-
8/14/2019 Thacheal ion and Bronchial Intubation
1/87
1
Tracheal intubation
and
bronchial intubation
-
8/14/2019 Thacheal ion and Bronchial Intubation
2/87
2
DefinitionDefinition
Endotracheal intubationis inserting a
special tube into the trachea through
oral or nares via laryngeal.If this special tube is inserted
into
the bronchus ,we call itendobronchial
intubation.
-
8/14/2019 Thacheal ion and Bronchial Intubation
3/87
3
ApplicationsApplications
General anesthesia
Treatment of airway obstruction, difficult
respiration
Cardiopulmonary cerebral resuscitation
Treatment of severe acute emptysis
Examination of pulmonary function
Pulmonary toilet
-
8/14/2019 Thacheal ion and Bronchial Intubation
4/87
4
Intubation can be performed with
the patient awake (local anaesthesia)or under general
anaesthesia.
-
8/14/2019 Thacheal ion and Bronchial Intubation
5/87
5
Section 1
Preanesthesia Preparation and Anesthesia
-
8/14/2019 Thacheal ion and Bronchial Intubation
6/87
6
1.Physical Examination and Evaluation of
the Airway
Neck mobility
The atlanto-occipital joint and cervical spine mobility
particularly with
extension
It is related to aligning the oral,pharyngeal, and laryngeal
axes
.
-
8/14/2019 Thacheal ion and Bronchial Intubation
7/87
7
-
8/14/2019 Thacheal ion and Bronchial Intubation
8/87
8
Normal head extension: 165-90 degrees
Head extension 80 degrees:representing increasing limitation
and
increased potential fordifficult laryngoscopy
Diseases: cervical spine rheumatoidarthritis or tuberculosis
with atlantoaxial
subluxation
, cervical spine fracture,
severe cervical spondylosis , morbid obesity, burn and so
on.
-
8/14/2019 Thacheal ion and Bronchial Intubation
9/87
9
The thyromental distance From the inner surface of the mandible
to
the thyroid cartilage during neck extension
Normal:3-4 cm (two large fingerbreadths)
in adults. 3cm: exposure
of the glottis
may be
inadequate.
-
8/14/2019 Thacheal ion and Bronchial Intubation
10/87
10
Mouth openingNormal: 4-5 cm (about two large
fingerbreadths)
2.5 cm: difficult laryngoscopy
Diseases: temporomandibular jointankylosis , arthritis,
burn, trauma, radiation, transtemporalcraniotomy , large
tongue.
-
8/14/2019 Thacheal ion and Bronchial Intubation
11/87
11
Teeth Dentures
Loose teeth
EdentiaProtuberant upper incisors
-
8/14/2019 Thacheal ion and Bronchial Intubation
12/87
12
Mallampati classes
-
8/14/2019 Thacheal ion and Bronchial Intubation
13/87
13
Nose: nasal obstruction, nasal trauma, epistaxis and
nasopharyngeal
surgery
Pharynx: inflammatory masses such as tonsillarhyperplasia,
retropharyngeal abscess
Larynx: laryngitis, laryngeal stenosis
-
8/14/2019 Thacheal ion and Bronchial Intubation
14/87
14
Trachea:tracheal stenosisresulted from:
the extrinsic airway compressionof
cervical mass, thyromegaly and aorta aneurysm
tracheal trauma
tracheotomy
luminal tumors
-
8/14/2019 Thacheal ion and Bronchial Intubation
15/87
15
2. Equipment of endotracheal intubation
Endotracheal Tubes
Material: rubber, plastic
or polyvinylchloride
Demand: The tube is freeof toxic, irritant or allergenic
properties. The tube wall
should be smooth and as thin
as possible.
-
8/14/2019 Thacheal ion and Bronchial Intubation
16/87
16
Types Internal diameter (ID) size: It reflects theinternal
diameter of the tube. Tubes are
manufactured in 0.5 mm ID increments from
2.0 to 9.0 mm.French size: It reflects the circumference
of the tube, it is the product of external
diameter and , and is therefore higher for
thicker-walled tubes than for thinner-walledtubes with the same
ID.
F size ID size4 2
-
8/14/2019 Thacheal ion and Bronchial Intubation
17/87
17
Choice of endotracheal tube sizes Adults adult males 8.0 mm
ID
adult females 7.0 mm ID
Given the variation between individuals, atube of 1 mm ID
sizesmallerorlargermay be
available for an individual patient.
nasal intubation 7.0 7.5mm ID
-
8/14/2019 Thacheal ion and Bronchial Intubation
18/87
18
Children:
formula: age 18 (French size)orage/4 4.5 (ID size)
Variation between individuals requires the
availability of 0.5 mm ID smallerand largertube
sizes. Uncuffed endotracheal tubes have generally
been used in children younger than 5 years old.
If there is a suspicion of laryngeal or tracheal
disease in any age group, smaller tubes should be
available.
-
8/14/2019 Thacheal ion and Bronchial Intubation
19/87
19
-
8/14/2019 Thacheal ion and Bronchial Intubation
20/87
20
Distance of insertion adult males about23 cmat the lips,
with thetube tipto be placed in themid-
trachea and an appropriate4 cmabove the
carina.
adult females about21 cm
children can be estimated from the
formula:12 + (age/2).
-
8/14/2019 Thacheal ion and Bronchial Intubation
21/87
21
CuffFunction to protect the airway from aspiration
and air leak on positive-pressure inspiration.
Types and characteristicslow-volume, high-pressure cuffs
high-volume, low-pressure cuffs
-
8/14/2019 Thacheal ion and Bronchial Intubation
22/87
22
Laryngoscope
Configuration and classificationlaryngoscope handle
laryngoscope blade: straight blade
curved blade
-
8/14/2019 Thacheal ion and Bronchial Intubation
23/87
23
Advantages and disadvantages of both
laryngoscopes
LaryngoscopeMove tongue and epiglottis
Allows visualization of cords and glottisMiller- straight
--Lift epiglottis
--pediatrics
Macintosh- curved--Fits in vallecula
--More room for visualization
--Reduced trauma/ gag reflex
-
8/14/2019 Thacheal ion and Bronchial Intubation
24/87
24
Fiberoptic bronchoscope
-
8/14/2019 Thacheal ion and Bronchial Intubation
25/87
25
Other equipment for endtracheal intubation
Connector
Stylet:It is a rigid implement usually made of
a flexible metal or rubber.
Forceps: Magill forceps and Rovenstine forceps
Bite block
Sprayer
-
8/14/2019 Thacheal ion and Bronchial Intubation
26/87
26
Preparation before endotracheal intubation
endotracheal tubes
laryngoscopeother essential items stylet, bite block, oxygen
source, bag and mask, airway, lubricant, tape, reliable
suction, anesthetic and monitoring apparatus.
-
8/14/2019 Thacheal ion and Bronchial Intubation
27/87
27
3. Anesthesia for endotracheal intubation
Anesthesia induction rapid-sequence induction
intravenous induction and intubation:
rapidly acting intravenous induction agents
and rapidly acting muscle relaxant inhalational induction and
intubation
Indications:Patients are not likely to
present difficult intubation.
-
8/14/2019 Thacheal ion and Bronchial Intubation
28/87
28
Local anesthesia
Indications:difficult intubation, severe risk forairway
obstruction or aspiration.
Topical anesthesia(Surface anesthesia)
The superior laryngeal nerve (SLN) blocking
Transtracheal anesthesia
-
8/14/2019 Thacheal ion and Bronchial Intubation
29/87
29
Local anesthesia combines general anesthesia
Indication:difficult intubation patients who
have the ability to maintain mask ventilation.
-
8/14/2019 Thacheal ion and Bronchial Intubation
30/87
30
Section 2 Endotracheal Intubation
-
8/14/2019 Thacheal ion and Bronchial Intubation
31/87
31
Classification
On the base ofintubating path:
oral endotracheal intubation
nasal endotracheal intubationOn the base ofglottis
visulization:
visualized intubation
blind intubation
Routes for Intubation
Orotracheal
Nasotracheal
Tracheotomy
-
8/14/2019 Thacheal ion and Bronchial Intubation
32/87
32
1.Indications and Advantages
Indications
General anesthesia
Respiratory treatmentCardiopulmonary resuscitation
-
8/14/2019 Thacheal ion and Bronchial Intubation
33/87
33
AdvantagesControls the airwayFacilitates ventilation/ O2
Prevents gastric inflationAllows for direct suctioningMedication
administration
-
8/14/2019 Thacheal ion and Bronchial Intubation
34/87
34
Contraindications
absolute contraindications:
laryngeal edema
acute airway inflammation
relative contraindications:
tracheal compression of aorta aneurysm
coagulopathy or other severe bleeding
diathesis
-
8/14/2019 Thacheal ion and Bronchial Intubation
35/87
35
2. Visualized oral endotracheal intubationIn
Mask ventilation
Head position for visualized
oral endotracheal intubation
Laryngoscope insertion
Endotracheal tube was insertedinto the glottis
-
8/14/2019 Thacheal ion and Bronchial Intubation
36/87
36
-
8/14/2019 Thacheal ion and Bronchial Intubation
37/87
37
-
8/14/2019 Thacheal ion and Bronchial Intubation
38/87
38
-
8/14/2019 Thacheal ion and Bronchial Intubation
39/87
39
-
8/14/2019 Thacheal ion and Bronchial Intubation
40/87
40
Advantages of Oral IntubationAdvantages of Oral Intubation
Larger tube can be insertedTube can be inserted usually with
more
speed and ease with less traumaEasier suctioningLess airflow
resistanceReduced risk of tube kinking
-
8/14/2019 Thacheal ion and Bronchial Intubation
41/87
41
Disadvantages of Oral Intubation
Gagging, coughing, salivation, and
irritation can be induced with intact airway
reflexes
Tube fixation is difficult, self-extubationGastric distention
from frequent
swallowing of airMucosal irritation and ulcerations of mouth
(change tube position)
-
8/14/2019 Thacheal ion and Bronchial Intubation
42/87
42
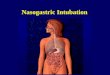
3. Nasal endotracheal intubation
Indications:surgery in the oral cavity anatomic distortion or
upper airway
diseases which limit direct laryngoscopy long time mechanical
ventilation postoperation difficult airway situations
-
8/14/2019 Thacheal ion and Bronchial Intubation
43/87
43
Contraindications
coagulopathy or other severe bleeding diathesis severe
intranasal disorder
basilar skull fracture cerebrospinal fluid leak
-
8/14/2019 Thacheal ion and Bronchial Intubation
44/87
44
Classfication
Visualized nasal intubation
Blind nasal intubation
-
8/14/2019 Thacheal ion and Bronchial Intubation
45/87
45
-
8/14/2019 Thacheal ion and Bronchial Intubation
46/87
46
Advantages of Nasal Intubation
More comfort long termDecreased gaggingLess salivation, easier
to swallow
Improved mouth careBetter tube fixationImproved
communication
-
8/14/2019 Thacheal ion and Bronchial Intubation
47/87
47
Disadvantages of Nasal Intub..
Pain and discomfortNasal and paranasal complications, I.e.,
epistaxis, sinusitis, otitis
More difficult procedureSmaller tube neededIncreased airflow
resistanceDifficult suctioning
Bacteremia
-
8/14/2019 Thacheal ion and Bronchial Intubation
48/87
48
4. Intubation of difficult airway
Fiberoptic bronchoscope intubation
Anterograde endotracheal intubation
Retrograde endotracheal intubation
5. Tube exchanging
(4)Laryngeal mask airway
(5)Esophageal-Tracheal Combitube
-
8/14/2019 Thacheal ion and Bronchial Intubation
49/87
49
6. Tracheotomy
-
8/14/2019 Thacheal ion and Bronchial Intubation
50/87
50
-
8/14/2019 Thacheal ion and Bronchial Intubation
51/87
51
-
8/14/2019 Thacheal ion and Bronchial Intubation
52/87
52
-
8/14/2019 Thacheal ion and Bronchial Intubation
53/87
53
-
8/14/2019 Thacheal ion and Bronchial Intubation
54/87
54
-
8/14/2019 Thacheal ion and Bronchial Intubation
55/87
55
-
8/14/2019 Thacheal ion and Bronchial Intubation
56/87
56
DisplacementTracheal tubes can be displaced after
correctinsertion. This is particularly likely when the patient
is moved or the position changed. Flexion or
extension of the head, or lateral neck movement, hasbeen shown
to cause movement of the tube of up to 5
cm within the trachea. Tracheal tubes should be fixed
securely to minimise accidental extubation and the
correct positioning should be checked regularly.
-
8/14/2019 Thacheal ion and Bronchial Intubation
57/87
57
C fi ti f t h l i t b ti
-
8/14/2019 Thacheal ion and Bronchial Intubation
58/87
58
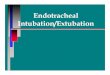
Confirmation of tracheal intubation
Clinical signs used to confirm tracheal intubatio
Direct visualisation of tracheal tube through vocal cords
Palpation of tube movement within the trachea
Chest movements
Breath sounds
Reservoir bag compliance and refill
Condensation of water vapour on clear tracheal tubes
-
8/14/2019 Thacheal ion and Bronchial Intubation
59/87
59
Section 3 Endobronchial Intubation
-
8/14/2019 Thacheal ion and Bronchial Intubation
60/87
60
1.Indications Advantages and DisadvantagesIndications
wet lung patients: severe emptysis
pulmonary abscess
bronchodilatationbronchopleural fistula
tracheoesophageal fistula
traumatic fraction of bronchus
tracheoplasty or bronchoplasty
-
8/14/2019 Thacheal ion and Bronchial Intubation
61/87
61
AdvantagesPrevent contamination or spillage:
infection ,hemorrage ,brochopulmonary lavageControl of the
distribution of ventilation:
bronchopleural fistulaEnhance surgical exposure:
pneumonectomy
Disadvantages
right-to left intrapulmonary shunt :arterial hypoxemia
-
8/14/2019 Thacheal ion and Bronchial Intubation
62/87
62
2. Double-lumen endobronchial intubation
Types Carlens double-lumen endobronchial tubes
White double-lumen endobronchial tubes
Robertshaw double-lumen endobronchial tubes
-
8/14/2019 Thacheal ion and Bronchial Intubation
63/87
63
-
8/14/2019 Thacheal ion and Bronchial Intubation
64/87
64
Section 4 Extubation
-
8/14/2019 Thacheal ion and Bronchial Intubation
65/87
65
Liberating from ETT
Obtain weaning parameters:
NIF (Negative inspiratory force) > -20 cmH2O
VC >10-15 mL/kg
Ve < 12 lpm
RR >10 or 5mL/kg IBW
-
8/14/2019 Thacheal ion and Bronchial Intubation
66/87
66
Extubation ProcedureExtubation Procedure
Assemble Equipment
- intubation equipment
- in addition to intubation
equipment, O2 device
and humidity, SVN (small-
volume nebulizer with
racemic epinephrineSuction ET tubeOxygenate patientUnsecure
tube, deflate cuff
-
8/14/2019 Thacheal ion and Bronchial Intubation
67/87
67
Extubation proced. (contd.)Extubation proced. (contd.)
Place suction catheter down tube and
remove ET tube as you suction
Apply appropriate O2 and humidityAssess/Reassess the patient
-
8/14/2019 Thacheal ion and Bronchial Intubation
68/87
68
Section 5 Complications of Endotracheal
and Endobronchial Intubation
-
8/14/2019 Thacheal ion and Bronchial Intubation
69/87
69
Complications during larngoscopy and intuation
1. Teeth and soft tissue injury1. Teeth and soft tissue
injury
Causes The laryngoscope is used improperly.
Laryngoscopy is particularly difficult.
There is dental/periodontal disease.
C li i d i l d i iC li ti d i l d i t ti
-
8/14/2019 Thacheal ion and Bronchial Intubation
70/87
70
Complications during larngoscopy and intuationComplications
during larngoscopy and intuation
2. Hypertension and arrhythmiaCause Stress reaction to
laryngoscopy and
intubationplasm catecholamine increase
Prevention
Maintaining adequate anesthetic depthAdministration of
appropriate fentanyl,
lidocaine, nitroglycerin or esmolol intravenously
before laryngoscopy
Sufficient topical anesthesia with lidocaine
Preoxygenate and adequately ventilate the patient
to prevent hypoxemia and hypercarbia
-
8/14/2019 Thacheal ion and Bronchial Intubation
71/87
71
Complications during larngoscopy and intuation
3. Esophageal intubation
Causes
Difficult intubation
Improper manipulationInexperienced practitioner
Diagnosis
Absence of bilateral breath sounds, chest
movement, epigastric auscultationReservoir bag not filling
during expiration
Routine monitoring of end-tidal CO2
-
8/14/2019 Thacheal ion and Bronchial Intubation
72/87
72
Complications while the tube is in place
1.1. Endotracheal tube obstructiontube obstruction
Clot, mucus
kinking
2. Inadvertent extubation
bevel against tracheal wall
3. Inadvertent Endobronchial intubation
C li ti hil th t b i i l
-
8/14/2019 Thacheal ion and Bronchial Intubation
73/87
73
Complications while the tube is in place
4. BuckingCauses
Laryngoscopy is performed under
inadequate anesthesia or without the use of muscle
relaxantPrevention
Maintenance of adequate anesthetic depth
Adequate muscle relaxant
Administration of appropriate fentanyl, lidocaineintravenously
before laryngoscopy
C li ti hil th t b i i l
-
8/14/2019 Thacheal ion and Bronchial Intubation
74/87
74
Complications while the tube is in place
5. Bronchospasm
CausesLaryngoscopy is performed under inadequate anesthesia
Aspiration
Treatment
Stop irritate ion at once
Deepening anesthesia with intravenous or inhaled
agents
Administration of aminophylline, steroid, and ketamine
intravenously
Administration of inhaled or IV2-agonists, lidocaine
Pulmonary toilet
Immediate and delayed complications
-
8/14/2019 Thacheal ion and Bronchial Intubation
75/87
75
Immediate and delayed complications
after extubation
1.Laryngospasm
2.Aspiration and foreign body obstraction
Patients with a full stomachTongue falling back to
retropharyngeal wall
3.Tracheal Collapse
4. Pharyngitis, Laryngitis
Immediate and delayed complications
-
8/14/2019 Thacheal ion and Bronchial Intubation
76/87
76
Immediate and delayed complications
after extubation
5. Laryngeal edema, Subglottic edema
6. Vocal cord paralysis
7. Arytenoid cartilage dislocation
8. Maxillary sinusitis
9. Pneumonia
10. Tracheal stenosis
-
8/14/2019 Thacheal ion and Bronchial Intubation
77/87
77
Section 6 Application of Laryngeal Mask Airway
-
8/14/2019 Thacheal ion and Bronchial Intubation
78/87
78
Outline: The laryngeal mask airway (LMA) is aningenious
supraglottic airway device that is designed
to provide and maintain a seal around the laryngeal
inlet for spontaneous ventilation and allow
controlledventilation at modest levels (up to 15 cmH2O) of
positive pressure. The overall role of the LMA in
clinical anesthesia would appear to be somewhat
between that of the face mask and that of the
endotracheal tube.
-
8/14/2019 Thacheal ion and Bronchial Intubation
79/87
79
1.Configuration
Airway mask
Airway tube
-
8/14/2019 Thacheal ion and Bronchial Intubation
80/87
80
LMA is currently available in seven sizes for
neonates, infants, young children, older children,
and small, normal, and large adults.
-
8/14/2019 Thacheal ion and Bronchial Intubation
81/87
81
2.Method of use
-
8/14/2019 Thacheal ion and Bronchial Intubation
82/87
82
-
8/14/2019 Thacheal ion and Bronchial Intubation
83/87
83
3.Advantages and indications
Be used as a substitute for the classic
mask airway to eliminate the presence of a
relatively large mask and practitioners
hand that may interfere with surgical
access.
To establish an emergency airway in
awkward settings for intubation such as thelateral or prone
positions.
3 Ad d i di i
-
8/14/2019 Thacheal ion and Bronchial Intubation
84/87
84
3.Advantages and indications
Be employed to establish an airway inthe patient in whom either
mask ventilation
or tracheal intubation is difficult.
Be used toprovide a conduit to facilitate
fiberoptic, gum bougie-guided or blind oral
tracheal intubation.
-
8/14/2019 Thacheal ion and Bronchial Intubation
85/87
85
-
8/14/2019 Thacheal ion and Bronchial Intubation
86/87
86
4.Disadvantages and contraindications
Pulmonary aspiration, laryngospasm, soft tissue injury.Need
forneck extensionin the patient with cervical
spine disorder.Failure to function properly in the presence
oflocal
pharyngeal orlaryngeal disease.In patients withdiminished
pulmonary compliance or
increased airway resistance, adequate ventilation may
not be possible because of the high inflation pressures
required and the resultant leaks.
Contraindicatedin any of the conditions associatedwith an
increased risk forregurgitation and aspiration.
-
8/14/2019 Thacheal ion and Bronchial Intubation
87/87
Thank You