderson MP, Nag S, Schneider JA, Bennett DA, Buchman AS. α-Synuclein pathology accumulates in sacral spinal visceral sensory pathways. Ann Neurol. 2015;78(1):142-149.
Verhaaren BF, Debette S, Bis JC, Smith JA, Ikram MK, Adams HH, Beecham AH, Rajan KB, Lopez LM, Barral S, van Buchem MA, van der Grond J, Smith AV, Hegenscheid K, Aggarwal NT, de Andrade M, Atkinson EJ, Beekman M, Beiser AS, Blanton SH, Boerwinkle E, Brickman AM, Bryan RN, Chauhan G, Chen CP, Chouraki V, de Craen AJ, Crivello F, Deary IJ, Deelen J, De Jager PL, Dufouil C, Elkind MS, Evans DA, Freudenberger P, Gottesman RF, Guðnason V, Habes M, Heckbert SR, Heiss G, Hilal S, Hofer E, Hofman A, Ibrahim-Verbaas CA, Knopman DS, Lewis CE, Liao J, Liewald DC, Luciano M, van der Lugt A, Martinez OO, Mayeux R, Mazoyer B, Nalls M, Nauck M, Niessen WJ, Oostra BA, Psaty BM, Rice KM, Rotter JI, von Sarnowski B, Schmidt H, Schreiner PJ, Schuur M, Sidney SS, Sigurdsson S, Slagboom PE, Stott DJ, van Swieten JC, Teumer A, Töglhofer AM, Traylor M, Trompet S, Turner ST, Tzourio C, Uh HW, Uitterlinden AG, Vernooij MW, Wang JJ, Wong TY, Wardlaw JM, Windham BG, Wittfeld K, Wolf C, Wright CB, Yang Q, Zhao W, Zijdenbos A, Jukema JW, Sacco RL, Kardia SL, Amouyel P, Mosley TH, Longstreth WT Jr, DeCarli CC, van Duijn CM, Schmidt R, Launer LJ, Grabe HJ, Seshadri SS, Ikram MA, Fornage M. Multiethnic genome-wide association study of cerebral white matter hyperintensities on MRI. Circ Cardiovasc Genet. 2015;8(2):398-409.
Verhagen Metman L, Stover N, Chen C, Cowles VE, Sweeney M. Gastroretentive carbidopa/levodopa, DM-1992, for the treatment of advanced Parkinson’s disease. Mov Disord. 2015;30(9):1222-1228.
Vinay DS, Ryan EP, Pawelec G, Talib WH, Stagg J, Elkord E, Lichtor T, Decker WK, Whelan RL, Kumara HM, Signori E, Honoki K, Georgakilas AG, Amin A, Helferich WG, Boosani CS, Guha G, Ciriolo MR, Chen S, Mohammed SI, Azmi AS, Keith WN, Bilsland A, Bhakta D, Halicka D, Fujii H, Aquilano K, Ashraf SS, Nowsheen S, Yang X, Choi BK, Kwon BS. Immune evasion in cancer: mechanistic basis and therapeutic strategies. Semin Cancer Biol. 2015;35(suppl):S185-S198.
Wakeman DR. Autologous iPSC-derived dopamine neuron grafts show considerable promise in a nonhuman primate model of Parkinson’s disease. Mov Disord. 2015;30(8):1034.
Wang JL, Lim AS, Chiang WY, Hsieh WH, Lo MT, Schneider JA, Buchman AS, Bennett DA, Hu K, Saper CB. Suprachiasmatic neuron numbers and rest-activity circadian rhythms in older humans. Ann Neurol. 2015;78(2):317-322.
Wang LS, Naj AC, Graham RR, Crane PK, Kunkle BW, Cruchaga C, Murcia JD, Cannon-Albright L, Baldwin CT, Zetterberg H, Blennow K, Kukull WA, Faber KM, Schupf N, Norton MC, Tschanz JT, Munger RG, Corcoran CD, Rogaeva E; Alzheimer’s Disease Genetics Consortium, Lin CF, Dombroski BA, Cantwell LB, Partch A, Valladares O, Hakonarson H, St George-Hyslop P, Green RC, Goate AM, Foroud TM, Carney RM, Larson EB, Behrens TW, Kauwe JS, Haines JL, Farrer LA, Pericak-Vance MA, Mayeux R, Schellenberg GD; National Institute on Aging-Late-
Onset Alzheimer’s Disease (NIA-LOAD) Family Study, Albert MS, Albin RL, Apostolova LG, Arnold SE, Barber R, Barmada M, Barnes LL, Beach TG, Becker JT, Beecham GW, Beekly D, Bennett DA, Bigio EH, Bird TD, Blacker D, Boeve BF, Bowen JD, Boxer A, Burke JR, Buxbaum JD, Cairns NJ, Cao C, Carlson CS, Carroll SL, Chui HC, Clark DG, Cribbs DH, Crocco EA, DeCarli C, DeKosky ST, Demirci FY, Dick M, Dickson DW, Duara R, Ertekin-Taner N, Fallon KB, Farlow MR, Ferris S, Frosch MP, Galasko DR, Ganguli M, Gearing M, Geschwind DH, Ghetti B, Gilbert JR, Glass JD, Graff-Radford NR, Growdon JH, Hamilton RL, Hamilton-Nelson KL, Harrell LE, Head E, Honig LS, Hulette CM, Hyman BT, Jarvik GP, Jicha GA, Jin LW, Jun G, Jun G, Kamboh MI, Karydas A, Kaye JA, Kim R, Koo EH, Kowall NW, Kramer JH, LaFerla FM, Lah JJ, Leverenz JB, Levey AI, Li G, Lieberman AP, Lopez OL, Lunetta KL, Lyketsos CG, Mack WJ, Marson DC, Martin ER, Martiniuk F, Mash DC, Masliah E, McCormick WC, McCurry SM, McDavid AN, McKee AC, Mesulam WM, Miller BL, Miller CA, Miller JW, Montine TJ, Morris JC, Murrell JR, Olichney JM, Parisi JE, Perry W, Peskind E, Petersen RC, Pierce A, Poon WW, Potter H, Quinn JF, Raj A, Raskind M, Reiman EM, Reisberg B, Reitz C, Ringman JM, Roberson ED, Rosen HJ, Rosenberg RN, Sano M, Saykin AJ, Schneider JA, Schneider LS, Seeley WW, Smith AG, Sonnen JA, Spina S, Stern RA, Tanzi RE, Thornton-Wells TA, Trojanowski JQ, Troncoso JC, Tsuang DW, Van Deerlin VM, Van Eldik LJ, Vardarajan BN, Vinters HV, Vonsattel JP, Weintraub S, Welsh-Bohmer KA, Williamson J, Wishnek S, Woltjer RL, Wright CB, Younkin SG, Yu CE, Yu L. Rarity of the Alzheimer disease-protective APP A673T variant in the United States. JAMA Neurol. 2015;72(2):209-216.
Warren Olanow C, Bartus RT, Baumann TL, Factor S, Boulis N, Stacy M, Turner DA, Marks W, Larson P, Starr PA, Jankovic J, Simpson R, Watts R, Guthrie B, Poston K, Henderson JM, Stern M, Baltuch G, Goetz CG, Herzog C, Kordower JH, Alterman R, Lozano AM, Lang AE. Gene delivery of neurturin to putamen and substantia nigra in Parkinson disease: a double-blind, randomized, controlled trial. Ann Neurol. 2015;78(2):248-257.
Webb AJ, Ullman NL, Morgan TC, Muschelli J, Kornbluth J, Awad IA, Mayo S, Rosenblum M, Ziai W, Zuccarrello M, Aldrich F, John S, Harnof S, Lopez G, Broaddus WC, Wijman C, Vespa P, Bullock R, Haines SJ, Cruz-Flores S, Tuhrim S, Hill MD, Narayan R, Hanley DF; MISTIE and CLEAR Investigators. Accuracy of the ABC/2 score for intracerebral hemorrhage: systematic review and analysis of MISTIE, CLEAR-IVH, and CLEAR III. Stroke. 2015;46(9):2470-2476.
Weinberg RB, Mufson EJ, Counts SE. Evidence for a neuroprotective microRNA pathway in amnestic mild cognitive impairment. Front Neurosci. 2015;9:430.
Westbay LC, Cao L, Burnett-Zeigler I, Reizine N, Barton B, Ippolito D, Weaver FM, Stroupe KT. Mental health-related healthcare use following bilateral deep brain stimulation for Parkinson’s disease. J Parkinsons Dis. 2015;5(3):497-504.
Wilson RS, Boyle PA, James BD, Leurgans SE, Buchman AS, Bennett DA. Negative social interactions and risk of mild cognitive impairment in old age. Neuropsychology. 2015;29(4):561-570.
Wilson RS, Boyle PA, Yang J, James BD, Bennett DA. Early life instruction in foreign language and music and incidence of mild cognitive impairment. Neuropsychology. 2015;29(2):292-302.
Select Publications (2015) 59

Wilson RS, Boyle PA, Yu L, Barnes LL, Sytsma J, Buchman AS, Bennett DA, Schneider JA. Temporal course and pathologic basis of unawareness of memory loss in dementia. Neurology. 2015;85(11):984-991.
Wilson RS, Boyle PA, Yu L, Segawa E, Sytsma J, Bennett DA. Conscientiousness, dementia related pathology, and trajectories of cognitive aging. Psychol Aging. 2015;30(1):74-82.
Wilson RS, Capuano AW, Sytsma J, Bennett DA, Barnes LL. Cognitive aging in older black and white persons. Psychol Aging. 2015;30(2):279-285.
Wong AP, Lall RR, Dahdaleh NS, Lawton CD, Smith ZA, Wong RH, Harvey MJ, Lam S, Koski TR, Fessler RG. Comparison of open and minimally invasive surgery for intradural-extramedullary spine tumors. Neurosurg Focus. 2015;39(2):E11.
Wong AP, Smith ZA, Nixon AT, Lawton CD, Dahdaleh NS, Wong RH, Auffinger B, Lam S, Song JK, Liu JC, Koski TR, Fessler RG. Intraoperative and perioperative complications in minimally invasive transforaminal lumbar interbody fusion: a review of 513 patients. J Neurosurg Spine. 2015;22(5):487-495.
Writing Group for the NINDS Exploratory Trials in Parkinson Disease (NET-PD) Investigators, Kieburtz K, Tilley BC, Elm JJ, Babcock D, Hauser R, Ross GW, Augustine AH, Augustine EU, Aminoff MJ, Bodis-Wollner IG, Boyd J, Cambi F, Chou K, Christine CW, Cines M, Dahodwala N, Derwent L, Dewey RB Jr, Hawthorne K, Houghton DJ, Kamp C, Leehey M, Lew MF, Liang GS, Luo ST, Mari Z, Morgan JC, Parashos S, Pérez A, Petrovitch H, Rajan S, Reichwein S, Roth JT, Schneider JS, Shannon KM, Simon DK, Simuni T, Singer C, Sudarsky L, Tanner CM, Umeh CC, Williams K, Wills AM. Effect of creatine monohydrate on clinical progression in patients with Parkinson disease: a randomized clinical trial. JAMA. 2015;313(6):584-593.
Yan L, Hicks M, Winslow K, Comella C, Ludlow C, Jinnah HA, Rosen AR, Wright L, Galpern WR, Perlmutter JS. Secured web-based video repository for multicenter studies. Parkinsonism Relat Disord. 2015;21(4):366-371.
Yang J, Yu L, Gaiteri C, Srivastava GP, Chibnik LB, Leurgans SE, Schneider JA, Meissner A, De Jager PL, Bennett DA. Association of DNA methylation in the brain with age in older persons is confounded by common neuropathologies. Int J Biochem Cell Biol. 2015;67:58-64.
Yokoyama JS, Sturm VE, Bonham LW, Klein E, Arfanakis K, Yu L, Coppola G, Kramer JH, Bennett DA, Miller BL, Dubal DB. Variation in longevity gene KLOTHO is associated with greater cortical volumes. Ann Clin Transl Neurol. 2015;2(3):215-230.
Yu L, Boyle PA, Leurgans S, Schneider JA, Kryscio RJ, Wilson RS, Bennett DA. Effect of common neuropathologies on progression of late life cognitive impairment. Neurobiol Aging. 2015;36(7):2225-2231.
Yu L, Boyle PA, Nag S, Leurgans S, Buchman AS, Wilson RS, Arvanitakis Z, Farfel JM, De Jager PL, Bennett DA, Schneider JA. APOE and cerebral amyloid angiopathy in community-dwelling older persons. Neurobiol Aging. 2015;36(11):2946-2953.
Yu L, Boyle PA, Segawa E, Leurgans S, Schneider JA, Wilson RS, Bennett DA. Residual decline in cognition after adjustment for common neuropathologic conditions. Neuropsychology. 2015;29(3):335-343.
Yu L, Boyle PA, Wilson RS, Levine SR, Schneider JA, Bennett DA. Purpose in life and cerebral infarcts in community-dwelling older people. Stroke. 2015;46(4):1071-1076.
Yu L, Chibnik LB, Srivastava GP, Pochet N, Yang J, Xu J, Kozubek J, Obholzer N, Leurgans SE, Schneider JA, Meissner A, De Jager PL, Bennett DA. Association of brain DNA methylation in SORL1, ABCA7, HLA-DRB5, SLC24A4, and BIN1 with pathological diagnosis of Alzheimer disease. JAMA Neurol. 2015;72(1):15-24.
Yu L, De Jager PL, Yang J, Trojanowski JQ, Bennett DA, Schneider JA. The TMEM106B locus and TDP-43 pathology in older persons without FTLD. Neurology. 2015;84(9):927-934.
Zhao L, Verhagen-Metman L, Kim JH, Liu CC, Lenz FA. EMG activity and neuronal activity in the internal globus pallidus (GPi) and their interaction are different between hemiballismus and apomorphine induced dyskinesias of Parkinson’s disease (AID). Brain Res. 2015;1603:50-64.
Zhao Z, Sagare AP, Ma Q, Halliday MR, Kong P, Kisler K, Winkler EA, Ramanathan A, Kanekiyo T, Bu G, Owens NC, Rege SV, Si G, Ahuja A, Zhu D, Miller CA, Schneider JA, Maeda M, Maeda T, Sugawara T, Ichida JK, Zlokovic BV. Central role for PICALM in amyloid-β blood-brain barrier transcytosis and clearance. Nat Neurosci. 2015;18(7):978-987. ◆
60 THE 2016 RUSH NEUROSCIENCE REVIEW

Select Research Grants (2015) 61
Select Research Grants (2015)
Department of Neurological Sciences
Neelum Aggarwal, MD
• Community Engagement for Early Recognition and Immediate Action in Stroke (CEERIAS)
• Community-Based End-of-Life Intervention for African American Dementia Caregivers
• Study in Patients With Mild to Moderate Alzheimer’s Disease
Zoe Arvanitakis, MD, MS
• Vascular Cognitive and Motor Decline: Impact of aPL
• Mechanisms Linking Insulin Resistance to Brain Structure, Pathology, and Function
Lisa Barnes Young, PhD
• Risk Factors for Cognitive Decline in African Americans
• Rush Center of Excellence on Disparities in HIV and Aging (CEDHA)
David Bennett, MD
• Epidemiologic Study of Neural Reserve and Neurobiology of Aging
• National Alzheimer’s Coordinating Center
• Risk Factors, Pathology, and Clinical Expressions of Alzheimer’s Disease
• Altered Monocyte Function in Relation to the CD33 Alzheimer’s Disease Locus
• Targeted Proteomics of Resilient Cognition in Aging
• Transcriptional Regulation and Novel Therapeutic Targets for Alzheimer’s Disease
• Neurobiology of Mild Cognitive Impairment in the Elderly
• The Brain Transcriptome and Lifetime Obesity Measures: The Framingham Study
• Development of Lewy Bodies Biofluid Signatures by Targeted Proteomics
• Clinical-Pathological Study of Cognitive Impairment in Essential Tremor
Patricia Boyle, PhD
• Epidemiologic Study of Impaired Decision-Making in Preclinical Alzheimer’s Disease
Aron Buchman, MD
• Brain and Spinal Cord Microvascular Pathology in Late-Life Motor Impairment
• Spinal Cord and Brainstem Pathology Contributions to Late-Life Gait Impairment
• The Clinical Profile of Parkinson’s Disease Pathology
James Conners, MD, MS
• Stroke Trials Network-Regional Coordinating Stroke Centers
Jennifer Goldman, MD
• Assessing Aberrant Motor Learning in Parkinson’s Disease Patients
• Study of Dual Antagonist in Parkinson's Disease Dementia
Diana Goodman, MD
• Futility Study of Deferoxamine Mesylate in Intracerebral Hemorrhage
Deborah Hall, MD, PhD
• RECRUIT: A Randomized Recruitment Intervention
• Adult Neurological Phenotypes of Fragile X Gray Zone Expansion
• Study of Different Doses of Endurance Exercise in People With Parkinson’s Disease
S. Duke Han, PhD
• Neural Correlates of Impaired Financial and Health Care Decision-Making in Old Age
Aikaterini Kompoliti, MD
• Disease Modifying Agent in Patients With Early Parkinson’s Disease
• Group Dosage Study in Subjects With Early Parkinson’s Disease
• Trial for Orally Administered Drug in Subjects With Drug-Induced Tardive Dyskinesia
• Study of SCN-102 in Subjects With Tourette Syndrome
Jeffrey Kordower, PhD
• Preclinical Evaluation of miSCA Expression Vectors for SCA1 Therapy
• Intranasal Delivery of Sponsor’s Molecules to Target Central Nervous System in Nonhuman Primates
George Lopez, MD, PhD
• Dose Escalation Study in Patients With Aneurysmal Subarachnoid Hemorrhage
Elliott Mufson, PhD
• Basic Neuroscience Training in Age-Related Disorders
Daniel Nicholson, PhD
• Proteomic Reconstructive Microscopy of Health and Diseased Dendrites
• Synaptic Mechanisms Maintaining Persistent Cocaine Craving
Kalipada Pahan, PhD
• Cinnamon, Ciliary Neurotrophic Factor (CNTF), and Experimental Autoimmune Encephalomyelitis (EAE)
• RANTES and Eotaxin: New Players in Parkinson’s Disease Progression
Sylvia Perez, PhD
• Neuronal Tangle Propagation in Preclinical Alzheimer’s Disease
Kathleen Shannon, MD
• Investigation of Levodopa Inhalation Powder in Parkinson’s Disease Patients With Motor Response Fluctuations
Julie Schneider, MD
• Epidemiologic Study of TDP-43 Pathology in Aging and Dementia

62 THE 2016 RUSH NEUROSCIENCE REVIEW
Raj Shah, MD
• Integrated Inpatient and Outpatient Care for Patients at High Risk of Hospitalization
• Aspirin in Reducing Events in the Elderly
Sarah Song, MD, MPH
• Mechanisms of Early Recurrence in Intracranial Atherosclerotic Disease (MyRIAD)
Dusan Stefoski, MD
• Safety Registry of Multiple Sclerosis Patients Who Have Participated in Cladribine Clinical Trials
• Impact on Central Nervous System Tissue Damage in Multiple Sclerosis
Leonard Verhagen Metman, MD, PhD
• Implantable Neurostimulator for the Treatment of Parkinson’s Disease
• Evaluation of Extended Release Tablets in Parkinson’s Disease Subjects With Levodopa-Induced Dyskinesias
Dustin Wakeman, PhD
• Transplantation of Cryopreserved Induced Pluripotent Stem Cell (iPSC)-Derived Dopamine Neurons for Parkinson’s Disease
Robert Wilson, PhD
• BAILA: Being Active, Increasing Latinos’ Healthy Aging
Lei Yu, PhD
• Role of Impaired Cognitive States and Risk Factors in Conversion to Mixed Dementia
Department of Neurological Surgery
Richard Byrne, MD
• Cortical Stimulation Mapping Techniques in Brain Tumor Patients
• Brain Tumor Database
• Evaluation of Cognitive Function From Subdural Electrodes in Patients Considered as Surgical Candidates for Intractable Epilepsy
• Predictors of Surgical Corridors to the Suprasellar Space
Michael Chen, MD
• Diffusion Weighted Imaging (DWI) or Computerized Tomography Perfusion (CTP) Assessment With Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention (DAWN) Trial
• Estrogen Therapy as Prevention in the Progression of Aneurysm (EPPA) Trial
• Post-Aneurysm Subarachnoid Hemorrhage Memory Loss
Harel Deutsch, MD
• LIFT: Lumbar Interbody Fusion Trial
• Safety and Efficacy of Staphylococcus Aureus Vaccine in Adults Undergoing Elective Posterior Instrumented Lumbar Spinal Fusion Procedures
Richard Fessler, MD, PhD
• Asterias Stem Cell Treatment for Spinal Cord Injury
• Minimally Invasive Surgery for the Treatment of Adult Spinal Deformity: A Multicenter Retrospective Study
Demetrius Lopes, MD
• ACE: An Aneurysm Coiling Efficiency Study of the Penumbra Coil 400 System
• Adjunctive Neurovascular Support for Wide-Neck Aneurysm Embolization and Reconstruction (ANSWER) Study
• FRED: Flow Re-Direction Endoluminal Device: Pivotal Study of the MicroVention Flow Re-Direction Endolumincal Device Stent System in the Treatment of Intracranial Aneurysms
• LVIS: Pivotal Study of MicroVention, Inc. Neurovascular Self-Expanding Retrievable Stent System in the Treatment of Wide-Necked Intracranial Artery Aneurysms
• MicroVention Low-Profile Visualized Intraluminal Support (LVIS) or LVIS Jr Humanitarian Use Device
• PREMIER Prospective Study on Embolization of Intracranial Aneurysms With Pipeline Embolization Device
• Safety and Effectiveness of the Treatment of Wide-Neck, Saccular Intracranial Aneurysms With the Neuroform Atlas Stent System
• Solitaire FR With the Intention for Thrombectomy as Primary Endovascular Treatment for Acute Ischemic Stroke (SWIFT PRIME)
• The Surpass IntraCranial Aneurysm Embolization System Pivotal Trial to Treat Large or Giant Wide-Neck Aneurysms (SCENT)
Lorenzo Muñoz, MD
• MISTIE Trial: tPA for Intracerebral Hemorrhage
John O’Toole, MD, MS
• Os Odontoideum in Adults
Sepehr Sani, MD
• High Order Spectral Analysis of Local Field Potential Data in Parkinson’s Disease
• Reclaim Deep Brain Stimulation for Obsessive Compulsive Disorder (OCD) Therapy
• Temporal Lobectomy, Memory, Sleep, and Dreams
Vincent Traynelis, MD
• Assessment of Perioperative Morbidity and Mortality Following Anterior-Posterior Cervical Spine Decompression and Fusion
• Cervical Retraction Study
• Clinical and Radiological Analysis Following Multilevel Anterior or Posterior Cervical Fusion
• Critical Analysis of Extubation Parameters for Patients Undergoing Combined Anterior-Posterior Cervical Spine Surgery ◆

Legacy Interview: Offering the Best Service 63
General neurologist Jacob Fox, MD, recently retired after 26 years as chairperson of the Department of Neurological
Sciences at Rush University Medical Center. During that time, the department sustained tremendous growth, all
while continuing to provide excellent clinical care to patients.
Jacob, or “Jack” to his friends and colleagues, Fox devoted much of his career to the study and treatment of
Alzheimer’s disease, for which he was honored by both the Chicago chapter of the Alzheimer’s Association and the
National Alzheimer’s Association.
Fox recently sat down with fellow general neurologist Allison Weathers, MD, to discuss changes in the field of
neurology, becoming a chairperson at an academic medical center, and why “legacy” isn’t something this interview
should even be called.
Weathers: What were the influences that led you to become a neurologist?
Fox: When I was in medical school, I really wasn’t interested in anything else. Among the various possibilities, neurology seemed the most interesting, but I doubt I decided until I was a senior medical student. The one thing I knew was that I didn’t care to do surgery. So the limitations would therefore have been something in internal medicine, psychiatry, or neurology.
Weathers: Once you decided on neurology, what drew you to study Alzheimer’s disease and dementia? How did you end up specializing?
Fox: It was purely happenstance. When I was in the military I was stationed at Fort Belfort in northern Virginia. Of course the military then took care of both active duty and retired, and there were many retired military there. After my residency, I accepted a job as the chief of neurology at
LEGACY INTERVIEW: OFFERING THE BEST SERVICE
General neurologists Allison Weathers, MD (left) and Jacob Fox, MD.

64 THE 2016 RUSH NEUROSCIENCE REVIEW
DeWitt Army Hospital in Belvoir, Virginia, and I saw a lot of patients there with cognitive dysfunction.
When I came back to Chicago in the early 70s, I took a faculty position at Rush and established my private practice where I just started seeing more patients who had dementia. And as you know, the idea that this dementia was Alzheimer’s was something that evolved in clarity through the 70s and early 80s.
But I would say basically I’m a general neurologist. I have always seen everything, except for a period of time shortly after I became chairperson when my clinical time was limited and I was seeing only patients with dementia in the Rush Alzheimer’s Disease Center.
And how that happened was I had the busiest Alzheimer practice, I guess you could say, in the area, as a private practitioner. When Rush decided to open the Alzheimer’s Disease Center in the mid-80s, they asked me to participate as co-director because I brought all of the patients.
Weathers: So you didn’t ever consider other subspecialties?
Fox: No, I’m not nearly as well thought out as that.
On changes in neurology over the last 20-plus years
Weathers: You spoke about it a little bit before, that there wasn’t even this realization then that the condition was Alzheimer’s. What do you think are the other really significant differences between the care of patients with neurological conditions now compared to the beginning of your career and your practice?
Fox: Unfortunately very little. It’s very discouraging. The treatment of Parkinson’s disease has improved since the availability of L-dopa, which was available when I finished my residency but not yet widely available and in use.
Headache: not all that much, really. Neuromuscular disease? Actually, during my residency was when it became clear that patients with myasthenia gravis benefited so much from steroids. And those patients do so much better than they did, let’s say, in the 40s or 50s.
But in the last couple of decades, I’d say the big things in stroke are first, the use of antiplatelets to prevent stroke, and then tPA to treat it. And particularly the recent advance of doing invasive vascular treatment of major internal carotid and proximal middle cerebral artery strokes: I think that’s just amazing. If you had asked me 30 years ago if I was going to be seeing people with major strokes really be helped a lot? I don’t think I would have said yes. That’s been unbelievable.
And actually the other thing that I really think is quite amazing is the treatment of patients with multiple sclerosis.
Weathers: I was thinking that.
Fox: Yeah, because I know from the early part of my career—of course I took care of hundreds of MS patients—and the fact was that their natural history was determined by their natural history, not by anything I did. And now you can see—whatever the side effects are—drugs like natalizumab really alter the natural history. So improvements in the treatment of stroke and MS in the last couple of decades I think have been truly remarkable and gratifying.
And, of course, neurointensive care didn’t exist when I first started my practice. I’m not sure how much data there is regarding how much better off the patients are in the more formalized neurointensive care compared to the way that it was done before. Undoubtedly they are better off, but I’m not sure there are studies that have been verified.
Weathers: Some interventions, such as with cooling, certainly there are strides.
Fox: Well, yes, but that’s very slight.
Weathers: Yes, I know.
Fox: I mean, discouraging, slight, but something. There are a lot of areas where you can say there’s something.
Weathers: There’s something.
Fox: But I think neurointensive care is certainly the next frontier as far as demonstrating that some of the interventions neurointensivists do really have efficacy in altering the natural history. The clinicians have to do them. And I think

Legacy Interview: Offering the Best Service 65
they should. But how one is going to demonstrate efficacy, I think, is challenging.
Weathers: Going back to Alzheimer’s and how you said it’s discouraging that things aren’t that much different. What do you think are the most important areas for future researchers to be focusing on for the treatment and care?
Fox: For sure, biology. The chemistry, the biology: That’s where it’s at. Now whether any of the things that are being planned regarding diminishing amyloid early on in the course of the pathology progression, whether they’re actually going to have efficacy or not, I think remains to be proven. There seem to be some very good studies in progress.
But, I should clarify, when I said I don’t think the care of Alzheimer’s patients has improved, I mean care provided by physicians. I think the recognition of the illness has been beneficial for the patients, for the families, and for how one deals with issues surrounding the disease. And it’s not that physicians have nothing to contribute to those patients; they just aren’t able to do anything to alter the natural history of the disease.
On life as a chairperson at an academic medical center
Weathers: About what you’ve accomplished in your tenure as chair, one of the most notable things is how our volume has grown, the size of our practice.
Fox: It’s exciting.
Weathers: It is. What do you think has contributed to that growth and to sustaining such a successful neurological sciences program?
Fox: We have the best doctors offering the best service. And that’s it. Nothing else. And to the extent that I’ve made any contribution to that is by trying to recruit the best doctors, and by trying to put them in a situation where they can offer the best service.
And by the way, the volumes are astonishing because I figured them out for FY15. We had almost 2900 admissions, and the next closest academic center to us in the area had 1900. I mean, the difference is amazing. And the other academic centers in the area had around 1300. We’re seeing almost 500 new patients per month, which is more than are seen by all of the neurologists in Scotland, as I always point out.
I really do think it’s the best doctors offering the best service. And of course, the best service has to include the opportunity to use the most advanced treatments. So I’ll use as an example—not because it’s the only example, but it’s an
obvious recent one—the idea of TeleStroke leading to prompt treatment of patients who are then candidates to get intravascular treatment that has to be done within 6 hours.
In these cases, that better service is even more important. The patients have to be handled quickly and efficiently so that they’re in a position to benefit from that treatment. And that’s very complicated. And that’s not me. That’s a whole group of people who are doing that. My own personal satisfaction is that I’ve allowed them the opportunity to do it, and they’re in a situation where they can.
Weathers: But I think your leadership and your ability to provide those opportunities is what facilitated that.
Fox: I hope so. But again, remember the other aspect of my leadership is I don’t interfere, and I’m not controlling. Being noncontrolling only works if you have very good people. So therefore, having the good people and then helping them do what they know is best is key. I mean, do I know anything about implementing TeleStroke? No. The fact is, okay, I’ve been able to facilitate that. But that’s the key thing: Letting clinicians do the things that they do so well, efficiently. And give good service to the patients.

66 THE 2016 RUSH NEUROSCIENCE REVIEW
Weathers: You’ve been here for many years and held many different positions at Rush. Not only chairperson for neurological sciences, but provost, and medical staff president. What has kept you here all these years?
Fox: I like seeing patients and teaching. And I like the people I work with. And Rush is a good place to do those things. As chairperson, I’ve been given an opportunity that I wouldn’t have normally expected with my own background. I’d simply be in private practice. Being able to facilitate some of these advances, like TeleStroke that I mentioned before, has been gratifying. So that’s been an additional opportunity for me, for which I consider myself very lucky.
Weathers: You and I have talked about that before. I think it’s interesting how you feel that your path was unique, and it wouldn’t happen again today.
Fox: I think it’s definitely possible for somebody in private practice to go into academics, but people in private practice are not often considered for chairperson positions in academic institutions. You know, I often say that I happened to be walking on a roof, and a hole opened up, and I landed in the chair.
I think people who are primarily clinicians and teachers can end up in charge of large groups of neurologists, but the nature of the academic selection process now is that they’re not the people who are necessarily selected to be chairperson. So, I consider myself particularly lucky in that regard.
On advice for future neurologists
Weathers: Along those lines, what are the biggest challenges you see for future neurologists and trainees who would like to follow in your footsteps?
Fox: I think the main thing is they should not be diverted by all of the things that administration, etcetera, are saying are so important like affiliating with other hospitals. My own
opinion is each individual physician has to concentrate exclusively on being the best physician, giving the best service he or she can.
Unless they get into some sort of administrative job, that’s what they should be thinking about. And to the extent they’re diverted from concentrating on being the best physician he or she can be, it’s not beneficial. It’s our job to offer services like TeleStroke or 2-BRAIN [a direct physician transfer service] because that’s what we do.
To the younger physicians, my advice is always the same: Pay much more attention to the history and the physical, and don’t concentrate on the imaging. Not because that’s the only thing we old people used to have for diagnoses, but because that’s how you do the best job as a neurologist. You concentrate on the history and physical, and then you do the imaging to support your suspected diagnosis. That’s what I say all the time to the younger doctors. But I’m not sure they’re really convinced.
Weathers: What would you like your legacy to be?
Fox: This word “legacy” doesn’t mean a thing to me. Honestly, it’s like, if you would ask me, what do you want your legacy to be to your daughter, what does that mean? What I want for my children and grandchildren—my own biological children and grandchildren—is for them to be happy and successful. That’s what I want for our department as well. I want our faculty to continue to be happy and successful. I don’t look at that at all as a legacy.
I want our department to continue to be composed of the best doctors giving the best service. If the department declines after I leave, it will be devastating to me, devastating. Because I truly look at our faculty as my professional family. And therefore, I want for our faculty professionally what I want for my own family personally: I want them to be happy and successful.
Weathers: I talk about that in each residency applicant interview. With every program they say, “What makes your program unique?” And I say, not only are we world-class clinically, but we’re a family.
Fox: Uh huh.
Weathers: And you feel it in everything we do here.
Fox: Yes. And so this legacy stuff—it’s not a word in my lexicon. ◆

For a patient consultation or referral to a neurologist at Rush, please call (312) 942-4500.
For a neurosurgeon at Rush, call (312) 942-6644.
RUSH’S HOSPITAL: DESIGNED AROUND THE PATIENT Rush’s hospital transforms medicine by focusing on one key element: quality patient care. That's why hundreds of doctors, nurses, and other
clinicians, with input from patients and families, worked with architects to design our state-of-the-art hospital Tower. One of the nation's most advanced
hospitals, the hospital houses acute and critical care patients, as well as technologically sophisticated surgical, diagnostic, and therapeutic services.

Rush is a not-for-profit health care, education and research enterprise comprisingRush University Medical Center, Rush University, Rush Oak Park Hospital and Rush Health.
PLEASE NOTE: All physicians featured in this publication are on the medical faculty of Rush University Medical Center. Some of the physicians featured are in private practice and, as
independent practitioners, are not agents or employees of Rush University Medical Center.
Rush University Medical Center1653 W. Congress Pkwy.
Chicago, IL 60612 www.rush.edu
M-4361 8/16
Cover art: Self Reflected 22K gilded microetching under white light
96" x 133", 2014–2016Greg Dunn and Brian Edwards
Photo credit: Greg Dunn and Will Drinker
Photography by the Rush Photo Group and Kevin Horan







![Sepehr Assadi Sanjeev Khanna arXiv:1801.02793v2 [cs.DS] 23 …sanjeev/papers/soda2018... · 2018. 10. 2. · Sepehr Assadi∗ Sanjeev Khanna∗ Abstract We study the maximum k-set](https://img.pdfslide.us/doc/110x75/60b5594d37c7d1323e717f0d/sepehr-assadi-sanjeev-khanna-arxiv180102793v2-csds-23-sanjeevpaperssoda2018.jpg)