Embed Size (px)
Citation preview

Thanks to our Sponsors
Sprague Israel Giles Inc. Finney, Neill & Co. P.S.



Remy Trupin, Executive Director
Kim Justice, Policy Analyst
Andy Nicholas, Senior Fiscal Analyst
TITLE


What Opportunities Does the
Exchange Offer Washington?
Emily Brice, Northwest Health Law AdvocatesDecember 2012

Easier Plan Comparisons
Qualified Health Plans Available to individual and small
group in Exchange Must meet certification criteria Will have metallic tiers indicating
actuarial value Goal: Make value clearer to
consumers Calculation: In-network, Essential
Health Benefits Tiers: Bronze – Platinum, plus limited
catastrophic (if under 30 or exempt from minimum essential coverage)

Richer Benefits
Essential Health Benefits Must cover 10 categories of services
Must be one of benchmark plans: Regence Innova (largest small group)
Must cover preventive services without cost-sharing Based on U.S. Preventive Services Task Force A & B
recommendations: www.healthcare.gov/news/factsheets/2010/07/preventive-services-list.html
This aspect largely already in effect
Ambulatory Rehabilitative & habilitative
Emergency Laboratory
Hospitalization Preventive, Wellness, & Chronic Disease Management
Maternity & Newborn Pediatric (including oral & vision)
Prescription Drugs Mental health & substance use disorder (including behavioral health)

Greater Affordability
Sliding Scale Subsidies & Cost Reductions Eligibility:
Under 400% FPL Not undocumented Not eligible for Medicaid, Medicare, CHIP, TriCare, etc. Not offered “affordable” coverage of “minimum value”
through employer Not actually enrolled in coverage through employer

Greater Affordability
Premium Tax Credits Cost-Sharing Reductions
Income Level
Maximum Premium
Up to 133% FPL
2% of income
133-150% FPL
3-4% of income
150-200% FPL
4-6.3% of income
200-250% FPL
6.3-8.05% of income
250-300% FPL
8.05-9.5% of income
300-400% FPL
9.5% of income
Income Level
Reduction in OOP Costs(compare to 70% silver)
100-150% 94% AV
150-200% 87% AV
200-250% 73% AV
• Select any AV tier except catastrophic
• Receive monthly in advance (paid directly to plan) or at close of tax year
• Possibility of reconciliation
• Select silver only! • Only applies to in-network, in-
EHB• Plus: For those under 400%
FPL, additional caps on maximum OOP spending

What Can Washington Do to Maximize
the Exchange Opportunity?

Promote Affordability
Above 400% FPL: Much still unknown about pricing...
Under 200% FPL: Even with subsidies, Exchange may be
unaffordable for 162,000 WA residents in this income bracket due to heightened price sensitivity.
Outcome: Many will remain uninsured, or enroll and then drop coverage.

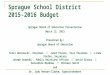
Promote Affordability: Basic Health Option
Source: Urban Institute, “Using the Basic Health Program to Make Coverage More Affordable to Low-Income Households” (2012)
Average Annual Costs for Adults Nationally with Incomes Between 138-200% FPL: BHP vs. Subsidized Coverage in the Exchange

Consumer Education
Trade-off: Plan Selection v. Cost-sharing Ex: 30-year old Ana earns 150% FPL.
Unsubsidized age-adjusted monthly premium for the second-lowest cost silver-level plan estimated at ~ $3,440 per member annually.
Based on her household size and income, Ana will pay a maximum of 4% of her income toward coverage – about $690 annually, or 20% of the total premium. She can receive a tax credit for the remaining 80% of the premium, $2,750.
Which plan will she choose? Silver Reference Plan
Bronze Plan
Net premium (annual after credit)
$690 Under $690
Cost-sharing Reduction
Yes ( 70% increases to 94%)
No (60%)
OOP Maximum Yes ($2,084) Yes ($2,083)Source of estimates: Kaiser Subsidy Calculator

Maintain Sustainable ExchangeFunding Exchange Operations? Insurance Premium Assessment
Starting 1/2014: Premium tax assessment totaling 0.5% of all premiums and prepayments for health care services received.
Starting 1/2015: Premium tax would rise to 1% of same.
Repurpose Existing Assessment (Hybrid) Starting 1/2014: Authorize and apportion to the Exchange the
premium tax collected on all premiums and prepayments for health care services attributable to the Exchange-generated premiums received.
Any funding shortfalls augmented by assessing a service charge payable by QHPs in the Exchange.
QHP Issuer-Based Revenue Model Starting 1/2014: Assess a service charge payable solely by QHPs
in the Exchange.

Stay Connected
@budget_policy
www.facebook.com/budgetandpolicy
Sign up for email updates at: www.budgetandpolicy.org
16
Kim Justice, Policy [email protected]