Embed Size (px)
Citation preview
This handbook contains general guidelines for use in common patient care situations that occur in the PICU.
- Always discuss specific patient care issues with the PICU fellow or attending - Always communicate changes in a patient’s status or plan with the fellow,
attending, and all services involved. PAGER / PHONE NUMBERS PICU Attending: 970-1904 / 613-5938 PICU Fellow: 970-6566 / 613-5935 PICU Resident: 613-5940 PICU NP: 970-4636 / 613-5939 PICU Charge Nurse: 812-9078 RT Team Lead: 812-6931 PCICU Attending: 970-1504 / 613-9721 PCICU Fellow: 970-2501 / 613-9723 PCICU NP: 970-7383 / 613-9722 For Code Team, Emergency Airway, Rapid Response Team: call 115 SBAR: to standardize communication S- Situation State name and reason to call B- Background State brief history of problems with pertinent information A- Assessment State your assessment R- Recommendation State your recommendations

1
TABLE OF CONTENTS Resuscitation PALS Algorithms Respiratory Airway / Intubation Mechanical Ventilation Ventilator Modes Ventilator Management Acute Respiratory Distress Syndrome High Frequency Oscillatory Ventilation High Frequency Jet Ventilation Asthma Care Map Cardiovascular Oxygen Delivery Shock Inotropes Antihypertensives / Antiarrhythmics Congenital Heart Disease Hypoplastic Left Heart ECMO Nutrition
Feeding Guidelines Ketogenic Diet Electrolytes Hypo/Hyperkalemia Hypo/Hypernatremia Hypoglycemia Endocrine DKA Endocrine Emergencies Infectious Disease Sepsis Antibiotics Hematology Anticoagulation Therapy Neurology Sedation and analgesia Status Epilepticus Closed Head Injury / Neuroprotection Guidelines Pediatric Brain Death Criteria Formulas and Notes
2
PALS / RESUSCITATION
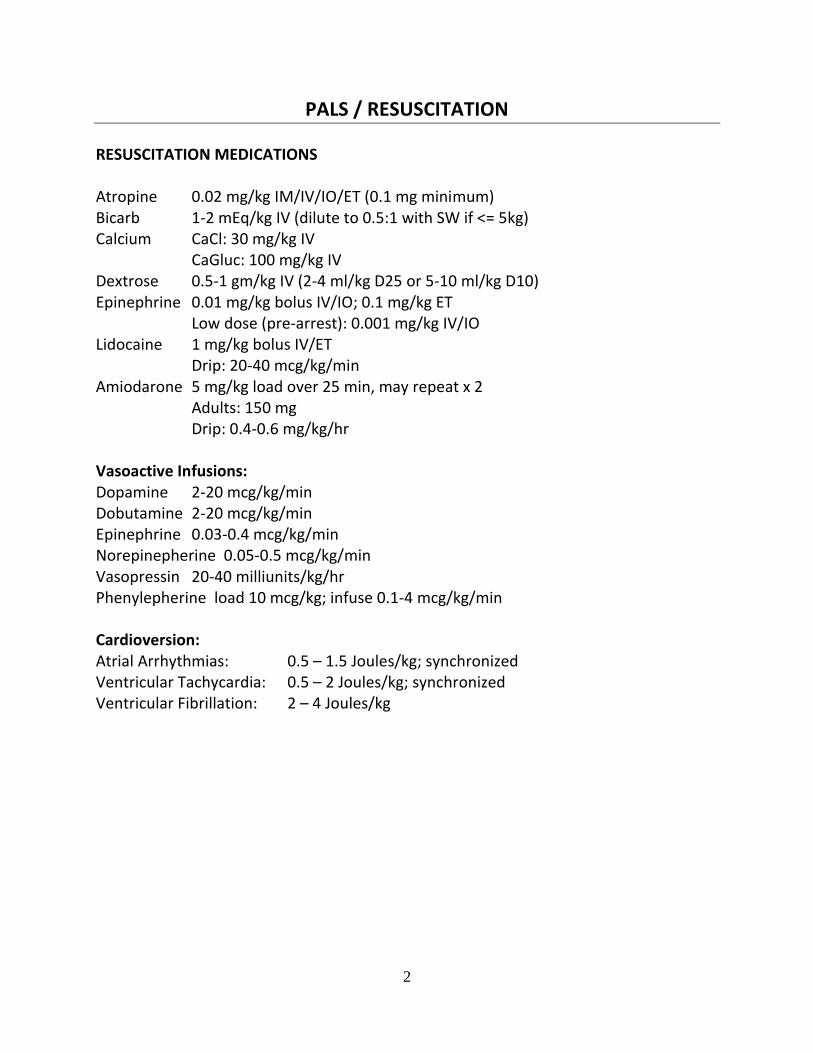
RESUSCITATION MEDICATIONS Atropine 0.02 mg/kg IM/IV/IO/ET (0.1 mg minimum) Bicarb 1-2 mEq/kg IV (dilute to 0.5:1 with SW if <= 5kg) Calcium CaCl: 30 mg/kg IV CaGluc: 100 mg/kg IV Dextrose 0.5-1 gm/kg IV (2-4 ml/kg D25 or 5-10 ml/kg D10) Epinephrine 0.01 mg/kg bolus IV/IO; 0.1 mg/kg ET Low dose (pre-arrest): 0.001 mg/kg IV/IO Lidocaine 1 mg/kg bolus IV/ET Drip: 20-40 mcg/kg/min Amiodarone 5 mg/kg load over 25 min, may repeat x 2 Adults: 150 mg Drip: 0.4-0.6 mg/kg/hr Vasoactive Infusions: Dopamine 2-20 mcg/kg/min Dobutamine 2-20 mcg/kg/min Epinephrine 0.03-0.4 mcg/kg/min Norepinepherine 0.05-0.5 mcg/kg/min Vasopressin 20-40 milliunits/kg/hr Phenylepherine load 10 mcg/kg; infuse 0.1-4 mcg/kg/min Cardioversion: Atrial Arrhythmias: 0.5 – 1.5 Joules/kg; synchronized Ventricular Tachycardia: 0.5 – 2 Joules/kg; synchronized Ventricular Fibrillation: 2 – 4 Joules/kg

3
ASYSTOLE / PULSELESS ARREST
CPR Oxygen
CR monitor
CPR 2 min IV/IO access
Epinephrine q 3min
Pulse check
If pulse → post arrest care
No pulse → resume Asystole / PEA algorithm
Rhythm shockable?
Yes
Yes
Shock
No
VF/VT Asystole/PEA
CPR 2 min IV/IO access
Rhythm shockable?
Rhythm shockable?
Shock
CPR 2 min Treat reversible causes
Yes Shock
CPR 2 min Epinephrine q 3min
CPR 2 min Amiodarone
Treat reversible causes
Rhythm shockable?
Yes
Yes
No
No
Rhythm shockable?
No
No
4
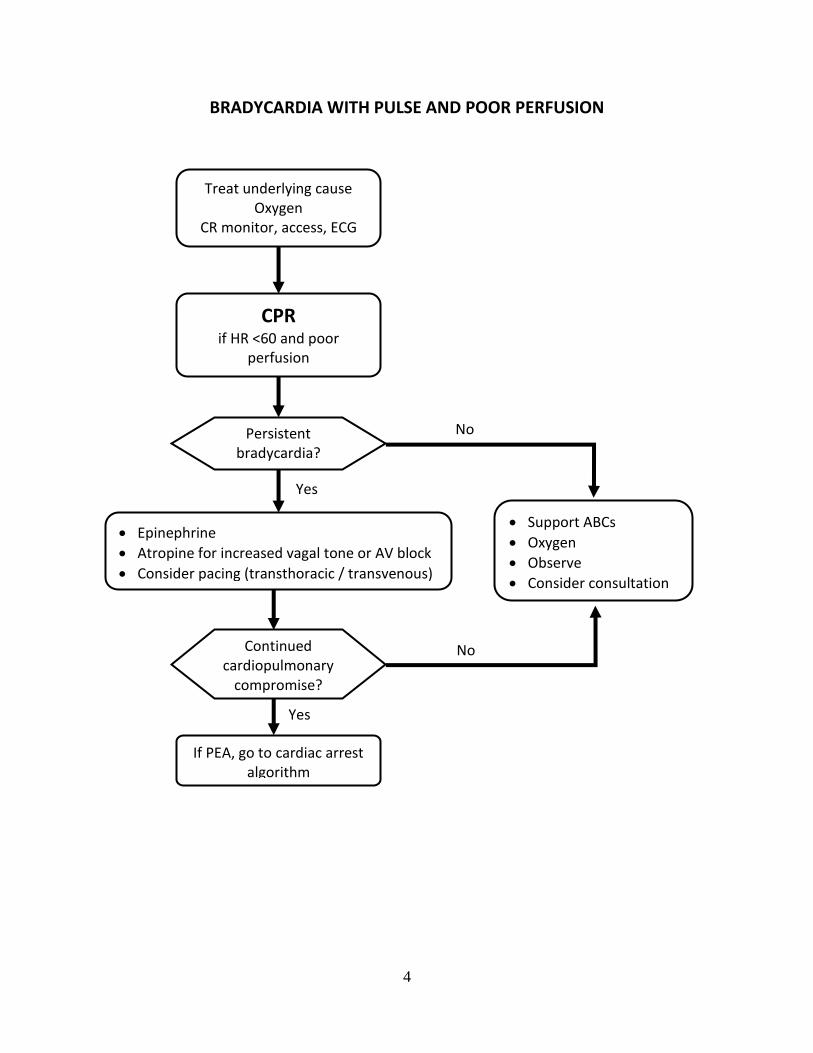
BRADYCARDIA WITH PULSE AND POOR PERFUSION
Treat underlying cause Oxygen
CR monitor, access, ECG
Continued cardiopulmonary
compromise?
CPR if HR <60 and poor
perfusion
Epinephrine
Atropine for increased vagal tone or AV block
Consider pacing (transthoracic / transvenous)
If PEA, go to cardiac arrest algorithm
Persistent bradycardia?
Support ABCs
Oxygen
Observe
Consider consultation
Yes
Yes
No
No
5
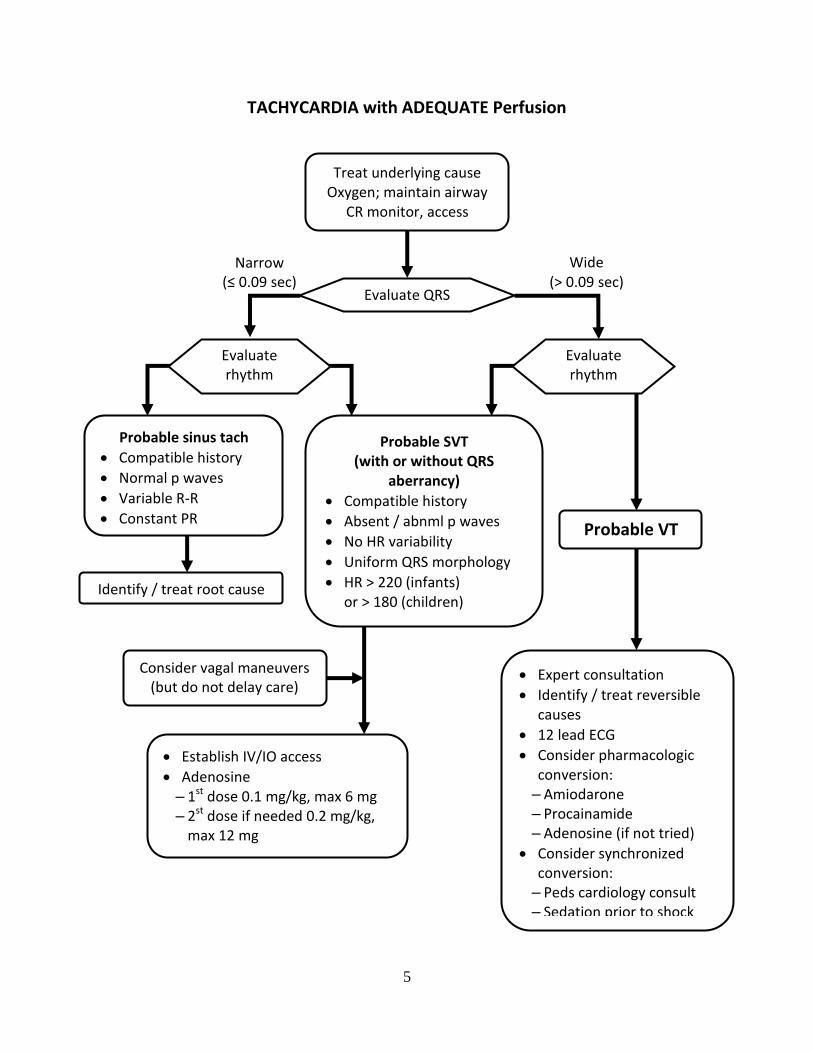
TACHYCARDIA with ADEQUATE Perfusion
Treat underlying cause Oxygen; maintain airway
CR monitor, access
Probable VT
Establish IV/IO access
Adenosine – 1st dose 0.1 mg/kg, max 6 mg – 2st dose if needed 0.2 mg/kg,
max 12 mg
Identify / treat root cause
Evaluate QRS
Probable sinus tach
Compatible history
Normal p waves
Variable R-R
Constant PR
Narrow (≤ 0.09 sec)
Evaluate rhythm
Wide (> 0.09 sec)
Probable SVT (with or without QRS
aberrancy)
Compatible history
Absent / abnml p waves
No HR variability
Uniform QRS morphology
HR > 220 (infants) or > 180 (children)
Consider vagal maneuvers (but do not delay care)
Expert consultation
Identify / treat reversible causes
12 lead ECG
Consider pharmacologic conversion: – Amiodarone – Procainamide – Adenosine (if not tried)
Consider synchronized conversion: – Peds cardiology consult – Sedation prior to shock
Evaluate rhythm

6
TACHYCARDIA with POOR Perfusion
Treat underlying cause Oxygen; maintain airway
CR monitor, access
Possible VT
IV/IO access → adenosine
No access or adenosine ineffective → synchronized cardioversion
Identify / treat root cause
Evaluate QRS
Probable sinus tach
Compatible history
Normal p waves
Variable R-R
Constant PR
Yes
Narrow (≤ 0.09 sec)
No
12 lead ECG
Wide (> 0.09 sec)
Probable SVT
Compatible history
Absent / abnormal p waves
No HR variability
HR > 220 (infants) or > 180 (children)
Cardiopulmonary compromise?
Synchronized cardioversion Consider vagal maneuvers (but do not delay care)
Consider adenosine if regular rhythm and monomorphic QRS
Expert consultation
Amiodarone
Procainamide
7
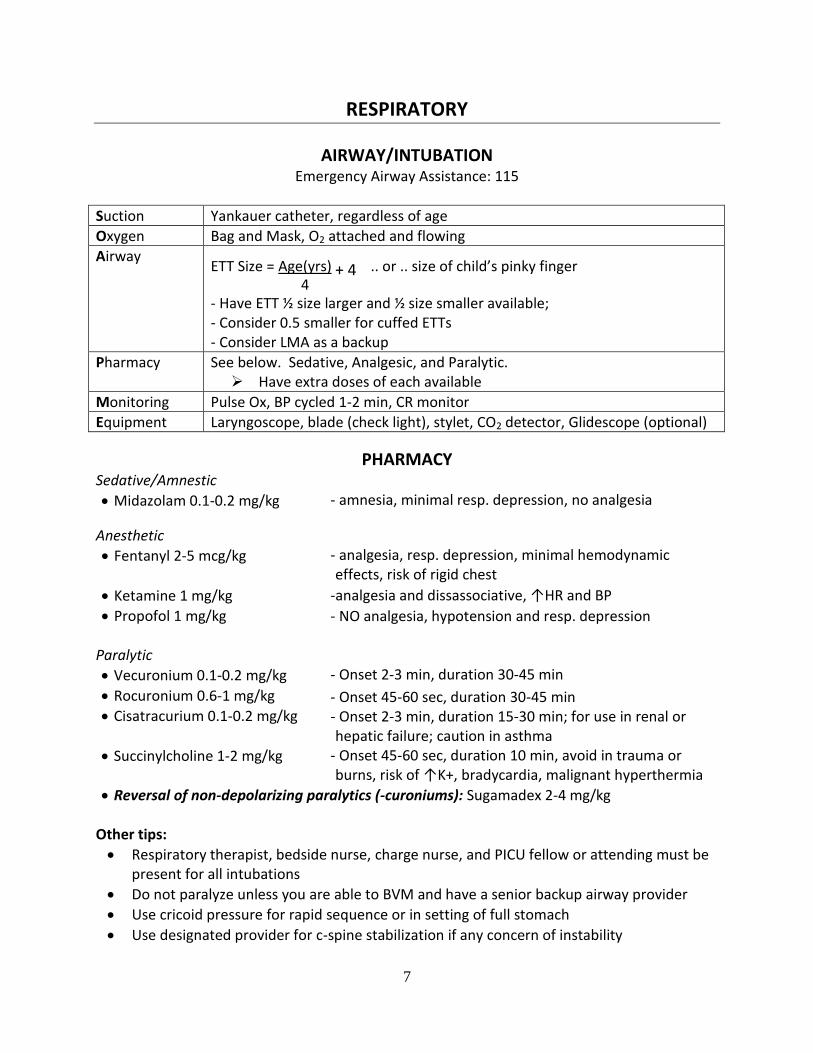
RESPIRATORY
AIRWAY/INTUBATION
Emergency Airway Assistance: 115
Suction Yankauer catheter, regardless of age
Oxygen Bag and Mask, O2 attached and flowing
Airway ETT Size = Age(yrs) + 4 .. or .. size of child’s pinky finger 4 - Have ETT ½ size larger and ½ size smaller available; - Consider 0.5 smaller for cuffed ETTs - Consider LMA as a backup
Pharmacy See below. Sedative, Analgesic, and Paralytic. Have extra doses of each available
Monitoring Pulse Ox, BP cycled 1-2 min, CR monitor
Equipment Laryngoscope, blade (check light), stylet, CO2 detector, Glidescope (optional)
PHARMACY Sedative/Amnestic
Midazolam 0.1-0.2 mg/kg - amnesia, minimal resp. depression, no analgesia
Anesthetic
Fentanyl 2-5 mcg/kg
Ketamine 1 mg/kg
Propofol 1 mg/kg
- analgesia, resp. depression, minimal hemodynamic effects, risk of rigid chest
-analgesia and dissassociative, ↑HR and BP
- NO analgesia, hypotension and resp. depression Paralytic
Vecuronium 0.1-0.2 mg/kg
Rocuronium 0.6-1 mg/kg
Cisatracurium 0.1-0.2 mg/kg
Succinylcholine 1-2 mg/kg
- Onset 2-3 min, duration 30-45 min
- Onset 45-60 sec, duration 30-45 min - Onset 2-3 min, duration 15-30 min; for use in renal or hepatic failure; caution in asthma
- Onset 45-60 sec, duration 10 min, avoid in trauma or burns, risk of ↑K+, bradycardia, malignant hyperthermia
Reversal of non-depolarizing paralytics (-curoniums): Sugamadex 2-4 mg/kg Other tips:
Respiratory therapist, bedside nurse, charge nurse, and PICU fellow or attending must be present for all intubations
Do not paralyze unless you are able to BVM and have a senior backup airway provider
Use cricoid pressure for rapid sequence or in setting of full stomach
Use designated provider for c-spine stabilization if any concern of instability
8
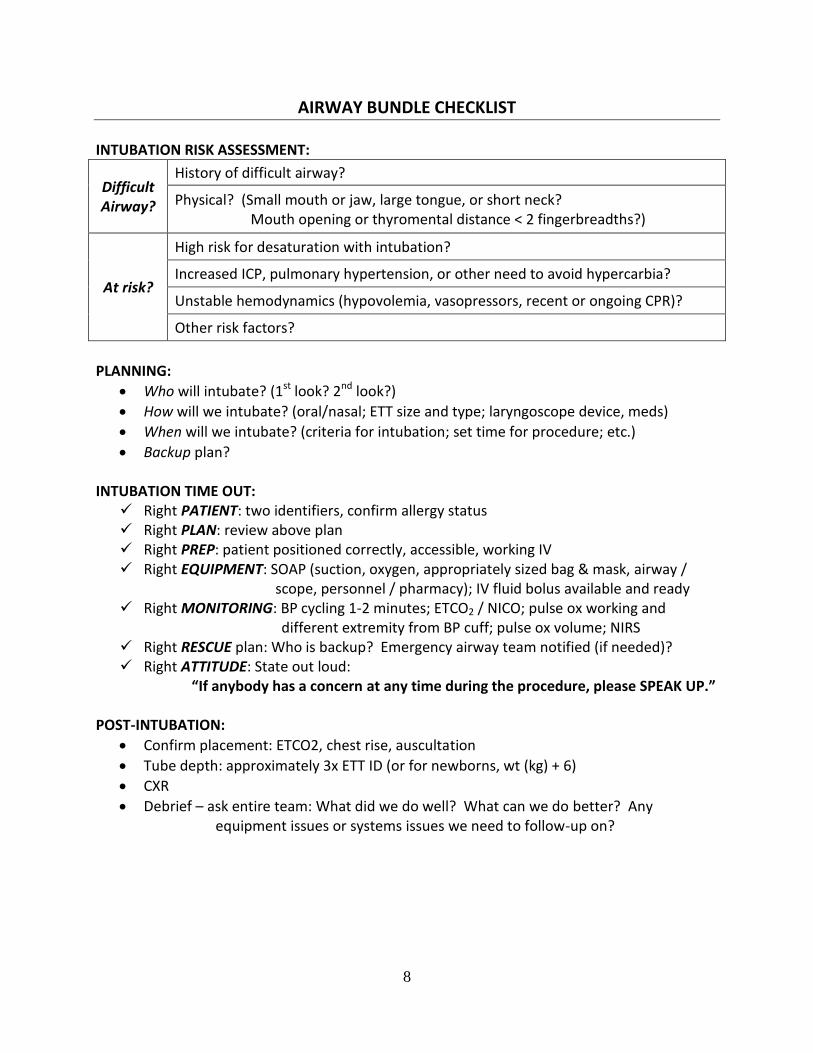
AIRWAY BUNDLE CHECKLIST
INTUBATION RISK ASSESSMENT:
Difficult Airway?
History of difficult airway?
Physical? (Small mouth or jaw, large tongue, or short neck? Mouth opening or thyromental distance < 2 fingerbreadths?)
At risk?
High risk for desaturation with intubation?
Increased ICP, pulmonary hypertension, or other need to avoid hypercarbia?
Unstable hemodynamics (hypovolemia, vasopressors, recent or ongoing CPR)?
Other risk factors?
PLANNING:
Who will intubate? (1st look? 2nd look?)
How will we intubate? (oral/nasal; ETT size and type; laryngoscope device, meds)
When will we intubate? (criteria for intubation; set time for procedure; etc.)
Backup plan? INTUBATION TIME OUT:
Right PATIENT: two identifiers, confirm allergy status Right PLAN: review above plan Right PREP: patient positioned correctly, accessible, working IV Right EQUIPMENT: SOAP (suction, oxygen, appropriately sized bag & mask, airway /
scope, personnel / pharmacy); IV fluid bolus available and ready Right MONITORING: BP cycling 1-2 minutes; ETCO2 / NICO; pulse ox working and
different extremity from BP cuff; pulse ox volume; NIRS Right RESCUE plan: Who is backup? Emergency airway team notified (if needed)? Right ATTITUDE: State out loud:
“If anybody has a concern at any time during the procedure, please SPEAK UP.”
POST-INTUBATION:
Confirm placement: ETCO2, chest rise, auscultation
Tube depth: approximately 3x ETT ID (or for newborns, wt (kg) + 6)
CXR
Debrief – ask entire team: What did we do well? What can we do better? Any equipment issues or systems issues we need to follow-up on?
9
VENTILATOR BASICS
Settings: Trigger: What starts the breath (flow, pressure, or time) Flow: How the air flows into the patient (constant, decelerating) Limit: What ends inspiration (a set pressure or volume) Cycle: What starts exhalation (inspiratory time or flow in circuit) FiO2: Fraction of inspired O2 (amount of O2 delivered to alveoli) PEEP: Positive End Expiratory Pressure, maintains lung recruitment
Oxygenation is dependent on mean airway pressure (MAP) & FiO2
MAP driven primarily by PEEP
Ventilation is dependent on minute ventilation (MV)
MV = tidal volume (Vt) X respiratory rate (IMV)
Monitoring:
CXR to confirm tube position (daily or upon admission to unit)
Ventilator graphics can monitor hypo- or hyperinflation, synchrony, air-trapping, airway resistance, auto-triggering, etc.
Oxygenation monitoring with pulse ox (SpO2) or NIRS (venous sats)
NICO monitor shows:
Vt (typical goal 5-8 ml/kg)
ETCO2 (end-tidal CO2, surrogate measure of paCO2)
Vd/Vt (dead space ratio, ideally < 0.5-0.65 for extubation)
Airway resistance
Volumetric CO2 (a surrogate for pulmonary blood flow)
Vent Management Protocol:
Appropriate for most ventilated children in the PICU, provides consistency of practice and optimizes timely care
Requires physician order
Clinical goals:
Maintain PIP ≤ 30 cm H2O with target Vt 5-8 ml/kg
Maintain arterial pH 7.25-7.45 and pCO2 35-55 mmHg
Maintain SpO2 ≥ 92%
10
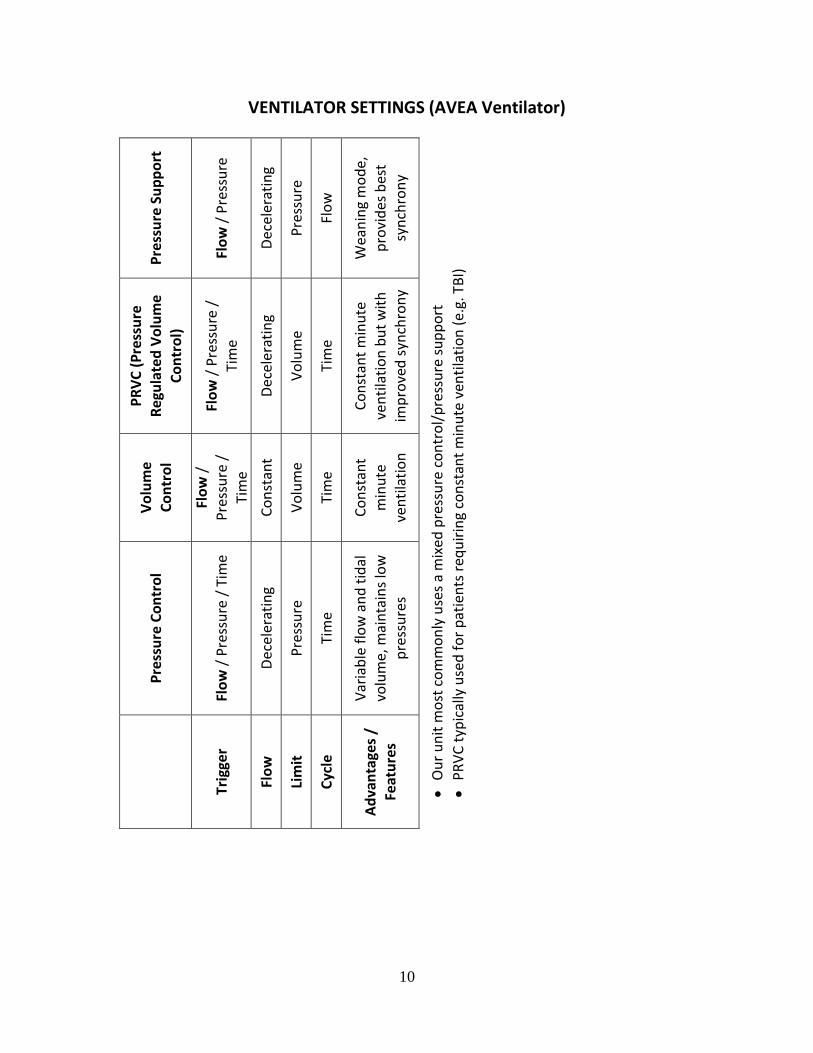
VENTILATOR SETTINGS (AVEA Ventilator)
Pre
ssu
re S
up
po
rt
Flo
w /
Pre
ssu
re
Dec
eler
atin
g
Pre
ssu
re
Flo
w
Wea
nin
g m
od
e,
pro
vid
es b
est
syn
chro
ny
Ou
r u
nit
mo
st c
om
mo
nly
use
s a
mix
ed p
ress
ure
co
ntr
ol/
pre
ssu
re s
up
po
rt
PR
VC
typ
ical
ly u
sed
fo
r p
atie
nts
req
uir
ing
con
stan
t m
inu
te v
enti
lati
on
(e.
g. T
BI)
PR
VC
(P
ress
ure
R
egu
late
d V
olu
me
Co
ntr
ol)
Flo
w /
Pre
ssu
re /
Tim
e
Dec
eler
atin
g
Vo
lum
e
Tim
e
Co
nst
ant
min
ute
ven
tila
tio
n b
ut
wit
h
imp
rove
d s
ynch
ron
y
Vo
lum
e C
on
tro
l
Flo
w /
P
ress
ure
/
Tim
e
Co
nst
ant
Vo
lum
e
Tim
e
Co
nst
ant
min
ute
ve
nti
lati
on
Pre
ssu
re C
on
tro
l
Flo
w /
Pre
ssu
re /
Tim
e
Dec
eler
atin
g
Pre
ssu
re
Tim
e
Var
iab
le f
low
an
d t
idal
volu
me,
mai
nta
ins
low
p
ress
ure
s
Trig
ger
Flo
w
Lim
it
Cyc
le
Ad
van
tage
s /
Feat
ure
s
11
VENTILATOR MANAGEMENT / TROUBLESHOOTING Initial Settings:
FiO2 1.0
PEEP 5-7 cm H2O
PIP to achieve Vt 5-8 ml/kg
RR 15-25
Inspiratory time 0.4-0.7 sec (infant) to 0.7-1.2 (adult) Hypoxia:
R to L Cardiac Shunt: ↑ cardiac output, ↑ Hgb, ↑ pulmonary blood flow (↓ PVR, ↑ RV fxn)
V/Q mismatch: Optimize PEEP, Recruitment maneuver?
Alveolar Hypoventilation: ↑ RR, ↑ Vt,↑ FiO2 Hypercapnia:
Bronchospasm: bronchodilators, consider ↓ RR (ensure full exhalation), ? sedation
V/Q mismatch: optimize PEEP
Mechanical obstruction: assess for ETT obstruction, suction patient, ↑ PEEP
Alveolar hypoventilation: ↑ RR, ↑ Vt Weaning:
If SaO2 ≥ 92%, consider weaning FiO2, PEEP
If PaCO2 ≤ 50 mmHg, consider weaning rate, PIP to keep Vt 5-8 ml/kg Extubation criteria:
PIP ≤ 24 PEEP ≤ 5 Rate ≤ 10 FiO2 ≤ 0.4 Vd/Vt ≤ 0.6 Passed ERT Awake (i.e. sedation
infusions off ~ 4hrs)
Extubation Readiness Trial (ERT)
Trial of minimal pressure support (per ETT size) on PEEP of 5 mmHg performed daily for all patients meeting criteria. Monitor for saturations, tachypnea, and work of breathing to assess extubation likelihood of success.
12
ACUTE RESPIRATORY DISTRESS SYNDROME / LUNG PROTECTIVE VENTILATION
Syndrome of diffuse inflammation, endothelial cell injury, permeability
Characterized by acute onset, infiltrates on CXR, no LA pressure Clinically:
Pulmonary edema
↓ Lung compliance
Hypoxemia
Heterogeneous opacities on CXR Continuum of injury (PALICC criteria for PARDS)
Mild ARDS = 4 ≤ OI < 8 or 5 ≤ OSI < 7.5
Moderate ARDS = 8 ≤ OI < 16 or 7.5 ≤ OSI < 12.3
Severe ARDS = OI ≥ 16 or OSI ≥ 12.3 Triggers:
Direct: Pneumonia, aspiration / inhalation, contusions, near drowning
Indirect: Sepsis, shock, trauma, multiple transfusions, burns, pancreatitis Management = support with lung protection strategies
Conventional Mechanical Ventilation (CMV) Low tidal volume ventilation: Vt = 5-8 ml/kg Permissive Hypercapnia / Hypoxemia
Acceptance of pCO2 to limit ventilator injury
Maintain pH 7.25
Tolerate SpO2 85% is adequate oxygen delivery Serious complications of conventional ventilation associated with:
PIP > 32 cm H2O FiO2 > 0.6 Failure to wean Patient ventilator dyssynchrony (documented by respiratory mechanics
and physical exam) Lung overdistension (documented by respiratory mechanics)
Nonconventional Ventilation – to recruit lung volume and lung injury Airway Pressure Release Ventilation High Frequency Oscillatory Ventilation (see section below) High Frequency Jet Ventilation (see section below)
13
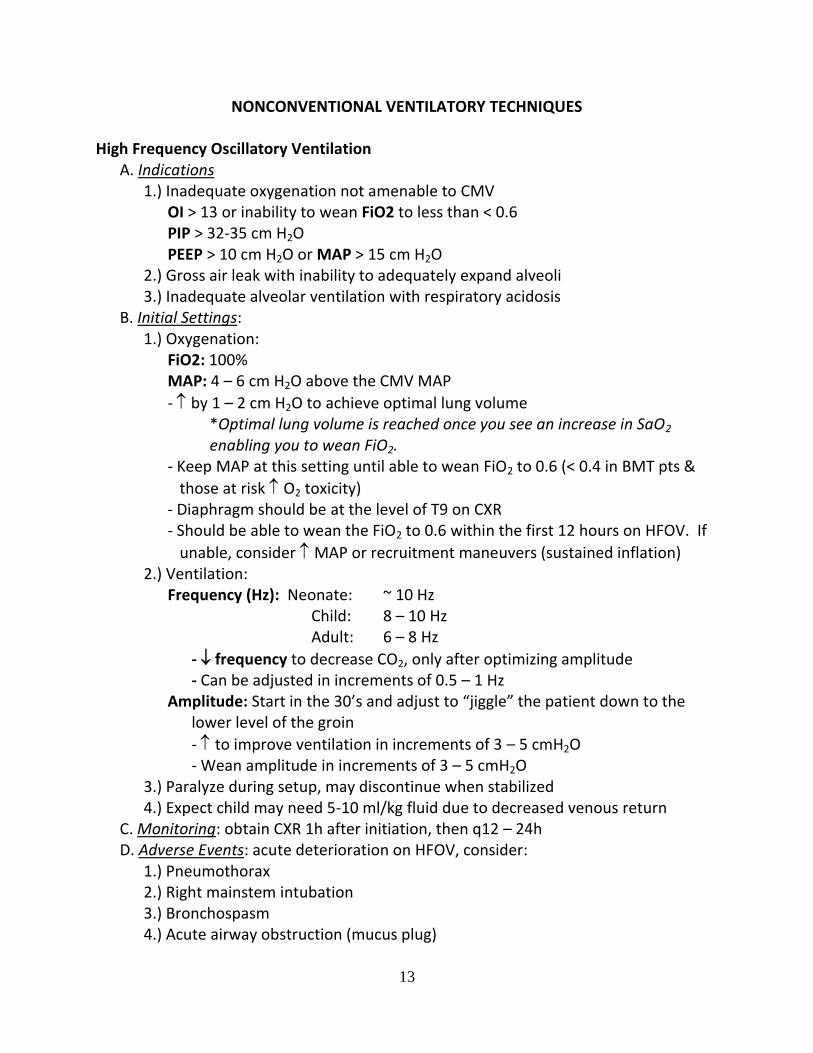
NONCONVENTIONAL VENTILATORY TECHNIQUES High Frequency Oscillatory Ventilation A. Indications 1.) Inadequate oxygenation not amenable to CMV OI > 13 or inability to wean FiO2 to less than < 0.6 PIP > 32-35 cm H2O PEEP > 10 cm H2O or MAP > 15 cm H2O 2.) Gross air leak with inability to adequately expand alveoli 3.) Inadequate alveolar ventilation with respiratory acidosis B. Initial Settings: 1.) Oxygenation: FiO2: 100% MAP: 4 – 6 cm H2O above the CMV MAP
- by 1 – 2 cm H2O to achieve optimal lung volume *Optimal lung volume is reached once you see an increase in SaO2 enabling you to wean FiO2.
- Keep MAP at this setting until able to wean FiO2 to 0.6 (< 0.4 in BMT pts &
those at risk O2 toxicity) - Diaphragm should be at the level of T9 on CXR - Should be able to wean the FiO2 to 0.6 within the first 12 hours on HFOV. If
unable, consider MAP or recruitment maneuvers (sustained inflation) 2.) Ventilation: Frequency (Hz): Neonate: ~ 10 Hz Child: 8 – 10 Hz Adult: 6 – 8 Hz
- frequency to decrease CO2, only after optimizing amplitude - Can be adjusted in increments of 0.5 – 1 Hz Amplitude: Start in the 30’s and adjust to “jiggle” the patient down to the lower level of the groin
- to improve ventilation in increments of 3 – 5 cmH2O - Wean amplitude in increments of 3 – 5 cmH2O 3.) Paralyze during setup, may discontinue when stabilized 4.) Expect child may need 5-10 ml/kg fluid due to decreased venous return C. Monitoring: obtain CXR 1h after initiation, then q12 – 24h D. Adverse Events: acute deterioration on HFOV, consider: 1.) Pneumothorax 2.) Right mainstem intubation 3.) Bronchospasm 4.) Acute airway obstruction (mucus plug)
14
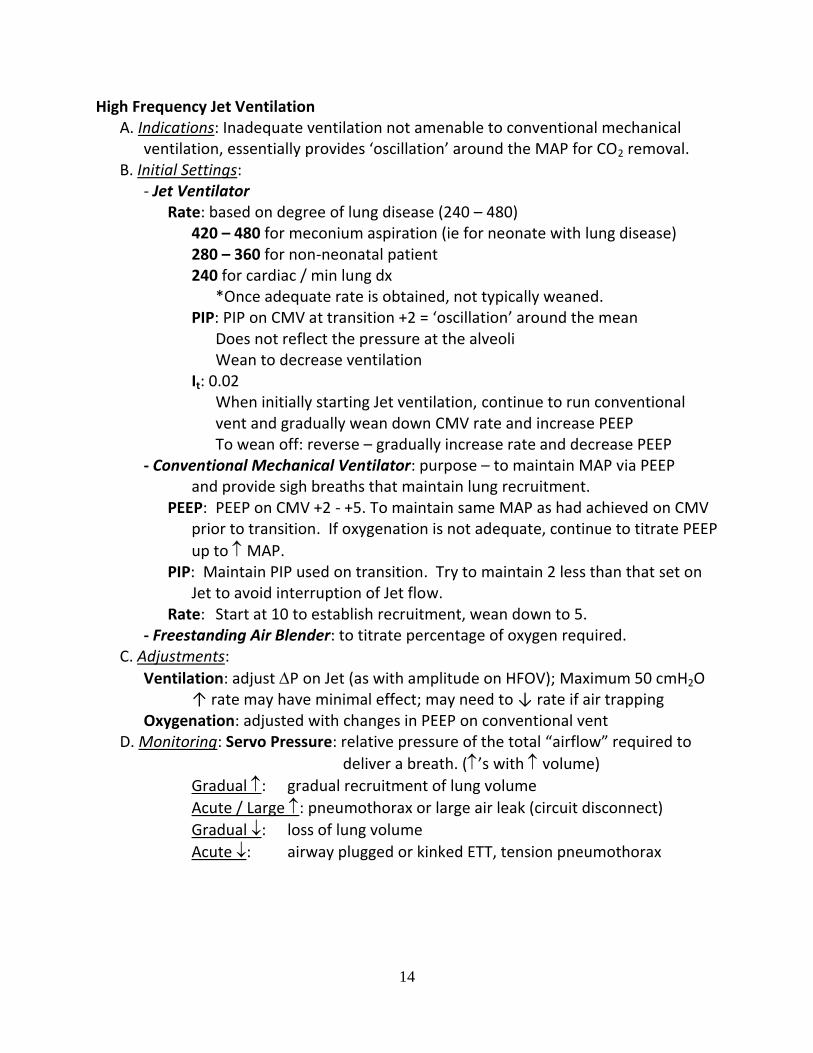
High Frequency Jet Ventilation A. Indications: Inadequate ventilation not amenable to conventional mechanical ventilation, essentially provides ‘oscillation’ around the MAP for CO2 removal. B. Initial Settings: - Jet Ventilator Rate: based on degree of lung disease (240 – 480) 420 – 480 for meconium aspiration (ie for neonate with lung disease) 280 – 360 for non-neonatal patient 240 for cardiac / min lung dx *Once adequate rate is obtained, not typically weaned. PIP: PIP on CMV at transition +2 = ‘oscillation’ around the mean Does not reflect the pressure at the alveoli Wean to decrease ventilation It: 0.02
When initially starting Jet ventilation, continue to run conventional vent and gradually wean down CMV rate and increase PEEP
To wean off: reverse – gradually increase rate and decrease PEEP - Conventional Mechanical Ventilator: purpose – to maintain MAP via PEEP and provide sigh breaths that maintain lung recruitment. PEEP: PEEP on CMV +2 - +5. To maintain same MAP as had achieved on CMV
prior to transition. If oxygenation is not adequate, continue to titrate PEEP
up to MAP. PIP: Maintain PIP used on transition. Try to maintain 2 less than that set on
Jet to avoid interruption of Jet flow. Rate: Start at 10 to establish recruitment, wean down to 5. - Freestanding Air Blender: to titrate percentage of oxygen required. C. Adjustments:
Ventilation: adjust P on Jet (as with amplitude on HFOV); Maximum 50 cmH2O ↑ rate may have minimal effect; may need to ↓ rate if air trapping Oxygenation: adjusted with changes in PEEP on conventional vent D. Monitoring: Servo Pressure: relative pressure of the total “airflow” required to
deliver a breath. (’s with volume)
Gradual : gradual recruitment of lung volume
Acute / Large : pneumothorax or large air leak (circuit disconnect)
Gradual : loss of lung volume
Acute : airway plugged or kinked ETT, tension pneumothorax
15
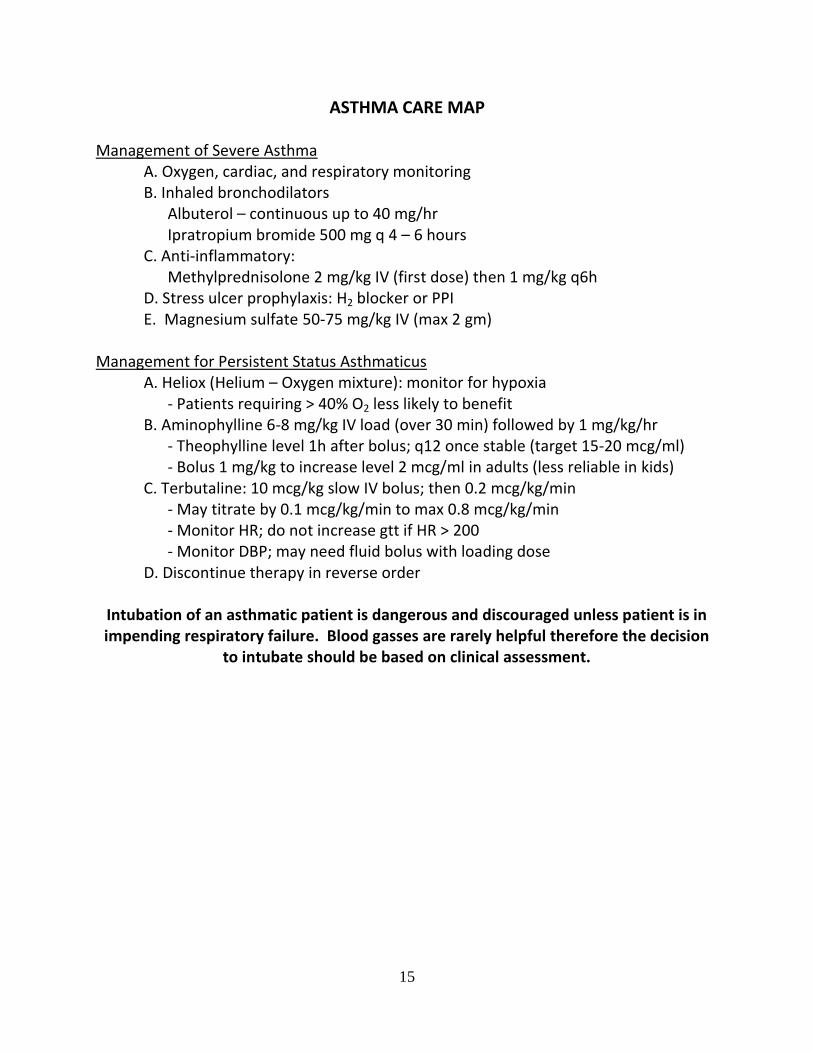
ASTHMA CARE MAP Management of Severe Asthma A. Oxygen, cardiac, and respiratory monitoring B. Inhaled bronchodilators Albuterol – continuous up to 40 mg/hr Ipratropium bromide 500 mg q 4 – 6 hours C. Anti-inflammatory: Methylprednisolone 2 mg/kg IV (first dose) then 1 mg/kg q6h D. Stress ulcer prophylaxis: H2 blocker or PPI E. Magnesium sulfate 50-75 mg/kg IV (max 2 gm) Management for Persistent Status Asthmaticus A. Heliox (Helium – Oxygen mixture): monitor for hypoxia - Patients requiring > 40% O2 less likely to benefit B. Aminophylline 6-8 mg/kg IV load (over 30 min) followed by 1 mg/kg/hr - Theophylline level 1h after bolus; q12 once stable (target 15-20 mcg/ml) - Bolus 1 mg/kg to increase level 2 mcg/ml in adults (less reliable in kids) C. Terbutaline: 10 mcg/kg slow IV bolus; then 0.2 mcg/kg/min - May titrate by 0.1 mcg/kg/min to max 0.8 mcg/kg/min - Monitor HR; do not increase gtt if HR > 200 - Monitor DBP; may need fluid bolus with loading dose D. Discontinue therapy in reverse order
Intubation of an asthmatic patient is dangerous and discouraged unless patient is in impending respiratory failure. Blood gasses are rarely helpful therefore the decision
to intubate should be based on clinical assessment.
16
CARDIOVASCULAR
OXYGEN DELIVERY:
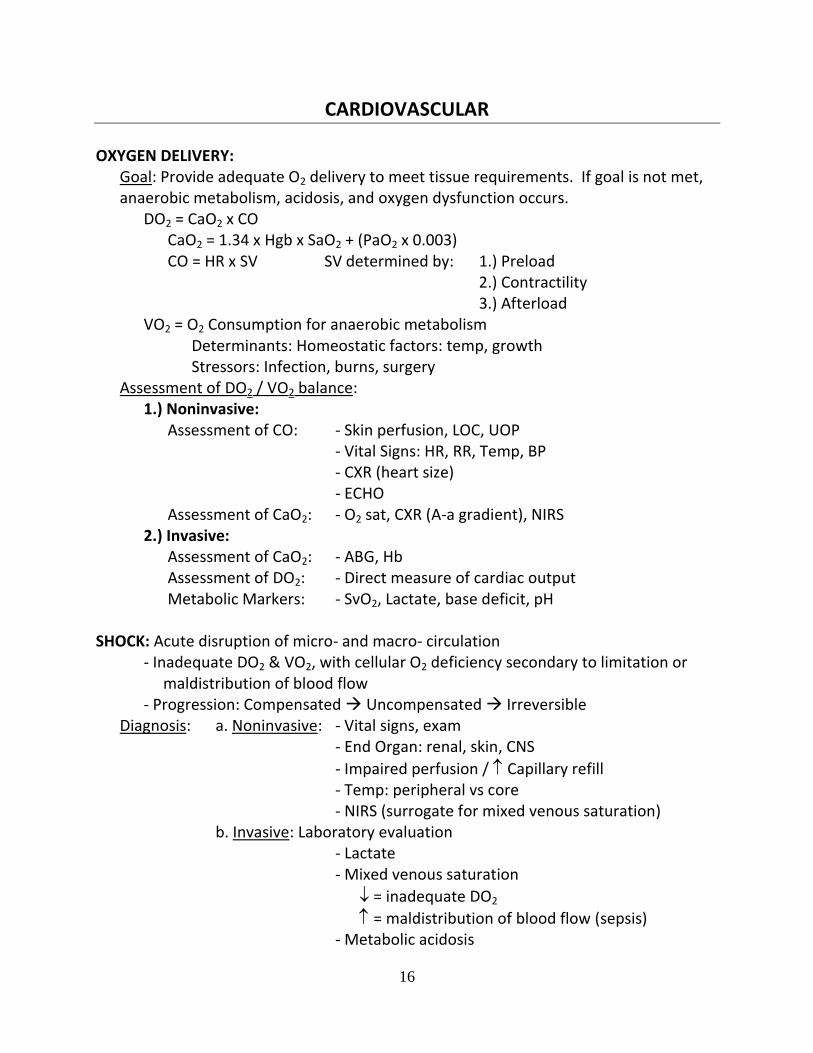
Goal: Provide adequate O2 delivery to meet tissue requirements. If goal is not met, anaerobic metabolism, acidosis, and oxygen dysfunction occurs.
DO2 = CaO2 x CO CaO2 = 1.34 x Hgb x SaO2 + (PaO2 x 0.003) CO = HR x SV SV determined by: 1.) Preload 2.) Contractility 3.) Afterload VO2 = O2 Consumption for anaerobic metabolism Determinants: Homeostatic factors: temp, growth Stressors: Infection, burns, surgery Assessment of DO2 / VO2 balance: 1.) Noninvasive: Assessment of CO: - Skin perfusion, LOC, UOP - Vital Signs: HR, RR, Temp, BP - CXR (heart size) - ECHO Assessment of CaO2: - O2 sat, CXR (A-a gradient), NIRS 2.) Invasive: Assessment of CaO2: - ABG, Hb Assessment of DO2: - Direct measure of cardiac output Metabolic Markers: - SvO2, Lactate, base deficit, pH SHOCK: Acute disruption of micro- and macro- circulation
- Inadequate DO2 & VO2, with cellular O2 deficiency secondary to limitation or maldistribution of blood flow
- Progression: Compensated Uncompensated Irreversible Diagnosis: a. Noninvasive: - Vital signs, exam - End Organ: renal, skin, CNS
- Impaired perfusion / Capillary refill - Temp: peripheral vs core - NIRS (surrogate for mixed venous saturation) b. Invasive: Laboratory evaluation - Lactate - Mixed venous saturation
= inadequate DO2
= maldistribution of blood flow (sepsis) - Metabolic acidosis

17
SHOCK: Determining Etiology
Type Physiology Causes Treatment
Hyp
ovo
lem
ic ↓intravascular
volume
↓preload = ↓SV
Hemorrhage
GI losses
Volume
Replace what is lost
Repeated 20 ml/kg boluses
Car
dio
gen
ic
CO=HRxSV ↓SV:
↓preload
↓contractility
↑afterload Tachycardia to compensate for ↓SV
↓ Preload
Regurgitant lesions
Dilated CM
Control infection
Inotropes
Correct pH, Ca++, glucose
Optimize preload
Lusitropes (milrinone)
Contractility
Systolic dysfxn
Diastolic dysfxn
↑ Afterload
Obstructive lesions
pulm htn, Hypertensive emergency
Intervention / surgery
Do not vasodilate for obstructive lesions
Pulmonary / arteriolar vasodilators
Sep
tic
Inflammatory response
Capillary leak
Intravascular volume depletion, ↓preload
Poor oxygen extraction
Systemic effects of endotoxins, cytokines, free radicals
Control infection
Aggressive volume resuscitation
Support cardiac dysfunction; inotropes
Monitor for ↓ Ca++, glucose
Dis
trib
uti
ve Maldistribution of
blood flow
↓preload
May have brisk capillary refill
Anaphylaxis
Toxic Shock Syndrome
Spinal shock
Vasoplegia
Volume
Reverse etiology
Vasoconstrictors
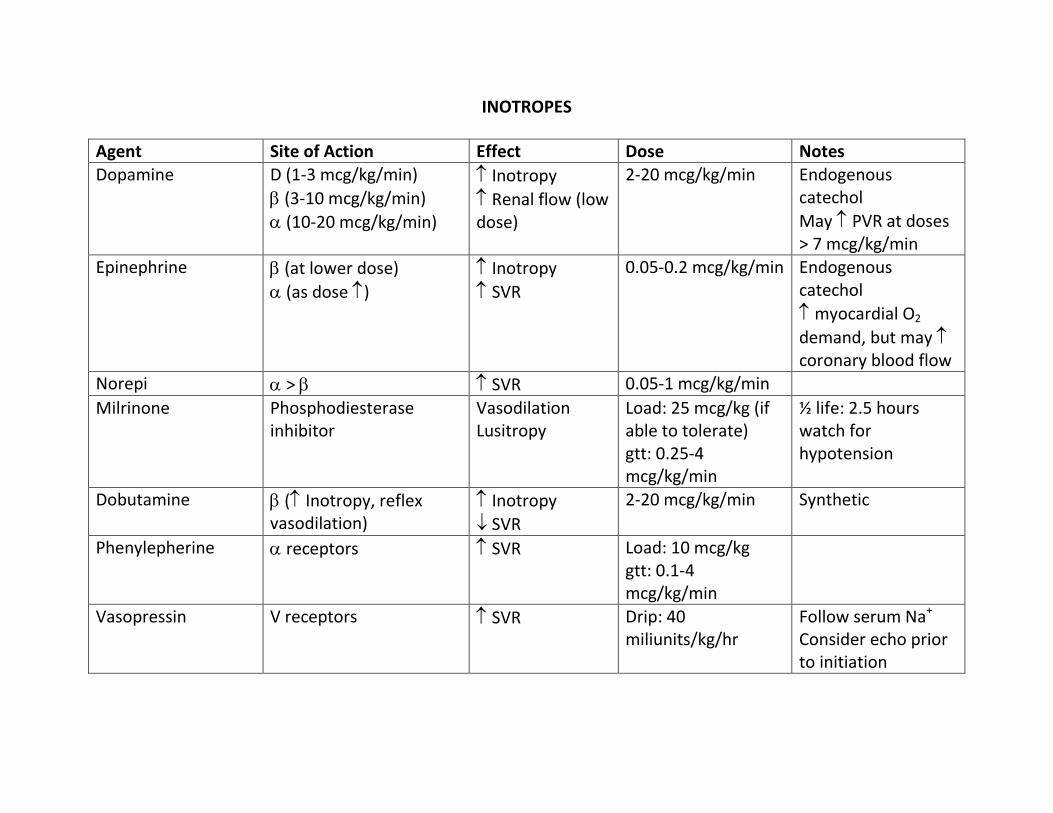
INOTROPES
Agent Site of Action Effect Dose Notes Dopamine D (1-3 mcg/kg/min)
(3-10 mcg/kg/min)
(10-20 mcg/kg/min)
Inotropy
Renal flow (low dose)
2-20 mcg/kg/min Endogenous catechol
May PVR at doses > 7 mcg/kg/min
Epinephrine (at lower dose)
(as dose )
Inotropy
SVR
0.05-0.2 mcg/kg/min Endogenous catechol
myocardial O2
demand, but may coronary blood flow
Norepi > SVR 0.05-1 mcg/kg/min
Milrinone Phosphodiesterase inhibitor
Vasodilation Lusitropy
Load: 25 mcg/kg (if able to tolerate) gtt: 0.25-4 mcg/kg/min
½ life: 2.5 hours watch for hypotension
Dobutamine ( Inotropy, reflex vasodilation)
Inotropy
SVR
2-20 mcg/kg/min Synthetic
Phenylepherine receptors SVR Load: 10 mcg/kg gtt: 0.1-4 mcg/kg/min
Vasopressin V receptors SVR Drip: 40 miliunits/kg/hr
Follow serum Na+
Consider echo prior to initiation
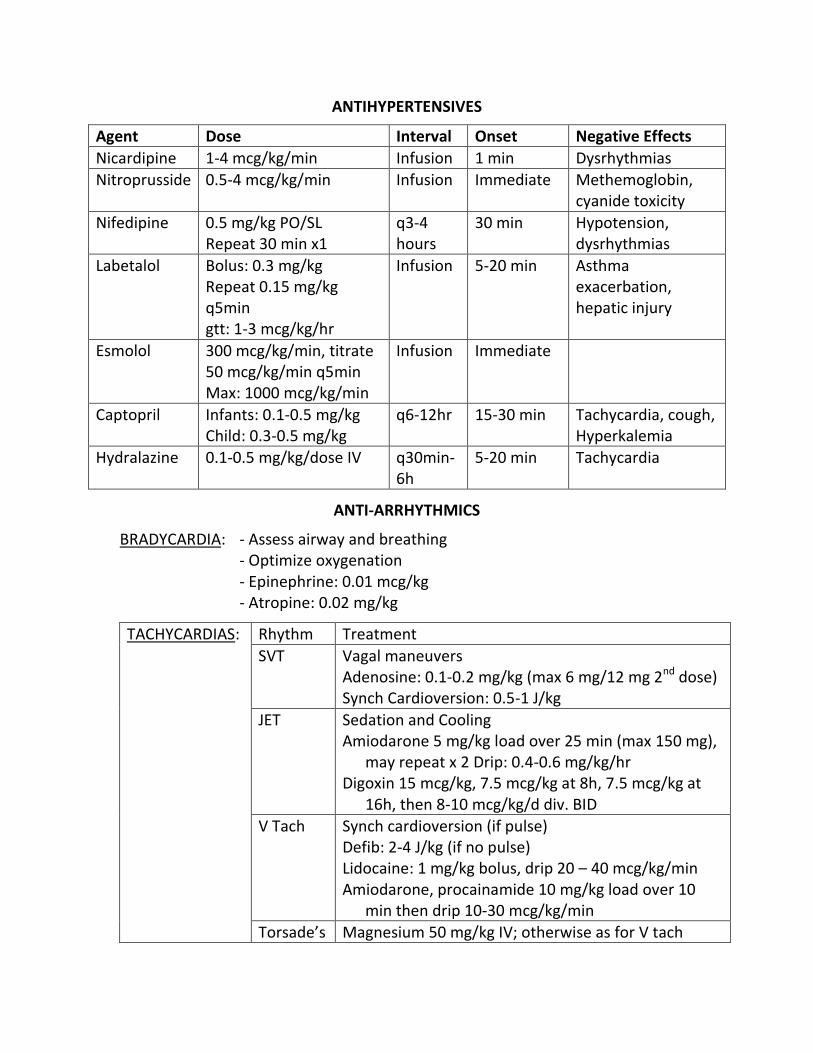
ANTIHYPERTENSIVES
Agent Dose Interval Onset Negative Effects
Nicardipine 1-4 mcg/kg/min Infusion 1 min Dysrhythmias
Nitroprusside 0.5-4 mcg/kg/min Infusion Immediate Methemoglobin, cyanide toxicity
Nifedipine 0.5 mg/kg PO/SL Repeat 30 min x1
q3-4 hours
30 min Hypotension, dysrhythmias
Labetalol Bolus: 0.3 mg/kg Repeat 0.15 mg/kg q5min gtt: 1-3 mcg/kg/hr
Infusion 5-20 min Asthma exacerbation, hepatic injury
Esmolol 300 mcg/kg/min, titrate 50 mcg/kg/min q5min Max: 1000 mcg/kg/min
Infusion Immediate
Captopril Infants: 0.1-0.5 mg/kg Child: 0.3-0.5 mg/kg
q6-12hr
15-30 min Tachycardia, cough, Hyperkalemia
Hydralazine 0.1-0.5 mg/kg/dose IV q30min-6h
5-20 min Tachycardia
ANTI-ARRHYTHMICS
BRADYCARDIA: - Assess airway and breathing - Optimize oxygenation - Epinephrine: 0.01 mcg/kg - Atropine: 0.02 mg/kg
TACHYCARDIAS: Rhythm Treatment
SVT Vagal maneuvers Adenosine: 0.1-0.2 mg/kg (max 6 mg/12 mg 2nd dose) Synch Cardioversion: 0.5-1 J/kg
JET Sedation and Cooling Amiodarone 5 mg/kg load over 25 min (max 150 mg),
may repeat x 2 Drip: 0.4-0.6 mg/kg/hr Digoxin 15 mcg/kg, 7.5 mcg/kg at 8h, 7.5 mcg/kg at
16h, then 8-10 mcg/kg/d div. BID
V Tach Synch cardioversion (if pulse) Defib: 2-4 J/kg (if no pulse) Lidocaine: 1 mg/kg bolus, drip 20 – 40 mcg/kg/min Amiodarone, procainamide 10 mg/kg load over 10
min then drip 10-30 mcg/kg/min
Torsade’s Magnesium 50 mg/kg IV; otherwise as for V tach
21
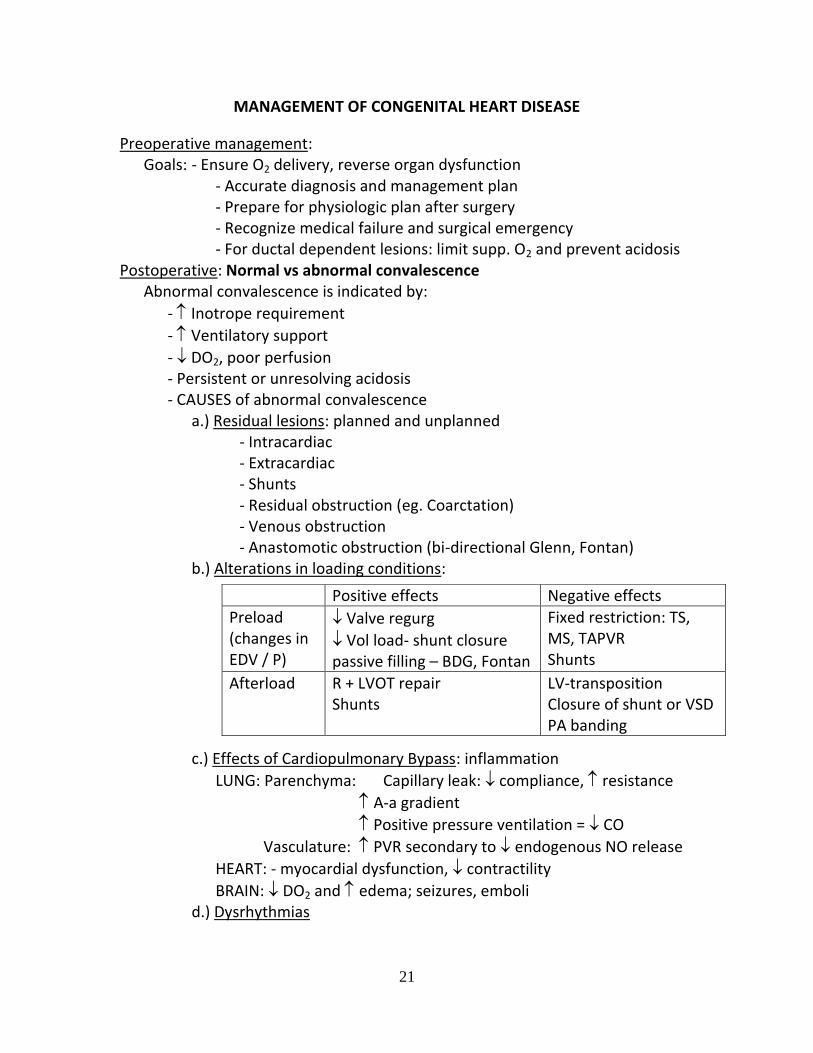
MANAGEMENT OF CONGENITAL HEART DISEASE
Preoperative management: Goals: - Ensure O2 delivery, reverse organ dysfunction - Accurate diagnosis and management plan - Prepare for physiologic plan after surgery - Recognize medical failure and surgical emergency - For ductal dependent lesions: limit supp. O2 and prevent acidosis Postoperative: Normal vs abnormal convalescence Abnormal convalescence is indicated by:
- Inotrope requirement
- Ventilatory support
- DO2, poor perfusion - Persistent or unresolving acidosis - CAUSES of abnormal convalescence a.) Residual lesions: planned and unplanned - Intracardiac - Extracardiac - Shunts - Residual obstruction (eg. Coarctation) - Venous obstruction - Anastomotic obstruction (bi-directional Glenn, Fontan) b.) Alterations in loading conditions: c.) Effects of Cardiopulmonary Bypass: inflammation
LUNG: Parenchyma: Capillary leak: compliance, resistance
A-a gradient
Positive pressure ventilation = CO
Vasculature: PVR secondary to endogenous NO release
HEART: - myocardial dysfunction, contractility
BRAIN: DO2 and edema; seizures, emboli d.) Dysrhythmias
Positive effects Negative effects
Preload (changes in EDV / P)
Valve regurg
Vol load- shunt closure passive filling – BDG, Fontan
Fixed restriction: TS, MS, TAPVR Shunts
Afterload R + LVOT repair Shunts
LV-transposition Closure of shunt or VSD PA banding
22
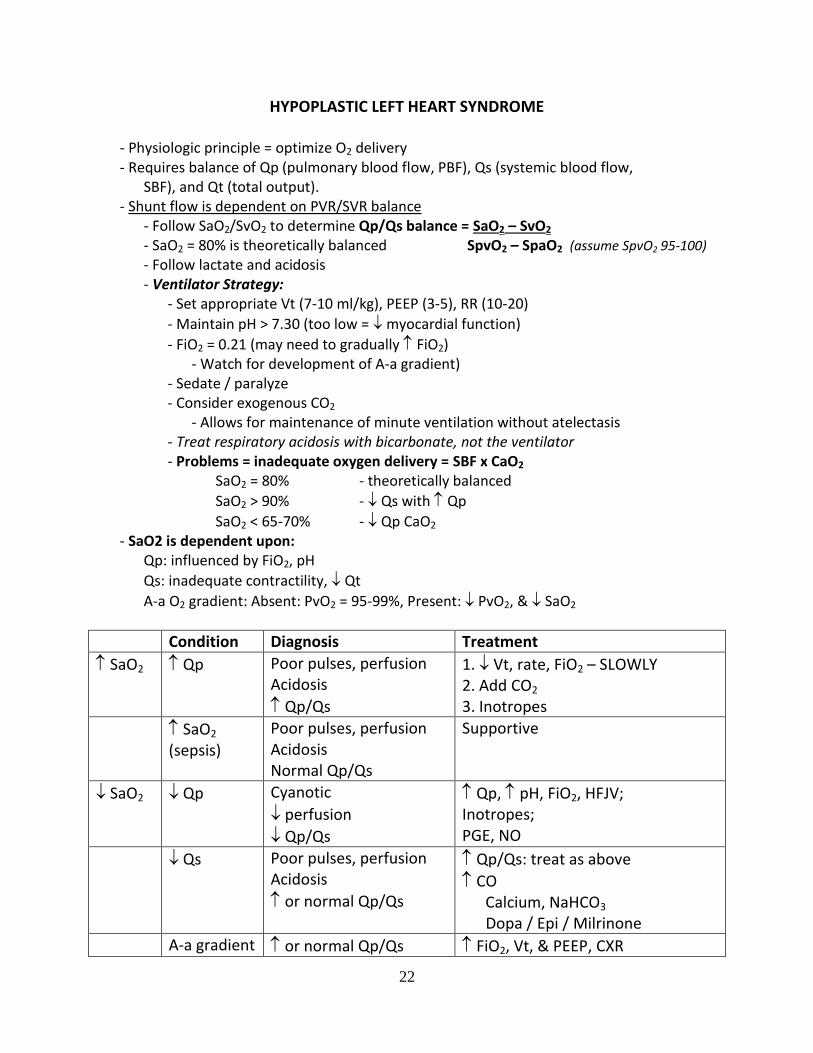
HYPOPLASTIC LEFT HEART SYNDROME
- Physiologic principle = optimize O2 delivery - Requires balance of Qp (pulmonary blood flow, PBF), Qs (systemic blood flow, SBF), and Qt (total output). - Shunt flow is dependent on PVR/SVR balance - Follow SaO2/SvO2 to determine Qp/Qs balance = SaO2 – SvO2 - SaO2 = 80% is theoretically balanced SpvO2 – SpaO2 (assume SpvO2 95-100) - Follow lactate and acidosis - Ventilator Strategy: - Set appropriate Vt (7-10 ml/kg), PEEP (3-5), RR (10-20)
- Maintain pH > 7.30 (too low = myocardial function)
- FiO2 = 0.21 (may need to gradually FiO2) - Watch for development of A-a gradient) - Sedate / paralyze - Consider exogenous CO2 - Allows for maintenance of minute ventilation without atelectasis - Treat respiratory acidosis with bicarbonate, not the ventilator - Problems = inadequate oxygen delivery = SBF x CaO2 SaO2 = 80% - theoretically balanced
SaO2 > 90% - Qs with Qp
SaO2 < 65-70% - Qp CaO2 - SaO2 is dependent upon: Qp: influenced by FiO2, pH
Qs: inadequate contractility, Qt
A-a O2 gradient: Absent: PvO2 = 95-99%, Present: PvO2, & SaO2
Condition Diagnosis Treatment
SaO2 Qp Poor pulses, perfusion Acidosis
Qp/Qs
1. Vt, rate, FiO2 – SLOWLY 2. Add CO2 3. Inotropes
SaO2 (sepsis)
Poor pulses, perfusion Acidosis Normal Qp/Qs
Supportive
SaO2 Qp Cyanotic
perfusion
Qp/Qs
Qp, pH, FiO2, HFJV; Inotropes; PGE, NO
Qs Poor pulses, perfusion Acidosis
or normal Qp/Qs
Qp/Qs: treat as above
CO Calcium, NaHCO3 Dopa / Epi / Milrinone
A-a gradient or normal Qp/Qs FiO2, Vt, & PEEP, CXR

23
EXTRACORPOREAL MEMBRANE OXYGENATION
1. Criteria for the initiation of ECMO: - Patient unresponsive to maximal conventional tx and has reversible disease - Oxygenation index: > 40 predicted mortality > 80% 25 – 40 predicted mortality 50 – 80% - Acute deterioration - Significant barotrauma 2. Contraindications: - Lethal underlying disease (genetic, pulmonary, cardiac, immunodeficiency) - Unwitnessed cardiac arrest - Relative: Mechanical ventilation > 14 days on high support 3. Pre-ECMO screening: Head ultrasound: IVH > grade I is a contraindication to ECMO secondary to heparinization ECHO: r/o structural heart defects 4. Initiation and management: see orderset 5. VA ECMO (veno-arterial): a. Provides pulmonary and cardiac support - Cardiac output is determined by pump flow and LV output b. Blood Flow: desaturated blood is drained from the RA via venous cannula flows by gravity to a reservoir centrifugal pump advances the blood in a nonpulsatile fashion to the membrane oxygenator oxygenated blood flows through the heat exchanger returns to the patient via the arterial cannula c. Cannula Placement: Venous cannula is placed in the RA via the IJ - catheter has multiple side ports; radiopaque dot at end aides placement Arterial cannula is placed in the R common carotid artery and advanced to the inominant artery and ascending aorta junction – close proximity to cerebral and coronary circulations. 6. VV ECMO (veno-venous): a. Provides pulmonary support only. No direct cardiac support. - Cardiac output may improve secondary to improved oxygenation and improved myocardial oxygen delivery - Allows for improved oxygenation without ligation of carotid artery b. Cannula placement: double lumen cannula with the tip in the RA; or 2 venous catheters: femoral IJ 7. ECMO Circuit Output: - Determined by the amount of venous blood withdrawn from patient - Dependent on gravity and systemic venous return (avoid hypovolemia, pneumothorax, cardiac tamponade).
24
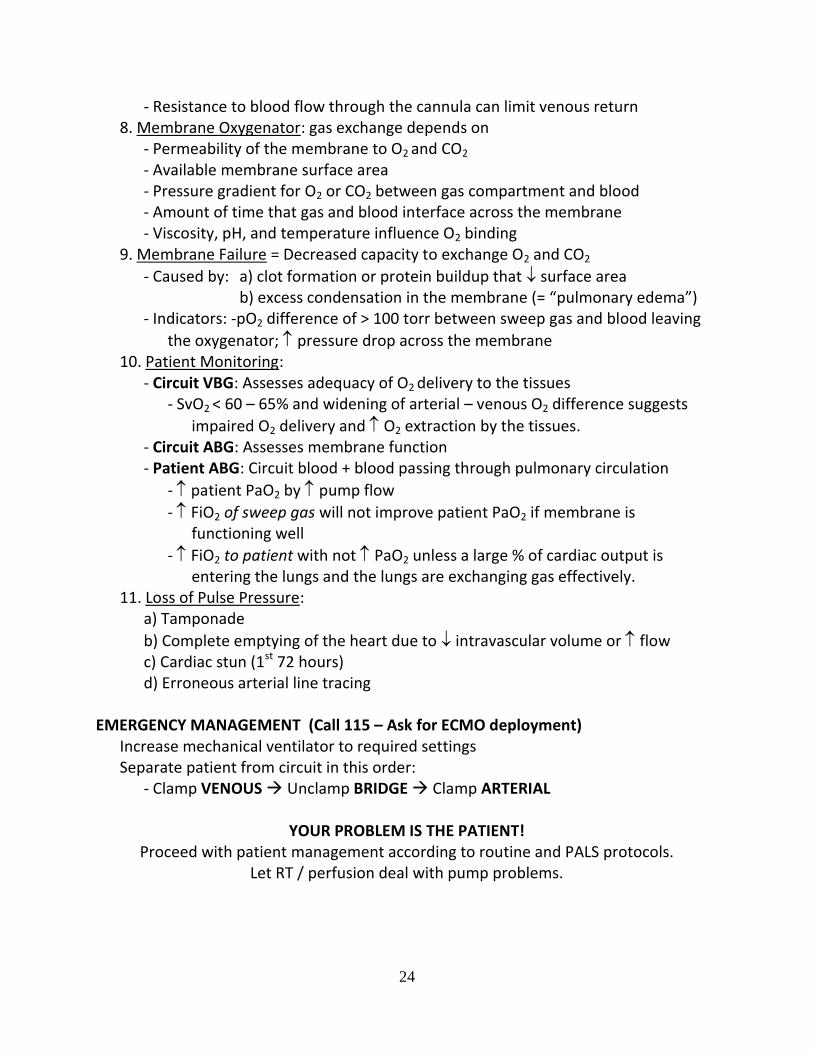
- Resistance to blood flow through the cannula can limit venous return 8. Membrane Oxygenator: gas exchange depends on - Permeability of the membrane to O2 and CO2 - Available membrane surface area - Pressure gradient for O2 or CO2 between gas compartment and blood - Amount of time that gas and blood interface across the membrane - Viscosity, pH, and temperature influence O2 binding 9. Membrane Failure = Decreased capacity to exchange O2 and CO2
- Caused by: a) clot formation or protein buildup that surface area b) excess condensation in the membrane (= “pulmonary edema”) - Indicators: -pO2 difference of > 100 torr between sweep gas and blood leaving
the oxygenator; pressure drop across the membrane 10. Patient Monitoring: - Circuit VBG: Assesses adequacy of O2 delivery to the tissues - SvO2 < 60 – 65% and widening of arterial – venous O2 difference suggests
impaired O2 delivery and O2 extraction by the tissues. - Circuit ABG: Assesses membrane function - Patient ABG: Circuit blood + blood passing through pulmonary circulation
- patient PaO2 by pump flow
- FiO2 of sweep gas will not improve patient PaO2 if membrane is functioning well
- FiO2 to patient with not PaO2 unless a large % of cardiac output is entering the lungs and the lungs are exchanging gas effectively. 11. Loss of Pulse Pressure: a) Tamponade
b) Complete emptying of the heart due to intravascular volume or flow c) Cardiac stun (1st 72 hours) d) Erroneous arterial line tracing EMERGENCY MANAGEMENT (Call 115 – Ask for ECMO deployment) Increase mechanical ventilator to required settings Separate patient from circuit in this order: - Clamp VENOUS Unclamp BRIDGE Clamp ARTERIAL
YOUR PROBLEM IS THE PATIENT! Proceed with patient management according to routine and PALS protocols.
Let RT / perfusion deal with pump problems.
25
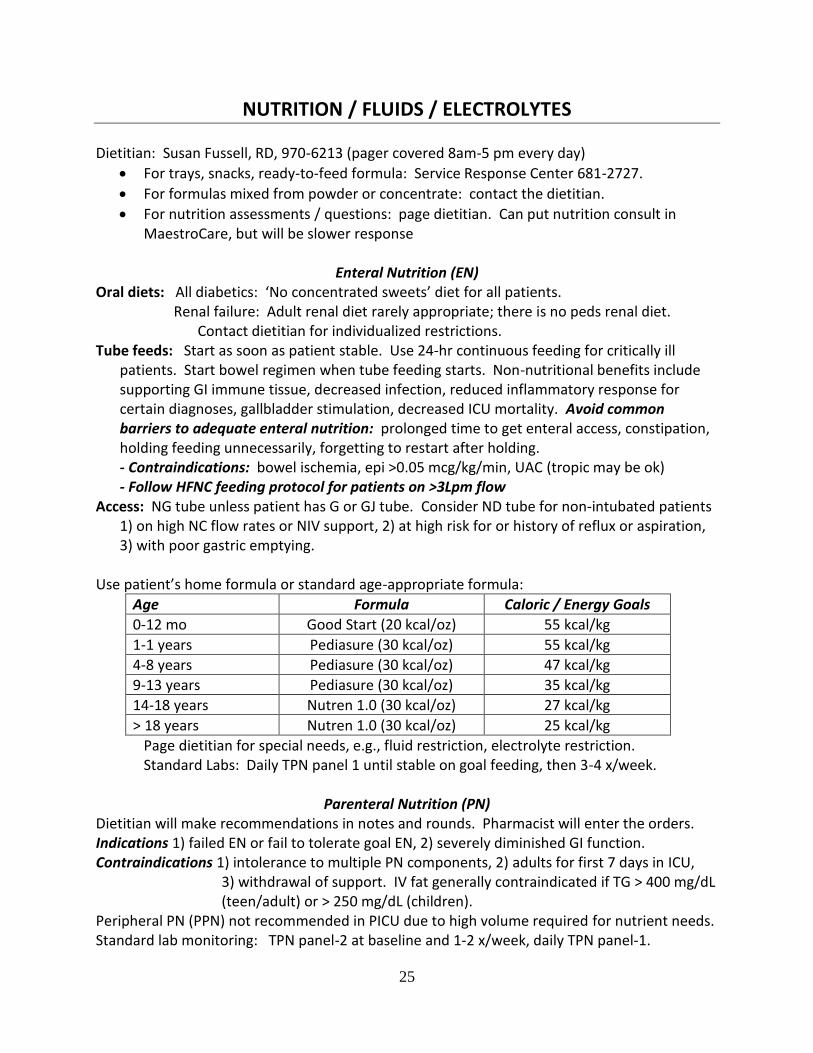
NUTRITION / FLUIDS / ELECTROLYTES
Dietitian: Susan Fussell, RD, 970-6213 (pager covered 8am-5 pm every day)
For trays, snacks, ready-to-feed formula: Service Response Center 681-2727.
For formulas mixed from powder or concentrate: contact the dietitian.
For nutrition assessments / questions: page dietitian. Can put nutrition consult in MaestroCare, but will be slower response
Enteral Nutrition (EN) Oral diets: All diabetics: ‘No concentrated sweets’ diet for all patients.
Renal failure: Adult renal diet rarely appropriate; there is no peds renal diet. Contact dietitian for individualized restrictions.
Tube feeds: Start as soon as patient stable. Use 24-hr continuous feeding for critically ill patients. Start bowel regimen when tube feeding starts. Non-nutritional benefits include supporting GI immune tissue, decreased infection, reduced inflammatory response for certain diagnoses, gallbladder stimulation, decreased ICU mortality. Avoid common barriers to adequate enteral nutrition: prolonged time to get enteral access, constipation, holding feeding unnecessarily, forgetting to restart after holding. - Contraindications: bowel ischemia, epi >0.05 mcg/kg/min, UAC (tropic may be ok) - Follow HFNC feeding protocol for patients on >3Lpm flow
Access: NG tube unless patient has G or GJ tube. Consider ND tube for non-intubated patients 1) on high NC flow rates or NIV support, 2) at high risk for or history of reflux or aspiration, 3) with poor gastric emptying.
Use patient’s home formula or standard age-appropriate formula:
Age Formula Caloric / Energy Goals
0-12 mo Good Start (20 kcal/oz) 55 kcal/kg
1-1 years Pediasure (30 kcal/oz) 55 kcal/kg
4-8 years Pediasure (30 kcal/oz) 47 kcal/kg
9-13 years Pediasure (30 kcal/oz) 35 kcal/kg
14-18 years Nutren 1.0 (30 kcal/oz) 27 kcal/kg
> 18 years Nutren 1.0 (30 kcal/oz) 25 kcal/kg
Page dietitian for special needs, e.g., fluid restriction, electrolyte restriction. Standard Labs: Daily TPN panel 1 until stable on goal feeding, then 3-4 x/week.
Parenteral Nutrition (PN)
Dietitian will make recommendations in notes and rounds. Pharmacist will enter the orders. Indications 1) failed EN or fail to tolerate goal EN, 2) severely diminished GI function. Contraindications 1) intolerance to multiple PN components, 2) adults for first 7 days in ICU,
3) withdrawal of support. IV fat generally contraindicated if TG > 400 mg/dL (teen/adult) or > 250 mg/dL (children).
Peripheral PN (PPN) not recommended in PICU due to high volume required for nutrient needs. Standard lab monitoring: TPN panel-2 at baseline and 1-2 x/week, daily TPN panel-1.
26
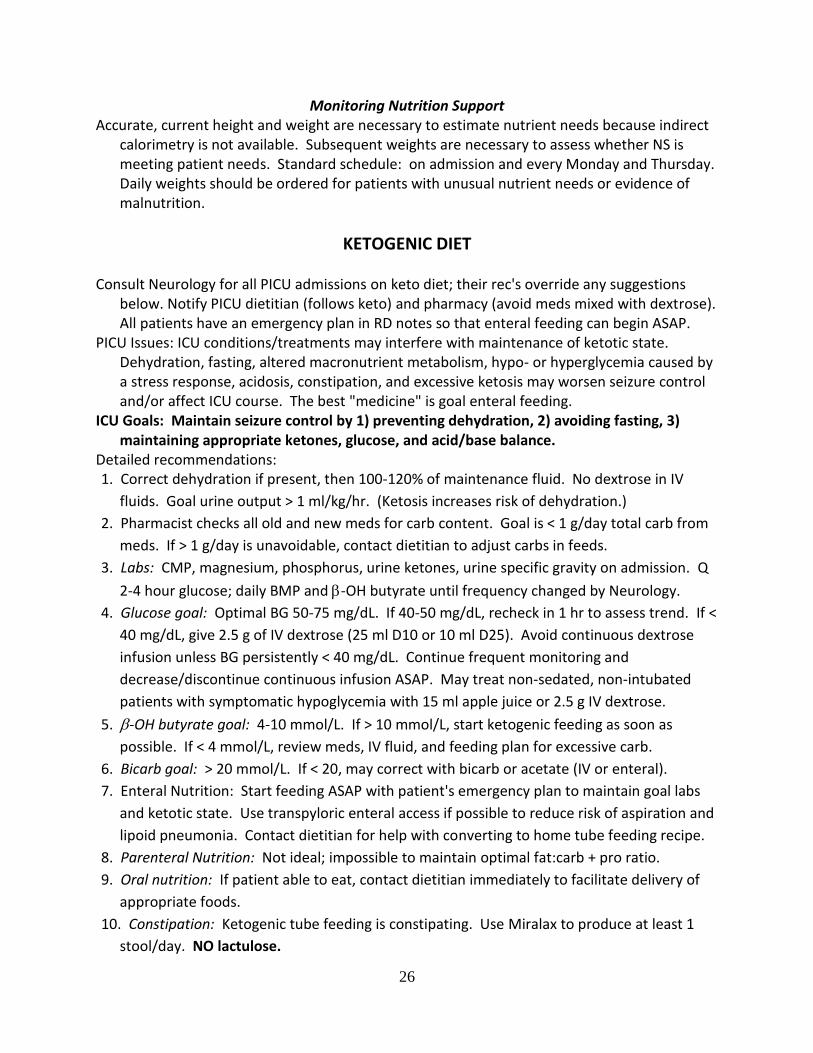
Monitoring Nutrition Support Accurate, current height and weight are necessary to estimate nutrient needs because indirect
calorimetry is not available. Subsequent weights are necessary to assess whether NS is meeting patient needs. Standard schedule: on admission and every Monday and Thursday. Daily weights should be ordered for patients with unusual nutrient needs or evidence of malnutrition.
KETOGENIC DIET Consult Neurology for all PICU admissions on keto diet; their rec's override any suggestions
below. Notify PICU dietitian (follows keto) and pharmacy (avoid meds mixed with dextrose). All patients have an emergency plan in RD notes so that enteral feeding can begin ASAP.
PICU Issues: ICU conditions/treatments may interfere with maintenance of ketotic state. Dehydration, fasting, altered macronutrient metabolism, hypo- or hyperglycemia caused by a stress response, acidosis, constipation, and excessive ketosis may worsen seizure control and/or affect ICU course. The best "medicine" is goal enteral feeding.
ICU Goals: Maintain seizure control by 1) preventing dehydration, 2) avoiding fasting, 3) maintaining appropriate ketones, glucose, and acid/base balance.
Detailed recommendations: 1. Correct dehydration if present, then 100-120% of maintenance fluid. No dextrose in IV
fluids. Goal urine output > 1 ml/kg/hr. (Ketosis increases risk of dehydration.)
2. Pharmacist checks all old and new meds for carb content. Goal is < 1 g/day total carb from
meds. If > 1 g/day is unavoidable, contact dietitian to adjust carbs in feeds.
3. Labs: CMP, magnesium, phosphorus, urine ketones, urine specific gravity on admission. Q
2-4 hour glucose; daily BMP and -OH butyrate until frequency changed by Neurology.
4. Glucose goal: Optimal BG 50-75 mg/dL. If 40-50 mg/dL, recheck in 1 hr to assess trend. If <
40 mg/dL, give 2.5 g of IV dextrose (25 ml D10 or 10 ml D25). Avoid continuous dextrose
infusion unless BG persistently < 40 mg/dL. Continue frequent monitoring and
decrease/discontinue continuous infusion ASAP. May treat non-sedated, non-intubated
patients with symptomatic hypoglycemia with 15 ml apple juice or 2.5 g IV dextrose.
5. -OH butyrate goal: 4-10 mmol/L. If > 10 mmol/L, start ketogenic feeding as soon as
possible. If < 4 mmol/L, review meds, IV fluid, and feeding plan for excessive carb.
6. Bicarb goal: > 20 mmol/L. If < 20, may correct with bicarb or acetate (IV or enteral).
7. Enteral Nutrition: Start feeding ASAP with patient's emergency plan to maintain goal labs
and ketotic state. Use transpyloric enteral access if possible to reduce risk of aspiration and
lipoid pneumonia. Contact dietitian for help with converting to home tube feeding recipe.
8. Parenteral Nutrition: Not ideal; impossible to maintain optimal fat:carb + pro ratio.
9. Oral nutrition: If patient able to eat, contact dietitian immediately to facilitate delivery of
appropriate foods.
10. Constipation: Ketogenic tube feeding is constipating. Use Miralax to produce at least 1
stool/day. NO lactulose.
27
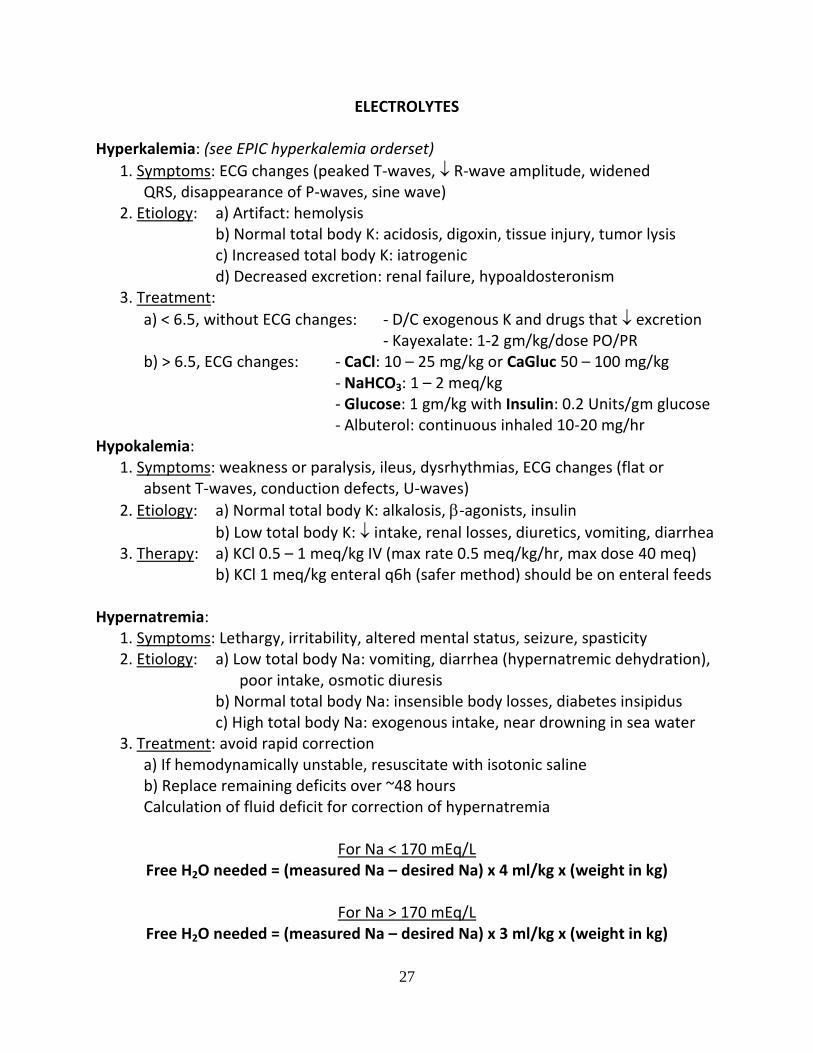
ELECTROLYTES Hyperkalemia: (see EPIC hyperkalemia orderset)
1. Symptoms: ECG changes (peaked T-waves, R-wave amplitude, widened QRS, disappearance of P-waves, sine wave) 2. Etiology: a) Artifact: hemolysis b) Normal total body K: acidosis, digoxin, tissue injury, tumor lysis c) Increased total body K: iatrogenic d) Decreased excretion: renal failure, hypoaldosteronism 3. Treatment:
a) < 6.5, without ECG changes: - D/C exogenous K and drugs that excretion - Kayexalate: 1-2 gm/kg/dose PO/PR b) > 6.5, ECG changes: - CaCl: 10 – 25 mg/kg or CaGluc 50 – 100 mg/kg - NaHCO3: 1 – 2 meq/kg - Glucose: 1 gm/kg with Insulin: 0.2 Units/gm glucose - Albuterol: continuous inhaled 10-20 mg/hr Hypokalemia: 1. Symptoms: weakness or paralysis, ileus, dysrhythmias, ECG changes (flat or absent T-waves, conduction defects, U-waves)
2. Etiology: a) Normal total body K: alkalosis, -agonists, insulin
b) Low total body K: intake, renal losses, diuretics, vomiting, diarrhea 3. Therapy: a) KCl 0.5 – 1 meq/kg IV (max rate 0.5 meq/kg/hr, max dose 40 meq) b) KCl 1 meq/kg enteral q6h (safer method) should be on enteral feeds Hypernatremia: 1. Symptoms: Lethargy, irritability, altered mental status, seizure, spasticity 2. Etiology: a) Low total body Na: vomiting, diarrhea (hypernatremic dehydration), poor intake, osmotic diuresis b) Normal total body Na: insensible body losses, diabetes insipidus c) High total body Na: exogenous intake, near drowning in sea water 3. Treatment: avoid rapid correction a) If hemodynamically unstable, resuscitate with isotonic saline b) Replace remaining deficits over ~48 hours Calculation of fluid deficit for correction of hypernatremia
For Na < 170 mEq/L Free H2O needed = (measured Na – desired Na) x 4 ml/kg x (weight in kg)
For Na > 170 mEq/L
Free H2O needed = (measured Na – desired Na) x 3 ml/kg x (weight in kg)
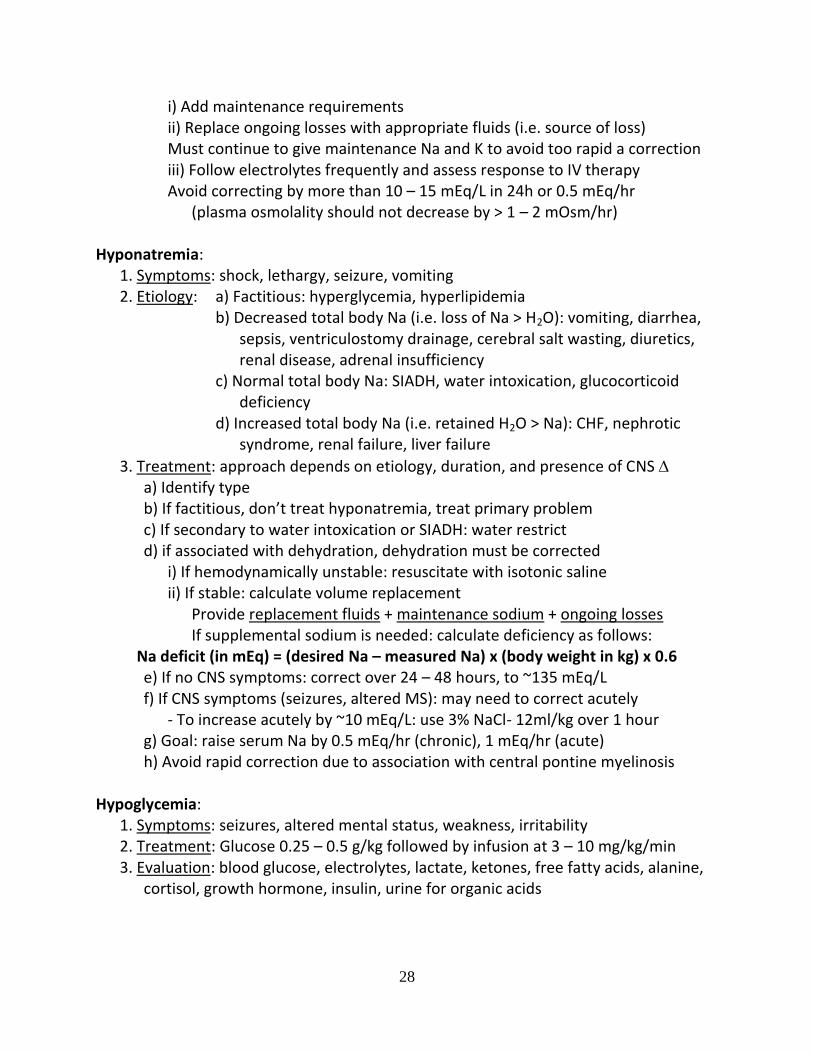
28
i) Add maintenance requirements ii) Replace ongoing losses with appropriate fluids (i.e. source of loss) Must continue to give maintenance Na and K to avoid too rapid a correction iii) Follow electrolytes frequently and assess response to IV therapy Avoid correcting by more than 10 – 15 mEq/L in 24h or 0.5 mEq/hr (plasma osmolality should not decrease by > 1 – 2 mOsm/hr) Hyponatremia: 1. Symptoms: shock, lethargy, seizure, vomiting 2. Etiology: a) Factitious: hyperglycemia, hyperlipidemia b) Decreased total body Na (i.e. loss of Na > H2O): vomiting, diarrhea, sepsis, ventriculostomy drainage, cerebral salt wasting, diuretics, renal disease, adrenal insufficiency c) Normal total body Na: SIADH, water intoxication, glucocorticoid deficiency d) Increased total body Na (i.e. retained H2O > Na): CHF, nephrotic syndrome, renal failure, liver failure
3. Treatment: approach depends on etiology, duration, and presence of CNS a) Identify type b) If factitious, don’t treat hyponatremia, treat primary problem c) If secondary to water intoxication or SIADH: water restrict d) if associated with dehydration, dehydration must be corrected i) If hemodynamically unstable: resuscitate with isotonic saline ii) If stable: calculate volume replacement Provide replacement fluids + maintenance sodium + ongoing losses If supplemental sodium is needed: calculate deficiency as follows:
Na deficit (in mEq) = (desired Na – measured Na) x (body weight in kg) x 0.6 e) If no CNS symptoms: correct over 24 – 48 hours, to ~135 mEq/L f) If CNS symptoms (seizures, altered MS): may need to correct acutely - To increase acutely by ~10 mEq/L: use 3% NaCl- 12ml/kg over 1 hour g) Goal: raise serum Na by 0.5 mEq/hr (chronic), 1 mEq/hr (acute) h) Avoid rapid correction due to association with central pontine myelinosis Hypoglycemia: 1. Symptoms: seizures, altered mental status, weakness, irritability 2. Treatment: Glucose 0.25 – 0.5 g/kg followed by infusion at 3 – 10 mg/kg/min 3. Evaluation: blood glucose, electrolytes, lactate, ketones, free fatty acids, alanine, cortisol, growth hormone, insulin, urine for organic acids

29
ENDOCRINE
DIABETIC KETOACIDOSIS a) Calculations: - Serum Osmolality = 2(Na) + (BUN) / 2.8 + (Glucose) / 18 - Corrected Sodium = Na + 1.6 [(Glucose – 100) / 100] - Serum Potassium: Levels rise 0.6mM for each 0.1 unit in serum pH b) Fluids: i) Resuscitation: bolus 10 – 20 ml/kg of NS for hemodynamic instability. Otherwise correct deficit slowly ii) Calculate fluid deficit based on degree of dehydration (see page 25) iii) Subtract amount given during resuscitation iv) Distribute the remainder over the next 48 hours (72 hours if severe hyperosmolality at onset) v) Add maintenance fluid required to fluid calculated for deficit
**USE DKA NAVIGATOR in MAESTRO CARE for 2 bag system** No dextrose bag Dextrose bag *NS + *D10 ½ NS + KCL 15 – 30 mEq/L + KCL 15 – 30 mEq/L + Kphos 15 – 30 mEq/L Kphos 15 – 30 mEq/L
*Consider half- or full acetate rather than full chloride. For children < 5 yr: use ¾ NS. Consider using NS if serum Na < 132 or > 150, or if corrected Na is < 140 or is decreasing with therapy.
When initial BG ≥ 800
BG No dextrose bag Dextrose Bag
> 501 100% Zero
401 – 500 75% 25%
301 – 400 50% 50%
201 – 300 25% 75%
< 200 Zero 100%
< 60 Zero 125%
When initial BG < 800
BG No dextrose bag Dextrose Bag
> 350 100% Zero
301 – 350 75% 25%
251 – 300 50% 50%
201 – 250 25% 75%
< 200 Zero 100%
< 60 Zero 125%
30
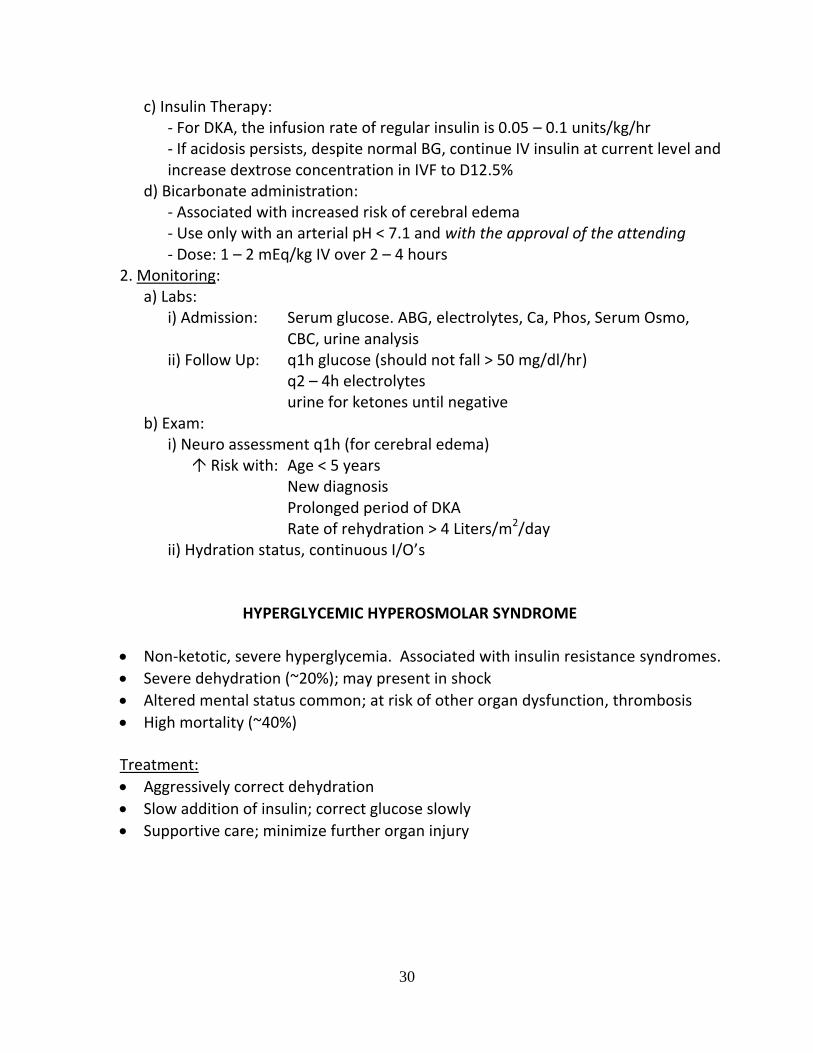
c) Insulin Therapy: - For DKA, the infusion rate of regular insulin is 0.05 – 0.1 units/kg/hr - If acidosis persists, despite normal BG, continue IV insulin at current level and increase dextrose concentration in IVF to D12.5% d) Bicarbonate administration: - Associated with increased risk of cerebral edema - Use only with an arterial pH < 7.1 and with the approval of the attending - Dose: 1 – 2 mEq/kg IV over 2 – 4 hours 2. Monitoring: a) Labs: i) Admission: Serum glucose. ABG, electrolytes, Ca, Phos, Serum Osmo, CBC, urine analysis ii) Follow Up: q1h glucose (should not fall > 50 mg/dl/hr) q2 – 4h electrolytes urine for ketones until negative b) Exam: i) Neuro assessment q1h (for cerebral edema) Risk with: Age < 5 years New diagnosis Prolonged period of DKA Rate of rehydration > 4 Liters/m2/day ii) Hydration status, continuous I/O’s
HYPERGLYCEMIC HYPEROSMOLAR SYNDROME
Non-ketotic, severe hyperglycemia. Associated with insulin resistance syndromes.
Severe dehydration (~20%); may present in shock
Altered mental status common; at risk of other organ dysfunction, thrombosis
High mortality (~40%) Treatment:
Aggressively correct dehydration
Slow addition of insulin; correct glucose slowly
Supportive care; minimize further organ injury
31
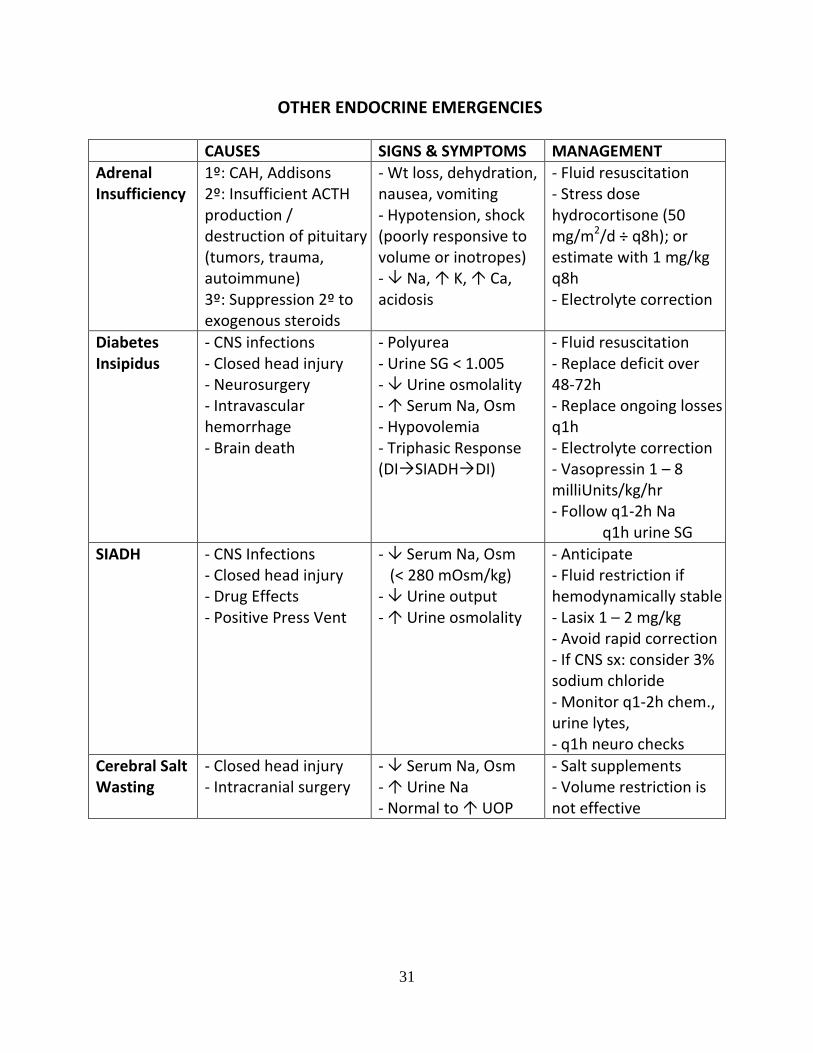
OTHER ENDOCRINE EMERGENCIES
CAUSES SIGNS & SYMPTOMS MANAGEMENT
Adrenal Insufficiency
1º: CAH, Addisons 2º: Insufficient ACTH production / destruction of pituitary (tumors, trauma, autoimmune) 3º: Suppression 2º to exogenous steroids
- Wt loss, dehydration, nausea, vomiting - Hypotension, shock (poorly responsive to volume or inotropes) - Na, K, Ca, acidosis
- Fluid resuscitation - Stress dose hydrocortisone (50 mg/m2/d ÷ q8h); or estimate with 1 mg/kg q8h - Electrolyte correction
Diabetes Insipidus
- CNS infections - Closed head injury - Neurosurgery - Intravascular hemorrhage - Brain death
- Polyurea - Urine SG < 1.005 - Urine osmolality - Serum Na, Osm - Hypovolemia - Triphasic Response (DISIADHDI)
- Fluid resuscitation - Replace deficit over 48-72h - Replace ongoing losses q1h - Electrolyte correction - Vasopressin 1 – 8 milliUnits/kg/hr - Follow q1-2h Na q1h urine SG
SIADH - CNS Infections - Closed head injury - Drug Effects - Positive Press Vent
- Serum Na, Osm (< 280 mOsm/kg) - Urine output - Urine osmolality
- Anticipate - Fluid restriction if hemodynamically stable - Lasix 1 – 2 mg/kg - Avoid rapid correction - If CNS sx: consider 3% sodium chloride - Monitor q1-2h chem., urine lytes, - q1h neuro checks
Cerebral Salt Wasting
- Closed head injury - Intracranial surgery
- Serum Na, Osm - Urine Na - Normal to UOP
- Salt supplements - Volume restriction is not effective
32
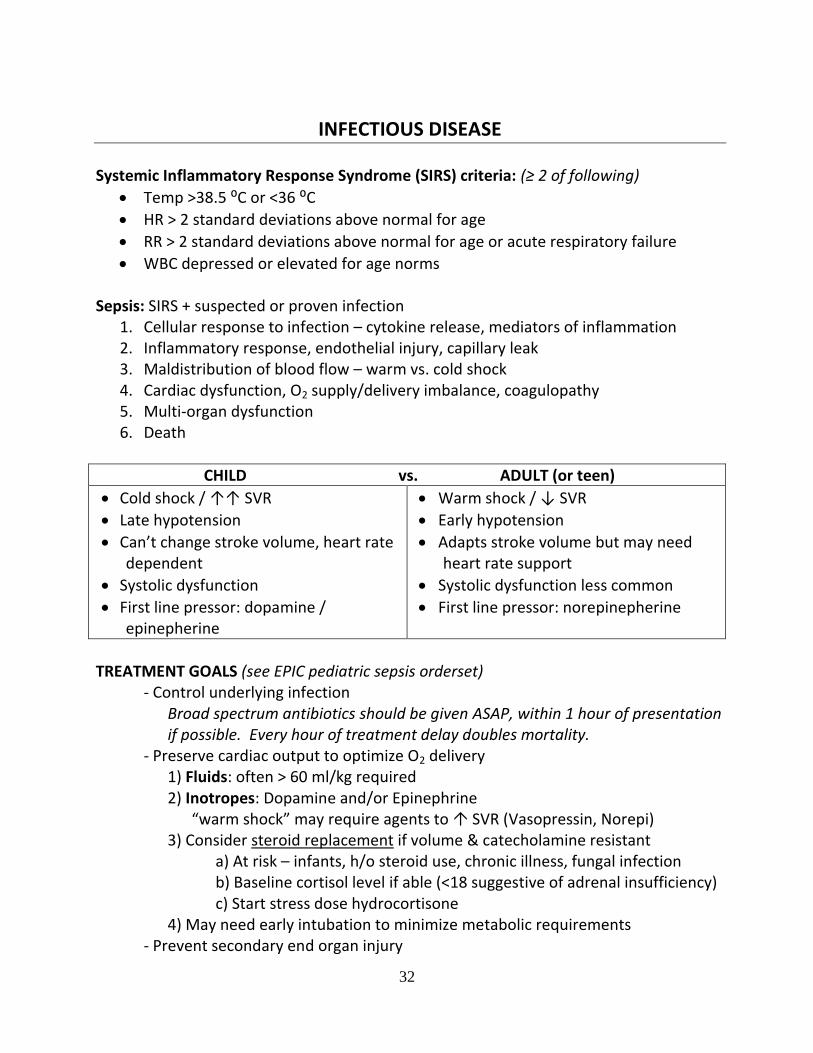
INFECTIOUS DISEASE Systemic Inflammatory Response Syndrome (SIRS) criteria: (≥ 2 of following)
Temp >38.5 ⁰C or <36 ⁰C
HR > 2 standard deviations above normal for age
RR > 2 standard deviations above normal for age or acute respiratory failure
WBC depressed or elevated for age norms Sepsis: SIRS + suspected or proven infection
1. Cellular response to infection – cytokine release, mediators of inflammation 2. Inflammatory response, endothelial injury, capillary leak 3. Maldistribution of blood flow – warm vs. cold shock 4. Cardiac dysfunction, O2 supply/delivery imbalance, coagulopathy 5. Multi-organ dysfunction 6. Death
CHILD vs. ADULT (or teen)
Cold shock / ↑↑ SVR
Late hypotension
Can’t change stroke volume, heart rate dependent
Systolic dysfunction
First line pressor: dopamine / epinepherine
Warm shock / ↓ SVR
Early hypotension
Adapts stroke volume but may need heart rate support
Systolic dysfunction less common
First line pressor: norepinepherine
TREATMENT GOALS (see EPIC pediatric sepsis orderset) - Control underlying infection
Broad spectrum antibiotics should be given ASAP, within 1 hour of presentation if possible. Every hour of treatment delay doubles mortality.
- Preserve cardiac output to optimize O2 delivery 1) Fluids: often > 60 ml/kg required 2) Inotropes: Dopamine and/or Epinephrine “warm shock” may require agents to SVR (Vasopressin, Norepi) 3) Consider steroid replacement if volume & catecholamine resistant a) At risk – infants, h/o steroid use, chronic illness, fungal infection b) Baseline cortisol level if able (<18 suggestive of adrenal insufficiency) c) Start stress dose hydrocortisone 4) May need early intubation to minimize metabolic requirements - Prevent secondary end organ injury
33
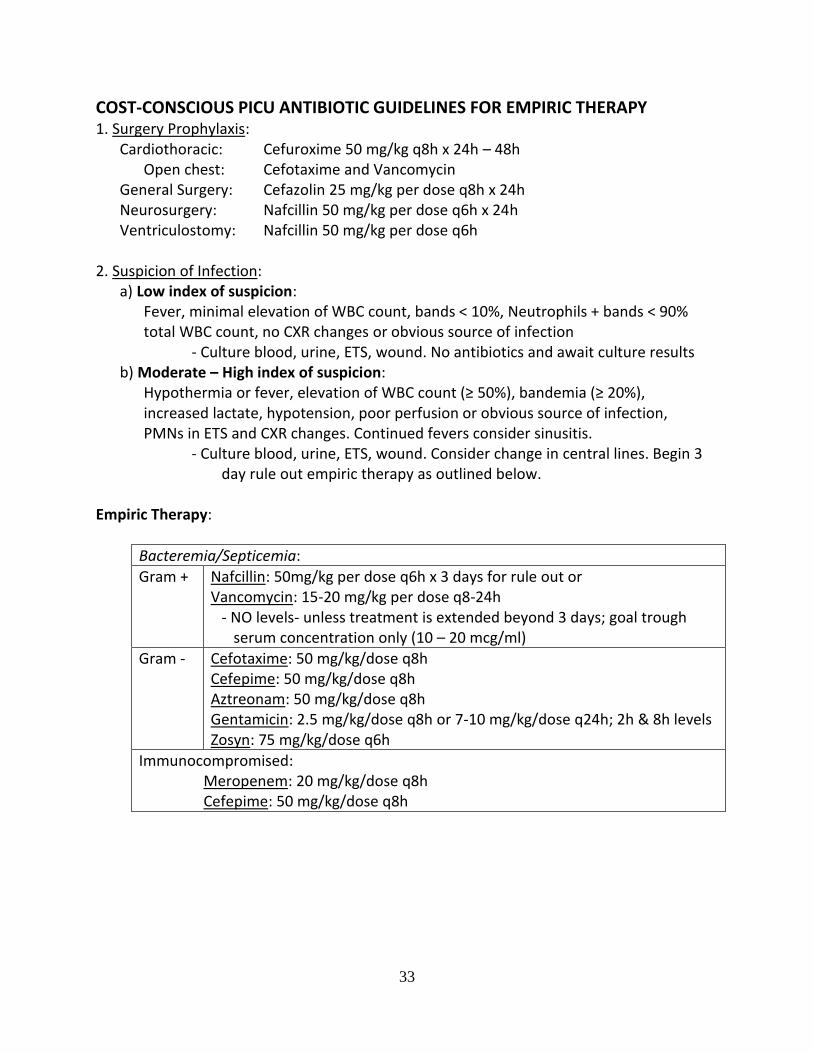
COST-CONSCIOUS PICU ANTIBIOTIC GUIDELINES FOR EMPIRIC THERAPY 1. Surgery Prophylaxis: Cardiothoracic: Cefuroxime 50 mg/kg q8h x 24h – 48h Open chest: Cefotaxime and Vancomycin General Surgery: Cefazolin 25 mg/kg per dose q8h x 24h Neurosurgery: Nafcillin 50 mg/kg per dose q6h x 24h Ventriculostomy: Nafcillin 50 mg/kg per dose q6h 2. Suspicion of Infection: a) Low index of suspicion: Fever, minimal elevation of WBC count, bands < 10%, Neutrophils + bands < 90% total WBC count, no CXR changes or obvious source of infection - Culture blood, urine, ETS, wound. No antibiotics and await culture results b) Moderate – High index of suspicion: Hypothermia or fever, elevation of WBC count (≥ 50%), bandemia (≥ 20%), increased lactate, hypotension, poor perfusion or obvious source of infection, PMNs in ETS and CXR changes. Continued fevers consider sinusitis.
- Culture blood, urine, ETS, wound. Consider change in central lines. Begin 3 day rule out empiric therapy as outlined below.
Empiric Therapy:
Bacteremia/Septicemia:
Gram + Nafcillin: 50mg/kg per dose q6h x 3 days for rule out or Vancomycin: 15-20 mg/kg per dose q8-24h
- NO levels- unless treatment is extended beyond 3 days; goal trough serum concentration only (10 – 20 mcg/ml)
Gram - Cefotaxime: 50 mg/kg/dose q8h Cefepime: 50 mg/kg/dose q8h Aztreonam: 50 mg/kg/dose q8h Gentamicin: 2.5 mg/kg/dose q8h or 7-10 mg/kg/dose q24h; 2h & 8h levels Zosyn: 75 mg/kg/dose q6h
Immunocompromised: Meropenem: 20 mg/kg/dose q8h Cefepime: 50 mg/kg/dose q8h

34
Meningitis:
< 6 weeks: Ampicillin: 100 mg/kg/dose q8h Cefotaxime: 100 mg/kg/dose q6h
6 wks – 3 m Cefotaxime: 50 mg/kg/dose q6h Vancomycin: 20 mg/kg/dose q8h + Ampicillin: 100 mg/kg/dose q8h if Listeria
> 3 month Cefotaxime: 100 mg/kg/dose q8h Vancomycin: 20 mg/kg/dose q8h **if cefotaxime resistant pneumococcus add Rifampin 10 mg/kg/dose q12h and maintain Vanc trough level 15-20 mcg/ml
HSV encephalitis
Acyclovir: 500 mg/m2/dose q8h
Pulmonary:
Cefotaxime: 65 mg/kg/dose q8h x 10 d if cx negative with clinical improvement
Neutropenic Cefepime: 50 mg/kg/dose q8h Vancomycin: 20 mg/kg/dose q8h
Tracheostomy Cefepime: 50 mg/kg/dose q8h or Piper/Tazo: 75 mg/kg/dose q6h Vancomycin: 20 mg/kg/dose q8h
Sickle Cell Cefotaxime: 65 mg/kg/dose q6h Vancomycin: 20 mg/kg/dose q8h
? Mycoplasma Azithromycin: 10 mg/kg/dose q24h x 5d
UTI:
Oral therapy TMP/SMX 5mg TMP/kg/dose q12h if possible Anaerobic coverage: Metronidazole 10 mg/kg/dose q8h Fungal: Fluconazole: 12 mg/kg/dose q24h Broader spectrum:
Ampicillin/Sulbactam: 50 mg/kg/dose q6h Piperacillin/Tazobactam: 75-100 mg/kg/dose q6h (gets Staph and Gram -) Clindamycin: 10 mg/kg/dose q6h (only covers 75% B. Fragilis at Duke) (gets Staph)

35
HEMATOLOGY
1. HEPARIN ADMINISTRATION PROTOCOL a) Loading dose: Heparin 75 – 100 units/kg over 10 min (often not given in post-op patients- requires surgical attending approval) b) Initial maintenance dose: 28 units/kg/hr for infants < 1 year c) Initial maintenance dose: 20 units/kg/hr for children > 1 year d) Adjust heparin for aPTT 60 – 85 sec (or anti-factor Xa / heparin level of 0.3 – 0.7) e) Obtain blood for aPTT 4 hours after administration of the heparin loading dose and 4 hours after every change in the infusion rate.
aPTT (sec) Bolus (units/kg) Hold (min) % Rate Change Repeat aPTT
< 50 50 0 + 10% 4 hours
50 – 59 0 0 + 10% 4 hours
60 – 85 0 0 0 Next day
86 – 95 0 0 - 10% 4 hours
96 – 120 0 30 - 10% 4 hours
> 120 0 60 - 10% 4 hours
When APTT values are therapeutic, obtain a daily CBC, aPTT, anti-Xa level Reversal: Protamine 1 mg = 100 units- use with caution- attending notification/guidance 2. WARFARIN PROTOCOL a) Loading dose: Day 1: if the baseline INR is 1 – 1.3 Dose = 0.2 mg/kg orally Day 2 – 4: INR Action 1.1 – 1.3 Repeat initial loading dose 1.4 – 1.9 50% of initial loading dose 2 – 3 50% of initial loading dose 3.1 – 3.5 25% of initial loading dose > 3.5 Hold until INR < 3.5, restart at 50% previous dose b) Maintenance oral anticoagulation dose guidelines: INR Action 1.1 – 1.4 Increase by 20% of dose 1.5 – 1.9 Increase by 10% of dose 2 – 3 No change 3.1 – 3.5 Decrease by 10% of dose > 3.5 Hold until INR < 3.5, then restart at 20% of previous dose c) Reversal: FFP, Vitamin K, KCentra (prothrombin complex)
36
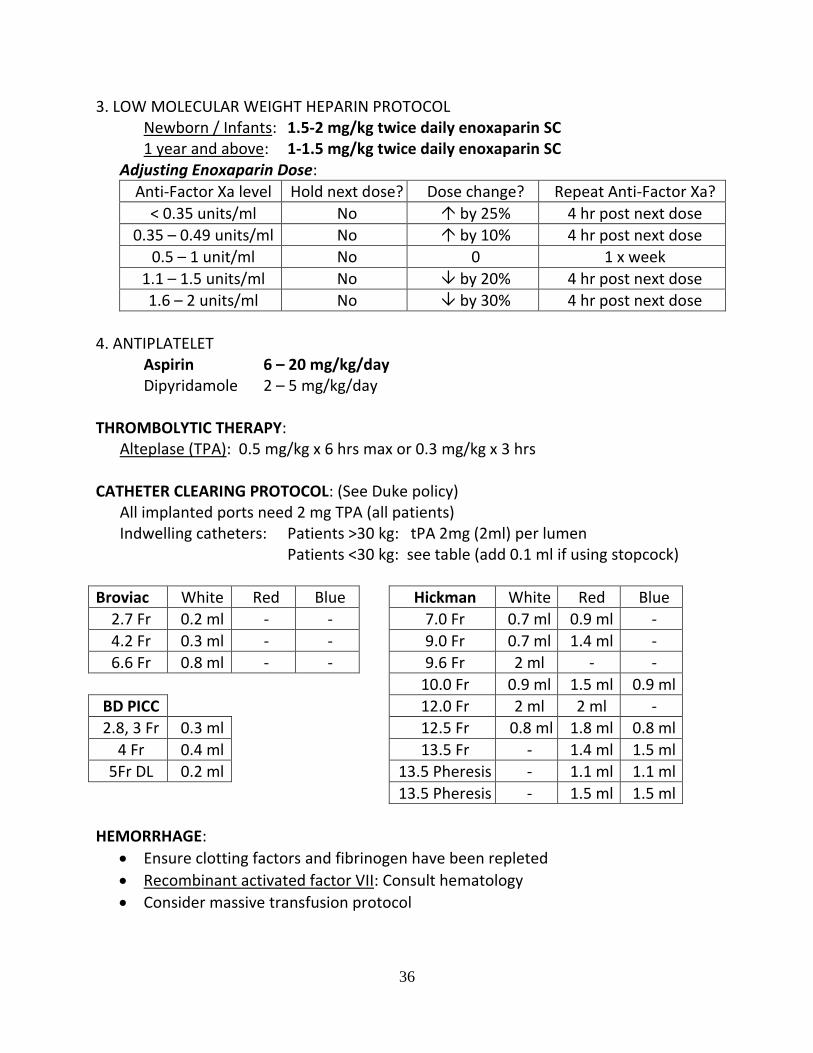
3. LOW MOLECULAR WEIGHT HEPARIN PROTOCOL Newborn / Infants: 1.5-2 mg/kg twice daily enoxaparin SC 1 year and above: 1-1.5 mg/kg twice daily enoxaparin SC Adjusting Enoxaparin Dose:
Anti-Factor Xa level Hold next dose? Dose change? Repeat Anti-Factor Xa?
< 0.35 units/ml No by 25% 4 hr post next dose
0.35 – 0.49 units/ml No by 10% 4 hr post next dose
0.5 – 1 unit/ml No 0 1 x week
1.1 – 1.5 units/ml No by 20% 4 hr post next dose
1.6 – 2 units/ml No by 30% 4 hr post next dose
4. ANTIPLATELET Aspirin 6 – 20 mg/kg/day Dipyridamole 2 – 5 mg/kg/day THROMBOLYTIC THERAPY: Alteplase (TPA): 0.5 mg/kg x 6 hrs max or 0.3 mg/kg x 3 hrs CATHETER CLEARING PROTOCOL: (See Duke policy) All implanted ports need 2 mg TPA (all patients) Indwelling catheters: Patients >30 kg: tPA 2mg (2ml) per lumen Patients <30 kg: see table (add 0.1 ml if using stopcock)
Broviac White Red Blue Hickman White Red Blue
2.7 Fr 0.2 ml - - 7.0 Fr 0.7 ml 0.9 ml -
4.2 Fr 0.3 ml - - 9.0 Fr 0.7 ml 1.4 ml -
6.6 Fr 0.8 ml - - 9.6 Fr 2 ml - -
10.0 Fr 0.9 ml 1.5 ml 0.9 ml
BD PICC 12.0 Fr 2 ml 2 ml -
2.8, 3 Fr 0.3 ml 12.5 Fr 0.8 ml 1.8 ml 0.8 ml
4 Fr 0.4 ml 13.5 Fr - 1.4 ml 1.5 ml
5Fr DL 0.2 ml 13.5 Pheresis - 1.1 ml 1.1 ml
13.5 Pheresis - 1.5 ml 1.5 ml
HEMORRHAGE:
Ensure clotting factors and fibrinogen have been repleted
Recombinant activated factor VII: Consult hematology
Consider massive transfusion protocol

37
NEUROLOGY
SEDATION / ANALGESIA
Acetaminophen 15 mg/kg q 4-6 hours; max 1000mg. IV for NPO patients: 12.5 mg/kg q4h or 15 mg/kg q6; max 1000mg Max daily dose (po or IV) 75 mg/kg or 4g
Midazolam Load 0.1 mg/kg; infuse 1 mcg/kg/min infusion by 1 mcg/kg/min after 0.1 mg/kg bolus Max: 15 mcg/kg/min
Morphine Load 0.1 mg/kg; infuse 50-100 mcg/kg/hr infusion by 20 mcg/kg/hr after 0.1 mg/kg bolus Max: 250 mcg/kg/hr
Dexmedetomidine Load 1-2 mcg/kg over 5-10 min; infuse 0.2-0.5 mcg/kg/hr infusion by 0.2-0.5 mcg/kg/hr after 0.5-1 mcg/kg bolus Max: 2.5 mcg/kg/hr
Lorazepam Load 0.1 mg/kg; infuse 0.1 mg/kg/hr infusion by 0.1 mg/kg/hr after 0.1 mg/kg bolus Max: 5 mg/hr; monitor serum osmolarity for infusions
Ketamine Load 1 – 2 mg/kg; infuse 5 – 20 mcg/kg/min Useful for asthmatics, drug holiday, or avoiding resp. depression Continue low dose benzos to prevent hallucinations
Fentanyl Load 1 – 2 mcg/kg; infuse 1 mcg/kg/hr infusion by 1 mcg/kg/hr after 1-2 mcg/kg bolus Max: 15 mcg/kg/hr Better cardiovascular stability than morphine (no histamine release)
Remifentanyl Good for pts with increased intracranial pressure Infusion: 0.05 mcg/kg/min – 2 mcg/kg/min (max) No bolus required- short t½ ; If requiring more, consider fentanyl
Propofol Restrict use for procedures or short term sedation (limit 12h) Load with 1 mg/kg; infuse 25 mcg/kg/min infusion by 25 mcg/kg/min after 1mg/kg bolus Max: 150 – 200 mcg/kg/min Stop all lipids; monitor q6 ABG and lactate, q12 CK, q24 serum TG
Ketorolac 0.5 mg/kg q6h x 48h for post-op patients Adult dose: 30 mg q6h; not approved for patients < 6 months
38
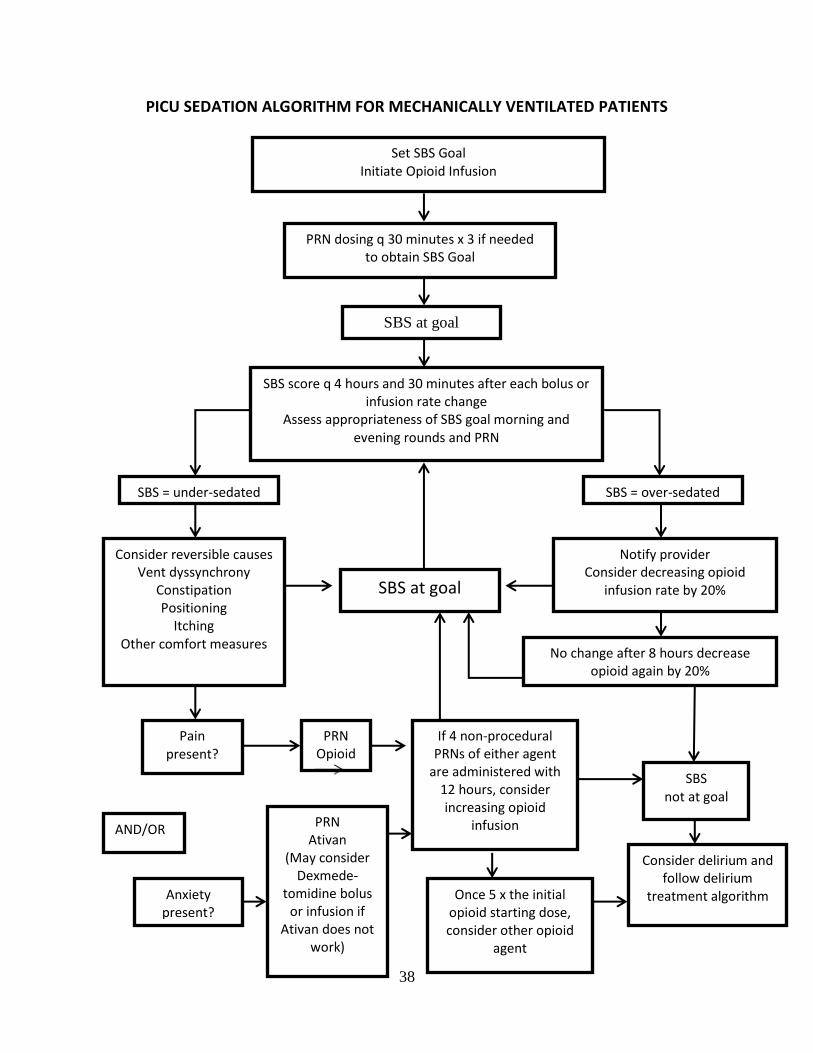
PICU SEDATION ALGORITHM FOR MECHANICALLY VENTILATED PATIENTS
Set SBS Goal Initiate Opioid Infusion
SBS at goal
PRN dosing q 30 minutes x 3 if needed to obtain SBS Goal
SBS score q 4 hours and 30 minutes after each bolus or infusion rate change
Assess appropriateness of SBS goal morning and evening rounds and PRN
Notify provider Consider decreasing opioid
infusion rate by 20%
Consider reversible causes Vent dyssynchrony
Constipation Positioning
Itching Other comfort measures
SBS = under-sedated
SBS at goal
Anxiety present?
Pain present?
If 4 non-procedural PRNs of either agent
are administered with 12 hours, consider increasing opioid
infusion PRN Ativan
(May consider Dexmede-
tomidine bolus or infusion if
Ativan does not work)
PRN Opioid
d SBS not at goal
Consider delirium and follow delirium
treatment algorithm
No change after 8 hours decrease opioid again by 20%
AND/OR
Once 5 x the initial opioid starting dose, consider other opioid
agent
SBS = over-sedated
39
STATUS EPILEPTICUS
1. Lorazepam 0.1 mg/kg IV for seizures > 5 min (may also give IM) 2. Repeat Lorazepam dose if needed 3. Phenobarbital 20 mg/kg (<2 yo) or Fosphenytoin 20 mg/kg (≥ 2yo)
Phenytoin caustic to veins and tissues – use fosphenytoin whenever possible, or ensure good IV or central line for phenytoin
Use fosphenytoin/phenytoin with caution with myocardial dysfxn
Check levels: 1-2 hrs for phenobarb, phenytoin 2 hrs for fosphenytoin
4. If seizure continues:
STAT neurology consult / EEG
STAT phenobarbital / phenytoin level (free and total)
Consider additional agents: Levetiracetam, Valproic Acid, etc. 5. Other options for persistent status:
Midazolam infusion up to 40 mcg/kg/min
Propofol infusion
Ketamine infusion
Pentobarbital coma / burst suppression
40
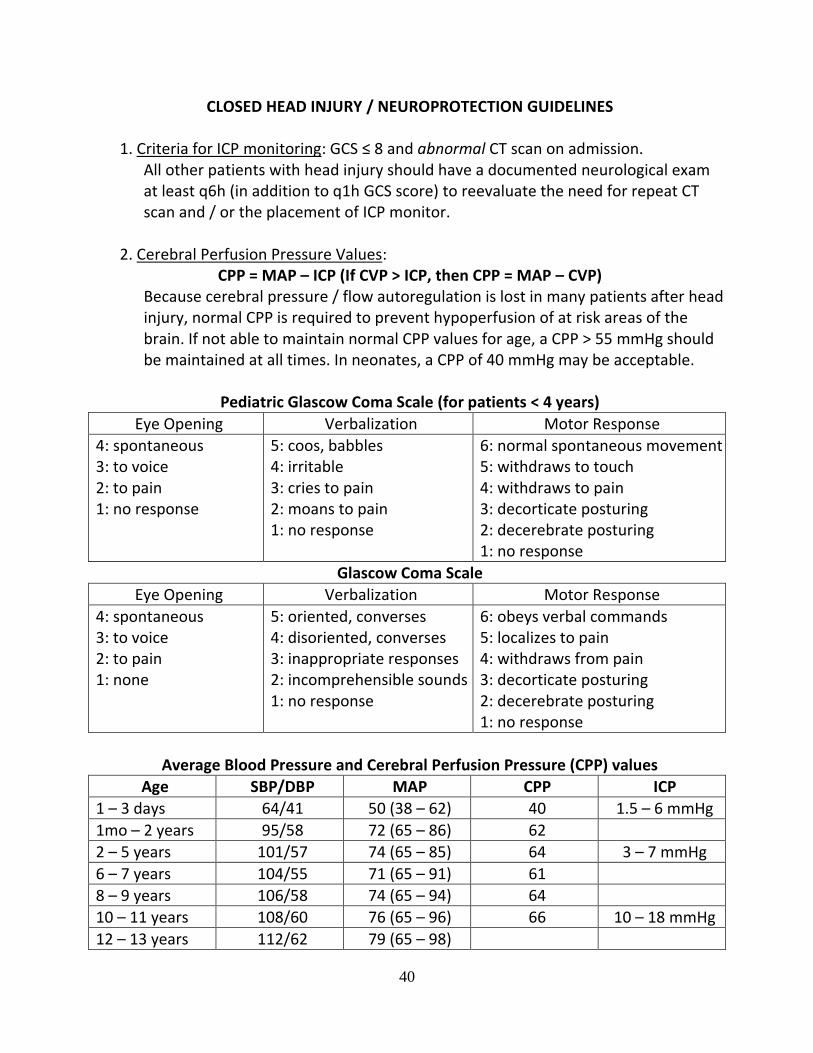
CLOSED HEAD INJURY / NEUROPROTECTION GUIDELINES
1. Criteria for ICP monitoring: GCS ≤ 8 and abnormal CT scan on admission. All other patients with head injury should have a documented neurological exam at least q6h (in addition to q1h GCS score) to reevaluate the need for repeat CT scan and / or the placement of ICP monitor.
2. Cerebral Perfusion Pressure Values: CPP = MAP – ICP (If CVP > ICP, then CPP = MAP – CVP)
Because cerebral pressure / flow autoregulation is lost in many patients after head injury, normal CPP is required to prevent hypoperfusion of at risk areas of the brain. If not able to maintain normal CPP values for age, a CPP > 55 mmHg should be maintained at all times. In neonates, a CPP of 40 mmHg may be acceptable.
Pediatric Glascow Coma Scale (for patients < 4 years)
Eye Opening Verbalization Motor Response
4: spontaneous 3: to voice 2: to pain 1: no response
5: coos, babbles 4: irritable 3: cries to pain 2: moans to pain 1: no response
6: normal spontaneous movement 5: withdraws to touch 4: withdraws to pain 3: decorticate posturing 2: decerebrate posturing 1: no response
Glascow Coma Scale
Eye Opening Verbalization Motor Response
4: spontaneous 3: to voice 2: to pain 1: none
5: oriented, converses 4: disoriented, converses 3: inappropriate responses 2: incomprehensible sounds 1: no response
6: obeys verbal commands 5: localizes to pain 4: withdraws from pain 3: decorticate posturing 2: decerebrate posturing 1: no response
Average Blood Pressure and Cerebral Perfusion Pressure (CPP) values
Age SBP/DBP MAP CPP ICP
1 – 3 days 64/41 50 (38 – 62) 40 1.5 – 6 mmHg
1mo – 2 years 95/58 72 (65 – 86) 62
2 – 5 years 101/57 74 (65 – 85) 64 3 – 7 mmHg
6 – 7 years 104/55 71 (65 – 91) 61
8 – 9 years 106/58 74 (65 – 94) 64
10 – 11 years 108/60 76 (65 – 96) 66 10 – 18 mmHg
12 – 13 years 112/62 79 (65 – 98)
41
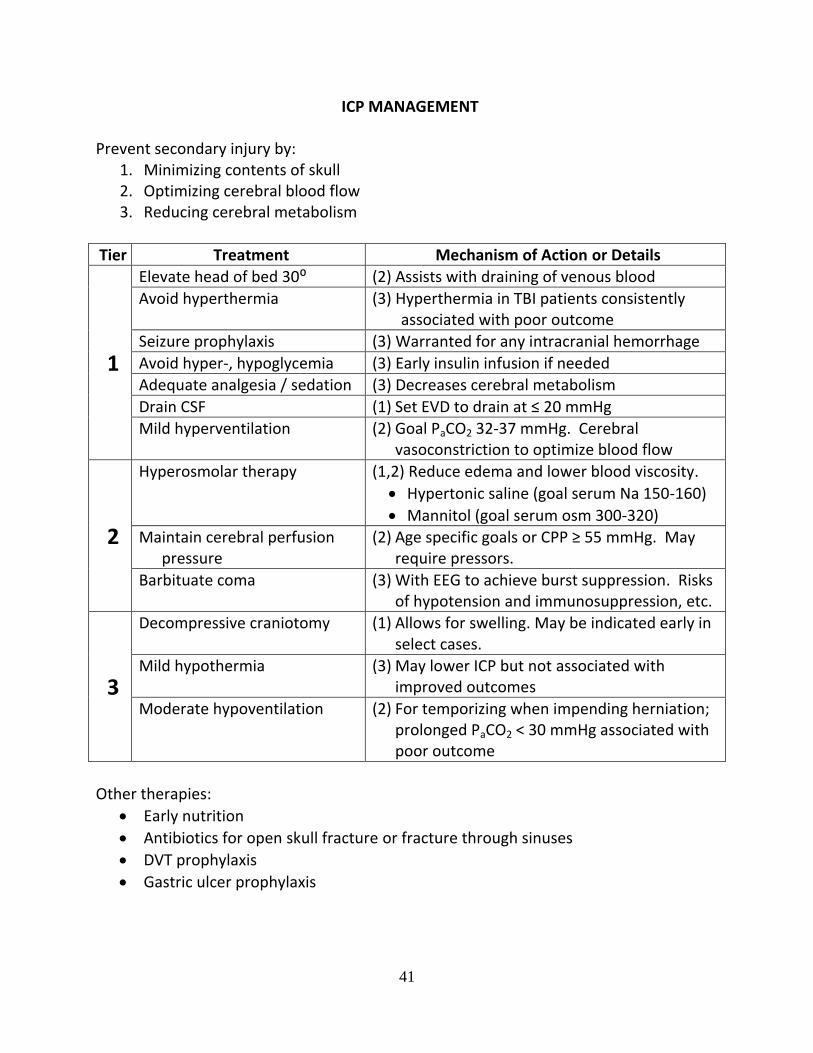
ICP MANAGEMENT
Prevent secondary injury by: 1. Minimizing contents of skull 2. Optimizing cerebral blood flow 3. Reducing cerebral metabolism
Tier Treatment Mechanism of Action or Details
1
Elevate head of bed 30⁰ (2) Assists with draining of venous blood
Avoid hyperthermia (3) Hyperthermia in TBI patients consistently associated with poor outcome
Seizure prophylaxis (3) Warranted for any intracranial hemorrhage
Avoid hyper-, hypoglycemia (3) Early insulin infusion if needed
Adequate analgesia / sedation (3) Decreases cerebral metabolism
Drain CSF (1) Set EVD to drain at ≤ 20 mmHg
Mild hyperventilation (2) Goal PaCO2 32-37 mmHg. Cerebral vasoconstriction to optimize blood flow
2
Hyperosmolar therapy (1,2) Reduce edema and lower blood viscosity.
Hypertonic saline (goal serum Na 150-160)
Mannitol (goal serum osm 300-320)
Maintain cerebral perfusion pressure
(2) Age specific goals or CPP ≥ 55 mmHg. May require pressors.
Barbituate coma (3) With EEG to achieve burst suppression. Risks of hypotension and immunosuppression, etc.
3
Decompressive craniotomy (1) Allows for swelling. May be indicated early in select cases.
Mild hypothermia (3) May lower ICP but not associated with improved outcomes
Moderate hypoventilation (2) For temporizing when impending herniation; prolonged PaCO2 < 30 mmHg associated with poor outcome
Other therapies:
Early nutrition
Antibiotics for open skull fracture or fracture through sinuses
DVT prophylaxis
Gastric ulcer prophylaxis
42
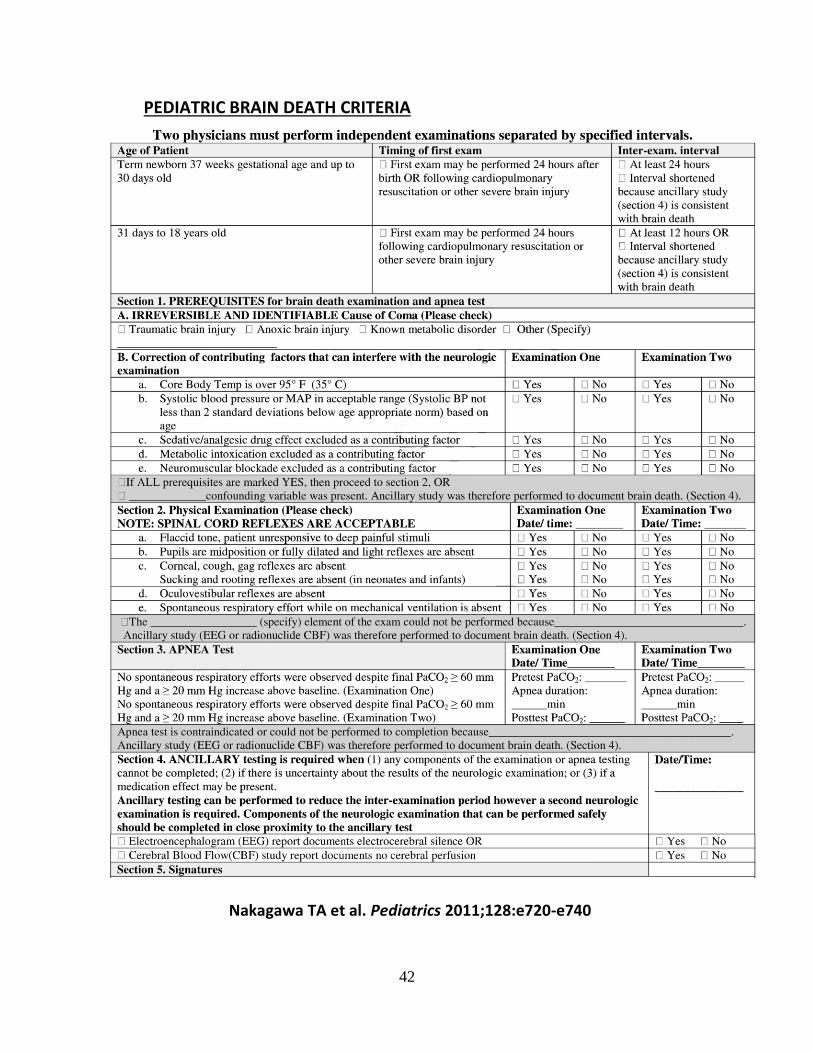
PEDIATRIC BRAIN DEATH CRITERIA
Nakagawa TA et al. Pediatrics 2011;128:e720-e740

43
USEFUL FORMULAS
Parameter Formula Normal Value
A-a Gradient [(713 x FiO2) – (PaCO2 / 8)] – PaO2 10 – 20 @ 21% 60 – 70 @ 100%
Oxygenation Index (OI) (MAP x FiO2) / PaO2 x 100
Oxygenation Saturation Index (OSI)
(MAP x FiO2) / SaO2 x 100 *Measure when SaO2 92-97%
PaO2 / FiO2 Ratio PaO2 / FiO2
Dynamic Compliance Vt / (PIP – PEEP)
Static Compliance Vt / (Pplat – PEEP)
Airway Resistance (PIP – Plateau Pressure) / Flow
Dead Space Fraction (PaCO2 – PECO2) / PaCO2 0.25 – 0.35
Arterial O2 Content (1.34 x hgb x arterial O2 sat) + (0.003 x PaO2)
18 – 21 ml/dl
Pulmonary Capillary Content
(hgb x 1.34) + (0.003 x PaO2)
Venous O2 Content (1.34 x hgb x venous O2 sat) + 0.003 x PaO2)
15 ml/dl
Art Blood Gas Rule 10 mmHg PaCO2 = 0.08 pH
CO2 Production Frequency x Vt x FECO2 3.2 ml/kg/min
Cardiac Output HR x SV 4 – 8 L/min
Cardiac Index CO / BSA 2.5 – 4 L/min
O2 Consumption CO x (CaO2 – CvO2) 115 – 165 ml/min/m2
O2 Delivery CO x CaO2 550 ml/min/m2
Qp / Qs (SaO2 – SvO2) / (SpvO2 – SpaO2)
Shunt Fraction (CcO2 – CaO2) / (CcO2 – CVO2) 3 – 8%
Pulm Vasc Resistance PAP – LAP / CI 2 – 4 woods or 50 – 150 dyn-sec/cm-5
Systemic Vasc Resistance
AO – CVP / CI < 20 woods or 900 – 1500 dyn-sec/cm-5
Starling Forces K (Pcap – Pint) - (cap – int)
Anion Gap Na – Cl – HCO3 8 – 12
Fractional Excretion of Sodium
Urine Na x Serum Creatinine Serum Na x Urine Creatinine
Body Surface Area (H (cm) x W (kg)) 60

44