Embed Size (px)
Citation preview
Prof. Romain Seil, MD, PhD
Centre Hospitalier
de Luxembourg Orthopaedic
Surgery
Sports Medicine
Research Laboratory
Centre de Recherche
Public – Santé,
Luxembourg
Management of ACL injuries in
the skeletally immature patient
5th course of advanced surgery of the knee
Val d’Isère, 02-2014
crp-sante.lu 2
Disclosures
chl.lu
None !
crp-sante.lu 3 3
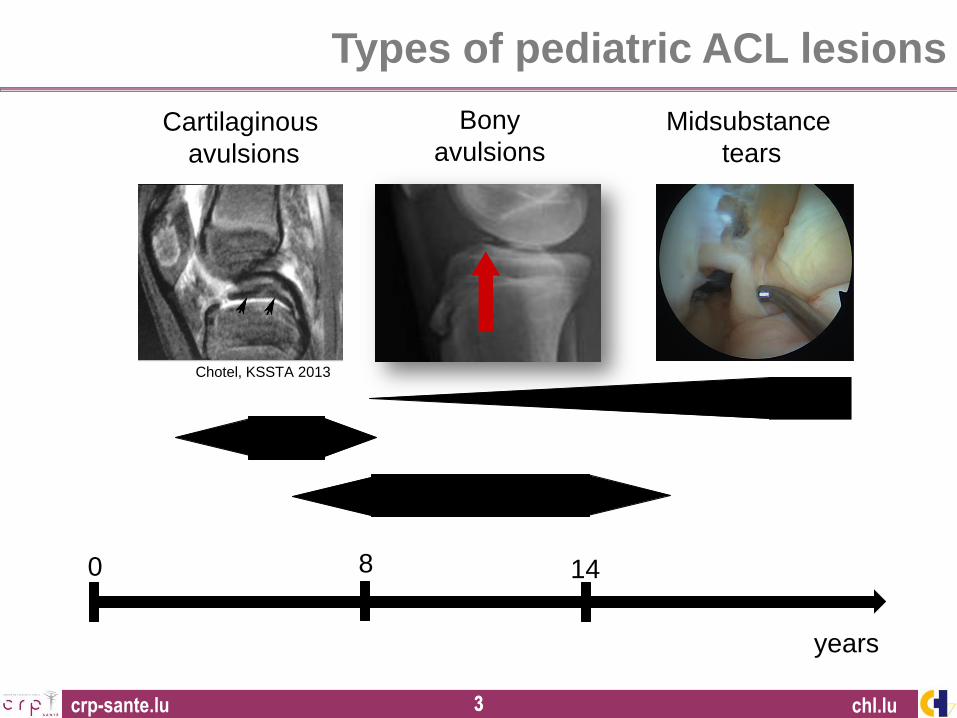
Types of pediatric ACL lesions
chl.lu
0 8 14
Bony
avulsions
years
Midsubstance
tears
Cartilaginous
avulsions
Chotel, KSSTA 2013
crp-sante.lu 4
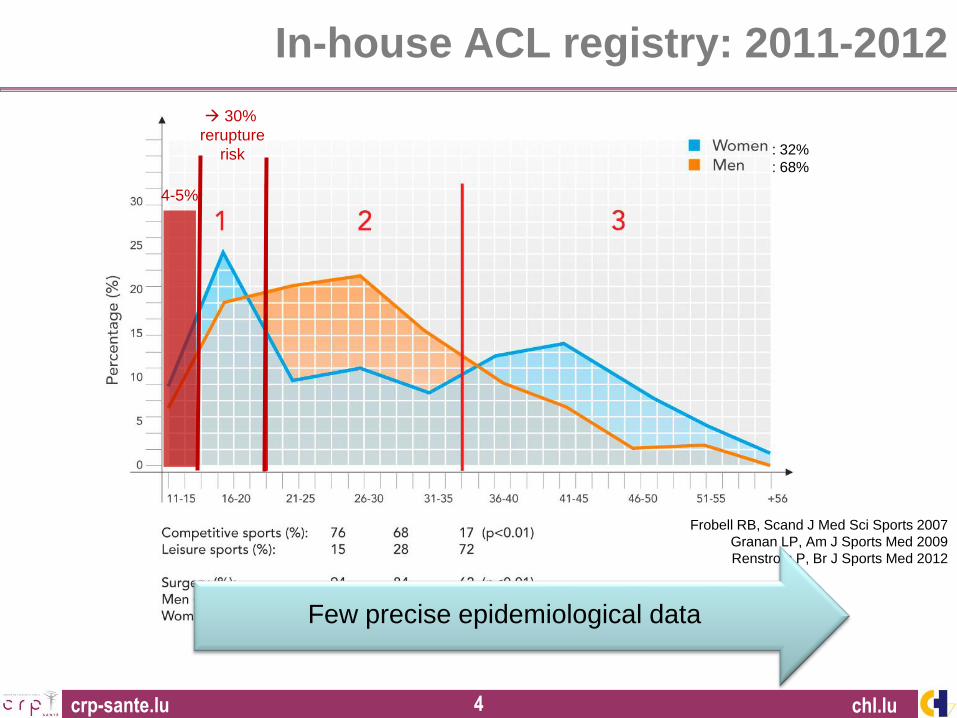
In-house ACL registry: 2011-2012
: 32%
: 68%
Frobell RB, Scand J Med Sci Sports 2007
Granan LP, Am J Sports Med 2009
Renstrom P, Br J Sports Med 2012
chl.lu
Few precise epidemiological data
4-5%
30%
rerupture
risk
crp-sante.lu 5
Boys
Girls
Gro
wth
sp
ee
d
1
2
3
4
5
6K
ne
e la
xity (
mm
)
0
20
40
60
80
100
120
140
9 10 11 12 13 14 15 16 17 18 19 20 21
Nu
mb
er
of
surg
erie
s /
yea
r
Age (years)
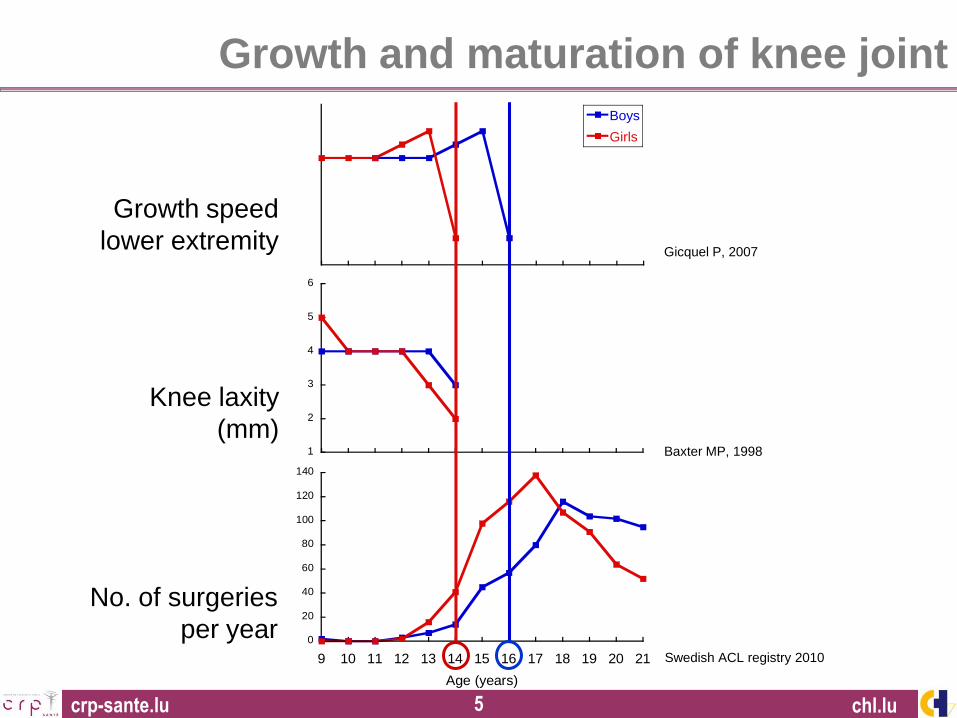
Baxter MP, 1998
Gicquel P, 2007
Swedish ACL registry 2010
Growth speed
lower extremity
Knee laxity
(mm)
No. of surgeries
per year
chl.lu
Growth and maturation of knee joint
crp-sante.lu 6 6
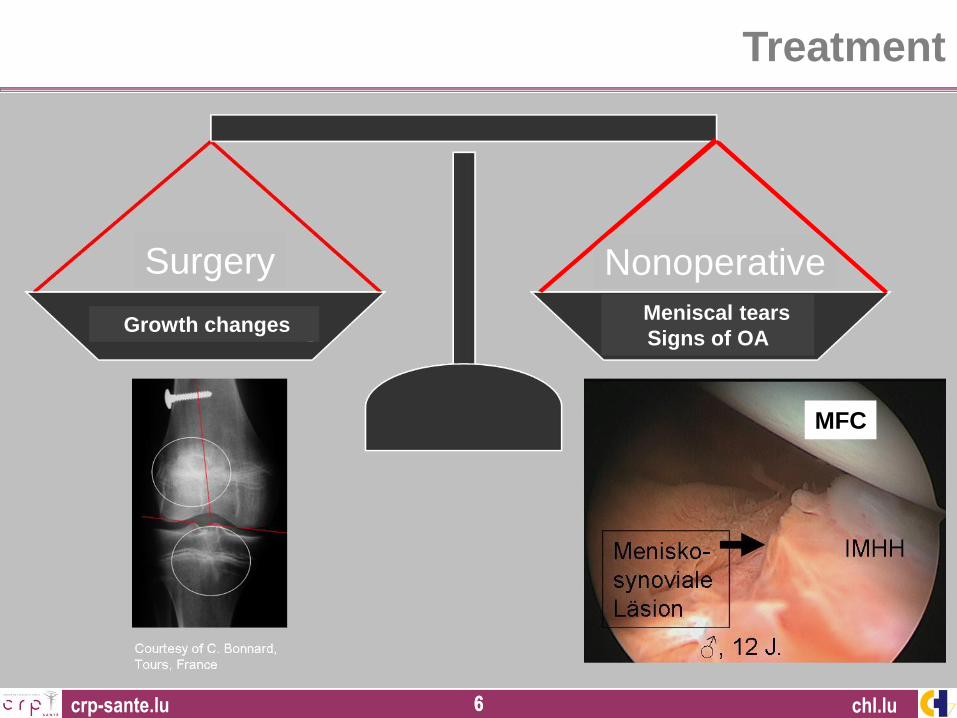
Treatment
chl.lu
Surgery Nonoperative
Growth changes Meniscal tears
Signs of OA
MFC
crp-sante.lu 7 7
Treatment
chl.lu
Low treatment evidence
crp-sante.lu 8 8
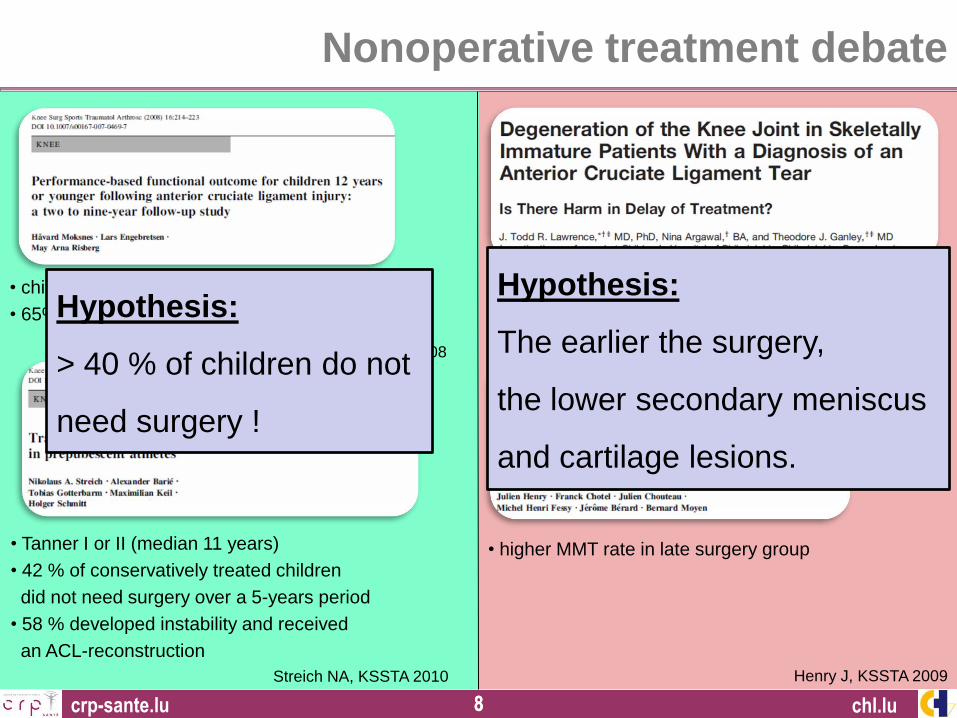
Nonoperative treatment debate
chl.lu
• children < 12 years, no surgery
• 65% returned to pre-injury level of sport
Streich NA, KSSTA 2010
• Tanner I or II (median 11 years)
• 42 % of conservatively treated children
did not need surgery over a 5-years period
• 58 % developed instability and received
an ACL-reconstruction
Moksnes H, KSSTA 2008
• children < 14 years, surgery
• more medial meniscus & cartilage lesions
if surgery > 3 months after injury
Henry J, KSSTA 2009
• higher MMT rate in late surgery group
Lawrence J, AJSM 2011
Hypothesis:
The earlier the surgery,
the lower secondary meniscus
and cartilage lesions.
Hypothesis:
> 40 % of children do not
need surgery !
crp-sante.lu 9 9 chl.lu
Nonoperative treatment debate
Patients’ & families’ adherence to:
• Less active lifestyle
• Damocles sword of later surgery and
subsequent meniscus tear / cartilage
lesions
• Level II sports
• Brace
Functional tests
Reliability ?
Sensibility ?
Limited option for some patients & their family
crp-sante.lu 10 10
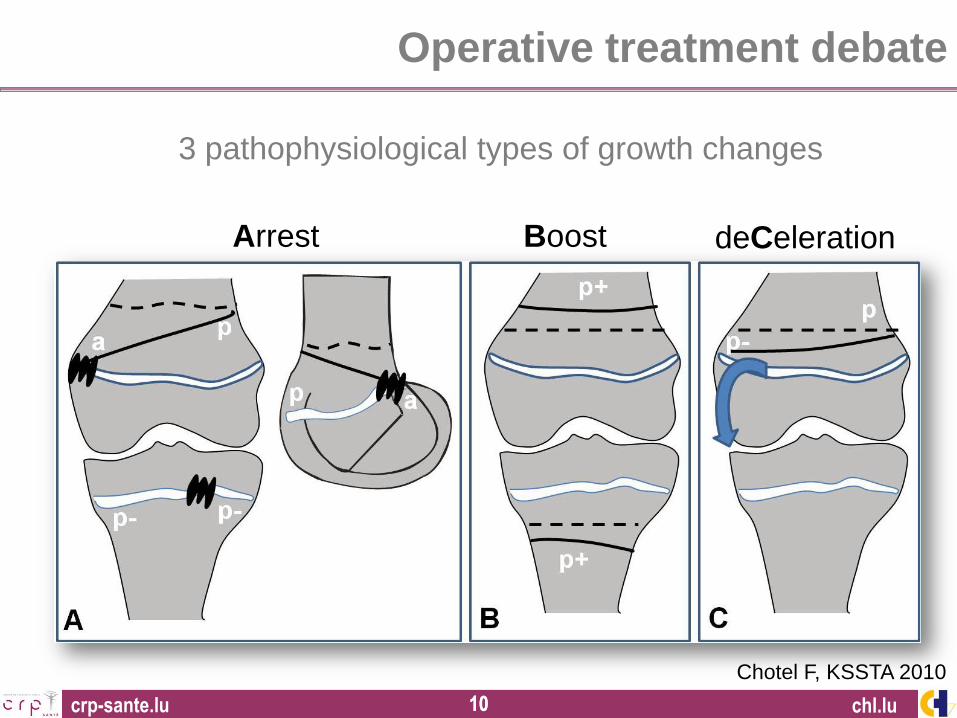
Growth arrest 3 pathophysiological types of growth changes
Chotel F, KSSTA 2010
Arrest Boost deCeleration
chl.lu
Operative treatment debate
crp-sante.lu 11 11
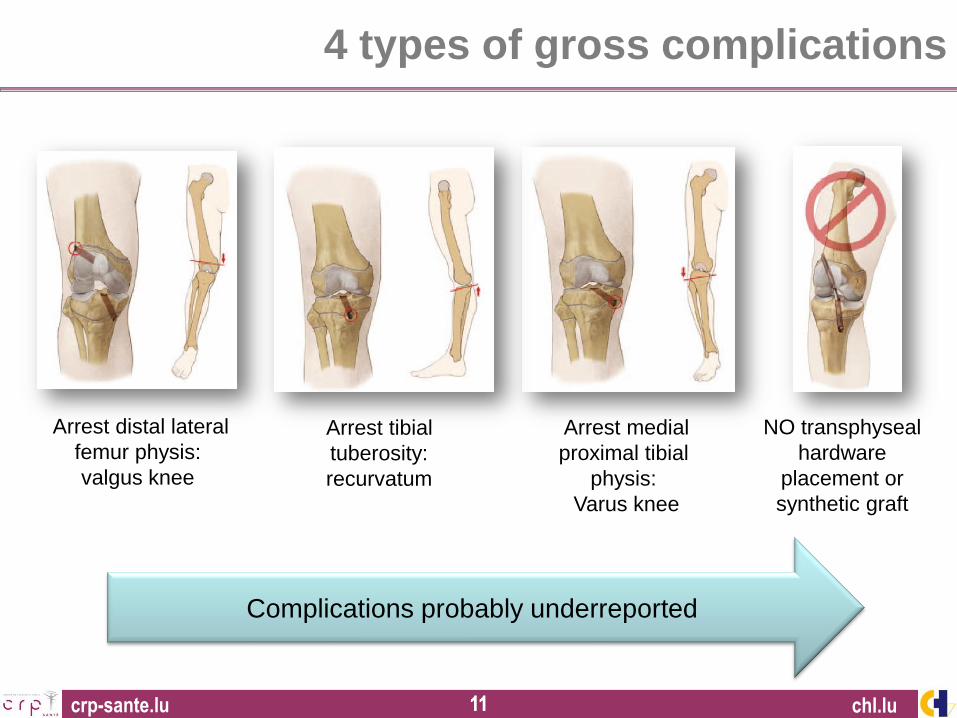
4 types of gross complications
chl.lu
Arrest distal lateral
femur physis:
valgus knee
Arrest tibial
tuberosity:
recurvatum
Arrest medial
proximal tibial
physis:
Varus knee
NO transphyseal
hardware
placement or
synthetic graft
Complications probably underreported
crp-sante.lu 12 12
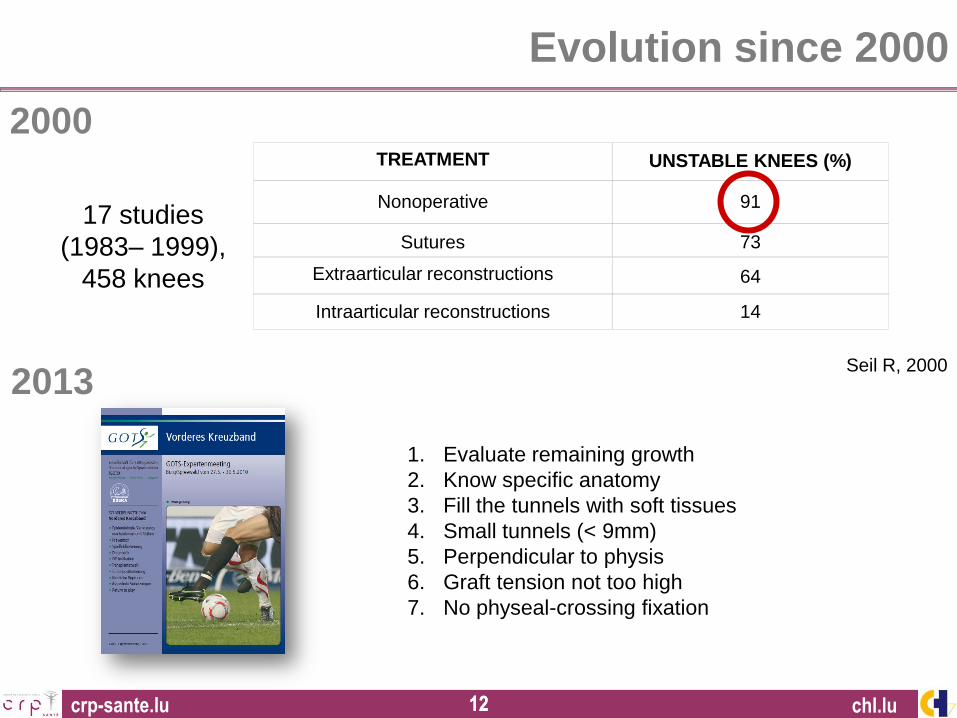
Evolution since 2000
1. Evaluate remaining growth
2. Know specific anatomy
3. Fill the tunnels with soft tissues
4. Small tunnels (< 9mm)
5. Perpendicular to physis
6. Graft tension not too high
7. No physeal-crossing fixation
chl.lu
TREATMENT UNSTABLE KNEES (%)
Nonoperative 91
Sutures 73
Extraarticular reconstructions 64
Intraarticular reconstructions 14
17 studies
(1983– 1999),
458 knees
Seil R, 2000
2000
2013
crp-sante.lu 13 13
Treatment algorithm
Isolated ACL tear:
NO early reconstruction !
• Explanations +++
• Rehabilitation for 3-6 mo.
• Limitation of physical activity
• Close FU
• (Brace)
Indication for surgery:
1. If primary meniscal tear
2. @ skeletal maturity
3. If secondary meniscus tear
4. If functional instability
5. High sports demand (?)
chl.lu
No international consensus,
expert-opinion level discussions
crp-sante.lu 14 14
Preoperative evaluation: diagnostic pitfalls
chl.lu
Pivot-shift test:
Hefti F, Muller W 1993
Frequently pathologic
in healthy children
Lachman test:
High physiologic laxity in children !
Baxter MP, J Ped Orthop, 1998
Haemarthrosis:
• 1/3 ligamentous tears (♂>♀)
• 1/3 patella dislocations (♀>♂)
• 1/3 meniscal tears
Luhmann SJ, 2003
crp-sante.lu 15 15
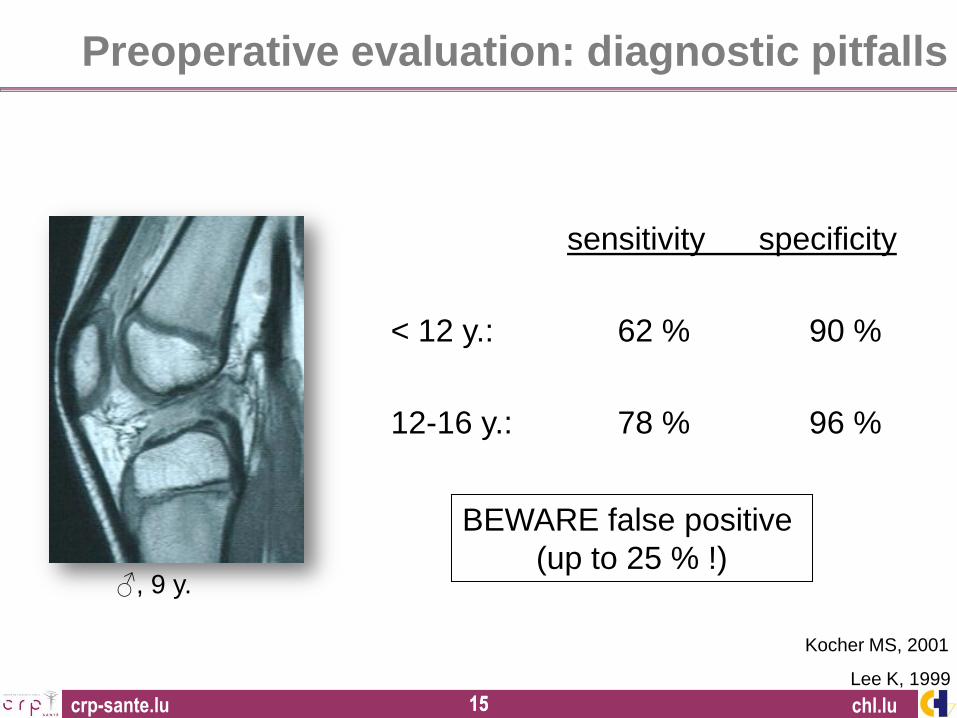
Kocher MS, 2001
sensitivity specificity
< 12 y.: 62 % 90 %
12-16 y.: 78 % 96 %
BEWARE false positive
(up to 25 % !) ♂, 9 y.
Lee K, 1999
chl.lu
Preoperative evaluation: diagnostic pitfalls
crp-sante.lu 16 16
Preoperative evaluation: functional testing
Moksnes H 2008
chl.lu
Current hop tests not specific enough
crp-sante.lu 17 17
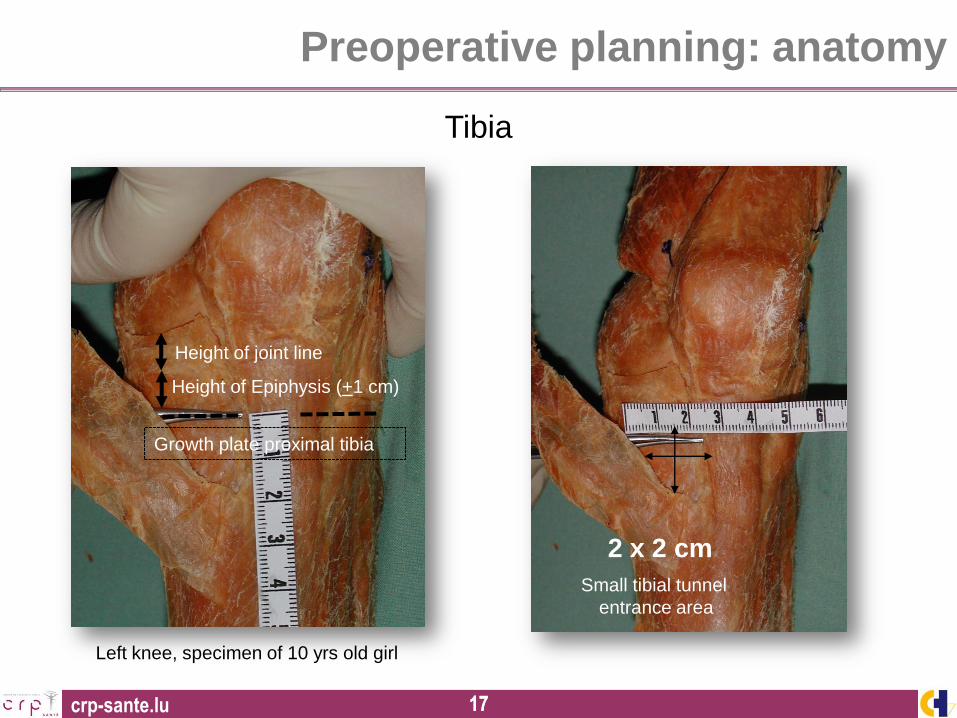
Height of joint line
Growth plate proximal tibia
Height of Epiphysis (+1 cm)
Tibia
Left knee, specimen of 10 yrs old girl
2 x 2 cm
Small tibial tunnel
entrance area
Preoperative planning: anatomy
crp-sante.lu 18 18
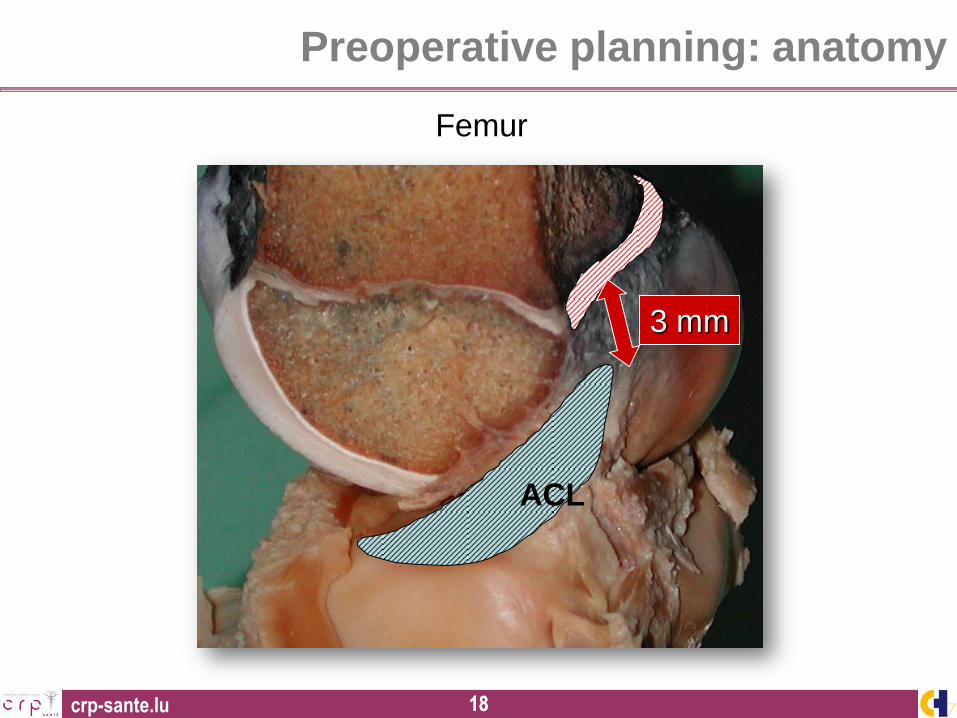
3 mm
ACL
Femur
Preoperative planning: anatomy
crp-sante.lu 19 19
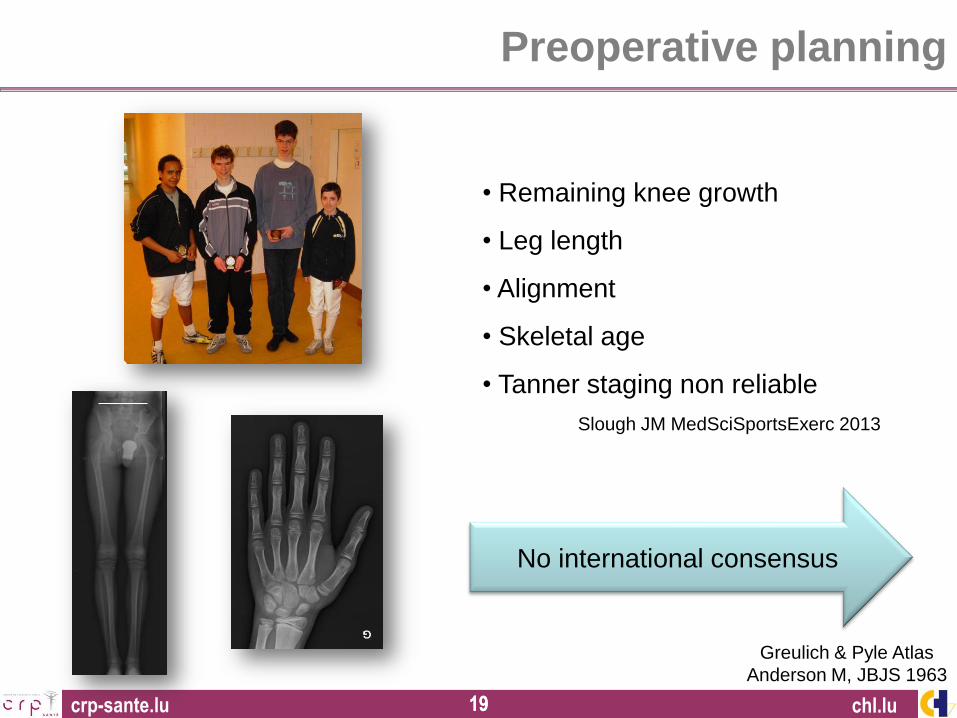
Preoperative planning
chl.lu
• Remaining knee growth
• Leg length
• Alignment
• Skeletal age
• Tanner staging non reliable
Slough JM MedSciSportsExerc 2013
Greulich & Pyle Atlas
Anderson M, JBJS 1963
No international consensus
crp-sante.lu 20 20
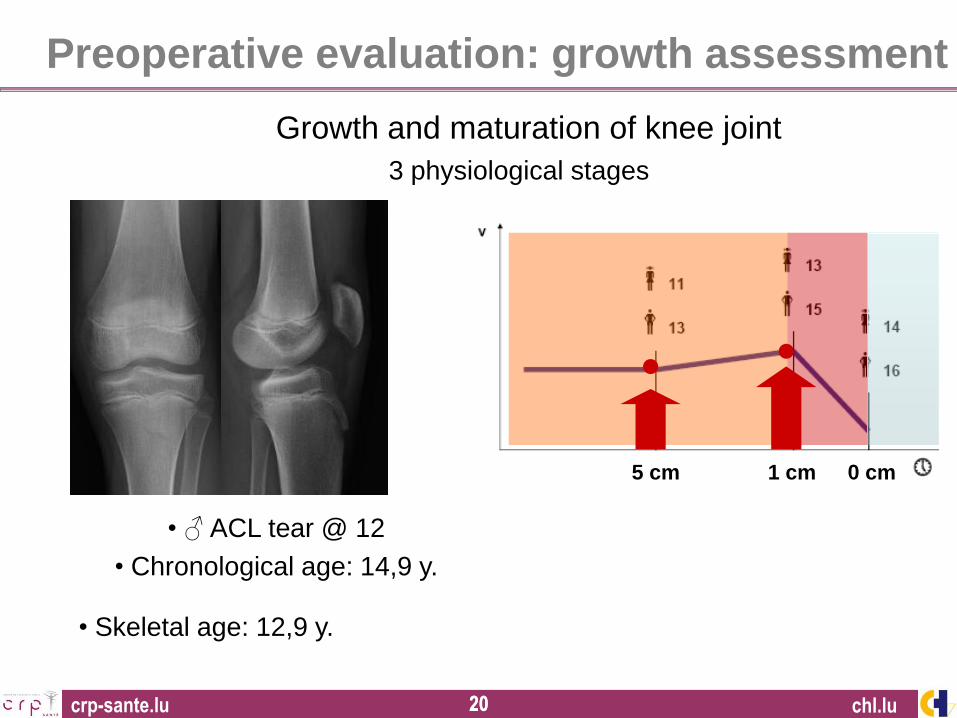
5 cm 1 cm 0 cm
• Skeletal age: 12,9 y.
• ♂ ACL tear @ 12
• Chronological age: 14,9 y.
chl.lu
3 physiological stages
Growth and maturation of knee joint
Preoperative evaluation: growth assessment
crp-sante.lu 21 21
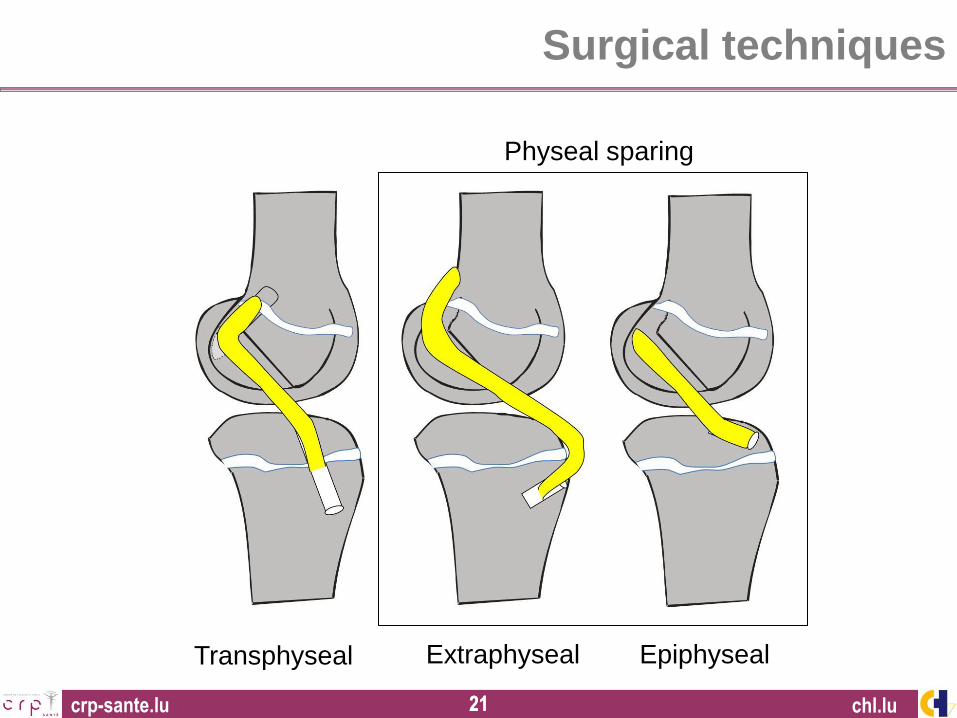
Surgical techniques
Transphyseal Extraphyseal Epiphyseal
chl.lu
Physeal sparing
crp-sante.lu 22 22
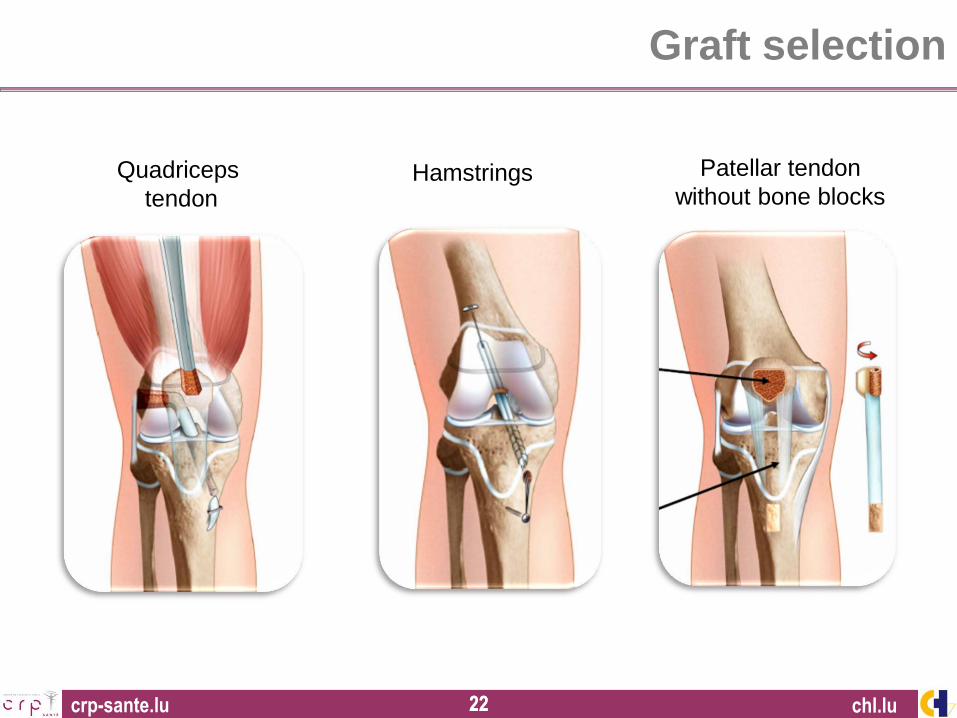
Quadriceps
tendon
chl.lu
Graft selection
Hamstrings Patellar tendon
without bone blocks
crp-sante.lu 23 23
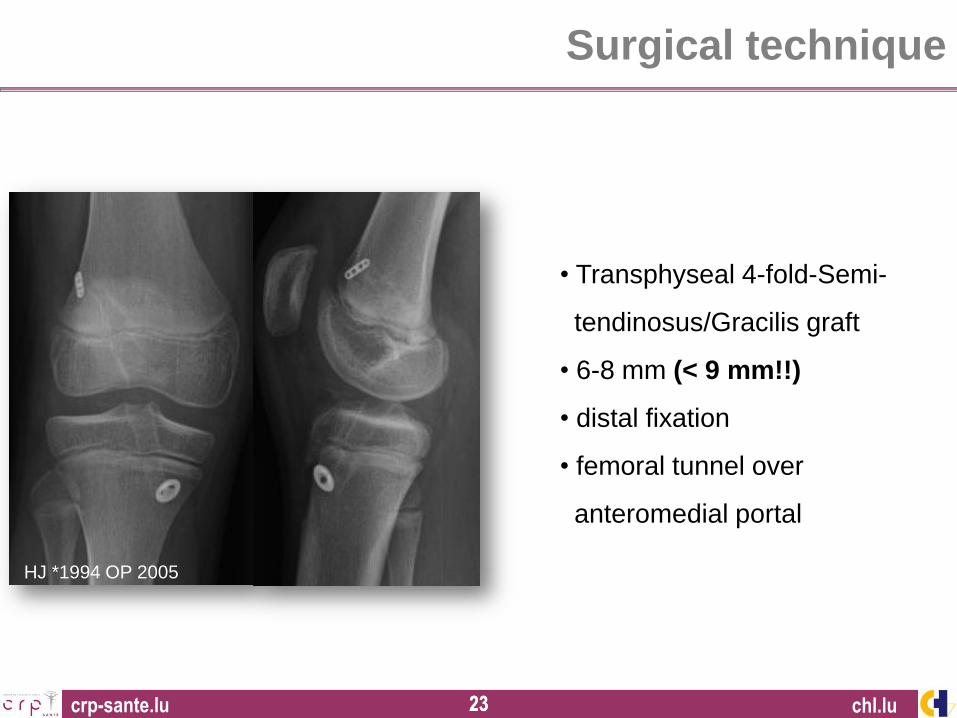
HJ *1994 OP 2005
• Transphyseal 4-fold-Semi-
tendinosus/Gracilis graft
• 6-8 mm (< 9 mm!!)
• distal fixation
• femoral tunnel over
anteromedial portal
chl.lu
Surgical technique
crp-sante.lu 24 24
Surgical technique
chl.lu
crp-sante.lu 25 25
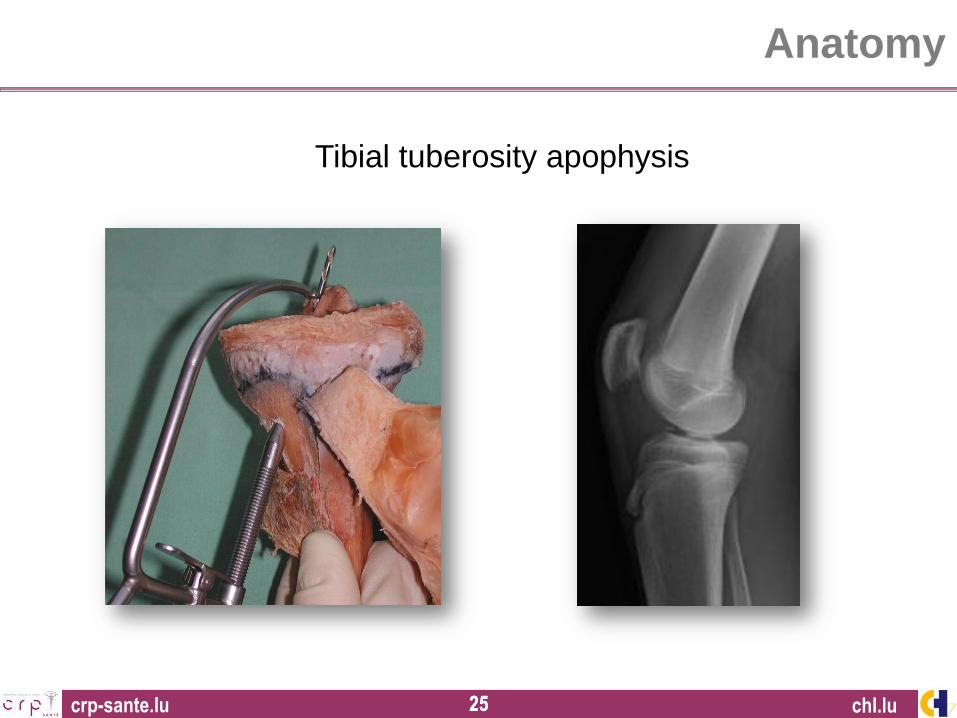
Tibial tuberosity apophysis
Anatomy
chl.lu
crp-sante.lu 26 26
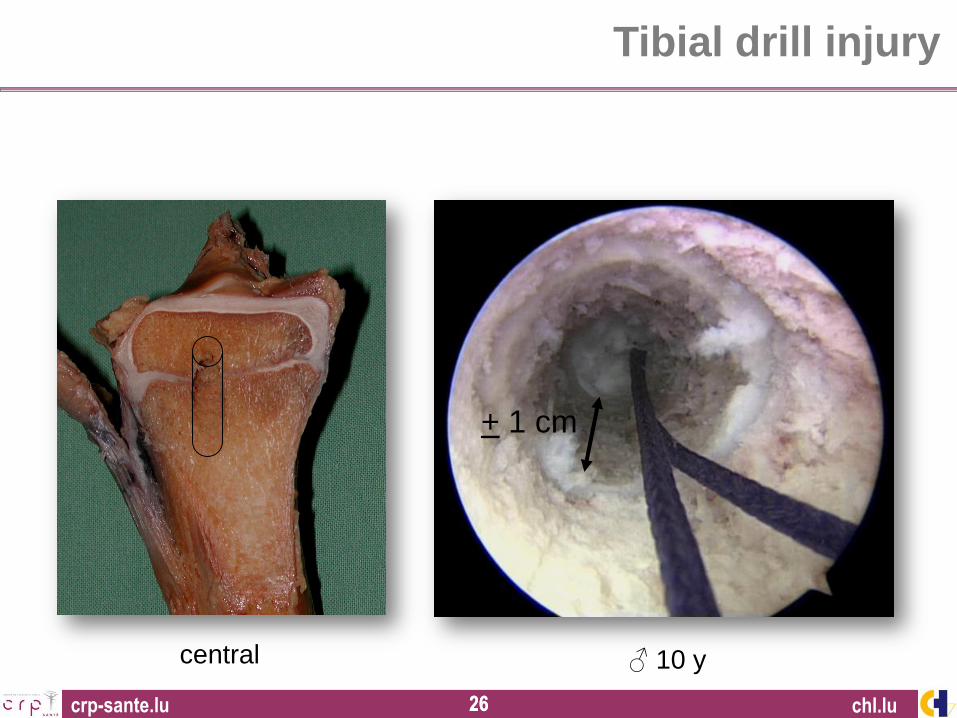
central
Tibial drill injury
♂ 10 y
+ 1 cm
chl.lu
crp-sante.lu 27 27
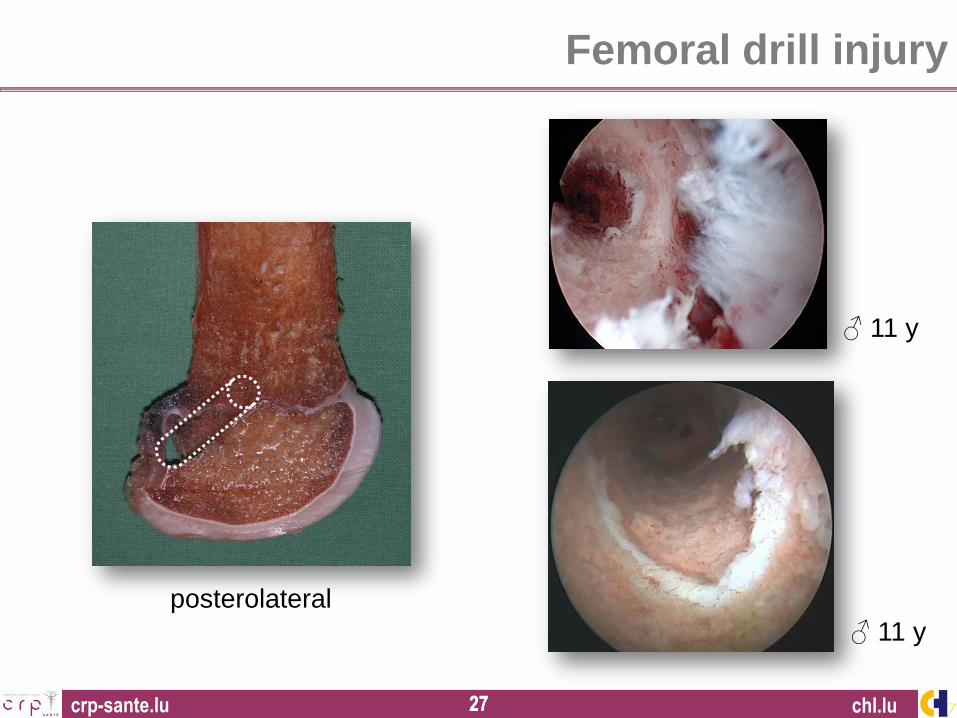
posterolateral
Femoral drill injury
chl.lu
♂ 11 y
♂ 11 y
crp-sante.lu 28 28
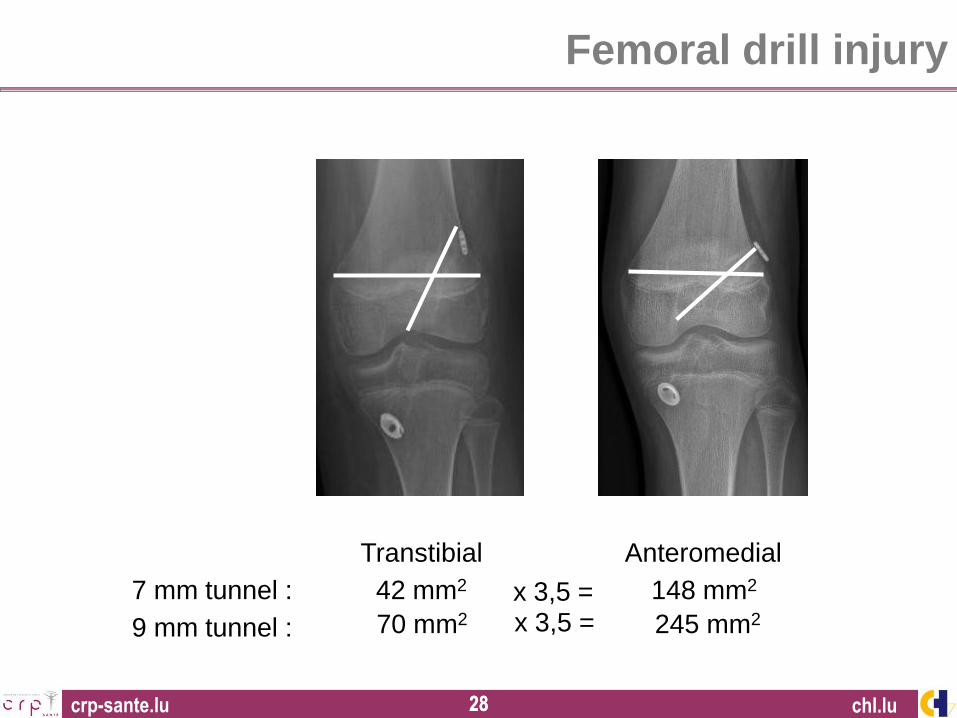
Transtibial
Anteromedial
9 mm tunnel : 70 mm2 245 mm2
7 mm tunnel : 42 mm2 148 mm2
Femoral drill injury
x 3,5 = x 3,5 =
chl.lu
crp-sante.lu 29 29
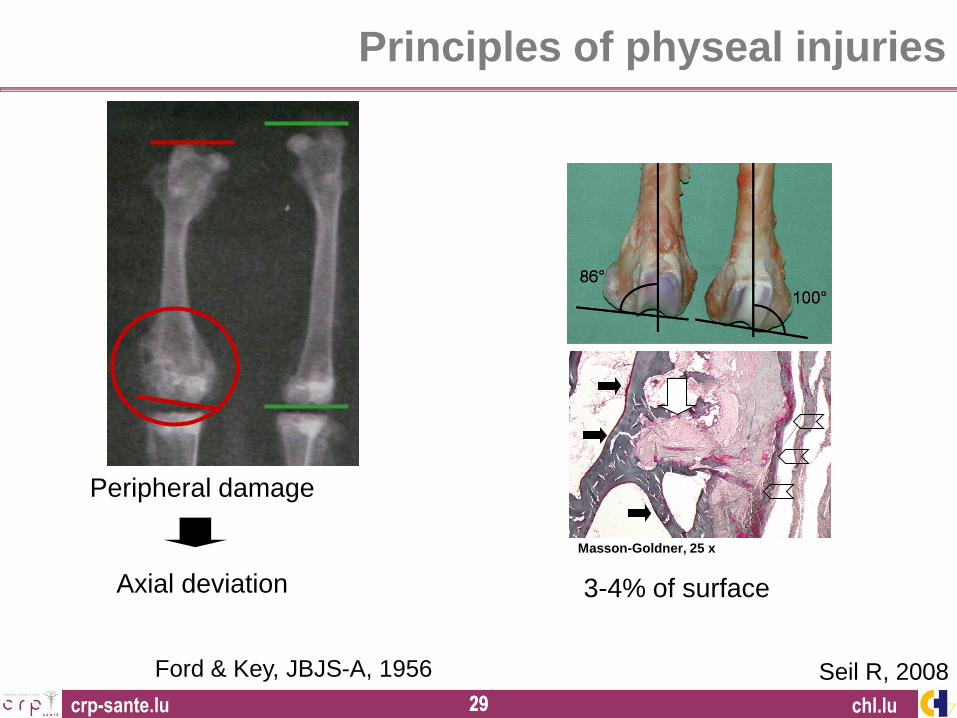
Ford & Key, JBJS-A, 1956
Peripheral damage
Axial deviation
Principles of physeal injuries
chl.lu
3-4% of surface
Seil R, 2008
Masson-Goldner, 25 x
crp-sante.lu 30 30
Isolated ACL replacement:
- 6 weeks brace
- FWB
- Free ROM
- Return to pivoting sports 9-12 months
Meniscal repair:
- 6 weeks brace
- 6 w. 0-0-90°
- 6 w. FWB in extension
Rehabilitation
1 y. postop.
chl.lu
crp-sante.lu 31 31
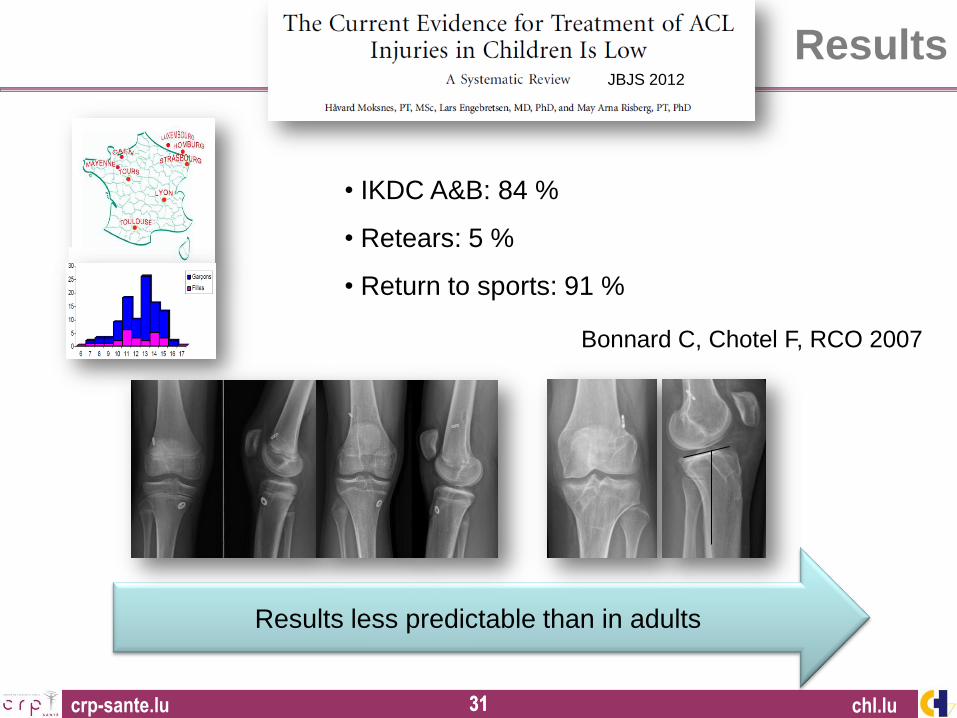
Bonnard C, Chotel F, RCO 2007
Results
• IKDC A&B: 84 %
• Retears: 5 %
• Return to sports: 91 %
chl.lu
JBJS 2012
Results less predictable than in adults
crp-sante.lu 32 32
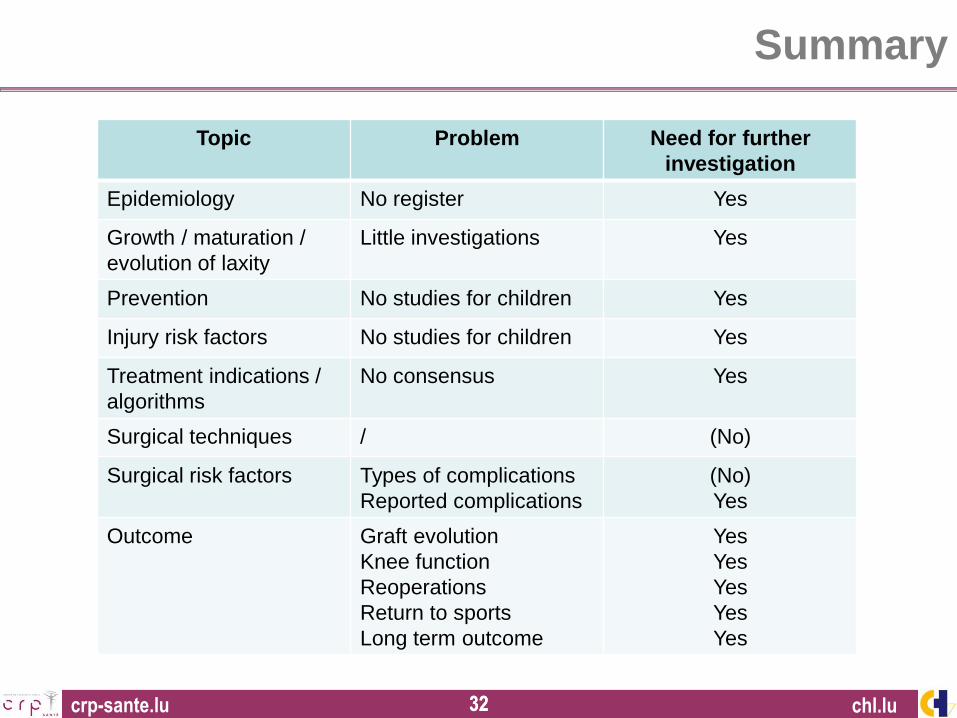
Summary
chl.lu
Topic Problem Need for further
investigation
Epidemiology No register Yes
Growth / maturation /
evolution of laxity
Little investigations Yes
Prevention No studies for children Yes
Injury risk factors No studies for children Yes
Treatment indications /
algorithms
No consensus Yes
Surgical techniques / (No)
Surgical risk factors Types of complications
Reported complications
(No)
Yes
Outcome Graft evolution
Knee function
Reoperations
Return to sports
Long term outcome
Yes
Yes
Yes
Yes
Yes
crp-sante.lu 33 33
Conclusions
chl.lu
Pediatric ACL reconstructions are safe if technically correct
But
Complications may occur
Some children do not need an immediate ACL reconstruction
crp-sante.lu 34 34
Conclusions
chl.lu
The art of pediatric ACL management is to choose:
The right child & family
The right indication
The right moment for reconstruction
The right technique
crp-sante.lu 35
Pediatric ACL Monitoring Initiative (PAMI)
Håvard Moksnes
Lars Engebretsen
Romain Seil
• Online survey on the current treatment of pediatric ACL injuries
• Planned submitted to ESSKA members and affiliates
• 2500 recipients, 500 answers

crp-sante.lu 36 36
16th ESSKA Congress
May 14-17, 2014
AMSTERDAM / THE NETHERLANDS
CONGRESS PRESIDENT
C. Niek van Dijk
ESSKA PRESIDENT
João Espregueira-Mendes
SCIENTIFIC CHAIRMEN
Stefano Zaffagnini
Roland Becker
Gino Kerkhoffs
ORGANISER
www.esska-congress.org















![Winners List - Motor Car [ACL] (motor car).pdfareej 14 Motor Car ACL 016 2,000 15,000 ACL-35202****9025-016 Shamaila Shafique 15 Motor Car ACL 017 2,000 10,100 ACL-35202****4553-017](https://img.pdfslide.us/doc/110x75/60e41d8b31ed9359ad784c32/winners-list-motor-car-acl-motor-carpdf-areej-14-motor-car-acl-016-2000.jpg)












